wcla mcle 11-2-11 utilization review: the new provisions & practical pointers wednesday november...
TRANSCRIPT

WCLA MCLE 11-2-11
• Utilization Review: The New Provisions & Practical Pointers
• Wednesday November 2, 2011• 12:00 noon to 1:00 pm • James R. Thompson Center Auditorium,
Chicago, IL• 1.0 Hour General MCLE Credit
Utilization Review Applicability & Medical Treatment Guidelines
Utilization ReviewMedical Treatment Guidelines
• IL does NOT ADOPT by law or by rule ANY ONE PARTICULAR set of medical treatment guidelines; no one set is correct, presumptively or otherwise
• There are MANY sets of medical treatment guidelines • National Guideline Clearinghouse: www.guideline.gov (2700?); EG:
American Academy of Neurology has 58, “Symptomatic Treatment For Muscle Cramps”
• Some are better than others; Institute of Medicine of the National Academies, “Clinical Practice Guidelines We can Trust;” March 2011, www.iom.edu
• Evidence-based medicine: levels of evidence for primary research question; I-V, from most to least rigorous
• Where does your medical treatment guideline fall?
Utilization ReviewURAC
• Utilization management standards (procedural: how is UR done)• www.urac.org “URAC, an independent, nonprofit organization …
accreditation, education and measurement programs.”• Where do I get the URAC standards?:
http://insurance.illinois.gov/URO/WorkersCompUMStdsv50.pdf• Standard WCUM 14: Peer review must be conducted by person who holds
valid license in “same licensure category” as the ordering provider (Pg. 70)• Standard WCUM 17: Review determination must be made within 72 hours
for urgent care, 15 days for non-urgent care (Pg. 72)• Definition: “Case involving Urgent Care”: 1) serious jeopardy to life or
health or regaining of maximum function ; or 2) severe pain in the opinion of the physician with knowledge (Page 21)
Utilization ReviewSection 8.7, added to subsec. (i)
• (i) Upon receipt of written notice that the employer or the employer's agent or insurer wishes to invoke the utilization review process, the provider of medical, surgical, or hospital services shall submit to the utilization review, following accredited procedural guidelines.
• (1) The provider shall make reasonable efforts to provide timely and complete reports of clinical information needed to support a request for treatment. If the provider fails to make such reasonable efforts, the charges for the treatment or service may not be compensable nor collectible by the provider or claimant from the employer, the employer's agent, or the employee. The reporting obligations of providers shall not be unreasonable or unduly burdensome.
• (2) Written notice of utilization review decisions, including the clinical rationale for certification or non-certification and references to applicable standards of care or evidence-based medical guidelines, shall be furnished to the provider and employee.
• (3) An employer may only deny payment of or refuse to authorize payment of medical services rendered or proposed to be rendered on the grounds that the extent and scope of medical treatment is excessive and unnecessary in compliance with an accredited utilization review program under this Section.
• (4) When a payment for medical services has been denied or not authorized by an employer or when authorization for medical services is denied pursuant to utilization review, the employee has the burden of proof to show by a preponderance of the evidence that a variance from the standards of care used by the person or entity performing the utilization review pursuant to subsection (a) is reasonably required to cure or relieve the effects of his or her injury.
Utilization Review Provider Obligation & Payment
• Added to Section 8.7: (i) Upon receipt of written notice that the employer or the employer's agent or insurer wishes to invoke the utilization review process, the provider of medical, surgical, or hospital services shall submit to the utilization review, following accredited procedural guidelines.
• (1) The provider shall make reasonable efforts to provide timely and complete reports of clinical information needed to support a request for treatment. If the provider fails to make such reasonable efforts, the charges for the treatment or service may not be compensable nor collectible by the provider or claimant from the employer, the employer's agent, or the employee. The reporting obligations of providers shall not be unreasonable or unduly burdensome.
• Is “no payment” penalty mandatory? “may not be compensable nor collectible”
• Who decides if “the provider fails to make such reasonable efforts”? IWCC makes this decision
• What is reasonable, unreasonable, unduly burdensome? Look to URAC procedural guidelines; expert testimony about URAC (EG, PEER TO PEER)
Utilization ReviewRequired in Necessity Dispute?
• 8.7(i) “(2) Written notice of utilization review decisions, including the clinical rationale for certification or non-certification and references to applicable standards of care or evidence-based medical guidelines, shall be furnished to the provider and employee.”
• Impact: Already required by URAC, WCUM 22 (pg. 74)• 8.7(i) “(3) An employer may only deny payment of or refuse to
authorize payment of medical services rendered or proposed to be rendered on the grounds that the extent and scope of medical treatment is excessive and unnecessary in compliance with an accredited utilization review program under this Section.”
• Impact: Necessity must be disputed with UR; IME alone insufficient to dispute necessity; careful practitioners will be wary of waiver of necessity defense; be careful of penalties for unreasonable (by law) defense (necessity dispute without UR)

