web viewthis restructuring included reorganization and ... interpretation of this information should...
TRANSCRIPT
A Report to the County Manager on the Local Management Entity (LME) and
LME Purchase of Services
2/26/10
Carlyle Johnson, Ph.D.LME AdministratorWCHS Local Management Entity401 E. Whitaker Mill Rd.Raleigh, NC 27608Tel: (919) 857-3787 Fax: (919) 856-5674 [email protected]
1

OVERVIEW Effective July 1, 2009, WCHS LME and Behavioral Health programs completed a reorganization to better align staffing with statutory requirements, ensure separation of LME and direct service functions and improve performance of LME functions. This restructuring included reorganization and refinement of Wake County HS & ES Board subcommittees and significant changes in LME and Behavioral Health Services organizational structure, leadership, supervisory roles, staff assignments, and physical location of staff.
This report provides a summary of the Local Management Entity (LME) and LME Purchase of Services programs as they are currently configured and provides a comparison of current and historical data to identify trends. Interpretation of this information should consider the differences between past and current organizational structures and functions, particularly with respect to comparison of budgets and programs such as Care Coordination and Screening/Triage and Referral (Access Center) that have shifted from LME/Services hybrid programs to separate services and LME programs.
For the purpose of this report, the LME Purchase of Service program includes those services that are purchased from community providers other than Wake County Human Services. Since WCHS Behavioral Health programs will be reviewed in a separate report, they are not covered in the review of the LME Purchase of Services program below.
SERVICES PROVIDED
The Wake County Local Management Entity (LME) is responsible for developing and managing a network of mental health, developmental disabilities and substance abuse (MHDDSA) services that enables consumers to live, work and participate in their community to the greatest extent possible. The LME provides 24/7/365 availability of screening, triage and referral for MH/DD/SA services, which are provided through a network of over 135 community service providers in Wake County. It is responsible for coordination of care for consumers transitioning from inpatient and residential treatment and implementation of plans for reducing utilization of state facilities. The LME ensures quality of care through training, technical assistance and collaboration with providers, program development and maintenance, endorsement of providers for Medicaid-funded services, monitoring of service quality, and investigation of complaints. It collaborates with providers, stakeholders and consumers to identify and address community MH/DD/SA needs and to improve the quality and accessibility of care. The Wake LME is also responsible for oversight of services purchased through contractual providers, authorization of services,
2
and management of federal, state and county funds allocated for MH/DD/SA care. The Wake County LME is funded entirely by State MH/DD/SA funding that is allocated for performance of statutorily required LME functions and requirements contained in the DHHS –LME contract.
Wake County Local Management Entity (LME) Purchase of Service funding consists of State, Federal and County funding allocated for purchasing MHDDSA services from a network of community providers. (Additional State, Federal and County MHDDSA funds that are budgeted in other WCHS Behavioral Health Divisions are not covered in this summary). Funds are allocated to specific age and disability groups and are distributed to community providers through Unit Cost Reimbursement (UCR) and Non-UCR contractual payments. Services that are funded through UCR reimbursement are paid based on a ‘fee-for-service’ arrangement, by which providers must request preauthorization for services and are reimbursed only for those services that have been authorized. Most outpatient treatment services are paid using this approach. LME Utilization Management Care Managers authorize services in accordance with the Wake LME’s benefit plans, which are designed to align type, intensity and duration of services with the service needs of prioritized target populations. Non-UCR contracts support programs and services that are not readily funded through a fee-for-service model, and are paid by invoice based on a program budget approved by the LME. Examples of Non-UCR contracts are those that assist with program start-up or those billable service codes that are insufficient to fund the service.
