waldenström macroglobulinemia: from biology to treatment · waldenström macroglobulinemia: from...
TRANSCRIPT

Waldenström macroglobulinemia: From biology to treatment
Ilyas Sahin1,*, Houry Leblebjian2,*, Steven P. Treon1, Irene M. Ghobrial1
1Department of Medical Oncology, Dana-Farber Cancer Institute, Harvard
Medical School, Boston, MA, USA
2Pharmacy Department, Dana-Farber Cancer Institute, Harvard Medical School,
Boston, MA, USA
* These authors have equal contribution
Corresponding author:
Irene M. Ghobrial, MD
Medical Oncology, Dana-Farber Cancer Institute,
450 Brookine Ave Boston, MA, 02115
Phone: (617)-632-4198
Fax: (617)-632-4862
Email: [email protected]
Key words: biology, Waldenström macroglobulinemia, MYD88, bruton tyrosine kinase, treatment
Running title: Waldenström macroglobulinemia
Abstract: 117; Text: 6127; Table: 2; References: 116
1

Abstract
Waldenström macroglobulinemia (WM) is distinct B-cell lymphoproliferative
disorder primarily characterized by bone marrow infiltration of lymphoplasmacytic
cells along with production of a serum monoclonal immunoglobulin M (IgM). In
this review, we describe the biology of WM, the diagnostic evaluation for WM with
a discussion of other conditions that are in the differential diagnosis and clinical
manifestations of the disease as well as current treatment options. Within the
novel agents discussed are everolimus, perifosine, enzastaurin, panobinostat,
bortezomib and carfilzomib, pomalidomide, and ibrutinib. Many of the novel
agents have shown good responses and have a better toxicity profile compared
to traditional chemotherapeutic agents, which makes them good candidates to be
used as primary therapies for WM in the future.
2

Introduction
Waldenström macroglobulinemia (WM) is a B-cell lymphoproliferative disorder
characterized by bone marrow infiltration of lymphoplasmacytic cells along with
production of a serum monoclonal immunoglobulin M (IgM)[1,2]. WM first
described by Jan Gosta Waldenström in 1944 by reporting two patients
presented with oronasal bleeding, anemia, high serum viscosity,
hepatosplenomegaly and infiltration of the BM by lymphoid cells. Unlike multiple
myeloma, the patients had lymphocytic bone marrow infiltration rather than
plasmacytic and no bone lesions or symptoms [3,4].
WM is classified as a lymphoplasmacytic lymphoma (LPL) according to World
Health Organization (WHO) and the Revised European American Lymphoma
(REAL) classificiations [4,5]. WM is a rare cancer with an incidence rate of about
3 cases per million people per year in the United States.1,500 new cases are
diagnosed with WM each year in the United States [6,7]. The median age at
diagnosis varies between 63 and 68 years [1]. Men are twice more commonly
affected compared to women and, incidence rates for white population are 2-3
fold higher than in black population [8].
Biology of WM
The cell of origin
WM is thought to originate from an arrested B cell that has undergone somatic
hypermutation in germinal center without differentiating to plasma cells [9]. It has
been shown that WM may originate from an IgM+ and/or IgM+IgD+ memory B
cell without initiating switching events. WM cells are characterized by a specific
immunophenotype (positive for surface IgM, CD19, CD20, CD22, CD25, CD27,
FMC7; negative for CD103, and variable CD5, 10, 23, CD138 expression), which
help in differentiating from other NHL and multiple myeloma that appear
morphologically similar.
Cytogenetic findings and copy number variations
3
The most common cytogenetic abnormality in WM patients is the deletion of the
long arm of chromosome 6, which was reported in about 40-50% in recent
studies [10-12]. Other studies demonstrated the presence of other cytogenetic
abnormalities, including trisomy 4, trisomy 5, monosomy 8, and deletion of the
long arm of chromosome 20 [10].
It has been reported that 83% of patients with WM have various chromosomal
abnormalities [13]. Gain of 6p was the second most common abnormality (17%),
which was always concomitant with 6q loss. B lymphocyte-induced maturation
protein-1 (BLIMP-1) and tumor necrosis factor α-induced protein 3 (TNFAIP3 or
A20) are the two candidate tumor suppressor genes mapping two distinct
minimal deleted regions on the long arm of chromosome 6 [14,15]. BLIMP-1 is a
transcription factor acting mainly as a repressor, which plays a crucial role in
orchestrating the differentiation of B cells into plasma cells [16]. TNFAIP3 is an
ubiquitin-modifying enzyme that acts as a negative regulator of TNF and toll-like
receptor (TLR) mediated responses. Inactivating mutations were observed in
TNFAIP3 and TNF receptor-associated factor 3 (TRAF3) resulting in activation of
the nuclear factor kappa B (NF-kB) signaling pathways. Moreover, a minimal
deleted region, including MIRN15A and MIRN16-1, was demonstrated on 13q14
in about 10-13% of patients [13,17].
Whole genome sequencing
Treon et al has recently reported the presence of MYD88 L265P somatic
mutation (in chromosome 3p22.2) in over 90% of WM patients via whole genome
sequencing [18]. High frequency of this mutation in WM patients (70-100%) was
also confirmed by other studies via Sanger sequencing, polymerase chain
reaction (PCR) or allele specific polymerase chain reaction (AS-PCR) [19-23].
MYD88 L265P was also detected in non-IgM LPL patients, suggesting that this
mutation can be seen in LPL patients independent of isotype [18,24,25]. Recent
studies also showed that this mutation might be seen in up to 80% of patients
with IgM monoclonal gammopathy of undetermined significance (MGUS) [18-
20,22,26]. In order to assess the impact of this mutation on the risk of
4

progression from IgM-MGUS to WM, Varettoni et al performed a case-control
approach in IgM-MGUS patients and found that the MYD88 L265P mutation was
associated with a significantly higher risk of progression to WM or to other
lymphoproliferative disorders [20]. Together, these findings suggest a key role of
MYD88 L265P somatic mutation for the development of WM. This
nonsynonymous mutation causes a leucine (L) to proline (P) substitution in
codon 265 (L265P) of MYD88, which is thought to be a crucial player in the
activation of the canonical NF-κB pathway, downstream of TLR and interleukin-1
receptor (IL-1R) signaling [18,27-29]. When combined with immunoglobulin
heavy chain variable gene (IGHV) mutation status, MYD88 L265P mutation
appears to be a unique genetic signature as a diagnostic tool that distinguishes
WM from other similar B cell malignancies [21]. The second most common
somatic gene mutation in WM are C-terminal mutations, which are similar to
those found in the germline of patients with WHIM syndrome [30]. Up to 30% of
WM patients harbor CXCR4 mutations which enhances tumor dissemination and
survival of WM cells [31,32].
Epigenetics
Epigenetic regulation of tumor suppressors and oncogenes play an important
role in the development of many tumor types [33,34]. The main epigenetic
changes include DNA methylation and histone modification [35]. Other regulators
include non-coding RNAs such as miRNAs.
Upregulation of miRs including 155, 184, 206, 363, 494 and 542-3p, and
downregulation of miR-9 are identified in WM cells. Among these, miRNA-155
was found to be a critical regulator of tumor growth and proliferation of WM cells
both in vitro and in vivo [36]. Increased expression of miRNA-206 and reduced
expression of miRNA-9 increased histone acetylation leading to enhanced gene
transcription [37]. In addition, MIRN15A and MIRN16-1 are believed to act as
tumor suppressors by preventing the transcription of mRNAs encoding for
proteins involved in proliferation, cell cycle and anti-apoptosis, such as BCL-2
[38].
5
Gene Expression Profiling (GEP)
A study of GEP in Waldenström macroglobulinemia demonstrated that WM has a
homogenous expression profile similar to that of patients with chronic
lymphocytic leukemia (CLL) [39]. Another study showed that the genes including
ATXN1, FMOD, LEF1 (WNT/b-catenin pathway), MARCKS discriminated WM
cells from CLL cells [14]. Furthermore, a recent study performed GEP on WM BM
CD19 + versus IgM MGUS BM CD19 + cells showed that 151 genes were
differently expressed. PI3K/Akt/mTOR, JAK/STAT and MAPK signaling pathways
were found to be the most important signaling pathways in these two disorders
[40].
Proteomic analysis
Hatjiharissi et al employed protein expression profiling of untreated WM and
normal bone marrow controls using antibody-based protein microarrays to
demonstrate proteins that are dysregulated in WM. The study showed that Ras
family proteins such as Rab-4 and p62DOK, as well as Rho family proteins such
as CDC42GAP and ROK α were up-regulated by >2-fold in WM. Other proteins
including cyclin-dependent kinases, apoptosis regulators, and histone
deacetylases were up-regulated by >1.3-fold [41].
Deregulated molecular pathways
MYD88/IRAK
Recent findings of the existence of a mutation in MYD88 in most of WM patients
have indicated that MYD88/IRAK signaling pathway might have a crucial role in
pathogenesis of WM. In this pathway, upon TLR or IL-1R stimulation, interleukin-
1 receptor-associated kinase 4 (IRAK4) recruited to the receptor by the adaptor
MyD88, which then activates IRAK1 that ultimately resulting in activation of NF-
κB [42]. However, the signaling cascade(s) by which MYD88 L265P induce NF-
κB activation in WM remains unclear. Studies showed that targeting
MYD88/IRAK signaling attenuated NF-κB signaling and survival of MYD88
6

