wandsworth respiratory clinical reference group annual ... board pa… · attach 3 1 wandsworth...
TRANSCRIPT

Attach 3
1
Wandsworth Respiratory Clinical Reference Group Annual Progress Report
2014/15
April 2015
Dr Kieron Earney & Kate Symons
Acknowledgements Dr Sarah Deedat Public Health Lead for Long Term Conditions
Attach 3
2
1. Introduction
The Purpose of this report is to provide the Wandsworth CCG Board with an update on the progress
on developing and delivering service improvements aimed at the identification, clinically accredited
diagnoses and treatment of Chronic Obstructive Pulmonary Disease (COPD) and Asthma for the
population of Wandsworth. The focus is on the outcomes achieved over the previous year and the
future plans for delivering service improvements lead by the Respiratory Clinical Reference Group
(RCRG) in Wandsworth.
This is the third year of the Respiratory Clinical Reference Group. The group consists of representatives
from St Georges including a Nurse Consultant, Community Specialist Nurses, Local GPs, Local Authority
Colleagues and CCG Medicine Management representation. This year has seen a change in Clinical
Leadership with Dr Charlotte Levitt stepping down from Clinical Chair to Locality Lead for Wandle and
Dr Kieron Earney taking on the Clinical Char role from his previous role as West Wandsworth Locality
Lead.
The purpose of the group is to implement the strategic intentions of Wandsworth Clinical
Commissioning Group in the commissioning of services for the identification, clinically accredited
diagnosis, and treatment of COPD & Asthma for the population of Wandsworth.
This is also the first year of implementing service improvements linked to the Out of Hospital Strategy
which sees the group working towards a number of key activities to deliver effective community based
services delivering high quality care for our patients in Wandsworth. This report is based on our
progress in delivering these outcomes in the first year of a two year programme. Significantly this
year we have also shifted some of our focus towards Asthma as the group has previously solely
focused on COPD as a priority.
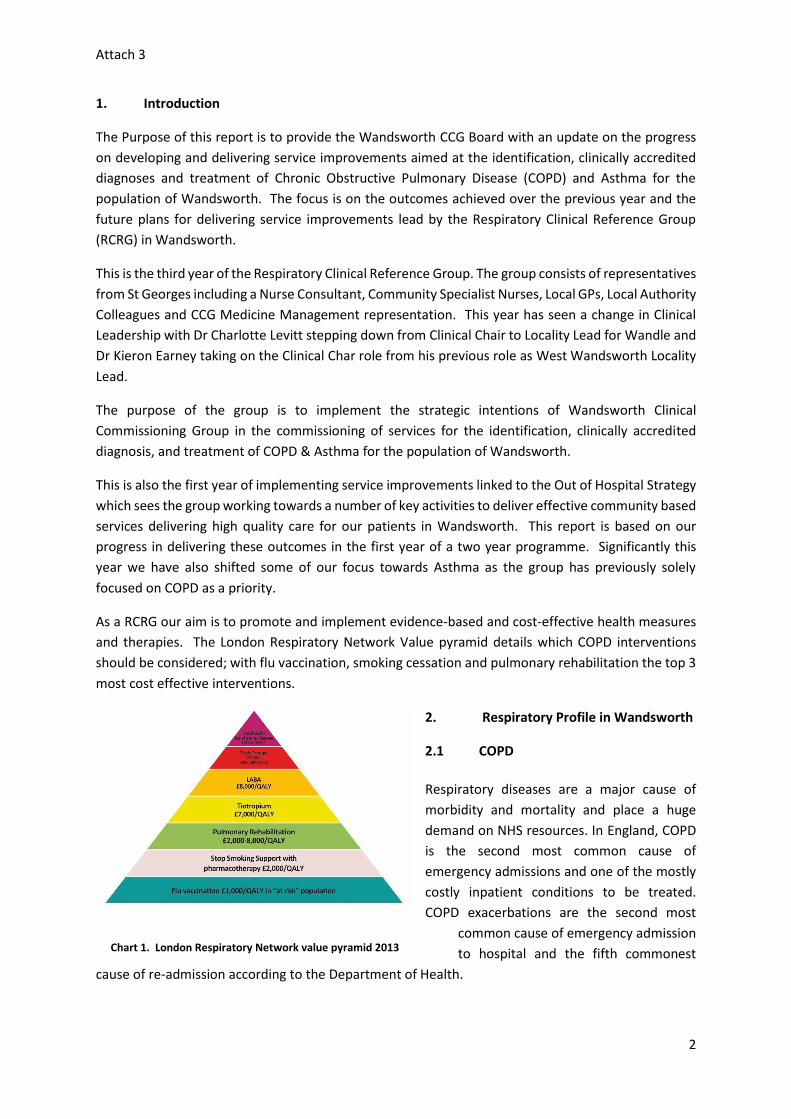
As a RCRG our aim is to promote and implement evidence-based and cost-effective health measures
and therapies. The London Respiratory Network Value pyramid details which COPD interventions
should be considered; with flu vaccination, smoking cessation and pulmonary rehabilitation the top 3
most cost effective interventions.