Budget management for this division requires regular monitoring of expenditures, referral and utilization trends, and other aspects of consumer demand and provider capacity monitoring to ensure that all funds are earned and paid to the LME from the State as well as to ensure that expenditures do not exceed available funding.
3

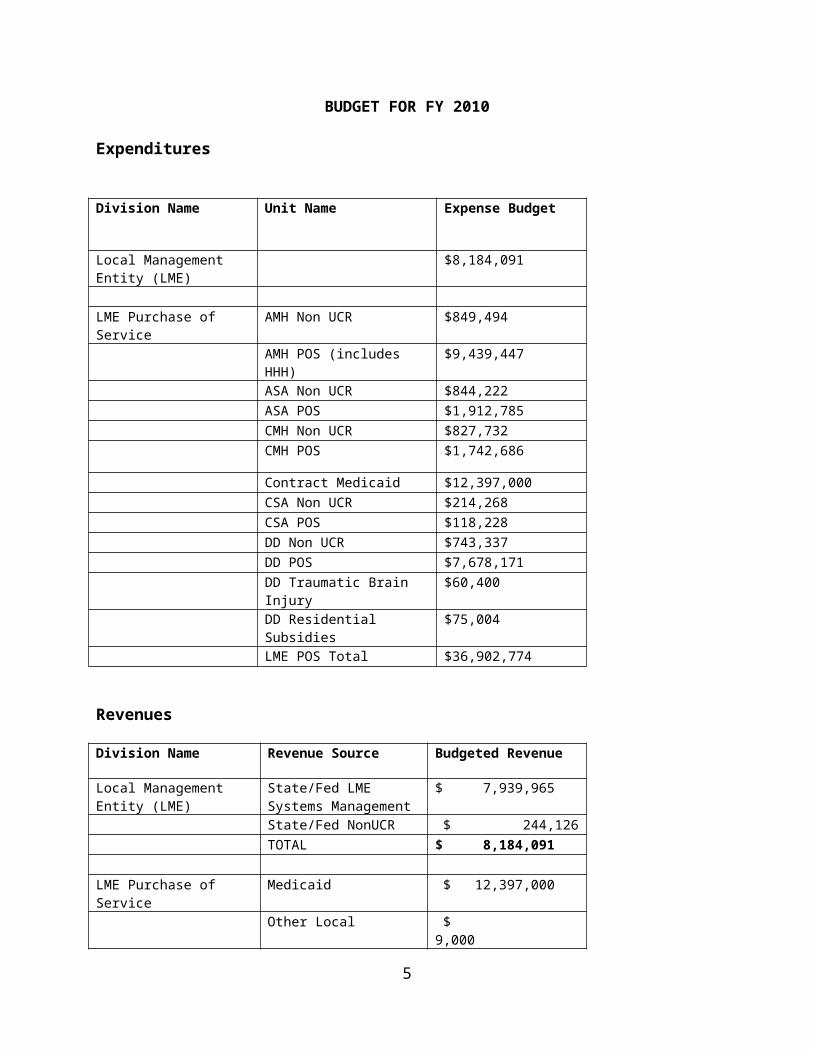
BUDGET FOR FY 2010
Expenditures
Division Name Unit Name Expense Budget
Local Management Entity (LME)
$8,184,091
LME Purchase of Service
AMH Non UCR $849,494
AMH POS (includes HHH)
$9,439,447
ASA Non UCR $844,222 ASA POS $1,912,785 CMH Non UCR $827,732 CMH POS $1,742,686
Contract Medicaid $12,397,000 CSA Non UCR $214,268 CSA POS $118,228 DD Non UCR $743,337 DD POS $7,678,171 DD Traumatic Brain Injury
$60,400
DD Residential Subsidies
$75,004
LME POS Total $36,902,774
Revenues
Division Name Revenue Source Budgeted Revenue
Local Management Entity (LME)
State/Fed LME Systems Management
$ 7,939,965
State/Fed NonUCR $ 244,126 TOTAL $ 8,184,091
LME Purchase of Service
Medicaid $ 12,397,000
Other Local $ 9,000 County Funds-Community $ 278,225 County Funds –Inpatient
$ 6,327,099
St/Fed UCR $ 14,391,122
4
St/Fed NonUCR $ 3,500,328 TOTAL $ 36,902,774
5

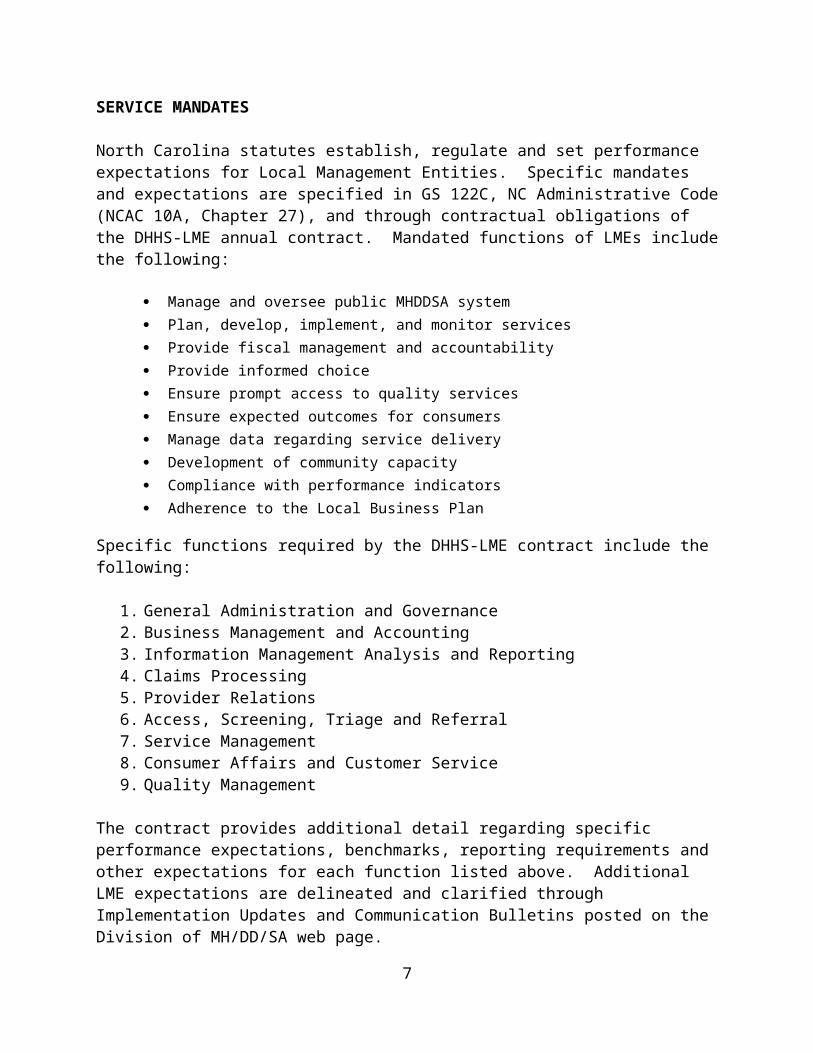
SERVICE MANDATES
North Carolina statutes establish, regulate and set performance expectations for Local Management Entities. Specific mandates and expectations are specified in GS 122C, NC Administrative Code (NCAC 10A, Chapter 27), and through contractual obligations of the DHHS-LME annual contract. Mandated functions of LMEs include the following:
Manage and oversee public MHDDSA system Plan, develop, implement, and monitor services Provide fiscal management and accountability Provide informed choice Ensure prompt access to quality services Ensure expected outcomes for consumers Manage data regarding service delivery Development of community capacity Compliance with performance indicators Adherence to the Local Business Plan
Specific functions required by the DHHS-LME contract include the following:
1. General Administration and Governance2. Business Management and Accounting3. Information Management Analysis and Reporting4. Claims Processing5. Provider Relations6. Access, Screening, Triage and Referral7. Service Management8. Consumer Affairs and Customer Service9. Quality Management
The contract provides additional detail regarding specific performance expectations, benchmarks, reporting requirements and other expectations for each function listed above. Additional LME expectations are delineated and clarified through Implementation Updates and Communication Bulletins posted on the Division of MH/DD/SA web page.
6
7

8
9
10
11
12

13
14

ORGANIZATIONAL UNITS
LME Governance / Administration
The Wake County Local Management Entity (LME) is responsible for developing, managing, coordinating, facilitating and monitoring the provision of mental health, developmental disabilities and substance abuse services in the catchment area (Wake County). The LME Administrator and Medical Director, along with the Managers of the LME Teams listed below make up the LME Management Team
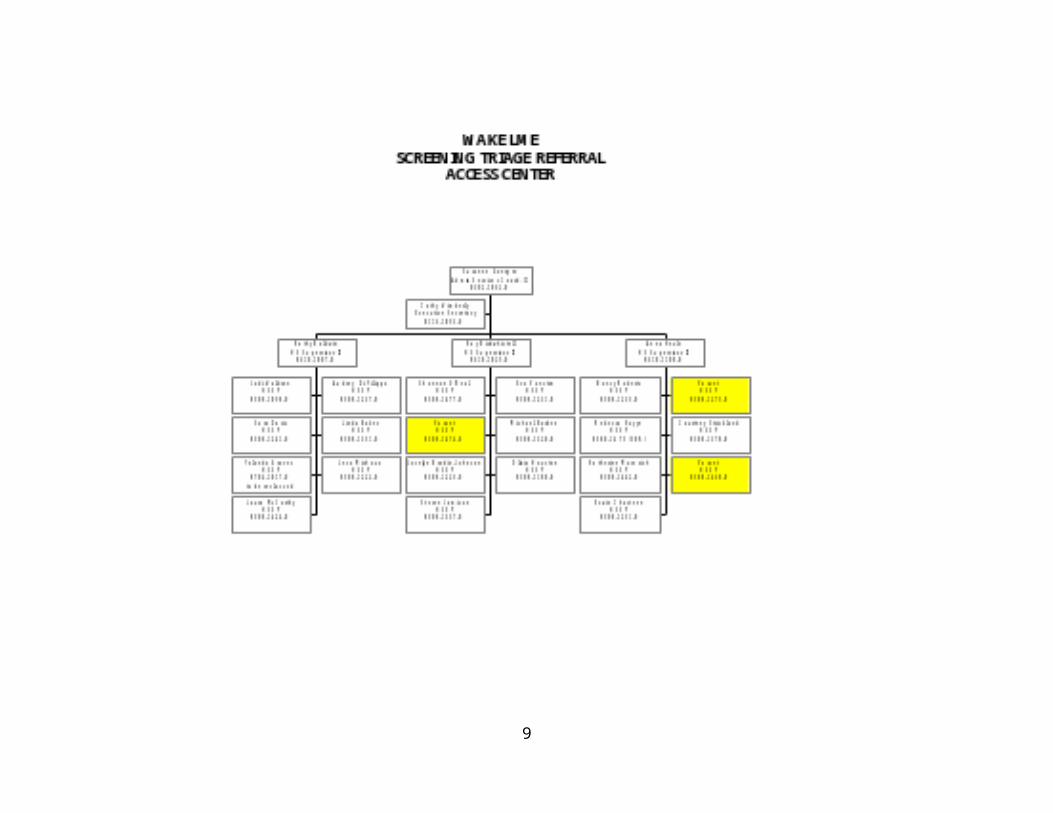
Screening, Triage and Referral (Access Center)
The Access Center is the doorway to MH/DD/SA services in the LME’s system of care. The Access Center provides telephonic screening for mental health, developmental disabilities, and substance abuse issues, 24 hours per day, 7 days a week, including access by toll-free number, TTY, and foreign language interpretation service.