L265P–expressing WM cells [18,23]. Moreover, Yang et al demonstrated
increased phosphorylated Bruton tyrosine kinase (BTK) in WM cells transduced
to overexpress L265P compared to wild-type MYD88 [43]. Taken together, these
findings would suggest that MYD88 L265P triggers NF-κB via dual, which signal
through BTK and/or IRAK1/IRAK4 [44]. Therefore, combined suppression of both
BTK and IRAK signaling may provide synergistic inhibition of NF-κB signaling.
PI3K/Akt/mTOR
PI3K/AKT signaling inhibits apoptosis and regulates cell growth, survival, and
proliferation [45]. Although there is no evidence that there are activating
mutations in the PI3K/Akt/mTOR pathway in WM, it has been shown that this
pathway is activated in WM [46,47]. Recently, Yang et al showed that MYD88
L265P can activate PI3K delta [48]. External stimulation through the bone
marrow microenvironment with cytokines such as insulin-like growth factor (IGF-
1) or stromal- derived factor (SDF-1) may also contribute to activation of this
pathway [46]. Gene and protein expression of PTEN, a negative regulator of
PI3K/Akt pathways, were found to be decreased which lead to consistent
activation of the PI3K/Akt pathway in WM [47]. Additionally, inhibition of Akt by
perifosine, mTOR by RAD001, or dual PI3K/ mTOR inhibitor (NVP-BEZ235)
display activity against WM even in the presence of bone marrow stromal cells
[46,49].
JAK/STAT
It was shown that expression of both Jak1 and Stat3 proteins is significantly
higher in the WM patients as compared to healthy controls [41]. Although no
mutations associated with this constitutive Jak/Stat signaling have been
described in WM to date, cytokine-mediated stimulation of this pathway may be
involved in the dysregulation of IgM [50]. One important cytokine believed to play
pivotal role is IL-6. It is widely accepted that IL-6 activates MAPK/ERK pathway
and the transcription factor Stat3 via the tyrosine kinase receptor signaling of
JAK1 and 2 [51].
7
The nuclear factor kappa B pathway
NF-kB comprises a family of transcription factors that serve as important
regulators of the transcription of many genes involved in inflammation, innate
immunity, cell growth, and apoptosis [52]. Inhibition of this pathway by
proteasome inhibitors such as bortezomib, NPI-0052 and Onyx0912 can inhibit
WM cells and overcome resistance induced by bone marrow stromal cells
[53,54]. Studies using bortezomib alone or in combination with rituximab in newly
diagnosed or even in relapsed WM patients have shown significant activity with
over 80% response rate [55-57].
Risk factors for developing WM
The underlying causes of WM are poorly understood. The main risk factor for the
development of WM is pre-existing IgM-MGUS. Other risk factors include familial
history of WM or other B-cell malignancies and immunological factors.
IgM-MGUS. IgM-MGUS patients are up to 46 times more likely to develop WM
than the general population [58]. IgM-MGUS progresses mostly to WM; Kyle et
al demonstrated the cumulative incidence of progression was 10% at 5 years,
18% at 10 years, and 24% at 15 years, respectively [58]. Abnormal serum free
light chain (FLC) ratio, the serum monoclonal protein and serum albumin
concentrations were shown to be risk factors for progression [58,59]. In addition,
recent work by Varettoni et al has shown that MYD88 L265P mutation is also an
independent predictor of progression [60]. IgM-MGUS patients are also at
increased risk of developing lymphoproliferative disorder, lymphoma, primary
amyloidosis and chronic lymphocytic leukemia [61]. We have previously
demonstrated that increased serum FLC (with a cut off of 60 mg/L) is a new
marker in WM disease and reflective of tumor burden. Therefore, it can be used
to differentiate IgM-MGUS from symptomatic WM [62]. Similarly, 6q deletion is
not seen in IgM- MGUS patients, whereas it is observed in about 30%-50% of
WM patients [63].
8
Familial WM. Although WM represents a sporadic disease in most cases; various
reports reported strong familial predisposition. A study with clinicopathological
analysis from 257 unrelated WM patients showed that 48 (18.7%) patients had at
least one first-degree relative with WM or another B-cell disorder, including non-
Hodgkin lymphoma (NHL), Hodgkin lymphoma, MGUS, MM, chronic lymphocytic
leukemia (CLL) and acute lymphoblastic leukemia [64]. A large study with 2144
LPL/WM patients has demonstrated first-degree relatives of LPL/WM patients to
have 20-fold, 3.0-fold, 3.4-fold, and 5.0-fold increased risks of developing
LPL/WM, NHL, CLL, and MGUS, respectively [65]. The excess risks among
parents, siblings, and offspring were similar.
Immunological Risk Factors. It has been shown that history of certain
autoimmune and infectious diseases was associated with an increased risk of
LPL/WM [65].
Diagnosis
WM is primarily characterized by bone marrow infiltration of lymphoplasmacytic
cells which produce excessive amounts of a serum monoclonal IgM [1,2]. Of
note, an IgM paraprotein of any level is not sufficient for the diagnosis of WM,
since there are other lymphoproliferative disorders that produce IgM [66]. In
clinical practice, characteristic immunophenotype of high levels of surface CD19,
CD20, and Ig light chain expression in association with nonparatrabecular pattern
of BM infiltration is diagnostic for WM [1,4,5,67]. The intratrabecular pattern of
BM infiltration is mostly found in WM, whereas an exclusively paratrabecular
pattern is rare and should raise suspicion of follicular lymphoma. Dutcher bodies-
containing plasma cells and increased number of mast cells close to lymphoid
aggregates are commonly found in WM.
Immunophenotypic studies showed the following profile for WM cells: positive for
surface IgM, CD19, CD20, CD22, CD25, CD27, FMC7; negative for CD103, and
variable CD5, 10, 23, CD138 expression [29,68].
Clinical features
9

The majority of WM patients present with signs and symptoms related to
elevated IgM levels and/or to infiltration of bone marrow and extramedullary sites
by malignant B cells. Cytopenia, which is associated with tumor cells
replacement in the BM, is the frequent clinical presentation of the disease.
Hyperviscosity resulting from high levels of proteins can lead to impairment of
microcirculation in the central nervous system. This may result in headache,
blurry vision, visual loss and epistaxis in WM patients. Some patients may
experience hepatosplenomegaly and lymphadenopathy, and some patients may
present with B symptoms including night sweats, fever, and weight loss.
Moreover, some patients with WM may present with other common
manifestations including neuropathy, cryoglobulinemia, skin rash (Schnitzler
syndrome), cold-agglutinin hemolytic anemia, and amyloidosis [69].
Progression in WM: IgM-MGUS, asymptomatic WM, and symptomatic WM
Normally, WM is preceded by IgM-MGUS or smoldering WM [70]. IgM-MGUS is
described as an IgM<3 g/dL and <10% lymphoplasmacytic cells in the BM,
whereas smoldering WM is described as an IgM>3 g/dL or >10% LPL cells in the
BM in the absence of any symptoms attributable to WM. A recent study showed
that the cumulative probability of progression of smoldering WM to symptomatic
WM, amyloidosis, or lymphoma is 6% at 1 year, 39% at 3 years, and 59% at 5
years, respectively [71]. The percentage of lymphoplasmacytic cells in the bone
marrow, size of the serum M-spike, and the hemoglobin value were the major risk
factors for the progression. Although abnormal serum FLC ratio was shown as a
risk factor for progression in MGUS, it was not a predictive factor of progression
in patients with smoldering WM [71]. Since the criteria used for IgM-MGUS and
smoldering WM are not widely adopted in the WM literature, another
classification based on the consensus recommendation is more frequently used,
According to this classification, patients present with Ig protein but no LPL cells in
the BM should be diagnosed with Ig-MGUS, and patients with any level of IgM
monoclonal protein and presence of lymphoplasmacytic cells in the BM should
10

