volatile substance abuse—post-mortem diagnosis
TRANSCRIPT

Volatile substance abuse—post-mortem diagnosis
Sarah M.R. Wille, Willy E.E. Lambert*
Laboratory of Toxicology, Ghent University, Harelbekestraat 72, B-9000 Gent, Belgium
Abstract
A substantial number of children and adolescents world-wide abuse volatile substances with the intention to experience an
euphoric state of consciousness. Although the ratio of deaths to nonfatal inhalation escapades is low, it is an important and
preventable cause of death in young people. In the analytical investigation of volatile substances proper sample collection,
storage and handling are important in view of the volatile nature of the compounds. Volatile organic compounds in post-mortem
matrices such as blood, urine and tissues are generally determined by gas chromatography after extracting the compounds with
methods such as static and dynamic headspace or even with pulse-heating and solvent extraction. In post-mortem cases,
metabolites in urine seem less relevant, however, trichloroethanol and trichloroacetic acid were determined in several cases.
When interpreting qualitative and quantitative results, researchers should be aware of false conclusions. The main reason why
scepticism is necessary is the occurrence of losses of analytes during sampling, sample handling and storage, which results in
false quantitation.
# 2004 Elsevier Ireland Ltd. All rights reserved.
Keywords: Volatile substance abuse; Post-mortem; Sample handling; Headspace analysis; Volatile organic compounds
1. Introduction
1.1. Prevalence
Epidemiological studies indicate that a substantial num-
ber of children and adolescents world-wide abuse volatile
substances with the intention to experience an euphoric state
of consciousness [1–3].
According to the National Institute on Drug Abuse [4,5]
use of inhalants in the US for 8th and 10th graders declined
from 21.6% in 1995 to 15.2% in 2002, while about 17%
of the adolescents have at least experimented with inhalants
[3–5]. On the contrary, inhalant abuse has emerged and
gradually increased in magnitude in most countries in Asia
and the Pacific region. In South-America about 10% of
Bolivian street youth is using inhalants. Approximately
80% of all Bolivian youth is at risk of becoming serious
inhalant abusers, which could lead to tremendous social
problems. Abuse of volatiles is also prevalent in Brazil
(24%) [2] and Mexico (22%) [5]. The prevalence of volatile
substance abuse in Colombia was about 1.7% in 1995, while
prevalence appears to be lower in the general population but
substantially higher among marginalized children in Peru. In
the UK and in Oslo, respectively, about 4–10% and 10% of
youth used volatile substances at least once [3]. In Poland
volatile substance abuse is second after heroin and morphine
abuse [3], while about 20% of the total number of registered
drug users in Budapest (Hungary) are inhalant abusers [5]. A
variety of products present at home and on working places
contain substances that can be inhaled, e.g. paints, glues,
correction fluid and gasoline. Volatile organic compounds
are appealing because they are inexpensive, legal, readily
available and easily concealed. The effect (high) occurs and
disappears relatively quickly, which forms an additional
advantage. Abuse of solvents is mostly seen in disrupted
families, economically disadvantaged groups and ethnic
minorities [5–7]. Use is not gender specific, but sustained
abuse is more common among males and 90% of deaths are
men [3]. About 70% of deaths occur under the age of 20,
with the highest number between the age of 14 and 19
[1,3,5]. Of all deaths in teenagers 5% are due to volatile
substance abuse and nearly one third of deaths resulted from
first time use [7]. More than 50% of the deaths were caused
by direct toxic effects of the substance (sudden sniffing
death), notably cardiac toxicity and respiratory depression.
Other causes included plastic bag asphyxia (21%), aspiration
Forensic Science International 142 (2004) 135–156
* Corresponding author. Tel.: þ32-9-264-81-35;
fax: þ32-9-264-81-83.
E-mail address: [email protected] (W.E.E. Lambert).
0379-0738/$ – see front matter # 2004 Elsevier Ireland Ltd. All rights reserved.
doi:10.1016/j.forsciint.2004.02.015

of stomach contents (18%) and trauma due to dangerous
behaviour (11%) [8]. Mostly the abuse of volatile organic
compounds is rapidly abandoned, while some degree of
inhalant use on a lifetime basis is also common. Sometimes
initiation of inhalant use precedes multiple substance abuse
[6].
Although the ratio of deaths to nonfatal inhalation esca-
pades is extremely low, it is an important and potentially
preventable cause of death in young people [1].
1.2. Modes of use
To achieve high concentrations in the lungs and the brains
for intensified and prolonged euphoria different methods
such as ‘sniffing’ (inhalation from an open container or
heated pan), ‘bagging’ (inhalation from a plastic bag) or
‘huffing’ (inhalation by using a piece of cloth soaked in a
volatile substance) can be used. Even oral use such as
drinking or squirting directly into the mouth has been
reported [6,9].
1.3. Classification
Volatile substances of abuse can be classified based on
their chemical structure [2,10], pharmacological and beha-
vioural effects [11] or even on their commercial use. As the
analytics are an important issue in this particular review,
chemical classification is of most interest. The chemical
structure of a compound will affect the whole analytical
process, e.g. sample preparation, chromatographic separa-
tion and detection. Inhaled volatile substances fall into
several chemical families, notably hydrocarbons, oxyge-
nated compounds and halogenated compounds (Table 1).
The hydrocarbons can be subdivided into aliphatic hydro-
carbons such as propane, butane, gasoline and aromatic
hydrocarbons such as toluene, xylene and ethyl benzene,
while oxygenated compounds are subdivided in ethers,
esters, alcohols, nitrites and ketones. Nitrites, ‘poppers’,
are a class of products mostly used in dancing clubs and
in the gay-community to enhance sexual activity. The group
of the halogenated compounds is a mixture of products,
which include several anaesthetics.
1.4. Toxicity
Because of the abuse of a wide variety of inhalants it is not
surprising to find a tremendous range of acute and chronic
physical problems [6]. The lipid solubility and volatility of
the compounds enhance their toxicity. Due to the extensive
capillary surface area of the lungs [6] blood levels peak
already within a few minutes after exposure. Because of their
lipid solubility volatiles easily cross lipid membranes and
distribute to well-perfused organs such as brains, liver, heart
and kidneys [10]. This condition will be retained if sudden
death occurs, but if exposure continues the compound will
slowly accumulate in poorly perfused tissues such as muscle
and fat [2]. The toxicity of volatiles depends on the com-
pound itself and on the magnitude, duration and the route of
exposure. Abused inhalants have different mechanisms for
their toxicological effects [11]. The most important toxico-
logical effects are those observed for the heart, lungs, kidney,
neurological system, liver and bone marrow.
1.4.1. Cardiovascular toxicity
Cardiac arrest is the most common cause of sudden death
in volatile substance abuse. Mostly it is caused by cardiac
arrhythmias due to sensitisation of the myocard to catecho-
lamines following exercise, fright or sexual activity. Stimu-
lation of the nervus vagus, due to spraying aerosol
propellants in the mouth, may lead to inhibition of the heart
and subsequent bradycardiac arrest, which is another cause
of sudden death [3]. Myocardial ischemia caused by cor-
onary vasospasm has also been hypothesised as a mechan-
ism. When nitrites are used a vasodilatation and pooling of
blood into the extremities can cause orthostatic hypotension
and syncope [3].
1.4.2. Neurological toxicity
Because of their lipophilic character, volatiles have a
serious impact on the brain and other parts of the nervous
Table 1
Volatile organic compounds classification
Hydrocarbons Oxygenated compounds Halogenated compounds
Aliphatic Aromatic Esters Alcohols Ethers Ketones Nitrites Anaesthetics Other
Propane Toluene Isoamylacetate Butanol tert-Butylether Acetone n-Butylnitrite Desflurane Chloral hydrate
Butane Ethylbenzene Butylacetate Propanol Dimethyl ether Butanone Amylnitrite Sevoflurane Tetrachloro-ethylene
Neopentane Xylene Pentylnitrite Isoflurane Trichloro-ethylene
Heptane Benzene Enflurane Methylene-chloride
Hexane Halothane Difluoroethane
Pentane Bromochlorodifluoromethane
Ethylchloride
Dichlorodifluoromethane
Trichlorofluoromethane
Adapted from [2,10,12].
136 S.M.R. Wille, W.E.E. Lambert / Forensic Science International 142 (2004) 135–156

system, especially in chronic users. Most volatiles, espe-
cially anaesthetics, act as a central nervous system depres-
sant [13]. The neurotoxic effects of prolonged inhalant abuse
include neurological syndromes that reflect damage to parts
of the brain involved in controlling cognition, movement,
vision and hearing. Cognitive abnormalities can range from
mild impairment to severe dementia [4].
1.4.3. Pulmonary toxicity
Volatile substances may evoke sudden death through
asphyxiation or they can cause direct damage to the pulmon-
ary tissue. Asphyxiation can be caused by oxygen displace-
ment, aspiration of vomit or suffocation in the used plastic
bag. Respiratory arrest may be caused by central nervous
respiratory depression or by vagal stimulation. Direct damage
of the pulmonary tissue can lead to physiologic and anatomic
pulmonary abnormalities. These abnormalities can be caused
by fire-breathing (filling the mouth with (butane) gas and
igniting it while exhaling), metabolites of the products or by
the products themselves [3].
1.4.4. Nephrotoxicity, hepatotoxicity and bone marrow
toxicity
Chronic exposure can produce significant damage not only
to heart and lungs but also to the liver and kidneys. There are a
variety of renal disorders due to the used compound or as a
result of metabolic transformation. Although metabolism
normally results in detoxification, enhanced toxicity may
also result. Carbon tetrachloride, chloroform, dichloro-
methane, n-hexane, trichloroethylene and possibly halothane
can cause the formation of toxic metabolites [2]. Free radicals
originated from metabolism can lead to hepatotoxicity by
causing peroxidation of the hepatocyte cell membranes [10].
Bone marrow suppression is a result of chronic toxicity of
volatile substances (e.g. benzene) and leads to several hae-
matological changes while abuse of nitrite inhalants is asso-
ciated with methemoglobinemia [14]. Other problems such as
peripheral neuropathy, peri-oral eczema, burns and gastro-
intestinal problems by swallowing the products can also occur
[3,6].
1.5. Strategy
This review will discuss the analytical methods to detect
volatile substances in post-mortem samples such as blood,
heart, kidney, brain, liver and urine. Volatiles are a wide-
spread group of compounds that can be subdivided in related
chemical structures (Table 1). However, it is more relevant to
discuss the analytical methods rather than the different
compounds, because one analytical method mostly detects
several compounds.
Analysis of a sample can be based on direct detection of
the compound itself in blood or tissues such as heart, liver,
kidney and brain, but also on detection of metabolites,
especially in urine [14]. Blood is the most interesting matrix,
but due to their lipophilic character volatile organic com-
pounds are detected also easily in brain tissue. Due to its high
fat content the brain is a reliable source of sampling, and is it
is more resistant (unless there is a severe trauma) to post-
mortem decomposition [15].
Analysis of urinary metabolites may extend the detection
window of inhalant abuse. However, of the compounds
commonly abused only the metabolites of toluene, trichlor-
oethylene, xylene and benzene i.e. hippuric acid, trichlor-
oacetic acid, methylhippuric acid and phenol can be used
[2,14,56]. In post-mortem analysis, however, metabolites
seem less important. In literature, only chloral hydrate,
tetrachloroethylene and trichloroethylene metabolites seem
worth to analyse [28,49,50,52–54].
2. Storage and sample handling
In the analytical investigation of volatile substances
proper sample collection, storage and handling are impor-
tant, in view of the chemical properties and volatile nature of
the compounds. However, useful qualitative results can also
be obtained if the conditions for sample storage and handling
are less ideal [2].
Loss of the volatile substances by evaporation is one of
the main causes of difficulties in quantitative analytical
procedures. Therefore analysis of the sample should start as
soon as possible. Volatile substances diffuse from the
sample into the atmosphere until equilibrium is reached.
Every time the container is opened, losses occur due to the
replacement of air. Losses may also occur if an aliquot of
the sample is taken without opening the container (piercing
through the septum) due to negative pressure, which will be
revealed after introduction of air. Every time fresh air
comes inside the container, diffusion of the compounds
will create a new equilibrium. Samples should therefore be
stored in gas-tight, good sealed containers with minimal
headspace. Addition of an internal standard to the sample
immediately after autopsy will minimise experimental
errors due to evaporation during storage or tissue homo-
genisation [16]. A good seal also protects the sample
against contamination from environmental and laboratory
sources of volatiles [17–19]. Storage, transport and hand-
ling of the sample should always occur at approximately�5
till 4 8C. Lower temperatures should be avoided for long-
term blood sample storage due to formation of n-hexanal
from degradation of fatty acids. n-Hexanal often leads to
interferences in the analysis of low toluene levels [20],
however, in intoxication cases the contribution remains
limited. Samples should only come in contact with inert
materials such as glass, teflon or aluminium foil. Soft
rubber stoppers should be avoided due to their high affinity
and permeability for toluene [21].
For non-post-mortem blood samples an anticoagulant
(lithium heparin) is required [19]. Tubes containing EDTA
and gel-separators should be avoided as false positive
results for xylene, ethylbenzene, toluene and 1-butanol
S.M.R. Wille, W.E.E. Lambert / Forensic Science International 142 (2004) 135–156 137