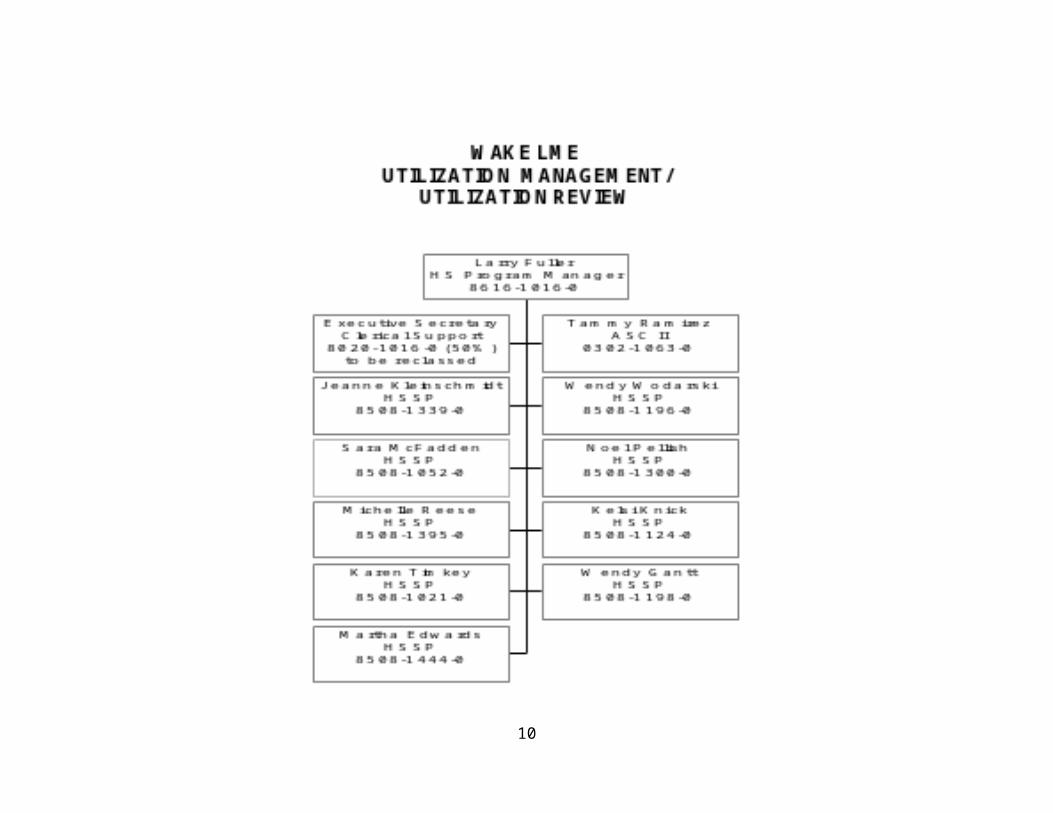
Utilization Review / Utilization Management
Utilization Management is responsible for service utilization review (UR). This includes the authorization and reauthorization of state funded (IPRS) MH/DD/SA services. The UR Care Managers provide consultation with service providers and consumer advocates regarding level-of-care criteria.
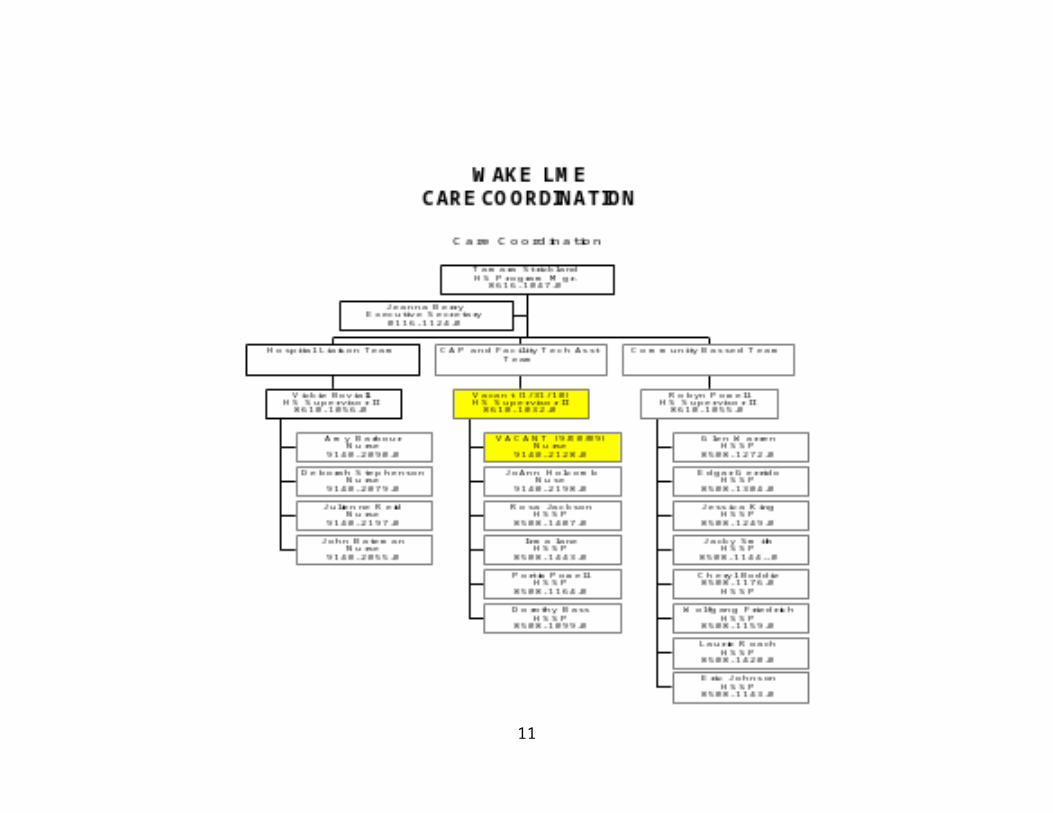
Care Coordination
Care Coordinators provide consultation and technical assistance for providers and consumers. This includes but is not limited to the following: Coordination of transitions from state and local facilities (criminal/juvenile
justice system, psychiatric hospitals, developmental centers, hospitals, nursing facilities)
Ensuring follow-up with hospital discharge instructions Assisting providers with continuity of care and coordination of community
services for high risk, high acuity, and high cost recipients
Network Development
The Network Development Team (NDT) serves as consultants to providers and LME staff. They manage system planning and conceptualization, community collaboration projects, provider recruitment, and the purchase of service budgets. They also support numerous committees and collaboratives including CFAC (Consumer & Family Advisory Committee), CPAC (Community
15
Provider Advisory Committee), the Behavioral Health Collaborative, and the Community Collaborative for Children and Families. The NDT consists of a team of professionals with varying areas of expertise.
