wear-of teeth-an update
TRANSCRIPT

8/7/2019 wear-of teeth-an update
http://slidepdf.com/reader/full/wear-of-teeth-an-update 1/10
General Dentistry
An update on the etiology of tooth wear
Abstract Tocth wear is an ever-increasing problem, and younger patients are particularly
atrisL The pnM ein is likely to continue as patients' deman ds and expectations rise
atid as mownatural teeth are retained into old age. T he etiohigy of tooth wear
is reviewed, with emph asis on those factors that appear to be major cutitributiirs lo
the ptvblent at tiie tmiment. The clinical appearance of tooth wear is also discussed.
It would appear that erosive lactors ar e a significant c ause of tooth wear. The
prominence of acidic damage qf tooth tissue is probably a re/lection oj society's
coneern with heahhy eating and appearance. (Quintessence Int 1997:28:305-313.)
the cause of tooth wear is important for
the long-term prognosis of the dentition and
of the etiologic factors
may be diffieult to
entify and control because ofconfiicting priorities
the patient.
rious loss of tooth tissue is a normal physiologicand oceurs throughout life,' Problems arise,
if the rate of loss or the degree of destructionor esthetic
or sensitivity for the patient. Diagnosis ofve loss can be difficult if dec isions are based on
of limited
in Reslorallve Denlislry, Charles Clifford Dciilüi
Hospilal, Shafnekl, England,
in ResUirative Denlibtry, Kmgs Denial Inslinite. Lon-
don, Enelancl.
inRcsnirjiive Dtiilislry, <liiiries CiiiTiird Denial Hosni-
lal, Slicflield, Englimd.
Dr Karl Bishop, Senior Re¡:istrar in ResloraliveCh arle s Clifford Denial Hos pitói, Wellesly Road, Slieffieid,
Il4 27l7)j jû,
and confiicting data, Lamhrechls et al.- for example,
considered normal loss of enamel to be between 20 to
38 iim per year, while Xhonga' reported similar
figures for a 6-month period. Because it is difficult to
quantify normal loss. Smith and Knighf̂ suggested that
the rate of loss be considered patho logic if it is likely to
prejudice the survival of the teeth or is a source of
concern to the patient.
Traditionally, the terms erosion, abrasion, and
attrition are tised to describe noncarious, pathologic
loss of tooth tissue," These terms refiect the specific
etiologic factors that are associated with the loss of
tooth tissue, Eccles," however, suggested that tooth
surface loss be used to embrace all three individual
descriptions because a single etiologic factor is often
difficult to identify (Figs la and lb). Subsequently.
Smith and Knighf* contended ihat tooth surface losbelittles the severity of the problem and advocated the