have been reported due to the presence of gel-separators,
while 1-butanol and 2-methyl-2-propanol have been
demonstrated in tubes coated with EDTA [19,22]. Addition
of sulphuric acid or sodium fluoride [2,20] is advised when
esters such as ethyl acetate are present in the sample to
abolish esterase activity. Sodium azide prevents growth of
micro-organisms [2,14,18,19,23].
3. Analytical techniques
3.1. Introduction
Volatile organic compounds are generally determined by
gas chromatography resulting in qualitative as well as
quantitative data. First, sampling, introduction of the sample
and the analytical separation will be discussed. Thereafter
the detection of the compounds will receive attention.
3.2. Sampling and introduction into the analytical column
3.2.1. Extraction techniques [16,23]
Today, sample handling and introduction aim to increase
sample load and thus sensitivity. It should be simple, effi-
cient, inexpensive and minimize the use of chemicals [24].
Therefore, headspace techniques have become very popular
in the past years. The headspace technique can be divided in
two modes: the static mode (headspace and variants (HS)
such as solid phase microextraction (HS-SPME), cryogenic
oven trapping (HS-COT), cryogenic focusing (HS-CF)) and
the dynamic mode, also referred to as purge and trap [16].
Other extraction techniques are pulse-heating and solvent
extraction. Modifications of ‘traditional’ headspace are
introduced to enhance sensitivity by concentration effects
(SPME) or increase of the volume injected into the column
(COT/CF). Changes are also made to improve quantification
by elimination of matrix effects (HS-multiple headspace
(MHE), HS-full evaporation technique (FET) and standard
addition (SAM)). These modifications will be discussed later
(see quantitation modes). Headspace techniques all have the
advantage of avoiding contamination of the chromato-
graphic system by non-volatile substances originating from
the sample matrix [25,26].
3.2.1.1. Static headspace (HS). The static mode refers to
partition and eventually equilibrium of the analyte between
the sample and the gas phase in a closed system. After
equilibrium is achieved, the vial is pressurised and an aliquot
of headspace air is sampled and injected into the gas
chromatograph. The headspace procedure is simple, mini-
mises the number of artefacts during analysis and can
measure water soluble compounds effectively. It is, however,
less sensitive for highly water soluble compounds [16]. If the
sample is a liquid, such as blood, urine or gastric content,
complete equilibrium is obtained relatively easy. The sam-
ple, mostly after addition of distilled water and an internal
standard solution, is heated for a period of time. Agitation of
the sample and addition of salt may be used to accelerate
evaporation. After heating, an aliquot of headspace air is
injected in the column either manually (needle) or with an
autosampler and injection loop. Tissues such as liver, kidney,
adipose tissue, lungs and brain are suitable matrices for the
determination of volatile organic compounds in post-mor-
tem sampling. They are analysed by following the same
procedures as the liquid samples. Sometimes, as in the
analysis of bromochlorodifluoromethane, butane and a
few other components, the tissues are treated with a pro-
teolytic enzyme such as Subtilisin A [20]. Homogenisation
using an Ultra-Turrax may also be necessary [27,28]. To
avoid evaporation of the compounds, homogenisation should
always occur at low temperature and in closed containers
[16] (Table 2).
3.2.1.2. HS-chemical (HS-c). El-Haj et al. [29] described a
chemical transformation of toluene and ethyl benzene to
relatively non-volatile products to overcome interferences in
the detection with flame ionisation detection (FID) or Four-
ier transform infrared detection (FTIR). Benzotrichloride is
almost quantitatively formed when toluene reacts with
chlorine gas under UV-light exposure. In the presence of
water, it is converted to benzoic acid and hydrochloric acid.
Under UV-light and in the presence of water ethyl benzene
reacts with chlorine to form benzoic acid, 1- and 2-phenyl
ethanol.
After addition of sodium chloride, headspace was per-
formed and 10 ml of headspace gas was introduced into a
chlorine gas containing vial. This was placed in the sun for
10 min and after addition of water and an evaporation step,
BSTFA (N,O-bis trimethylsilyl trifluoroacetamide) was
added. After heating the sample, an aliquot was injected
(Fig. 1).
3.2.1.3. HS-solid phase microextraction (HS-SPME). Solid
phase microextraction is a sampling and concentration
technique based on the principle of ‘likes dissolves likes’,
thus the affinity of the compound for a fibre and partitioning
of analytes between the solid phase (fibre) and the matrix
[30]. Sorption modes are direct immersion and headspace
sampling. The main considerations for mode selection are
the nature of the sample matrix, the analyte’s volatility and
the affinity for the matrix [31]. Direct immersion of the fibre
into the sample is not relevant here due to the physicochem-
ical characteristics of the analytes discussed in this review.
The time and temperature of conditioning, extraction and
desorption can vary. An overview of typical conditions is
given in Table 3. The most applied fibre is coated with a 100-
mm polydimethylsiloxane phase (PDMS) for absorption of
apolair compounds such as toluene and halothane. A poly-
acrylate 85-mm fibre was used for absorption of hydrolysed
n-butylnitrite [24,32] to overcome specific problems of
extracting polar analytes from a polar matrix. One case
described the use of a Carboxen/PDMS (75 mm) fibre to
138 S.M.R. Wille, W.E.E. Lambert / Forensic Science International 142 (2004) 135–156

Table 2
Analytical data for HS extraction
Reference Matrix Compounds Add./IS HS time
(min)
HS temp.
(8C)
Inj. Comments Inj. vol. (ml)
[20] Blood, urine,
tissue
Bromochlorodifluoromethane,
butane, FC11, FC12, isobutane,
propane, dimethylether
Tissue: Subtilisin A
IS: ethylbenzene,
1,1,2-trichloroethane
15 65 Manual Warm needle (10 min on
heating block)
0.10–0.30
[25] Blood Isoflurane IS: 1,4-dioxane 30 55 Autosampler Needle temperature: 120 8C 1.0
[32] Urine, gastric
content
Methylene chloride, volatile
petroleum contents, (ethanol)
Sodium chloride
(urine), IS: t-butanol
20 60 Manual 0.250
[40] Blood Hydrocarbons IS: toluene d8, cold water 20 60 Manual 2
[42] Blood Halothane, enflurane, isoflurane,
sevoflurane
IS: dichloromethane 15 55 Manual 1
[43] Blood Hydrocarbons, esters, aldehydes,
ketones, ethers, (alcohols)
Potassium fluoride,
sodium chloride
33 50 Autosampler Valve/loop temperature: 54 8C,
Aux. gas pressure: 130 kPa,
vial pressurisation time: 15 s,
carrier gas: He 70 ml/min
1
[58] Blood, lung,
gastric content,
urine, bile, brain,
liver, kidney,
vitreous humor
Methyl-2-pentane,
methyl-3-hexane,
methylcyclohexane, heptane
20 80 Autosampler Needle temperature: 90 8C,
loop temperature: 100 8C, vial
pressurisation time: 2 min,
carrier gas: He 10 psi,
pressurisation pressure: 17 psi
0.070
[59] Blood Desflurane, sevoflurane,
isoflurane, enflurane, halothane
Anticoagulant, IS:
1,4-dioxane
Autosampler
[63] Blood, urine,
tissue
Ethylchloride Sodium chloride,
IS: 1-propanol
5 37 0.7
[64] Blood, brain,
lung, liver, spleen,
kidney, muscle,
adipose tissue
Enflurane Distilled water,
IS: 1,4-dioxane
30 55 Autosampler Vial pressurisation time:
0.13 min, pressurisation:
124 kPa, transferline and loop
temperature: 100 8C, loop fill
time: 0.15 min, injection
time: 0.20 min, loop
equilibration time: 0.15 min
1
[65] Blood, urine Toluene Sodium citrate solution, IS:
isobutanol
20 55 Autosampler 0.250
[66] Blood, urine Difluoroethane IS: 1-propanol 15 37 Manual 0.3
[67] Blood, brain, lung Propane Fluoride (blood) Manual 0.5
[68] Blood, urine, lung Diethylether, hydrocarbons Sodium chloride 26 80 Autosampler Valve/loop temperature: 85 8C,
Aux. gas pressure: 130 kPa,
vial pressurisation time: 15 s,
sample loop V: 1 ml, vent loop
fill time: 1 s, injection time: 2 min
[69] Blood Hydrocarbons Cold water, IS 20 60 Manual
[70] Blood, urine Toluene Sodium citrate solution,
shaken, IS: 1,4-dioxane
20 60 Autosampler Valve and transferline
temperature: 140 8C1.0
S.M
.R.
Wille,
W.E
.E.
La
mb
ert/Fo
rensic
Scien
ceIn
terna
tiona
l1
42
(20
04
)1
35
–1
56
13
9

