waiting to exhale: optimizing patient outcomes in the ... · pdf fileclinical copd...
TRANSCRIPT
3/11/2013
1
Waiting to Exhale:
Optimizing Patient
Outcomes
in the Management of COPD
Kyle Copeland, PharmD
Clinical Pharmacist Specialist
Parkwest Medical Center
Knoxville, Tennessee
Presenter:
Kyle Copeland, PharmD Clinical Pharmacist Specialist Parkwest Medical Center Knoxville, Tennessee Moderator:
Elena Beyzarov, PharmD Director of Scientific Affairs Pharmacy Times Office of Continuing Professional Education Plainsboro, New Jersey
This activity is supported by an educational grant from
Boehringer Ingelheim Pharmaceuticals, Inc. and Sunovion
Pharmaceuticals, Inc.
Faculty Information
3/11/2013
2
Disclosures Kyle Copeland, PharmD, has no financial relationships with commercial interests to disclose
Pharmacy Times Office of Continuing Professional Education
Planning Staff—Judy V. Lum, MPA, Elena Beyzarov, PharmD, and Donna W. Fausak—have no financial relationships with commercial interests to disclose.
The contents of this webinar may include information regarding the use of products that may be inconsistent with or outside the approved labeling for these products in the United States. Pharmacists should note that the use of these products outside current approved labeling is considered experimental and are advised to consult prescribing information for these products.
Explore current prevalence, diagnosis, and treatment of COPD
Evaluate the GOLD recommendations on COPD management and apply current guideline recommendations to improve standards of care and patient outcomes
Examine proper selection and use of currently available medication devices for COPD
Discuss the pharmacist’s role in optimizing management of COPD
Objectives
3/11/2013
3
Pharmacy Times Office of Continuing
Professional Education is accredited by
the Accreditation Council for Pharmacy
Education (ACPE) as a provider of
continuing pharmacy education. This
activity is approved for 1.0 contact hours
(0.10 CEUs) under the ACPE universal
activity number 0290-0000-13-113-L01-P.
The activity is available for CE credit
through February 28, 2013.
Type of Activity: Knowledge
Pharmacy Accreditation
Waiting to Exhale:
Optimizing Patient Outcomes
in the Management of COPD
Kyle Copeland, PharmD
Clinical Pharmacist Specialist
Parkwest Medical Center
Knoxville, Tennessee
3/11/2013
4
Prevalence and Diagnosis
GOLD Guideline, 2013 www.goldcopd.org
J Am Pharm Assoc. 2011;51:203-211.
N Engl J Med. 2004;350:2689-2697.
4th leading cause of death in the U.S.
Expected to become 3rd leading cause of
death very soon
Accounts for 10% of hospital occupancy
More than 24 million Americans
estimated to have COPD
Prevalence
3/11/2013
5
Common preventable and treatable
disease, characterized by persistent
airflow limitation that is usually
progressive and associated with
enhanced chronic inflammatory
response in the airways and the lung to
noxious particles or gases.
GOLD Guideline, 2013 www.goldcopd.org
COPD: Definition
Burden
GOLD Guideline, 2013 www.goldcopd.org
Economic Burden (U.S.)