use of the term tooth wear{T<N). For clarity's sake, TW
will be used throughout this article to describe the
pathologic, noncarious ioss of tooth tissue. However,
care should be taken in the tise of this term because it
may suggest an attritional or abrasive etiology and
diminish the importance of erosion, which appears to
bea ma jorcon tributorto the loss of tooth tissue,'^ The
terms erosion, abrasion, and attrition will be used,
however, lo describe specific etiologie factors.
The dental management of patients with TW ha
provided d illkultics for the dental profession for many
8/7/2019 wear-of teeth-an update
http://slidepdf.com/reader/full/wear-of-teeth-an-update 2/10
Bisflop et al
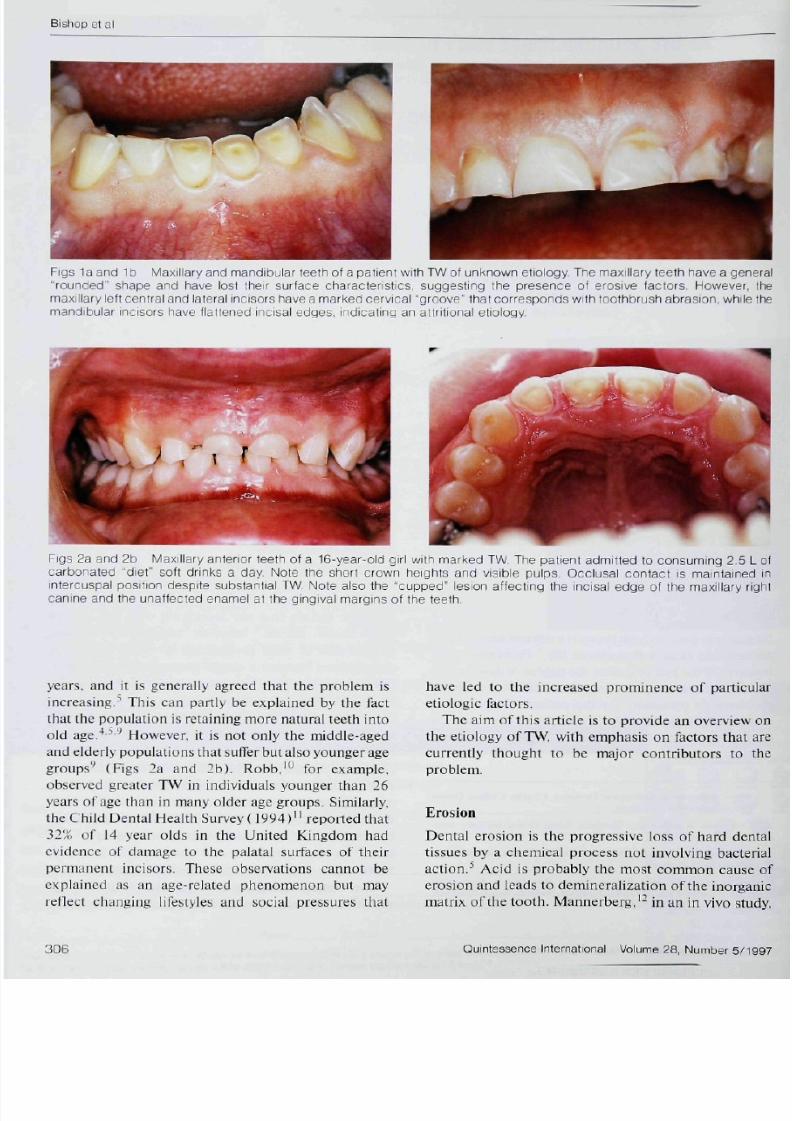
Figs la and 1 b Ma>;illary and mandibular teefh of a patienf wifh TW of unknown efiology The rTia;<illary leelh fiave a g"rounded" sfiape and have lost their surface characfenslics, suggesting tfie presence of erosive fac fors Howevemaxillary le fl cenfral and lateral incisors fiave a marked cervical "grooue" ffiaf corresponds wifh toothbrush abraston, whirnandibular incisors fiave tiatfened incisai edges, indicating an aftritional etiology.
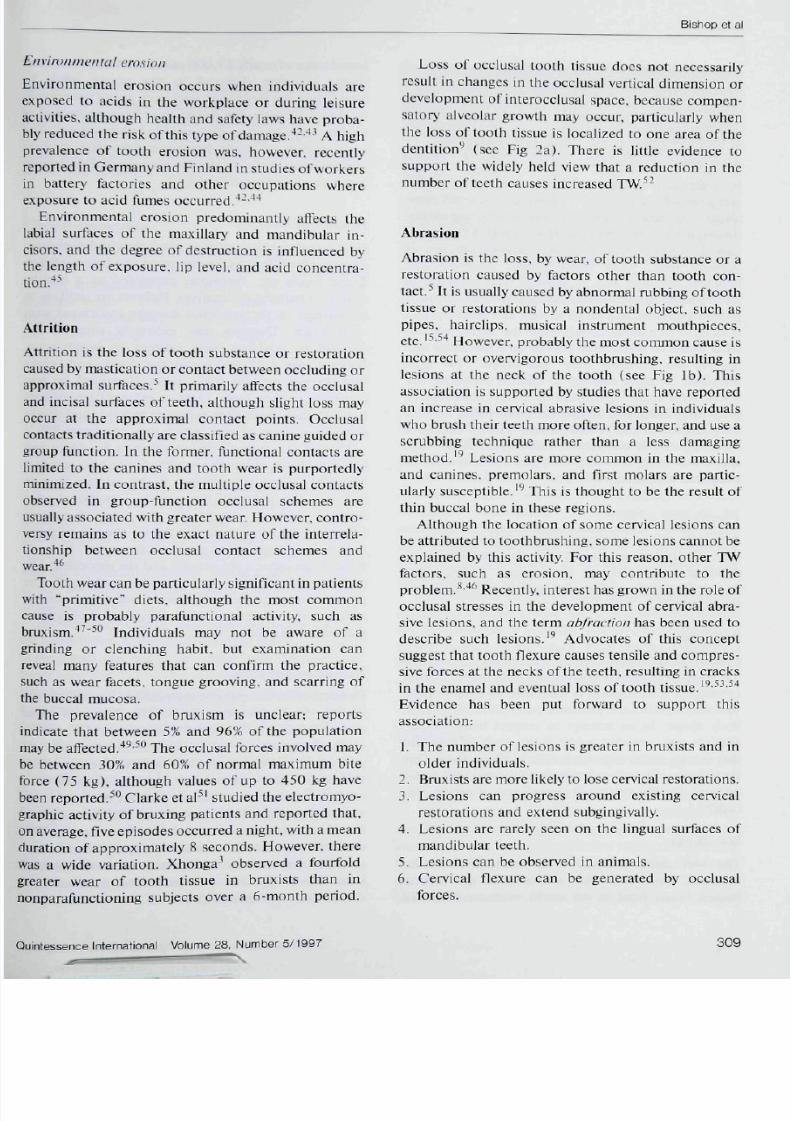
Figs 2a and 2b fvlaxillary anterior teeth of a f6-yea r-old girl wifh marked TW The palienf adm itted fo consuming 2.5carbonafed "diet" scfl drinks a day. Note fhe sfiorf crown heights and visible pulps Occlusal contact is mainfaineintercuspal position despite substanfial TW Nofe also tfie "cupped" lesion affecfing the incisai edge of fhe maxillary canine and the unaffected enamel at the gingival margins of fhe teefh
years, and it is generally agreed that tfie profilcm is
increasing," This can partly be explained by tfie factthat the population is retaining more natural leeth into
old age."'""'' Hovvever. it ¡s not only the middle-agedand e lderly populations thai suffer but also younger age
groups'' (Rgs 2a and 2bl. Robb,'" for example,observed greater TW in individuals younger than 26
years of age than in many older age groups. Similarly,the Child Dental Health Survey ( 1994 ) " reported that
32% of 14 year olds in the United Kingdom hadevidence of damage to the palatal surfaces of their
permanent incisors. These observations cannot be
explained as an age-related phenomenon but mayreflect changing lifestyles and soeial pressures that
have led to the increased prominence of partic
etiologic factors.The aim of this article is to provide an overview
the etiology of TW„ with emphasis on factors that
currently thought to be major contributors to problem.