Table 2 (Continued )
Reference Matrix Compounds Add./IS HS time
(min)
HS temp.
(8C)
Inj. Comments Inj. vol. (ml)
[74] Brain, liver,
lung, blood
Chlorodifluoromethane IS: genetron 502, shaken 60 RT
[75] Heart, lung, brain,
liver, blood,
spleen, kidney
Trichlorofluoromethane IS: dichloromethane 30 40 Manual
[76] Blood, lung Methylchloroform 60 20
[77] Blood, brain, heart Dichloromethane, chloroform NaCl, IS: sec-butanol 20 55 0.250
Metabolites
[28] Blood, tissue Tetrachloroethylene,
trichloroethylene,
trichloroacetic acid
IS: chloroform
[52] Blood, lung,
liver, kidney,
stomach content
Trichloroethylene,
trichloroacetic acid
IS: n-butanol, NaCl,
water, vortex, sonication
35 80 Autosampler Loop temperature: 110 8C,
transferline temperature 120 8C
HS quantification
[44] Blood, tissue Acetone, 2-propanol, 2-butanone,
tert-butylether, benzene, toluene,
ethylbenzene, propyl-benzene,
o-, p-, m-xylene
28 130 (FET),
80 (MHE)
Aux. gas pressure: 210 kPa, not
more than 10 mg of compound
HS chemical
[29] Blood Toluene, ethylbenzene Distilled water 3–5 65 2
HS followed by COT
[35] Blood, urine Ethylacetate, benzene, butan-1-ol,
toluene, butylacetate, isoamyl-
acetate (¼thinner components)
Distilled water, stirring
bar, heparin sodium (in
blood), IS: ethylbenzene
30 90 Manual 5
[39] Blood o-, m-, p-Xylenes Distilled water,
IS: aniline
30 100 Manual 2
[60] Blood, lung Propane, isobutane, butane,
neopentane, n-pentane,
bromochlorodifluoromethane
10 50 0.100–0.250
[61] Blood Sevoflurane, isoflurane,
enflurane, halothane
Distilled water,
IS: halothane
15 55 Manual 10
[62] Blood Chloroform, methylene chloride Distilled water,
IS: methylenechloride,
chloroform
20 55 Manual 5
HS followed by Tenax-trap
[37] Blood n-Propane, isobutane, n-butane IS: t-butyl-methyl ether 20 60 Autosampler,
Tenax-trap
Vial pressurisation time: 1 min 0.5
Abbreviations: Add., addition to headspace vial; IS, internal standard; HS time, headspace heating time; Aux., auxiliary; HS temp., headspace heating temperature; FET, full evaporation
technique; Inj., injection mode; MHE, multiple extraction method; Inj. vol., injection volume; RT, room temperature.
14
0S
.M.R
.W
ille,W
.E.E
.L
am
bert/F
oren
sicS
cience
Intern
atio
na
l1
42
(20
04
)1
35
–1
56

extract chloroform and methylene chloride from blood and
urine [73].
The extraction can be accelerated by agitation, addition of
salts or through heating (the rate of absorption decreases,
while the rate of release increases with higher temperature)
[30]. In case of highly volatile compounds equilibration
times are short even without agitating [33].
SPME can be applied to small sample volumes and is a
solvent-free, simple and rapid technique [15]. There is no
intense air peak in the chromatogram often observed
with headspace direct injection [30]. The clean extracts
enhance reproducibility [32], selectivity [31] and sensitiv-
ity [30].
However, the absorption capacity is more sensitive for
highly volatile and low molecular mass compounds. Some-
times a cooling device is applied to create better peak shapes
[34], thereby combining SPME and cryogenic oven trapping
[24,34].
3.2.1.4. HS-cryogenic trapping (HS-COT, HS-CF). HS-
cryogenic trapping is a combination of HS or HS-SPME
and a low temperature of the whole column (COT) or the
sample-introduction region at the inlet of the column (CF) to
trap volatile organic compounds [35]. A microcomputer-
controlled device can lower the oven temperature to less than
0 8C with use of liquid carbon dioxide or liquid nitrogen.
Fig. 1. Extracted ion chromatogram (A) and EI mass spectrum (B) of the TMS derivative of the benzoic acid obtained from the reaction of
headspace of a blood sample obtained from a glue abuser with chlorine/sunlight and then water. The molecular ion mass of 194 and the base
peak ion mass of 179 were used in the extraction of chromatogram. Source: [29] Fig. 4 (p. 393).
S.M.R. Wille, W.E.E. Lambert / Forensic Science International 142 (2004) 135–156 141

Table 3
Analytical data for HS-SPME extraction
Reference Matrix Compounds Cond. time/temp. HS time/temp. Ad. time/temp. Desorp. time/temp. Fibre Add.
[15] Blood, lung,
brain, fat
VOC, incl xylene, butane,
halothane, toluene,
petroleum residues
5 min/200 8C 1.5 h/80 8C 30 min/– 1 min/220 8C 100 mm PDMS Distilled water,
IS: cyclohexanone
[27] Blood, urine,
tissues
Tetrachloroethylene,
trichloroethylene,
trichloroacetic acid
5 min/60 8C 1 min/60 8C 15 s/250 8C 100 mm PDMS Ultra Turrax, IS:
carbontetrachloride
[32] Urine, gastric
contents
Methylenechloride,
volatile petroleum
products (ethanol)
5–10 min/260 8C 20 min/60 8C 10 min/60 8Curine, 5 min/
60 8C gastric
1 min/225 8Curine, 1 min/
250 8C gastric
100 mm PDMS,
85 mm PA
Sodium chloride in
urine, IS: t-butanol
[70] Blood, urine Toluene 20 min/60 8C 1 min/60 8C 1 min/250 8C 100 mm PDMS 0.1% sodium azide,
shaken (rpm 85), IS:
1,4-dioxane,
(iso-butanol)
[71] Blood, urine Thinner components:
toluene, benzene,
n-butylacetate, n-butanol,
n-isoamylacetate
1 h/250 8C 15 min/80 8C 5 min/80 8C 3 min/200 8C 100 mm PDMS Distilled water,
magnetic stirring bar,
IS: ethylbenzene
[72] Blood, liver,
kidney, brain,
urine, bile,
stomach contents
Halothane, isoflurane,
chloroform, diethylether
1 h/250 8C 15 min/100 8C 15 min/100 8C 2 min/250 8C 100 mm PDMS Ammonium
sulphate, sulphuric
acid solution
[73] Blood, urine Chloroform,
methylene chloride
10 min/30 8C 20 min/30 8C 2 min/240 8C 75 mm carboxen/
PDMS
Distilled water,
shaken 10 s IS:
methylene chloride,
chloroform
SPME followed by COT
[24] Blood, urine Hydrolysed n-butyl-nitrite 30 min/155 8C 1–3 h/20-23 8C 5–20 min/60 8C 1 min/240 8C 100 mm PDMS,
85 mm PA
IS: n-propanol
[34] Blood Hydrocarbons 2 min/�5 8C 300/�5 8C 3 min (1 min
sampling)/250 8C(2 min purging)
100 mm PDMS VOC-free water,
IS: toluene d8
Abbreviations: SPME, solid phase micro extraction; Ad. time, adsorption time; Cond. time, conditioning time; Ad. temp., adsorption temperature; Cond. temp., conditioning temperature;
Desorp. time, desorption time; HS time, headspace time before fibre introduction; Desorp. temp., desorption temperature; HS temp., headspace temperature; Add., addition in headspace vial;
VOC, volatile organic compounds; PA, polyacrylate; PDMS, polydimethylsiloxane.
14
2S
.M.R
.W
ille,W
.E.E
.L
am
bert/F
oren
sicS
cience
Intern
atio
na
l1
42
(20
04
)1
35
–1
56

The temperature needed to trap the volatiles, depends on the
volatile in question [36] (Table 4). While in the headspace
technique only a maximum of 1 ml of headspace air could
be injected into narrow bore columns in the split mode,
injection of 2 till 10 ml of the headspace air was described
for medium bore columns in the splitless mode without any
loss using the HS-COT method [36] (Fig. 2).
Cryogenic trapping is more than ten times more sensitive
than SPME due to higher possible sample load and better
peakshape [36]. When carbon dioxide is used to cool the
column, one has to be aware of the danger for suffocation
due to large carbon dioxide leaks [36].
Not always the whole column is cooled (CF). Bouche et al.
[37] have described the determination of n-propane, n-
butane and isopropane in post-mortem blood by combination
of static HS with cold trapping on a Tenax sorbent followed
by flash desorption to enhance sensitivity, while Tytgat and
Daenens [24] cooled the inception of the column with liquid
carbon dioxide using SPME as extraction method for hydro-
lysed n-butyl nitrite.
3.2.1.5. Headspace dynamic mode: purge and trap. The
dynamic mode is accomplished by purging a carrier gas
constantly above the sample and trapping the evaporated
volatiles in a cryogenic and/or adsorbent trap [16,23].
Extensive heating afterwards releases the analytes from
the trap into the column. The dynamic procedure is effec-
tive for compounds with moderate to high water solubility
and the concentration step, ‘the trapping’, enhances sensi-
tivity. It is, however, difficult, costly and artefacts due to
impurities in the purging gas occur. Attention has to be paid
to contamination of the trap and to occurrence of leaks
[24]. Precise quantification suffers from incomplete recov-
ery after purging, trapping and desorption [16]. Recoveries
are increased by heating the sample and increasing purge
time [26]. For apolar compounds such as toluene lower
detection limits are obtained than for polar ones (propanol,
acetone, isopropanol) partly due to the fact that purging
and trapping of polar compounds is less efficient [38].
Although Watanabe-Suzuki and co-workers [36,39] sug-
gest that the purge-trapping technique is not suitable for
biological samples due to foaming, it seems to offer better
recoveries and lower detection limits in the analysis of
volatile organic compounds as compared to headspace
extraction [26]. Ojanpera et al. even applied the technique
to the analysis of tert-butylmethyl ether and 1,1,2-trichlor-
oethene in post-mortem blood samples after addition of
Antifoam B emulsion. A purge-trap concentrator equipped
with a cooled Tenax-trap (2,6-diphenyl-p-phenylene oxide
polymer) was used [38]. Despite the relatively low specific
surface area of the Tenax-trap, it has a high sorption
capacity and thermal stability. The retention of water is
relatively small, thus it is possible to trap compounds
efficiently from water saturated headspace gases [23].
Water can cause problems, especially if a cryogenic trap
is used. Morinaga et al. [40] described a purge and trap
method with a Tenax TA-trap combined with a dehydrata-
tion agent Chromosorb G for the analysis of toluene,
benzene, xylenes and ethylbenzene in blood. Tenax-traps
can also be used in combination with static headspace as
described by Bouche et al. [37] (Table 5).
3.2.1.6. Solvent extraction. Although headspace and solid
phase microextraction are the most commonly used sam-
pling techniques over the past few years, solvent extraction
is used for chloral hydrate, trichloroethylene and their
metabolites. Solvent extraction, however, is time consum-
ing, laborious and more difficult to automate. Interferences
Table 4
Analytical data for HS-COT/CF extraction
Reference Matrix Compounds Extr. method Cooling gas Oven temp. (8C) Comments
[24] Blood, urine Hydrolysed n-butyl nitrite SPME Liquid CO2 �5 to 5 inception
of the column
[34] Blood Hydrocarbons SPME Liquid CO2 �40
[35] Blood, urine Ethyl acetate, benzene,
butan-1-ol, toluene, butyl
acetate, isoamyl-acetate
HS Liquid CO2 5
[37] Blood n-Propane, n-butane,
isopropane
HS þ Tenax Liquid N2 �80 cooled
inlet-liner
(Tenax-trap)
Tenax-trap heated
to 200 8C for
6 min
[39] Blood o-, m-, p-Xylenes HS Liquid CO2 5
[60] Blood Propane, butane, isobutane HS NS 0–10
[61] Blood Sevoflurane, isoflurane,
enflurane, halothane
HS NS �40
[62] Blood Chloroform, methylene
chloride
HS Liquid CO2 �30
Abbreviations: HS-COT, headspace cryogenic oven trapping; Extr. method, extraction method; HS-CF, headspace cryogenic focussing; Oven
temp., oven temperature; HS, headspace; SPME, solid phase microextraction; NS, not specified.
S.M.R. Wille, W.E.E. Lambert / Forensic Science International 142 (2004) 135–156 143