Direct costs: $29.5 billion
Indirect costs: $20.4 billion
Economic Burden (Europe)
€38.6 billion euros
3.3% of total health care budget in
European Union
3/11/2013
6
GOLD Guideline, 2013 www.goldcopd.org
Key indicators for considering COPD
Dyspnea
Chronic cough
Chronic sputum production
Exposure to risk factors
Family history of COPD
Additional risk factors
Pattern of symptom development
History of previous hospitalizations
Diagnosis
GOLD Guideline, 2013 www.goldcopd.org
Diagnosis
Spirometry
Required to make diagnosis clinically
post-bronchodilator fixed ratio of
FEV1/FVC of <0.7 confirms COPD
Degree of reversibility of airflow limitation
(FEV1 before and after bronchodilators) no
longer recommended
3/11/2013
7
Assessment
of Disease
GOLD Guideline, 2013 www.goldcopd.org
Symptoms
Modified British Medical Council (mMRC)
Grade 0 (breathless with exercise) to
Grade 4 (breathless at rest)
Predicts future mortality risk
COPD Assessment Test (CAT)
8 item, uni-dimensional measure of
impairment of health status in COPD
Score ranges from 0 (lowest) to 40 (highest)
3/11/2013
8
Clinical COPD Questionnaire (CCQ)
-- NEW --
Self-administered questionnaire developed
specifically to measure clinical control
Data supports validity, reliability, &
responsiveness
Short and easy to administer
GOLD Guideline, 2013 www.goldcopd.org
Symptoms
GOLD Guideline, 2013 www.goldcopd.org
Airflow Limitation
Spirometric Assessment
Based on % FEV1 compared with predicted
Performed post-bronchodilator
GOLD Level
1. Mild: FEV1 > 80% predicted
2. Moderate: 50% < FEV1 < 80%
3. Severe: 30% < FEV1 < 50%
4. Very Severe: FEV1 < 30%
3/11/2013
9
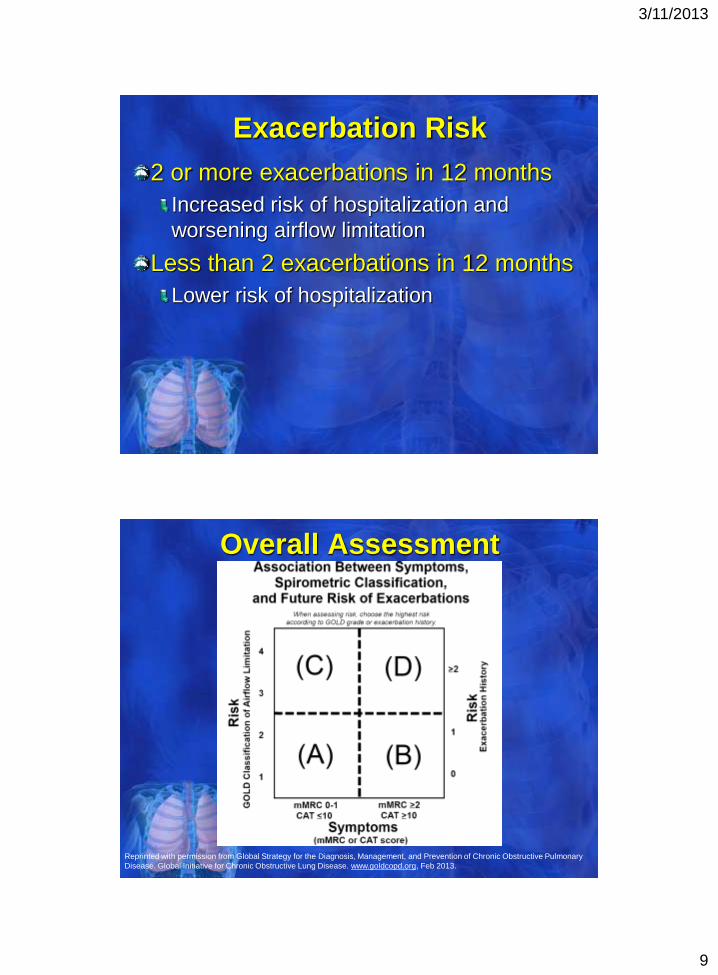
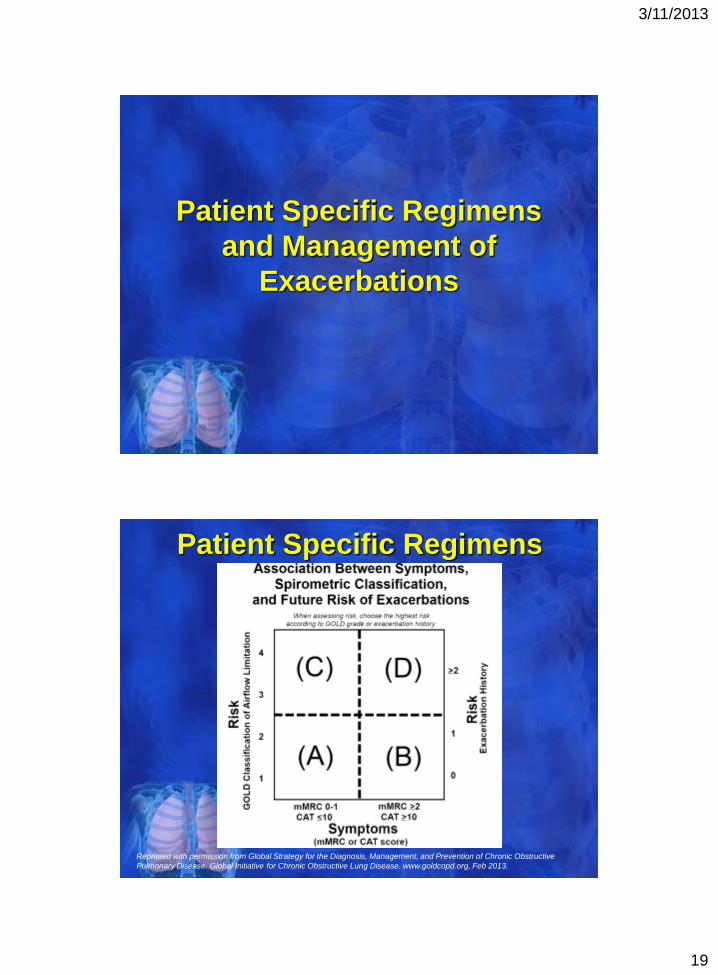
Exacerbation Risk
2 or more exacerbations in 12 months
Increased risk of hospitalization and
worsening airflow limitation
Less than 2 exacerbations in 12 months
Lower risk of hospitalization
Reprinted with permission from Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary
Disease. Global Initiative for Chronic Obstructive Lung Disease. www.goldcopd.org, Feb 2013.
Overall Assessment
3/11/2013
10