Erosion
Dental erosion is the progressive loss of hard de
tissnes by a chemieal process not involving bact
action," Acid is probably the most common causerosion and leads to demineralization o fthe inorgmatrix ofthe tooth, Mannerberg,'- in an in vivo st

8/7/2019 wear-of teeth-an update
http://slidepdf.com/reader/full/wear-of-teeth-an-update 3/10
Bishop et a
Total Soft Drinks Sales (VK\.Peicentage MaiketShare for
^Diet 'Soft Drinks.
g 3 Total Suit drink sales (United Kingdom ), Fig 4 Market share for diet sott drinks.
bed two distinct erosive lesions; active lesions, in
It wotild appear that erosion either by itself or in
TW, Smith and Kjiighl.''^ for example, could
11% ofthe
Acidic foods and drinks are now widely available
gnificant com ponent of many diets. This is
65% of sales, and 42% of fruit drinks are
2 and 9
years.** '̂ It has been suggested that theconsu tnp tion ofsoft drink s by the yo ting, in particular, accounts for thehigh incidence of TW observed in the United King-
dom." Hccles-' confirmed the impoHance of softdrinks when he reported that they are implicated as
etiologic factors in 40% of patients with TW,
Societal concern with slimncss and "healthy eatitig"has lead to an Increase in consumption of "diet" foods
and beverages. For example, diet drinks now accountfor a large share ofthe market in the United Kingdom
(Fig 41 , These low-calorie beverages are also acidicand hav econ stituentssim ilarto those of the traditional
beverages. It is unclear whether diet drinks are more
destructive of tooth tissue than the sugar-containingalternatives, although there is some evidence to
suggest that carbonated drinks are less destructive thannoncarbonated drinks,'''-" Unfortunately, unlike the
sugar-containing drinks, the potential for erosivedamage by these diet beverages may not be well
understood by the public,
A healthy diet may also contain substantial acidic
foods,-'"-'' which also have the potential to cause lossof tooth tissue. Furthermore, the abrasive nature of
many ofthe components of these diets may accelerateTW,
Another source of dietary acids is associated with
orally adm inistered medicines and drugs, such as irontonics, chewable vitamin C tablets, and replacement
hydroc hloric acid used by patients with gastric achlor-
Régurgitation ero.'iion
Régurgitation is the return of gastric contents to the
mouth and is usually described as involuntary or

8/7/2019 wear-of teeth-an update
http://slidepdf.com/reader/full/wear-of-teeth-an-update 4/10
Bishop et al
Fig 5 Maxillary teeth of a professional pck ey who usedrégurgitation as a method to control his weight. Note thedistribution of the looth surface loss; the palatal surfaces ofthe maxillary leeth are predominantly affected (perimolysisl.The rounded appearance ol the leelh suggests an erosiveetiology.