Fig. 2. Left: Schematic diagram of the instrumentation used for cryogenic oven-trapping (COT)-capillary GC (A) and for cryo-focusing (B).
The COT conditions for analysis of chloroform or dichloromethane are shown. For cryo-focusing the chamber can be cooled to �180 8C(minimum) with gas from liquid N2 and down to �90 8C with gas from liquid CO2. Right: Headspace capillary GC for chloroform (peak 2)
and dichloromethane (peak 1) as a function of initial oven temperature. Each compound (5 mg) was added to 0.5 ml human whole blood for
headspace extraction. Source: [36] Fig. 1 (p. 76), Fig. 2 (p. 78).
144 S.M.R. Wille, W.E.E. Lambert / Forensic Science International 142 (2004) 135–156

Table 5
Solvent-, pulse-heated purge and trap extraction
Reference Matrix Compounds Add./IS Extraction
liquid
Vortex
time
Centrifuge
Solvent extraction
[49] Blood, liver,
kidney, stomach
contents
Chloral hydrate,
trichloroethanol,
trichoroacetic acid
Water, sulphuric
acid, IS: 1,3
dichloro-2-propanol
Diethylether 2 min 10 min,
2500 � g
[50] Blood, urine,
stomach content
Chloral hydrate,
trichloroethanol
IS:
tetrachloroethylene
Chloroform 30 s 30 s,
10000 rpm
[53] Blood, liver,
kidney, lung,
stomach contents
Trichloroethylene,
trichloroethanol,
trichloroacetic acid
Water, sulphuric
acid, IS: 1,3
dichloro-2-propanol
Diethylether 2 min 10 min,
2500 � g
[54] Blood, urine Trichloroethanol
(chloral hydrate,
trichloroacetic acid)
Diethylether 3 min 4 min,
2500 rpm
Reference Matrix Compounds Add./IS Heating
time (s)
Ferromag.
cond. temp.
Oven
temp. (8C)
Needle
temp. (8C)
Pulse-heated extraction
[42] Blood Halothane, enflurane,
isoflurane, sevoflurane
4 160 170 200
Reference Matrix Compounds Add./IS Gas flow
(ml/min)
Purge time
(min)
Dry purge
time (min)
Line/valve
temp. (8C)
Trap Extraction
temp. (8C)
Trap
temp. (8C)
Desorption
time/temp.
Sample
P (kPa)
Trap
P (kPa)
Purge-trap extraction
[38] Blood Aceton, isopropanol,
1-propanol,
1,1,1-trichloro-ethane,
isoflurane, diethylether,
tert-butanol, toluene,
isobutylmethylketone,
ethylacetate
Antifoam b He 35 10 6 Tenax
1/8 in. � 12 in.
�20 4 min/
225 8C140 40
[40] Blood Hydrocarbons Cold water,
IS: toluene d8
N2 500 Tenax TA
(60/80 mesh)
40 220 8C
[57] Blood 27 VOC’s Antifoam b, NaF,
IS: diethylketone
He 38 15 6 150 Tenax
1/8 in. � 12 in.
Room
temperature
�20 2 min/
225 8C140 50
Abbreviations: Add., addition; Ferromag. cond. temp., ferromagnetic conduction time; temp., temperature; IS, internal standard.
S.M
.R.
Wille,
W.E
.E.
La
mb
ert/Fo
rensic
Scien
ceIn
terna
tiona
l1
42
(20
04
)1
35
–1
56
14
5

in the chromatographic run can occur because of co-extrac-
tion of non-volatiles or due to the solvent front [16]. Precise
determination, especially of low boiling compounds, cannot
be expected [16] (Table 5).
3.2.1.7. Pulse-heating. Although post-mortem relevance
was not quite clear in the cited reference [26], pulse-heating
can be a possible detection method for volatiles such as
anaesthetics in post-mortem samples. Alcohol is not dis-
cussed in this review, however, pulse-heating was used for
the determination of alcohol in post-mortem blood, urine
and synovial fluid [41]. Pulse-heating of a biological sample
is performed by a curie point pyrolyser, which is a ferro-
magnetic coil quickly heated up by electromagnetic induc-
tion [26]. After introduction and heating of the sample in the
pyrolyser, volatiles can evaporate from the matrix directly
into the column, without interference of the macromolecules
present in the matrix. Advantages include the small sample
volume needed, short extraction time and especially the
elimination of matrix effects [26,42] (Table 5).
3.2.2. Sample introduction
The sample is mostly introduced in the splitless mode
because of the higher sensitivity as compared to the split
mode. However, also split and programmed temperature
vaporisation (PTV) are possible injection modes.
3.3. Separation
3.3.1. Columns
At first, packed columns were used to determine volatile
compounds [16]. Currently, almost all laboratories use
capillary columns due to practical advantages and improved
sensitivity (partially caused by a new sample introduction),
efficiency, reproducibility and reliability [20]. Therefore we
only discuss analytical methods using capillary columns. In
capillary columns the length, film thickness and stationary
phase all influence the retention and separation of the
compounds. The phases used (Table 6) vary from polar
(polyethylene glycol) to apolair (dimethylpolysiloxane),
due to the broad range of polarity (e.g. toluene versus
acetone) of the target compounds. The length is mostly
30 m, but can vary depending on separation requirements.
Increase of column length results in better resolution, but
also in an increased runtime and column bleed, which causes
lower sensitivity.
Volatiles are analysed on columns with film thickness
between 0.25 and 10 mm. On the latter, volatiles are retained
longer resulting in an enhanced resolution. However, also a
higher column bleed occurs. When selecting the internal
diameter of the column (0.25, 0.32 or 0.53 mm), attention
has to be paid to different aspects. The maximum sample
volume that can be loaded depends on the film thickness and
the column internal diameter. The smaller the diameter, the
faster the analysis and the better the resolution. A 0.25-mm
internal diameter is advised for MS use.
3.3.2. Temperature programme
The temperature programme is either isothermal or
(mostly) programmed depending on the number and the
type of compounds to be separated (Table 6).
3.4. Detection
Usually electron capture detection (ECD), flame ionisa-
tion detection and mass spectrometry (MS) (SIM-mode)
are used for quantitation purposes, while MS an Fourier
transform infrared are used for identification purposes
(Table 6).
3.4.1. Non-spectral techniques
3.4.1.1. ECD. Electron capture detection is applied for
compounds with high electron affinities such as halogenated
substances and compounds containing nitro- and keto-func-
tions: e.g. bromochlorodifluoromethane, trichloroethylene,
hexane-2,5-dione and amylnitrite. ECD is very sensitive, but
has a more narrow linear range as compared to FID [20].
3.4.1.2. FID. Flame ionisation detection is sensitive to
hydrocarbons in general. It has a wide linear range and
excellent baseline stability. As seen in Fig. 3, the selectivity
and sensitivity of detection largely depends on the com-
pound and detection technique used (ECD versus FID).
3.4.2. Spectral techniques
3.4.2.1. MS. Although low molecular compounds often give
less specific mass spectra due to background interferences
and similar spectra of related compounds (e.g. butane and 2-
methylpropane, Fig. 4A), GC–MS has become very popular
to detect volatile organic compounds. It is applied for
screening with identification based on relative retention
and spectral information, and for quantitation, especially
in the single ion monitoring (SIM) mode [43].
3.4.2.2. FTIR. FTIR often gives more informative spectra
especially for low molecular weight compounds (e.g.
butane, acetone, ethylacetate, Fig. 4B) but sensitivity is
lower and interferences due to water and carbon dioxide
can be troublesome [20].
3.5. Quantitation
Determination of the initial concentration of volatiles in
the sample matrix can be done through the measurement of
the equilibrated vapour phase concentration and the partition
coefficient.
However, the most common method for quantitation is
based on standard calibration curves and internal standardi-
sation [16]. The interaction of analytes with matrix compo-
nents can result in binding of the volatile organic compounds
thus becoming unavailable for determination in the gas
146 S.M.R. Wille, W.E.E. Lambert / Forensic Science International 142 (2004) 135–156