GOLD Guideline, 2013 www.goldcopd.org
Imaging
Lung Volumes & Diffusing Capacity
Oximetry & ABG Measurements
Alpha-1 Antitrypsin Deficiency Screening
Exercise Testing
Additional
Treatment of
COPD
3/11/2013
11
GOLD Guideline, 2013 www.goldcopd.org
Therapeutic Goals
Reduce Symptoms
Relieve immediate symptoms
Improve exercise tolerance
Improve health status
Reduce Risk of Exacerbations
Prevent disease progression
Prevent & treat exacerbations
Reduce mortality
GOLD Guideline, 2013 www.goldcopd.org
Non-Pharmacologic
Smoking Cessation
Rehabilitation
Oxygen Supplementation
Pharmacologic
Bronchodilators
Corticosteroids
Other Options
Therapeutic Options
3/11/2013
12
GOLD Guideline, 2013 www.goldcopd.org
Smoking Cessation
The intervention with the greatest
capacity to influence the natural history
of COPD
Nicotine Replacement (vs) Medications
The 5 “A’s”
Ask, Advise, Assess, Assist, & Arrange
GOLD Guideline, 2013 www.goldcopd.org
Non-Pharmacologic
Rehabilitation
Exercise
Education
Assessment and Follow-up
Nutrition Counseling
Oxygen Therapy
Improves survival in patients with chronic
respiratory failure & severe resting hypoxia
3/11/2013
13
GOLD Guideline, 2013 www.goldcopd.org
Pharmacologic
Bronchodilators
Beta2-agonists
Anticholinergics
Theophylline
Corticosteroids
Inhaled
Systemic
Other Therapies
Phosphodiesterase-4
Inhibitors
Alpha-1 Antitrypsin
Therapy
Increase FEV1 or change other
spirometric variables, usually by altering
airway smooth muscle tone
Inhaled therapy is preferred
Dose-response relationships
Outcomes in acute episodes
Toxicity
As needed (vs.) regular basis
GOLD Guideline, 2013 www.goldcopd.org
Bronchodilators
3/11/2013
14
GOLD Guideline, 2013 www.goldcopd.org
Beta2-Agonists
Short-Acting
Regular and “as needed” use improve FEV1 and symptoms
Usually wear off in 4-6 hours
Long-Acting
Significantly improve FEV1, lung volumes, dyspnea, quality of life, exacerbation rates
Adverse Effects
Sinus tachycardia, cardiac arrhythmias
Beta2-Agonists
Short-Acting
Albuterol
Levalbuterol
Terbutaline
Long-Acting
Formoterol
Arformoterol
Salmeterol
GOLD Guideline, 2013 www.goldcopd.org
3/11/2013
15
GOLD Guideline, 2013 www.goldcopd.org