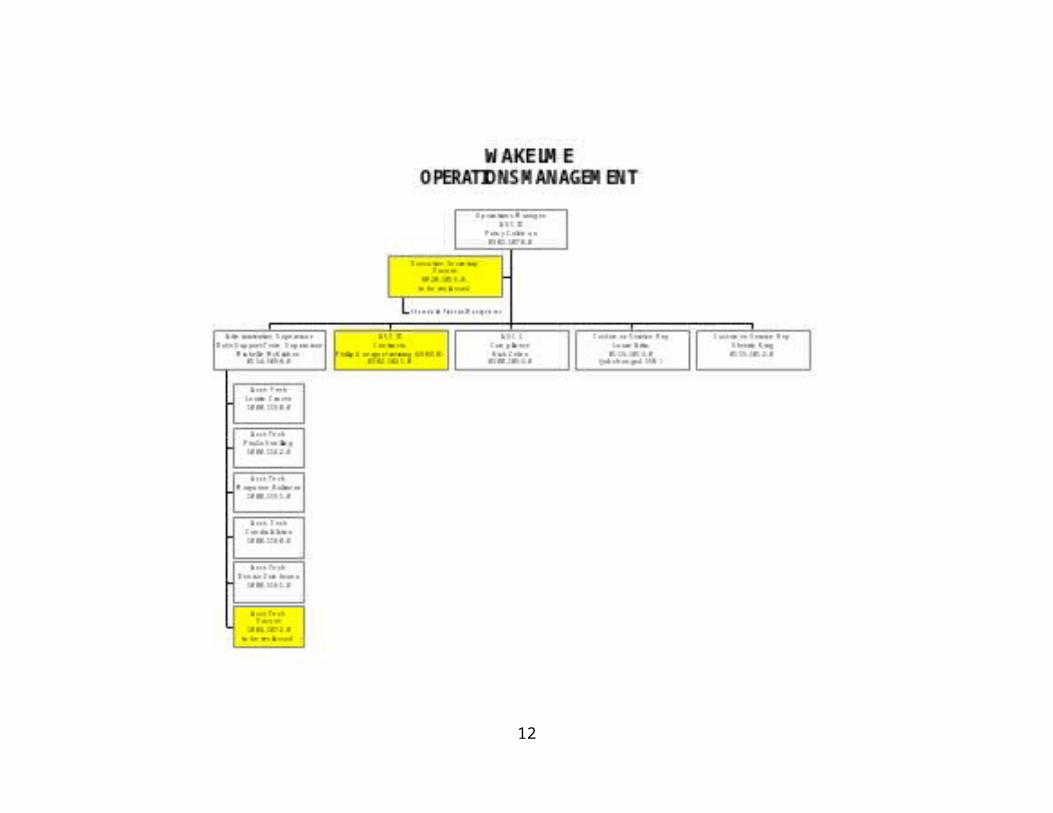
Operations and Financial Management
LME Operations and Financial Management Units are responsible for supporting the other units in the LME by providing financial analysis and projections, program evaluation, tracking consumer demographic and financial data, processing claims, paying invoices, contracting, and working with QM to monitor provider compliance with IPRS service provision rules.
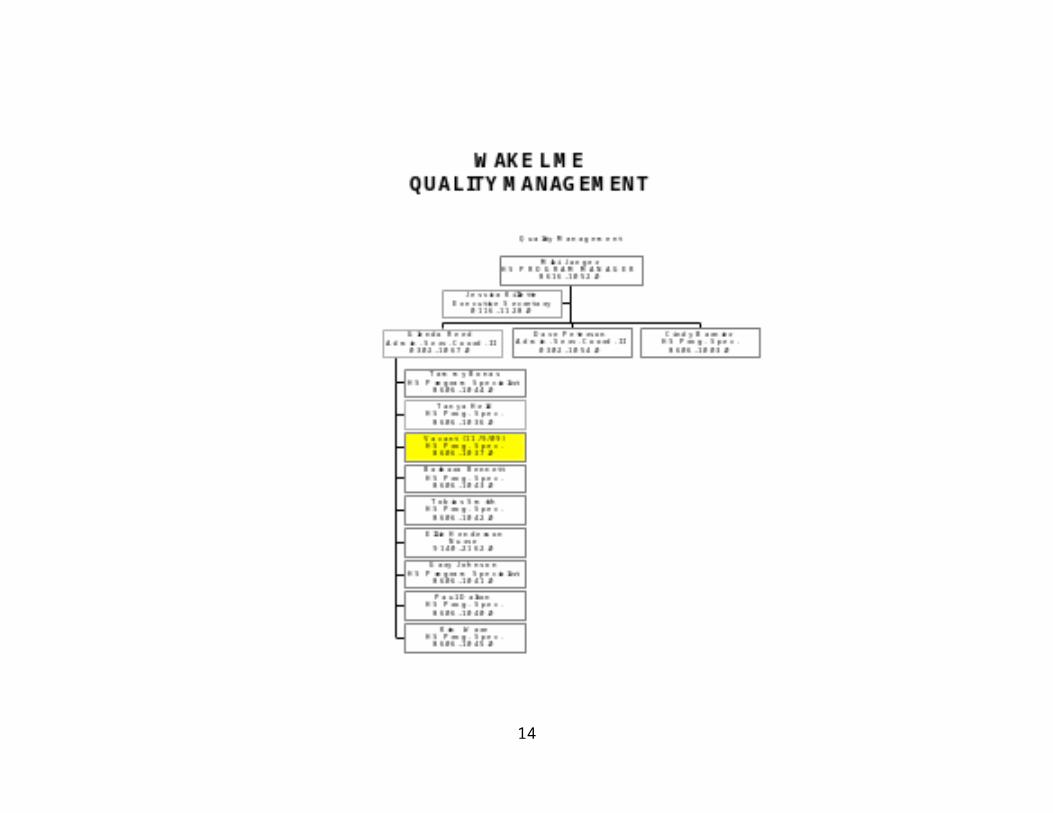
Quality Management
The Quality Management Team monitors services of licensed and non-licensed providers, receives and reviews incident reports, provides endorsement reviews, assists in complaint mediation, and offers provider training and technical assistance.
Information Management
The Information Management unit provides information technology support to the LME, including Avatar systems administration, state reporting, data analysis, data submission, and overall technical support for all LME programs.