Table 6
Analytical data of separation and detection modes
Reference Matrix Compounds Extr.
method
Inj. temp.
(8C)
Inj. M Inj. vol. Column Gas
flow
Oven Detector Det.
limit
Quant.
limit
Derivat.
[20] Blood, urine,
tissue
Bromochlorodifluoromethane
butane, FC11, FC12,
isobutane, propane,
dimethylether (224 comp)
HS 150 Splitless 0.10–
0.30 ml
SPB-1, 60 m �0.53 mm � 5 mm
He
8.6 cm3/
min
40 8C (6 min)–5 8C/
min!80 8C;
80 8C–10 8C/
min!200 8C
FID/ECD
[25] Blood Isoflurane HS 100 Split
1:30
1.0 ml DB 5, 30 m �0.25 mm �0.25 mm
He 40
cm/s
35 8C (1.4 min)–
40 8C/min!80 8C(2 min)
MS 1.2 mg/ml 4.7 mg/ml
[28] Blood, tissue Tetrachloroethylene,
trichloroethanol,
trichloroacetic acid
HS 150 ECD: WCOT
SPSIL5CB,
25 m � 0.53 mm
N2 3 ml/
min
ECD: 65 8C(2 min)–10 8C/
min!130 8C(1.5 min)
ECD 0.25 mg/ml 0.36 mg/m1 BSTFA
MS: BP20, 25 m �0.22 mm � 0.25 mm
MS: 45 8C–10 8C/
min!200 8CMS
[42] Blood Halothane, enflurane,
isoflurane, sevoflurane
HS 120 1 ml DB 1, 30 m �0.53 mm � 5 mm
He
15 ml
/min
Isothermal: 60 8C MS
PH 170 GS-Q-GC, 30
mm � 0.53 mm
Isothermal: 160 8C 0.2 mg/ml
[43] Blood Hydrocarbons, esters,
aldehydes, ketones, ethers,
(alcohols)
HS 60 Split 1 ml DB 1, 30 m �0.25 mm � 0.1 mm
He
18 m1/
min
40 8C (4 min)–
10 8C/min!200 8C,
200 8C–50 8C/
min!250 8C
MS-ITD 0.03 till
0.74 mmol/l
[44] Blood, tissue Acetone, 2-propanol,
2-butanone, tert-butylether,
benzene, toluene,
ethylbenzene, propyl-benzene,
o-, p-, m-xylene
HS
(FET,MHE)
35 mg
150 DB 1, 30 m �0.25 mm � 1 mm
MS-ITD 0.4–1 nmol polar
voc (blood),
0.03–0.1 nmol
nonpolar (brain)
[52] Blood, lung,
liver, kidney,
stomach
content
Trichloroethylene,
trichloacetic acid
HS 220 2 ml 100%
dimethylsilicone,
30 m � 0.32 mm
� 1.0 mm
He
51713 Pa
40 8C (12 min)
20 8C/min!2408 C
MS
140 DB 1301, 30 m �0.53 mm � 1 mm
He
27580 Pa
FID
[58] Blood, lung,
gastric
content, urine,
bile, brain,
liver, kidney,
vitreous humor
Methyl-2-pentane,
methyl-3-hexane,
methylcyclohexane,
heptane
HS Splitless 0.070 m1 624CB, 30 m �0.25 mm
35 8C (5 min)–
15 8C/min!150 8C (5 min)
MS 0.0005 mg/ml
(blood,
heptane)
[59] Blood Desflurane,
sevoflurane, isoflurane,
enflurane, halothane
HS 100 Split
1:30
XTI-5, 60 m �0.25 mm �0.24 mm
He
40 cm/s
35 8C (3.5 min)–
40 8C/min!120 8C (0.68 min)
MS 1 mg/ml Below
10 mg/ml
[63] Blood, urine,
tissue
Ethylchloride HS 250 0.7 m1 Innowax, 15 m �0.25 mm � 0.5 mm
He 1.05
ml/min
Isothermal: 50 8C FID
S.M
.R.
Wille,
W.E
.E.
La
mb
ert/Fo
rensic
Scien
ceIn
terna
tiona
l1
42
(20
04
)1
35
–1
56
14
7
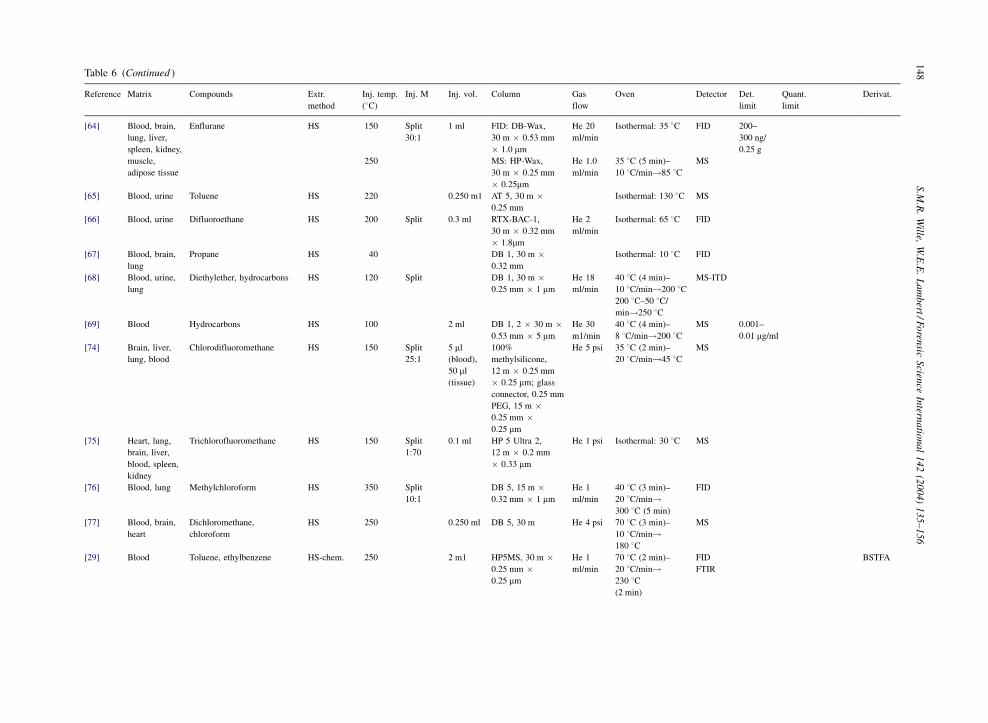
Table 6 (Continued )
Reference Matrix Compounds Extr.
method
Inj. temp.
(8C)
Inj. M Inj. vol. Column Gas
flow
Oven Detector Det.
limit
Quant.
limit
Derivat.
[64] Blood, brain,
lung, liver,
spleen, kidney,
muscle,
adipose tissue
Enflurane HS 150 Split
30:1
1 ml FID: DB-Wax,
30 m � 0.53 mm
� 1.0 mm
He 20
ml/min
Isothermal: 35 8C FID 200–
300 ng/
0.25 g
250 MS: HP-Wax,
30 m � 0.25 mm
� 0.25mm
He 1.0
ml/min
35 8C (5 min)–
10 8C/min!85 8CMS
[65] Blood, urine Toluene HS 220 0.250 m1 AT 5, 30 m �0.25 mm
Isothermal: 130 8C MS
[66] Blood, urine Difluoroethane HS 200 Split 0.3 ml RTX-BAC-1,
30 m � 0.32 mm
� 1.8mm
He 2
ml/min
Isothermal: 65 8C FID
[67] Blood, brain,
lung
Propane HS 40 DB 1, 30 m �0.32 mm
Isothermal: 10 8C FID
[68] Blood, urine,
lung
Diethylether, hydrocarbons HS 120 Split DB 1, 30 m �0.25 mm � 1 mm
He 18
ml/min
40 8C (4 min)–
10 8C/min!200 8CMS-ITD
200 8C–50 8C/
min!250 8C[69] Blood Hydrocarbons HS 100 2 ml DB 1, 2 � 30 m �
0.53 mm � 5 mm
He 30
m1/min
40 8C (4 min)–
8 8C/min!200 8CMS 0.001–
0.01 mg/ml
[74] Brain, liver,
lung, blood
Chlorodifluoromethane HS 150 Split
25:1
5 ml
(blood),
50 ml
(tissue)
100%
methylsilicone,
12 m � 0.25 mm
� 0.25 mm; glass
connector, 0.25 mm
He 5 psi 35 8C (2 min)–
20 8C/min!45 8CMS
PEG, 15 m �0.25 mm �0.25 mm
[75] Heart, lung,
brain, liver,
blood, spleen,
kidney
Trichlorofluoromethane HS 150 Split
1:70
0.1 ml HP 5 Ultra 2,
12 m � 0.2 mm
� 0.33 mm
He 1 psi Isothermal: 30 8C MS
[76] Blood, lung Methylchloroform HS 350 Split
10:1
DB 5, 15 m �0.32 mm � 1 mm
He 1
ml/min
40 8C (3 min)–
20 8C/min!300 8C (5 min)
FID
[77] Blood, brain,
heart
Dichloromethane,
chloroform
HS 250 0.250 ml DB 5, 30 m He 4 psi 70 8C (3 min)–
10 8C/min!180 8C
MS
[29] Blood Toluene, ethylbenzene HS-chem. 250 2 m1 HP5MS, 30 m �0.25 mm �0.25 mm
He 1
ml/min
70 8C (2 min)–
20 8C/min!230 8C(2 min)
FID
FTIR
BSTFA
14
8S
.M.R
.W
ille,W
.E.E
.L
am
bert/F
oren
sicS
cience
Intern
atio
na
l1
42
(20
04
)1
35
–1
56
[70] Blood, urine Toluene HS-SPME 250 Split
30:1
FID: HP-Innowax,
30 m � 0.25 mm
� 0.25 mm
FID: 60 8C(6 min)–10 8C/
min!140 8C(3 min)
FID 0.001 mg/
ml SPME,
0.01 mg/ml
HS
HS MS: HP 5ms,
30 m � 0.25 mm
� 0.25 mm
MS: isothermal:
60 8CMS
[15] Blood, lung,
brain, fat
VOC, incl xylene, butane,
halothane, toluene, petrole
residues
HS-SPME 220 Splitless DE 1701,
30 m � 0.25 mm
� 0.25 mm
He
1 ml/min
35 8C (1 min)–
8 8C/min!270 8C(1 min)
MS
[27] Blood, urine,
tissues
Tetrachloroethylene,
trichloroethylene,
trichloroacetic acid
HS-SPME 250 SPB 1, 30 m �0.25 mm
N2
3 m1/min
ECD: 60 8C(1 min)– 10 8C/
min!130 8C(1.54 min)
ECD 3–5 ng/g 3-Methyl-
1-p-toyl
triazene in
diethyl
oxideMS: 45 8C–10 8C/
min!200 8CMS
[32] Urine, gastric
contents
Methylene chloride,
volatile petroleum
contents, (ethanol)
HS-SPME 225, 250 Splitless DB 1, 30 m �0.25 mm �0.25 mm
30 8C (5 min)–5 8C/
min!125 8C (5 min)
or 40 8C (5 min)–
5 8C/min!125 8C(9 min)
MS
[71] Blood, urine Thinner components:
toluene, benzene,
n-butylacetate, n-butanol,
n-isoamylacetate
HS-SPME 200 Splitless DB-Wax, 30 m �0.32 mm �0.25 mm
He
4 m1/min
35 8C (1 min)–
20 8C/min!230 8CFID 0.0022–
0.0048
mg/ml
[72] Blood, liver,
kidney, brain,
urine, bile,
stomach
contents
Halothane, isoflurane,
chloroform, diethylether
HS-SPME 250 Splitless HP 5ms, 30 m �0.25 mm �0.25 mm
He 1.0
ml/min
40 8C (2 min)–
30 8C!280 8CMS 0.004
mg/kg
[73] Blood, urine Chloroform,
methylene chloride
HS-SPME 240 Splitless RTX 624, 30 m �0.32 mm �1.80 mm
He
2 ml/min
35 8C (1 min)–
10 8C/min!105 8CFID 0.3 mg/ml
(blood),
0.2 mg/ml
(urine)
[34] Blood Hydrocarbons HS-
SPME-COT
250 Splitless XTI 5, 30 m �0.25 mm �0.25 mm
He 2.1
ml/min
�40 8C (1 min)–
30 8C/min!290 8CMS 0.01 mg/g
blood
[24] Blood, urine Hydrolysed n-butylnitrite HS-
SPME-CF
240 Splitless HP 1, 30 m �0.53 mm �2.64 mm
He
4 ml/min
50 8C (5 min)–
10 8C/min!260 8C(5 or 10 min)
FID 0.001
mg/ml
[35] Blood, urine Ethytacetate, benzene,
butan-1-ol, toluene,
butylacetate,
isoamylacetate
HS-COT 200 Splitless 5 ml DB624, 30 m �0.32 mm �1.80 mm
He
5 ml/min
5 8C (1 min)–
20 8C/min!100 8CFID 0.0005–
0.005
mg/ml
1008 C (3 min)!110 8C
[39] Blood o-, m-, p-Xylenes HS-COT 180 Splitless 2 ml AT-WAX, 30 m �0.32 mm � 0.5 mm
He 2.2
ml/min
5 8C (1 min)–
15 8C/min!180 8C(4 min)
FID 0.020
mg/ml
[60] Blood, lung Propane, isobutane,
butane, neopentane,
n-pentane,
bromochlorodifluoromethane
HS-COT 30 0.100–
0.250 m1
DB5 Isothermal: between
0 and 10 8CMS
S.M
.R.
Wille,
W.E
.E.
La
mb
ert/Fo
rensic
Scien
ceIn
terna
tiona
l1
42
(20
04
)1
35
–1
56
14
9