2. Respiratory Profile in Wandsworth
2.1 COPD
Respiratory diseases are a major cause of
morbidity and mortality and place a huge
demand on NHS resources. In England, COPD
is the second most common cause of
emergency admissions and one of the mostly
costly inpatient conditions to be treated.
COPD exacerbations are the second most
common cause of emergency admission
to hospital and the fifth commonest
cause of re-admission according to the Department of Health.
Chart 1. London Respiratory Network value pyramid 2013

Attach 3
3
National surveys suggest the number of patients recorded as having COPD is low compared to the
number diagnosed. The QOF COPD register in Wandsworth for 2013/2014 shows a population
prevalence of 0.90% (3340), this is lower than both the London Average of 1.08% and the National
average of 1.80%.
For every patient with COPD registered in Wandsworth, 2.7 remain undiagnosed, this is similar to our
statistically comparable neighbour of Hammersmith and Fulham who are ‘missing’ 2.6 people.
Appendix 1 details how we compare against some our Inner London neighbours, the lowest performer
being Lambeth where there are 3.4 potentially ‘missing patients’ for every person registered.
2.2 Asthma
Prevalence levels for asthma can be derived from local general practice Quality and Outcomes
Framework (QOF) information, as all patients with a diagnosis of asthma should be on their general
practitioners asthma register. For Wandsworth CCG, 15,390 people were on an asthma register in
2013/14 (a population prevalence of 4.1%). However, this method of measuring prevalence relies on
the diagnostic accuracy of the GP’s in the area and coding activity. It is possible that there will be
significant levels of undiagnosed asthma in the community.
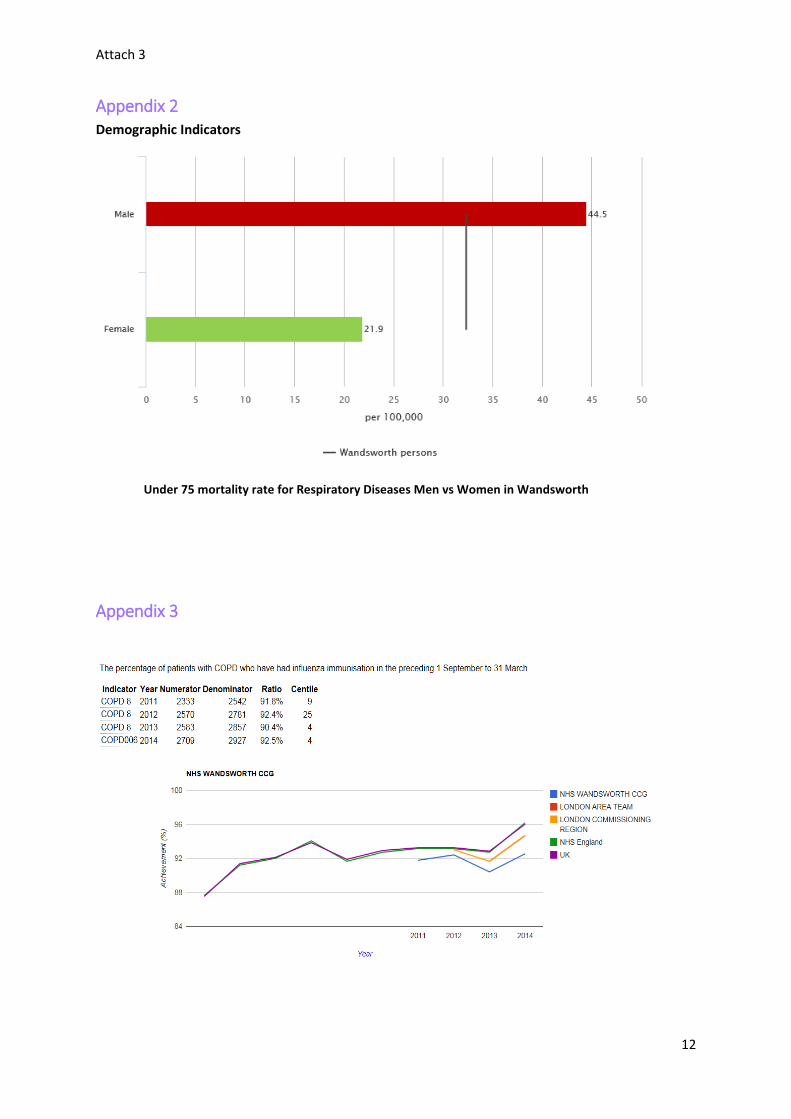
Mortality from Respiratory Diseases
The under 75 mortality rate in Wandsworth for respiratory diseases is 23.0 per 100,000
however this figure conceals important gendered variations in mortality.