voluntary,'' •'' The gastric environment is highly acidic(approximately pH 2), and régurgitation can expose
the teeth to highly erosive facfors. Although isolatedincidents are unlikely to cause long-term problem s, the
teeth may be severely affected by repeated o r con tinualepisodes of régurgitation.-^ -'
Involuntary régurgitation
Involuntary régurgitation, or gastroesophageal refiux.is a common complication of gastrointestinal prob-
lems, such as hiatus hernia, or as a consequence of
pregnancy. Some dietary components, such as spicyfoods and onions, can aiso promote refiux as can
smoking and certain types of exercise.-**-''
Gastritis and acid régurgitation can also occur as aconsequence of chronic alcoholism, although patients
may not be aware of the problem,'"" Often the
individual is secretive about the habit, and confirma-tion can be difficult. Some patients, for example, some
young adulls, have frequent atid repeated alcoholbinges. These binges are often associated with epi-
sodes of vomiting but, unlike alcoholics, the patientstend to be less secretive. Soft drinks, which are
frequently used as mixers with alcoholic drinks, mayalso contribute to TW,
Refiux can also occur in the absence of any clinicalsigns and symptoms normally associated with the
problem,-^-'- It has been suggested that this couldaccount for some situations in which TW occurs in the
absence o fan iden tifiable c tio logic f a ^ ' '
Voluntary régurgitation
Voluntary régurgitation is usually associated wi
underlying psychological problem, such as an edisorder."--'"' However, there is a group of pa
who repeatedly regurgitate in the absence of anypathologic or psychoiogical disorder. T hese indivi
after deliberately returning food to the mouth, usexpel some of the contents prior to swallowin
remainder. This habit, termed nuiünuiion. hasdescribed in institutionalized individuals with lea
difficulties,-'' Gihnour and Beckett,'^ however
ported similar practices in highly motivated, intelprofessional people who use the habit as a respo
stress. Voluntary régu rgitation in the absence opsychological problems may also occur in indivi
whose occupations depend on control of body wefor example, professional jockies (Fig 5).-''*
The eating disorders most commonly assoc
with TW are anorexia nervosa and bulimia nerThese problems, a feature ofa body-conscious so
ofien begin in early adolescence, frequently runnchronic course with substantial complications.''
prevalence of eating disorders in the general potion is unclear, although studies suggest the incid
of anorexia and bulimia nervosa are 0,1% to Ù.T
1% to 2X, respectively. However, patients with e
disorders may actively avoid detection or be relu
to disclose deta ils, and the true prevalence munderestimated,'^-"' It is generally agreed tha
problem is increasing and that groups such as dandieticians, and Asian females are particularly at
Although studies indicate that eating disordermore prevalent in fetnales, males may be equally
but do not necessarily seek medical help.
The effect of acid régurgitation in bulimia ne
patients has been well documented.'^'"" The common sign is peritnolysis—erosive lesions loca
to the palatal aspect of the maxillary teeth (F
These lesions are thought to result because the todirects gastric contents forward during voluntaryprepared vomiting and the lateral spread of the to
protects the mandibular teeth."-'' ' However,idiosyncratic distribution of lesions may also oc
The pattern of TW in patients with eating disomay also be affected by othe r etiologic factors, su
consumption of erosive diet beverages and hefoods as patients strive to control their w
xerostomia, caused by vomit-induced dehydratidrugs such as diuretics, appetite suppressants
antidepressants; and long-term co mp lications, s
gastric ulcers and hiatus hernia,-^
8/7/2019 wear-of teeth-an update
http://slidepdf.com/reader/full/wear-of-teeth-an-update 5/10
5ishop et al
enisinn
the risk o fth is type ofdatiiage.•*-•*' A high
ed in Germ any and Finland in studies of workers
Environmental erosion predominaiitiy atlects the
and the degree of destruction is intluenced by
used by mastication or contact between occluding or
s traditionally are classified as canine guided or
ally associated with greater wear. However, contro-
Tooth wear can be particularly significant in patients
The prevalence of bruxism is unclear; reports
cate that between 5% and 96% of th e populationy be affected.''^ "̂ The occlusal forces involved may
e et al''' studied the electromyo-
age, five episod es occurred a night, with a mean
a wide variation. Xh on ga ' observed a fourfold
nctioning subjects over a 6-month period .
Loss of occlusal tooth tissue does not necessarily
restilt in changes in the occlusal vertical dimension or
development of interocciusül space, because compen-
satory alveolar growth may occur, particularly when
the loss of tooth tissue is localized to one area ofthe
den tition '' (see Fig 2a}. The re is little evidence to
support the wideiy held view that a reduction in the
number of teeth causes increased TW."^-
Abras ion
Abrasion is the loss, by wear, of tooth substance or a
restoration caused by factors other than tooth con-
tact.̂ It is usually caused by abnormal rubbing oftoothtissue or restorations by a nondenta! object, such as
pipes, hairclips, musical instrument mouthpieces,
etc. '-''-'''' However, probably the most comm on cause is
incorrect or overvigorous tooth brush i tig, resulting inlesions at the neck ofthe tooth (see Fig Ib). This
association is supported by studies that have reportedan increase in cervical abrasive lesions in individuáis
who brush their teeth tiiore often, for longer, and use ascrubbing technique rather than a less damaging
method.''' Lesions are more common in the maxilla,
and canines, premolars, and first molars are patiic-ularly susceptible.''' This is thottght to be the result of
thin buccal bone in these regions.