Table 6 (Continued )
Reference Matrix Compounds Extr.
method
Inj. temp.
(8C)
Inj. M Inj. vol. Column Gas
flow
Oven Detector Det.
limit
Quant.
limit
Derivat.
[61] Blood Sevoflurane, isoflurane,
enflurane, halothane
HS-COT 150 Splitless 10 ml RTX-Votatile,
30 m � 0.32
� 1.5 mm
He 2
ml/min
�40 8C (1 min)–
10 8C/min!70 8CFID 0.010–
0.100
mg/ml70 8C–20 8C/min!250 8C (4 min)
[62] Blood Chloroform, methylene
chloride
HS-COT 250 Splitless 5 ml RTX-Volatile,
30 m � 0.32 mm
� 1.5 mm
He 3
ml/min
�30 8C (1 min)–
10 8C/min!100 8CFID 0.004
mg/ml
100 8C–20 8C/
min!280 8C[37] Blood n-Propane, isobutane,
n-butane
HS-CF/Tenax 200 Split
(0.7:1,
40:1)
0.5 ml WCOT CP624,
41 m � 0.25 mm
� 2.1 mm
He 1.0
ml/min
Isothermal: 35 8C MS 0.0013–
0.00301
mg/ml
0.0055–0.012 mg/ml
[38] Blood Aceton, isopropanol,
1-propanol, 1,1,1-trichloro-
ethane, isoflurane, diethylether,
tert-butanol, toluene, isobuty
methylketone, ethylacetate
PT Tenax 240 Split
1:4
PoraPLOT Q,
25 m � 0.32
� 10 mm
He 1.5
ml/min
30 8C (2 min)–
15 8C/min!240 8C (2 min)
FID
FTIR
0.05–
10 mg/ml
(low mol
alcohols:
100 mg/ml)
[40] Blood Hydrocarbons PT Tenax 250 2 ml DB 5, 15 m �0.53 mm � 15 mm
40 8C–4 8C/
min!90 8CMS 0.001–
0.01 mg/g
[57] Blood 27 VOC PT Tenax 250 Splitless PoraPLOT Q,
25 m � 0.32
� 10 mm
He 3.8
ml/min
30 8C (2 min)–
15 8C/min!250 8C (5 min)
FlD 0.01–
24 mg/ml
FTIR
[49] Blood, liver,
kidney,
stomach
contents
Chloral hydrate,
trichloroethanol,
trichloroacetic acid
Solvent 150 Splitless 0.001 m1 DB 1, 30 m �0.32 mm � 5 mm
80 8C (1 min)–
10 8C/min!110 8C,
110 8C (12 8C)–20
8C/min!250 8C
ECD Diazome-
thane
[50] Blood, urine,
stomach
content
Chloral hydrate,
trichloroethanol
Solvent 250 Splitless 100%
methylsilicone,
15 m � 0.25 mm
� 1.0 mm
He 1.5
ml/min
Isothermal: 50 8C MS
[53] Blood, liver,
kidney, lung,
stomach
contents
Trichloroethylene,
trichloroethanol,
trichloroacetic acid
Solvent 150 PTV 0.0001 ml ECD: DB 1, 30 m �0.32 mm � 5 mm
ECD: 80 8C(1 min)–10 8C/
min!110 8C,
110 8C (12 8C)–
20 8C/min!250 8C
ECD 5–10 pg 25 pg Diazome-
thane
0.001 ml FTIR: HP Ultra 1,
25 m � 0.32 mm �0.5 mm
FTIR: 40 8C(1 min)–10 8C/
min!250 8C
FTIR
Abbreviations: Extr. method, extraction method; PH, pulse-heating; PT, purge and trap; Inj. temp., injection temperature; He, helium; FID, flame ionization detection; Inj. M, injection mode; MS, mass spectrometer; FTIR,
Fourier transformation infrared detector; Inj. vol., injection volume; ITD, ion trap detection; ECD, electron capture detector; Det. limit, detection limit; COT, cryogenic oven trapping; FET, full evaporation technique; Quant.
limit, quantitation limit; CF, cryogenic focusing; MHE, multiple headspace; Derivat., derivatisation method; chem., chemical; SPME, solid phase microextraction; HS, headspace; PTV, programmed temperature vaporization.
Column phase: wax, innowax: crosslinked polyethylene glycol; 5: 5% diphenyl–195% dimethylsiloxane; 1: polydimethylsiloxane; 624: 6% cyanopropylphenyl–94% methlylpolysiloxane; Pora PLOT Q: styrene-divinyl benzene
porous polymer; RTX volatile: diphenyl-dimethylpolysiloxane; WCOT SPSIL 5CB: 100% polydimethylsiloxane; DB 1701: 14% cyanopropylphenyl–86% dimethylpolysiloxane; DB 1301: 6% cyanopropylphenyl–94% phenyl.
15
0S
.M.R
.W
ille,W
.E.E
.L
am
bert/F
oren
sicS
cience
Intern
atio
na
l1
42
(20
04
)1
35
–1
56
phase. This matrix effect limits the use of direct headspace
as a simple quantitative method, especially for forensic
post-mortem samples [44]. The standard addition method
(SAM), multiple headspace extraction method (MHE) and
full evaporation technique (FET) [44] are quantitative
procedures that try to overcome this matrix effect [16].
The standard addition procedure compares the signal of
the sample with and without addition of a known amount
of the analyte in question. The assumption is made that the
dispersion in the matrix of the added analyte is the same as
for the original analyte. This is not always correct, espe-
cially when it involves heterogeneous biological samples
such as tissues [16,44]. The multiple headspace technique
is a stepwise extraction of volatile organic compounds into
the gas phase by using a series of regular headspace
analyses. Every time an aliquot is taken and analysed
re-equilibration occurs. The vapour concentration will
reduce logarithmically by each step and eventually it is
possible to extrapolate the original concentration from the
curves obtained after a few analyses, in combination with
internal of external standardisation or standard addition
[16,26,44,78].
The full evaporation technique approach is based on the
equilibration of a small amount of sample at high tempera-
ture so that the analyte is (almost) fully evaporated. The
main drawback here is the lower sensitivity as compared to
headspace analysis. FET is nevertheless also applicable to
forensic work if a sensitive detection system is used as
described by Schuberth [44] for the determination of ben-
zene, toluene and other volatiles in post-mortem blood and
tissues with a MS-ion trap detector.
4. Metabolites
4.1. Introduction
Elimination of volatile organic compounds can occur
unchanged in exhaled air or through metabolism occurring
mainly in the liver, resulting in elimination of more polair
and thus less volatile compounds in the exhaled air and
urine. Factors such as age, disease, dose and exposure may
effect the rate and extent of metabolism [2]. Analysis of
metabolites from volatiles are of importance in occupational
and environmental exposure and in monitoring of abuse as is
seen in the literature [45–48]. A variation of methods such as
high performance liquid chromatography, high performance
capillary electrophoresis and gas chromatography are used
for the determination of metabolites of volatiles in urine. In
post-mortem cases, metabolites in urine seem less relevant,
as the mother component in blood or tissues can give a direct
toxicological link. However, chloral hydrate, due to its fast
metabolism by alcohol dehydrogenase is unlikely to be
detected post-mortem, and thus determination of its active
metabolite in urine, trichloroethanol, is relevant [49–51].
Trichloroethanol and trichloroacetic acid, both metabolites
of trichloroethylene are determined together with their
mother compound in several post-mortem cases [52,53].
Phenol was analysed [56], however, not as metabolite of
benzene.
4.2. Sampling
Static headspace and solvent extraction are the methods
used for sampling of the compounds. The headspace
Fig. 3. Analysis of the qualitative standard mixture with detector
sensitivities (FSD) (a) FID 3.2 nA and (b) ECD 64 kHz. Column,
60 m � 0:53 mm i.d. SPB-1 (5 mm film); oven temperature, 40 8C(6 min), then to 80 8C at 5 8C min�1, then to 200 8C at
10 8C min�1; and injection volume, �0.010 cm3. Peaks: 1:
propane, 2: FC12, 3: dimethyl ether, 4: isobutane, 5: butane, 6:
BCF, 7: ethanol, 8: acetone, 9: propan-2-ol, 10: FC11, 11: FC113,
12: halothane, 13: butanone, 14: hexane, 15: chloroform, 16: 1,1,1-
trichloroethane, 17: carbon tetrachloride, 18: trichloroethylene, 19:
methyl isobutyl ketone, 20: 1,1,2-trichloroethane (internal stan-
dard), 21: toluene, 22: tetrachloroethylene, 23: 2,2,2-trichloroetha-
nol, and 24: ethylbenzene (internal standard). Source: [20] Fig. 2
(p. 1114).
S.M.R. Wille, W.E.E. Lambert / Forensic Science International 142 (2004) 135–156 151

technique is used for the extraction of trichloroacetic acid in
combination with its mother compound, as well as for the
extraction of tetrachloroethylene and its metabolite tri-
chloroacetic acid [28]. Trichloroethanol, a urinary meta-
bolite of chloral hydrate, is extracted by solvent extraction
[49,50,54].
4.3. Separation and detection
4.3.1. Spectrophotometric detection
Heating trichloroethanol in combination with pyridine
and sodium hydroxide results in a reaction product with a
spectral maximum at 368 nm, while reaction products with
Fig. 4. (A) Mass spectra of butane and 2-methylpropane. Source: Mass Spectral and GC Data (second ed., ISBN 3-527-26989-4) p. 57. (B)
Gram-Schmidt reconstruction chromatogram obtained from 0.5 ml of case 1 blood and the vapour phase FTIR spectrum of ethyl acetate (7)
superimposed with the corresponding library spectra. And the mass spectrum of ethylacetate. Source: [38] Fig. 1 a, h (p. 205), Mass Spectral
and GC Data (second ed., ISBN 3-527-26989-4) p. 278.
152 S.M.R. Wille, W.E.E. Lambert / Forensic Science International 142 (2004) 135–156