There is a greater burden of mortality for respiratory diseases among men than women in
Wandsworth.
The under 75 mortality rate for respiratory diseases for men in Wandsworth is double that
of women (44.5/100,000 vs. 21.9/100,000) (Appendix 2)
There were 45 excess deaths due to respiratory disease among men in the most deprived
deprivation quintile and 48 excess deaths among women in the poorest deprivation
quintile.
3. Performance/Progress over the last 12 months
The work that we have focussed on in 2014/15, and we are working towards in 2015/16, can be
divided into 3 broad categories: prevention of disease, detection of existing disease and treatment.
3.1 Prevention of Respiratory Disease
3.1.1 Smoking
Smoking is thought to have an attributable fraction of between 80 and 90% for COPDi, and as such
COPD can largely be considered preventable due to its link with smoking. Understanding the pattern
of smoking in Wandsworth is therefore important to understanding the pattern of disease. According
to the JSNA 55,000 people are estimated to smoke in Wandsworth. This equates to approximately
16% of the population. Smoking prevalence is 15% higher in the most deprived wards; 28% vs 13%.
Smoking Cessation programmes are led by Wandsworth Borough Council however the RCRG are
working jointly with the Wandsworth Borough Smoking Cessation Team piloting an approach to

Attach 3
4
identifying the undiagnosed COPD smokers. 2014/15 data from the smoking cessation services shows
a reduction in individuals setting a quit date and in 4 week quit rates
3.1.2 Flu Vaccination
The COPD value pyramid notes that the most cost effective intervention for COPD is the flu
vaccination. Around 17% of deaths from flu each year are in people with chronic respiratory disease.
People with COPD and some people with asthma are eligible for the seasonal flu vaccine. Based on
QOF data, 2013/14 saw an increase in the numbers of people with COPD who have had a flu
vaccination from 90.4% to 92.5% (see Appendix 3), in line with an increase seen both across London
and England. In the coming year we would like to work with Public Health to see if we can support
the Flu Vaccination plan in order to increase up-take where this is low.
3.1.3 Air Quality
According to the Department of Health “….air pollution may have made some contribution to the
earlier deaths of up to 200,000 people in 2008, with an average loss of life of about two years per
death affected.”
In Wandsworth poor air quality is a contributory factor to 6.6% of deaths annually the effects of poor
air quality are likely to have a greater impact on those with respiratory conditions.
Public Health Outcomes Framework indictors on mortality for Wandsworth Council
Deaths per 100,000 per year
Cancer (premature deaths) 140.8
Cardiovascular disease (premature deaths) 89.1
Cancer (preventable, premature deaths) 81.7
Communicable diseases 72
Cardiovascular disease (preventable, premature deaths) 45.7
Deaths attributable to long term exposure to PM2.5 (6th) 40.5
Respiratory disease (premature deaths) 33.8
Respiratory disease (preventable, premature deaths) 20
The lead for Air Quality from Wandsworth Borough Council attended the RCRG in order to raise
awareness of the impact on air quality on respiratory conditions. It is understood that the Council will
be going out to consultation on the Air Quality Plan after May 2015 and it may be useful for the RCRG
to be involved as part of this consultation process. The impact on air quality to both COPD and Asthma
patients was also noted in training given to Member Practices and raised internally with CCG staff
during a market place event. As a result of this the RCRG promoted the use of airTEXT (an air pollution
texting service) to our clinical staff within the RCRG as a way of identifying incidences when air quality
could exacerbate people’s respiratory conditions. Although this is not a piece of work that the CRG
have prioritised, and lies outside of the remit of the RCRG, it is worth considering in future joint work
with the Local Authority.