Anticholinergics
Short-Acting
Longer duration than short-acting beta2-agonists
Long-Acting
Reduce exacerbations & related hospitalizations, improve symptoms & health status
Adverse Effects
Dryness of mouth, bitter taste
GOLD Guideline, 2013 www.goldcopd.org
Anticholinergics
Short-Acting
Ipratropium
Long-Acting
Tiotropium
3/11/2013
16
GOLD Guideline, 2013 www.goldcopd.org
Methylxanthines
Theophylline
Less effective and less tolerated than
long-acting bronchodilators
Not recommended if other options available
and affordable
Problems include: atrial & ventricular
arrhythmias, grand mal convulsions
Significant drug-drug interactions
GOLD Guideline, 2013 www.goldcopd.org
Corticosteroids
Inhaled vs. Systemic
Inhaled always chosen for regular therapy
Systemic reserved only for short courses in treatment of exacerbations
Regular Treatment
Improves symptoms, lung function, quality of life,
Reduces frequency of exacerbations in patients with FEV1 <60% predicted
3/11/2013
17
GOLD Guideline, 2013 www.goldcopd.org
Corticosteroids
Adverse Effects
Oral candidiasis, hoarse voice, skin bruising
Combination with Bronchodilators
Inhaled corticosteroid combined with a
long-acting beta2-agonist more effective
than the individual components in patients
with moderate to severe COPD
Corticosteroids
GOLD Guideline, 2013 www.goldcopd.org
Inhaled
Beclomethasone
Budesonide
Fluticasone
Systemic
Prednisone
Methylprednisone
3/11/2013
18
GOLD Guideline, 2013 www.goldcopd.org
PDE4 Inhibitors
Single Agent Roflumilast
No direct bronchodilator activity
Improves FEV1 in patients treated with
salmeterol or tiotropium
Adverse Effects
More common than inhaled medications
Nausea, abdominal pain, diarrhea,
sleep disturbances, headache
Other Therapies
Vaccines
Alpha-1 Antitrypsin Therapy
Antibiotics
Mucolytics
Antitussives
GOLD Guideline, 2013 www.goldcopd.org
3/11/2013
19
Patient Specific Regimens
and Management of
Exacerbations
Reprinted with permission from Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive
Pulmonary Disease. Global Initiative for Chronic Obstructive Lung Disease. www.goldcopd.org, Feb 2013.