chloral hydrate and trichloroacetic acid have maxima at 368
and 530 nm, respectively [54].
4.3.2. Gas chromatographic determination
Gas chromatography is used in combination with ECD,
FID, MS or FTIR. Polar metabolites have a lower volatility
and therefore derivatisation could be necessary for a better
peak shape and thus higher sensitivity. BSTFA is used for
silylation of trichloroacetic acid [28], while methylation of
this acid also occurred after use of diazomethane [49,53].
Column phases vary from apolair such as 100% methylsi-
licone to polair phases such as a cyanopropyl phenyl phase.
5. Precautions in interpretation of results
When interpreting qualitative results attention should be
paid to wrong conclusions due to the fact that compounds of
related character generate very similar mass spectra such as
butane and 2-methylpropane, thus resulting in several can-
didates as possible cause of death [43]. Detection of volatile
organic compounds does not always indicate death by
solvent abuse. Not only must the possibility of environmen-
tal, occupational and therapeutic exposure of the deceased
be evaluated, also the possible formation of endogenous
volatile compounds due to several inborn errors of metabo-
lism must be taken in account [2,14,20]. Ketotic patients
have a high concentration of acetone in their blood, while
acetone and butanone are seen in large quantities in children
with acetoacetyl CoA thiolase deficiency. Volatiles such as
halothane are used for therapeutic purposes, while chloro-
butanol is a sedative and a bactericide present in some
heparin preparations [20].
Volatiles may also occur in vivo after metabolism of
specific compounds such as acetone after metabolism of
isopropanol. Compounds such as alkylnitrites are unstable
and degrade rapidly in vivo into the corresponding alcohol
[19]. Hippuric acid can originate from ingestion of benzo-
ates, added to food as a preservative.
The simultaneous detection of several compounds may
also lead to determination of the source, for example pet-
roleum consists of aliphatic and aromatic hydrocarbons,
naphtalenes, paraffin, alkenes and eventually tetra-ethyl lead
[55]. Trichloroacetic acid can originate from trichloroethy-
lene, chloralhydrate, triclofos and dichloral phenazone [19],
while a thermal decomposition of trichloroacetic acid can
lead to chloroform. Most abused products are commonly
used in the lab and therefore are an easy source of con-
tamination of the sample. Xylene, toluene, butanol and
ethylbenzene can be detected after storage of blood in a
Sarstedt Monovette Serum gel blood collection tube,
whereas 1-butanol and 2-methyl-2-propanol are detected
in EDTA-coated tubes [19].
The main reason why scepticism of quantitative results is
necessary is the occurrence of losses of analytes during
sampling, sample handling and storage, which results in
‘false’ quantitation, especially in the case of very volatile
analytes such as propane, butane and the halon aerosol
propellants [19]. Due to the volatile nature of the compounds
and individual differences in susceptibility such as rates of
absorption, delivery to target tissue compartments, rates of
metabolism and elimination, and protective response, differ-
ences in blood concentrations may occur, thus leading to a
lack of a strong correlation between blood levels and clinical
features [2,14].
6. Summary
The extraction methods for volatile compounds are sim-
ple, inexpensive and solvent-free in most cases. Injection of
large volumes or preconcentration of the sample is applied in
view of the low levels of the target compounds in the sample.
By HS-COT, HS-CF, SPME, sample loads are higher and
thus sensitivity is enhanced. A variety of capillary columns
can be used for the separation of volatile organic compounds
due to differences in polarity of these compounds, com-
pound mixes and differences in extraction techniques and
detectors used. The large variety of volatiles requires an
analytical method that both detects and identifies the com-
pounds. MS, ECD and FID are usually used for quantitation
purposes, while MS and FTIR have a screening and con-
firmation purpose. Quantification can be based on addition
of an internal standard or by matrix-negating procedures
such as MHE, FET and SAM.
For occupational and environmental exposure and in
monitoring of abuse of volatile organic compounds, analysis
of metabolites in urine can be interesting because of the
extended detection window and ease of sampling. In post-
mortem cases, metabolites seem of less importance,
although trichloroethanol and trichloroacetic acid are ana-
lysed in cases of chloral hydrate and trichloroethylene
(ab)use. These analytes were determined after solvent- or
HS-extraction through spectrophotometric detection or GC
detection after derivatization.
Of great importance are sample handling due to the
volatile nature of the compounds and caution remains
necessary by the interpretation of the qualitative and quan-
titative results.
References
[1] A. Esmail, L. Meyer, A. Pottier, S. Wright, Deaths from
volatile substance-abuse in those under 18 years—results
from a National Epidemiologic-Study, Arch. Dis. Child. 69
(1993) 356–360.
[2] R.J. Flanagan, M. Ruprah, T.J. Meredith, J.D. Ramsey, An
introduction to the clinical toxicology of volatile substances,
Drug Saf. 5 (1990) 359–383.
[3] G.P. Marelich, Volatile substance abuse, Clin. Rev. Allergy
Immunol. 15 (1997) 271–289.
[4] N. Infofacts, http://www.drugabuse.gov.
S.M.R. Wille, W.E.E. Lambert / Forensic Science International 142 (2004) 135–156 153

[5] Z.S. Nicolas Kozel, M. De La Rosa, Epidemiology of
inhalant abuse: an international prespective (NIDA), 1995,
http://www.drugabuse.gov/pdf/monographs/148.pdf.
[6] S.H. Dinwiddie, Abuse of inhalants—a review, Addiction 89
(1994) 925–939.
[7] Y.D. Neumark, J. Delva, J.C. Anthony, The epidemiology of
adolescent inhalant drug involvement, Arch. Pediatr. Adolesc.
Med. 152 (1998) 781–786.
[8] D.R. Williams, S.J. Cole, Ventricular fibrillation following
butane gas inhalation, Resuscitation 37 (1998) 43–45.
[9] C.H. Steffee, G.J. Davis, K.K. Nicol, A whiff of death: fatal
volatile solvent inhalation abuse, South. Med. J. 89 (1996)
879–884.
[10] T.L. Kurtzman, K.N. Otsuka, R.A. Wahl, Inhalant abuse by
adolescents, J. Adolesc. Health 28 (2001) 170–180.
[11] R.L. Balster, Neural basis of inhalant abuse, Drug Alcohol
Depend. 51 (1998) 207–214.
[12] C.H. Ashton, Solvent abuse—little progress after 20 years,
BMJ 300 (1990) 135–136.
[13] F. Musshoff, H. Junker, B. Madea, An unusual case of driving
under the influence of enflurane, Forensic Sci. Int. 128 (2002)
187–189.
[14] B. Larry, in: B. Larry (Ed.), Principles of Forensic
Toxicology, ISBN 1-890883-07-7, 1999.
[15] D.J. Tranthim-Fryer, R.C. Hansson, K.W. Norman, Head-
space/solid-phase microextraction/gas chromatography–mass
spectrometry: a screening technique for the recovery and
identification of volatile organic compounds (VOC’s) in
postmortem blood and viscera samples, J. Forensic Sci. 46
(2001) 934–946.
[16] Y. Seto, Determination of volatile substances in biological
samples by headspace gas-chromatography, J. Chromatogr. A
674 (1994) 25–62.
[17] F.L. Cardinali, J.M. McCraw, D.L. Ashley, M.A. Bonin,
Production of blank water for the analysis of volatile organic-
compounds in human blood at the low parts-per-trillion level,
J. Chromatogr. Sci. 32 (1994) 41–45.
[18] R. Gill, S.E. Hatchett, M.D. Osselton, H.K. Wilson, J.D.
Ramsey, Sample handling and storage for the quantitative-
analysis of volatile compounds in blood—the determination
of toluene by headspace gas-chromatography, J. Anal.
Toxicol. 12 (1988) 141–146.
[19] R.J. Flanagan, P.J. Streete, J.D. Rampsey, Practical guidelines
for analytical investigation of suspected cases and interpreta-
tion of results, http://www.unodc.org/pdf/technical_series_
1997-01-01_1.pdf.
[20] P.J. Streete, M. Ruprah, J.D. Ramsey, R.J. Flanagan,
Detection and identification of volatile substances by head-
space capillary gas-chromatography to aid the diagnosis of
acute-poisoning, Analyst 117 (1992) 1111–1127.
[21] D. Dyne, J. Cocker, P.J. Streete, R.J. Flanagan, Toluene, 1-
butanol, ethylbenzene and xylene from Sarstedt Monovette
serum gel blood collection tubes, Ann. Clin. Biochem. 33
(1996) 355–356.
[22] P.J. Streete, R.J. Flanagan, Ethylbenzene and xylene from
Sarstedt Monovette serum gel blood-collection tubes, Clin.
Chem. 39 (1993) 1344–1345.
[23] J. Drozd, J. Novak, Headspace gas-analysis by gas-chroma-
tography, J. Chromatogr. 165 (1979) 141–165.
[24] J. Tytgat, P. Daenens, Solvent-free sample preparation by
headspace solid-phase microextraction applied to the tracing
of n-butyl nitrite abuse, Int. J. Legal Med. 109 (1996) 150–
154.
[25] N.C. Yang, K.L. Hwang, D.Z. Hung, H.H. Wuhh, W.M. Ho,
Reliable gas chromatographic–mass spectrometric method
combined with a headspace autosampler for isoflurane
determination in blood, J. Chromatogr. B 742 (2000) 277–282.
[26] K. Pihlainen, I. Ojanpera, Analytical toxicology of fluori-
nated inhalation anaesthetics, Forensic Sci. Int. 97 (1998)
117–133.
[27] B. Dehon, L. Humbert, L. Devisme, M. Stievenart, D.
Mathieu, N. Houdret, M. Lhermitte, Tetrachloroethylene and
trichloroethylene fatality: case report and simple headspace
SPME-capillary gas chromatographic determination in tis-
sues, J. Anal. Toxicol. 24 (2000) 22–26.
[28] Y. Gaillard, F. Billault, G. Pepin, Tetrachloroethylene fatality:
case report and simple gas chromatographic determination in
blood and tissues, Forensic Sci. Int. 76 (1995) 161–168.
[29] B.M. El-Haj, A.M. Al-Amri, M.H. Hassan, R.K. Bin-
Khadem, A.A. Al-Hadi, A GC–MS method for the detection
of toluene and ethylbenzene in volatile substance abuse, J.
Anal. Toxicol. 24 (2000) 390–394.
[30] J.T. Liu, P. Cheng, O. Suzuki, Solid-phase microextraction
(SPME) of drugs and poisons from biological samples,
Forensic Sci. Int. 97 (1998) 93–100.
[31] G. Theodoridis, E.H.M. Koster, G.J. de Jong, Solid-phase
microextraction for the analysis of biological samples, J.
Chromatogr. B 745 (2000) 49–82.
[32] W.E. Brewer, R.C. Galipo, S.L. Morgan, K.H. Habben, The
confirmation of volatiles by solid-phase microextraction and
GC-MS in the investigation of two traffic fatalities, J. Anal.
Toxicol. 21 (1997) 286–290.
[33] D.B.E. Poli, P. Manini, R. Andreoli, A. Mutti, Solid-phase
microextraction gas chromatographic–mass spectrometric
method for the determination of inhalant anesthetics in urine,
J. Chromatogr. B 732 (1999) 115–125.
[34] J.T. Liu, K. Hara, S. Kashimura, M. Kashiwagi, T.
Hamanaka, A. Miyoshi, M. Kageura, Headspace solid-phase
microextraction and gas chromatographic–mass spectrometric
screening for volatile hydrocarbons in blood, J. Chromatogr.
B 748 (2000) 401–406.
[35] X.P. Lee, T. Kumazawa, K. Sato, K. Watanabe, H. Seno, O.
Suzuki, Determination of solvent thinner components in
human body fluids by capillary gas chromatography with
trapping at low oven temperature for headspace samples,
Analyst 123 (1998) 147–150.
[36] K. Watanabe-Suzuki, A. Ishii, O. Suzuki, Cryogenic oven-
trapping gas chromatography for analysis of volatile organic
compounds in body fluids, Anal. Bioanal. Chem. 373 (2002)
75–80.
[37] M. Bouche, W.E. Lambert, J.F.P. Van Bocxlaer, M.H. Piette,
A.P. De Leenheer, Quantitative determination of n-propane,
iso-butane, and n-butane by headspace GC–MS in intoxica-
tions by inhalation of lighter fluid, J. Anal. Toxicol. 26 (2002)
35–42.
[38] I. Ojanpera, R. Hyppola, E. Vuori, Identification of volatile
organic compounds in blood by purge and trap PLOT-
capillary gas chromatography coupled with Fourier transform
infrared spectroscopy, Forensic Sci. Int. 80 (1996) 201–209.
[39] H. Hattori, M. Iwai, S. Kurono, T. Yamada, K. Watanabe-
Suzuki, A. Ishii, H. Seno, O. Suzuki, Sensitive determination
of xylenes in whole blood by capillary gas chromatography
154 S.M.R. Wille, W.E.E. Lambert / Forensic Science International 142 (2004) 135–156

