vol. 18 - issue 10
DESCRIPTION
A European Outlook on the World of OphthalmologyTRANSCRIPT
VOLUME 18 ISSUE 10 OCTOBER 2013
A GLOBAL VISION

Bre
ath
taki
ng
Strong
Any nucleus from soft to hardest, any incision from
1.6 to 3.2 mm, fast, safe and the AC always stable.
That’s easyPhaco®. CortexModeTM for precisely con-
trolled cortical clean-up. HF capsulotomy for difficult
cases. 1200 cuts anterior vitrectomy.
Beautiful
So easy to operate! DirectAccess® to any function
without confusion. Programmable for 20 surgeons.
Bright, easy to read display. A marvel of design,
brings a friendly note in your OR.
Unique
Truly portable, 5 kg, fits in a pilot’s case. HFDS ab
interno glaucoma function, the future of combined
glaucoma surgery. Fantastic toe tip of flow control.
Built-in compressor. Just plug to 90-230 V.
For You
Lets you enjoy most advanced surgery from low to
highest volume in any set-up at controlled costs.
www.oertli-catarhex3.com
Eckn
auer
+Sc
hioc
h A
SW

4
24
62
14
32
70
THIS ISSUE...
Cover Story 4 ESCRS developing global vision by
linking with other societies
Special Focus: Cataract & Refractive 8 NSAID use more common in North
America than Europe9 Refractive surgery in strabismus patients
safe and effective10 Study highlights advantages of femto-
cataract12 Newer ablation profiles improve results
but caution urged 14 ‘Dry lab’ training for phacoemulsification
surgery15 Refractive errors lower with right closed-
loop haptics16 Moving in the right direction with
laser-assisted phaco18 Questions over femtosecond cataract
surgery19 Refractive efficacy in
keratoconus patients
Cornea 21 Fungal keratitis needs more research 22 Femtosecond laser and intracorneal ring
segment implantation24 Options for intervention after corneal
perforation26 FD-OCT helps assess stem cell
transplants27 Femtosecond layers in corneal surgery28 Dua’s Layer is significant breakthrough29 Techniques for indentifying dry eye
Glaucoma 31 Nitric oxide-donating prostaglandin
analogue32 OSD diagnosis often overlooked34 One-site and two-site surgery35 Pattern laser trabeculoplasty for OAG36 Glaucoma patients should reduce
caffeine intake38 Rock inhibitors have benefits and
side effects39 Preservative-free glaucoma medications 40 Glucosamine supplements may induce
IOP elevation
Retina 42 Imaging and clinical trials for hereditary
retinal diseases43 Anti-VEGF treatment and branch retinal
vein occlusion44 Comparison of submacular haemorrhage
treatments46 French population study sheds light on
AMD prevalence
Ocular 48 ‘Clip-on’ smartphone adaptor for
education and teaching50 Dutch ophthalmologists facing
challenges of recession
Paediatric Ophthalmology 52 Indications for phaco-refractive surgery
very rare in children
Global Ophthalmology 53 Ophthalmologists and global blindness
News 56 Frontalis Sling Surgery57 PREMED study has enrolled first
patients58 International AMD and Retina Congress
convenes in Dublin
Features 60 Eye on Travel62 Resident’s Diary64 Industry News65 Book Review67 Practice Development 69 JCRS Highlights70 Eye on History71 Ophthalmologica72 Calendar
1
OCTOBER 2013Volume 18 | Issue 10
EUROTIMESESC
RS ™
Publisher Carol FitzpatrickExecutive Editor Colin KerrEditors Sean Henahan Paul McGinn
Managing Editor Caroline BrickProduction Editor Angela SweetmanAdvertising Executive Mairin Condon Senior Designer Janice Robb
Designer Lara FitzgibbonCirculation Manager Angela Morrissey Contributing Editors Howard Larkin Dermot McGrath Roibeard Ó hÉineacháin Contributors Devon Schuyler Eisele Stefanie Petrou-Binder Maryalicia Post
Leigh Spielberg Pippa Wysong Gearóid Tuohy Priscilla LynchColour and Print W&G Baird PrintersAdvertising Sales ESCRS, Temple House, Temple Road Blackrock, Co. Dublin, Ireland Tel: 353 1 209 1100 Fax: 353 1 209 1112 email: [email protected]
Published by the European Society of Cataract and Refractive Surgeons Temple House, Temple Road, Blackrock, Co Dublin, Ireland. No part of this publication may be reproduced without the permission of the managing editor. Letters to the editor and other unsolicited contributions are assumed intended for this publication and are subject to editorial review and acceptance.
ESCRS EuroTimes is not responsible for statements made by any contributor. These contributions are presented for review and comment and not as a statement on the standard of care. Although all advertising material is expected to conform to ethical medical standards, acceptance does not imply endorsement by ESCRS EuroTimes.ISSN 1393-8983
edito
rial s
taff
EUROTIMESESC
RS ™
Published byThe European Society of Cataract and Refractive Surgeons
As certified by ABC, the EuroTimes average net circulation for the 11 issues distributed between 01 January 2012 and 31 December 2012 is 37,563.

by Rudy Nuijts
It is my pleasure to welcome you to the XXXI ESCRS Congress in Amsterdam, the Netherlands, the birthplace of world-famous ophthalmologists such as Cees Binkhorst and Jan Worst.
The ESCRS is Europe's leading organisation for cataract and refractive surgeons and our annual meeting covers the forefront of innovative developments in anterior segment surgery. ESCRS offers a unique forum for discussion and learning which ensures that international expertise is shared by ophthalmologists all over the globe. The mission of my own Maastricht University, “Leading in learning”, certainly applies to the annual ESCRS meeting. For our young colleagues, residents and fellows, who have free ESCRS membership, ESCRS is offering greatly reduced meeting registration rates. As a Dutch ophthalmologist, I am very proud to be part of a professional organisation that continuously invests in our young generation.
As always the programme consists of free papers, posters, videos, instructional and didactic courses and a practice development day. Hot topics that will be covered in the main symposia are the safety of refractive surgery in risky corneas (in a combined EuCornea-ESCRS symposium), the mixed feelings in our community around the value of femtosecond-assisted cataract surgery, a journey into the mysteries of myopia and new developments in the management of hyperopia and astigmatism during cataract surgery. Scientific symposia will address research topics such as treatment of macular edema, basic research on the crystalline lens and IOLs restoring accommodation, effects of phakic IOLs and the future of corneal stem cells. A new format of an interactive video symposium on surgical complications will take place on Sunday, organised by ESCRS in conjunction with the Netherlands IntraOcular Implant Club (NIOIC).
Education is the main mission of ESCRS and in the past few years a special focus has been the development of a comprehensive educational programme for young ophthalmologists. During the meeting, this consists of a full-day Young Ophthalmologists Programme with lectures on Saturday, the refractive surgery didactic course and the EBO-accredited instructional courses. For young ophthalmologists, ESCRS has established a Europe-wide Observership programme, the podcast series “Eye Chat” and the new e-learning platform “iLearn” which ESCRS members can access free of charge. Of course, the presence of social media like a Facebook page are a “sine qua non” for appropriate communication of the young generation.
Opening Ceremony A highlight of the meeting is certainly the Opening Ceremony where Douglas D Koch will present the Binkhorst Medal Lecture entitled, "The ablated cornea: what have we done?” I am also delighted to welcome delegates attending the EuCornea annual meeting, the ESCRS Glaucoma Day and the EPOS/WSPOS paediatric sub-specialty day.
EuCornea will hold its 4th congress on Friday 4 and Saturday 5 October in conjunction with the ESCRS Congress. The EuCornea programme includes 12 symposia that will cover the whole corneal
field from new areas of corneal research to the latest innovations in lamellar corneal surgery.
Immediately preceding the ESCRS meeting on Friday 4 October, the ESCRS Glaucoma Day will be organised in conjunction with the European Glaucoma Society (EGS). The day will focus on the burden of glaucoma for patients and society, risk factors for disease progression and new surgical approaches for IOP reduction.
We are also looking forward to the European Paediatric Ophthalmological Society (EPOS)/World Society of Paediatric Ophthalmology & Strabismus (WSPOS) subspecialty day which takes place on Wednesday 9 October. Among the topics to be discussed are paediatric ocular surface disease, visual rehabilitation of the aphakic child and novel therapies in glaucoma: can we use them in children?
Well organised As at the previous ESCRS Congresses in Amsterdam in 1995 and 2001, the venue is the RAI convention center which is a modern, convenient congress centre close to the heart of the city. This makes it easy to reach by public transportation.
The compactness of the conference centre facilitates comfortable switches from one session to the other without spending too much walking time. As always, the staff from Agenda have worked effortlessly to guarantee a well-organised meeting.
I am looking forward to welcoming you to Amsterdam and wish you a very enjoyable congress. I am convinced you will have a wonderful time full of education, science and discussion with your peers from abroad. Thank you for supporting the ESCRS and for visiting our country.
2
EDITORIAL Volume 18 | Issue 10
Editorial
ESCRS INNOVATIONThe XXXI ESCRS Congress in Amsterdam, The Netherlands, will celebrate education and science in ophthalmology
José Güell
Clive Peckar
Emanuel RosenChairman
ESCRS Publications Committee
Ioannis Pallikaris
Paul Rosen
Medical Editors
International Editorial Board
EUROTIMESESC
RS ™
Noel Alpins AUSTRALIA
Bekir Aslan TURKEY
Bill Aylward UK
Peter Barry IRELAND
Roberto Bellucci ITALY
Béatrice Cochener FRANCE
Hiroko Bissen-Miyajima JAPAN
John Chang CHINA
Alaa El Danasoury SAUDI ARABIA
Oliver Findl AUSTRIA
I Howard Fine USA
Jack Holladay USA
Vikentia Katsanevaki GREECE
Thomas Kohnen GERMANY
Anastasios Konstas GREECE
Dennis Lam HONG KONG
Boris Malyugin RUSSIA Marguerite McDonald USA
Cyres Mehta INDIA
Thomas Neuhann GERMANY
Rudy Nuijts THE NETHERLANDS
Gisbert Richard GERMANY
Robert Stegmann SOUTH AFRICA
Ulf Stenevi SWEDEN
Emrullah Tasindi TURKEY
Marie-Jose Tassignon BELGIUM
Manfred Tetz GERMANY
Carlo Enrico Traverso ITALY
Roberto Zaldivar ARGENTINA
Oliver Zeitz GERMANY
EUROTIMES | Volume 18 | Issue 10
* Rudy Nuijts MD, PhD, is treasurer of the ESCRS and chairman of the NIOIC (Netherlands IntraOcular Implant Club).


by Colin Kerr
A GLOBAL VISION
When he finishes his term of office as ESCRS president in December 2013, Dr Peter Barry will have led ESCRS
delegations to more than 20 ophthalmology meetings all over the world. The venues for these meetings stretched from Chicago to Tokyo and Rome to Tbilisi.
These visits are not merely courtesy calls, but underpin a strategic goal of the ESCRS to build links and share scientific knowledge and know- how with colleagues across the globe. This level of outreach is a natural extension of the role ESCRS played in the last century consolidating education in cataract and refractive surgery across Europe.
"We should distinguish first of all," Dr Barry told EuroTimes, "between the supraregional meetings hosted by ASCRS, APACRS, ALACCSA and ourselves in ESCRS. Supporting the participation of key ESCRS opinion leaders in these symposia facilitates global communication among leading clinicians in the field and provides outstanding learning opportunities for ophthalmologists across the globe. It also gives ESCRS the opportunity to promote the ethos of the society and to share with an international audience the scientific projects which are supported by ESCRS, including Guidelines on Endophthalmitis Prevention and Treatment, the European Registry of Quality Outcomes for Cataract and Refractive Surgery (EUREQUO) and the PREMED study on prevention of cystoid macular oedema," he said."These activities demonstrate to our colleagues that we have a strong research interest, not just in theory, but in practice."
Attending the supraregional meetings also offers ESCRS the opportunity to promote our annual congresses, said Dr Barry, which is reflected in a progressive increase in attendance from delegates who traditionally had not included the ESCRS meeting on their calendars.
The recently published book, European Society of Cataract & Refractive Surgeons
- A History (1982-2012), documents the origins of the society from its roots as the European Intraocular Implant Club, whose first meeting was held in The Hague in 1982. The burning clinical issue at that time was the future of the IOL and the glue that held this group together was a passionate belief that the IOL would change forever the practice of cataract surgery. The founders also knew that to bring about this change in the face of strong opposition they needed to support rigorous scientific research and communicate this scientific validation to the widest audience possible. This is the ethos that still permeates ESCRS.
National and regional societies The ESCRS sends delegations to national and regional ophthalmology meetings every year. "We have something to offer these societies. Bringing an ESCRS symposium to a regional society is attractive to them because it gives their delegates an
opportunity to interact with key European surgeons and opinion leaders,” said Dr Barry. "In the eyes of delegates in their own countries, the inclusion of ESCRS symposia enhances the quality of their meeting programme. The ESCRS members who present at these symposia are respected on the European and international stage and are welcomed warmly at these meetings."
There are also many regions around the world that do not have access to the newest technology or the quality of training that is available in Europe. "Those are the same areas where frequently doctors do not have the income or the funding to attend international meetings themselves," said Dr Barry. "While the ESCRS supports younger ophthalmologists to attend our meetings through special bursaries, it is very rewarding to attend those national meetings and reach out to doctors who are in many ways isolated from developments and technologies of Western Europe.”
By sending delegations to supraregional, regional and national meetings, the ESCRS is helping ophthalmologists who may not have access to the cutting-edge technologies
EUROTIMES | Volume 18 | Issue 10
Roberto Bellucci addressing the ESCRS/ASCRS/JSCRS joint symposium during the 28th Annual Meeting of the Japanese Society of Cataract and Refractive Surgery in Tokyo
4
ESCRS NEWSCover Story
These activities demonstrate to our colleagues that we have a strong research interest, not just in theory, but in practice
“
Peter Barry
Things have evolved considerably - in a most positive sense and direction - since my presidency
“Thomas Neuhann
The president of the ESCRS is indeed invited by many societies to participate at national and international meetings
“
Marie-Jose Tassignon
Cour
tesy
of H
iroko
Biss
en-M
iyajim
a M
D, P
hD

Past ESCRS president Thomas Neuhann has commented that while the ESCRS has been attending supranational and national and regional meetings since its foundation in 1982, the reason for these visits has changed. "Things have evolved considerably – in a most positive sense and direction – since my presidency," said Dr Neuhann. "When I travelled to national society meetings, it was to get the major players to support ESCRS to get things going and grown. Today ESCRS is well established," he said.
Last May, an ESCRS delegation attended the Black Sea Ophthalmological Society (BSOS) meeting in Tbilisi, Georgia. The BSOS is a federation of ophthalmic societies with representatives from a number of countries including Georgia, Russia, Ukraine, Bulgaria and Turkey.
"In some of those countries," said Dr Barry, "medicine in general is very poor in terms of financing and ophthalmology is particularly poor. In some areas, the standard cataract operation is not accompanied by an intraocular lens implant and if patients require such an implant then the entire procedure becomes a private one which the patient must fund in its entirety. In that environment, it is very difficult for the ophthalmology leaders to sustain the development of their departments. Good trainees travel abroad for fellowships and are very reluctant to return because they are offered positions with a better standard of living for themselves and their families. By sending delegations to meetings like the BSOS we are elevating the level of ophthalmology training in those countries and hopefully in that way we are indirectly encouraging their trainees to return. I believe the ESCRS has a role and responsibility to help develop the practice of ophthalmology in poorer countries.”
Changing role Another former ESCRS president Dr Marie-Jose Tassignon also reflected on the importance of these visits.
"The president of the ESCRS is indeed invited by many societies to participate at national and international meetings," she said. "It is not the ESCRS asking for exposure. This is important to stress because this means that the ESCRS as a society is well respected and its scientific or political messages are considered important by the organisers and the delegates of the inviting society. However, the most important motivation of these national societies is to belong to the ESCRS network and be part of it because the ESCRS has many educational and research benefits to offer, including access to international opinion leaders," she said.
In recent years, the ESCRS has also supported ophthalmologists in developing regions in Europe by organising its winter meetings in eastern European countries. "At our last four winter meetings we have supported ophthalmologists from the local
host countries in Hungary, Turkey, the Czech Republic and Poland and neighbouring countries by offering them a very reduced registration fee," said Dr Barry. "We are also giving trainees three years free membership of the society. We have an Observership Programme which offers bursaries to young ophthalmologists and our writing prize for young ophthalmologists, the John Henahan prize, has a first prize of a travel bursary to allow a young ophthalmologist attend our annual congress," he said.
Developing European Community The ESCRS has always been conscious of the need to be part of the continually developing European community of nations and as that family has grown, so has the society. "If you go back to the very early years of the society and its foundation at The Hague in 1982, we had less than 200 delegates at our first meeting," said Dr Barry. "It was more of a club of those who were committed to the world of intraocular lens implantation. As the council developed and intraocular lens implantation became the norm, the whole stage changed and so did the role of the society. We were no longer pioneering the concept of intraocular lens implantation but the concept of progressively more sophisticated cataract surgery through phacoemulsification and refractive cataract surgery.
“Many of the innovations in cataract and refractive surgery have come from Europe and have been announced at the ESCRS annual meetings. That is why our meetings continue to attract the top ophthalmologists not only from Europe but also from America and the rest of the world," said Dr Barry.
Dr Roberto Bellucci, takes up the position of president in January 2014. He looks forward to continuing this tradition of building educational links with ophthalmologists worldwide.
"Attending international meetings is an important duty for the president," he said, "because ESCRS is introduced to local ophthalmologists, and the level of scientific discourse within the society is explained. They are happy to host us, and consider our lectures and symposia as ‘state of the art’. This communication of scientific knowledge whether through its annual meetings or its support of international and regional meetings is the most important role of the ESCRS.”
5
EUROTIMES | Volume 18 | Issue 10
They are happy to host us, and consider our lectures and symposia as ‘state of the art’
“Roberto Bellucci
Peter Barry – [email protected] Neuhann – [email protected] Tassignon – [email protected] Bellucci – [email protected]
contacts
Wojciech Omulecki, president of the Polish Society of Ophthalmology, pictured with ESCRS president Peter Barry
One of the last national meetings to be attended by Dr Barry is the annual
Spanish Ophthalmological Society (SE0) meeting, September 25-28, Spain, when he delivered the keynote lecture on, "Endophthalmitis prophylaxis - where are we now in 2013?". (This meeting is taking place after EuroTimes goes to press.)
Augusto Abreu, chairman of the SEO Meeting organising committee, and Luis Cordoves, a member of the organising committee, explained the importance of inviting Dr Barry to their meeting.
"We invited Dr Peter Barry because he was the chairman of the ESCRS Endophthalmitis study, the biggest multicentre study ever performed about antibiotic prophylaxis in this area, and some of us had the privilege to take part in it," they said. "His hard work has made intracameral cefuroxime become a standard of care for endophthalmitis prevention in cataract surgery and we believe most Spanish ophthalmologists have adopted its use. We are delighted to hear first-hand how this long story took place and it will support those colleagues who started using 'off-label' cefuroxime with all the possible risks and perhaps convince those who are still skeptical about its use."
Spanish Ophthalmological Society Meeting
William De La Peña MD, chairman of the Board of Directors of
LASCRS (Latin American Society of Cataract and Refractive Surgeons) said it was important that the four supranational societies further their relationship.
“This project now in the form of the joint symposia of LASCRS highlights the concept that even if the world is going global, significant differences still exit," he said. "These differences are not only in care, but also in the system of delivery of care. A variety of economic differences also bring a different perspective. Our symposia, which have been hosted by all four of us, have been of great interest. The attendees have found the symposia very valuable and look forward to the next ones.
"Dr Peter Barry has been a great supporter and a pioneer in this regional alliance. We all are grateful for his leadership as we are to our other pioneering partners. We look forward to coming up with different ideas so that the regional differences can be expressed and we can all learn from them," said Dr La Peña.
Supraregional Meetings
Hiroko Bissen-Miyajima MD, PhD, president of JSCRS said the joint ESCRS/JSCRS
symposium was highly regarded and well attended by Japanese ophthalmologists.
"We appreciate the support of our guest speakers from ESCRS and the joint symposium added important perspectives on new techniques and technologies," she said. "Also, we are glad to know that ESCRS welcomes JSCRS members to attend its annual meeting. Although I have attended ESCRS meetings for many years and have recommended the meeting to my Japanese colleagues, having the ESCRS delegation at our meeting provided an excellent opportunity to introduce ESCRS to JSCRS members.
“It was an equally rewarding experience to work with ESCRS in
planning the joint symposium, which I hope will be carried forward for future meetings. I also hope to build the relationships with my counterparts in Europe," said Professor Bissen-Miyajima.
Japanese Society of Cataract and Refractive SurgeryAn ESCRS delegation attended the 28th annual meeting of the Japanese Society of Cataract and Refractive Surgery ( JSCRS) in Tokyo in June, 2013
It was an equally rewarding experience to work with ESCRS in planning the joint symposium, which I hope will be carried forward for future meetings
“
Hiroko Bissen-Miyajima MD, PhD

Dr Boris Malyugin is the editor of the special Russia language EuroTimes website (www.eurotimesrussia.
org) and a member of the EuroTimes International Editorial Board. He also was one of the organisers of the Russian Society of Ophthalmologists meeting held from 25-27 October 2012 at the Fyodorov Institute in Moscow which an ESCRS delegation attended.
"I believe that organising the ESCRS Academy or ESCRS Symposia or Joint Symposia of the Cataract and refractive Surgery Societies during the major National Ophthalmological Society meetings is an integral part of the ESCRS commitment to education," said Dr Malyugin.
"In the Eastern part of Europe and in the ex-SU states not all ophthalmologists can travel abroad and not all of them are exposed to the latest state-of-the-art technologies. I have to mention here that it is not only the young ophthalmologists in training, but also
a significant number of their older colleagues who do not speak very good English. The latter is a very significant restriction for them even if they can afford travelling abroad. In Russia, by joining efforts with the ESCRS and by organising the symposia that are simultaneously translated, I think we are doing a great job for all these people," he said.
"The ESCRS Academy in Moscow in 2012 was a huge success."
6 Cover Story
ESCRS NEWS
EUROTIMES | Volume 18 | Issue 10
Russian Society of Ophthalmologists
To date, the eye is one of the most successfully targeted organs in the genetic therapy revolution, and paediatric applications are among the most promising. Better testing and treatment could prevent many genetic diseases from ever developing, saving sight for a lifetime. Our November Cover Story will examine the current state of genetic screening for guiding early conventional treatment; genetic screening and treatments that are close to clinical use for conditions including Leber’s congenital amaurosis and choroideraemia; the huge role played by biology such as anti-VEGF; and treatments in the research pipeline, including optogenetic approaches that seek to restore light sensitivity to cells that have lost it. Obstacles to implementing genetic therapies, such as issues with viral vectors and specifically targeting cell layers, will also be discussed.
Genetic medicine: promise and progress in paediatric ophthalmology
COMING SOON IN NOVEMBER EUROTIMES...
The ESCRS Academy in Moscow in 2012 was a huge success
“Boris Malyugin
Black Sea Ophthalmological Society
Prof Merab Dvali, one of the organisers of the Black Sea Ophthalmological Society (BSOS)
Meeting in Georgia, Tbilisi, from May 24-26, said ESCRS symposia helped to significantly increase the level of ophthalmology in the host country.
"Of course in the 21st century, the era of the Internet, one can see a lot and learn a lot, even without attending quite expensive foreign conferences – technology is definitely bringing us closer together. But nothing can be compared to direct communication during the courses or live roundtable discussion after scientific sessions of practical courses or in between the sessions and beyond conference halls.
“Local ophthalmologists have an opportunity to discuss their opinions and new methods of treatments with ESCRS authorities. By breaking down the geographic and psychological borders
we create a team, we share our successes and practices and we learn about challenging cases. But most important of all, by working with the ESCRS we are developing a partnership that will continue for many years to come.
“In my toast at the ESCRS & BSOS Academy Joint Meeting’s farewell banquet, I addressed Peter Barry and said: ‘Please, take care of the East, don’t forget us!’”
Local ophthalmologists have an opportunity to discuss their opinions and new methods of treatments with ESCRS authorities
“
Merab Dvali
The moment you help your patients see the whole picture.This is the moment we work for.
True Living Vision becomes reality with ZEISS AT LISA® tri and the new
ZEISS AT LISA® tri toric. Excellent near, far and intermediate vision. Under
all light conditions. For maximized independency from spectacles.
Visit us at ESCRS at hall 1 booth G02 to learn more about True Living Vision.www.meditec.zeiss.com/escrs
// TRUE LIVING VISION MADE BY ZEISS
AT L
ISA
tri a
nd A
T LI
SA tr
i tor
ic a
re n
ot a
ppro
ved
for s
ale
in th
e U.
S.