Utilization ReviewBurden of Proof
• 8.7(i): “(4) When a payment for medical services has been denied or not authorized by an employer or when authorization for medical services is denied pursuant to utilization review, the employee has the burden of proof to show by a preponderance of the evidence that a variance from the standards of care used by the person or entity performing the utilization review pursuant to subsection (a) is reasonably required to cure or relieve the effects of his or her injury.”
• Impact: “When”: always; UR is required to dispute necessity• Impact: “Burden of proof”: No change; EMPLOYEE HAS ALWAYS
HAD BURDEN OF PROOF OF NECESSITY• Impact: “Variance from standards of care”: No change; EG:
Treatment plan different from ACOEM (18 rather than 12 PT’s); Yes, why would Petitioner try case if agrees with ACOEM
• Impact: “Reasonably required…”: No change; straight out of 8(a)

Utilization Review Depositions
• 8.7(i) “(5) The medical professional responsible for review in the final stage of utilization review or appeal must be available in this State for interview or deposition; or must be available for deposition by telephone, video conference, or other remote electronic means. A medical professional who works or resides in this State or outside of this State may comply with this requirement by making himself or herself available for an interview or deposition in person or by making himself or herself available by telephone, video conference, or other remote electronic means. The remote interview or deposition shall be conducted in a fair, open, and cost-effective manner. The expense of interview and the deposition method shall be paid by the employer. The deponent shall be in the presence of the officer administering the oath and recording the deposition, unless otherwise agreed by the parties. Any exhibits or other demonstrative evidence to be presented to the deponent by any party at the deposition shall be provided to the officer administering the oath and all other parties within a reasonable period of time prior to the deposition. Nothing shall prohibit any party from being with the deponent during the deposition, at that party's expense; provided, however, that a party attending a deposition shall give written notice of that party's intention to appear at the deposition to all other parties within a reasonable time prior to the deposition.”
• Impact: A lot more depositions of UR experts; a lot more litigation over dedimus to take UR expert’s deposition
• Impact : Interaction with Rule 7030.60 & Section 16?

Utilization ReviewConsideration & Weight
Utilization ReviewCase Summaries (Win A Few, Lose A Few)– Venable v. United Airlines, 08 W.C. 047340
• UR rejected since purported to impose California standards in Illinois– Chamorro v. Workforce Staffing, 09 I.W.C.C. 55
• UR unpersuasive since answered biased questions posited by employer and misconstrued basic facts of the case, i.e., non-compliant with URAC guidelines
– Salgado v. Cardone Record Service, 09 I.W.C.C. 171• UR adopted to limit chiropractic care to 6 visits
– Garcia v. Executive Mailing Service, 09 I.W.C.C. 0310• UR was rejected since efficacy requirement too restrictive for the proposed
treatment – discogram and intradiscal electrothermic therapy– Jackson v. City of Springfield, 09 I.W.C.C. 1124
• UR adopted to find that 3 to 5 of 68 chiropractic visits were medically necessary
– Cantua v. United Airlines, 09 W.C. 041232– Ramirez v. Gill Management, Inc., 10 I.W.C.C. 0141
• UR adopted to find that only 10 chiropractic visits were medically necessary• UR adopted to deny discogram