Patient Specific Regimens
3/11/2013
20
“A” – Few Symptoms, Low Risk
Recommended First Choices:
• Short-acting anticholinergic “prn”
• Short-acting beta2-agonist “prn”
Alternates:
• Short-acting anticholinergic PLUS
Short-acting beta2-agnoist
• Long-acting anticholinergic
• Long-acting beta2-agonist
GOLD Guideline, 2013 www.goldcopd.org
Patient Specific Regimens
“B” – More Symptoms, Low Risk
Recommended First Choices:
• Long-acting anticholinergic
• Long-acting beta2-agonist
Alternate:
• Long-acting anticholinergic PLUS
Long-acting beta2-agonist
GOLD Guideline, 2013 www.goldcopd.org
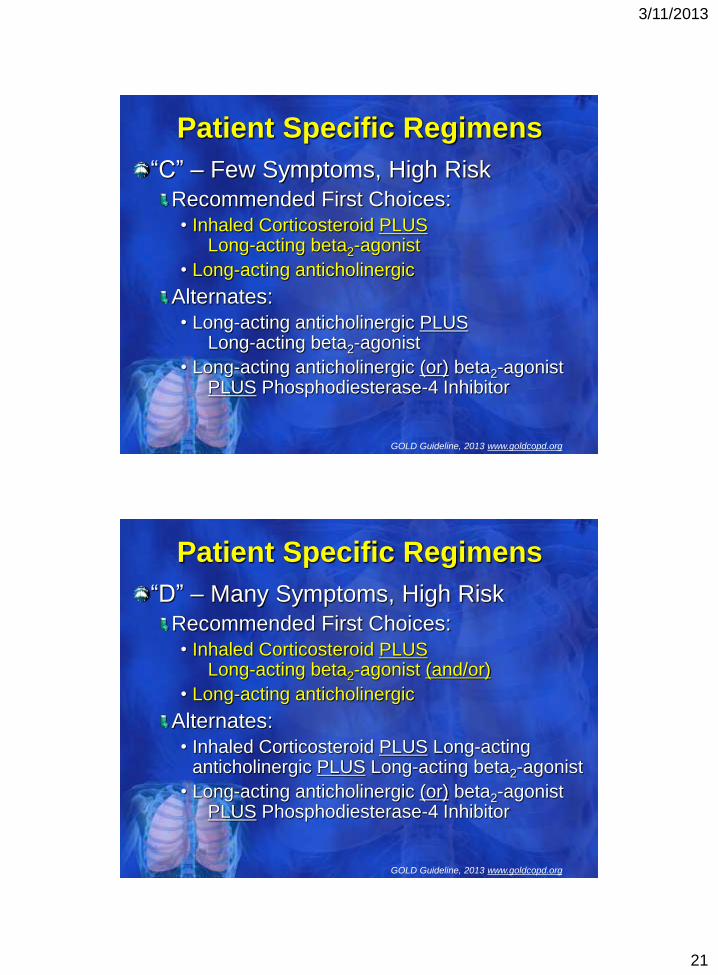
Patient Specific Regimens
3/11/2013
21
“C” – Few Symptoms, High Risk
Recommended First Choices:
• Inhaled Corticosteroid PLUS Long-acting beta2-agonist
• Long-acting anticholinergic
Alternates:
• Long-acting anticholinergic PLUS Long-acting beta2-agonist
• Long-acting anticholinergic (or) beta2-agonist PLUS Phosphodiesterase-4 Inhibitor
GOLD Guideline, 2013 www.goldcopd.org
Patient Specific Regimens
“D” – Many Symptoms, High Risk
Recommended First Choices:
• Inhaled Corticosteroid PLUS Long-acting beta2-agonist (and/or)
• Long-acting anticholinergic
Alternates:
• Inhaled Corticosteroid PLUS Long-acting anticholinergic PLUS Long-acting beta2-agonist
• Long-acting anticholinergic (or) beta2-agonist PLUS Phosphodiesterase-4 Inhibitor
GOLD Guideline, 2013 www.goldcopd.org
Patient Specific Regimens
3/11/2013
22
Short-Acting Bronchodilators
Increased doses and/or frequency
Corticosteroids, Systemic
Short duration
Shortens recovery, reduce early relapse risk
Antibiotics
Recommended duration 5-10 days
Oxygen & ventilator support as needed
GOLD Guideline, 2013 www.goldcopd.org
Exacerbations
Heart Failure
Osteoporosis
Lung Cancer
Difficult to Treat
3/11/2013
23
Proper Device Selection and
Utilization
Delivery Systems
Nebulized Solutions (Nebs)
Metered Dose Inhalers (MDI’s)
Dry-Power Inhalers (DPI’s)
Breath-Actuated MDI’s (BA-MDI’s)
Soft-Mist Inhalers (SMI’s)
J Am Acad Nurs Pract. 2012;24:113-20
www.nationalasthma.org.au, 2008
Selection & Utilization
3/11/2013
24
Selection & Utilization
Considerations
Medication availability / Insurance coverage
Previous / current inhaler types
Cognitive function
Lung function
Strength & Dexterity
Patient specific issues
Selection & Utilization
Virchow et al.