Although the location of some cervical lesions canbe attributed to toothbrushin g. some lesions canno t beexplained by this activity. For this reason, other TW
factors, such as erosion, may contribute to theproblem.*'**' Recently, interest has grown in the role of
occlusal stresses in the developtnent of cet^ical abra-sive lesions, and the term abfructioti has been used to
describe such lesions.'" Advocates of this conceptsuggest that tooth flexure causes tensile and com pres-
sive forces at the necks ofthe teeth, resulting in cracksin the enamel and eventual loss oftooth tissue.'^•^^•^''
Evidence has been put forward to support thisassociation:
1. The number of lesions is greater in bruxists and inolder individuals.
2. Bruxists are m ore likely to lose cervical re storations.
3. Lesions can progress around existing cervicalrestorations and extend subgingivally.
4. Lesions are rarely seen on the lingual surfaces of
mandibular teeth.
5. Lesions can be observed in animals.
6. Cervical flexure can be generated by occlusalforces.

8/7/2019 wear-of teeth-an update
http://slidepdf.com/reader/full/wear-of-teeth-an-update 6/10
Bishop et al
7, Often adjacent teeth are not affected.8, Lesions ate less common if the tooth is mohilc.
Prevalence
Assess tuet It
It is generally accepted that the prevalence of TWincreases with age,'"'*''"'^'' However, the exact prev-alence is unclear, primarily because of differing assess-ment crite ria,'" For exam ple. Hugoson etal-''̂ reportedthat 13% and 24% of surfaees show evidence ofocclusal wear, while other studies observed thatbetween 25% and 50% of subjects have evidence ofTW," Some loss of tooth tissue is normal during apatient's lifetime, as a result of wear and tear. The lossis likely lo be a problem only when the degree exceeds
what would be considered normal for a particular age.Studies that consider only "pathologic" TW may,therefore, be more relevant to clinical dentistry. TheTooth Wear Index'' attempted to achieve relevance hyproposing maximum acceptable tooth tissue loss foreach decade of life. Tooth surface joss in excess ofthese figures is considered pathologic. When thisindex was nsed, between 4,5% and 5,7% of surfacesexamined exhibited TW,''-'"
Contriinning factorsAlthough the actual prevalence of TW is unknown,there is general agreement that the problem is in-creasing, particularly in the young.''"" The exactreason for this is unclear, but several factors may beimplicated.
Body image
Fashion designers and image makers have promotedthe concept that siimness equates with attractiveness
or success. This concept is supported by role models,who may significantly influence perceptio n of the idealbody shape. In an attempt to control body weight,patients may consume acidic foods, such as fruit anddiet drmks, rather than high-calorie alternatives. Thisstruggle to achieve the ideal body shape may also partlyaccount for the increased prevalence of eating dis-orders.
Soft drinks
The soft drink industry is a muitimillion dollarbusiness. Coea-Cola, for example, is the secondbiggest brand label in the world, with an estimated
brand value of nearly $ 9.00 0 million. M arketing odrinks is often directed to the young aduassociating the beverages with peer group accepity. More recently, the drinks have been protnothealthy and linked to high-profile sports figuresconsumption of acidic beverages following ex
may be particularly dangerous because of dehydand lack of salivary buffering.
Health care workers
Health care worke rs, such as physicians and dietiadvocate fresh fruit as A component of a balancedThese foods are, therefore, promoted as a heoption to harmful alternatives. Patients are unlikebe warned of the potential damage associated such foods. Dentists may indirectly support
concept by advising their patients to avoid Patients may further perceive that foods and dthat do not contain sugar must, therefore, bedamaging to their teeth. Dentists often advise pato hrush their teeth after exposure to foods and dcontaining stigar or acid, which may accelerate T
One of the major roles of saliva is to dilutehufler acid that enters the mouth. Saliva also actlubricant during mastication. If the salivary fioreduced, the potential for erosive, attritional,
abrasive damage increases,-'''^ As medieal scadvances and life expectancy grows, the use of within the population is more widespread,^^ Mathese drugs cause a dry m outh, and the associateproblems are likely to become more prevalent,^"^problem may be compounded if patients conacidic drinks in an attempt to alleviate the sympand stimulate salivary flow.