Nearly half of Canadian cataract surgeons corrected astigmatism at the time of surgery in 2012, with more than 80 per cent of those using toric lenses, according to a survey by Lindsay
Ong-Tone MB, CHB, FRCSEd, FRCOphth, FRCSC, of the University of Saskatchewan, Canada. Canadian surgeons are also embracing non-steroidal anti-inflammatory drops before and after cataract surgery.
In 2012, 63 per cent prescribed NSAIDs preoperatively with most starting two to three days before surgery, according to the fourth annual survey of Canadian Ophthalmology Society members, which had a 30 per cent response rate. Nevanac (nepafenac ophthalmic suspension 0.1%, Alcon) was the most common choice.
Nearly 90 per cent also used steroid drops postoperatively, with prednisolone acetate the top choice, Dr Ong-Tone reported. However, NSAIDs are gaining for controlling postoperative pain and inflammation.
“It is interesting to note that about 10 per cent used an NSAID drop-only postoperatively while the use of steroid drops-only dropped gradually over the past four years, with a corresponding increase in the use of a combination of NSAID and steroid drops.”
Comparing data Comparing 2011 Canadian data with ESCRS and ASCRS survey data collected by David Leaming MD, preoperative NSAID use was more common throughout North America than in Europe, as was the use of temporal incisions. The top lens material of choice in all three surveys was hydrophobic acrylic. However, hydrophilic acrylic took second place in Canada and Europe, at 26 per cent and 18 per cent respectively, while silicone was the second choice in the US at 16 per cent.
In Canada, the 1-piece aspheric hydrophobic acrylic lenses are gradually gaining popularity as use of the 1-piece aspheric hydrophobic lenses with blue blockers declines slightly, Dr Ong-Tone noted. Use of premium lenses increased in 2011, and maintained gains in 2012, with about 72 per cent using toric lenses and 38 per cent multifocal lenses.
At 66 per cent, intracamerally injected antibiotics were much more commonly used in Europe in 2011, more than
double the Canadian rate of 29 per cent and triple the US rate of 18 per cent, though the US rate continued a gradual increase in 2012 to about 23 per cent (see graphic). For 2012, IC moxifloxacin use doubled to 67 per cent, supplanting vancomycin as the top choice in Canada, Dr Ong-Tone said.
About 80 per cent of Canadian surgeons also use antibiotic eye drops preoperatively, with most starting treatment two to three days before surgery, though about 16 per cent start on the day of surgery. The most common anaesthetic approach was combined topical with intracameral xylocaine, followed by topical xylocaine only.
Gradual trend Divide and conquer was the top Canadian nucleofractis technique at 42 per cent, followed by vertical chop at 23 per cent, Dr Ong-Tone said.
“There is a slow, gradual trend toward divide and conquer with a relative decrease in the vertical chop technique over the years.”
In 2011, more than 13 per cent of Canadian surgeons reported doing simultaneous bilateral cataract surgery compared with eight per cent in Europe and 0.4 per cent in the US. In 2012, the percentage of US surgeons reporting same-day bilateral cataract surgery rose to 0.9 per cent for cataract surgery, while 4.1 per cent of those doing refractive lens exchange said they always try to do same-day bilateral surgery in patients seeking surgery in both eyes, Dr Leaming noted. Reimbursement arrangements may influence the choice as the US Medicare program pays less for a second surgery on the same day than on two separate dates. However, RLE patients also are generally younger and healthier than cataract patients, potentially making them better candidates for same-day bilateral surgery.
Lindsay Ong-Tone – [email protected] Leaming – [email protected]
cont
acts
PRACTICE PATTERNSCanadians embrace toric lenses, hydrophobic acrylic top choice globallyby Howard Larkin
8
EUROTIMES | Volume 18 | Issue 10
Special Focus
CATARACT & REFRACTIVE
2008 2009 2010 2011 2012
25%
20%
15%
10%
5%
0%
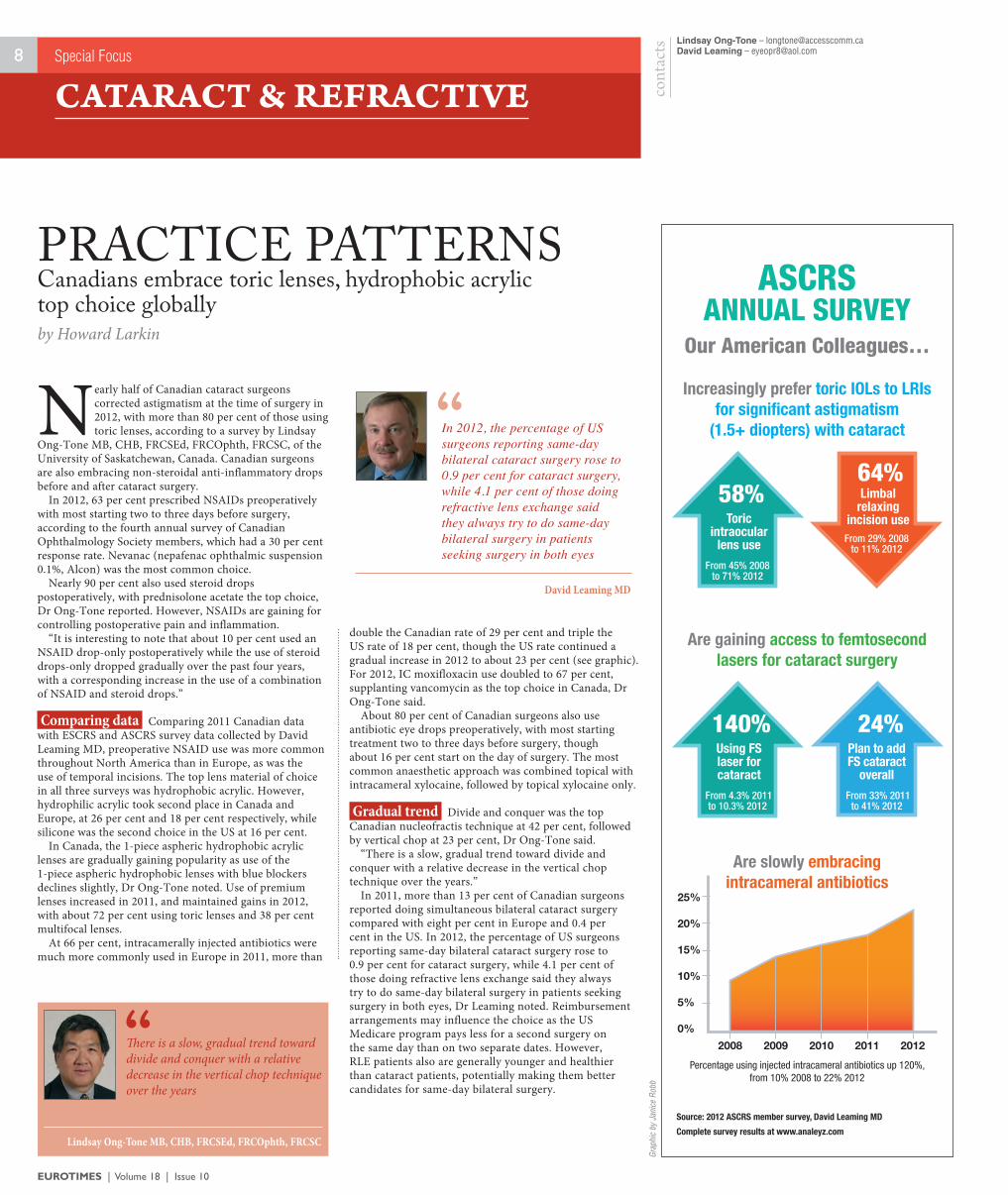
ASCRSANNUAL SURVEY
Our American Colleagues…
Increasingly prefer toric IOLs to LRIs for signifi cant astigmatism
(1.5+ diopters) with cataract
Are gaining access to femtosecond lasers for cataract surgery
Are slowly embracing intracameral antibiotics
58%
140% 24%
64%
Toric intraocular
lens use
Using FS laser for cataract
Plan to add FS cataract
overall
Limbal relaxing
incision use
From 45% 2008to 71% 2012
From 4.3% 2011 to 10.3% 2012
From 33% 2011 to 41% 2012
From 29% 2008 to 11% 2012
Percentage using injected intracameral antibiotics up 120%, from 10% 2008 to 22% 2012
Source: 2012 ASCRS member survey, David Leaming MD
Complete survey results at www.analeyz.com
There is a slow, gradual trend toward divide and conquer with a relative decrease in the vertical chop technique over the years
“Lindsay Ong-Tone MB, CHB, FRCSEd, FRCOphth, FRCSC
In 2012, the percentage of US surgeons reporting same-day bilateral cataract surgery rose to 0.9 per cent for cataract surgery, while 4.1 per cent of those doing refractive lens exchange said they always try to do same-day bilateral surgery in patients seeking surgery in both eyes
“
David Leaming MD
Grap
hic
by J
anice
Rob
b

9
Refractive surgery is safe and effective in patients with strabismus over the longer term, suggests new data presented at
the 2013 Irish College of Ophthalmologists Annual Conference in Killarney, Ireland.
Stephen Farrell MD, Mater Private Hospital, Dublin, presented the study data, which examined the long-term outcomes and safety of refractive surgery on ocular alignment, motor fusion and stereoacuity in adult patients with accommodative and non-accommodative strabismus.
Refractive surgery in this cohort usually carries greater risk, particularly in relation to decompensation of ocular alignment over time, thus careful patient selection is vital.
Under the Irish study, all patients with manifest strabismus undergoing refractive surgery, including LASIK, LASEK or phakic intraocular lens (IOL) insertion, over a 27-month period at a single centre were included. Patients with best-corrected visual acuity (BCVA) of worse than 6/18 in either eye, a greater than two dioptre change in refraction following cycloplegia, and those unavailable for long-term follow up were excluded, Dr Farrell said.
This left 14 patients in the study, who had a mean follow-up duration of 4.5 years (range of 3.5 to 6.5 years). Six of these patients had accommodative esotropia, three had non-accommodative esotropia and five had exotropia.
Following analysis, postoperative uncorrected Snellen visual acuity was found to be within one line of preoperative BCVA in all cases, and no patients suffered from diplopia at follow-up, Dr Farrell told the meeting.
There was also no significant difference between the angle of deviation preoperatively with spectacle correction and postoperatively unaided at follow-up in all groups. Stereoacuity decreased in one patient, increased in four patients and remained unchanged in nine patients.
Dr Farrell said the study confirmed the efficacy and safety of refractive surgery in this cohort over the longer term – no patients developed decompensation of strabismus or diplopia, and ocular alignment unaided remained similar to pre-operative ocular alignment with spectacles.
Safe and effective “This study provides strong evidence that refractive surgery is safe and effective over the longer term. With a mean follow-up of 4.5 years this study provides longer follow-up than any other study published to date, “ he commented.
As well as refractive surgery providing all the benefits of being spectacle-free for these patients, it has now been found to be as effective as glasses at controlling strabismus over the longer term.
“We would always stress the importance of careful patient selection and detailed orthoptic assessment preoperatively, however,” he remarked.
When asked about the potential for paediatric patients, he noted refractive surgery on children is usually for anisometropia rather than strabismus. “With longer follow-up of phakic intraocular lenses in children, they may in the future be an option for patients with strabismus, but given the changing nature of children's refraction spectacles are likely to remain the mainstay of treatment,” he told EuroTimes.
STRABISMUS STUDYRefractive surgery in strabismus patients found to be safe and effectiveby Priscilla Lynch in Killarney
Stephen Farrell – [email protected]
contact
C
M
Y
CM
MY
CY
CMY
K
add-vsybio.pdf 1 9/5/13 11:30 AM
EUROTIMES | Volume 18 | Issue 10
Special Focus
CATARACT & REFRACTIVE
This study provides strong evidence that refractive surgery is safe and effective over the longer term. With a mean follow-up of 4.5 years this study provides longer follow- up than any other study published to date
“
Stephen Farrell MD

10
A recent French study adds to the growing number of reports suggesting that the femtosecond laser can provide improved
control and precision for key steps of the procedure for cataract removal, according to Jean Claude Rigal-Sastourne MD.
Addressing delegates attending the annual meeting of the French Implant and Refractive Surgery Association (SAFIR) annual meeting, Prof Rigal-Sastourne, an ophthalmologist at the Hôpital Percy in Clamart, Paris, said that the femtosecond laser enables surgeons to achieve greater precision, control and reproducibility in their cataract treatments.
“In our experience, cataract removal with the Victus femtosecond laser (Bausch + Lomb) is an easy, reliable and safe procedure to perform capsulotomy and achieve smooth lens fragmentation. It enables us to create accurate, well-centred anterior capsulotomies, which may lead to better IOL positioning and overlap,” he said.
Prospective study Prof Rigal-Sastourne’s prospective study set out to compare the results between cataract surgery performed by femtosecond laser and by traditional manual methods looking at three key areas: capsulotomy, ultrasound time and effective lens position after surgery.
The study included 32 eyes of 24 patients operated for cataracts using bimanual MICS and implanted with the Micro AY lens implant (PhysIOL). Half the eyes were treated using the femtosecond laser and half with traditional manual methods. Postoperative examination took place at one week and one month after surgery.
Creating the capsulotomy with the femtosecond laser was found to be an efficient and effective technique with easy removal of the rhexis and without any adverse events. Moreover, the laser-created capsulotomies were significantly more precise in size and shape than manually created capsulorhexes, said Prof Rigal-Sastourne.
The intended capsulotomy diameter in the study was 5.2mm, although the software on the Victus machine allows the size to be customised, said Prof Rigal-Sastourne. After seven days postoperatively, the mean diameter of the
capsulorhexis for the Victus group was 5.35mm (± 0.22mm), with 85 per cent of the rhexis within ±0.35mm of the targeted diameter.
A round and symmetric capsulorhexis with the anterior lens capsule overlapping the optic’s edge is optimal for accurate postoperative IOL centration, noted Prof Rigal-Sastourne, with this goal achieved in 100 per cent of the femtosecond- created rhexes.
For the manual capsulorhexis patients, the intended diameter was 5.5mm, whereas the actual diameter of the rhexis after seven days was 6.1mm (±-0.21mm), with 15 per cent of eyes within ±0-35mm of the targeted diameter.
Capsulotomy A statistically significant difference in the circularity of the capsulotomy using the femtosecond laser compared with the manual technique was also observed. Centration was also better with the femtosecond group, said Prof Rigal-Sastourne.
He added that a number of different lens fragmentation patterns, such as ring or radial cuts, can be used and applied depending on the cataract grade. Using the femtosecond laser seems to enable easier cracking of the nucleus following lens fragmentation, which reduces the phaco energy required for lens removal.
“The average reduction of ultrasound energy being delivered into the eye was about 35 per cent in our study, which means greater protection for the endothelial cells and less trauma to the eye,” said Prof Rigal-Sastourne.
The study also found improved effective lens position (ELP) with the eyes treated by femtosecond laser. The reproducible, central and circular capsulorhexis created by the femtosecond laser is a prerequisite for good postoperative effective lens position, especially with the latest premium IOLs, said Prof Rigal-Sastourne. IOL power calculations were also more accurate in the femtosecond-treated eyes, leading to better refractive outcomes.
Jean Claude Rigal-Sastourne – [email protected]
contact
IMPROVED CONTROLFrench study highlights advantages of femto-cataract procedureby Dermot McGrath in ParisMaster your refractive outcomes
with the LENSTAR LS 900Venue: ESCRS at Amsterdam RAIDate: Saturday October 5, 2013Time: 13:00 – 14:00Room: D203 / 204
Chairman:Dr. Thomas Olsen (Denmark)
Speakers:Dr. Warren Hill (USA)First experience with the LENSTAR T-Cone topography add-on and toric IOL planning
Dr. Eduard Meier (USA)Excellent refractive outcomes with 5th generation IOL calculation formula: The Olsen vs. Holladay 2 Formula, which road to go
Dr. H. John Shammas (USA)Improved cataract penetration using DCM Mode and Shammas no-history for prior hyperopic post refractive cataract patients with the LENSTAR
www.haag-streit.com
ESCRS Lunchtime Symposium
LENSTAR LS 900®
Biometry
ADV_Lensstar_Eurotimes_ESCRS'13_23-08-2013.indd 1 23.08.2013 09:35:04EUROTIMES | Volume 18 | Issue 10
Special Focus
CATARACT & REFRACTIVE

SCHWIND eye-tech-solutions · fon: +49 6027 508-0 · email: [email protected] · www.eye-tech-solutions.com
Performance in an entirely new dimension – SCHWIND AMARIS® 1050RS.
Experience the evolution of innovation with the most powerful excimer
laser from the technology leader. Its 1050 Hz repetition rate provides for
an extremely short ablation time of just 1.3 seconds per dioptre. Equipped
with 7D eye tracking, this pioneering laser system makes it possible to
achieve an ablation without latency. The result is an unsurpassed level of
precision and patient comfort. SCHWIND AMARIS 1050RS – the newest
TotalTech Laser of the SCHWIND AMARIS family.
Impressively evolutionaryThe SCHWIND AMARIS® 1050RS
AMARIS® 500EAMARIS® 1050RS AMARIS® 750S
• 1050 Hz Repetition Rate – unprecedented
• Extremely short ablation time
• Maximum precision thanks to 7D eye tracking
• Latency-Free Tracking
• Intelligent Thermal Effect Control
• Online Pachymetry
• Extraordinarily broad treatment spectrum
1050 Hz Repetition Rate7D Eye Tracking
130830_AZ_AMARIS_1050RS_270x320+5_UK_RZ_v1-0.indd 1 30.08.13 11:09

LASIK approaches that combine increased depth of field with micro-monovision are yielding some of the best results yet for
laser correction of presbyopia. However, the approximately 1.5 D add effect achieved with presbyLASIK is not enough for most older patients, presenters told the 2013 American Society of Cataract and Refractive Surgery (ASCRS) symposium.
“The procedure is time limited. Presbyopia increases with age as well as with changes in the crystalline lens,” said W Bruce Jackson MD, FRCSC, University of Ottawa, Ontario, Canada.
Improvements in near vision with presbyLASIK also come at the expense of some loss of distance vision, and some patients have trouble adjusting, Dr Jackson added. Outcomes are generally less predictable than with standard LASIK, resulting in retreatment rates ranging up to 30 per cent.
Ocular surface instability is another factor that affects patients' vision and satisfaction, and must be well controlled for best results, Dr Jackson said.
Monovision, with the ideal correction of plano in the dominant eye and about -1.5 D in the non-dominant eye, remains the most common laser presbyopia treatment. It is also the only currently approved option in North America.
Patient satisfaction with monovision in published studies ranges from 72 per cent to 96 per cent, with two per cent to seven per cent wanting reversals, Dr Jackson said. Enhancement rates run about 20 per cent, with retreatment of the distance vision eye more common. Drawbacks include a slight decrease in binocular distance visual acuity, reduced contrast sensitivity and problems with stereopsis.
Contact lens trials are not always a good predictor of monovision success, Dr Jackson said. Patient selection is critical and
expectations must be reasonable as glasses are often required for distance or near vision.
Several manufacturers, including VISX/AMO, Schwind and Technolas PerfectVision, offer presbyLASIK ablation profiles with a near vision zone in the corneal centre, Dr Jackson said. In a company-sponsored trial he conducted with the VISX/AMO S4 using a bilateral wavefront-guided hyperprolate central 3.0mm near ablation profile, 100 per cent of 66 patients achieved 20/25 distance and J3 or better near at 12 months, with 88 per cent at 20/25 and J1 or better.
Mesopic contrast sensitivity declined slightly from pre-op values, but remained well within normal range. Sixty per cent lost no distance Snellen lines, 28 per cent lost one line and 10 per cent lost two lines, while 1.7 per cent gained one line. Distance vision improved between six months and 12 months after surgery, with improved control of tear film mostly responsible, he reported.
Spectacle free “We met our target of 20/25 and J3 in all eyes at one year. However, only one-third were spectacle free, with the others using glasses at some time during the day or week,” Dr Jackson said.
Overall, published studies show about 85 per cent of patient treated with central near presbyLASIK performed with VISX, Schwind and Technolas systems achieved 20/25 to 20/30 and J3, with three to 10 per cent losing two lines corrected distance vision from pre-op refractions of -7.0 to +3.5 D, Dr Jackson said.
However, outcomes with the same equipment and parameters are variable depending on patient selection and
technique, he noted. Generally, though, hyperopes were more satisfied and myopes more spectacle dependent with the central near add approach.
VISX, Technolas, Nidek and Wavelight all offer peripheral, or paracentral, near add profiles, which induce negative spherical aberration about 2.5mm from the corneal vertex, increasing depth of field. Studies show about 80 per cent achieved 20/25 to 20/30 and J3 from -8.25 to +4.0. Myopes were more satisfied than hyperopes with the peripheral add approach. Enhancements range from 2-30 per cent.
However, peripheral add performance is highly pupil dependent, said Sri Ganesh MD, Bangalore, India. “Miotic near performance is degraded and when the pupil dilates, distance vision is compromised.”
Dual construction By contrast, central add performance is enhanced by pupil constriction. Peripheral add also requires more neuroadaptation and distance vision recovery takes longer, he added. Treatment times are also longer with more tissue removed.
Laser blended vision, pioneered by Dan Reinstein MD with the Carl Zeiss Meditec MEL 80 excimer laser, uses non-linear aspheric ablation profiles to increase depth of field in both eyes, combined with monovision. The dominant eye target depth of field is plano to -0.75 D and the non-dominant nominally -1.5 D with a field depth from -0.75 to -2.25. The overlap in field depths is intended to promote stereopsis and improve distance, intermediate and near vision with low corrections.
In a test of a similar approach with a Nidek system, 60 eyes of myopes underwent optimised prolate ablation for presbyopia, with a spherical aberration target of -0.3 microns in both eyes and the non-dominant eye targeted at -0.75 D, Dr Jackson said. Seventy-six per cent achieved 20/25 and J2 uncorrected.
“The new generation of bi-aspheric centre near ablation profile combined with micro-monovision shows promising results. Laser blended vision with enhanced depth of field in both eyes may be a good option,” Dr Ganesh said.
W Bruce Jackson – [email protected] Ganesh – [email protected]
cont
acts
Newer ablation profiles improve results, but correction range still limitedby Howard Larkin in San Francisco
12
PRESBYOPIC LASIK
EUROTIMES | Volume 18 | Issue 10
9th International Congress of Corneal Cross-Linking
December 6-7 2013
Dublin / Ireland
The CXL Congress is an international forum for the most recent advance in corneal cross-linking
For more information please contact: CBS Congress & Business Services Technoparkstrasse 1, CH-8005 Zurich, [email protected] Switzerland Registration: www.cxl-congress.com
PROGRAM: FRIDAY, DECEMBER 6th One day instructional course on CXL - all levels SATURDAY, DECEMBER 7th Scientific presentation, laboratory science, clinical results and latest developments
www.cxl-congress.com
www.cxl-congress.com
Special Focus
CATARACT & REFRACTIVE
We met our target of 20/25 and J3 in all eyes at one year. However, only one-third were spectacle free, with the others using glasses at some time during the day or week
“
W Bruce Jackson MD, FRCSC
“The new generation of bi-aspheric centre near ablation profile combined with micro-monovision shows promising results”Sri Ganesh MD

FUSION Pump Fluidics Management
ELLIPS FX Handpiece Ultrasound Energy Management
Proven peristaltic pump provides excellent holdability
Advanced venturi pump provides outstanding followability
ELLIPS FX Handpiece delivers smooth cutting and excellent efficiency
WHITESTAR SIgnATURE SyStem with
FUSION PHACO Technology
This ad is not approved for Algeria, Montenegro, Albania, Macedonia, Kosovo, and Moldavia as the WHITESTAR Signature System is not registered in these countries.
WhITeSTAR Signature, FUSIon, and ellIPS are trademarks owned by or licensed to Abbott laboratories, it subsidiaries or affiliates. © 2013 Abbott Medical optics Inc. www.AbbottMedicaloptics.com2013.05.28-cT7022
Experience FUSION PHACO Technology. www.WHITESTARSignature.com
PhAg-11527 eAM Fusion Phaco Trade Ad-eT.indd euroTimes 0 7/30/13
245mm x 300mm 270mm x 320mm +5mm 100%