Utilization ReviewCase Summaries
– Masso v. Frontline Transportation, 10 I.W.C.C. 0314• UR adopted to find six chiropractic visits reasonable; Commission
rejected arbitrator’s concern that UR could deny necessary prospective medical care
– Vadakin v. Subway, 10 I.W.C.C. 0414• UR that did not include a written report was rejected
– Keafer v. City of Kincaid ,10 I.W.C.C. 0707• UR adopted to find prospective fusion medically unnecessary
– Gomez v. Juno Mfg., 10 I.W.C.C. 1256• UR adopted to find 3-5 weeks of a 10 month period of chiropractic care
was medically necessary– Escatel v. Civil Contractors, 10 IWCC 1255
• UR adopted to find that medical providers billed for unreasonable and excessive care
– Barlow v. Johnny’s Restaurant, 10 IWCC 1291• UR results and objective testing established that elbow surgery was not
medically necessary

Utilization ReviewCase Summaries
– Noemi Solis v. Hospitality Staffing Solutions, 11 I.W.C.C. 792• UR not persuasive because it ignores the complexity of the injuries
– Rosales v. Robert W. Hendricksen Co., 11 I.W.C.C. 776• UR rejected given apparent confusion over location of symptoms –
left vs. right– Carpenter v. State of Illinois, State Retirement System, 11 I.W.C.C. 798
• UR rejected since opined on causation– Coor v. Lagrou Distribution, 11 I.W.C.C. 0660
• UR adopted to support IME finding of MMI– Wilcox v. Professional Transportation, 11 I.W.C.C. 0544
• UR rejected since failed to consider full medical records
Utilization ReviewCase Summaries
– Medrano v. Scholoss Co., 11 I.W.C.C. 919• UR adopted to determine final date for medically necessary care
– Melvan, v. Holcim Cement, 11 I.W.C.C. 819• UR rejected since conclusions mirrored employer’s unsuccessful 19(b)
hearing arguments– Bonadonna v. Wings Program, Inc., 11 I.W.C.C. 448
• UR rejected since UR doctor’s testimony revealed bias to limit treatment in conflict with the ODG
– Hamilton v. David Renshaw D/B/A Dairy Queen, 11 I.W.C.C. 226• UR unpersuasive since “internally inconsistent” and because the UR
doctor not registered or certified to perform a UR– Lorena v. Elite Staffing, Inc., 11 I.W.C.C. 0494
• UR rejected since failed to address significant medical evidence and reference guidelines
– King v. RGIS Inventory Specialists, 11 I.W.C.C. 0579• UR unpersuasive since based solely on one IME and did not consider the
treatment records
Utilization ReviewCase Summaries
– Pinnell v. State of Illinois, Department of Transportation, 11 I.W.C.C. 0218• UR declined to certify massage therapy as well as use of prescription
medications; employer not liable for treatments that URs (conducted by two board certified orthopedic surgeons) did not certify
– Avila v. Elite Staffing, 11 I.W.C.C. 0217• Treatment prescribed by doctor found medically necessary though contrary
to UR findings; ordering physician’s opinion more credible given UR’s qualifications and the UR’s lack of response to the ordering physician’s opinion
– Mejia v. Ron’s Staffing, 11 I.W.C.C. 0164• UR certified only 6 of 107 chiropractic visits. Arbitrator found no credible
medical basis to justify all the chiropractic treatments and PT relying on UR– Fernandez v. ADP Total Source/ H.R. Slater Co., 11 I.W.C.C. 0164
• UR non-certification of recommended lumbar-fusion, citing the need for multiple issues to be addressed pre-operatively, ordering doctor failure to appeal, and opinion of IME physician resulted in denial of surgery
Utilization Review in IllinoisNovember 2011
Utilization Review - history
State of Illinois requirements of URO
URAC Standards
Types of Review / URAC Process/Timeframes
Guidelines – Evidence-based Medicine
Arbitrator Feedback
Review UR determinations closely
Request Attorney Packet from UR
CorVel contact information
© 2011 CorVel Corporation.
Overview