1. Determine devices in which the medication is available
2. Determine inspiratory effort
a. If sufficient inspiratory flow or effective vital capacity, DPI is preferred
b. Second choice is MDI w/ spacer
3. Use same device type, if possible, for continuity when multiple inhalers are used
a. DPI preferred when multiple inhalers used
Respir Med. 2008;102:10-19
3/11/2013
25
Nebulized Meds
Oldest form of inhaled medication
delivery
Requires “nebulizer”
machine
Uses oxygen, compressed air, or
ultrasonic power to aerosolize the
medication
Delivered to using mouthpiece or mask
Limited to hospital and home use
One of the most common delivery
systems
Medication delivered as a mist
Slowly inhaled into lungs and
held for a few seconds before
being exhaled
Higher degree of coordination / strength
Spacer or no spacer?
Metered Dose Inhalers
3/11/2013
26
Developed as alternative to MDI’s
Multiple delivery systems
Proprietary Systems
Capsule-Based Delivery
Minimum inspiratory requirements
Minimum coordination / strength needed
Wide number of medications available
Dry Powder Inhalers
Breath-Actuated MDI’s
Derivative of traditional MDI’s
Incorporates flow trigger
Removes coordination requirement
Highly preferred among patients who
have tried it
Limited by minimal number of available
meds utilizing it
3/11/2013
27
Soft-Mist Inhalers
Approved in July 2012
Currently only one (combination) product is approved
Propellant-free device
Generates very fine, slow moving mist
Very specific priming steps
Extra education required
The Pharmacist’s
Role
3/11/2013
28
Counseling
Patients up to 68% unable to use inhaler
devices properly
Healthcare up to the same percent
cannot demonstrate proper use
Must be routine part of care from
prescribing to dispensing
Every time a prescription is filled,
new (or) refill… check technique GOLD Guideline, 2013 www.goldcopd.org
Jour Asthma. 2007;44:593-598
Respir Care. 2005;50:1360-1374
Pharmacist’s Role
Pharmacist’s Role
Am J Health-Syst Pharm. 2011;68:1221-32
Proper Device Selection
What is available?
What are they using now?
Can they demonstrate proper use?
What do they prefer?
All Things Equal…
First Choice: Dry Powder Inhaler
Second Choice: MDI (with spacer)
3/11/2013
29
Get Proactive!
COPD will soon be the number 3 cause
of death in the U.S.
Chronic airway disease management is
“10% medication & 90% education”
COPD is “preventable” with irreversible
airway progression
Educate & reinforce at every opportunity
GOLD Guideline, 2013 www.goldcopd.org
Jour Asthma. 2007;44:593-598
Pharmacist’s Role
Questions

3/11/2013
30
Disclaimer The information provided in this CPE activity is for continuing
medical and pharmacy education purposes only and does not
constitute any form of professional advice or referral. Discussions
concerning drugs, dosages, and procedures may reflect the clinical
experience of the faculty or they may be derived from the
professional literature or other sources and may suggest uses that
are investigational in nature and not based on approved labeling or
indications. Participants are encouraged to refer to primary
references or full prescribing information resources for all products
discussed.
The opinions expressed in the content and provided verbally by
faculty in this Webinar are solely those of the individual faculty
members and do not reflect those of Pharmacy Times Office of
Continuing Professional Education or the company providing
commercial support for this CPE activity.
Thank You!