A new ‘dry lab’ training methodology for phacoemulsification surgery may prove to be a useful adjunct to traditional training methods, suggests research presented during the 2013 Irish
College of Ophthalmologists Annual Meeting.Princeton Lee MD, an ophthalmic surgery specialist
registrar in the Royal Victoria Eye and Ear Hospital, Dublin, Ireland, has developed a new programme for teaching phacoemulsification surgery. He presented the pilot study results at the conference.
While learning phacoemulsification is an exciting process for trainees, the learning process can be slow and risky for patients due to the high skill-set required to perform the surgery, he noted.
Dr Lee said he thus set out to design a proficiency-based training methodology that would increase trainees’ confidence, reduce training costs and improve patient safety. The programme consists of both didactic and practical skill components and takes place in a real operating theatre using real surgical instruments utilising a plastic model eye to
build up trainees’ surgical skills. The skill training focuses on imitating the instrument manoeuvring inside the plastic eye, therefore, no consumable components such as artificial capsules and lens materials are required.
Traditionally, trainees learn by repeating the same step on patients a few times before moving on to the next step. This training programme requires the trainees to master the knowledge and skills required in all steps before starting to operate on patients. After each step was learned, the trainees rehearsed the entire operation repeatedly until thorough familiarity with the procedure was achieved. Once competency was reached, the trainees then commenced cataract surgery on a real patient, Dr Lee said.
The success of the study was determined by the number of patients required by the trainee to complete a full case under the supervision of their hospital trainer without any intervention.
Two trainees without prior ophthalmic surgical experience took part in Dr Lee’s pilot study of this new training programme. The trainees spent an average of 50 hours on lectures, reading and practising their manual skills. They learned proper microscope operation, effective instrument handling and manoeuvring, and then learned how to precisely control the phaco machine with their foot.
When operating on real patients they reached their first fully completed, unaided case after an average of six patients (range of 4-8 patients), compared to a random survey of Irish trainees who were trained in the traditional way who reached their first unaided completed case following an average of 36 patients, Dr Lee told the conference.
“At the end of the training programme, trainees developed a thorough understanding of the procedure and good eye-hand co-ordination. Therefore when it came to their very first case, they were more confident as nothing was unfamiliar, except for the handling of biological tissues,” he stated.
Dr Lee said the effectiveness of the new training programme is evident by the small number of patients the trainees needed to complete their first full case.
Furthermore, as training takes place primarily away from actual patients, it is safer. It is also cheaper because there are no consumable components or replaceable technology required.
“It incurs minimal cost yet achieves the most direct transfer of skill from a dry lab to the operating room,” he commented.
Concluding, Dr Lee said his dry lab training model addressed the key concerns of effectiveness, safety and cost and offers a real alternative to traditional phaco surgery training methods.
PHACO TRAININGNew dry lab training system for phacoemulsification surgeryby Priscilla Lynch in Killarney
14Princeton Lee – [email protected]
cont
act
EUROTIMES | Volume 18 | Issue 10
Special Focus
CATARACT & REFRACTIVE
At the end of the training programme, trainees developed a thorough understanding of the procedure and good eye-hand co-ordination. Therefore when it came to their very first case, they were more confident as nothing was unfamiliar, except for the handling of biological tissues
“
Princeton Lee MD
An eye model created by Dr Lee for practising lens rotating manoeuvre with a second instrument
A trainee practising foot pedal control for phaco machine at the end of a case
Cour
tesy
of P
rince
ton
Lee
MD
EUROTIMESESC
RS ™
INDIA
VISIT OUR WEBSITE FOR INDIAN DOCTORS
www.eurotimesindia.org
IOLs with rigid unbending haptics are likely to have the most predictable effective lens position and postoperative refraction, according to Albert Galand
MD, PhD, Liege, Belgium. In a study presented at the 26th
International Congress of German Ophthalmic Surgeons in Nurnberg this year, Dr Galand reviewed the refractive results achieved with three different types of IOLs. His findings showed that the refractive results fell within a tighter range in eyes with IOLs with rigid closed-loop haptics than in eyes with IOLs with conventional C-loop haptics.
Dr Galand, former head of the Ophthalmology Department at the Hospital of the Université de Liege, Belgium, noted that the effective lens position is the key determinant of the refractive result in eyes that have undergone implantation of an IOL.
However, the effective lens position can be inconsistent from patient to patient when the lens is in the capsular bag. That is because the implanted lens is much smaller than the natural crystalline lens it replaces and because capsular fibrosis and contraction can cause the haptic to bend in such a way as to push the optic forward or backward.
“If the haptic is very soft in the anterior-posterior direction, the optic position, vis-à-vis the equator location, will be rather varying, particularly when the capsule has fibrosed,” he said.
There were three groups of 30 patients in the study. Each group received one of three IOL models, namely, the AcrySof ® SA60AT (Alcon), the Tecnis® ZCB00 (AMO), and the SAV-MultiLink (Swiss Advanced Vision). The AcrySof and Tecnis IOLs are composed of a hydrophobic material and have conventional C-loop haptics. The SAV-MultiLink IOL is composed of a hydrophilic material and has rigid closed-loop haptics. All are uniplanar without vaulting. None of the IOLs in the study had a dioptric power under 20.0 D or more than 25.0 D.
Dr Galand and his associates performed IOL calculations with measurements made with the IOLMaster (Zeiss) and the SRK-T formula with an A-constant 118.6.
One year postoperatively, the spherical equivalent refraction prediction errors, as measured by the Nidek refractometer,
ranged -0.65 D to +1.5 D in the AcrySof group, from -0.6 D to +2.20 D in the Tecnis group and from -1.75 D to -0.05 D in the SAV-MultiLink group. Therefore, the dispersal of prediction errors was 2.15 D and 2.80 D respectively, in the AcrySof and Tecnis group, compared to only 1.70 D in the SAV-MultiLink group
He noted that the difference in dispersal values did not reach statistical significance and should therefore be regarded as a trend.
VISIT US at Booth B07
• Hydrophobic Acrylic – Non Stick• CVA = ±0.3 Diopter*• Stable and Dependable Performance• Preloaded• Made in USA
MBI Family of IOL’s
A family experience...
360 E. Bonita Ave.Pomona, CA 91767 USAwww.mbius.com
“We let the family do the talking”
Aspheric Toric Multifocal
*As reported in a special study in Australia.
Albert Galand – [email protected]
cont
act
Special Focus
CATARACT & REFRACTIVE15
IOL STUDYRange of refractive errors lower with rigid closed-loop haptics by Roibeard O’hEineachain
EUROTIMES | Volume 18 | Issue 10
If the haptic is very soft in the anterior-posterior direction, the optic position, vis-à-vis the equator location, will be rather varying...
“
Albert Galand MD, PhD,

EUROTIMES | Volume 18 | Issue 10
The idea of using lasers to emulsify cataracts is nothing new, but in fact goes back over 30 years to a time when ECCEs accounted for
most cataract surgeries, said Lucio Buratto MD who presented his personal perspective on the development of laser-assisted phaco at Femto 2013, an international meeting on anterior segment surgery.
“Over the years of my surgical life I've had many wonderful experiences and one of the best has been to participate in the evolution of lasers for performing cataract surgery,” said Dr Buratto, Milan, Italy.
He noted that the original idea of using a laser was to perform a capsulorhexis and/or emulsify the lens from the outside of the eye. The earliest use of lasers in relation to cataract surgery was in 1982 when Franz Fankhauser performed the first laser posterior capsulotomy on a human patient with a neodymium: yttrium aluminium garnet (Nd:YAG) laser. The indication for treatment in this case, as in most cases today, was a posterior capsulotomy to remove posterior capsule opacification.
Dr Fankhauser had worked closely with Danièle Aron-Rosa MD in the development of the Nd:YAG laser. Their research showed that application of the laser in this way was unlikely to damage the surrounding tissue. However, he was reluctant to use the laser out of fear that it might damage the lens. He nonetheless performed the procedure and saw that the lens remained intact, thus beginning a new era in ophthalmic surgery.
The following year, Dr Buratto began using the Nd:YAG laser for performing anterior capsulotomies during cataract surgery. He used the laser to pierce holes in the capsule in the style of a can-opener capsulotomy. However, he found that while it was generally possible to perform an anterior capsulotomy in this way, in many cases there were problems with pupil constriction and there were pronounced anterior chamber reactions. He therefore decided that the bent-needle cystotome anterior capsulotomy technique was better.
A decade later, in 1993, the introduction of picosecond lasers for cataract surgery renewed Dr Buratto’s interest in laser-
assisted cataract surgery. Leading the research was Vincenzo Marchi MD in Rome, who demonstrated that it was possible to perform anterior capsulotomy and nucleofragmentation with the laser. Like the Nd:YAG laser and the femtosecond lasers of today, the picosecond laser was designed to perform procedures on the inside of the eye from the outside of the eye.
“I was almost ready to buy a laser but finally I decided not to because it didn't
really look all that promising for the future,” Dr Buratto said.
The close of the millennium saw the introduction of several lasers that were designed basically as laser versions of ultrasound phacoemulsification devices. The first to come along was an erbium:YAG laser which had a fibre-optic probe deliver the laser pulses in a non-contact mode to induce photo vapourisation.
Next came the Paradigm Nd: YAG laser which had a wavelength of 1064 nm and like the erbium YAG laser transmitted laser energy through a fibre optic probe. Unlike the erbium:YAG laser, which applied energy directly to the cataract, the Paradigm laser shot its beam at a titanium target to create shockwaves causing optical breakdown and plasma formation.
Unfortunately for the new technology, lasers were still playing catch-up with ultrasound phacoemulsification, which at the time was itself undergoing a steady evolution, with greatly reduced effective phaco times. Therefore, Dr Buratto and most ophthalmologists could not see any advantages in the new lasers.
“One drawback was that they didn't work as well in hard cataracts, which we still were doing fairly frequently back in those days. Nowadays, we mainly treat softer cataracts,” he added.
Finally in 2000, Dr Buratto began using the ruby phaco laser which he said was quite effective in emulsifying cataracts with few complications. However, he became disenchanted with the machine when he had a case where there was a posterior capsule rupture and a dropped nucleus.
“We were initially happy with this machine and we didn't have that many complications, but when I had a case where I lost the nucleus into the vitreous after rupturing the capsule, I realised it had no safety advantages over ultrasound phacoemulsification,” he said.
He noted that the introduction of femtosecond laser-assisted cataract surgery in recent years has brought laser cataract surgery full circle, returning once more to an ab externo technique. This became possible not only because of the lasers themselves, but also because of the concurrent emergence of highly reliable imaging technology, such as Scheimpflug cameras and OCT devices which guide the lasers with extreme precision.
“Femtosecond laser-assisted seems to solve all the problems we had with previous lasers, so I think with this new technology we're moving in the right direction,” Dr Buratto added.
Lucio Buratto – [email protected]
cont
act
LASERS FOR CATARACTSFemtosecond laser-assisted cataract surgery a product of decades of researchby Roibeard O’hEineachain in Verona
16 Special Focus
CATARACT & REFRACTIVE
Lucio Buratto and his staff ready to perform a case of femtolaser-assisted cataract surgery
Over the years of my surgical life I’ve had many wonderful experiences and one of the best has been to participate in the evolution of lasers for performing cataract surgery
“
Lucio Buratto MD
“One drawback was that they didn’t work as well in hard cataracts, which we still were doing fairly frequently back in those days. Nowadays, we mainly treat softer cataracts”
Don’t Miss Eye on Technology, see page 56
Cour
tesy
of L
ucio
Bur
atto
MD
Ultra PureIOL MaterialsBenz Quality. Benz Innovation.
99.9% Pure Raw Material Has Its Advantages
6.5 Million Hydrophilic Implants Per Year
Zero Recalls
Benz Research & Development benzrd.com

There is currently no peer-reviewed evidence supporting the idea that femtosecond-assisted cataract surgery is safer and more effective than traditional phacoemulsification techniques in
routine cataract cases, George H H Beiko BM, BCh, FRCSC reminded delegates attending the 2013 Congress of the Society of European Ophthalmology.
“We know that the femtosecond lasers can be used to create corneal incisions, capsulotomies and to liquefy and fragment the lens. However, if you look carefully at all these indications there is currently no peer-reviewed data to support the case for doing femtosecond laser cataract surgery,” said Dr Beiko.
Dr Beiko, assistant clinical professor of ophthalmology at McMaster University, Ontario, Canada, noted that femtosecond technology is not the first laser technology that has been used over the years to remove cataracts.
“We have seen various systems and devices such as Daniel Eichenbaum’s YAG laser, Jack Dodick’s NG-YAG laser and Michael Colbert’s erbium YAG laser, all of which have fallen by the wayside and have not stood the test of time for routine cataract cases,” said Dr Beiko.
Some of the femtosecond laser systems currently on the market are FDA approved, but none have actually undergone controlled FDA-approved trials, said Dr Beiko.
“All have been approved through a side system which allows them to come into use without any FDA-approved trials,” he said.
In economic terms, Dr Beiko said it was very hard to make a compelling case for femtosecond laser use in cataract surgery.
“The cost to our hospital (in Canada) is about $650 for a routine cataract case. That is the direct and indirect cost, including nurses, the hospital and the capital cost. For femtosecond cataract surgery, we add in the cost of the laser, which is typically about $500,000, a maintenance contract which is about $40,000 a year and then there is the click fee of about $400 dollars per case. Depending on the volume of the practice, this works out to a charge between $1,500 and $2,500 dollars per case, which is a very significant difference indeed,” he said.
While it has been suggested that femtosecond cataract surgery results in better self-sealing incisions, more accurate reduction of astigmatism, better quality of vision and faster visual recovery, scrutiny of the scientific literature shows little evidence to back up these claims, said Dr Beiko.
Taking the example of astigmatism, Dr Beiko said laser correction is possible for the 35 per cent to 40 per cent of patients with astigmatism between 0.75 D to 2.0 D.
“We know that using toric lenses and limbal relaxing incisions is comparable in that range. So you are effectively spending $1,500 to $2,500 dollars for a technology to do what a toric lens can already do at a significantly reduced cost,” he said.
Dr Beiko noted that studies by Nagy et al. have shown that the femtosecond laser is more reproducible and
accurate than manual methods for creating capsulotomies. “However, Burkhard Dick has shown that using a data-
injection system (DIS, Carl Zeiss Meditec) to project a reference ring onto the anterior capsule can accomplish a similar level of accuracy for the capsulotomy as with a femtosecond laser,” he said.
A recent study by J A Davison of 468 patients showed that an incomplete overlap of the optic in one or more quadrants versus a complete overlap resulted in only 0.12 D more myopia, said Dr Beiko.
“In other words, if you do not have a perfect capsulotomy it is about one-eighth of a dioptre of difference compared to having a perfect capsulotomy. So having a perfect capsulotomy does not seem to impact that much on the end result,” he said.
The idea that femtosecond cataract surgery results in much less energy being delivered into the eye should also be placed in its proper context, said Dr Beiko.
“We have seen studies by Dr Nagy and others showing that they can reduce the amount of phaco energy into the eye by around 50 per cent by using femtosecond technology. However, I presented a study back in 2002 showing how to use the Akahoshi pre-chopper to reduce phaco energy by as much as 55.79 per cent in my cases. And the chopper is much cheaper than the laser and there is no click fee to use it,” he added.
On the subject of anterior and posterior capsular tears, Dr Beiko said that their incidence seemed to be related more to the experience of the surgeon than the type of technology being used.
“One study shows that four per cent of the first 200 cases had anterior capsular tears with femtosecond laser and just 0.3 per cent in the subsequent 1,300 cases. With traditional phaco, another study showed the rate of anterior capsular tears in the first 300 cases was five per cent and less than one per cent thereafter. The same also holds true for posterior capsular tears, with experienced phacoemulsification surgeons reporting tear rates of less than one per cent which is in the same range as femtosecond technology,” he said.
18
EUROTIMES | Volume 18 | Issue 10
FEMTO CATARACTMore compelling evidence is needed for femtosecond cataract surgeryby Dermot McGrath in Copenhagen
Special Focus
CATARACT & REFRACTIVE
contact George Beiko – [email protected]
All have been approved through a side system which allows them to come into use without any FDA-approved trials
“ George H H Beiko BM, BCh, FRCSC
Goodbye Phaco, Hello FemtoDr Oliver Findl talks with Dr Burkhard Dick about how femto cataract surgery appears to offer greater accuracy and consistency, while reducing or eliminating the need for phaco.
EYE CHAT
Exclusive interviewsUp to date informationProblem solving
Scan this QR code to gain access to EuroTimes podcasts
podcastwww.eurotimes.org
Also available on iTunes
Photorefractive keratectomy (PRK) in eyes with suspected keratoconus appears to be safe and effective in carefully selected patients,
according to a long-term study presented at the French Implant and Refractive Surgery Association (SAFIR) annual meeting.
Jean-Marc Ancel MD, in private practice at Clinique Lamartine in Paris, presented five-year data from a retrospective study of 29 eyes of 16 patients who were classified as having forme fruste keratoconus.
“Five years is the minimum follow-up time needed to observe whether or not there was a progression in the disease. We found that the refractive results were stable and there was no evidence of any evolution towards ectasia for any of the patients,” he said.
Dr Ancel said that the results showed very good long-term refractive stability and topographic integrity for PRK treatment in selected keratoconic eyes and accorded with data presented recently by Damian Gatinel et al.
“In preserving the biomechanical properties of the anterior stroma, PRK allows us to perform a refractive treatment for these selected patients with suspected or confirmed keratoconus without any additional risk as compared to PRK performed on a healthy eye,” he said.
Dr Ancel noted that suspect topography indicative of keratoconus usually constitutes a formal and definitive contraindication for all LASIK refractive surgery owing to the obvious risk of post-operative ectasia.
“On the same basis, patients with advanced or progressive keratoconus may only rarely benefit from a refractive correction by photoablation. However we are now seeing more teams proposing PRK as a possible refractive solution for either suspect or ‘forme fruste’ keratoconus, or confirmed keratoconus in combination with intracorneal rings or crosslinking. At the moment, less than 10 cases of postoperative ectasia have been reported in the scientific literature after PRK without any pre-selection in terms of whether the patients were at risk or not,” he said.
The goal of Dr Ancel’s study was to evaluate the refractive efficacy as well as biomechanical stability of PRK treatments in keratoconus patients over time.
“We wanted to see if there was any deterioration of the initial topographical anomalies. All patients in our study had stable preoperative refraction and a best corrected visual acuity close to 10/10,” he said.
After one year, the refractive results were in conformity with those known for PKR in myopes in the scientific literature, said Dr Ancel.
“We had the same safety margins with no loss of lines of best-corrected vision and a mean BCVA of 9.7/10. After five years, we see that the refractive results are perfectly stable and there is no trend towards ectasia in any of the patients,” he said. Those results were confirmed over five years.
Summing up, Dr Ancel said that the overall outcomes of these forme fruste or confirmed keratoconus patients were very satisfactory.
PRK TREATMENTStudy evaluates refractive efficacy in keratoconus patientsby Dermot McGrath in Paris
Jean Marc Ancel – [email protected]
contact
19
MORIA S.A. 15, rue Georges Besse 92160 Antony FRANCE Phone: +33 (0) 1 46 74 46 74 - Fax: +33 (0) 1 46 74 46 70
[email protected] - www.moria-surgical.com
Single-UseInstruments
Corneal Vacuum Punch• Diameters from
7.00mm to 9.50mm• Top lateral window• 20 vacuum holes and
4 cardinal holes
Vacuum Trephine• Designed to produce
straight-walled cuts and no parallax errors
• Accurate centration indicator
• Adjustable preset depth setting
Compatible with a Moria Single-Use Artificial Chamber to cut the donor cornea from the epithelial side.
ESCRS Amsterdam October 5-8, 2013
Come and visit us at Moria booth #E04
EUROTIMES | Volume 18 | Issue 10
Special Focus
CATARACT & REFRACTIVE
Don’t Miss Eye on Travel, see page 60
Five years is the minimum follow-up time needed to observe whether or not there was a progression in the disease. We found that the refractive results were stable and there was no evidence of any evolution towards ectasia for any of the patients
“
Jean-Marc Ancel MD
London2014
XXXII Congress of the ESCRS
13-17 September
www.escrs.org
Instructional CourseSubmission Deadline:
31 October 2013

Fungal keratitis continues to be a major cause of corneal blindness in some areas of the world, and yet treatment of these sight-threatening
infections has not received the research attention it deserves.
Therefore, the Mycotic Ulcer Treatment Trial (MUTT) is noteworthy for being a rigorous prospective study addressing this important therapeutic area and particularly because it generated clear, but unexpected results showing that natamycin five per cent is superior to voriconazole one per cent as topical treatment for filamentous fungal keratitis. This study was a collaborative effort between Aravind Eye hospitals in India and Proctor foundation in the US and was funded by the National Eye Institute.
Speaking on behalf of his collaborators, Venkatesh Prajna MD, MUTT principal investigator, discussed the study’s recently published findings at the first Cornea Day during the 26th Asia-Pacific Association of Cataract & Refractive Surgeons Annual Meeting.
Dr Prajna told attendees that in this large, randomised, double-masked study’s primary efficacy analysis of best spectacle-corrected visual acuity at three months, as well as in various secondary clinical and microbiological endpoints, natamycin was consistently associated with significantly better outcomes than voriconazole. Therefore, the investigators concluded that voriconazole should not be used as monotherapy for filamentous fungal keratitis.
“We were very surprised by the findings of this study because they were not consistent with results from in vitro susceptibility testing favouring voriconazole over natamycin or from a survey of corneal specialists worldwide showing voriconazole was the preferred topical agent for treatment of filamentous keratitis,” said Dr Prajna, chief, cornea clinic, Aravind Eye Hospital, Madurai, India.
The MUTT was conducted in Tamilnadu, South India and undertaken after a pilot trial of 120 patients found a trend for better vision with voriconazole versus natamycin, but no statistically significant differences in primary or secondary efficacy outcomes.
Patients were eligible for MUTT if they had a smear-positive filamentous fungal ulcer and visual acuity of 20/40 to 20/400. Median ulcer size at enrolment was 3.2mm2.
Participants were treated in-house for at least two weeks to ensure treatment compliance.
Planned enrolment for MUTT was for 368 patients, but based on the recommendation of an international data and safety monitoring committee, recruitment was stopped after entry of only 323 patients as interim analyses showed clear differences favouring natamycin. Best spectacle-corrected visual acuity at three months was 1.4 lines better in patients treated with natamycin compared with the voriconazole group. In addition, the natamycin group had a significantly lower treatment failure rate (based on development of perforation or need for penetrating keratoplasty) and a lower rate of culture positivity when smears were repeated at six days. There were no between-group differences in time to re-epithelialisation or eventual scar size, Dr Prajna reported.
Microbiological analyses showed Fusarium was the most common causative organism for the fungal ulcers, isolated at entry in about half of the 256 culture-positive eyes. Subgroup analyses showed the superiority of voriconazole over natamycin was mainly attributable to its providing better results in the Fusarium cases. Outcomes for eyes with infection caused by other filamentous fungi were similar in the two treatment groups.
Dr Prajna commented that the predominance of Fusarium cases is one of the limitations of the study. In addition, he noted there were no contact lens wearers in the population, the participants were recruited from a single geographic location, and the study investigated only monotherapy.
21
rinco
n.de
WWW.GEUDER.COM
C O L O R L I N E
THE NEW HIGH-SPEED VITREOUS CUTTER MACH2
FAST CORE VITRECTOMY AND SAFE VITREOUS BASE SHAVING.
THE DOUBLE-BLADE
EFFICIENCY.
PERMANENTLY OPENFast core vitrectomy
CUTTING RATE5,000 cpm
DOUBLE-BLADELong lasting,excellent cuttingquality
CONSTANT FLOWControlled and safe shaving
IMMEDIATELYAVAILABLE
LY_Cutter Mach2_blau_Eurotimes_120x300_290813.indd 1 29.08.13 15:01EUROTIMES | Volume 18 | Issue 10
Update
CORNEA
FUNGAL KERATITISRandomised, controlled study leads to clear therapeutic recommendationby Cheryl Guttman Krader in Singapore
The predominance of Fusarium cases is one of the limitations of the study
“Venkatesh Prajna MD
Venkatesh Prajna – [email protected]
contact