16
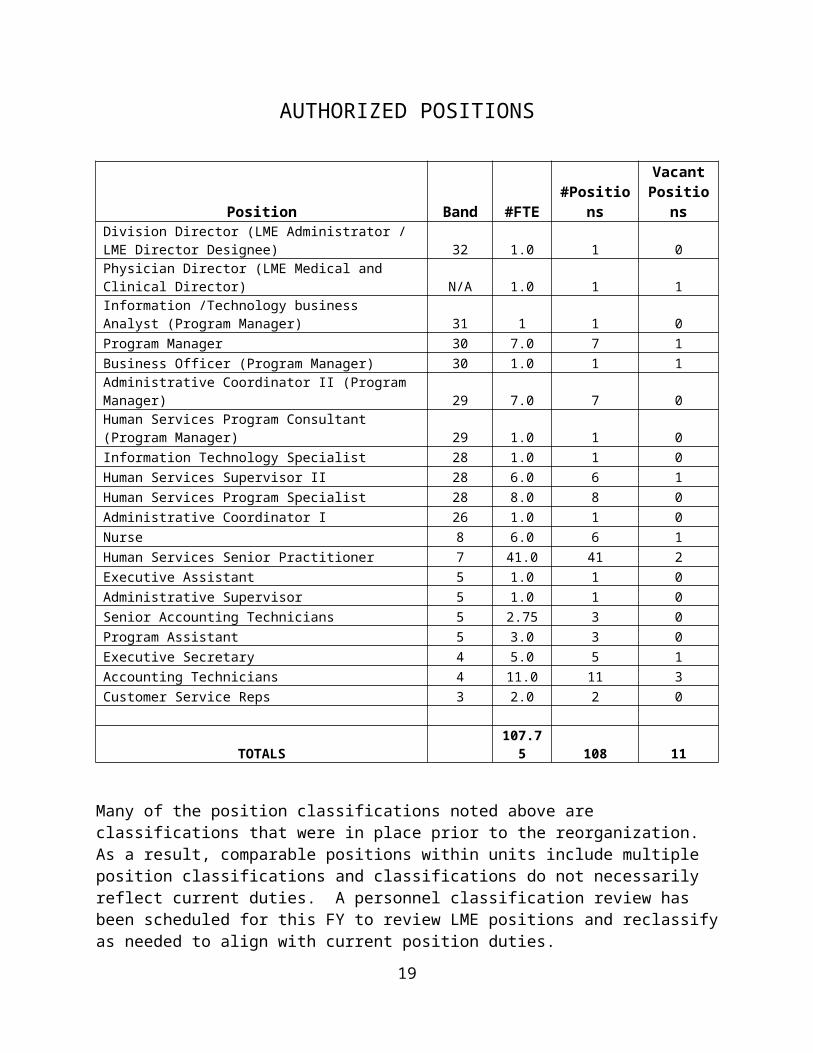
AUTHORIZED POSITIONS
Position Band #FTE #PositionsVacant
PositionsDivision Director (LME Administrator / LME Director Designee) 32 1.0 1 0Physician Director (LME Medical and Clinical Director) N/A 1.0 1 1Information /Technology business Analyst (Program Manager) 31 1 1 0Program Manager 30 7.0 7 1Business Officer (Program Manager) 30 1.0 1 1Administrative Coordinator II (Program Manager) 29 7.0 7 0Human Services Program Consultant (Program Manager) 29 1.0 1 0Information Technology Specialist 28 1.0 1 0Human Services Supervisor II 28 6.0 6 1Human Services Program Specialist 28 8.0 8 0Administrative Coordinator I 26 1.0 1 0Nurse 8 6.0 6 1Human Services Senior Practitioner 7 41.0 41 2Executive Assistant 5 1.0 1 0Administrative Supervisor 5 1.0 1 0Senior Accounting Technicians 5 2.75 3 0Program Assistant 5 3.0 3 0Executive Secretary 4 5.0 5 1Accounting Technicians 4 11.0 11 3Customer Service Reps 3 2.0 2 0
TOTALS 107.75 108 11
Many of the position classifications noted above are classifications that were in place prior to the reorganization. As a result, comparable positions within units include multiple position classifications and classifications do not necessarily reflect current duties. A personnel classification review has been scheduled for this FY to review LME positions and reclassify as needed to align with current position duties.
17

REVENUES AND EXPENDITURES
Current FY budgeted revenues and expenditures are provided on page 4, for both LME and LME Purchase of Service budgets. Given the changes associated with the reorganization of the LME and Services functions, revenue and expenditure data for past years are not easily compared to the current FY budget. For example, LME budgets for past years included funding for combined Crisis/STR and Care Coordination functions that are now split between LME (STR, Care Coordination) and WCHS Behavioral Health (Crisis Services and Bridging Services). Comparisons between current and past budgets are more readily accomplished for the LME Purchase of Service expenditure budgets, although past revenue budgets reflect earnings by program areas that are no longer LME programs.
Expenditure budget data for community-based, non-Medicaid Purchase of Services are as follows:
Budget ActualFY06 16,307,306 $16,245,959FY07 $19,623,797 $16,472,735FY08 $23,512,960 $19,991,622FY09 $22,093,845 $22,642,115FY10 $18,193,555
Note: Does not include pass-through Medicaid or HHH.
FLOW CHARTS
The LME is currently transitioning to a new software system, Netsmart Avatar (and CareLink), that is resulting in numerous changes in processes and work flow for the LME and community providers. Additional changes in business processes have resulted from changes associated with the LME reorganization and the implementation of the Access Center. The LME Provider Operations Manual contains information about procedures and processes that pertain to the LME’s community providers. This manual is being revised to reflect pending changes, and therefore does not currently reflect some of the new processes. This manual is posted on the LME’s website at: http://www.wakegov.com/lme/members.htm
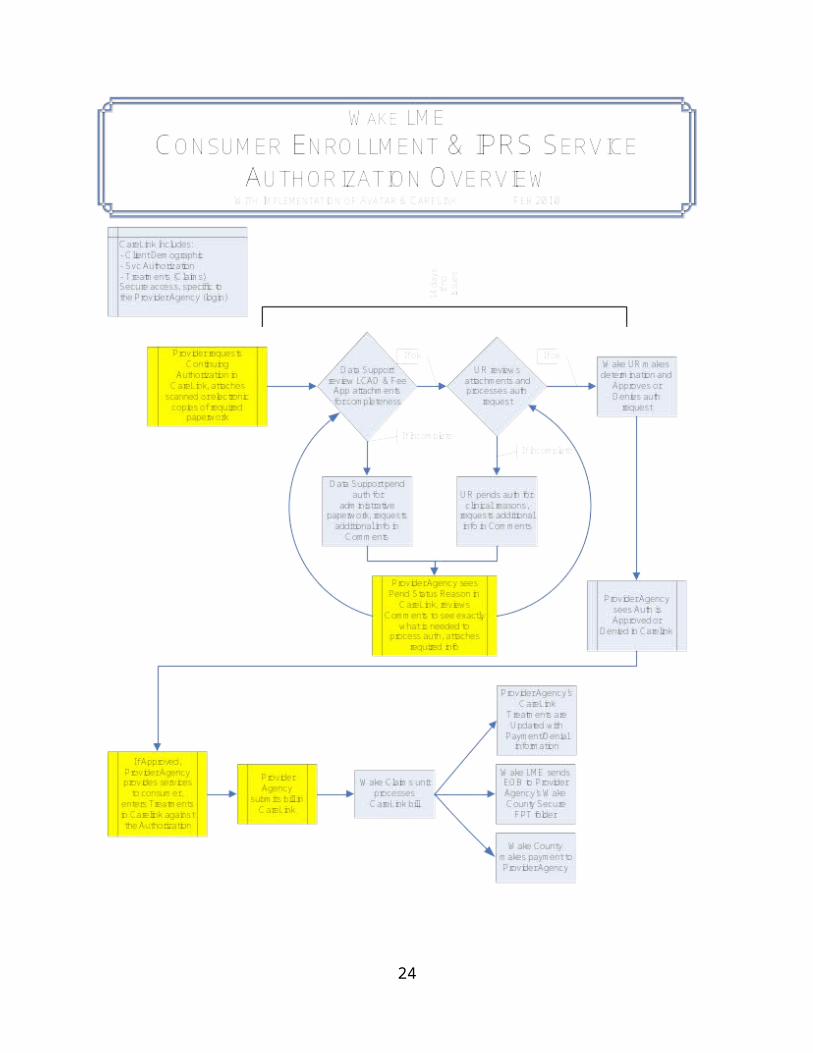
The following page includes the revised flow chart for providers to enroll consumers with the LME and to request service authorization for state-
funded (IPRS) care.