be diagnosed with WM (asymptomatic or symptomatic) [4]. Patients diagnosed
with asymptomatic WM should be recognized and not treated because of the
stability of the disease for many years. In an analysis of 31 asymptomatic
patients, the median time to disease progression was 6.9 years [5].
Prognosis
In a study of 337 symptomatic WM patients, the median survival of patients was
6.4 years, and the median disease-specific survival was11.2 years [72]. Despite
indolent nature of the disease, WM prognosis shows wide variation, which makes
important to define prognostic factors. Cytopenias, high β2-microglobulin, low
albumin, serum IgM monoclonal protein, organomegaly and advanced age have
shown to be poor prognostic factors for WM patients [72-76]. International
Prognostic Scoring System (ISS-WM) is the most commonly used prognostic
system, which is based on 5 risk factors and the survival of patients at 5 years
[77]. Based on this system, high-risk WM patients were shown to have a 5-year
survival of 36%, whereas low-risk patients had a 5-year survival of 87%.
Diagnostic workup and differential diagnosis
Important points of workup for a patient with WM are summarized in Table 1.
Diseases that need to be considered for differential diagnosis are IgM-MM,
mantle cell lymphoma, marginal zone lymphoma (MZL), and other IgM-secreting
lymphomas.
Plasmacytic cell infiltration of BM and the presence of osteolytic lesions
differentiate IgM-MM from WM [1,5,69]. Renal insufficiency can be seen in IgM-
MM, whereas it is rare in WM. Some cytogenetic characteristics such as 13q
deletion, 11:14, or 4:14 translocations may also help to differentiate MM from
WM. In addition, MYD88 L265P mutation presents in over 90% of WM patients
but not MM patients [18-20]. This may also help to differentiate WM from not only
from MM but also from other B cell malignancies.
11
Infiltration of BM by monomorphous, small medium lymphoid cells with irregular
nuclei may help to differentiate mantle cell lymphoma from WM. In addition to
the BM, involvement of extranodal sites and lymph nodes may be observed in
mantle cell lymphoma. Moreover, almost all cases present with t(11;14) (q13;q32)
[1,5,69].
Distinguishing WM from MZL can be difficult, particularly from splenic MZL
(SMZL). SMZL mostly involves the spleen and only rarely presents with
lymphadenopathy. It virtually always infiltrates the bone marrow with a
characteristic intertrabecular and intrasinusoidal pattern, which is not typical of
NMZL [78]. In immunophenotyping, some markers such as CD22 and CD11c are
overexpressed in patients with SMZL compared to patients with WM, whereas
CD25 is mostly seen in WM (88% vs 44%). Therefore, combination of CD25 and
CD22 may help to differentiate between WM and SMZL [69]. The CD103 Ag is
absent in WM patients, whereas it is present in 40% of SMZL patients. The most
common cytogenetic abnormality in WM patients is 6q deletion (30%-50% in
WM), whereas the most common abnormalities in SMZL are loss of 7q (19%)
along with +3q (19%) and +5q (10%). The use of MYD88 L265P may be
particularly helpful, as few if any patients with MZL demonstrate this mutation
whereas >90% of WM patients express this mutation [18].
Follicular lymphoma can be differentiated from WM with BM infiltration of small,
cleaved cells that are usually paratrabecular. In addition, rearrangement of Bcl-2
is the molecular hallmark in follicular lymphoma and seen in 70%-90% of the
cases [1,5,69].
Lastly, IgM myeloma may also share similar morphological features with WM,
including expression of CD20. Translocation involving chromosome 11 (t 11;14)
are common in IgM myeloma, but absent in WM [79].
Primary treatment options for WM
Despite the advances in the biology and treatment of WM, there is no standard of
care for the treatment of WM. Treatment decisions are based on the presence of
12

symptoms, patient factors including age and functional status and disease factors
including presence of cytopenias, rate of disease progression, the level of IgM
protein, the presence of neuropathy, cryoglobulinemia, and hyperviscosity.
Current treatment options for WM include alkylating agents (e.g. chlorambucil,
and cyclophosphamide), nucleoseide analogue (fludarabine and cladribine), the
monoclonal antibody rituximab, and the proteasome inhibitor bortezomib [80-83].
Consensus-based response criteria for WM are found in table 2 [84].
Plasma exchange is a treatment technique used for hyperviscosity associated
with WM. Symptoms of hyperviscosity are generally present when IgM exceeds
4000mg/dL and includes epistaxis, gingival bleeding and visual changes due to
retinal hemorrhages. Plasma exchange is a temporary solution that is used for
short-term management of hyperviscosity until initiating systemic chemotherapy,
which treats the underlying cause of the hyperviscosity by reducing the IgM
[85,86].
Rituximab
One of the most widely available agents used for the treatment of WM is
rituximab, which is used either as a single agent or in combination regimes. It is a
chimeric monoclonal antibody that binds to the CD20 antigen on B-cell
lymphocytes. As a single agent it gives response rates of 35-48% [87-90], which
is inferior than response rates seen with combination regimens. In addition,
single agent rituximab can cause a “rituximab flare” phenomenon, which results
in a transient rise in IgM level producing symptoms of hyperviscosity and
requiring plasma exchange. This phenomenon is infrequently seen when
rituximab is used in combination with chemotherapy. Some of the combination
agents studied with rituximab include cyclophosphamide, bendamustine, and
bortezomib [55-57,91,92].
In a study by Dimopoulos et al, 72 patients with newly diagnosed WM received
rituximab, oral cyclophosphamide and dexamethasone. Overall response rate
(ORR), which includes minimal response or better, was 83%, including 7%
13

complete response (CR), 67% partial remission (PR). The median time to
progression was 35 months with a median overall survival (OS) of 95 months.
Only 9% of patients experienced grade 3 or 4 neutropenia and none experienced
grade 3 or 4 thrombocytopenia [91,93].
A phase III trial conducted by the Study group Indolent Lymphomas (StiL)
included 549 patients with low grade lymphomas of which 162 were newly
diagnosed WM patients who were received 6 cycles of bendamustine and
rituximab (BR). Responding patients were randomized to rituximab every 2
months for 2 years or observation. In the 116 evaluable patients, ORR was 86%.
The results of the maintenance arm of this study remain to be reported. No
uncommon toxicities were observed during BR induction [94].
Maintenance therapy with rituximab is being used more commonly in patients
with WM. A retrospective study showed improvement in progression free and
overall survival among patients receiving maintenance rituximab when used at
375mg/m2 every 3 or 6 months over 2 years. A prospective study on
maintenance regimen of rituximab given every 2 months for 2 years is now being
studied [95].
Nucleoside analogues
Nucleoside analogs are conventional chemotherapeutic agents that inhibit DNA
synthesis through interfering with different steps in the process of DNA synthesis.
Fludarabine and cladribine are nucleoside analogues studied as single agent or
in combination with rituximab or cyclophosphamide.
A recent phase III study by Leblond et al showed the superiority of fludarabine
compared with chlorambucil in the treatment of WM. Three hundred and thirty
nine WM patients were included in this trial and the study showed no difference
in overall response rate between the two arms. However, the median PFS and
duration of response were significantly higher in the fludarabine arm then
chlorambucil with a median follow up of 36 months (PFS 36.3 vs 27.1 months
14
p=0.012). Median overall survival was not reached in the fludarabine arm versus
69.8 months in the chlorambucil arm (p=0.014). Secondary malignancies were
more frequent in the chlorambucil arm with a 6-year cumulative incidence rate of
20.6% versus 3.7% in the fludarabine arm (p=0.001) [96]. This rate is
inconsistent with prior retrospective studies, which have shown higher rates of
secondary malignancies with fludarabine [97].
Adding rituximab to fludarabine can significantly enhance response without
added toxicity [98]. Combinations of fludarabine and rituximab or fludarabine,
cyclophosphamide and rituximab have shown response rates of 70-85%
[99,100].
New developments in WM
Many novel agents have promising results and are at various stages of study in
WM. These include everolimus, an mTOR inhibitor; perifosine, an AKT inhibitor;
enzastaurin, a PI3K/AKT inhibitor; panobinostat, a histone deacetylase inhibitor;
bortezomib, first in class of protasome inhibitor and carfilzomib, a new
irreversible proteasome inhibitor; pomalidomide, a new immunomodulatory
agent; and ibrutinib, a Bruton tyrosine kinase inhibitor [101,102].
Proteasome Inhibitors
Bortezomib is a reversible proteasome inhibitor that specifically acts on the 20S
of the proteasome. Blocking proteasomal degradation causes protein
accumulation, which can alter the normal progression of the cell cycle, which is
necessary for cell survival. Bortezomib in combination with rituximab with or
without dexamethasone is being commonly used in either newly diagnosed or
relapsed WM. The overall response rates with these combinations are more than
80%. Peripheral neuropathy is one of the adverse effects of bortezomib therapy,
which is less when bortezomib is given weekly instead of the twice-weekly
regimen [55-57].
15
Carfilzomib, an irreversible proteasome inhibitor, was approved by the FDA in
July of 2012 for the treatment of patients for relapsed/refractory myeloma and is
also being studied in WM. Antitumor activity of carfilzomib was validated in vivo
by Sacco et al who demonstrated that carfilzomib targeted the chymotrypsin-like
(CT-L) activity of both constitutive-(c20S) and immuno-(i20S) proteasome. This
led to the induction of toxicity in primary WM cells, as well as in other IgM-
secreting lymphoma cells [103].
The results recently reported from the CaRD trial by Treon et al in 31 patients.
Eighty seven percent of patients were previously untreated. Symptomatic
patients received carfilzomib in combination with rituximab and dexamethasone,
and were eligible for maintenance therapy with all three agents if they had stable
disease or better. The overall response rates and major response rates were
81% and 65% with 9 very good partial responses, 11 partial responses, and 4
minor responses. With a median follow-up of 9 months, 20 patients are free of
disease progression. Most common toxicities which were hyperglycemia related
to steroids; asymptomatic elevation of lipase and hypersensitivity to rituximab. All
toxicities were reversible, and no grade ≥2 peripheral neuropathy was observed
[104].
Oprozomib, an oral proteasome inhibitor, is in clinical development for MM and
other hematologic malignancies. A phase 1b/2 trial of once-daily, modified-
release oprozomib tablets was studied in 24 patients with hematologic
malignances. Dose escalation of oprozomib is currently being implemented using
two dosing schedules: oprozomib was given at 2 different dosing schedules;
once-daily, modified-release tablets (150 mg/d), on either days 1, 2, 8, and 9
(QDx2) or on days 1 to 5 (QDx5), both on a 14-day cycle. From the data that Dr.
Kaufman presented at the EHA meeting 2013, 24 patients were enrolled in the
study (16 with MM; 8 with WM) in 7 cohorts. WM patients on the QDx2 schedule
have shown no response while patients on the QDx5 schedule have shown 80%
ORR. The MTD of oprozomib had not been reached for either schedule. Most of
16