Restorative materials
Dentists often use esthetic re storatio ns, irrespectwhether the restoration is visible. Many of malerials have the potential to accelerate TW, pularly if used on occluding surfaces in parafunc
patients. Potentially less destructive matesuch as "softer" porcelains and fine-particle composites, have been developed but have not clinically evaluated, particularly in TW patientsFor this reason, metal occlusal surfaces are thechoice in patients w ith extreme TW. particularly w
an attritional etiology is suspected. However, pamust be aware that all restorative materials

8/7/2019 wear-of teeth-an update
http://slidepdf.com/reader/full/wear-of-teeth-an-update 7/10
Bishop et al
Flattening of the cusp tips or incisai edges and
and movement ofthe oppo sing too th. If the
a\' occur as ilie dentin is lost m ore quickly
he surrounding enam el. This unsupported enam-
Erosive lesions eause cupping or grooves to form in
unlike attritional lesions, the base
an irregular appea rance because of fractures ofthe
differential loss of the soffer
ral area of exposed dentin surroun ded by a border
This feature has been attributed to the buffering
Traditionally, cervical lesions caused by abrasion
the lesion is more rounded and shallower (see
Fig C V'vo"i -.- .KK Pia n-tui '='n-lü nvXal tr i invns in a bru^in g
pat ient These restoiat ian s v jcrc place d 2 years previouslybecause of TW. The pat ient had nof been provided witb an
occlusal spl inf
Fig 2 ), Lesions assoeiated with toothbrushing are also
thought to have rounded internal angles, while those
caused by abfraction are more angular and may initially
have a corrugated appearance , '''
The clinical appearance of restorations may also
reflect the major cause of TW, Amalgam and resin
composite restorations, for example, tend to be
unaHeeted by erosive factors and remain "proud" ofthesurrounding tooth tissue. However, both restorative
materials show evidence of faceting if attrition is the
major etiologic factor,''
Despite exp osure of extensive areas of dentin, acute
sensitivity is rarely a problem. This is probably due to
the developtnent of sclerosed dentin and smear layers
on the surface of the toofh. Pain can be a problem,
however, when the TW is rapid and ongoing and is
common when erosion is a major etiologic factor.
Conclusion
The management of TW is a major challenge to the
denfal profession, and this is likely to continue as
changing lifestyles highlight particular etiologic factors
to which younger individuals are especially sus-
ceptible. It is important that these causes be identified
and, if possible, eliminated before restorative therapy
is initiated. Failure to eliminate the cause may com-
promise the long-term survival of restorations andfurther deterioration ofthe dentition.
8/7/2019 wear-of teeth-an update
http://slidepdf.com/reader/full/wear-of-teeth-an-update 8/10
Bishop et al
References
1. Flint S, Scuily C. Oroli icial age changes and reialed disease. DentUpdate l9NN:15: , ' !37-342,
2. Lamhrechts P, Braenie M, Viiylsleke-Wauters M, Vanherle G,Quantitative in vivo ivear of human enamel. J Di' i i i Res 1989;
3, Xlionga FA. Bruxism and its clïeei on the teeth. J Oral Rehabil
l977 ;4 ;65-7 ( i .
4, Smith B G N , Knight JK. A n indes for measuring the wear of teeth. BrDentJ I9S4:I5(1:4 . Î5-4.1K
Watson IB , Tulloch EtM. Cl inic al ass.loss. Br Dent J 19S5:159:144- I4S.
t of eases of too th surfsee
6. Eccles JD . Tooth surface loss from abrasion, attr it io n and erosion.Dem Upda le liíJ-Jí .17.1-381
7. Smilh B GN . Some tacets of loo lhw ejr An n R Aust Co l l Dent Sure
S. Shaw L, Smith A . Erosion m chi ldren : An increasing cl in icalproblem. ' Dent Updaie I 9 9 4 ; 2 1 : I U 3 - 1 0 6 .
9. Bishop K A , Br iggs PFA , Kel leher MG D . The et io logy and
management of localized anterior tooth wear in the young adultDent Update I994 :21 ' 15 . 1 - 161 .
Robb N. EpidemiologiL-al Study of Toolh Weo f L o n d o n . 19 1 ! .
O Br i c n M . Ch i l d r eL o n d o n ; Her Majesly
Dental Health m Ihe United KingdomStat ionery Ulf ice, 1994.
Man nerberg F, Changes in lhe enamel surface in cases of eros ion; ,Arep l ica s tudy . Arch Ora l B io i l96h41supp l ) :59-62 .
Van Meerbeek B, Inokoshi S. Braem M. Lambrechts P, Vanherle G.Morp holog ical aspects of the resin-denime i nterd i l lusion zone withdi f ferent dent in adhesive systems, J Dent Res I992;7I : I5 .1 O-¡54 O.
Smith BG N, K nig lnJ K. A com pari son of pat terns of loot h wear withaet io logic i i l faetors, Br D en tJ 19a4; 157; 16-1 9.
Mair LH, Wear in dent ist ry—Current terminology. J Dent 1992;2 0 : 14 0 - 14 4 ,
Jarvinen VK, Rytomaa I I . Heinonen OP, Risk factors in dentaieros ion . J Dent Res 1991:7n:942-947.
Mi lle r C D , Enamei erosive properties of fruits and various bever-ages, J Am Die t Assoc l952 ;28 ; . í l9 -32 4 ,
Rugg-Gunn AJ , Hacket t AF , Ap p le ton DR , Jenk ins G N , Eas toe JE,Relationship between dietary habits and earies inerement assessedover two years in 405 Engl ish adoleseent school ehi ldren . Arc h OralB io i l9S4;29 ;9 i t3 -987 .
Levi tch LC, Bader JD, Shugars DA, Hcymann HO, Non-car iouscervical lesions. J Dent I994;22: i95-2O7.
20. Grob ler SR, Senekal PJC, Laubscher JA In v i t ro dém inéral isat ionof enamel by orange juice, apple juice, Pepsi Cola and Diel PepsiC o l a , Cl in Prev Dent 1990; 1 2,5-9.