18
Flow Chart for Consumer Enrollment and IPRS Service Authorization
19

20

PERFORMANCE STANDARDS AND DATA
Performance expectations for LMEs are established annually in the contract between DHHS and the LME, and are monitored quarterly by the Division of MH/DD/SA. Specific performance expectations, by function, for the LME are as follows:
General Administration and Governance: Active Board that meets at least (6) times a year Active CFAC that meets at least six (6) times a year; Qualified CEO that meets required qualifications per NCGS 122C-121(d) Satisfaction of SPMP (FFP) requirements Qualified clinical staff in all three disability areas
Business Management and Accounting Management of IPRS funds to reimburse providers for authorized, delivered, and billed
services; Quarterly written reports including a balance sheet provided to the Board and CFAC Standardized statewide contract with all providers of state-funded services and
standardized MOA with all endorsed Medicaid providers Submission of Reports to DHHS as required
Information Management Fully functioning IT infrastructure, HIPAA compliant, electronic connection to State IT,
and capability to communicate with providers electronically Submission of consumer screening, admissions, and eligibility data Analysis of services authorizations and claims data Timely response to data requests Informative, user-friendly website with current (evergreen) information
Claims Processing Process for prompt payment of claims including Medicaid pass-through Process to identify all relevant payer information for each consumer Process to pursue all applicable first and third party payments for service Identification of all payer information for each consumer
Provider Relations Annual review and update of the assessment of community need and provider capacity
with 3rd quarter progress update, and quarterly updates reported to Board & CFAC Minimum number of provider agencies for every service necessary to ensure consumer
choice Process for timely endorsement and enforcement of endorsement requirements Appropriate provider manual, trainings and technical assistance Process for ongoing evaluation and monitoring of provider quality and compliance with
data submission requirements Process for resolving provider complaints
Access / Screening, Triage and Referral
21
Toll-free phone line 24-hour access 365 days a year Calls answered within 30 seconds by qualified professional TTY and/or Relay capability and foreign-language interpreter Ability to schedule appointments with an appropriate provider within 24 hours of initial
contact Process for managing DHHS bed-day allocations Report to Board and CFAC on access patterns and trends Screening consumers using the standard state form or all of the elements of the
standard form.
Service Management (UM, Care Coordination, Community Collaboration, and SOC) Published State-Funded Consumer Benefit Plan Implementation of approved LME crisis services plan Process for review of person-centered plans Service authorization decisions within required timelines Notification to consumers of rights and appeals regarding LME service authorization
decisions Audit and Post-payment review of services by licensed staff Management and prioritization of requests for CAP-MR/DD Waiver services Coordination of care for high cost/high risk consumers and consumers without a clinical
home Active collaborative relationships with other human service agencies Activities to encourage use of natural and community supports Full-time System of Care coordinator Designated staff to coordinate deaf services, school-based child and family teams, and
development of housing opportunities Quarterly Report to the Board on service utilization patterns
Consumer Affairs and Customer Service A customer service staff person shall respond to inquires within one business day. Outreach/education activities and materials (English & Spanish) Consumer Manual Timely response and resolution (disposition) to consumer questions and complaints Staff support to the CFAC and Human Rights Committees Report to Board, human rights committee and CFAC on consumer incidents, complaints,
appeals, and satisfaction with services at least quarterly
Quality Management Timely identification and remediation of problems Production and review of regular management reports Collection and submission of consumer data Analysis and use of data for planning, decision making and improvement Active Quality Improvement committee Report on QI activities to Board and CFAC quarterly and to DHHS annually
LME contractual reporting requirements and quarterly monitoring reports are provided on the Division of MH/DD/SA website at: http://www.ncdhhs.gov/mhddsas/performanceagreement/index.htm
22
DEMAND, CAPACITY AND OUTCOMES DATA
The following table provides a summary of consumers served through contractual providers in FY09 using state (IPRS) funds.
Unduplicated Consumers Served
Billable Units of Service (Hours)
Billable Units of Service (Days)
Developmental Disabilities875 321,079 37,750
Adult Substance Abuse1,056 19,845 8,508
Child Mental Health and Substance Abuse 384 13,121 17,845Adult Mental Health
1,762 38,582 3,079Total (Unduplicated)
4,461 392,627 67,182
As the implementation of the new Access Center and Avatar software progresses, additional data will be available for FY10 regarding demand for service through the LME’s Screening, Triage and Referral (Access Center) service. This information was not available in prior years due to the combination of LME STR and Crisis Services functions.
The LME also conducts a thorough assessment of its community needs and provider network capacity on an annual basis and prepares quarterly updates. This annual report is developed in collaboration with the Consumer and Family Advisory Committee (CFAC) and the Human Services & Environmental Services Board. The 2009 Community Need and Provider Capacity Assessment is available on the LME website at: http://www.wakegov.com/lme/
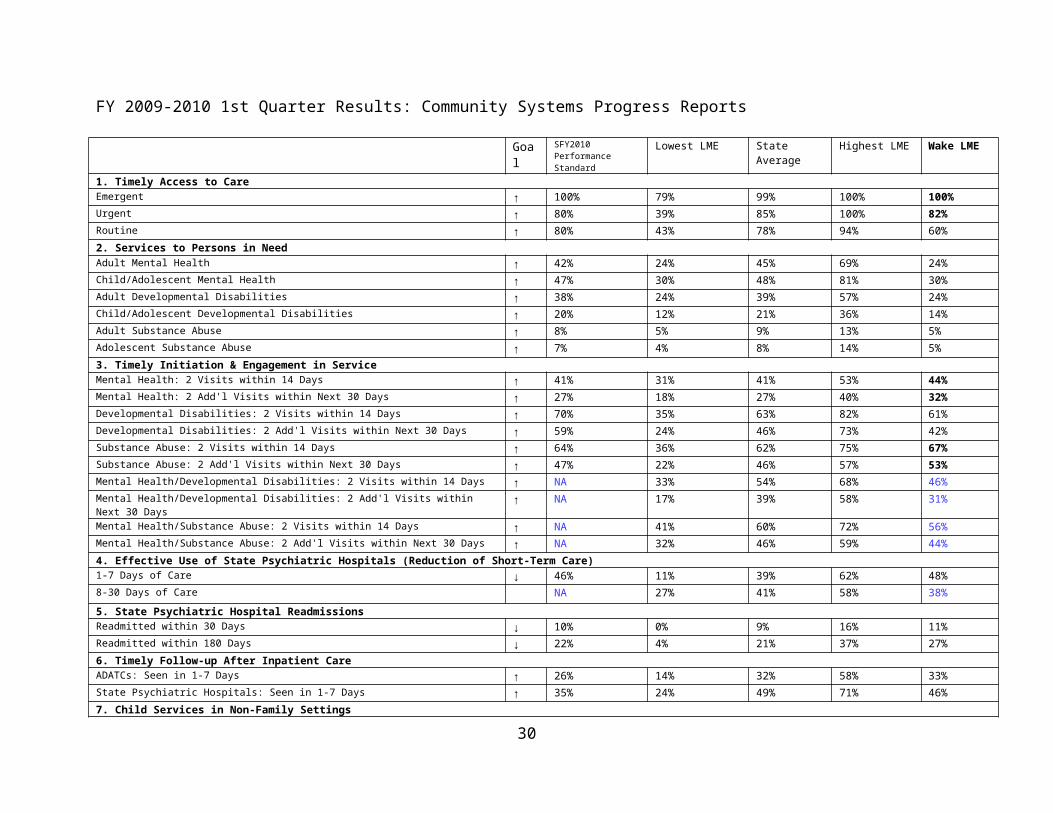
As a requirement of the DHHS-LME performance contract, the Division of MH/DD/SA monitors the Wake LME on its performance on measures of consumer access to care, timeliness of initiation of treatment, effective use of inpatient psychiatric care, hospital readmissions and aftercare, and residential child placement. Reports are posted on the DMH website quarterly, and attainment of state performance expectations is tied to single stream funding (SSF) status, which provides increased flexibility in disbursement of state funds. The Wake County LME has not yet met requirements for SSF. The table on the following page provides an overview of Wake LME’s performance on the most recent quarterly report.