the adverse effects seen were gastrointestinal. Dose escalation will continue in
this study until the MTD of oprozomib is reached. This data
Everolimus
Everolimus (RAD001) is an inhibitor of MTORC1, a component of the Akt-MTOR
pathway, which regulates growth, and survival of lymphoplasmacytic cells in WM.
A phase II trial of single agent everolimus was studied in 50 patients with
relapsed/ refractory WM. The overall response rate was 70% with a PR of 40%
and MR of 30%. The most common adverse events were cytopenias. Pulmonary
toxicity, which is a serious adverse effect of everolimus, was seen in 10% of
patients [105]. Another phase I/II study explored the use of everolimus in
combination with rituximab and/or bortezomib in 23 relapsed/refractory patients.
From the 19 patients who were evaluable for response, 1 (5%) patient very good
partial response (VGPR) and 9 (47%) minimal response (MR), for an overall
response rate including MR of 10/19 (53%) in this relapsed/refractory population
[106]. A prospective, multicenter study of everolimus as primary therapy was
conducted in 33 WM patients. The best overall response rate utilizing consensus
criteria was 72.2% (2 Very Good Partial Responses, 18 Partial Responses, 4
Minor Responses, and 9 Stable Disease), and the major response rate (PR or
better) was 60.6%. However, discordance between serum IgM levels upon which
consensus criteria for response are based, and BM disease response were
common and complicated response assessment. At 6-month assessments, 10 of
22 (45.5%) patients for whom both serum IgM and BM assessments were
performed, discordance between serum IgM and BM disease involvement were
observed. Among these patients, 2 had no change, and 8 had increased bone
marrow disease involvement despite decreases in serum IgM levels. Grade ≥2
hematologic and non-hematologic toxicities possibly, probably or definitively
associated with everolimus included anemia (39.4%), thrombocytopenia (12%),
neutropenia (18.2%), hyperglycemia (9.1%), oral ulcerations (27.3%), and
pneumonitis (15%) with a median follow-up of 9 months (range 1-45 months), 6
patients remain on study [107].
17
Enzastaurin
Enzastaurin is an oral serine/threonine kinase inhibitor that targets the PKC and
PI3/AKT pathway. A phase II trial of enzastaurin was studied in 42 patients with
WM who were previously treated with 1 to 5 regimens. Oral enzastaurin was
given at 250 mg twice daily (500 mg total) after a single loading dose (day 1,
cycle 1) of 375 mg 3 times daily (1,125 mg total) for 8 cycles of 28 days each or
until progressive disease. The objective response rate was 38.1%, with 2
patients achieving PR and 14 achieving minor response. Grade 3 adverse events
seen were leukopenia in one patient and septic shock in another one [107].
These results warrant further investigation of enzastaurin for the treatment of
WM.
Perifosine
Perifosine is an Akt inhibitor that belongs to a class of lipid-related compounds
called alkylphospholipids. A phase II trial was conducted with perifosine and
included 37 patients with WM who were previously treated with 1 to 5 regimens.
Oral perifosine was given at 150 mg daily until progression. The objective
response rate (MR or better) was 35% with 11% achieving PR and 24%
achieving MR. Progressive disease was observed in only 11% of patients since
54% had stable disease. Median PFS was 12.6 months. The most common
adverse events were GI toxicities including diarrhea, nausea and vomiting [108].
Immunomodulatory Drugs
Thalidomide and lenalidomide are immunomodulatory agents that are studied in
combination with Rituximab in symptomatic WM patient [109,110]. A phase 2
study included 25 patients, 20 of whom were previously untreated. They received
thalidomide (200 mg for 2 weeks, then 400 mg for a total of 1 year) and
Rituximab. Overall and major response rate were 72% and 64%, respectively,
with complete response (n = 1), partial response (n = 15), and major response (n
= 2). Median time to progression for all evaluable patients was 34.8 months.
Peripheral neuropathy was the most common adverse event (grade ≥2 in 44%),
18

and therefore limits the use of thalidomide in WM [109]. Lenalidomide was also
poorly tolerated in WM patients. It was tested in combination with rituximab in 16
patients, 12 of whom were previously untreated. The overall response and major
response (<50% decrease in serum IgM) rates were 50% and 25%, respectively,
with a median time to progression of 18.9 months. Premature discontinuation of
lenalidomide therapy occurred in 14 of 16 (88%) patients, which was most
commonly due to an acute decrease in hematocrit in 13 of 16 patients, which
resulted in 4 patients requiring hospitalizations due to anemia complications. This
was attributable to lenalidomide and led to cessation of further enrollment on this
study [110].
Pomalidomide, a 3rd generation immunomodulatory agent, has demonstrated
efficacy, as a single agent and with dexamethasone for the treatment of
relapsed/refractory multiple myeloma and as a single agent for myelofibrosis. A
phase I trial was conducted on 6 patients with relapsed and/or refractory WM.
Patients received daily oral pomalidomide (28 day cycles), starting with a dose of
1 mg. The median number of prior lines of therapy was 1-4. No dose limiting
toxicities (DLTs) were encountered at the 1mg dose. At the 2 mg dose level, 2
patients experienced DLTs (grade 4 dizziness and grade 3 syncope in 1 and
grade 4 neutropenia in the second); a 3rd withdrew from the study after
experiencing mild fever, headaches and blurred vision, which resolved after
plasma exchange and discontinuing pomalidomide. Other grade 3-4 adverse
events have been neutropenia and infection. The best response to date for the 5
evaluable patients was stable disease in 3 patients, and progressive disease in 2
[111]. A study looking into the combination of pomalidomide, dexamethasone and
rituximab was reported recently. Patients were enrolled on a dose escalating
Phase 1 study (3+3 design). Following amendment, dose level one was rolled
back to 0.5 mg daily, with intended escalation to 1, 2, 4 mg daily. Therapy
consisted of 52 weeks of daily POM with rituximab (375 mg/m2/wk) IV and
dexamethasone (40 mg) IV on weeks 1-4 and 12-15. Patients were required to
be on aspirin (325 mg) prophylaxis. Patients with IgM >4,000 mg/dL had
prophylactic pheresis to avoid symptomatic rituximab- related IgM flare. 7
19