21 . Eccles JD. Erosion affecting the palatal surlhces of upper anteriortee lh in young peop le Br Dent J l98 2 ; l5 2 ;3 75-3 78 ,
22, Hel lstro m 1 . Oral compl icat ions in anorexia nervosa, Scand J Den tRes I977 ;B5 ;7 I -S6 .
2 3 , Giunta JL, Dental erosion resul t ing f rom cheivahle v i tamin Clablets. J A m D ent Assoc 19S3; IO7;2 53-25 6.
2 4 , Lmkosalo E, Markkanen H, Dental erosions in rc iat ion lo laclo-vegetar ian diet , Scand J Denl Res I9S5;93:436-441.
25. Rytomaa I, Jarvinen V. Heinonen OP, l it iological factors in dentalerosion ¡abstract 5871 . J Dent Res I99O;69:1 82,
3 6 , Jarvinen V, Meurman JH , Hyvar inen H . Rytomaa 1, Mt i r tom aa H,Dental erosion and upp er gastro intest inal d isorders. Oral Sure Oral
27. i lowdei iGl- , Erosion as the present ing symptom in h iatus herD e n t J l 9 7 1 ; l 3 l ; 4 5 5 - 4 5 6 .
lit. Bart let l DW, tvans DF, Smith BUN. The re lat ionship begjs lro-oesophage al ref lux d isease and denia l eros ion, J Oral Rl9 9 6 i2 3 : 2 H9 - 2 9 7 .
29 Bar t le l t DW, Simlh B G. The dental impact of eat ing d isordersUp d a t e I 9 9 4 ; 2 h 4 1 l 4 - 4 n 7
.10. Simmons MS, Thompson DV . Dental erosion seeondaiy to etinduced emesis. Oral Surg Oral Med O ral Palhol 19 S7;h4;7.1
,11. Smi th BGN, Robb ND. Denta l e ros ion in pa t ien ts w i th caleohol ism. J Dent 1987; 1 7 : 21 9 -221 ,
32. Ta y lo rG. Ta y lo rS, Ab rams R, Mue l le r W, Denta l e ros ion assowith asymptomat ic gastroesophageal ref lux, J Denl Chi ld 5 9 : I S 2 - I S 5 .
3.1, Gi lmour AG, Becke t t HA. The vo lun l i i r y re f lux phenomenoDe n t J I 9 9 3 ; l 7 5 ; . 16 t t - 3 7 1 ,
'4 Bishop K, Deans R. Ac id regu ig i tat ion ; A n occupat ional hazaDe ntJ 1996 : IH 343-34 5 .
3 Í , Treasure J. Long-term management of eating disorders. InPsych ia tiy 1 991 : , ' 43 -5 X.
36. Kid d E A M , Smilh B C N . Toolhw ear h istor ies; A sensit ive Dent Update I989 ;2 ( ) ' l74 -17 i ( ,
37. Al len D N . Denta l e ros ion f rom vomi t ing Or De n l J 1 9 6 9 ; i 2312,
38 . Andre ws l -TTI . Dental erosion due to anorexia nervosa with buBr DemJ I9>Í2 : I52 K9-9O.
39. Stege P, Vi seo-Da ngler L, Rye L. An or ex ia nervosa: Rincluding oral dental manifestat ions J Am Dent Asaoc
411. Abrams RA, RufI LC" Oral sign'^ symptoms in Ihe diagnobu l im ia . J Am Dem Assoc l9Mi i , l 13 :761-764 .
4 I . Robb N Ü , Smi lh BG , Ge id rys-Leeper E, The d is t r ibu t ion o f ein the dent ihons of pat ients with eat ing disorders. Br D
I 9 9 5 ; l 7 8 ; 1 7 i - I 7 5
4 2 , Petersen PE, Gormsen C. Oral condi t ions among German bfac to ry workers , { "ommu n i ty Dent Ora i Ep idem io l I99 I ; I9m 6 .
4 3 , Centerwa i l BS, Arms t rong CW , Funkerhouser LS, E lzay R. t rof dentai enamel among com pet i t ive sw immers at a gas-chlorSw im m in g p o o l . A m J Ep id e m io l 1 9 X6 M 2 3 ; 6 4 l - 6 4 7 .
4 4 , TuominenM, Tuominen R, Ranta K, Rants H, Associat ion beacid fumes in the work environmen t and dental eros ion. ScWork Env i ron Hea l th 1989 :15 :335-338 .
4 5 , Ten Bruggen Cate HJ, Dental erosion in indusiry . Br J Ind19 6 8 : 2 5 : 2 4 9 - 2 6 6 .
4 6 , Abdul iah A, Sher fudhin H, Omar R, Johansson A. Prevalenocclusat toolh wear and its relationship to laterai and proteontact schemes in a young adul t Indian popuiat ion. Acta OScand 1994 :52 :191-197 .