Attach 3
5
3.2 Identifying the Undiagnosed
3.2.1 GRASP COPD Toolkit pilot
Previously the RCRG implemented a COPD ‘Missing Millions’ programme across Wandsworth practices
using practice EMIS searches and the Lung Function Questionnaire to identify possible at-risk COPD
patients. This pilot programme aims to build on the success of the previous project with a targeted
approach to identifying potential COPD patients using the newly released GRASP COPD software
programme.
The aims of the COPD identification programme is to provide:
Screening and early detection of undiagnosed Chronic Obstructive Pulmonary Disease (COPD)
Risk-assessment and therapeutic optimisation of patients with a known diagnosis of COPD.
Increase COPD QOF prevalence
Improve coding for patient safety and maintenance of accurate medical records
Enhance patients quality of life
This year the RCRG have been working on developing the outline for this programme to target the
practices with the highest number of potentially undiagnosed COPD patients. Two practices have
been piloting the IT software to review the process involved and the outcomes of implementing the
project.
Initial data from the pilots showed that of those identified from GRASP at potentially high risk COPD
patients:
5% were diagnosed with COPD following an initial review of their notes
30% were identified as needing further investigation
These patients are currently in the process of being reviewed and as such we do not yet have
information as to whether further new diagnoses have been made.
3.1.2 Lung Function Questionnaire Smoking Cessation Pilot
The RCRG are working with the Wandsworth Borough Smoking Cessation Team to pilot the use of the
Lung Function Questionnaire as part of the Smoking Cessation pathway. The Lung Function
Questionnaire (LFQ) has been developed as a case finding tool to identify patients who are appropriate
for spirometry testing to confirm the diagnosis of COPD.
As previously noted smoking is a major contributing factor for COPD, therefore it was felt that utilising
the LFQ as part of a smoking cessation appointment could identify potentially undiagnosed and
previously unidentified COPD patients. This work-stream has been developed within the group
throughout the year and we are now in a position to begin this pilot in collaboration with the Public
Health Smoking Team.
4. Improving treatment and management of Respiratory Conditions
4.1 Integrated COPD Model – Specialist Tier 3 Community Clinic
The integrated COPD commissioning model was launched in November 2011 which described
integrated provision of COPD care and management with the emphasis of patient centred care
Attach 3
6
delivered through a primary & community care led service. The integrated model adopts a tiered
approach to service delivery in line with department of health guidance, NHS & NICE guidance. In
2014/15, a CQUIN was established with St Georges to pilot part of the Integrated Pathway; a
consultant led community COPD clinic in order to evaluate the model and gauge an understanding of
the outcomes and potential future costs of delivering this service. The service was implemented on
a small scale out of Queen Mary’s Hospital with one clinic taking place every week. The aim of the
clinic is to receive referrals for the following:
Support in making a diagnosis of COPD
Questions over the diagnosis of COPD
Rapid deterioration in lung function
Deterioration in symptoms
Post discharge
The pilot clinic was established later than anticipated therefore a request was made to extend the
service beyond the lifetime of the CQUIN to ensure that valuable data on outcomes was available to
evaluate the success of the service.
This pilot is currently being reviewed along with the whole pathway to identify the best option for
providing an integrated approach to managing COPD.
4.2 Asthma Review
In 2014/15 a review of Asthma Services in Wandsworth was undertaken as it was acknowledged that
the group had previously focussed their work plans around COPD. The review mapped current
services across Wandsworth against current NICE quality standards and quality outcome measures
with the overarching aim of improving the identification, diagnosis and treatment of patients with
asthma. In May 2014 The National Review of Asthma Deaths was published, which was the first
national investigation of asthma deaths in the UK. Some of the key points to note from the review
were that:
During the final attack of asthma 45% were known to have died without seeking medical
attention
There was a history of a previous hospital admission for asthma in 47% of those who died
Better education is needed for doctors, nurses, patients and carers to make them aware of
the risks. They need to be able to recognise the warning signs of poor asthma control and
know what to do during an attack.