patients were enrolled (3 at 0.5 mg, 4 at 1.0 mg of POM) before closure for
rituximab-related IgM flare events. The best overall response rate is 42.8% (1
VGPR; 2 PR). Grade ≥2 treatment related toxicities include neutropenia (43%),
symptomatic hyperviscosity from IgM flare with 3 patients (43%) all of whom had
a baseline IgM >4,000 requiring emergent pheresis for IgM flaring while on
therapy. Median response duration was 15.1 months, and all 3 patients continue
to respond [112].
Histone-Deacetylase Inhibitors (HDACi)
Preclinical studies have shown that epigenetic regulators, including histone
acetylation, regulate tumor progression. In vitro studies have confirmed the
antitumor activity of panobinostat (HDACi) in primary tumor cells and cell lines
[113] A phase II trial of panobinostat was studied in 36 patients with relapsed or
relapsed/refractory WM. Patients received oral panobinostat at 30 mg 3 times a
week. Overall response rate (MR or better) was achieved in 17 (47%) of patients,
with 22% partial remissions and 25% MR. In addition, 18 (50%) patients
achieved stable disease and none showed progression while on therapy. The
median progression-free survival was 6.6 months. Grade 3 and 4 toxicities
included thrombocytopenia, neutropenia, anemia, leukopenia, and fatigue [114].
Further studies are under way to better define the efficacy of HDAC inhibitors in
WM.
Bruton Tyrosine Kinase (BtK) inhibitor
Bruton’s tyrosine kinase (BtK) is an essential element of the BCR signaling
pathway, which regulates apoptosis, adhesion, and cell migration and homing.
BTK activation is facilitated by MYD88 pathway signaling in L265P expressing
WM cells, and participates in MYD88 downstream signaling. Ibrutinib (previously
PCI-32765) is an oral agent designed to specifically target and selectively inhibit
the enzyme Bruton's tyrosine kinase (BTK) leading to tumor cell killing of MYD88
L265P expressing WM cells [115].
20
A phase I study of ibrutinib was conducted in 56 patients with a variety of B-cell
malignancies including chronic lymphocytic leukemia/small lymphocytic
lymphoma, mantle cell lymphoma, diffuse large B-cell lymphoma, follicular
lymphoma, Waldenstrom's macroglobulinemia and multiple myeloma. Objective
response rate in 50 evaluable patients was 60%, including complete response of
16%. Median progression-free survival in all patients was 13.6 months. Partial
responses were seen in 3 of the 4 patients with WM and the drug was well
tolerated [116].
63 patients including 17 with refractory disease were enrolled on a dedicated
ongoing phase II trial (ClinicalTrials.gov Identifier: NCT01614821) in patients with
relapsed/refractory WM disease. Patients had a median of 2 prior therapies,
hemoglobin of 10.5 g/dL, serum IgM of 3,610 mg/dL, and a median BM disease
involvement of 65%. At best response, median serum IgM level declined to
1,340 mg/dL, and median hemoglobin rose to 12.6 g/dL. With a median follow-up
of 6 (range 2-15 cycles), the best overall response rate i.e. minor response (MR)
or better using consensus criteria adapted from the 3rd International Workshop
on WM is 81% (4 VGPR; 32 PR, 15 MR), with a major response rate (PR or
better) of 57.1% and a median time to response of 4 weeks. 11 patients have
stable disease, and 1 patient was a non-responder. The most common grade >2
treatment related toxicities were thrombocytopenia (14.3%); neutropenia
(19.1%); stomatitis (1.6%); atrial fibrillation (1.6%); diarrhea (1.6%); herpes
zoster (1.6%); hematoma (1.6%); and epistaxis (1.6%). Attainment of major
responses was impacted by mutations in CXCR4. The major response rate was
77% for patients with wild-type CXCR4 vs. 30% in those with WHIM-like CXCR4
mutations.
Conclusion
Waldenstrom macroglobulinemia is a distinct lymphoproliferative disorder with
specific epigenetic/genetic aberrations, and characterized by production IgM
monoclonal secretion and lymphoplasmacytic cells in the BM. With the change in
understanding the pathogenesis of WM, many new targets and therapies have
21
emerged within the past couple of years. Current therapies used in the upfront or
relapsed setting include alkylating agents, bendamustine, nucleoside analogues,
bortezomib and the monoclonal antibody rituximab. Newer options include
everolimus and ibrutinib. However, targeted therapies are still warranted and
recent revelations from whole genome sequencing have provided opportunities
for their development.
Expert commentary & five-year view
To date there are no FDA approved therapeutic agents for treatment of WM.
Recently, whole genome sequencing helped us identify specific mutations in
subgroups of patients with WM (eg. MYD88 L265P mutation which is present in
over 90% of WM) which provides the framework for the investigation of BTK
inhibitors like ibrutinib. These newer agents show improved responses and lower
long term toxicities. In addition, many of the newer agents are orally administered
which makes them more convenient for patients. Some of the challenges for the
future of WM include combining of agents to achieve higher response rates, and
prolonged survival for patients, but with less toxicity.
Key Issues
Recent findings demonstrated that MYD88/IRAK signaling pathway might
have a critical role in pathogenesis of WM.
Somatic mutations in MYD88 are found in over 90% of WM patients,
which may help to differentiate WM from other B cell malignancies.
22

Current research efforts in inhibtion of BTK and IRAK signaling might
provide better treatment strategy for WM.
Many treatment options are available for WM patients and some of these
include rituximab, bortezomib, cyclophosphamide, and nucleoside
analogues fludarabine and cladribine which are less commonly used.
Novel agents under study are showing promising results as a single agent
or in combination. Some of these include everolimus, ibrutinib, as well as
the newer proteasome inhibitors carfilzomib and oprozomib.
There is a need for studies with PFS and OS as endpoints combined with
quality of life assessment as well as randomized phase III studies to
evaluate the benefit of different treatments for patients with WM.
23

Table : Workup for WM
Table 2: Response Definitions
Response Category Definition
Complete response (CR) Absence of serum monoclonal IgM protein by
immunofixation
Normal serum IgM level
Complete resolution of extramedullary disease*
Morphologically normal bone marrow aspirate
Very good partial response (VGPR) Monoclonal IgM protein is detectable
≥90% reduction in serum IgM level from baseline
24
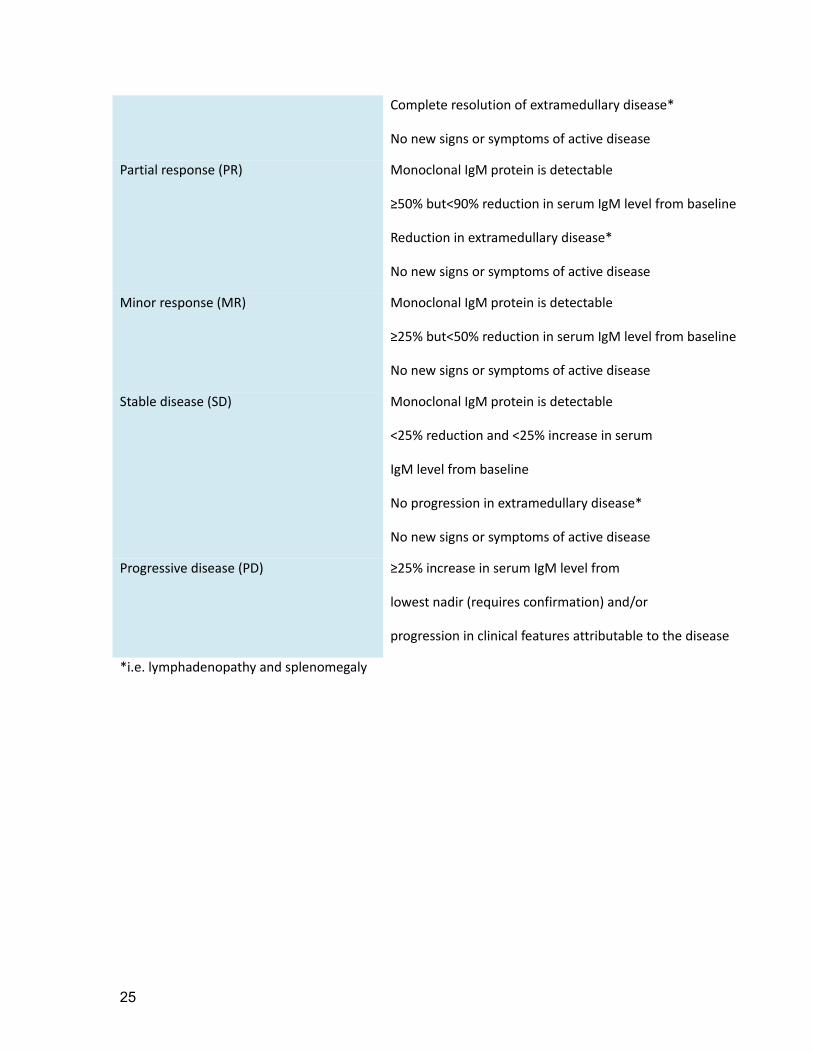
Complete resolution of extramedullary disease*
No new signs or symptoms of active disease
Partial response (PR) Monoclonal IgM protein is detectable
≥50% but<90% reduction in serum IgM level from baseline
Reduction in extramedullary disease*
No new signs or symptoms of active disease
Minor response (MR) Monoclonal IgM protein is detectable
≥25% but<50% reduction in serum IgM level from baseline
No new signs or symptoms of active disease
Stable disease (SD) Monoclonal IgM protein is detectable
<25% reduction and <25% increase in serum
IgM level from baseline
No progression in extramedullary disease*
No new signs or symptoms of active disease
Progressive disease (PD) ≥25% increase in serum IgM level from
lowest nadir (requires confirmation) and/or
progression in clinical features attributable to the disease
*i.e. lymphadenopathy and splenomegaly
25