with cryogenic trapping, J. Chromatogr. B 718 (1998) 285–
289.
[40] M. Morinaga, K. Hara, M. Kageura, Y. Hieda, M. Takamoto,
S. Kashimura, A simple, rapid and simultaneous analysis of
complex volatile hydrocarbon mixtures in blood using gas-
chromatography mass-spectrometry with a wide-bore capil-
lary column, J. Legal Med. 103 (1990) 567–572.
[41] T. Ohshima, T. Kondo, Y. Sato, T. Takayasu, Postmortem
alcohol analysis of the synovial fluid and its availability in
medico-legal practices, Forensic Sci. Int. 90 (1997) 131–138.
[42] K. Saito, T. Takayasu, J. Nishigami, T. Kondo, M. Ohtsuji,
Z.Q. Lin, T. Ohshima, Determination of the volatile
anesthetics halothane, enflurane, isoflurane, and sevoflurane
in biological specimens by pulse-heating GC–MS, J. Anal.
Toxicol. 19 (1995) 115–119.
[43] J. Schuberth, Joint use of retention index and mass-spectrum
in postmortem tests for volatile organics by headspace
capillary gas-chromatography with ion-trap detection, J.
Chromatogr. A 674 (1994) 63–71.
[44] J. Schuberth, A full evaporation headspace technique with
capillary GC and ITD: a means for quantitating volatile
organic compounds in biological samples, J. Chromatogr. Sci.
34 (1996) 314–319.
[45] A. Astier, Chromatographic determination of volatile solvents
and their metabolites in urine for monitoring occupational
exposure, J. Chromatogr. 643 (1993) 389–398.
[46] Y.D. Yang, Simultaneous determination of creatine, uric acid,
creatinine and hippuric acid in urine by high performance
liquid chromatography, Biomed. Chromatogr. 12 (1998) 47–
49.
[47] T. Fujii, S. Kawabe, T. Horike, T. Taguchi, M. Ogata,
Simultaneous determination of the urinary metabolites of
toluene, xylene and styrene using high-performance capillary
electrophoresis—comparison with high-performance liquid
chromatography, J. Chromatogr. B 730 (1999) 41–47.
[48] B. Raikhlin-Eisenkraft, E. Hoffer, Y. Baum, Y. Bentur,
Determination of urinary hippuric acid in toluene abuse, J.
Toxicol. Clin. Toxicol. 39 (2001) 73–76.
[49] E. Meyer, J.F. Van Bocxlaer, W.E. Lambert, M. Piette, A.P. De
Leenheer, Determination of chloral hydrate and metabolites in
a fatal intoxication, J. Anal. Toxicol. 19 (1995) 124–126.
[50] P.F. Heller, B.A. Goldberger, Y.H. Caplan, Chloral hydrate
overdose—trichloroethanol detection by gas-chromatography
mass-spectrometry, Forensic Sci. Int. 52 (1992) 231–234.
[51] B. Levine, J. Park, T.D. Smith, Y.H. Caplan, Chloral
hydrate—unusually high-concentrations in a fatal overdose,
J. Anal. Toxicol. 9 (1985) 232–233.
[52] V.A.E. Coopman, J. Cordonnier, E.A. De Letter, M.H.A.
Piette, Tissue distribution of trichloroethylene in a case of
accidental acute intoxication by inhalation, Forensic Sci. Int.
134 (2003) 115–119.
[53] S. De Baere, E. Meyer, I. Dirinck, W. Lambert, M. Piette, C.
Van Peteghem, A. De Leenheer, Tissue distribution of
trichloroethylene and its metabolites in a forensic case, J.
Anal. Toxicol. 21 (1997) 223–227.
[54] A.J. McBay, V.R. Boling, P.C. Reynolds, Spectrophotometric
determination of trichloroethanol in chloral hydrate poison-
ing, J. Anal. Toxicol. 4 (1980) 99–101.
[55] S. Cairney, P. Maruff, C. Burns, B. Currie, The neurobeha-
vioural consequences of petrol (gasoline) sniffing, Neurosci.
Biobehav. Rev. 26 (2002) 81–89.
[56] T. Tanaka, K. Kasai, T. Kita, N. Tanaka, Distribution of
phenol in a fatal poisoning case determined by gas
chromatography mass spectrometry, J. Forensic Sci. 43
(1998) 1086–1088.
[57] I. Ojanpera, K. Pihlainen, E. Vuori, Identification limits for
volatile organic compounds in the blood by purge-and-trap
GC-FTIR, J. Anal. Toxicol. 22 (1998) 290–295.
[58] J.M. Gaulier, V. Tonnay, T. Faict, H. Sayer, P. Marquet, G.
Lachatre, Analytical aspects of volatile substance abuse
(VSA), J. Forensic Sci. 48 (2003) 880–882.
[59] N.C. Yang, K.L. Hwang, C.H. Shen, H.F. Wang, W.M. Ho,
Simultaneous determination of fluorinated inhalation anes-
thetics in blood by gas chromatography–mass spectrometry
combined with a headspace autosampler, J. Chromatogr. B
759 (2001) 307–318.
[60] V.F. Kalasinsky, GC/MS characterization of inhalants in
blood and tissue, in: Proceedings of Tiaft Meeting Thessa-
loniki, Macedonia, Greece, 1995, pp. 6–9.
[61] T. Kojima, A. Ishii, K. Watanabe-Suzuki, R. Kurihara, H.
Seno, T. Kumazawa, O. Suzuki, Y. Katsumata, Sensitive
determination of four general anaesthetics in human whole
blood by capillary gas chromatography with cryogenic oven
trapping, J. Chromatogr. B 762 (2001) 103–108.
[62] K. Watanabe, H. Seno, A. Ishii, O. Suzuki, T. Kumazawa,
Capillary gas chromatography with cryogenic oven tempera-
ture for headspace samples: analysis of chloroform or
methylene chloride in whole blood, Anal. Chem. 69 (1997)
5178–5181.
[63] L.A. Broussard, A.K. Broussard, T.S. Pittman, D.K. Lirette,
Death due to inhalation of ethyl chloride, J. Forensic Sci. 45
(2000) 223–225.
[64] H. Ise, K. Kudo, N. Jitsufuchi, T. Imamura, N. Ikeda, Simple
and rapid determination of enflurane in human tissues using
gas chromatography and gas chromatography mass spectro-
metry, J. Chromatogr. B 698 (1997) 97–102.
[65] S.W. Park, N.Y. Kim, Y.G. Yang, B. Seo, K.J. Paeng, Toluene
distribution of glue sniffers’ biological fluid samples in
Korea, J. Forensic Sci. 43 (1998) 888–890.
[66] L.A. Broussard, T. Brustowicz, T. Pittman, K.D. Atkins, L.
Presley, Two traffic fatalities related to the use of difluor-
oethane, J. Forensic Sci. 42 (1997) 1186–1187.
[67] S.P. Avis, J.T. Archibald, Asphyxial suicide by propane
inhalation and plastic bag suffocation, J. Forensic Sci. 39
(1994) 253–256.
[68] J. Schuberth, Gas residues of engine starting fluid in
postmortem sample from an arsonist, J. Forensic Sci. 42
(1997) 144–147.
[69] M. Morinaga, S. Kashimura, K. Hara, Y. Hieda, M. Kageura,
The utility of volatile hydrocarbon analysis in cases of carbon
monoxide poisoning, Int. J. Legal Med. 109 (1996) 75–79.
[70] N.Y. Kim, S.W. Park, The comparison of toluene determina-
tion between headspace-solid phase microextraction and
headspace methods in glue-sniffer’s blood and urine samples,
J. Forensic Sci. 45 (2000) 702–707.
[71] X.P. Lee, T. Kumazawa, K. Sato, A simple analysis of 5
thinner components in human-body fluids by headspace solid-
phase microextraction (SPME), Int. J. Legal Med. 107 (1995)
310–313.
[72] F. Musshoff, H. Junker, B. Madea, Rapid analysis of halothane
in biological samples using headspace solid-phase microex-
traction and gas chromatography–mass spectrometry—a
S.M.R. Wille, W.E.E. Lambert / Forensic Science International 142 (2004) 135–156 155

case of a double homicide, J. Anal. Toxicol. 24 (2000) 372–
376.
[73] H. Seno, A. Ishii, K. Watanabe, O. Suzuki, T. Kumazawa,
Extraction of chloroform and methylene chloride in human
whole blood and urine by headspace solid phase microextrac-
tion (SPME), Med. Sci. Law 39 (1999) 332–336.
[74] R.L. Fitzgerald, C.E. Fishel, L.L.E. Bush, Fatality due to
recreational use of chlorodifluoromethane and chloropenta-
fluoroethane, J. Forensic Sci. 38 (1993) 476–482.
[75] A. Groppi, A. Polettini, P. Lunetta, G. Achille, M. Montagna,
A fatal case of trichlorofluoromethane (freon 11) poisoning—
tissue distribution study by gas-chromatography mass-spec-
trometry, J. Forensic Sci. 39 (1994) 871–876.
[76] C.L. Winek, W.W. Wahba, R. Huston, L. Rozin, Fatal
inhalation of 1,1,1-trichloroethane, Forensic Sci. Int. 87
(1997) 161–165.
[77] N.Y. Kim, S.W. Park, J.K. Suh, Two fatal cases of
dichloromethane or chloroform poisoning, J. Forensic Sci.
41 (1996) 527–529.
[78] B. Kolb, L.S. Ettre, in: Static Headspace-Gas Chromatogra-
phy Theory and Practice, ISBN 0-471-19238-4, Wiley-VCh
Inc., 1997, 298 pp.
156 S.M.R. Wille, W.E.E. Lambert / Forensic Science International 142 (2004) 135–156

Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.