23
24
FY 2009-2010 1st Quarter Results: Community Systems Progress ReportsGoal SFY2010
Performance Standard
Lowest LME State Average
Highest LME Wake LME
1. Timely Access to CareEmergent ↑ 100% 79% 99% 100% 100%Urgent ↑ 80% 39% 85% 100% 82%Routine ↑ 80% 43% 78% 94% 60%2. Services to Persons in NeedAdult Mental Health ↑ 42% 24% 45% 69% 24%Child/Adolescent Mental Health ↑ 47% 30% 48% 81% 30%Adult Developmental Disabilities ↑ 38% 24% 39% 57% 24%Child/Adolescent Developmental Disabilities ↑ 20% 12% 21% 36% 14%Adult Substance Abuse ↑ 8% 5% 9% 13% 5%Adolescent Substance Abuse ↑ 7% 4% 8% 14% 5%3. Timely Initiation & Engagement in ServiceMental Health: 2 Visits within 14 Days ↑ 41% 31% 41% 53% 44%Mental Health: 2 Add'l Visits within Next 30 Days ↑ 27% 18% 27% 40% 32%Developmental Disabilities: 2 Visits within 14 Days ↑ 70% 35% 63% 82% 61%Developmental Disabilities: 2 Add'l Visits within Next 30 Days ↑ 59% 24% 46% 73% 42%Substance Abuse: 2 Visits within 14 Days ↑ 64% 36% 62% 75% 67%Substance Abuse: 2 Add'l Visits within Next 30 Days ↑ 47% 22% 46% 57% 53%Mental Health/Developmental Disabilities: 2 Visits within 14 Days ↑ NA 33% 54% 68% 46%Mental Health/Developmental Disabilities: 2 Add'l Visits within Next 30 Days ↑ NA 17% 39% 58% 31%Mental Health/Substance Abuse: 2 Visits within 14 Days ↑ NA 41% 60% 72% 56%Mental Health/Substance Abuse: 2 Add'l Visits within Next 30 Days ↑ NA 32% 46% 59% 44%4. Effective Use of State Psychiatric Hospitals (Reduction of Short-Term Care)1-7 Days of Care ↓ 46% 11% 39% 62% 48%8-30 Days of Care NA 27% 41% 58% 38%5. State Psychiatric Hospital ReadmissionsReadmitted within 30 Days ↓ 10% 0% 9% 16% 11%Readmitted within 180 Days ↓ 22% 4% 21% 37% 27%6. Timely Follow-up After Inpatient CareADATCs: Seen in 1-7 Days ↑ 26% 14% 32% 58% 33%State Psychiatric Hospitals: Seen in 1-7 Days ↑ 35% 24% 49% 71% 46%7. Child Services in Non-Family SettingsResidential Treatment: Levels 2 (Program), 3, and 4 ↓ 4% 3% 4% 7% 5%
25
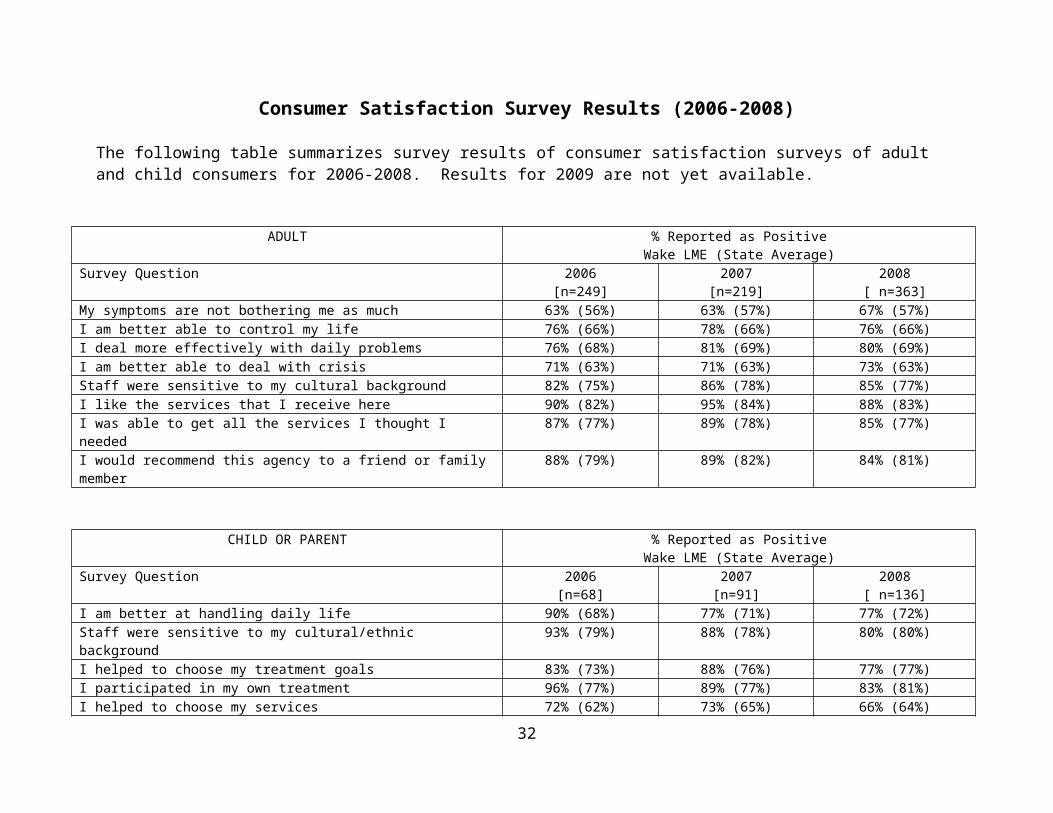
Consumer Satisfaction Survey Results (2006-2008)The following table summarizes survey results of consumer satisfaction surveys of adult and child consumers for 2006-2008. Results for 2009 are not yet available.
ADULT % Reported as PositiveWake LME (State Average)
Survey Question 2006 [n=249]
2007 [n=219]
2008[ n=363]
My symptoms are not bothering me as much 63% (56%) 63% (57%) 67% (57%) I am better able to control my life 76% (66%) 78% (66%) 76% (66%)I deal more effectively with daily problems 76% (68%) 81% (69%) 80% (69%)I am better able to deal with crisis 71% (63%) 71% (63%) 73% (63%)Staff were sensitive to my cultural background 82% (75%) 86% (78%) 85% (77%)I like the services that I receive here 90% (82%) 95% (84%) 88% (83%)I was able to get all the services I thought I needed 87% (77%) 89% (78%) 85% (77%)I would recommend this agency to a friend or family member 88% (79%) 89% (82%) 84% (81%)
CHILD OR PARENT % Reported as PositiveWake LME (State Average)
Survey Question 2006 [n=68]
2007 [n=91]
2008[ n=136]
I am better at handling daily life 90% (68%) 77% (71%) 77% (72%)Staff were sensitive to my cultural/ethnic background 93% (79%) 88% (78%) 80% (80%)I helped to choose my treatment goals 83% (73%) 88% (76%) 77% (77%)I participated in my own treatment 96% (77%) 89% (77%) 83% (81%)I helped to choose my services 72% (62%) 73% (65%) 66% (64%)I got the help I wanted 90% (72% 85% (77%) 80% (77%)Overall, I am satisfied with the services I received 91% (79%) 88% (83%) 87% (82%)I am better able to cope when things go wrong 72% (61%) 69% (64%) 67% (66%)I am doing better in school and/or work 75% (64%) 66% (65%) 74% (69%)
26
WORKLOAD MEASURES
The following data provide a summary of LME systems management outputs and workload measures. Data for Quality Management and Utilization Review/Utilization Management units were selected because comparable data exist for prior fiscal years. Other units such as the Access Center and Care Coordination have limited comparable prior years data due to changes in their structure and function associated with the LME reorganization, but will gather baseline data beginning this FY.