Implantation of intracorneal ring segments (ICS) using channels created with a femtosecond laser can provide keratoconus patients with improvements in uncorrected and best-corrected visual acuity, and could delay or
avoid keratoplasty, according to Beatrice Cochener MD, PHD, CHU Brest, France.
“The femtosecond laser has become an essential tool for intracorneal ring segment implantation, offering perfect customisation of channels for placement of any model of ring segment on one single platform providing perfect control of total size and depth with better safety,” she said at Femto 2013, an international meeting on anterior segment surgery.
Prof Cochener presented the results she and her associates achieved in 94 eyes implanted with INTACS or INTACS SK (Addition Technology) and 194 eyes implanted with Kerarings (Mediphacos) using femtosecond laser-created channels.
Among 54 patients who received the INTACS of the original design for ectasia and for myopia with a risk for ectasia, uncorrected visual acuity and best corrected visual acuity improved in 57 per cent. In addition, aberrometry showed a significant reduction in higher order aberrations.
There were complications in four per cent of eyes, which included one case of infection (to an atopic patient with MGD) and two case of extrusion (induced by too superficial channel). In addition, there was loss of two lines in nine per cent of eyes.
INTACS SK a step forward Results were somewhat better among 40 eyes which underwent implantation of the newer INTACS SK implants. Some 48 per cent were 20/40 or better and 72 per cent gained one or two lines of vision. A majority, 79 per cent, had improvements in both UCVA and BCVA.
She noted that the INTACS SK are different from the original INTACS design in a few essential ways. The newer model has a 6.0mm inner diameter to provide a better flattening of the central cornea than that achieved with the 6.8mm inner diameter of the older design.
In addition, the INTACS SK has an ellipse-shaped rather than hexagonal cross-section to further enhance central corneal effects and reduce haloes. The INTACS SK ring segments range in thickness from 0.21mm to 0.45mm. At present they are only available with 150-degree arcs. However, Addition Technologies have announced that they are planning to launch INTACS with arc lengths ranging from 90 degrees to 230 degrees.
Kerarings with femto The Kerarings are already available in several different arc lengths, ranging at present from 90 degrees to 210 degrees. They are triangular in cross-section and have an inner diameter of 5.0 and more recently 6.0mm and range in thickness from 0.15mm to 0.35mm.
In 47 eyes that were implanted with the 5.0mm Keraring with femtosecond laser-created channels, mean visual acuity improved from 0.05 to 0.4 and best corrected visual acuity improved from 0.54 to 0.71. In addition, keratometry was reduced by 2.24 D and higher order aberrations decreased by mean of 62 per cent. The results achieved with the 6.0mm model in 147 eyes were statically identical with the benefit of a better quality of vision thanks to a larger optical zone, although Prof Cochener said that it has become her first choice among the Kerarings.
Beatrice Cochener – [email protected]
cont
act
INTRACORNEAL RING SEGMENTSFemtosecond laser-created channels can enhance the efficacy of cone-correcting implants by Roibeard O’hEineachain in Verona
22
EUROTIMES | Volume 18 | Issue 10
Update
CORNEA
INTACS SK Kerarings 5mm
INTACS non-SK Kerarings 6mm
The femtosecond laser has become an essential tool for intracorneal ring segment implantation, offering perfect customisation of channels for placement of any model of ring segment on one single platform providing perfect control of total size and depth with better safety
“
Beatrice Cochener MD, PHD, CHU
Don’t Miss Resident’s Diary, see page 62
Cour
tesy
of B
eatri
ce C
oche
ner M
D, P
HD, C
HU
P R O G R E SS I V E V I S I O N W I T H I N
F U L L AC C O M M O DAT I V E R A N G E
medicontur.com
Ad BiFlex M EuroTimes 2013+__ 29.08.13 14:15 Seite 1
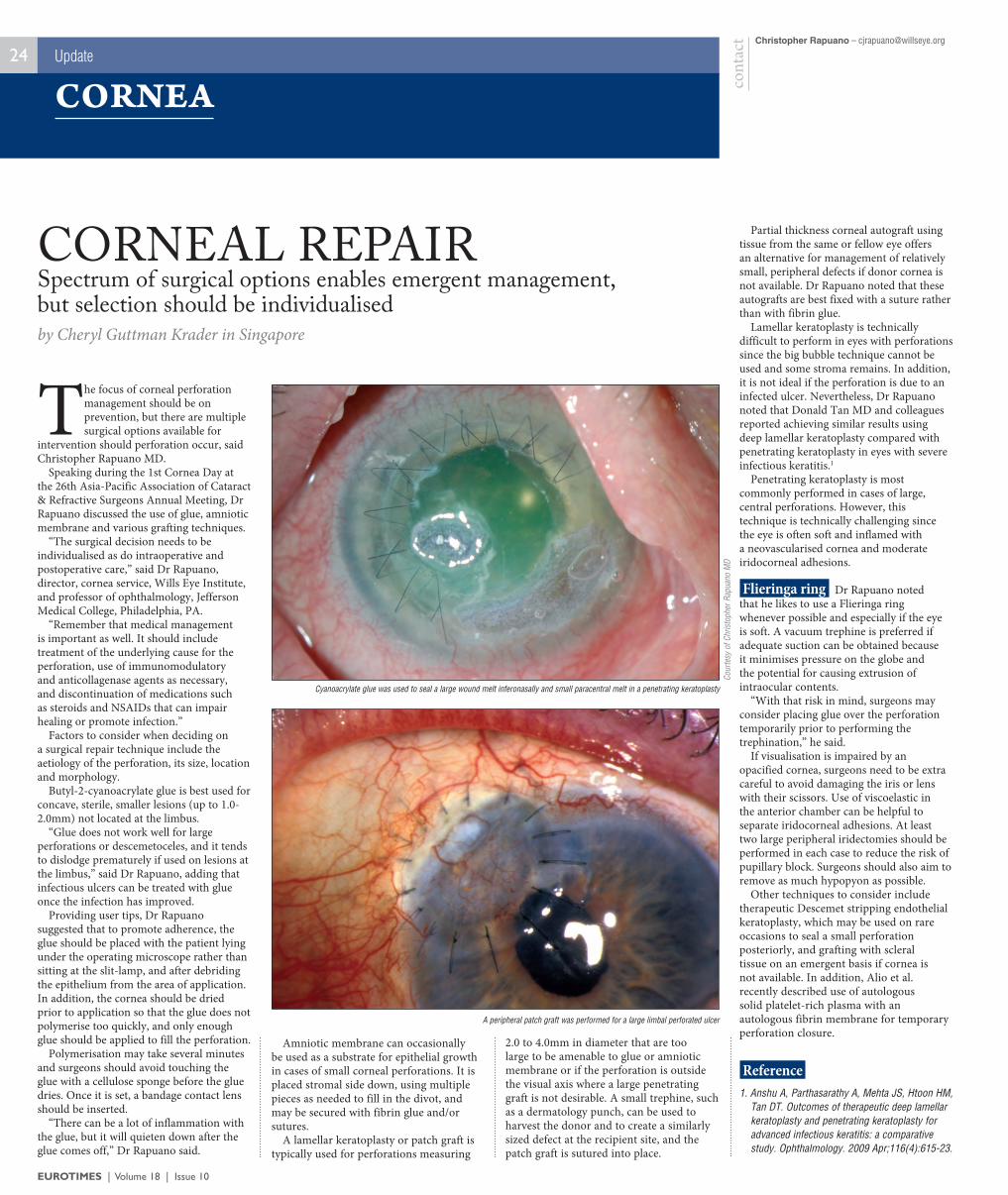
The focus of corneal perforation management should be on prevention, but there are multiple surgical options available for
intervention should perforation occur, said Christopher Rapuano MD.
Speaking during the 1st Cornea Day at the 26th Asia-Pacific Association of Cataract & Refractive Surgeons Annual Meeting, Dr Rapuano discussed the use of glue, amniotic membrane and various grafting techniques.
“The surgical decision needs to be individualised as do intraoperative and postoperative care,” said Dr Rapuano, director, cornea service, Wills Eye Institute, and professor of ophthalmology, Jefferson Medical College, Philadelphia, PA.
“Remember that medical management is important as well. It should include treatment of the underlying cause for the perforation, use of immunomodulatory and anticollagenase agents as necessary, and discontinuation of medications such as steroids and NSAIDs that can impair healing or promote infection.”
Factors to consider when deciding on a surgical repair technique include the aetiology of the perforation, its size, location and morphology.
Butyl-2-cyanoacrylate glue is best used for concave, sterile, smaller lesions (up to 1.0-2.0mm) not located at the limbus.
“Glue does not work well for large perforations or descemetoceles, and it tends to dislodge prematurely if used on lesions at the limbus,” said Dr Rapuano, adding that infectious ulcers can be treated with glue once the infection has improved.
Providing user tips, Dr Rapuano suggested that to promote adherence, the glue should be placed with the patient lying under the operating microscope rather than sitting at the slit-lamp, and after debriding the epithelium from the area of application. In addition, the cornea should be dried prior to application so that the glue does not polymerise too quickly, and only enough glue should be applied to fill the perforation.
Polymerisation may take several minutes and surgeons should avoid touching the glue with a cellulose sponge before the glue dries. Once it is set, a bandage contact lens should be inserted.
“There can be a lot of inflammation with the glue, but it will quieten down after the glue comes off,” Dr Rapuano said.
Amniotic membrane can occasionally be used as a substrate for epithelial growth in cases of small corneal perforations. It is placed stromal side down, using multiple pieces as needed to fill in the divot, and may be secured with fibrin glue and/or sutures.
A lamellar keratoplasty or patch graft is typically used for perforations measuring
2.0 to 4.0mm in diameter that are too large to be amenable to glue or amniotic membrane or if the perforation is outside the visual axis where a large penetrating graft is not desirable. A small trephine, such as a dermatology punch, can be used to harvest the donor and to create a similarly sized defect at the recipient site, and the patch graft is sutured into place.
Partial thickness corneal autograft using tissue from the same or fellow eye offers an alternative for management of relatively small, peripheral defects if donor cornea is not available. Dr Rapuano noted that these autografts are best fixed with a suture rather than with fibrin glue.
Lamellar keratoplasty is technically difficult to perform in eyes with perforations since the big bubble technique cannot be used and some stroma remains. In addition, it is not ideal if the perforation is due to an infected ulcer. Nevertheless, Dr Rapuano noted that Donald Tan MD and colleagues reported achieving similar results using deep lamellar keratoplasty compared with penetrating keratoplasty in eyes with severe infectious keratitis.1
Penetrating keratoplasty is most commonly performed in cases of large, central perforations. However, this technique is technically challenging since the eye is often soft and inflamed with a neovascularised cornea and moderate iridocorneal adhesions.
Flieringa ring Dr Rapuano noted that he likes to use a Flieringa ring whenever possible and especially if the eye is soft. A vacuum trephine is preferred if adequate suction can be obtained because it minimises pressure on the globe and the potential for causing extrusion of intraocular contents.
“With that risk in mind, surgeons may consider placing glue over the perforation temporarily prior to performing the trephination,” he said.
If visualisation is impaired by an opacified cornea, surgeons need to be extra careful to avoid damaging the iris or lens with their scissors. Use of viscoelastic in the anterior chamber can be helpful to separate iridocorneal adhesions. At least two large peripheral iridectomies should be performed in each case to reduce the risk of pupillary block. Surgeons should also aim to remove as much hypopyon as possible.
Other techniques to consider include therapeutic Descemet stripping endothelial keratoplasty, which may be used on rare occasions to seal a small perforation posteriorly, and grafting with scleral tissue on an emergent basis if cornea is not available. In addition, Alio et al. recently described use of autologous solid platelet-rich plasma with an autologous fibrin membrane for temporary perforation closure.
Reference 1. Anshu A, Parthasarathy A, Mehta JS, Htoon HM,
Tan DT. Outcomes of therapeutic deep lamellar keratoplasty and penetrating keratoplasty for advanced infectious keratitis: a comparative study. Ophthalmology. 2009 Apr;116(4):615-23.
Christopher Rapuano – [email protected]
cont
act
CORNEAL REPAIRSpectrum of surgical options enables emergent management, but selection should be individualisedby Cheryl Guttman Krader in Singapore
24
EUROTIMES | Volume 18 | Issue 10
Update
CORNEA
Cyanoacrylate glue was used to seal a large wound melt inferonasally and small paracentral melt in a penetrating keratoplasty
A peripheral patch graft was performed for a large limbal perforated ulcer
Cour
tesy
of C
hrist
ophe
r Rap
uano
MD
12-13 September 2014
www.eucornea.org
LONDON5th EuCornea Congress
Eu C o r n e
a
European Society of Cornea andOcular Surface Disease Specialists
Eu
C o r n ea
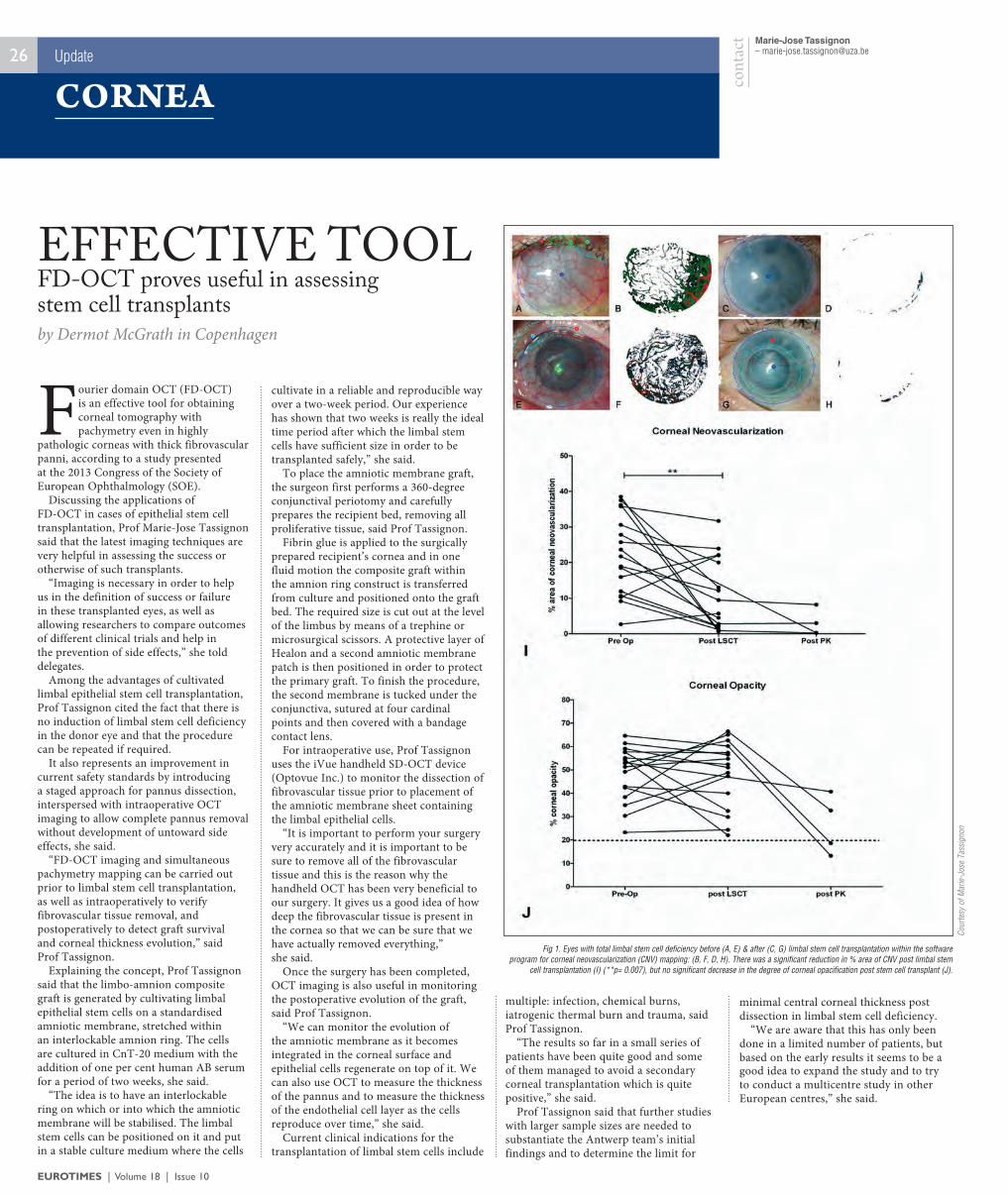
Fourier domain OCT (FD-OCT) is an effective tool for obtaining corneal tomography with pachymetry even in highly
pathologic corneas with thick fibrovascular panni, according to a study presented at the 2013 Congress of the Society of European Ophthalmology (SOE).
Discussing the applications of FD-OCT in cases of epithelial stem cell transplantation, Prof Marie-Jose Tassignon said that the latest imaging techniques are very helpful in assessing the success or otherwise of such transplants.
“Imaging is necessary in order to help us in the definition of success or failure in these transplanted eyes, as well as allowing researchers to compare outcomes of different clinical trials and help in the prevention of side effects,” she told delegates.
Among the advantages of cultivated limbal epithelial stem cell transplantation, Prof Tassignon cited the fact that there is no induction of limbal stem cell deficiency in the donor eye and that the procedure can be repeated if required.
It also represents an improvement in current safety standards by introducing a staged approach for pannus dissection, interspersed with intraoperative OCT imaging to allow complete pannus removal without development of untoward side effects, she said.
“FD-OCT imaging and simultaneous pachymetry mapping can be carried out prior to limbal stem cell transplantation, as well as intraoperatively to verify fibrovascular tissue removal, and postoperatively to detect graft survival and corneal thickness evolution,” said Prof Tassignon.
Explaining the concept, Prof Tassignon said that the limbo-amnion composite graft is generated by cultivating limbal epithelial stem cells on a standardised amniotic membrane, stretched within an interlockable amnion ring. The cells are cultured in CnT-20 medium with the addition of one per cent human AB serum for a period of two weeks, she said.
“The idea is to have an interlockable ring on which or into which the amniotic membrane will be stabilised. The limbal stem cells can be positioned on it and put in a stable culture medium where the cells
cultivate in a reliable and reproducible way over a two-week period. Our experience has shown that two weeks is really the ideal time period after which the limbal stem cells have sufficient size in order to be transplanted safely,” she said.
To place the amniotic membrane graft, the surgeon first performs a 360-degree conjunctival periotomy and carefully prepares the recipient bed, removing all proliferative tissue, said Prof Tassignon.
Fibrin glue is applied to the surgically prepared recipient’s cornea and in one fluid motion the composite graft within the amnion ring construct is transferred from culture and positioned onto the graft bed. The required size is cut out at the level of the limbus by means of a trephine or microsurgical scissors. A protective layer of Healon and a second amniotic membrane patch is then positioned in order to protect the primary graft. To finish the procedure, the second membrane is tucked under the conjunctiva, sutured at four cardinal points and then covered with a bandage contact lens.
For intraoperative use, Prof Tassignon uses the iVue handheld SD-OCT device (Optovue Inc.) to monitor the dissection of fibrovascular tissue prior to placement of the amniotic membrane sheet containing the limbal epithelial cells.
“It is important to perform your surgery very accurately and it is important to be sure to remove all of the fibrovascular tissue and this is the reason why the handheld OCT has been very beneficial to our surgery. It gives us a good idea of how deep the fibrovascular tissue is present in the cornea so that we can be sure that we have actually removed everything,” she said.
Once the surgery has been completed, OCT imaging is also useful in monitoring the postoperative evolution of the graft, said Prof Tassignon.
“We can monitor the evolution of the amniotic membrane as it becomes integrated in the corneal surface and epithelial cells regenerate on top of it. We can also use OCT to measure the thickness of the pannus and to measure the thickness of the endothelial cell layer as the cells reproduce over time,” she said.
Current clinical indications for the transplantation of limbal stem cells include
multiple: infection, chemical burns, iatrogenic thermal burn and trauma, said Prof Tassignon.
“The results so far in a small series of patients have been quite good and some of them managed to avoid a secondary corneal transplantation which is quite positive,” she said.
Prof Tassignon said that further studies with larger sample sizes are needed to substantiate the Antwerp team’s initial findings and to determine the limit for
minimal central corneal thickness post dissection in limbal stem cell deficiency.
“We are aware that this has only been done in a limited number of patients, but based on the early results it seems to be a good idea to expand the study and to try to conduct a multicentre study in other European centres,” she said.
Marie-Jose Tassignon – [email protected]
cont
act
EFFECTIVE TOOLFD-OCT proves useful in assessing stem cell transplantsby Dermot McGrath in Copenhagen
26
EUROTIMES | Volume 18 | Issue 10
Update
CORNEA
Fig 1. Eyes with total limbal stem cell deficiency before (A, E) & after (C, G) limbal stem cell transplantation within the software program for corneal neovascularization (CNV) mapping: (B, F, D, H). There was a significant reduction in % area of CNV post limbal stem
cell transplantation (I) (**p= 0.007), but no significant decrease in the degree of corneal opacification post stem cell transplant (J).Co
urte
sy o
f Mar
ie-Jo
se T
assig
non
27
Intracorneal pockets created with femtosecond lasers have a wide variety of potential uses, said Ioannis G Pallikaris MD PhD, University of
Crete, Heraklion, Greece.“Femtosecond lasers allow us to create
corneal pockets safely and accurately with few complications and their versatility means that we have many new potential techniques to explore,” he reported at Femto 2013, an international meeting on anterior segment surgery.
Dr Pallikaris described his experience with the use of femtosecond lasers for creating intrastromal pockets for the placement of Flexivue Microlens (Presbia) presbyopic corneal inlays. He also described two new femtosecond laser techniques he and his team have developed, one for using an intrastromal pocket for delivering medicine and the other for placing a layer of biocompatible silicone to control corneal oedema in eyes with bullous keratopathy.
Focal points The Flexivue Microlens is a doughnut-shaped hydrophilic polymer lens that is designed for implantation in the non-dominant eye. The inlay is 3.0mm in diameter and 20 µm in thickness. It is designed to provide two focal points, one for far vision and the other for near.
Dr Pallikaris said that he uses the Intralase femtosecond laser (AMO) to create the pockets for the inlays. Using the system’s iPockets software, he creates the pockets at a depth of microns with width of 4.0mm. Thus far the results with the implants have been encouraging. In a study involving 45 patients who received the implant, the mean uncorrected near visual acuity improved from 20/100 to 20/25.
Although uncorrected distance visual acuity decreased in the operated eye, binocular uncorrected distance visual acuity remained unchanged. In addition, 92 per cent said they never used reading glasses.
A more novel use of intrastromal pockets created with femtosecond lasers is to provide a means of delivery of medication to tissues of the inner cornea. Dr Pallikaris described a case where he used the technique in a patient with refractory oedema. The 74-year-old woman presented with photophobia, blurred vision
and pain. She had been having recurrent episodes of corneal oedema that was unresponsive to antibiotic therapy and anterior keratectomy.
Corneal abcess Dr Pallikaris used the Intralase iFS 150-kHz femtosecond laser to create a ring-shaped corneal pocket into the region of the corneal abscess at a depth of 380 µ with an inner diameter of 7.0mm, outer diameter of 7.1mm and an entry port for the injection of 1.4mm in width. Five days after an injection of moxifloxacin into intracorneal the patients showed a clear improvement in her condition, he noted.
He noted that he has also successfully used femtosecond lasers in a series of patients with bullous keratopathy. The technique involves the creation of a keyhole-shaped pocket in the cornea with a Wavelight FS-200 femtosecond laser using its lamellar keratoplasty software, followed by insertion of a biocompatible silicone material. In each of the cases Dr Pallikaris described there was complete re-epithelialisation followed by complete relief of symptoms.
CORNEAL POCKETSUses of femtosecond lasers in corneal surgery continue to expandby Roibeard O’hEineachain in Verona
Ioannis G Pallikaris – [email protected]
contact
See the new pulse in perimetry
OCTOPUS® 600
Perimetry
www.haag-streit.com
■One device does it all Novel perimeter technology for early diagnosis and standard white-on-white perimetry.
■Perimetry simplified Streamlined operation with special touchscreen optimized and proven EyeSuite™ software.
■World innovation in perimetryFast and reliable Pulsar test method for early glaucoma detection.
ADV_Eurotimes_260713_O600.indd 1 26.08.2013 10:09:43EUROTIMES | Volume 18 | Issue 10
Update
CORNEA
Femtosecond lasers allow us to create corneal pockets safely and accurately with few complications and their versatility means that we have many new potential techniques to explore
“
Ioannis Pallikaris MD PhD
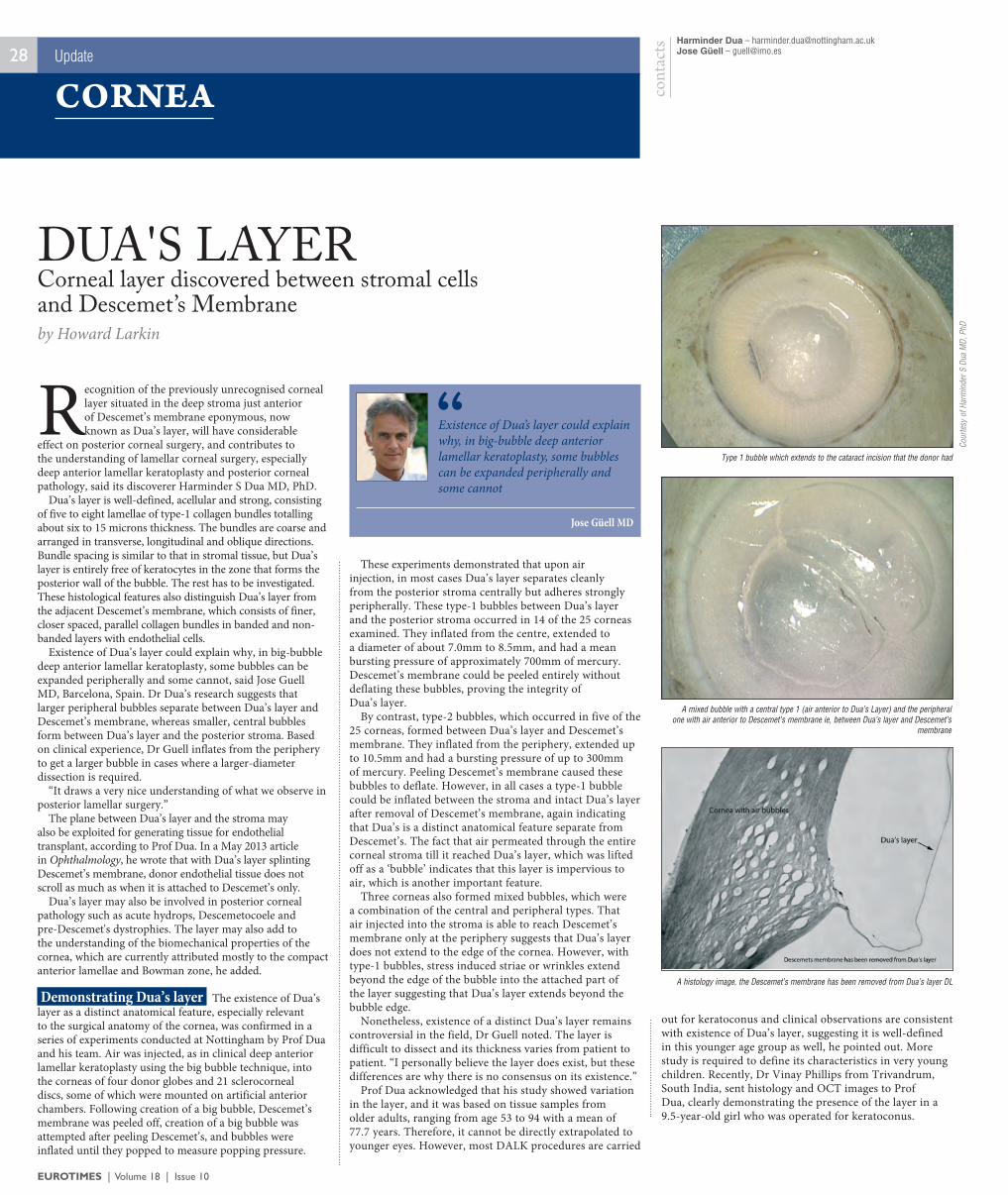
Recognition of the previously unrecognised corneal layer situated in the deep stroma just anterior of Descemet’s membrane eponymous, now known as Dua’s layer, will have considerable
effect on posterior corneal surgery, and contributes to the understanding of lamellar corneal surgery, especially deep anterior lamellar keratoplasty and posterior corneal pathology, said its discoverer Harminder S Dua MD, PhD.
Dua’s layer is well-defined, acellular and strong, consisting of five to eight lamellae of type-1 collagen bundles totalling about six to 15 microns thickness. The bundles are coarse and arranged in transverse, longitudinal and oblique directions. Bundle spacing is similar to that in stromal tissue, but Dua’s layer is entirely free of keratocytes in the zone that forms the posterior wall of the bubble. The rest has to be investigated. These histological features also distinguish Dua’s layer from the adjacent Descemet’s membrane, which consists of finer, closer spaced, parallel collagen bundles in banded and non-banded layers with endothelial cells.
Existence of Dua’s layer could explain why, in big-bubble deep anterior lamellar keratoplasty, some bubbles can be expanded peripherally and some cannot, said Jose Guell MD, Barcelona, Spain. Dr Dua’s research suggests that larger peripheral bubbles separate between Dua’s layer and Descemet’s membrane, whereas smaller, central bubbles form between Dua’s layer and the posterior stroma. Based on clinical experience, Dr Guell inflates from the periphery to get a larger bubble in cases where a larger-diameter dissection is required.
“It draws a very nice understanding of what we observe in posterior lamellar surgery.”
The plane between Dua’s layer and the stroma may also be exploited for generating tissue for endothelial transplant, according to Prof Dua. In a May 2013 article in Ophthalmology, he wrote that with Dua’s layer splinting Descemet’s membrane, donor endothelial tissue does not scroll as much as when it is attached to Descemet’s only.
Dua’s layer may also be involved in posterior corneal pathology such as acute hydrops, Descemetocoele and pre-Descemet's dystrophies. The layer may also add to the understanding of the biomechanical properties of the cornea, which are currently attributed mostly to the compact anterior lamellae and Bowman zone, he added.
Demonstrating Dua’s layer The existence of Dua’s layer as a distinct anatomical feature, especially relevant to the surgical anatomy of the cornea, was confirmed in a series of experiments conducted at Nottingham by Prof Dua and his team. Air was injected, as in clinical deep anterior lamellar keratoplasty using the big bubble technique, into the corneas of four donor globes and 21 sclerocorneal discs, some of which were mounted on artificial anterior chambers. Following creation of a big bubble, Descemet’s membrane was peeled off, creation of a big bubble was attempted after peeling Descemet’s, and bubbles were inflated until they popped to measure popping pressure.
These experiments demonstrated that upon air injection, in most cases Dua’s layer separates cleanly from the posterior stroma centrally but adheres strongly peripherally. These type-1 bubbles between Dua’s layer and the posterior stroma occurred in 14 of the 25 corneas examined. They inflated from the centre, extended to a diameter of about 7.0mm to 8.5mm, and had a mean bursting pressure of approximately 700mm of mercury. Descemet’s membrane could be peeled entirely without deflating these bubbles, proving the integrity of Dua’s layer.
By contrast, type-2 bubbles, which occurred in five of the 25 corneas, formed between Dua’s layer and Descemet’s membrane. They inflated from the periphery, extended up to 10.5mm and had a bursting pressure of up to 300mm of mercury. Peeling Descemet’s membrane caused these bubbles to deflate. However, in all cases a type-1 bubble could be inflated between the stroma and intact Dua’s layer after removal of Descemet’s membrane, again indicating that Dua’s is a distinct anatomical feature separate from Descemet’s. The fact that air permeated through the entire corneal stroma till it reached Dua’s layer, which was lifted off as a ‘bubble’ indicates that this layer is impervious to air, which is another important feature.
Three corneas also formed mixed bubbles, which were a combination of the central and peripheral types. That air injected into the stroma is able to reach Descemet’s membrane only at the periphery suggests that Dua’s layer does not extend to the edge of the cornea. However, with type-1 bubbles, stress induced striae or wrinkles extend beyond the edge of the bubble into the attached part of the layer suggesting that Dua’s layer extends beyond the bubble edge.
Nonetheless, existence of a distinct Dua’s layer remains controversial in the field, Dr Guell noted. The layer is difficult to dissect and its thickness varies from patient to patient. “I personally believe the layer does exist, but these differences are why there is no consensus on its existence.”
Prof Dua acknowledged that his study showed variation in the layer, and it was based on tissue samples from older adults, ranging from age 53 to 94 with a mean of 77.7 years. Therefore, it cannot be directly extrapolated to younger eyes. However, most DALK procedures are carried
out for keratoconus and clinical observations are consistent with existence of Dua’s layer, suggesting it is well-defined in this younger age group as well, he pointed out. More study is required to define its characteristics in very young children. Recently, Dr Vinay Phillips from Trivandrum, South India, sent histology and OCT images to Prof Dua, clearly demonstrating the presence of the layer in a 9.5-year-old girl who was operated for keratoconus.
28Harminder Dua – [email protected] Güell – [email protected]
cont
acts
by Howard Larkin
Corneal layer discovered between stromal cells and Descemet’s Membrane
DUA'S LAYER
EUROTIMES | Volume 18 | Issue 10
Update
CORNEA
Existence of Dua’s layer could explain why, in big-bubble deep anterior lamellar keratoplasty, some bubbles can be expanded peripherally and some cannot
“Jose Güell MD
A histology image, the Descemet’s membrane has been removed from Dua’s layer DL
A mixed bubble with a central type 1 (air anterior to Dua’s Layer) and the peripheral one with air anterior to Descemet’s membrane ie, between Dua’s layer and Descemet’s
membrane
Type 1 bubble which extends to the cataract incision that the donor had
Cour
tesy
of H
arm
inde
r S D
ua M
D, P
hD
Speaking during the first Cornea Day of the 26th Asia-Pacific Association of Cataract and Refractive Surgeons Annual Meeting, Peter Zloty MD, provided some perspective on current techniques
and technology for identifying dry eye in clinical practice. Discussing measurement of tear film osmolarity, Dr
Zloty concluded that the commercially available point-of-care system (TearLab Osmolarity System, TearLab) could prove to be a useful tool to use in research studies, but that it should not be relied on as a stand-alone evaluation for diagnosing dry eye in daily patient care.
“Some individuals are saying that tear film osmolarity is necessary and the gold standard for accurately diagnosing dry eye syndrome, while others observe it as a snapshot observation,” said Dr Zloty, a cornea specialist in private practice in Alabama.
He noted that absolute values of tear film osmolarity that are diagnostic of dry eye are not yet determined, and unless the result is very hyperosmolar, the analysis may not be conclusive. Various studies investigating osmolarity cut points for differentiating between normal and dry eye have suggested numbers ranging from >305 up to 318 mOsmol/L, while in their seminal work, Tomlinson et al. reported that using ≥316 mOsmol/L as the diagnostic threshold provided 59 per cent sensitivity and 94 per cent specificity.
Dr Zloty suggested that a fundamental problem with using the point-of-care tear film osmolarity platform for diagnosing dry eye is that it only measures the dissolved ions in the aqueous matrix lying under the amphiphilic lipid layer of the tear film. Unlike the original laboratory-based method for determining tear film osmolarity that is based on freezing point depression, which is affected by all solutes in the solvent, the commercially available platform uses electrical conductivity, which is affected only by ions that are present.
“Measurement of tear film osmolarity with this device has nothing to do with the lipid layer of the tear film. That may explain the variability of studies evaluating its usefulness in diagnosing chronic ocular surface disease and why it will not necessarily detect patients with dry eye associated with lipid abnormalities,” Dr Zloty said.
He also cited a study presented at ARVO 2012 by Mudgil et al who reported that hyperosmolarity had no adverse effect on the stability of the tear film, and a published paper by Szalai et al who reported wide overlap in tear film osmolarity values comparing patients with Sjogrens syndrome and normal controls.
“However, Szalai et al found tear film breakup time had predictive value,” noted Dr Zloty, “and it may be that tear film breakup time is the most useful test for diagnosing dry eye.”
Discussing other diagnostic testing, Dr Zloty said that the Schirmer I test (without anaesthesia) is useful for identifying patients with aqueous deficient dry eye if the result is positive. However, individuals with pure aqueous
deficient disease account for less than 20 per cent of the dry eye population.
Dr Zloty also reminded his colleagues that when performing a Schirmer test with anaesthesia, they should take care to standardise the materials and methods of their testing since meaningful interpretation of serial measurements depends on using a consistent technique.
All patients with dry eye-related complaints should be carefully examined for lid margin disease, especially if they are found to have adequate aqueous production, said Dr Zloty, noting evidence that evaluation of the lids is underperformed.
“According to one study, fewer than one out of 20 ophthalmologists assess the meibomian glands. I encourage everyone to look carefully at the lids, manipulate them and document the quantity and quality of the meibomian gland secretions,” he said.
Dr Zloty also categorised the Ocular Surface Disease Index (OSDI) and meibometry as diagnostic tools having value in research studies but with questionable utility in the office setting. For example, OSDI data may be useful for finding small differences between treatment groups in a clinical trial, he said.
As an alternative to administering the OSDI, Dr Zloty suggested simply querying patients with typical dry eye complaints if their symptoms are worse in the morning or at the end of the day as this information may provide a clue to underlying aetiology.
“The response to this question can help to identify whether a patient is suffering because of lid dysfunction, sleep apnoea that causes eye rubbing through the night, lagophthalmos, or classic keratoconjunctivitis sicca,” he said.
Dr Zloty concluded with a pearl for treatment of dry eye that he derived from a retrospective review published by Jonisch et al in 2010 – use of 0.01 per cent dexamethasone compounded in preservative-free artificial tears.
“This dilute corticosteroid preparation did not increase IOP, and it has tremendously augmented use of cyclosporine in my practice,” he said.
DRY EYE DIAGNOSISNew tools emerging, but old tests still usefulby Cheryl Guttman Krader in Singapore
29
EUROTIMES | Volume 18 | Issue 10
ExploreNEWFRONTIERS
40 grants of €1000 to young ophthalmologists
who want to travel abroad to improve their skills
The ESCRS is awarding
Visit www.escrs.orgto apply
Update
CORNEA
“According to one study, fewer than one out of 20 ophthalmologists assess the meibomian glands”
Peter Zloty – [email protected]
contact