Medicare
Medicaid
HMO plans
PPO Plans
Slowly states have begun to adopt this practice for workers’ compensation cases
© 2011 CorVel Corporation.
Utilization review is NOT new

Abuses
Overuse of testing
Inappropriate testing for diagnosis
Inappropriate hospital stays
Lengthy hospital stays
Medical studies – that physicians rely on – have always been around to help physicians – specialty organizations decide on treatment
© 2011 CorVel Corporation.
Why was UR instituted?
UROs are required to follow the URAC standards “sufficient to achieve URAC accreditation” (820 ILCS 305/8/7)
“Nothing in this Act shall be construed to require an employer or insurer or its subcontractors to become URAC accredited.” (820 ILCS 305/87)
Must register and apply for certification with the State of IL every 2 years.
© 2011 CorVel Corporation.
State of Illinois requires companies who perform UR

“Protector of the Utilization Process” Originally URAC was incorporated under the name Utilization Review Accreditation Commission” – the name was shortened to just the acronym “URAC”
Accreditation serves as a symbol of excellence in the health care industry
The standards apply to the utilization management process when it occurs in a workers’ compensation setting
There are CORE Standards and WCUM standards - primary element has direct & significant impact on the welfare and safety of consumers/patients. The secondary element is desirable of a high quality program but does not have a direct impact on welfare and safety of consumers
© 2011 CorVel Corporation.
URAC and its Standards (WCUM)
Utilization Review
Types
Process
© 2011 CorVel Corporation.
Prospective reviews (pre-certs)
Concurrent reviews (ongoing treatment)
Retrospective reviews (treatment has been rendered)
© 2011 CorVel Corporation.
Types of Utilization Review
Initial Review
The nurse receives the request for review and medical records
If additional records are required, the nurse can contact the provider
Nurse reviews the medical records and the treatment under review
Applies to ODG guidelines
Certifies if treatment is appropriate
Informs the provider by phone of the certification
Sends certification letters to provider, injured employee, attorney, adjuster
If the treatment does not meet guidelines
© 2011 CorVel Corporation.
UR Process
The UR nurse refers to Clinical Peer Reviewer
Utilizing evidence based medicine and nationally recognized guidelines, the Clinical Peer Reviewer (medical doctor) reviews & provides a UR determination
Based on Peer decision, the Certification or Non-Certification Letters are sent to all parties
Appeal process and peer report are sent with all non-certifications
© 2011 CorVel Corporation.
UR Process – when guidelines not met
Licensed doctor of medicine or doctor of osteopathic medicine
or
Licensed health professional in the same licensure category as the ordering provider
or
Health professional with the same clinical education as the ordering provider in clinical specialties where licensure is not issued
© 2011 CorVel Corporation.
Clinical Peer Reviewer
Clinical Peer must be available to discuss review determinations with the treating provider
Requested by treating provider
Purpose: allows treating provider a chance to discuss a UM determination before the initiation of the appeal process. (hopefully avoiding need for formal and adversarial appeal process)
© 2011 CorVel Corporation.
Peer-to-Peer Conversations
30 days to Appeal
UR Organization receives appeal request via fax or phone - can be made by treating provider, injured employee, attorney
Sent to Clinical Peer Reviewer w/ any addl medical info
Nurse sends out Cert or Non-Cert Ltr based on Peer determination
2 types of appeals: expedited and standard
Right to standard appeal, if utilized expedited
© 2011 CorVel Corporation.
Appeal process
Hold an active, unrestricted license to practice medicine or a health profession
Must be Board-certified
Are in the same profession and in a similar specialty as typically manages the medical condition
Are neither the individual who made the original non-certification, nor the subordinate of such individual
© 2011 CorVel Corporation.
Clinical Peer Reviewer for Appeals
For lack of medical records
UR calls provider requesting records
Calls 2nd day requesting same
3rd day sends out Non-Cert for Lack of Medical Records
Once records received – UR process continued
© 2011 CorVel Corporation.
Administrative Non-Cert