All patients should be provided with a personal asthma action plan (PAAP), which can help
them to identify if their asthma is worsening and tell them how and when to seek help
Many of the RCRG priorities for 2015/16 are in response to the outcomes of the Asthma review,
targeting our future programmes of work on some of the key recommendations.
4.3 Medicine Management Initiatives
The RCRG supported the use of high dose steroid cards developed by the London Respiratory Network,
as part the work to ensure that patients are receiving the appropriate information and support when
prescribed high doses of Inhaled Corticosteroid (ICS) agents. The aim of these cards is to ensure that
healthcare professionals use them as an opportunity to consider the appropriateness of ICS

Attach 3
7
prescribing as well as increasing an individual’s ICS dose, and that in doing so the patient is made
aware of the possible risks.
4.4 Training and Education
Providing regular accredited training is considered key to successfully implementing improvements in
the detection and management of people with Respiratory conditions in primary care. In recognition
of this a number of training programmes for Health Care Professionals have been commissioned in
2013/14. These include accredited spirometry training, basic spirometry workshops, asthma
workshops, and Respiratory Diploma.
A respiratory focused Members Development Programme took place in November where general
practice staff received training, presentations and updates from various members of the RCRG. This
included the launch of the high dose steroid cards.
4.5 CCG Market Stall
In November the RCRG held a successful market stall within the CCG offices to promote the work of
the group. We had information stands from Wandsworth Borough Council on air quality as well as
the pulmonary rehabilitation Service.
4.6 Spirometry Service Spec Development
The RCRG supported the development of the Spirometry Specification as part of a wider diagnostic
pathway work within the CCG. The group reviewed the specification and a number of the HealthCare
Professional involved in the group inputted into the development of the document.
4.7 Patient and Public Involvement
The group continue to work with the PPI team to look at the most effective ways of engaging patients
and the public in the work of the group. A PPI action plan is in place which includes a plan to include
patient discovery interviews as part of our development of asthma pathways, development of a critical
friends group and look at making links with programme such as pulmonary rehabilitation and the
expert patient programme.
5 Spotlight on Community Pulmonary Rehab Service
Pulmonary rehabilitation has Grade A clinical evidence to support improvements in exercise capacity,
dyspnoea and health status. Pulmonary Rehabilitation has been provided at St Georges for over 10
years, but as diagnosis of COPD has increased and the research behind Pulmonary rehabilitation
developed, referrals from both primary and secondary care increased for predominantly patients with
COPD, but also other chronic respiratory disease such as bronchiectasis, chronic asthma and Lung
Diseases. Guidelines suggested that programmes should be provided in convenient locations to
patients to avoid long distances travelled, with research showing the benefits to starting Pulmonary
Rehab earlier following acute exacerbations of COPD, something which was not possible in the existing
service at St Georges. Following secured non recurrent funding as part of the Out of Hospital Strategy
a Community Respiratory Physiotherapy Programme was developed to deliver a pulmonary
rehabilitation service (for both routine and post exacerbation) which is based in community and home
based settings across Wandsworth borough localities. Since the initiation of this new service it is now

Attach 3
8
available at an additional three locations around the borough along with a new programme providing
pulmonary rehabilitation to housebound patients.
This new service also covers the provision of a rapid access to community respiratory physiotherapy to assist with admission avoidance. The outcomes to date from the service include:
Reduction in the Pulmonary rehabilitation Service waiting list from 12 weeks to 5 weeks and
an increase in completion rate
Development of a new pathway which sees community respiratory provision to prevent COPD
hospital admissions and readmissions
A reduction in 30 day admissions following this from 41% to 23.5%. This can partly be
attributed to the rapid referral process for COPD patients discharged from A&E to the
community physiotherapy team who will visit within 2 weeks of discharge
As per the service specification the team have the ability to provide specialist assessment and
treatment for exacerbating COPD patients.
Reduction in the respiratory physiotherapy out-patient waiting list from 6 months to 3 months
No patients dying on the waiting list.
In the 2 months (Dec-Jan) the respiratory therapy team have identified 36 Wandsworth COPD patients
who attended A&E during exacerbation who had an average hospital length of stay of less than 72
hours in AMU. These patients were referred to the community respiratory physiotherapy team who
assessed and treated these patients at home. Only 4 of these patients have been re-admitted
suggesting only a 11% readmission rate following follow up in community.
There is currently a 36% unmet need for COPD patients admitted to A&E who are not being followed
up by the respiratory physiotherapy team. With increased capacity this could further improve the 30
day re- admission rates for COPD patients. A business case to secure recurrent funding which will also
support an increase in capacity has been submitted to secure this service in the future.