31
Latanoprostene bunod, a novel investigational IOP-lowering agent combining a prostaglandin analogue with a nitric oxide (NO)
donating moiety, has produced promising results in early clinical trials.
The new agent demonstrated greater efficacy and similar safety compared with latanoprost 0.005 per cent in a Phase 2b clinical trial. Now, Phase 3 studies are under way evaluating it as a treatment for patients with glaucoma and ocular hypertension.
The Phase 2b study was a dose-ranging trial that compared four different concentrations of latanoprostene bunod against latanoprost 0.005 per cent in patients with ocular hypertension or open angle glaucoma whose IOP was between 26 and 32 mmHg. Results for the groups treated with latanoprostene bunod 0.024 per cent (83 patients), the most efficacious and well tolerated concentration tested, and latanoprost 0.005 per cent (82 patients) were reported in a poster presented at the 2013 annual meeting of the Association for Research in Vision and Ophthalmology.
Assigned study Patients used their assigned study medication once nightly for 28 days and returned for IOP measurements on days seven, 14, 28, and 29. Mean diurnal IOP reduction was significantly greater in the latanoprostene bunod group compared with latanoprost on days seven (8.3 vs. 7.3 mmHg), 14 (8.9 vs. 7.7 mmHg), and 28 (9.0 vs. 7.8 mmHg). In addition, the proportion of patients achieving a mean diurnal IOP of 18 mmHg or less was significantly greater in the latanoprostene bunod group than in the control arm at all follow-up visits.
Safety analyses showed all treatment-emergent adverse events were mild or moderate in severity and similar in type and frequency in the latanoprostene bunod and latanoprost groups. Reports of stinging upon instillation were slightly higher for the investigational agent.
“For the past 17 years since latanoprost was first approved by the US FDA, prostaglandin analogues have been our most potent class of IOP-lowering drugs.
However, the search has continued for new compounds that are even more powerful but still offer the benefit of once daily dosing,” said L Jay Katz, MD, lead author of the poster, and director of the glaucoma service, Wills Eye Institute, and professor of ophthalmology, Thomas Jefferson University, Philadelphia.
Dual mechanisms “The Phase 2b study results for latanoprostene bunod are encouraging as they suggest it may lower IOP more effectively than a prostaglandin analogue without compromising safety and tolerability. Now we await the results from the Phase 3 studies that will provide data on longer term use from a larger population.”
As NO has been shown to relax the trabecular meshwork and ciliary muscle, NO donors are thought to lower IOP by improving aqueous outflow through the trabecular meshwork.
“In theory, the increased potency of latanoprostene bunod might be explained by its having a dual mechanism of action, increasing uveoscleral outflow because of the latanoprost component, but also enhancing trabecular outflow,” said Dr Katz.
IOP LOWERINGNitric oxide-donating prostaglandin analogue shows promise for greater potencyby Cheryl Guttman Krader
L Jay Katz – [email protected]
contact
Beautiful......The New beautifully crafted Slit Lamp
from Keeler.
Quality build and leading technology
with a contemporary design.
Digital......The New digital generation Keeler D-KAT.
The future of applanation tonometry.
Available......to view at ESCRS stand A11A www.keeler-symphony.com
D-KAT
EUROTIMES | Volume 18 | Issue 10
Update
GLAUCOMA
Don’t Miss Book Review, see page 65
“For the past 17 years since latanoprost was first approved by the US FDA, prostaglandin analogues have been our most potent class of IOP-lowering drugs”

The diagnosis of ocular surface disease (OSD) is often overlooked or underestimated in glaucoma patients, even though recognising
and treating the condition can greatly improve both quality of life and adherence to the glaucoma treatment, says Prof Maurizio Rolando, Clinica Oculistica, University of Genoa, Italy.
“We need to be aware of the dynamic nature of the ocular surface which is continuously adapting to environmental, toxic, infective, traumatic and inflammatory conditions that the eye is exposed to,” he told delegates attending the 2013 Congress of the Society of European Ophthalmology.
“We need to think about tear and ocular surface dysfunction in our glaucoma patients and look for clinical signs of OSD, which are not difficult to identify but which must be looked for in the first place.”
Dr Rolando said that the association between ocular surface changes and IOP-lowering medications to treat glaucoma has been long established.
“In the 1970s, Dr Pfister showed the deleterious impact of 0.01 per cent benzalkonium chloride (BAK) on the corneal epithelium. After several minutes, large numbers of surface cells were shown to retract from their cell contacts leaving retraction fibrils. Many cell edges peeled up, with the loss of microvilli and rupture of intercellular tight junctions. After three hours of BAK exposure, the second layer cells have also undergone extensive degenerative membrane changes,” he said.
The specific term for such medication-related alterations is “medicamentosa,” noted Prof Rolando.
“This is what we are seeing in the ocular surface of these patients, a condition used in or caused by a drug or combination of drugs. We see a toxic response with no underlying immune dysfunction and it is one of the most common disorders seen in the subspecialty of cornea and external diseases,” he said.
Prof Rolando emphasised the importance of staining the ocular surface in order to assess the integrity of the superficial cell layers and to give clues to the diagnosis.
“Staining the conjunctiva is essential to determining if patients have OSD or not. Because the main focus is on their glaucoma and reducing their IOP, we may miss
problems on the ocular surface and fail to recognise the problems that they have,” he said.
The ocular surface has two main abilities, said Prof Rolando, the first one being to protect the eye and the second to maintain the quality of vision
“The ocular surface is a functional unit that maintains the integrity of the cornea, preserves the quality of the refractive surface of the eye and visual function. It also resists injury and protects the eye against changing bodily and environmental conditions,” he said.
Quality of vision largely depends on the quality of the tear film, said Prof Rolando.
“We are all aware of the detrimental effect of dry eye on a patient’s quality of life, because this is a problem that they have to deal with all day, every day. We know that moderate to severe dry eye syndrome can adversely affect a person's ability to perform vision-intensive tasks due to pain and impaired vision. In addition, dry eye disease is associated with increased ocular and corneal higher order aberrations,” he said.
He noted that artificial tear administration significantly improves reliability parameters and visual field indices. Rieger in 1992 was one of the first to report that threshold perimetry improved in dry eye patients after instillation of artificial tears, suggesting that tear film supplements stabilised the tear film and improved the optical quality of the eye.
The ocular surface disease index (OSDI) is a useful measure of the severity of the OSD, and underscores the frequency of the problem in glaucomatous patients under medical treatment.
Impaired visual acuity, contrast sensitivity and visual function can have a profound effect on vision-related quality of life.
“Dry eye syndrome significantly decreases quality of life and patients’ ability to perform daily functions. One of the few studies by Nordmann et al. that looked at side effects from glaucoma treatment and quality of life showed that 62 per cent of patients reported more than one adverse effect from their treatment including burning, blurred vision, tearing sensation and itchy eyes,” he said.
This has a direct impact on the efficacy of the glaucoma treatment, said Prof Rolando. “You are not going to have a good adherence if a patient’s quality of life is impacted negatively by their treatment. Adverse
effects are the third most common reason for non-compliance and they may well be underestimated in clinical trials,” he said.
The ocular surface is a dynamic system with a self-maintaining visual cycle that responds to changing conditions and stimuli. When the cycle is disturbed, intervention is necessary to prevent a cascade of negative effects such as tear evaporation, epithelial cell damage and inflammation, he said.
For patients with a chronic disease such as glaucoma, switching to preservative-
free medications may help to reduce the toxic stress on the ocular surface, said Prof Rolando.
“Switching from BAK-preserved to BAK-free medication has been shown to improve epithelial barrier function. Furthermore, some studies have shown that the deleterious effect of BAK on trabecular meshwork cells may be an under-appreciated concern in patients receiving long-term glaucoma treatment,” he concluded.
Maurizio Rolando – [email protected]
cont
act
VICIOUS CYCLEAssociation between ocular surface changes and IOP lowering medicationsby Dermot McGrath in Copenhagen
32
EUROTIMES | Volume 18 | Issue 10
Update
GLAUCOMA
Figure 1: Pre-corneal tear film instability has been reported to be present in over 50 per cent of patients using multiple topical therapies for glaucoma
Figure 2: Fluorescein conjunctival staining of the conjunctiva in a patient undergoing topical anti-glaucoma therapy. Fluorescein or Lissamine Green conjunctival staining is mandatory to understand the inflammatory conditions of the ocular surface of the
patient. Conjunctival inflammation could affect the behaviour of the disease both under topical and surgical therapyCo
urte
sy o
f Mau
rizio
Rol
ando
©2013 HOYA Surgical Optics. All rights reserved.
HSOE-013-EN-1013
See for yourself. Visit us at Booth B01 at ESCRS 2013 Amsterdamor www.HOYA.com/SurgicalOptics
Singularly Focused. Globally Powered.TM
We enjoy a different world view An entrepreneurial company, in diverse world markets, with emerging innovative products.
HSOE398-October-2013-eurotimes-print-ad-082913.indd 1 8/29/13 11:18 AM
34
When it comes to performing one- or two-site phacotrabeculectomy, evidence suggests outcomes
are the same for most patients. But one-site phacotrabeculectomy may have an advantage in terms of preserving corneal health, reports Yvonne Buys MD, FRCSC, professor at the Department of Ophthalmology and Vision Sciences, University of Toronto, Canada.
"If you have a patient whose corneal health is of special concern, you may want to consider one-site," she told a session of the 5th World Glaucoma Congress where she reviewed the evidence for one- versus two-site phacotrabeculectomy plus discussed surgical approaches.
A randomised, controlled trial of 79 patients (which she co-authored), found when it came to IOP, visual acuity and the number of medications, there was no difference in outcome between one- and two-site patients. However, corneal endothelial cell counts proved to be better in the one-site patients at three and 12 months, with lower counts in the two-site patients.
"It's not surprising to see this kind of outcome. With one-site surgery you're a little bit more posterior entering the anterior chamber, and you're also having one less incision than in two-site surgery," she said.
She also co-authored a meta-analysis which showed that after three years of follow-up, there were no differences between one- and two-site surgery in lowering IOP, or in other measures. The only difference was that one-site surgery took less time to perform - on average by 13 minutes. The meta-analysis included studies with similar patient populations, an important detail in this type of study.
"Your choice comes down to what your preferred surgery is," she said.
In her own practice, she prefers one-site phacotrabeculectomy and uses a corneal traction suture and subconjunctival anaesthesia with one per cent lidocaine. Dr. Buys incorporates the anaesthesia injection site into the conjunctival incision and does a fornix-based conjunctival flap. She noted it's important to dissect well posteriorally
to create a pocket for fluid to drain into afterwards, and added that judicious cautery is important.
"I like to cauterize along the limbus as well, to try to encourage the anterior edge of that conjunctiva to stick down so that you minimise the risk of leaks," she said.
For most cases she said she uses mitomycin, noting that various studies show mitomycin is associated with positive outcomes.
Sclera flap dissection She inserts a sponge soaked in mitomycin posteriorly under the conjunctiva before performing the sclera flap dissection.
As for the flap, the design doesn't affect results though it should be approximately ½ sclera thickness. She usually creates a four-by-four millimetre triangular flap.
She uses a two-incision approach for the phaco, and suggests when performing combined procedures it is okay to leave some of the viscoelastic - as long as it's not behind the IOL. This reduces the risks of hypotony and lens-corneal touch.
In trabeculectomy alone she uses three sutures in the sclera flap, but in phacotrabeculectomy, she uses only two, with one being alongside the relaxing incision and the other at the apex. The flap shouldn't be too tight to allow drainage and preventing the conjunctiva from adhering to the sclera, she said.
Yvonne M Buys – [email protected]
contact
PREFERRED SURGERYMeta-analysis shows no difference between one- and two-site surgery in lowering IOP by Pippa Wysong in Vancouver
THE IOL FOR DAY & NIGHT
CROMA GmbH • www.croma.atAECOP000Ab | 0123
Now in the preloaded system
Fully preloaded hydrophobic IOL
• 2.1 mm mini incision• Easy and convenient handling• No risk of cross contamination
Excellent quality of vision
• Optimal contrast sensitivity – blue light � lter• Glare free vision – sand blasted like edge surface• Maximum depth of focus – aberration control
Enduring reliability
• No microvacuoles – dense polymer network• 360° sharp edge design – reduced risk of PCO
CROMA GmbH • www.croma.atAECOP000Ab | 0123
Optimal contrast sensitivity – blue light � lterGlare free vision – sand blasted like edge surfaceMaximum depth of focus – aberration control
Enduring reliability
• No microvacuoles – dense polymer network• 360° sharp edge design – reduced risk of PCO
ad-half page vertical-Eurotimes-ENG EyeCeeO PRL-1306v03 pva RZ.indd 1 12.09.13 17:03EUROTIMES | Volume 18 | Issue 10
Update
GLAUCOMA
“If you have a patient whose corneal health is of special concern, you may want to consider one-site”
Don’t Miss Practice Development update, see page 67