ODG, ACOEM, Milliman-Roberts, Interqual
Best practice, evidence-based medicine
Evidence-based recommendations are based on valid scientific outcomes research, preferably research that has been published in peer reviewed scientific journals.
Evidence-based information can be used to develop protocols, pathways, standards of care or clinical practice guidelines and related educational materials
ODG updated regularly at 3 month, 6 month or yearly episodes
© 2011 CorVel Corporation.
Guidelines utilized by Nurses and Peer Physicians – Nationally Recognized
The practice of evidence-based medicine means integrating individual clinical expertise with the best available external clinical evidence from systematic research.
Physicians arrive at medical decisions by relying on standards of care and individual clinical experience:
Without clinical expertise, practice risks becoming tyrannized by evidence, for even excellent external evidence may be inapplicable to or inappropriate for an individual patient
Without current best evidence, practice risks becoming rapidly out of date, to the detriment of patients
© 2011 CorVel Corporation.
Physicians utilize evidence-based medicine – what is evidence-based medicine?
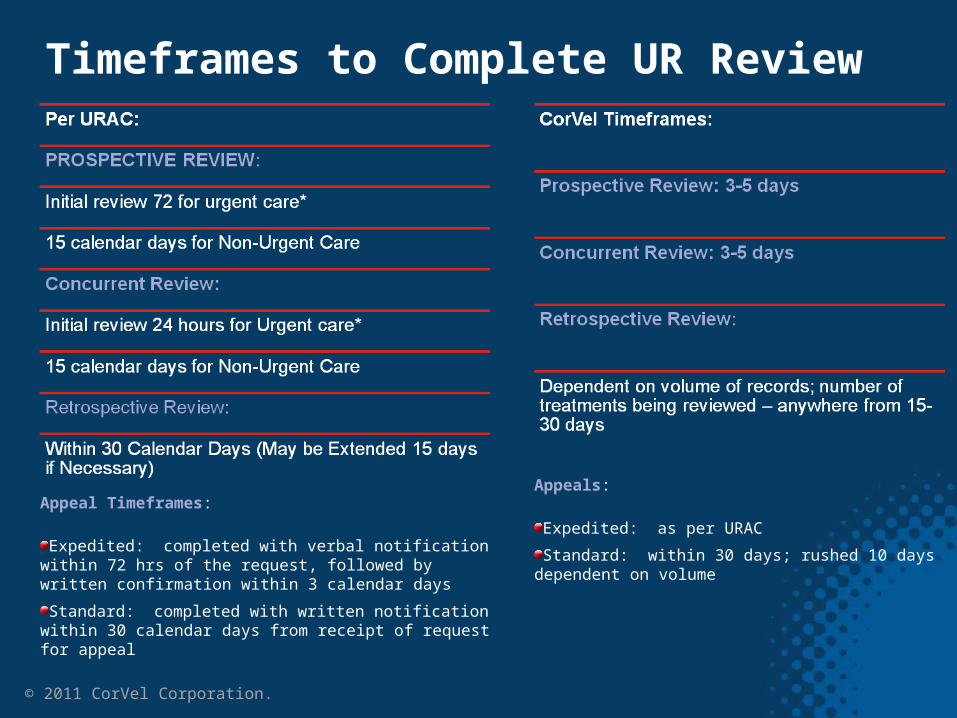
Appeal Timeframes:
Expedited: completed with verbal notification within 72 hrs of the request, followed by written confirmation within 3 calendar days
Standard: completed with written notification within 30 calendar days from receipt of request for appeal
© 2011 CorVel Corporation.
Timeframes to Complete UR Review
Appeals:
Expedited: as per URAC
Standard: within 30 days; rushed 10 days dependent on volume
Notified by Phone
Followed up with a letter of certification
Non-certification letters include the Appeals Process and Peer Report
© 2011 CorVel Corporation.
How is the Treating provider contacted?
© 2011 CorVel Corporation.
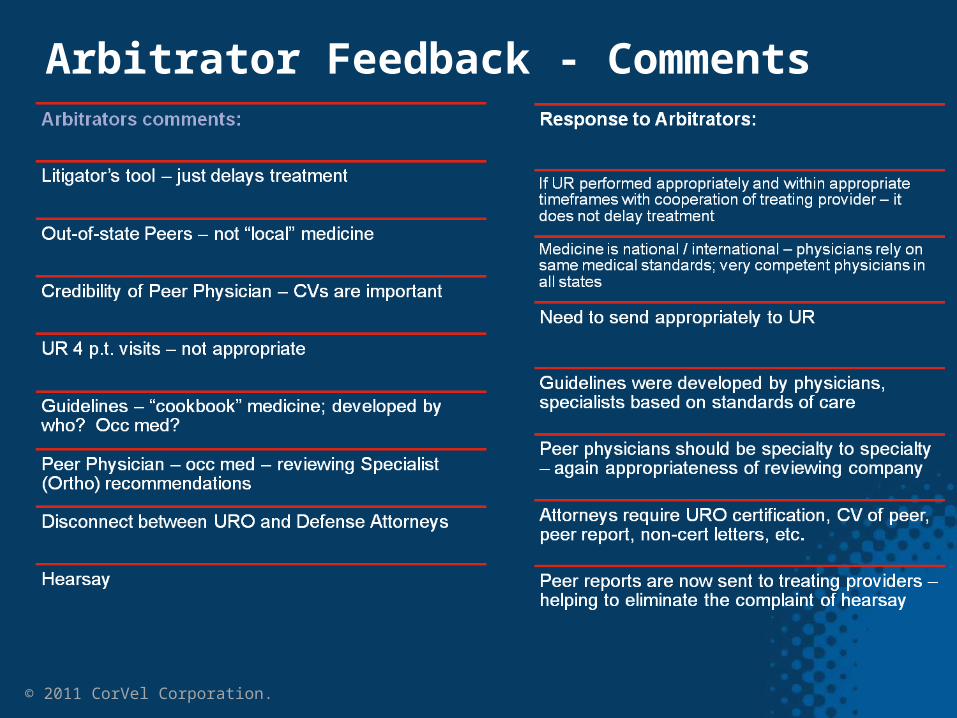
Arbitrator Feedback - Comments