Financial and competing interests disclosure
IM Ghobrial is on the advisory board for Onyx, BMS and Celgene and receives research lab support from Genzyme and BMS. SP Treon receives research support from honoraria, and consulting fees from pharmacyclics, janssen pharmacuticals, and onyx pharmaceuticals. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed. No writing assistance was utilized in the production of this manuscript.
26
References
Papers of special note have been highlighted as:
• of interest
•• of considerable interest
1. Dimopoulos MA, Panayiotidis P, Moulopoulos LA, Sfikakis P, Dalakas M. Waldenstrom's macroglobulinemia: clinical features, complications, and management. Journal of clinical oncology : official journal of the American Society of Clinical Oncology 18(1), 214-226 (2000).
2. Ghobrial IM, Gertz MA, Fonseca R. Waldenstrom macroglobulinaemia. The lancet oncology 4(11), 679-685 (2003).
3. Kyle RA, Anderson KC. A tribute to Jan Gosta Waldenstrom. Blood 89(12), 4245-4247 (1997).
4. Owen RG, Treon SP, Al-Katib A et al. Clinicopathological definition of Waldenstrom's macroglobulinemia: consensus panel recommendations from the Second International Workshop on Waldenstrom's Macroglobulinemia. Seminars in oncology 30(2), 110-115 (2003).
5. Dimopoulos MA, Kyle RA, Anagnostopoulos A, Treon SP. Diagnosis and management of Waldenstrom's macroglobulinemia. Journal of clinical oncology : official journal of the American Society of Clinical Oncology 23(7), 1564-1577 (2005).
6. Herrinton LJ, Weiss NS. Incidence of Waldenstrom's macroglobulinemia. Blood 82(10), 3148-3150 (1993).
7. Jemal A, Murray T, Ward E et al. Cancer statistics, 2005. CA: a cancer journal for clinicians 55(1), 10-30 (2005).
8. Cancer Facts and Figures 2012. Cancer Facts and Figures 2012 (2012).9. Sahota SS, Forconi F, Ottensmeier CH et al. Typical Waldenstrom macroglobulinemia
is derived from a B-cell arrested after cessation of somatic mutation but prior to isotype switch events. Blood 100(4), 1505-1507 (2002).
10. Schop RF, Kuehl WM, Van Wier SA et al. Waldenstrom macroglobulinemia neoplastic cells lack immunoglobulin heavy chain locus translocations but have frequent 6q deletions. Blood 100(8), 2996-3001 (2002).
11. Braggio E, Keats JJ, Leleu X et al. High-resolution genomic analysis in Waldenstrom's macroglobulinemia identifies disease-specific and common abnormalities with marginal zone lymphomas. Clinical lymphoma & myeloma 9(1), 39-42 (2009).
12. Chang H, Qi X, Xu W, Reader JC, Ning Y. Analysis of 6q deletion in Waldenstrom macroglobulinemia. European journal of haematology 79(3), 244-247 (2007).
13. Braggio E, Keats JJ, Leleu X et al. Identification of copy number abnormalities and inactivating mutations in two negative regulators of nuclear factor-kappaB signaling pathways in Waldenstrom's macroglobulinemia. Cancer research 69(8), 3579-3588 (2009).
14. Gutierrez NC, Ocio EM, De Las Rivas J et al. Gene expression profiling of B lymphocytes and plasma cells from Waldenstrom's macroglobulinemia: comparison with expression patterns of the same cell counterparts from chronic lymphocytic leukemia, multiple myeloma and normal individuals. Leukemia 21(3), 541-549 (2007).
27
15. Poulain S, Braggio E, Roumier C et al. High-throughput genomic analysis in Waldenstrom's macroglobulinemia. Clinical lymphoma, myeloma & leukemia 11(1), 106-108 (2011).
16. Turner CA, Jr., Mack DH, Davis MM. Blimp-1, a novel zinc finger-containing protein that can drive the maturation of B lymphocytes into immunoglobulin-secreting cells. Cell 77(2), 297-306 (1994).
17. Nguyen-Khac F, Lambert J, Chapiro E et al. Chromosomal aberrations and their prognostic value in a series of 174 untreated patients with Waldenstrom's macroglobulinemia. Haematologica 98(4), 649-654 (2013).
18. Treon SP, Xu L, Yang G et al. MYD88 L265P somatic mutation in Waldenstrom's macroglobulinemia. The New England journal of medicine 367(9), 826-833 (2012).
•• The presence of a widely expressed somatic mutation (MYD88 L265P) was described in patients with Waldenstrom's macroglobulinemia.
19. Xu L, Hunter ZR, Yang G et al. MYD88 L265P in Waldenstrom macroglobulinemia, immunoglobulin M monoclonal gammopathy, and other B-cell lymphoproliferative disorders using conventional and quantitative allele-specific polymerase chain reaction. Blood 121(11), 2051-2058 (2013).
20. Varettoni M, Arcaini L, Zibellini S et al. Prevalence and clinical significance of the MYD88 (L265P) somatic mutation in Waldenstrom's macroglobulinemia and related lymphoid neoplasms. Blood 121(13), 2522-2528 (2013).
21. Gachard N, Parrens M, Soubeyran I et al. IGHV gene features and MYD88 L265P mutation separate the three marginal zone lymphoma entities and Waldenstrom macroglobulinemia/lymphoplasmacytic lymphomas. Leukemia 27(1), 183-189 (2013).
22. Jimenez C, Sebastian E, Chillon MC et al. MYD88 L265P is a marker highly characteristic of, but not restricted to, Waldenstrom's macroglobulinemia. Leukemia 27(8), 1722-1728 (2013).
23. Poulain S, Roumier C, Decambron A et al. MYD88 L265P mutation in Waldenstrom macroglobulinemia. Blood 121(22), 4504-4511 (2013).
24. Mori N, Ohwashi M, Yoshinaga K et al. L265P Mutation of the MYD88 Gene Is Frequent in Waldenstrom's Macroglobulinemia and Its Absence in Myeloma. PloS one 8(11), e80088 (2013).
25. Ondrejka SL, Lin JJ, Warden DW, Durkin L, Cook JR, Hsi ED. MYD88 L265P somatic mutation: its usefulness in the differential diagnosis of bone marrow involvement by B-cell lymphoproliferative disorders. American journal of clinical pathology 140(3), 387-394 (2013).
26. Landgren O, Staudt L. MYD88 L265P somatic mutation in IgM MGUS. The New England journal of medicine 367(23), 2255-2256; author reply 2256-2257 (2012).
27. Muzio M, Ni J, Feng P, Dixit VM. IRAK (Pelle) family member IRAK-2 and MyD88 as proximal mediators of IL-1 signaling. Science 278(5343), 1612-1615 (1997).
28. Wesche H, Henzel WJ, Shillinglaw W, Li S, Cao Z. MyD88: an adapter that recruits IRAK to the IL-1 receptor complex. Immunity 7(6), 837-847 (1997).
29. Bianchi G, Sacco A, Kumar S, Rossi G, Ghobrial I, Roccaro A. Candidate genes of Waldenstrom's macroglobulinemia: current evidence and research. The application of clinical genetics 6, 33-42 (2013).
30. Hunter Z, Xu L, Yang G et al. The genomic landscape of Waldenstom's Macroglobulinemia is characterized by highly recurring MYD88 and WHIM-like CXCR4 mutations, and small somatic deletions associated with B-cell lymphomagenesis. Blood (2013).
28