4 7 , Smith BGN. Toothwear: Et io logy and diagnosis. Dent Ul9 K9 : | { i : 2 O 4 - 2 l 2 .
4K, Da hl B L, Krogstad O, Kar lsen K. , A n af ternat ive t reatment inwith advaneed loeali¿ed al t r i l i on , J Oral Reh abi l 19 75:2:209
4 9 , Ekfe ld l A, Hugoson A, Bergenda l T , He lk imo M, A n ind itooth wear inde\ and an analysis of factors correlated to incisaocclusal wear in an adul t Swedish popu lat ion Acta O don tol 19 9 0 , 4 8 : 3 4 3 - 3 4 9 ,
50, Boero RP. The physio logy of spl int therap>; A l i terature r
An g le O r t h o d l 9 K9 i5 9 :16 5 - 1 X0 .
51 , Clarke NG, Townsend GC, Carey SE. Bruxing patterns in
8/7/2019 wear-of teeth-an update
http://slidepdf.com/reader/full/wear-of-teeth-an-update 9/10
Bishop et al
bh ND , Siniih B GN. The iiiltiLeiice of missing poslenor teeili oiiSM I i. I Dem Res
Inpleby J , Mackie R-. C Í Ü L - rtporL: .-̂ n iiiiuaiL;il ouibe c ifu iiu li weiir,IJem Vpdíile 19')5;2; 4.!4-,l."o.
Biirke HT. Wliiiehead SA, McCaiíglioy AD. Conlemporary an yD L I I L
Uptiaii.- i 'm i , : : ; : ! s - . i : .
I liig,ivin A. ikrSL-iiilal T. Ekfeldl A, Helkimo M, freviüeiice :iiiJsoiCdti < > { mcisal and iiccliisal toolli wear in an acliill Swedishpopiiku ioii Ai-ia OdiiiüDl Sc;ind
Donat-liie M A. The Denial H ealtli iif the Aging PopiikiLion uístle nponT>ne I thesis |. University of Neweasllu, \'i')2.
D.uis W B , Wlnlcr P J. Til« elTeet oinbras ion on enamel iiniJ denuncaller e\posiiie to dieurj Lieid. Br Denl J I9K0; MH iíí.l-ÜSó.
BluüinTJ. Metiowell Ü C. Líinü t í R . e t a l . t n viiro wear. Pan 11 . Wearand abrasión o l" coniposile reslorative imiterials, J Proslhel DeiiE
Sejmour RA. Dental pliarm.icology pruhlenis iii Ihe C I Ü L T I S . Dem
Lc\ine RS. Saliva. ! Xerostomia—el olo gj anü m.inagcineni. Dem
Jaeobi R, Shillirsbiiii! HHT, Diincanson MG, A compiirison of th eabrasiveness uf si\ ceramic snrfaces and gold. J Proslhel Dcnl
Hudson JD, Goldslein GR. Geiireescii M. Eiiiiniel wear aiiised bythree diHerent resU.ralne maleriais. J Proslhel Dem l')4.'i;74:647-54
Railedse DK, Smilh BGN. Wilson Rt, The eftecl of re5lor;Uivematerials un Ihe ".ear of human en.imel ,1 Pnisthet Den l 1^44;7: l94- : i l?,
Krejci I. L L I I Z F. Reimer M . Heinzmíinii JL , Wear ot"ceramic inlays,ilieiranlagon isls. and lining cements, J Proslhet Den l I99,.';69.425-
Hussey DL , irw in C R, Kime DL , Trealmenl olante rior luolh wearW im gold palatal yeneers. Br Dent J 1994^176:423-425 C
David Korson
Aesthetic Designfor Ceramic Restorations
The most
Hi) tu r a l ,
cstheric restilts
in dental
ceramics cati
be achieved
with contem-
r a r } ' techniques—and this book describes
how. Investigated arc the cha racteristics of
natural dctitition, tissue martagemetit, impres-
sions, occlusal rec ords, waxing techniques ,
color, and laboratory- techniques, including
methods for an aesthetic ceramic margin,
opalescence, and development of the dentine
ma melo n. Filled with practical tips, this book
is ideal for dentists and technicians.
US$7fi
159 pages; 292 color illus; ISBN 1-85097-ÍI34-3
Contents
1 Studies of Natniral Dentitio n
2 Dcntist-Technician-Patjenr Commi.inication
3 Tissue Managem ent for Aesthetic
and Biological Harmony
4 Impressions and Occlusai Records
5 Aesthetic Wii\ Diagnostic Control
6 Accurate Registration and Communicationof Colour Characteristics
7 Advanced Laboratory Techniques
8 Case Studies
quintswcnccbook/
O r d e r N o w
Toll free 1-800-621-0387
Fax 630 682-3288

8/7/2019 wear-of teeth-an update
http://slidepdf.com/reader/full/wear-of-teeth-an-update 10/10