35
Pattern laser trabeculoplasty (PLT) using a 577nm laser with computer-guided scanning technology (PASCAL Streamline
577, Topcon Medical Laser Systems) appears to be effective treatment for open-angle glaucoma (OAG) offering potential advantages relative to other laser techniques, reported Japanese researchers at the 2013 annual meeting of the Association for Vision in Research and Ophthalmology.
In PLT, the laser delivers a treatment pattern of 39 100-micron spots over 22.5º of arc (2.75mm) and then rotates automatically so that the next pattern is precisely aligned and applied onto an untreated location. The software was first introduced for the 532nm pattern scanning laser and subsequently became available as an upgrade for the 577nm laser.
Miho Nozaki MD, PhD, and colleagues reported their experience with 577nm PLT in a series of 11 eyes of nine patients. Primary open angle glaucoma (POAG) was the most common diagnosis in the series, followed by pseudoexfoliation glaucoma, steroid-induced glaucoma and pigmentary glaucoma. Laser power was initially titrated to produce trabecular meshwork blanching with a 10 ms pulse, and then subvisible treatment was applied using a 5.0 ms pulse duration.
The treatment was delivered in 32 steps to cover 360º of the trabecular meshwork with a mean of 1287 spots per eye. Mean laser power was 344 mW and mean pulse energy was 1.7 mJ.
The treatment reduced mean IOP from 20.5 mmHg at baseline to 15.0 mmHg at one month. Among eight eyes evaluated at six months, mean IOP was 13.4 mmHg (-31 per cent relative to baseline). Patients were using a mean of 2.6 medications prior to PLT, and that number was unchanged at six months. The only adverse event recorded was transient IOP elevation in one eye.
“The concept of PLT is similar to selective laser trabeculoplasty (SLT) as it minimises thermal injury that leads to structural tissue damage in the trabecular meshwork. However, because there are no clinically visible tissue changes, the laser operator performing SLT may unintentionally leave some areas of the trabecular meshwork untreated. This problem is avoided with PLT thanks to computer guidance of
treatment delivery,” said Dr Nozaki, associate professor of ophthalmology and visual science, Nagoya City University Graduate School of Medical Sciences, Japan.
“Perhaps the enhanced accuracy of PLT treatment may result in greater durability of the IOP-lowering effect. However, a larger, controlled study with longer follow-up is needed to definitively evaluate the efficacy of PLT and its durability,” Dr Nozaki told EuroTimes.
She added that in contrast to argon laser trabeculoplasty, so far PLT appears not to result in the development of peripheral anterior synechiae, and it is better tolerated than ALT. Patients undergoing PLT were asked to rate treatment pain using a visual analogue scale where zero represents no pain and 10 is the worst possible pain imaginable. Based on data from eight eyes, the pain score averaged 3.3 and exceeded five in only one eye, which was the first treated.
PATTERN LASERNew approach minimises tissue damage and maximises precisionby Cheryl Guttman Krader
Miho Nozaki – [email protected]
contact
The power of oneTwo types of incisions – one module
The Ziemer FEMTO LDV Z Models are FDA cleared and CE marked and available for immediate delivery. For some countries, availability may be restricted due to local regulatory requirements. Cataract procedures are not approved in the United States and in some other countries. Please contact Ziemer for details.
Refractive laser-assisted CATARACT surgery
CLEAR CORNEAL & RELAXING INCIsIONs• Custom-designed incisions• Topographically matched • Added precision and reproducibility• Intrastromal incisions possible
Exclusively available for the FEMTO LDV Z6 Power Plus
www.femtoldv.com
Please vi
sit us a
t
EsCRs Booth # C05
EuroTimes_oct2013_FEMTO_LDV_Corneal_Inscisions_Ad_120x300mm.indd 1 02.09.13 16:44EUROTIMES | Volume 18 | Issue 10
Update
GLAUCOMA
The arc patterns of 39 spots automatically rotate, so the physician only has to rotate the contact lens to adjust aiming
pattern and trabecular meshwork
Perhaps the enhanced accuracy of PLT treatment may result in greater durability of the IOP-lowering effect
“Miho Nozaki MD, PhD
Cour
tesy
of M
iho
Noza
ki M
D, P
hD

Ophthalmologists may want to advise glaucoma patients to reduce their intake of caffeine. A recent study suggests that
the greater the intake of caffeine, the more intraocular pressure increases, reported Damrong Wiwatwongwana MD at the 5th World Glaucoma Congress.
Caffeine is known to produce a number of physiologic changes, including temporary increases in blood pressure and increased heart rate. It is a vasoconstrictor, and can affect muscle contractility. In the eye, animal studies show it can increase aqueous production, plus can reduce aqueous drainage by causing the fenestrae at the chamber angle to narrow, according to Dr Wiwatwongwana, Department of Ophthalmology at Chiang Mai University, Thailand.
The evidence in the scientific literature about the effects of caffeine on IOP is conflicting. Importantly, there were no studies investigating possible dose-effects of caffeine on IOP. To address this, Dr Damrong Wiwatwongwana and colleagues conducted a study comparing the effects of different levels of caffeine on the IOP of healthy, non-glaucomatous volunteers in a double-blinded, randomised, controlled trial.
A total of 63 healthy young adults, half of who were female, were randomly assigned to one of three coffee-drinking groups, with 21 subjects in each. People with a baseline IOP of 21mmgHg or higher were excluded. Subjects were asked to avoid beverages that contained caffeine for three days before the study.
IOP was measured prior to coffee consumption, and again 30, 60 and 90 minutes after drinking coffee. Central corneal thickness (CCT) was also measured. Each
subject was given 360ml of coffee, with the caffeine levels being 2.0mg of caffeine in the decaffeinated group; 170mg in the second group, and 340mg in the third.Baseline IOP was an average of 13.25 mmHg across the groups. Thirty minutes after caffeine consumption, there was no significant change in IOP in any of the groups. At 60 minutes, IOP had increased to an average of 14.6 mmHg in the 340mg group, 13.6 mmHg in the 170mg groups and 13.4 mmHg in the 170mg group. The change in the high dose caffeine group was statistically significant.
By 90 minutes after consuming caffeine, IOP in the 340mg group increased to an average of 15.19mmHg, a significant change Dr Wiwatwongwana said. Those in the 170mg caffeine and control groups had an average IOP of about 13.7 mmHg at 90 minutes.
This level of an effect of higher levels of caffeine consumption over a short period of time could have clinical implications for both screening and monitoring of glaucoma patients, he said. Whether this effect is magnified in glaucoma patients needs further study.
Caffeine appears in a number of products including coffee, tea, cola beverages and chocolate. A regular cup of coffee of 236ml typically contains 135 to 150mg of caffeine. A single shot of espresso typically contains 106mg of caffeine. A 16 ounce or grande cup of brewed coffee usually contains the same as three espresso shots.
“Patients who are heavy coffee drinkers should be advised to reduce their consumption,” he said.
EUROTIMES | Volume 18 | Issue 10
contact Damrong Wiwatwongwana – [email protected]
CAFFEINE AND IOPGlaucoma patients cautionedby Pippa Wysong in Vancouver
36 Update
GLAUCOMA
Optimize Patient Care Recognize and Treat MGD
Visit TearScience Booth #I03 at ESCRS
Speak with the Experts on Saturday, 5 October
Eric Donnenfeld, MD Alan Carlson, MD12:00 - 1:00 p.m.
Lunch Meeting: Sunday, 6 October 1:00 - 2:00 p.m.
Elicium Building, Level 5, Room D503
Guest Speakers:Alan Carlson, MDDavid Finis, MD
Thomas Kaercher, MDStephen Lane, MD
Matteo Piovella, MDRohit Shetty, MD
RSVP for lunch meeting to [email protected]. 13-ADV-121 REV A
Marguerite McDonald, MD3:00 - 4:00 p.m.
Cour
tesy
of D
amro
ng W
iwat
wong
wana
MD

Technolas Perfect Vision GmbH - A Bausch + Lomb CompanyMesserschmittstr. 1 + 3, 80992 Munich, Germany www.technolas.com / www.bausch.com
BAUSCH + LOMB TECHNOLAS ® Laser Suite -
Only Bausch + Lomb Technolas offers such a level of versatility and performance.
VICTUS™
FemtosecondLaserPlatform
The VICTUS platform has CE Marking for capsulotomy, lens fragmentation, arcuate corneal incisions, LASIK flap, INTRACOR®, and keratoplasty. Indications may vary by country.The VICTUS platform is cleared in the United States for creation of a corneal flap in patients undergoing LASIK surgery or other treatment requiring initial lamellar resection of the cornea and
anterior capsulotomy during cataract surgery. The New TECHNOLAS® TENEO™ 317 Excimer Laser is CE Mark pending. Indications may vary by country.The trademarks (™ and ®) and logos used in this document are the property of Bausch & Lomb Incorporated or its a�liates. kbcomunicacion Ref BLT 053-09/13
© 2013 Bausch & Lomb Incorporated. All rights reserved.
Register for our LUNCHTIME SYMPOSIUM
Eurotimes Ad ESCRS 2013:BLT 6/9/13 14:52 Página 1
EUROTIMES | Volume 18 | Issue 10
38
www.karger.com/cop
New Books in OphthalmologyESASO Course Series
F. Bandello, B. Corcóstegui
Vol. 3
CataractEditor
J.L. Güell
Developments in Ophthalmology, Vol. 50
Glaucoma Surgery Editors: Bettin, P. (Milan); Khaw, P.T. (London) XII + 188 p., 45 fig., 38 in color, 8 tab., hard cover, 2012 CHF 198.– /EUR 165.– / USD 233.00 ISBN 978–3–8055–9937–5
Prices subject to changeEur price for Germany,
USD price for USA only
ESASO Course Series
F. Bandello, B. Corcóstegui
Vol. 2
Surgical RetinaEditors
F. BandelloM. Battaglia Parodi
Developments in Ophthalmology
Editor: F. Bandello
Vol. 52
Ophthalmic Radiation Therapy Techniques and Applications
Editors
A.D. SinghD.E. PelayesS. SeregardR. Macklis
ESASO Course Series
F. Bandello, B. Corcóstegui
Vol. 1
Medical RetinaEditors
F. BandelloG. Querques
De elopments in Ophthalmolog
Developments in Ophthalmology
Editor: F. Bandello
Vol. 50
GlaucomaSurgeryEditors
P. BettinP.T. Khaw
Developments in Ophthalmology
Editor: F. Bandello
Vol. 51
New Treatments in Noninfectious UveitisEditors
E. MiserocchiG. ModoratiC.S. Foster
ESASO Course Series, Vol. 3
CataractEditor: Güell, J.L. (Barcelona)VIII +140 p., 178 fig., 168 in color, 5 tab., soft cover, 2013CHF 98.– / EUR 82.– / USD 115.00ISBN 978–3–318–02410–4
ESASO Course Series, Vol. 2
Surgical Retina ESASO modules 2009 and 2010:Selected contributions Editors: Bandello, F. (Milan); Battaglia Parodi, M. (Milan) X + 178 p., 89 fig., 56 in color, 23 tab., soft cover, 2012 CHF 98.– / EUR 82.– / USD 115.00 ISBN 978–3–318–02158–5
ESASO Course Series, Vol. 1
Medical Retina ESASO modules 2009 and 2010: Selected contributions Editors: Bandello, F. (Milan); Querques, G. (Paris) X + 160 p., 88 fig., 68 in color, 10 tab., soft cover, 2012 CHF 98.– / EUR 82.– / USD 115.00 ISBN 978–3–8055–9990–0
Developments in Ophthalmology, Vol. 52
Ophthalmic Radiation TherapyTechniques and ApplicationsEditors: Singh, A.D. (Cleveland, Ohio); Pelayes, D. (Buenos Aires); Seregard, S. (Stockholm); Macklis, R. (Cleveland, Ohio)XIV + 126 p., 49 fig., 42 in color, 7 tab., hard cover, 2013CHF 189.– / EUR 158.– / USD 222.00 ISBN 978–3–318–02440–1
Developments in Ophthalmology, Vol. 51
New Treatments in Noninfectious Uveitis Editors: Miserocchi, E. (Milan); Modorati, G. (Milan); Foster, C.S. (Cambridge, Mass.) XII + 166 p., 14 fig., 8 in color, 24 tab., hard cover, 2012 CHF 159.– / EUR 133.– / USD 187.00 ISBN 978–3–8055–9986–3
S. Karger AGP.O. BoxCH–4009 Basel (Switzerland)Tel. +41 61 306 11 11 Fax +41 61 306 12 [email protected]
Journals Ophthalmologicawww.karger.com/oph
Open access, online only, peer reviewed
For further information and easy ordering please go to www.karger.com/ophthalmology
www.karger.com/orewww.karger.com/oop
NEW!
KI13
476_
ESCR
S
While ophthalmologists eagerly await the appearance of ROCK (Rho-associated protein kinase)-inhibitors,
a potential new class of anti-glaucoma medication, there are still some bumps along the way. One is that a frequent side effect of candidate compounds is hyperaemia.
But early indicators show a substantial range of benefits from ROCK-inhibition make them worthy of pursuit, and one candidate has even made it to a phase-3 clinical trial, according to Megumi Honjo MD, PhD, from the Department
of Ophthalmology, Tokyo Metropolitan Geriatric Hospital. At the 5th World Glaucoma Congress she presented an update of research pertaining to ROCK-inhibitors.
ROCK-inhibitors target the trabecular meshwork causing it to undergo some degree of remodelling of tissue architecture to improve aqueous flow. The compounds play a role in regulating the shape and movement of cells by acting on the cytoskeleton.
"The behaviour of cells and extracellular matrix is responsible for the resistance of the outflow. Various drugs (in the ROCK-inhibitor category) acting on the
cytoskeleton have also been shown to increase aqueous outflow by acting directly on outflow tissue," she said.
Her group reported IOP-lowering effects of the ROCK inhibitor Y-27632 in 2001, though there are several additional compounds under development by various research groups globally.
At this point approval of the clinical use of ROCK inhibitors is still uncertain, she said. But this category of drug is an exciting direction for new glaucoma treatments. In an earlier animal study, her group applied a topical ROCK-inhibitor in living rabbits and
showed a significantly lowered rabbit IOP with a two-fold increase in aqueous outflow.
IOP lowering In humans, some studies demonstrated a lowering of IOP by 3.0 to 4.0 mmHg within a couple of hours of topical administration. ROCK-inhibitors increase retinal blood flow around the optic disc, can protect neurons against various stresses and promote regeneration of crushed retinal ganglion cell axons. They may even reduce post-surgical scarring, she said.
Overall, several candidate drugs didn’t make it past phase 1 and 2 human clinical trials due to safety and tolerability issues, Dr Honjo said. In one study, of Y-39983, IOP levels decreased following administration in a dose-dependent manner in human volunteers, and normal levels were restored by 24 hours, but conjunctive hyperaemia was observed.
In fact, one study showed conjunctival hyperaemia occurred in 60 per cent of patients – showing this is a recurring problem with these agents. Several agents have been taken out of the race because of side effects.
by Pippa Wysong in Vancouver
ROCK-inhibitors still promising, but associated with increased hyperaemiaGLAUCOMA PIPELINE
Update
GLAUCOMA
Megumi Honjo – [email protected]
cont
act

39
EUROTIMES | Volume 18 | Issue 10
However you say it, the EyeBag is the one effective, fully compliant treatment for patients suffering from Blepharitis, MGD or Dry Eye Syndromes.
Warm CompressWarme KompresseMascara CalienteMasque ChauffantMaschera CaldaCiepły Kompres
For product information or details of how to become a stockist, please visit www.eyebags.com
of users report a significant improvement in symptoms.95%EyeBags sold to date200,000
Invented and developed by: Consultant ophthalmic surgeon, Teifi James FRCP FRCS FRCOphth
Philippe Denis – [email protected]
contact
Many glaucoma patients present with an ocular surface disease related to their therapy, in particular those using
IOP-lowering medications containing the preservative benzalkonium chloride (BAK). This can directly affect their quality of life and compliance rates.
“In recent years, we have become more aware of the negative effects of BAK on the ocular surface, so we need to consider preservative-free glaucoma medications where possible in order to preserve the ocular surface and help contain the onset or worsening of this secondary condition in glaucoma patients,” Philippe Denis MD told the 2013 Congress of the European Society of Ophthalmology (SOE).
Dr Denis, Hopital de la Croix-Rousse, Lyon, France, noted that ocular surface disease is commonly associated with glaucoma.
“Both glaucoma and dry eye syndrome (DES) occur in older populations so it is not surprising that there is a clear overlap between the two conditions, with DES prevalent in glaucoma patients and vice versa. There is also a clear relationship between glaucoma eye drops and dry-eye symptoms, and glaucoma surgery may also be a risk factor for patients with DES,” he said.
The association between glaucoma and DES has been borne out by research in the scientific literature, said Dr Denis. One study by Leung et al in 2008 showed that a large proportion of patients (59 per cent) with open-angle glaucoma or ocular hypertension had signs and/or symptoms of ocular surface disease in at least one eye.
“Glaucoma is a chronic life-long condition and glaucoma and DES are often concomitant diseases. Ocular tolerability influences quality of life and adherence. Insufficient tolerability may lead to discontinuation of the glaucoma treatment and a lack of compliance, so the consequences are potentially very serious,” he said.
Focusing on BAK, Dr Denis noted that it is responsible for several components of poor ocular tolerability and worsening of dry eye symptoms.
“Studies have shown that topical anti-glaucoma eye drops containing BAK alter the conjunctival surface, with increased
conjunctival inflammation and activation of macrophages, lymphocytes and mast cells, and an increase in the number of fibroblasts increasing connective tissue and conjunctival metaplasia,” said Dr Denis.
BAK also has implications for glaucoma surgery, said Dr Denis.
“Bleb failure has been associated with increased conjunctival infiltration of fibroblasts and inflammatory cells. Long-term anti-glaucoma therapy is associated with increased rates of surgical failure, with the failure risk depending on the duration and number of treatments,” he said.
A study by Fukuda et al. comparing additives in anti-glaucoma prostaglandin ophthalmic formulations which compared symptoms of eye drops with and without BAK found significant differences between the medications, said Dr Denis. Symptoms such as red eye, burning, foreign body sensation, dryness and itching were all worse with medications containing BAK.
Another study by Jaenen et al also found that preserved eye drops showed much higher readings for anterior blepharitis, posterior blepharitis, eczema, conjunctival signs and hyperaemia than with non-preserved drops.
BAK toxicity is a rapid, cumulative, dose-related and chronic phenomenon, said Dr Denis. While BAK is also neurotoxic, a study by Sarkar et al suggests that discontinuing BAK exposure to the cornea may allow some nerves with disrupted axonal function to recover structurally.
“Therefore it is possible that discontinuation of BAK-preserved eye drops improves corneal function,” concluded Dr Denis.
Update
GLAUCOMA
by Dermot McGrath in Copenhagen
BAK-free alternatives may preserve ocular surface in glaucoma patients
GLAUCOMA AND DES
BAK toxicity is a rapid, cumulative, dose-related and chronic phenomenon
“Philippe Denis