Mr B – A Patient Story
Mr B was referred to the community respiratory physiotherapy team following a prolonged stay in
hospital including an ITU admission. On assessment at home he was struggling with airway clearance,
breathlessness on minimal exertion leaving him unable to sleep upstairs or leave the house. His
daughters were concerned about him managing at home and felt that he needed to go back to
hospital. Patient and carer education regarding airway clearance techniques, inhaler technique, and
contact numbers for the community respiratory nurses was provided from the Pulmonary Rehab Team.
A programme of strengthening and cardiovascular exercise was started at home, and continued twice
a week supervised by physiotherapy assistant. He was able to be transferred to one of the Community
Pulmonary Rehabilitation classes after 4 weeks and was now able to climb the stairs and home, and
make his own way to Pulmonary Rehabilitation.
His daughters felt supported at home knowing community nurses and physiotherapists were available
to call for advice if needed rather than calling an ambulance.
Mr B is enjoying the class and said “I never thought I would be able to do this when I came home from
hospital”.
Attach 3
9
6. Future Plans & Priorities for 2015/16
Asthma care planning
The previous focus of the RCRG has been on COPD care pathways, as such it is recognised that a shift
in focus towards Asthma is required to ensure that the group develop robust high quality pathways
and programmes in order to meet national quality standards and guidelines. It is recognised that less
than a quarter of Asthma patients have an Asthma Care Plan.
In 2015/16 the RCRG will prioritise and promote the use of Asthma Care plans in general practice as
part of a systematic care management pathway. EMIS have recently released an integrated electronic
Asthma Care plan in conjunction with Asthma UK. The inclusion in EMIS of the care plan will mean
that the system will prompt GPs to complete an action plan if a patient doesn’t have one.
Medicine management – review of salbutamol prescribing
Our prescribing advisor is currently developing an audit that practices can carry out which looks at
prescribing of high dose steroids in COPD and Asthma, incorporating and promoting the use of high
dose steroid cards as a learning tool and serves as a reminder about what constitutes a high dose of
steroid and when to reduce down after an increase in the steroid dose.
Finding the undiagnosed patients
LFQ and Smoking cessation programme
During 2015/16 a joint pilot programme will be implemented with the Smoking Cessation Team to
include Lung Function Questionnaires as part of the smoking cessation pathway. This will include work
with Public Health data to target the programme in the deprived wards in the Borough, where there
is a high prevalence of smoking adults.
GRASP COPD Missing Millions
The Group will continue with the implementation of the GRASP toolkit in Primary Care initially
targeting the top five practices which have the largest gap between the observed and estimated
prevalence rate for COPD.
Primary Care pathways
Closer working with public health to utilise data to improve diagnosis and treatment programmes to
target individual practices where the prevalence would be far lower than expected.
Pulmonary rehabilitation
The funding for the Community Pulmonary Rehabilitation Programme is currently only non-recurrent
and will end in 2015/16. An additional business case has been submitted to secure further recurrent
funding for the service which will also support an increase in capacity. The group will continue to work
with the Pulmonary Rehabilitation Team to review the service developments.
Generic Improvement Principles
The RCRG aims to develop joint working opportunities with Public Health on some of the more wider
determinants of health, this could include targeting men as part of our missing millions programmes,
and supporting the smoking cessation initiatives in general practice. The group would also support
some joint working with the local authority to look at identifying best practice from other areas to
share learning and support improvements.
Attach 3
10
7. Conclusions and Recommendations
The Board are asked to note the work of the CRG. The Board are also asked to note the outcomes
from the first year of the Community Pulmonary Rehab service in particular and support our approach
to securing the future of this successful and evidence based programme via our CCG investment
process.
The Board are also asked to note our move to look at joint working opportunities with the Local
Authority.

Attach 3
11
Appendix 1
Attach 3
12
Appendix 2 Demographic Indicators
Under 75 mortality rate for Respiratory Diseases Men vs Women in Wandsworth
Appendix 3

Attach 3
13
Appendix 4 Examples of Pulmonary Rehabilitation Classes in Wandsworth

Attach 3
14
iMannino DM. COPD: epidemiology, prevalence, morbidity and mortality, and disease heterogeneity. Chest 2002; 121: Suppl. 5, 121S–126S.