31. Roccaro AM, Sacco A, Jimenez C, Et Al. A Novel Activating Mutation Of CXCR4 Plays a Crucial Role In Waldenstrom Macroglobulinemia Biology. Blood (ASH annual meeting abstracts). 122(21), 272 (2013).
32. Cao Y, Xu L, Liu X, Et Al. Whole Genome Sequencing Identifies Recurring Somatic Mutations in the C-Terminal Domain of CXCR4, Including a Gain of Function Mutation in Waldenstrom's Macroglobinemia. Blood (ASH annual meeting abstracts). 120(21), 2715 (2012).
33. Esteller M. Epigenetics provides a new generation of oncogenes and tumour-suppressor genes. British journal of cancer 94(2), 179-183 (2006).
34. Esteller M. Epigenetics provides a new generation of oncogenes and tumour-suppressor genes. British journal of cancer 96 Suppl, R26-30 (2007).
35. Esteller M. Epigenetics in cancer. The New England journal of medicine 358(11), 1148-1159 (2008).
36. Roccaro AM, Sacco A, Chen C et al. microRNA expression in the biology, prognosis, and therapy of Waldenstrom macroglobulinemia. Blood 113(18), 4391-4402 (2009).
37. Sacco A, Ghobrial IM, Roccaro AM. Epigenetics in Waldenstrom's macroglobulinemia. Epigenomics 2(5), 691-696 (2010).
38. Calin GA, Cimmino A, Fabbri M et al. MiR-15a and miR-16-1 cluster functions in human leukemia. Proceedings of the National Academy of Sciences of the United States of America 105(13), 5166-5171 (2008).
39. Chng WJ, Schop RF, Price-Troska T et al. Gene-expression profiling of Waldenstrom macroglobulinemia reveals a phenotype more similar to chronic lymphocytic leukemia than multiple myeloma. Blood 108(8), 2755-2763 (2006).
40. Trojani A, Greco A, Tedeschi A et al. Microarray demonstrates different gene expression profiling signatures between Waldenstrom macroglobulinemia and IgM monoclonal gammopathy of undetermined significance. Clinical lymphoma, myeloma & leukemia 13(2), 208-210 (2013).
41. Hatjiharissi E, Ngo H, Leontovich AA et al. Proteomic analysis of waldenstrom macroglobulinemia. Cancer research 67(8), 3777-3784 (2007).
42. Gottipati S, Rao NL, Fung-Leung WP. IRAK1: a critical signaling mediator of innate immunity. Cellular signalling 20(2), 269-276 (2008).
43. Yang G, Zhou Y, Liu X et al. A mutation in MYD88 (L265P) supports the survival of lymphoplasmacytic cells by activation of Bruton tyrosine kinase in Waldenstrom macroglobulinemia. Blood 122(7), 1222-1232 (2013).
• The study showed that combined inhibition of BTK and IRAK in MYD88 L265P expressing WM cells provides synergistic inhibition of NF-κB signaling and WM cell killing.
44. Treon SP, Hunter ZR. A new era for Waldenstrom macroglobulinemia: MYD88 L265P. Blood 121(22), 4434-4436 (2013).
45. Vivanco I, Sawyers CL. The phosphatidylinositol 3-Kinase AKT pathway in human cancer. Nature reviews. Cancer 2(7), 489-501 (2002).
46. Leleu X, Jia X, Runnels J et al. The Akt pathway regulates survival and homing in Waldenstrom macroglobulinemia. Blood 110(13), 4417-4426 (2007).
47. Sacco A, Roccaro A, Ghobrial IM. Role of dual PI3/Akt and mTOR inhibition in Waldenstrom's Macroglobulinemia. Oncotarget 1(7), 578-582 (2010).
48. Yang G, Liu X, Zhou Y, Et Al. PI3K/AKT Pathway Is Activated By MYD88 L265P and Use Of PI3K-Delta Inhibitors Induces Robust Tumor Cell Killing In Waldenstrom’s Macroglobulinemia. Blood (ASH annual meeting abstracts). 122(21), 4255 (2013).
29
49. Roccaro AM, Sacco A, Husu EN et al. Dual targeting of the PI3K/Akt/mTOR pathway as an antitumor strategy in Waldenstrom macroglobulinemia. Blood 115(3), 559-569 (2010).
50. Hodge LS, Ansell SM. Jak/Stat pathway in Waldenstrom's macroglobulinemia. Clinical lymphoma, myeloma & leukemia 11(1), 112-114 (2011).
51. Elsawa SF, Novak AJ, Ziesmer SC et al. Comprehensive analysis of tumor microenvironment cytokines in Waldenstrom macroglobulinemia identifies CCL5 as a novel modulator of IL-6 activity. Blood 118(20), 5540-5549 (2011).
52. Hayden MS, Ghosh S. Signaling to NF-kappaB. Genes & development 18(18), 2195-2224 (2004).
53. Roccaro AM, Leleu X, Sacco A et al. Dual targeting of the proteasome regulates survival and homing in Waldenstrom macroglobulinemia. Blood 111(9), 4752-4763 (2008).
54. Roccaro AM, Sacco A, Aujay M et al. Selective inhibition of chymotrypsin-like activity of the immunoproteasome and constitutive proteasome in Waldenstrom macroglobulinemia. Blood 115(20), 4051-4060 (2010).
55. Treon SP, Ioakimidis L, Soumerai JD et al. Primary therapy of Waldenstrom macroglobulinemia with bortezomib, dexamethasone, and rituximab: WMCTG clinical trial 05-180. Journal of clinical oncology : official journal of the American Society of Clinical Oncology 27(23), 3830-3835 (2009).
56. Ghobrial IM, Xie W, Padmanabhan S et al. Phase II trial of weekly bortezomib in combination with rituximab in untreated patients with Waldenstrom Macroglobulinemia. American journal of hematology 85(9), 670-674 (2010).
57. Ghobrial IM, Hong F, Padmanabhan S et al. Phase II trial of weekly bortezomib in combination with rituximab in relapsed or relapsed and refractory Waldenstrom macroglobulinemia. Journal of clinical oncology : official journal of the American Society of Clinical Oncology 28(8), 1422-1428 (2010).
58. Kyle RA, Therneau TM, Rajkumar SV et al. Long-term follow-up of IgM monoclonal gammopathy of undetermined significance. Blood 102(10), 3759-3764 (2003).
59. Rajkumar SV, Kyle RA, Therneau TM et al. Serum free light chain ratio is an independent risk factor for progression in monoclonal gammopathy of undetermined significance. Blood 106(3), 812-817 (2005).
60. Varettoni M, Zibellini S, Arcaini L et al. MYD88 (L265P) mutation is an independent risk factor for progression in patients with IgM monoclonal gammopathy of undetermined significance. Blood 122(13), 2284-2285 (2013).
61. Kyle RA, Garton JP. The spectrum of IgM monoclonal gammopathy in 430 cases. Mayo Clinic proceedings. Mayo Clinic 62(8), 719-731 (1987).
62. Leleu X, Moreau AS, Weller E et al. Serum immunoglobulin free light chain correlates with tumor burden markers in Waldenstrom macroglobulinemia. Leukemia & lymphoma 49(6), 1104-1107 (2008).
63. Schop RF, Van Wier SA, Xu R et al. 6q deletion discriminates Waldenstrom macroglobulinemia from IgM monoclonal gammopathy of undetermined significance. Cancer genetics and cytogenetics 169(2), 150-153 (2006).
64. Treon SP, Hunter ZR, Aggarwal A et al. Characterization of familial Waldenstrom's macroglobulinemia. Annals of oncology : official journal of the European Society for Medical Oncology / ESMO 17(3), 488-494 (2006).
65. Kristinsson SY, Bjorkholm M, Goldin LR, Mcmaster ML, Turesson I, Landgren O. Risk of lymphoproliferative disorders among first-degree relatives of lymphoplasmacytic lymphoma/Waldenstrom macroglobulinemia patients: a population-based study in Sweden. Blood 112(8), 3052-3056 (2008).
30