EUROTIMES | Volume 18 | Issue 10
40
People with ocular hypertension or glaucoma who take glucosamine supplements for osteoarthritis may be increasing their risk for
glaucoma onset or progression, according to the results of a study by a team of researchers at the University of New England College of Osteopathic Medicine, Biddeford, Maine, US.
The retrospective study, reported in a research letter in the July 2013 issue of JAMA Ophthalmology, involved 17 patients with ocular hypertension or open-angle glaucoma who were also taking glucosamine supplements. The study showed that the patients' mean IOP rose significantly after they started talking the supplement and fell when they stopped taking it.
The study included six men and 11 women with a mean age of 76 years. The researchers divided the patients into two groups. One group was composed of 11 patients who had undergone at least one IOP measurement before they began glucosamine supplementation and the other group was composed of six patients who had no IOP measurements before they began taking the supplement. None of the patients had any changes in their medication regimens that might have confounded the study results.
“Once I began to notice a possible correlation between glucosamine and IOP, I began to ask patients if they would mind stopping their supplement and re-measure their IOP on the hunch that
it might have a bearing on their problem. As I thought I was seeing a trend, I began to advise all of my patients where I suspected an association between the supplement and elevated IOP that if they chose to stop the glucosamine, I would recheck IOPs for them. After we tripped over 20 such patients, we decided to do a retrospective study in order to see if my hunch stood up to scientific scrutiny,” Edward Hall Jaccoma MD, the study’s principal investigator told EuroTimes in an interview.
In the patients with IOP measurements from before they began the supplementation, IOP increased significantly while they received the supplement (P=.001) and then decreased significantly when they stopped taking the supplement (P=.002). In the group with no IOP measurements prior to glucosamine supplementation IOP also decreased significantly following discontinuation of the supplement (P=.008). In the two
cohorts combined, discontinuation of the supplement regimen resulted in a mean decrease in IOP of 2.8mmHg in right eyes, from 19.5 mmHg to 16.7 mmHg, and a mean decrease of 3.0 mmHg in left eyes, from 20.3 mmHg to 17.3 mmHg (P<.001).
“Many questions are raised by glucosamine supplementation-associated IOP changes. This study shows a reversible effect of those changes, which is reassuring. However, the possibility that permanent damage can result from prolonged use of glucosamine supplementation is not eliminated,” the authors concluded.
Role of glycosaminoglycans The mechanism whereby glucosamine supplementation might cause IOP to rise may relate to its role in the body as precursor for glycosaminoglycans. There is some research which indicates that deposits of glycosaminoglycans in the trabecular meshwork restrict the outflow of aqueous. Alternatively, the release of high amounts of glycosaminoglycans into the aqueous may result in an osmotic effect that draws more water into the anterior chamber which in turn causes swelling and a decrease of pore size in the trabeculum leading ultimately to a resistance in outflow.
It remains to be seen whether pharmacologically modulating the glycosaminoglycan content of the eye could have therapeutic effects, Dr Jaccoma said
“Glycosaminoglycans are a critical element of the trabecular meshwork and anything that can influence them, may also
influence glaucoma - either for the good, in a therapeutic role, or for the bad, as may be the case with glucosamine for some patients,” he added. “Since the study I have continued to monitor patients who are taking glucosamine supplements and find that there is a great deal of variability in how patients' IOP is affected. It appears to follow the steroid link to glaucoma in that some patients appear totally unaffected while others can have significant IOP spikes on this supplement. It does seem to affect patients with known glaucoma more frequently than those who don’t. So far, like steroids, the affect appears to wear off - usually over a month or so, once the supplement is stopped.”
Glucosamine supplements are widely used as a non-prescription treatment for osteoarthritis, a condition that affects around 27 million adults in the US alone. If the findings of this study are borne out by further research, it could have important public health implications. Unlike most of Europe, where glucosamine is approved as a medical drug, glucosamine is regarded by the USA FDA as a dietary supplement and evidence of safety and efficacy is not required as long as it is not advertised as a treatment for a medical condition. There are a range of supplements for which the potential for adverse effects are largely unknown and which may also pose dangers to ocular health, Dr Jaccoma said.
“We already know that many supplements can influence bleeding times and there are others that influence how some medications are absorbed, or can compete with other medications - and there are so many out there in an unregulated way, that great potential exists for untoward side effects. I am not advocating supplements be stopped, but I do think we need to continue to study their effects, including side effects, and to add some greater degrees of regulation to this industry,” he added.
Edward Hall Jaccoma – [email protected]
cont
act
GLUCOSAMINE AND GLAUCOMASupplement appears to induce elevation of IOP by Roibeard O’hEineachain
Update
GLAUCOMA
I am not advocating supplements be stopped, but I do think we need to continue to study their effects...
“Edward Hall Jaccoma MD
EUROTIMESESC
RS ™
РОССИЙСКИЙ ВЫПУСК
RUSSIAN LANGUAGE EDITION NOW ONLINE
Visit: www.eurotimesrussian.org
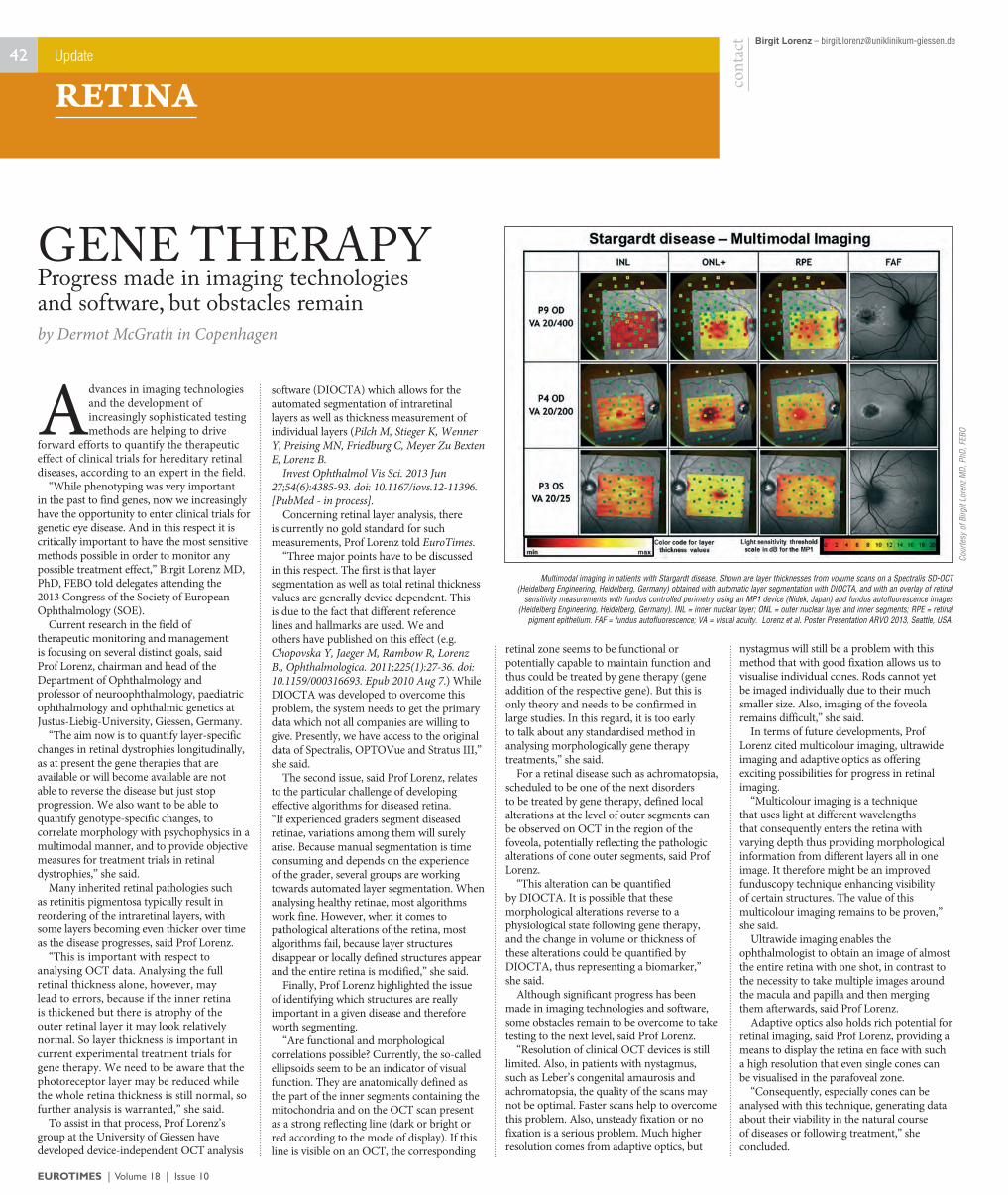
EUROTIMES | Volume 18 | Issue 10
42
Advances in imaging technologies and the development of increasingly sophisticated testing methods are helping to drive
forward efforts to quantify the therapeutic effect of clinical trials for hereditary retinal diseases, according to an expert in the field.
“While phenotyping was very important in the past to find genes, now we increasingly have the opportunity to enter clinical trials for genetic eye disease. And in this respect it is critically important to have the most sensitive methods possible in order to monitor any possible treatment effect,” Birgit Lorenz MD, PhD, FEBO told delegates attending the 2013 Congress of the Society of European Ophthalmology (SOE).
Current research in the field of therapeutic monitoring and management is focusing on several distinct goals, said Prof Lorenz, chairman and head of the Department of Ophthalmology and professor of neuroophthalmology, paediatric ophthalmology and ophthalmic genetics at Justus-Liebig-University, Giessen, Germany.
“The aim now is to quantify layer-specific changes in retinal dystrophies longitudinally, as at present the gene therapies that are available or will become available are not able to reverse the disease but just stop progression. We also want to be able to quantify genotype-specific changes, to correlate morphology with psychophysics in a multimodal manner, and to provide objective measures for treatment trials in retinal dystrophies,” she said.
Many inherited retinal pathologies such as retinitis pigmentosa typically result in reordering of the intraretinal layers, with some layers becoming even thicker over time as the disease progresses, said Prof Lorenz.
“This is important with respect to analysing OCT data. Analysing the full retinal thickness alone, however, may lead to errors, because if the inner retina is thickened but there is atrophy of the outer retinal layer it may look relatively normal. So layer thickness is important in current experimental treatment trials for gene therapy. We need to be aware that the photoreceptor layer may be reduced while the whole retina thickness is still normal, so further analysis is warranted,” she said.
To assist in that process, Prof Lorenz’s group at the University of Giessen have developed device-independent OCT analysis
software (DIOCTA) which allows for the automated segmentation of intraretinal layers as well as thickness measurement of individual layers (Pilch M, Stieger K, Wenner Y, Preising MN, Friedburg C, Meyer Zu Bexten E, Lorenz B.
Invest Ophthalmol Vis Sci. 2013 Jun 27;54(6):4385-93. doi: 10.1167/iovs.12-11396. [PubMed - in process].
Concerning retinal layer analysis, there is currently no gold standard for such measurements, Prof Lorenz told EuroTimes.
“Three major points have to be discussed in this respect. The first is that layer segmentation as well as total retinal thickness values are generally device dependent. This is due to the fact that different reference lines and hallmarks are used. We and others have published on this effect (e.g. Chopovska Y, Jaeger M, Rambow R, Lorenz B., Ophthalmologica. 2011;225(1):27-36. doi: 10.1159/000316693. Epub 2010 Aug 7.) While DIOCTA was developed to overcome this problem, the system needs to get the primary data which not all companies are willing to give. Presently, we have access to the original data of Spectralis, OPTOVue and Stratus III,” she said.
The second issue, said Prof Lorenz, relates to the particular challenge of developing effective algorithms for diseased retina. “If experienced graders segment diseased retinae, variations among them will surely arise. Because manual segmentation is time consuming and depends on the experience of the grader, several groups are working towards automated layer segmentation. When analysing healthy retinae, most algorithms work fine. However, when it comes to pathological alterations of the retina, most algorithms fail, because layer structures disappear or locally defined structures appear and the entire retina is modified,” she said.
Finally, Prof Lorenz highlighted the issue of identifying which structures are really important in a given disease and therefore worth segmenting.
“Are functional and morphological correlations possible? Currently, the so-called ellipsoids seem to be an indicator of visual function. They are anatomically defined as the part of the inner segments containing the mitochondria and on the OCT scan present as a strong reflecting line (dark or bright or red according to the mode of display). If this line is visible on an OCT, the corresponding
retinal zone seems to be functional or potentially capable to maintain function and thus could be treated by gene therapy (gene addition of the respective gene). But this is only theory and needs to be confirmed in large studies. In this regard, it is too early to talk about any standardised method in analysing morphologically gene therapy treatments,” she said.
For a retinal disease such as achromatopsia, scheduled to be one of the next disorders to be treated by gene therapy, defined local alterations at the level of outer segments can be observed on OCT in the region of the foveola, potentially reflecting the pathologic alterations of cone outer segments, said Prof Lorenz.
“This alteration can be quantified by DIOCTA. It is possible that these morphological alterations reverse to a physiological state following gene therapy, and the change in volume or thickness of these alterations could be quantified by DIOCTA, thus representing a biomarker,” she said.
Although significant progress has been made in imaging technologies and software, some obstacles remain to be overcome to take testing to the next level, said Prof Lorenz.
“Resolution of clinical OCT devices is still limited. Also, in patients with nystagmus, such as Leber’s congenital amaurosis and achromatopsia, the quality of the scans may not be optimal. Faster scans help to overcome this problem. Also, unsteady fixation or no fixation is a serious problem. Much higher resolution comes from adaptive optics, but
nystagmus will still be a problem with this method that with good fixation allows us to visualise individual cones. Rods cannot yet be imaged individually due to their much smaller size. Also, imaging of the foveola remains difficult,” she said.
In terms of future developments, Prof Lorenz cited multicolour imaging, ultrawide imaging and adaptive optics as offering exciting possibilities for progress in retinal imaging.
“Multicolour imaging is a technique that uses light at different wavelengths that consequently enters the retina with varying depth thus providing morphological information from different layers all in one image. It therefore might be an improved funduscopy technique enhancing visibility of certain structures. The value of this multicolour imaging remains to be proven,” she said.
Ultrawide imaging enables the ophthalmologist to obtain an image of almost the entire retina with one shot, in contrast to the necessity to take multiple images around the macula and papilla and then merging them afterwards, said Prof Lorenz.
Adaptive optics also holds rich potential for retinal imaging, said Prof Lorenz, providing a means to display the retina en face with such a high resolution that even single cones can be visualised in the parafoveal zone.
“Consequently, especially cones can be analysed with this technique, generating data about their viability in the natural course of diseases or following treatment,” she concluded.
by Dermot McGrath in Copenhagen
Progress made in imaging technologies and software, but obstacles remain
GENE THERAPY
Update
RETINA
Birgit Lorenz – [email protected]
cont
act
Multimodal imaging in patients with Stargardt disease. Shown are layer thicknesses from volume scans on a Spectralis SD-OCT (Heidelberg Engineering, Heidelberg, Germany) obtained with automatic layer segmentation with DIOCTA, and with an overlay of retinal
sensitivity measurements with fundus controlled perimetry using an MP1 device (Nidek, Japan) and fundus autofluorescence images (Heidelberg Engineering, Heidelberg, Germany). INL = inner nuclear layer; ONL = outer nuclear layer and inner segments; RPE = retinal
pigment epithelium. FAF = fundus autofluorescence; VA = visual acuity. Lorenz et al. Poster Presentation ARVO 2013, Seattle, USA.
Cour
tesy
of B
irgit
Lore
nz M
D, P
hD, F
EBO

43
EUROTIMES | Volume 18 | Issue 10
Sheraz M. Daya, MD Damien Gatinel, MD
ESCRS Lunch Symposium
13:00-14:00 on 6th October 2013 @ E107, Amsterdam RAI
Sheraz M. Daya, MD, FACP, FACS, FRCS (Ed), FRCOphthMedical Director, Centre for Sight, UK
A New Fast Biometer: The AL-Scan Technology and Comparative Data with Zeiss IOL Master
Damien Gatinel, MDHead of Anterior Segment and Refractive Surgery Dept.,
Optimizing Pre-Cataract Diagnostics: Efficient Data Collection with NIDEK
Instruments and IOL-Station Software
Speakers
Moderators
Ekkehard Fabian, MDAugenCentrum Rosenheim, Germany
The Importance of Endothelial Cell Count in Cataract Surgery: Evaluation of The NIDEK CEM-530 Specular Microscope
Omid Kermani, MDAugenklinik am Neumarkt, Germany
My Experience with NIDEK IOL Aktis SP, SZ-1 and Pre-Cataract WF Aberrometry
New Diagnostic Frontiersin Cataract and Refractive Lens Exchange
New Diagnostic Frontiersin Cataract and Refractive Lens Exchange
Rothschild Foundation, France
D04
The inhibition of vascular endothelial growth factor provides a substantial long-term benefit in patients with macular oedema
secondary to branch retinal vein occlusion, Sandra Rezar MD told delegates attending the 2013 Congress of the Society of European Ophthalmology (SOE).
“Our study with a mean follow-up of five years found good long-term functional and anatomical outcomes using anti-VEGF treatment in patients with branch retinal vein occlusion, with an average gain of 15 letters of visual acuity, significantly reduced retinal thickness and improved retinal sensitivity,” she reported.
She added that early intervention and rigorous follow-up with anti-VEGF agents such as bevacizumab or ranibizumab are important to ensure optimal patient outcomes, and advised using 200-degree wide-field angiography for the evaluation of the peripheral retina.
Dr Rezar, Medical University of Vienna, Austria, said that retinal vein occlusion (RVO) is a sight-threatening retinal vascular disorder associated with macular oedema and neovascularisation that affects an estimated 16.4 million people worldwide. Branch retinal vein occlusion is the most common type (13.9 million) compared to central retinal vein occlusion (2.5 million).
While the exact pathogenesis of the occlusion is not well understood, various local and systemic factors appear to play a role in the pathological closure of the retinal veins. Patients with retinal vein occlusion can additionally suffer from cardiovascular disease or stroke, said Dr Rezar.
In the event of macular oedema occurring secondary to the RVO, the standard treatment is now to use anti-VEGF injections or corticosteroids such as dexamethasone or triamcinolone.
“While a number of studies have demonstrated the short-term safety and efficacy of anti-VEGF treatments for RVO, there really is not a lot of data available concerning the long-term outcome of these patients,” said Dr Rezar.
The study conducted by the Macula Study Group of Vienna evaluated an initial cohort of 54 patients treated for macula oedema secondary to branch retinal vein occlusion. Twenty-five patients received intravitreal
ranibizumab injections and the remaining 29 patients were treated with bevacizumab. After a mean follow-up of five years, 28 of the patients were included in the cross-sectional study.
Main outcome measures included mean change in best-corrected visual acuity (BCVA) from baseline, change in central retinal thickness (CRT) and retinal sensitivity (CRS). Follow-up at a mean of six years was slightly longer for the bevacizumab patients compared to four years for those treated with ranibizumab.
Mean time The mean time between onset of RVO and initial treatment was 188 days (±141) for the 14 patients in the bevacizumab treated group and 51 days (±31) for the other 14 patients in the ranibizumab group.
Patients received an average of nine intravitreal injections for bevacizumab and six for ranibizumab, while another 10 patients received segmental laser coagulation.
Dr Rezar noted that the frequency of injections diminished significantly over time, from an average of 3.82 per patient in the first six months of treatment, to 0.25 in months 37 to 42.
In the bevacizumab group, the average visual acuity increased by six letters, which was not, however, statistically significant, CRS improved by 3.1dB and CRT thickness decreased by 162 µm. In the ranibizumab group, visual acuity and CRS also increased significantly (27 letters and 4.6dB) and the CRT decreased 229µm.
by Dermot McGrath in Copenhagen
Safe and effective long-term in retinal vein occlusion
Update
RETINA
ANTI-VEGF
contact Sandra Rezar & Stefan Sacu
Our study with a mean follow-up of five years found good long-term functional and anatomical outcomes
“Sandra Rezar MD

EUROTIMES | Volume 18 | Issue 10
44
What is the optimal approach for treating a patient with macular degeneration who develops a submacular
haemorrhage? Jan van Meurs MD, a vitreoretinal surgeon at the Rotterdam Eye Hospital, and colleagues have initiated a prospective clinical trial to compare existing treatments.
Treatment options are generally quite limited and the prognosis is guarded. Intravitreal anti-VEGF agents are the standard of care for exudative AMD. However, they are not effective in restoring or improving visual acuity when a large submacular haemorrhage is present. Further, the haemorrhage causes not only immediate visual loss, it is also retinotoxic, leading to permanent damage.
Designed with colleague Elsbeth van Zeeburg MD at the Rotterdam Ophthalmic Institute, the prospective, single-centre, comparative intervention study is randomising patients with a submacular haemorrhage of less than two weeks old to either a more invasive approach - vitrectomy followed by submacular rt-PA, intravitreal C3F8 / air mixture and intravitreal bevacizumab, or a less invasive approach utilising intravitreal (rather than submacular) rt-PA, C3F8 gas tamponade and intravitreal bevacizumab.
In preparation for this ambitious study, the researchers performed a literature review of the procedures. The Submacular Surgery Trial, a randomised, prospective trial published nearly 10 years ago, evaluated the outcomes of observation versus surgery. The trials found that vitrectomy
with removal of the (older) subretinal haemorrhage could not improve or stabilise visual acuity compared to observation. However, eyes receiving surgery were more likely to avoid severe vision loss despite a higher complication rate compared with controls.
An alternative technique of more acute hemorrhages involves pneumatic displacement of the blood, to an area inferior in the eye, away from the fovea, where it causes less damage when resorbed. A standard vitrectomy is performed, subretinal tissue plasminogen activator (rt-PA) is delivered via a 41-gauge cannula, and gas is instilled into the eye. Postoperative half-prone (45° anterior head-tilt) positioning can result in extramacular displacement of blood.
A third technique, intravitreal injection of expansile gas such as SF6 or C3F8, along with the same half-prone positioning, with or without adjunctive intravitreal rt-PA, has also been described.
Despite the various possibilities, many patients have gone untreated because of
the lack of proper comparative research to determine the safest and most effective modality or combination thereof. The recent trend has been towards the most invasive combination, namely vitrectomy followed by subretinal rt-PA and gas tamponade. However, whether the primary mechanism for haemorrhage displacement is the pushing or rolling action of a partial tamponade or the effect of gravity or pressure due to a complete tamponade is as yet unclear.
Besides their review of the literature, Drs van Meurs and van Zeeburg had prior experience evaluating this procedure, although for another indication. In this case, it was for acute haemorrhages caused by retinal arterial macroaneurysms. In this study, large haemorrhages were completely displaced from the submacular retina of 10 of 11 patients. Mean visual acuity improvement of all patients was 1.3 logMAR, suggesting outcomes better than natural history.
Macular Function But what about those patients whose macular function has been essentially destroyed in the course of exudative AMD? This includes those patients where anti-VEGF has proven futile; patients with AMD and a tear in the retinal pigment epithelium; or in patients with AMD and massive haemorrhage, too old to be displaced with rtPA (greater than14 days).
The macular surgery research team has developed a technique to replace the damaged tissue with healthy autologous tissue. The surgeon removes the damaged choroid and RPE and translocates healthy
choroid and RPE from the periphery to the macula. This free transplant is inserted under the retina via a parafoveal retinotomy.
Prof van Meurs, Dr van Zeeburg and Kristel Maaijwee MD, a fellow in vitreoretinal surgery, have made this topic a primary focus of their research work. A prospective study of 133 consecutive patients who underwent the procedure, reported encouraging results. Re-vascularisation and subsequent perfusion of the graft, as visualised on OCT, has been confirmed, with this study published in IOVS (Van Zeeburg et al, 2011, July 29 ; 52(8)). Fixation on the graft, as evaluated by microperimetry, suggests that the graft, and not the removal of the pathology submacular tissue or haemorrhage, was responsible for the preservation of macular function in these patients.
The multicentre, randomised trial comparing RPE-choroid graft surgery with anti-VEGFstarted in 2010 was, unfortunately, aborted because inclusion was as calculated in Rotterdam only, with the consequence that an insufficient number of patients could be recruited. The procedure is apparently not yet sufficiently standardised; a simplification of the technique (with a 180 degree peripheral retinotomy) may meet this failing.
Complications What about the complications of such an unusual surgery? Considering the retinotomies at the donor and recipient locations, retinal detachment due to proliferative vitreoretinopathy (PVR) might be a potential concern. Indeed, PVR occurred, in 10-16 per cent of patients.
When it comes to advanced exudative macular degeneration or large haemorrhages due to macroaneurysms, medical treatment is often insufficient. Submacular surgery might represent a viable option for those whose prognosis with standard treatment is highly guarded, Dr van Meurs commented. Most importantly, however, it is very likely that patients with an acute haemorrhage benefit from early displacement by a TPA and gas procedure, followed by continuation of anti-VEGF treatment.
AMD COMPLICATIONSSubmacular haemorrhage treatments comparedby Leigh Spielberg MD in Rotterdam
Read EuroTimes on the move!
Our new mobile website is designed for tablets and smartphones and includes content from the print edition of the magazine.
Visit the new EuroTimes mobile website at
http://m.eurotimes.org
Update
RETINA
Jan van Meurs – [email protected]
cont
act
“Submacular surgery might represent a viable option for those whose prognosis with standard treatment is highly guarded”