Avoids unnecessary surgery
2nd or 3rd or 4th surgeries
Promotes discussion between physicians on controversial treatment
Patient is not a candidate
Experimental
Success rate
Serves the patient if utilized appropriately
© 2011 CorVel Corporation.
Utilization Review is Beneficial

Is the non-cert due to poor documentation of the treating provider?
Is the non-cert for a minimal amount of p.t. visits?
Did the URO have the correct medicals in order to process UR?
MRIs are needed to review for appropriateness of surgery
If there is a case manager on the case, ask the nurse to closely review the rationale for non-cert
URO should have QA’d the peer report for accuracy
© 2011 CorVel Corporation.
Review the UR determination closely
Refer to UR prospectively, concurrently
Notify the provider in writing upon acceptance of the claim that utilization review is utilized on certain treatment
Follow the process – allow appeals, peer-to-peer conversations
© 2011 CorVel Corporation.
Encourage your clients to:
CorVel’s State of IL certification
URAC Accreditation certificate
UR non-certification letter
Peer Report & Peer CV
Appeal confirmation
Appeal determination, Peer Report & Peer CV
Reports on Peer-to-Peer conversations
© 2011 CorVel Corporation.
Call CorVel UR to Request an “Attorney Packet”
© 2011 CorVel Corporation.
CorVel UR – Contact and Referral Information
Jenny Weber, RN, UR Supervisor
Phone: 630-874-7357
e-mail: [email protected]
Complete referral form – in packet
E-mail: [email protected]
Questions for referral: Kim Lindholm at
630-874-7362

© 2011 CorVel Corporation.
Questions?