66. Vos JM, Minnema MC, Wijermans PW et al. Guideline for diagnosis and treatment of Waldenstrom's macroglobulinaemia. The Netherlands journal of medicine 71(2), 54-62 (2013).
67. Ghobrial IM, Witzig TE. Waldenstrom macroglobulinemia. Current treatment options in oncology 5(3), 239-247 (2004).
68. Hunter ZR, Branagan AR, Manning R et al. CD5, CD10, and CD23 expression in Waldenstrom's macroglobulinemia. Clinical lymphoma 5(4), 246-249 (2005).
69. Ghobrial IM. Are you sure this is Waldenstrom macroglobulinemia? Hematology / the Education Program of the American Society of Hematology. American Society of Hematology. Education Program 2012, 586-594 (2012).
70. Gertz MA. Waldenstrom macroglobulinemia: 2012 update on diagnosis, risk stratification, and management. American journal of hematology 87(5), 503-510 (2012).
71. Kyle RA, Benson JT, Larson DR et al. Progression in smoldering Waldenstrom macroglobulinemia: long-term results. Blood 119(19), 4462-4466 (2012).
72. Ghobrial IM, Fonseca R, Gertz MA et al. Prognostic model for disease-specific and overall mortality in newly diagnosed symptomatic patients with Waldenstrom macroglobulinaemia. British journal of haematology 133(2), 158-164 (2006).
73. Dhodapkar MV, Jacobson JL, Gertz MA et al. Prognostic factors and response to fludarabine therapy in patients with Waldenstrom macroglobulinemia: results of United States intergroup trial (Southwest Oncology Group S9003). Blood 98(1), 41-48 (2001).
74. Dimopoulos MA, Hamilos G, Zervas K et al. Survival and prognostic factors after initiation of treatment in Waldenstrom's macroglobulinemia. Annals of oncology : official journal of the European Society for Medical Oncology / ESMO 14(8), 1299-1305 (2003).
75. Kyle RA, Treon SP, Alexanian R et al. Prognostic markers and criteria to initiate therapy in Waldenstrom's macroglobulinemia: consensus panel recommendations from the Second International Workshop on Waldenstrom's Macroglobulinemia. Seminars in oncology 30(2), 116-120 (2003).
76. Dimopoulos M, Gika D, Zervas K et al. The international staging system for multiple myeloma is applicable in symptomatic Waldenstrom's macroglobulinemia. Leukemia & lymphoma 45(9), 1809-1813 (2004).
77. Morel P, Duhamel A, Gobbi P et al. International prognostic scoring system for Waldenstrom macroglobulinemia. Blood 113(18), 4163-4170 (2009).
78. Van Den Brand M, Van Krieken JH. Recognizing nodal marginal zone lymphoma: recent advances and pitfalls. A systematic review. Haematologica 98(7), 1003-1013 (2013).
79. Avet-Loiseau H, Garand R, Lode L, Robillard N, Bataille R. 14q32 Translocations discriminate IgM multiple myeloma from Waldenstrom's macroglobulinemia. Seminars in oncology 30(2), 153-155 (2003).
80. Dimopoulos MA, Gertz MA, Kastritis E et al. Update on treatment recommendations from the Fourth International Workshop on Waldenstrom's Macroglobulinemia. J Clin Oncol 27(1), 120-126 (2009).
81. Gertz MA. Waldenstrom macroglobulinemia: is newer really better? Leuk Lymphoma 51(12), 2152-2153 (2010).
82. Treon SP, Patterson CJ, Kimby E, Stone MJ. Advances in the biology and treatment of Waldenstrom's macroglobulinemia: a report from the 5th International Workshop on Waldenstrom's Macroglobulinemia, Stockholm, Sweden. Clin Lymphoma Myeloma 9(1), 10-15 (2009).
31
83. Anderson KC, Alsina M, Bensinger W et al. Waldenstrom's macroglobulinemia/lymphoplasmacytic lymphoma, version 2.2013. J Natl Compr Canc Netw 10(10), 1211-1219 (2012).
84. Owen RG, Kyle RA, Stone MJ et al. Response assessment in Waldenstrom macroglobulinaemia: update from the VIth International Workshop. British journal of haematology 160(2), 171-176 (2013).
85. Blum W, Porcu P. Therapeutic apheresis in hyperleukocytosis and hyperviscosity syndrome. Semin Thromb Hemost 33(4), 350-354 (2007).
86. Stone MJ, Bogen SA. Role of plasmapheresis in Waldenstrom's macroglobulinemia. Clin Lymphoma Myeloma Leuk 13(2), 238-240 (2013).
87. Rourke M, Anderson KC, Ghobrial IM. Review of clinical trials conducted in Waldenstrom macroglobulinemia and recommendations for reporting clinical trial responses in these patients. Leuk Lymphoma 51(10), 1779-1792 (2010).
88. Treon SP. How I treat Waldenstrom macroglobulinemia. Blood 114(12), 2375-2385 (2009).
89. Dimopoulos MA, Zervas C, Zomas A et al. Extended rituximab therapy for previously untreated patients with Waldenstrom's macroglobulinemia. Clin Lymphoma 3(3), 163-166 (2002).
90. Dimopoulos MA, Zervas C, Zomas A et al. Treatment of Waldenstrom's macroglobulinemia with rituximab. J Clin Oncol 20(9), 2327-2333 (2002).
91. Dimopoulos MA, Anagnostopoulos A, Kyrtsonis MC et al. Primary treatment of Waldenstrom macroglobulinemia with dexamethasone, rituximab, and cyclophosphamide. J Clin Oncol 25(22), 3344-3349 (2007).
92. Treon SP, Hanzis C, Tripsas C et al. Bendamustine therapy in patients with relapsed or refractory Waldenstrom's macroglobulinemia. Clin Lymphoma Myeloma Leuk 11(1), 133-135 (2011).
93. Dimopoulos MA, Roussou M, Kastritis E, Et Al. Primary Treatment of Waldenstrom's Macroglobulinemia with Dexamethasone, Rituximab and Cyclophosphamide (DRC): Final Analysis of a Phase II Study. Blood (ASH annual meeting abstracts). 120(21), 438 (2012).
94. Rummel MJ, Lerchenmüller C, Greil R, Et Al. Bendamustin-Rituximab Induction Followed by Observation or Rituximab Maintenance for Newly Diagnosed Patients with Waldenström's Macroglobulinemia: Results From a Prospective, Randomized, Multicenter Study (StiL NHL 7–2008 –MAINTAIN-; ClinicalTrials.gov Identifier: NCT00877214). Blood (ASH annual meeting abstracts). 120(21), 2739 (2012).
95. Treon SP, Hanzis C, Manning RJ et al. Maintenance Rituximab is associated with improved clinical outcome in rituximab naive patients with Waldenstrom Macroglobulinaemia who respond to a rituximab-containing regimen. Br J Haematol 154(3), 357-362 (2011).
96. Leblond V, Johnson S, Chevret S et al. Results of a randomized trial of chlorambucil versus fludarabine for patients with untreated Waldenstrom macroglobulinemia, marginal zone lymphoma, or lymphoplasmacytic lymphoma. J Clin Oncol 31(3), 301-307 (2013).
97. Leleu X, Soumerai J, Roccaro A et al. Increased incidence of transformation and myelodysplasia/acute leukemia in patients with Waldenstrom macroglobulinemia treated with nucleoside analogs. J Clin Oncol 27(2), 250-255 (2009).
98. Treon SP, Branagan AR, Ioakimidis L et al. Long-term outcomes to fludarabine and rituximab in Waldenstrom macroglobulinemia. Blood 113(16), 3673-3678 (2009).
32

99. Tam CS, Wolf M, Prince HM et al. Fludarabine, cyclophosphamide, and rituximab for the treatment of patients with chronic lymphocytic leukemia or indolent non-Hodgkin lymphoma. Cancer 106(11), 2412-2420 (2006).
100. Tedeschi A, Benevolo G, Varettoni M et al. Fludarabine plus cyclophosphamide and rituximab in Waldenstrom macroglobulinemia: an effective but myelosuppressive regimen to be offered to patients with advanced disease. Cancer 118(2), 434-443 (2012).
101. Issa GC, Leblebjian H, Roccaro AM, Ghobrial IM. New insights into the pathogenesis and treatment of Waldenstrom macroglobulinemia. Curr Opin Hematol 18(4), 260-265 (2011).
102. Treon SP, Patterson CJ, Munshi NC, Anderson KC. Proceedings of the Seventh International Workshop on Waldenstrom Macroglobulinemia. Clin Lymphoma Myeloma Leuk 13(2), 181-183 (2013).
103. Sacco A, Aujay M, Morgan B et al. Carfilzomib-dependent selective inhibition of the chymotrypsin-like activity of the proteasome leads to antitumor activity in Waldenstrom's Macroglobulinemia. Clin Cancer Res 17(7), 1753-1764 (2011).
104. Treon Sp TC, Sheehy P, Et Al. Prospective Phase II Clinical Trial of Carfilzomib, rituximab and Dexamethasone (CARD) in Patients with Symptomatic Waldenstrom's Macroglobulinemia (WM) [abstract]. IWWM-7 (2012).
105. Ghobrial IM, Gertz M, Laplant B et al. Phase II trial of the oral mammalian target of rapamycin inhibitor everolimus in relapsed or refractory Waldenstrom macroglobulinemia. J Clin Oncol 28(8), 1408-1414 (2010).
106. Ghobrial IM, Boswell E, Banwait R, Et Al. Phase I Trial of Everolimus and Rituximab or Everolimus, Bortezomib and Rituximab in Relapsed or Relapsed/Refractory Waldenstrom's Macroglobulinemia. Blood (ASH annual meeting abstracts). 118(21), 2705 (2011).
107. Ghobrial IM, Moreau P, Harris B et al. A multicenter phase II study of single-agent enzastaurin in previously treated Waldenstrom macroglobulinemia. Clin Cancer Res 18(18), 5043-5050 (2012).
108. Ghobrial IM, Roccaro A, Hong F et al. Clinical and translational studies of a phase II trial of the novel oral Akt inhibitor perifosine in relapsed or relapsed/refractory Waldenstrom's macroglobulinemia. Clin Cancer Res 16(3), 1033-1041 (2010).
109. Treon SP, Soumerai JD, Branagan AR et al. Thalidomide and rituximab in Waldenstrom macroglobulinemia. Blood 112(12), 4452-4457 (2008).
110. Treon SP, Soumerai JD, Branagan AR et al. Lenalidomide and rituximab in Waldenstrom's macroglobulinemia. Clin Cancer Res 15(1), 355-360 (2009).
111. Sheeba K. Thomas1 RA, L. Michael Wang1, Sattva S. Neelapu1, A. Georgina Melendez1, Roxana Duran1, Lei Feng2, Jatin J. Shah1, Robert Z. Orlowski1, Donna M. Weber1. A Phase I Trial of Pomalidomide in Patients with Relapsed and/or Refractory Waldenström's Macroglobulinemia (WM). IWWM-7 Session-9 Friday August 24 (2012).
112. Treon SP, Tripsas C, Warren D, Et Al. Phase I Study of Pomalidomide, Dexamethasone and Rituximab (PDR) in Patients with Relapsed or Refractory Waldenstrom's Macroglobulenima. Hematological Oncology (Abstract). 31(S1), 536 (2013).
113. Grant S. Targeting Waldenstrom macroglobulinemia with histone deacetylase inhibitors. Leuk Lymphoma 52(9), 1623-1625 (2011).
114. Ghobrial IM, Campigotto F, Murphy TJ et al. Results of a phase 2 trial of the single-agent histone deacetylase inhibitor panobinostat in patients with relapsed/refractory Waldenstrom macroglobulinemia. Blood 121(8), 1296-1303 (2013).
33

115. Yang G XL, Zhou Y, Et Al. Participation of BTK in MYD88 signaling in malignant cells expressing the L265P mutation in Waldenstrom's macroglobulinemia, and effect on tumor cell with BTK-inhibitor PCI-32765 in combination with MYD88 pathway inhibitors [abstract]. J Clin Oncol suppl;abstract 8106(2012).
116. Advani RH, Buggy JJ, Sharman JP et al. Bruton Tyrosine Kinase Inhibitor Ibrutinib (PCI-32765) Has Significant Activity in Patients With Relapsed/Refractory B-Cell Malignancies. J Clin Oncol (2012).
• Phase I study of ibrutinib, BKT inihbitor, showed activity in patients with relapsed/refractory B-cell malignancies including Waldenström's macroglobulinemia.
34