The LME Utilization Review Unit activities processed the following number of authorizations:
FY 2006 18,519 FY 2007 19,721 FY 2008 19,541 FY 2009 21,801 FY 2010 13,487 (7/1/09 thru 1/21/10; projected to approx. 25,000 for FY
2010)
Payments were processed totaling $24 million in State/Federal IPRS funds, $10 million in pass-through Medicaid, and $500,000 in pass-through CAP Medicaid.
The LME Care Coordination Unit provided assertive engagement and/or bridging services to over 600 clients, primarily upon discharge from inpatient psychiatric care.
The Quality Management unit conducts routine monitoring of provider agencies based upon standards of monitoring determined by the State, as measured by the Frequency and Extent of Monitoring (FEM) tool. In addition to performing routine monitoring, the LME may choose to conduct supplemental targeted monitoring if issues or concerns are identified during routine monitoring or as a result of information obtained from other sources (including, but not limited to, a complaint investigation, incident investigation, audit, feedback received from another oversight agency, or analysis of provider incidents, complaints, or performance data). The LME Quality Management Team completed the following number of monitoring events since 2005:
2005:472006:1182007:172008:56
27

2009:212010:14 (Jan. & Feb.)
Provider Agency Incidents Reported to LME
The following table summarizes Level II and III incidents reported to date. Level I incidents are less severe than II and III and are not held to the same reporting requirements as levels II and III.
Total FY05-
06
TotalFY06-
07
Total FY07-
08
TotalFY08-
09
TotalFY09-10*
Total providers reporting 171 242 307 362 174*
Death(Level III suicide, homicide, accident related deaths)
28
(18)
49
(10)
41
(14)
21
(3)
10
(1)Restrictive Intervention 17 47 71 93 78
Consumer Injury 47 53 85 126 73
Abuse/Neglect** 50 44 101 97 53
Medication Error 10 18 12 33 15
Consumer Behavior 118 199 363 510 303
Other 89 160 170 223 76
TOTAL 359 570 776 1,103 608*
*1st and 2nd quarter 0910 only** Not all abuse/neglect incidents are perpetrated by agencies, majority by parent or guardian but must be reported as abuse/neglect
Complaints About Community ProvidersComplaints Total
0506Total0607
Total 0708
Total0809
Total0910*
Total Complaints 49 92 97 104 28
Substantiated Complaints 13 50 29 18 8
28

Endorsement Actions Summary (2006-present)
The following table summarizes provider endorsement actions for Medicaid enhanced benefit services since 2006.
Service Type Fully Endorsed
LME Withdrew
Provider Withdrew
Community Support Child 36 6 30
Community Support Adult 28 7 30
Community Support Team 39 2 16
Multi-Systemic Therapy 4 0 1
Assertive Community Tx Team 2 0 1
Diagnostic Assessment 34 6 24
Mobile Crisis 1 0 3
Intensive In-Home 37 4 20
Partial Hospitalization 0 0 0
Child Day Treatment 7 1 1
Opiod Treatment Program 1 0 0
Sub Abuse Intensive Out Pt. (SAIOP) 6 1 1
Sub Abuse Compr. Out Pt. (SACOT) 4 1 5
Psychosocial Rehabiltation 3 2 2
Child Residential 29 4 6
CAP Services 24 2 5
Detox Services 0 0 1
29
ENVIRONMENTAL SCANThe following factors that may affect service delivery, demand, systems management, and community capacity to provide MH/DD/SA services:
The State has issued a Request for Applications that will allow LME’s to assume local responsibility for Medicaid utilization management as Medicaid Waiver (1915b/c) sites. State performance expectations of LMEs will likely be increased to ensure capacity to perform expanded roles. LMEs that are approved as Medicaid waiver sites will be required to obtain accreditation through a different accrediting body than the one that provides our current national accreditation. There is also a movement toward consolidation of LME functions and mergers of LMEs. The statewide transformation of the MH/DD/SA system will have a significant impact on local management of the service delivery system in Wake County, and will require important planning and decision-making regarding Wake County’s preparation for these changes.
State Medicaid waiver plans may result in transfer of Medicaid utilization review and/or CAP/MRDD Local Approval responsibilities to LMEs within the next several years. These transitions would have a significant impact on our management of purchase of service funding, broadening the scope of our responsibilities and oversight significantly.
State budget reductions have resulted in significant decreases in funding for MH/DD/SA services. These reductions will result in decreased access to care at a time when demand for services is increasing, and have reduced access to services within a system that had limited resources and has historically received one of the lowest per capita state service allocations in the state. Economic forecasts suggest that funding reductions will continue next FY, despite continued growth and demand for services.
The state MH/DD/SA system is undergoing a major transformation that will result in major changes in Medicaid covered services, including elimination of Community Support, consolidation of case management services, transformation of child residential services, and reduction in Medicaid rates.
Community providers face significant financial challenges due to budget reductions, elimination of Community Support services, increased expectations for service delivery which require higher provider expenses, and reduced reimbursement rates for most services. The State MH/DD/SA system is undergoing a major transformation that will have a profound impact on the scope, type,
30
models of care and financial viability of services provided. The overall instability of the provider network environment will also impact our ability to project service utilization, develop and maintain provider network capacity, and ensure continuity of care for existing consumers and access to care for new consumers.
Wake County continues to face limitations in availability of local inpatient psychiatric beds, particularly for consumers who have Medicaid coverage, and there are currently limited services available to divert consumers from inpatient treatment.
Loss of services to consumers based on State Medicaid plan changes may result in an increasingly litigious service environment and increased demands for time of LME administrative and care coordination staff.
Wake County has experienced continued growth in population and demand for MH/DD/SA services over the past year, during a period in which MH/DD/SA funding has been cut significantly. The combination of increased demand and reductions in funding has had an adverse impact on access to services.
31
EXTERNAL COUNTY COMPARISON
Wake Mecklenburg Durham PBH OPCTotal population (July, 2009) 898,818 919,372 263,857 734,328 230,640FY09-10 Final Services Allocation (excludes CASP, includes non-recurring cuts)
$ 17,586,442 $ 14,432,563 $ 8,351,962
$ 14,405,146
$ 7,939,465
Services Funding Per Capita (range: $10.42 - $43.60)
$ 19.57 $ 15.70 $ 31.65 $ 19.62 $ 34.42
FY09-10 Final Services Allocation (excludes CASP, includes only recurring cuts)
$ 19,592,447 $ 19,864,339 $ 8,814,519
$ 16,745,773
$ 9,345,820
Services Funding Per Capita (range: $18.46 - $50.65)
$ 21.80 $ 21.61 $ 33.41 $ 22.80 $ 40.52
Medicaid Enrollment 66,942 102,780 32,432 90,470 21,421Medicaid % of Population 5.2% 8% 2.5% 7.0% 1.7%LME Systems Management Funds (FY09) $ 7,939,965 $
8,165,508.00 $4,577,988 N/A $ 4,403,940
LME Systems Management Funds Per Capita (FY09)
$ 8.83 $ 8.88 $ 17.35 N/A $ 19.09
32