See your success in the eyes of your patients
De� ning the standard of care in myopic CNV*
©2013 Novartis Pharma AG LUC.146879August 2013Lucentis Indications may vary from country to country. Physicians should refer to their National Prescribing Information.Novartis Pharma AG CH-4002 Basel, Switzerland
LUCENTIS® (ranibizumab) ABBREVIATED UK PRESCRIBING INFORMATION Please refer to the SmPC before prescribing LUCENTIS 10mg/ml solution for injection. Presentation: A glass single-use vial containing 0.23ml solution containing 2.3mg of ranibizumab (10mg/ml). Indications: The treatment in adults of neovascular (wet) age-related macular degeneration (AMD), the treatment of visual impairment due to diabetic macular oedema (DMO), the treatment of visual impairment due to macular oedema secondary to retinal vein occlusion (branch RVO or central RVO), and the treatment of visual impairment due to choroidal neovascularisation (CNV) secondary to pathologic myopia (PM). Administration and Dosage: Single-use vial for intravitreal use only. LUCENTIS must be administered by a quali� ed ophthalmologist experienced in intravitreal injections under aseptic conditions. The recommended dose is 0.5 mg (0.05ml). For treatment of wet AMD: Treatment is given monthly and continued until maximum visual acuity is achieved i.e. The patient’s visual acuity is stable for three consecutive monthly assessments performed while on ranibizumab. Thereafter patients should be monitored monthly for visual acuity. Treatment is resumed when monitoring indicates loss of visual acuity due to wet AMD. Monthly injections should then be administered until stable visual acuity is reached again for three consecutive monthly assessments (implying a minimum of two injections). The interval between two doses should not be shorter than 1 month. For treatment of visual impairment due to either DMO or macular oedema secondary to RVO: Treatment is given monthly and continued until maximum visual acuity is achieved i.e. the patient’s visual acuity is stable for three consecutive monthly assessments performed while on ranibizumab treatment. If there is no improvement in visual acuity over the course of the � rst three injections, continued treatment is not recommended. Thereafter patients should be monitored monthly for visual acuity. Treatment is resumed when monitoring indicates loss of visual acuity due to DMO or to macular oedema secondary to RVO. Monthly injections should then be administered until stable visual acuity is reached again for three consecutive monthly assessments (implying a minimum of two injections). The interval between two doses should not be shorter than 1 month. LUCENTIS and laser photocoagulation in DMO and in macular oedema secondary to BRVO: When given on the same day, LUCENTIS should be administered at least 30 minutes after laser photocoagulation. LUCENTIS can be administered in patients who have received previous laser photocoagulation. For treatment of visual impairment due to CNV secondary to PM: Treatment is initiated with a single injection. If monitoring reveals signs of disease activity, e.g. reduced visual acuity and/or signs of lesion activity, further treatment is recommended. Monitoring for disease activity may include clinical examination, optical coherence tomography (OCT) or � uorescein angiography (FA). While many patients may only need one or two injections during the � rst year, some patients may need more frequent treatment. Therefore, monitoring is recommended monthly for the � rst two months and at least every three months thereafter during the � rst year. After the � rst year, the frequency of monitoring should be determined by the treating physician. The interval between two doses should not be shorter than one month. LUCENTIS and Visudyne photodynamic therapy in CNV secondary to PM: There is no experience of concomitant administration of LUCENTIS and Visudyne. Before treatment, evaluate the patient’s medical history for hypersensitivity. The patient should also be instructed to self-administer antimicrobial drops, 4 times daily for 3 days
before and following each injection. Children and adolescents: Not recommended for use in children and adolescents due to a lack of data. Elderly: No dose adjustment is required in the elderly. There is limited experience in patients older than 75 years with DMO Hepatic and renal impairment: Dose adjustment is not needed in these populations. Contraindications: Hypersensitivity to the active substance or excipients. Patients with active or suspected ocular or periocular infections. Patients with active severe intraocular in� ammation. Special warnings and precautions for use: LUCENTIS is for intravitreal injection only. Intravitreal injections have been associated with endophthalmitis, intraocular in� ammation, rhegmatogenous retinal detachment, retinal tear and iatrogenic traumatic cataract. Monitor during week following injection for infections. Patients should be instructed to report symptoms suggestive of any of the above without delay. Transient increases in intraocular pressure (IOP) within 1 hour of injection and sustained IOP increases have been identi� ed. Both IOP and perfusion of the optic nerve head should be monitored and managed appropriately. Concurrent use in both eyes has not been studied and could lead to an increased systemic exposure. There is a potential for immunogenicity with LUCENTIS which may be greater in subjects with DMO. Patients should report an increase in severity of intraocular in� ammation. LUCENTIS should not be administered concurrently with other anti-VEGF agents (systemic or ocular). Withhold dose and do not resume treatment earlier than the next scheduled treatment in the event of the following: a decrease in best corrected visual acuity (BCVA) of ≥30 letters compared with the last assessment of visual acuity; an intraocular pressure of ≥30 mmHg; a retinal break; a subretinal haemorrhage involving the centre of the fovea, or if the size of the haemorrhage is ≥50% of the total lesion area; performed or planned intraocular surgery within the previous or next 28 days. Risk factors associated with the development of a retinal pigment epithelial (RPE) tear after anti-VEGF therapy for wet AMD include a large and/or high pigment epithelial retinal detachment. When initiating LUCENTIS therapy, caution should be used in patients with these risk factors for RPE tears. Discontinue treatment in cases of rhegmatogenous retinal detachment or stage 3 or 4 macular holes. There is only limited experience in the treatment of subjects with DMO due to type I diabetes. LUCENTIS has not been studied in patients who have previously received intravitreal injections, in patients with active systemic infections, proliferative diabetic retinopathy, or in patients with concurrent eye conditions such as retinal detachment or macular hole. There is also no experience of treatment with LUCENTIS in diabetic patients with an HbA1c over 12% and uncontrolled hypertension. In PM patients there are no data on the use of LUCENTIS in patients with extrafoveal lesions and only limited data on its use in those who have had previous unsuccessful therapy with vertepor� n photodynamic therapy. Systemic adverse events including non-ocular haemorrhages and arterial thromboembolic events have been reported following intravitreal injection of VEGF inhibitors. There are limited data on safety in the treatment of DMO, macular oedema due to RVO and CNV secondary to PM patients with prior history of stroke or transient ischaemic attacks. Caution should be exercised when treating such patients. There is limited experience with treatment of patients with prior episodes of RVO and of patients with ischaemic BRVO and CRVO. Treatment is not recommended in RVO patients presenting with clinical signs of irreversible ischaemic visual function loss. Interactions: No formal interaction studies have been performed. In DMO and BRVO adjunctive use of laser therapy and LUCENTIS was not associated with any new ocular or non-ocular safety � ndings. Pregnancy and lactation: Women of
childbearing potential should use e¦ ective contraception during treatment. No clinical data on exposed pregnancies are available. Ranibizumab should not be used during pregnancy unless the expected bene� t outweighs the potential risk to the foetus. For women who wish to become pregnant and have been treated with ranibizumab, it is recommended to wait at least 3 months after the last dose of ranibizumab before conceiving. Breast-feeding is not recommended during the use of LUCENTIS. Driving and using machines: The treatment procedure may induce temporary visual disturbances and patients who experience these signs must not drive or use machines until these disturbances subside. Undesirable e� ects: Most adverse events are related to the injection procedure. Serious adverse events reported include endophthalmitis, blindness, retinal detachment, retinal tear and iatrogenic traumatic cataract. The safety data below include adverse events experienced following the use of LUCENTIS in the entire clinical trial population. Those marked * were only seen in the DMO population. Very Common: Intraocular pressure increased, headache, vitritis, vitreous detachment, retinal haemorrhage, visual disturbance, eye pain, vitreous � oaters, conjunctival haemorrhage, eye irritation, foreign body sensation in eyes, lacrimation increased, blepharitis, dry eye, ocular hyperaemia, eye pruritus, arthralgia, nasopharyngitis. Common: Urinary tract infection*, anaemia, retinal degeneration, retinal disorder, retinal detachment, retinal tear, detachment of the retinal pigment epithelium, retinal pigment epithelium tear, visual acuity reduced, vitreous haemorrhage, vitreous disorder, uveitis, iritis, iridocyclitis, cataract, cataract subcapsular, posterior capsule opaci� cation, punctuate keratitis, corneal abrasion, anterior chamber � are, vision blurred, injection site haemorrhage, eye haemorrhage, conjunctivitis, conjunctivitis allergic, eye discharge, photopsia, photophobia, ocular discomfort, eyelid oedema, eyelid pain, conjunctival hyperaemia, cough, nausea, allergic reactions, hypersensitivity, anxiety. Product-class-related adverse reactions: There is a theoretical risk of arterial thromboembolic events, including stroke and myocardial infarction, following intravitreal use of VEGF inhibitors. A low incidence rate of arterial thromboembolic events was observed in the LUCENTIS clinical trials in patients with AMD, DMO, RVO and PM and there were no major di¦ erences between the groups treated with ranibizumab compared to control. Please refer to the SmPC for full listing of all undesirable e¦ ects.
For UK: Adverse events should be reported. Reporting forms and information can be found at www.mhra.gov.uk/yellowcard. Adverse events should also be reported to Novartis Pharmaceuticals UK Ltd on (01276) 698370 or [email protected]
Legal category: POM, UK Basic NHS cost: £742.17. Marketing authorisation number: EU/1/06/374/001. Marketing authorisation holder: Novartis Europharm Limited, Wimblehurst Road, Horsham, West Sussex, RH12 5AB, United Kingdom. Full prescribing information, including SmPC, is available from: Novartis Pharmaceuticals, Frimley Business Park, Frimley, Camberley, Surrey, GU16 7SR. Telephone: 01276 692255. Fax: 01276 692508. Prepared July 2013.
* Visual impairment due to choroidal neovascularisation (CNV) secondary to pathologic myopia (PM)
48198 Eurotimes mCNV ad 270x320mm.indd 1 06/08/13 17:25
46
EUROTIMES | Volume 18 | Issue 10
Age-related macular degeneration (AMD) constitutes one of the main causes of macular disease in an elderly population,
affecting about one in every seven patients examined in a recent French population study, according to Catherine Creuzot-Garcher MD, PhD, FEBO.
“The initial results of this study looking at the prevalence of atrophic and neovascular age-related macular degeneration concurs with the findings of other population-based studies conducted in the literature. Nevertheless, we think that it would be interesting to compare these data, which were derived exclusively from fundus photographs, alongside those taken from optic coherence tomography, to give us a clearer picture of the disease prevalence in this population group,” she told the annual meeting of the French Society of Ophthalmology (SFO).
Prof Creuzot-Garcher, professor of ophthalmology and chair at the University Hospital of Dijon, France, noted that there is a critical need to learn as much as possible about the evolution of macular degeneration in older populations.
“This disease is the primary cause of reduced visual acuity in persons older than 50 in developed countries and is the third overall cause of blindness worldwide. And with populations tending to live longer in developed countries we are likely to see a huge increase in age-related diseases such as macular degeneration in the coming years,” she said.
Prof Creuzot-Garcher explained that the MONTRACHET study (Maculopathy, Optic Nerve, Nutrition, Neurovascular and heart diseases) was part of a wider population study of 9,000 patients older than 65 that began in 1999 in the French cities of Bordeaux, Dijon and Montpellier.
After 10 years of follow-up, the Dijon patient cohort also underwent a complete ophthalmological examination that included systematic colour fundus photographs of all patients.
The fundus images were analysed by two trained technicians and an ophthalmologist, and the prevalence of macular degeneration was classified according to objective criteria including number and size of drusen, presence of geographic atrophy and/or macular
degeneration based on the AREDS study classification.
The preliminary analysis included a total of 1,035 patients - 385 male and 650 female - with a mean age of 82.2 years (± 3.8), were included in the study. After analysis of the fundus photographs, 937 patients whose images were deemed to be of sufficient quality to enable interpretation were included in the final analysis.
AMD prevalence The prevalence of AMD was 4.2 per cent which was comparable to ALIENOR or the EUREYE studies, noted Prof Creuzot-Garcher.
Summing up, Prof Creuzot-Garcher said that population-based studies were extremely valuable in trying to learn more about possible risk factors for age-related pathologies such as macular degeneration.
“These are preliminary studies but they do give us valuable new data on the prevalence of macular degeneration and age-related maculopathy in a French population. We need more research to explore possible links between AMD and environmental factors, as well as neurological diseases linked to age and cardiovascular diseases,” she said.
by
I am quality
I am durable
I am reusable
I am innovative
I am effective
I am unique
I am cost-efficient
I am modern
I am steel & composite made
I am made by Moria
I am...
Moria is pleased to introduce coMposites! Composites by Moria is an innovative range of reusable instruments set to push the boundaries of ophthalmic instrumentation. This new generation of instruments offers the quality and precision you would expect from Moria, at a competitive price that will surprise the market. www.moria-surgical.com
escrs amsterdam october 5-8, 2013
come and visit us at Moria booth #e04
Catherine Creuzot-Garcher [email protected]
contact
by Dermot McGrath in Paris
French population study sheds light on AMD prevalence
MACULAR DISEASE
Update
RETINA
“With populations tending to live longer in developed countries we are likely to see a huge increase in age-related diseases such as macular degeneration in the coming years”

Building your ownpractice
Assumptions and truths
Measuringperformance
PracticeManagementWeekend 20131–3 NovemberFrankfurt, Germany
Meet the experts
From Concept to Commercial Product – An Entrepreneur’s StoryJohn Marshall
Growing a Small Ophthalmological PracticeArthur Cummings
Re-Inventing a Large Eye ClinicThomas Kohnen
Medicine, Marriage and MotherhoodEva-Maria Kohnen (pictured right) & Ina Conrad-Hengerer
From Small to Big – A Personal VoyageManfred Tetz
What they Don’t Teach you in Medical Training About the Business of HealthcarePaul Ursell
The Perfect/Imperfect BossKris Morrill
Analyse Your Practice Position bySetting Clear Targets Eckhard Weingaertner
Managing a DirectoratePaul Rosen
How Medical Marketing Can Help Build a Thriving ClinicRod Solar
€300 Registration fee Discounts available for additional practice members
Register online and see full programme:http://pmfrankfurt.escrs.org/
ESC
RS

EUROTIMES | Volume 18 | Issue 10
48
The potential of a revolutionary adaptor for ‘smartphones’ that allows telemedicine, surgery recording and high-quality
digital imaging during ophthalmic clinical exams, was showcased during the 2013 Irish College of Ophthalmology Annual Conference in Killarney, Ireland.
Princeton Lee MD, an ophthalmic surgery specialist registrar in the Royal Victoria Eye and Ear Hospital, Dublin, Ireland, gave a presentation on the ‘clip-on’ adaptor device he has created, which can be used to easily attach the majority of smart phones to slit lamps and operating microscopes.
This enables the capturing of digital images and videos with sound, of ocular examinations and procedures, and allows the digital files to be transferred to a computer via Wi-Fi or a direct connection.
“The other models that have been developed to date are phone specific and have limited adaptability to fit eyepieces of differing diameters. The difference between my design and what is currently available in the market is that my design can connect different brands of smartphone to eyepieces with varying diameters,” he told EuroTimes.
While the optical quality of ophthalmic examination instruments is very high, the lack of a built-in camera in most devices prevents the digital recording of important clinical information, Dr Lee told the conference, when explaining his rationale for designing the device.
Smartphones contain relatively high-quality cameras and file sharing capabilities, are widely available and portable, and by using the adaptor provide a very cost-effective way of digitising high-quality clinical images and videos for ophthalmic practice, he maintained.
The ease of transferring files from a smartphone to a computer allows rapid record keeping and is convenient for the clinician. For example, images can be used for personalised patient consultations and monitoring of progression, Dr Lee explained.
Telemedicine The device also enables the use of telemedicine by allowing the doctor to remotely assess the patient via a video telephone call, on Skype for example, with the adaptor attached so high-quality images and video can be seen directly in the clinic.
The adaptor can also be connected to the assistant eyepiece on an operating microscope allowing the viewing of live surgery in a remote location making it a useful education and teaching aid, especially in underdeveloped or disadvantaged areas, he told the conference.
Dr Lee is now in the process of patenting his device and negotiating with a manufacturer so that his adaptor can be purchased by the ophthalmic community in the near future.
Princeton Lee – [email protected]
cont
act
by Priscilla Lynch in Killarney
Smartphone adaptor allows convenient recording of photos and images in ophthalmology practice
EYE PHONE
Update
OCULAR
“ The adaptor can also be connected to the assistant eyepiece on an operating microscope allowing the viewing of live surgery in a remote location making it a useful education and teaching aid, especially in underdeveloped or disadvantaged areas.”
Images can be used for personalised patient consultations and monitoring of progression
“Princeton Lee MD
Different smartphones attached to the slit lamp with adaptors
Posterior segment photos taken with a smartphone attached to the slit lamp with an adaptor
Cour
tesy
of P
rince
ton
Lee
MD

MORE
Join this year’s
ESCRS symposia
with Bausch + Lomb
5th – 7th OCTOBER
13:00 – 14:00
Don’t forget to visit us at Booth G01
EXCLUSIVE
INSTRUMENTS
OFFERPurchase our top selling
instruments at special congress
prices. Reserve your favourite
instruments at www.storzeye.eu
PROCEDURAL
CHOICE
REGISTER TODAY!www.escrs.org/amsterdam2013/satellite-meetings.asp
®/™ are trademarks of Bausch & Lomb Incorporated or its affiliates. All other brand/product names are trademarks of their respective owners. © Bausch & Lomb Incorporated. EMEA/YEL/13/005c August 2013. SUR/SRG/13/082.
SATURDAY 5th OCTOBER Leading the way in new laser technology: Bausch + Lomb Technolas laser suite
RoomElicium 1
SpeakersProf R. Bellucci - Clinical Experience and Learnings with the VICTUS® Femtosecond Laser Platform
Prof S.P. Chee - Use of the VICTUS Femtosecond Laser Platform in both Routine and Challenging Cataract Cases
Dr P. Stodulka - Introducing the new TECHNOLAS Teneo™ 317 Excimer Laser Platform
Dr R.E. Ang - The Bausch + Lomb Technolas Laser Suite - How it has Expanded My Practice
SUNDAY 6th OCTOBER Sophisticated cataract surgery: Quantity and quality of vision
RoomEmerald
SpeakersProf D. Spalton - Phacoemulsifi cation in the 21st century: meeting patient expectations
Prof O. Findl - Correlating visual outcomes with OCT fi ndings
Prof R. Bellucci - Preventing common complications of cataract surgery
MONDAY 7th OCTOBER The cutting edge of MICS: Introducing INCISE® IOL
RoomEmerald
SpeakersProf D. Spalton - Introducing INCISE IOL
Prof B. Dick - INCISE IOL in clinical practice
Dr S. Morselli - Redefi ning MICS for every procedure
Prof R. Bellucci - Conclusion: the future of MICS
101776_symposium ad_270x320_v3.indd 1 02/09/2013 16:50

EUROTIMES | Volume 18 | Issue 10
50
“The financial crisis didn’t dominate my decision-making when I was looking for a job,” says
Sharmila Boekhoorn MD, who finished her ophthalmology residency in 2012. “My goal was to work in a large, high-quality, non-academic hospital with pleasant and engaging colleagues. And if I had to pay a members’ fee to join this type of partnership, then so be it.”
Dr Boekhoorn found full-time employment immediately after graduation. “I’m happy with ophthalmologists’ current situation, financially,” she continued, “but it’s widely known that finances will become tighter in the near future.”
With this in mind, the Dutch Ophthalmic Society has embarked on a wide scale policy of reorganisation over the past decade. The goal was to increase efficiency and reduce costs without compromising on quality or patients’ access to care, and also without drastically increasing the number of ophthalmologists per capita.
This reorganisation was initiated with the knowledge that the ageing of the population would lead to an increased demand for eye care while money available to pay for this care was unlikely to increase. It was achieved by transferring many non-invasive tasks from ophthalmologists to optometrists, orthoptists, opticians, ophthalmic technicians and even general practitioners.
The consensus is that this reorganisation was generally successful. Peter van Etten MD, has experienced the advantages of this reorganisation from two different positions. He is currently an ophthalmology resident in Rotterdam, but before going to medical school, he completed the optometry training and worked full-time as an optometrist for six years.
“The reorganisation was beneficial for us as optometrists because it expanded our role within the frame of patient care. We were brought right into the ophthalmology clinics to screen patients, participate in diagnostics, see patients postoperatively and follow up patients with chronic diseases. Our work became more interesting due to the broader scope of responsibilities that we have assumed.”
And now, as an ophthalmologist-in-training, Dr van Etten is again experiencing the benefits of the reorganisation. “Treating standard conditions like cataracts, advanced diabetic retinopathy, glaucoma and age-related macular degeneration has become more interesting and efficient for the ophthalmologist, because we can now focus our knowledge and energy on diagnostics, serious pathology and surgery. We can allow others to perform refraction, fundus photography, contact lens fitting and screening procedures. For example, optometrists do an excellent job screening fundus photographs for diabetic retinopathy.”
Although the Netherlands spends a relatively high percentage of its GNP on health care, relative to other countries, these costs come primarily from nursing homes and retirement homes rather than from hospital care. Further, quality is high and the patients’ financial contributions remain relatively low, notes Kees Sol, the Chief Financial Officer of the Rotterdam Eye Hospital.
This has all allowed the Netherlands to continue providing top-quality care despite having relatively few ophthalmologists per capita. There are approximately 740
ophthalmologists serving a population of nearly 17 million. Besides the reorganisation, ophthalmology started out with a built-in advantage prior to the financial crisis based on two situations. First, the amount of money allocated to ophthalmology in medical budgets in the past was very low, so efficiency has long been a priority. Second, with the introduction of a market system within the past few years, in which insurers and hospitals bargain amongst themselves to determine the level of payments for clinical activities, payment levels in ophthalmology became more reasonable, so that the financial crisis did not hit ophthalmology particularly hard in comparison with other medical specialties.
This has allowed the Netherlands to avoid having to decrease the number of residency training positions. Further, in contrast to many other European counties, every resident is surgically trained and emerges from residency theoretically able to perform standard ophthalmic surgeries independently.
Research funding, however, has suffered somewhat due to the crisis, according to Willem van den Bosch, MD, PhD, director of the Rotterdam Ophthalmic Institute.
“Lower interest rates have decreased the funds available from both governmental and private sources.”
Besides the reorganisation of care, modern developments will make an impact on the delivery of care.
“Technology will continue to change the face of ophthalmology,” says Mr Sol. “Eye care will be delivered closer and closer to the consumer. Digital screening will continue to increase, and patients will require fewer visits to the hospital. And when patients do come to the hospital, they can expect high-quality care as well as short waiting lists and anxiety reduction measures.”
What the future holds for young ophthalmologists, however, is difficult to predict. Recent developments have suggested that all medical residents might have to help pay for their training. Physicians’ salaries have been sharply reduced in recent years by around 20 per cent across the board, with more cuts likely. Further, working in private practice will likely become more difficult, as the government works to force all physicians into salaried positions. Physicians’ freedom to work as they please has always been vastly more restricted than their counterparts in the United States, and this freedom will likely continue to diminish.
Sharmila Boekhoorn – [email protected] van Etten – [email protected] Sol – [email protected] van den Bosch – [email protected]
cont
acts
by Leigh Spielberg MD
A continuing series looking at how the recession is affecting eye care in EuropeTHE NETHERLANDS FACES CHALLENGES
Update
OCULAR
Rotterdam Eye Hospital
Don’t Miss JCRS Highlights, see page 69
See your success in the eyes of your patients
De� ning the standard of care in RVO*
©2013 Novartis Pharma AG LUC.146879August 2013Lucentis Indications may vary from country to country. Physicians should refer to their National Prescribing Information.Novartis Pharma AG CH-4002 Basel, Switzerland
LUCENTIS® (ranibizumab) ABBREVIATED UK PRESCRIBING INFORMATION Please refer to the SmPC before prescribing LUCENTIS 10mg/ml solution for injection. Presentation: A glass single-use vial containing 0.23ml solution containing 2.3mg of ranibizumab (10mg/ml). Indications: The treatment in adults of neovascular (wet) age-related macular degeneration (AMD), the treatment of visual impairment due to diabetic macular oedema (DMO), the treatment of visual impairment due to macular oedema secondary to retinal vein occlusion (branch RVO or central RVO), and the treatment of visual impairment due to choroidal neovascularisation (CNV) secondary to pathologic myopia (PM). Administration and Dosage: Single-use vial for intravitreal use only. LUCENTIS must be administered by a quali� ed ophthalmologist experienced in intravitreal injections under aseptic conditions. The recommended dose is 0.5 mg (0.05ml). For treatment of wet AMD: Treatment is given monthly and continued until maximum visual acuity is achieved i.e. The patient’s visual acuity is stable for three consecutive monthly assessments performed while on ranibizumab. Thereafter patients should be monitored monthly for visual acuity. Treatment is resumed when monitoring indicates loss of visual acuity due to wet AMD. Monthly injections should then be administered until stable visual acuity is reached again for three consecutive monthly assessments (implying a minimum of two injections). The interval between two doses should not be shorter than 1 month. For treatment of visual impairment due to either DMO or macular oedema secondary to RVO: Treatment is given monthly and continued until maximum visual acuity is achieved i.e. the patient’s visual acuity is stable for three consecutive monthly assessments performed while on ranibizumab treatment. If there is no improvement in visual acuity over the course of the � rst three injections, continued treatment is not recommended. Thereafter patients should be monitored monthly for visual acuity. Treatment is resumed when monitoring indicates loss of visual acuity due to DMO or to macular oedema secondary to RVO. Monthly injections should then be administered until stable visual acuity is reached again for three consecutive monthly assessments (implying a minimum of two injections). The interval between two doses should not be shorter than 1 month. LUCENTIS and laser photocoagulation in DMO and in macular oedema secondary to BRVO: When given on the same day, LUCENTIS should be administered at least 30 minutes after laser photocoagulation. LUCENTIS can be administered in patients who have received previous laser photocoagulation. For treatment of visual impairment due to CNV secondary to PM: Treatment is initiated with a single injection. If monitoring reveals signs of disease activity, e.g. reduced visual acuity and/or signs of lesion activity, further treatment is recommended. Monitoring for disease activity may include clinical examination, optical coherence tomography (OCT) or � uorescein angiography (FA). While many patients may only need one or two injections during the � rst year, some patients may need more frequent treatment. Therefore, monitoring is recommended monthly for the � rst two months and at least every three months thereafter during the � rst year. After the � rst year, the frequency of monitoring should be determined by the treating physician. The interval between two doses should not be shorter than one month. LUCENTIS and Visudyne photodynamic therapy in CNV secondary to PM: There is no experience of concomitant administration of LUCENTIS and Visudyne. Before treatment, evaluate the patient’s medical history for hypersensitivity. The patient should also be instructed to self-administer antimicrobial drops, 4 times daily for 3 days
before and following each injection. Children and adolescents: Not recommended for use in children and adolescents due to a lack of data. Elderly: No dose adjustment is required in the elderly. There is limited experience in patients older than 75 years with DMO Hepatic and renal impairment: Dose adjustment is not needed in these populations. Contraindications: Hypersensitivity to the active substance or excipients. Patients with active or suspected ocular or periocular infections. Patients with active severe intraocular in� ammation. Special warnings and precautions for use: LUCENTIS is for intravitreal injection only. Intravitreal injections have been associated with endophthalmitis, intraocular in� ammation, rhegmatogenous retinal detachment, retinal tear and iatrogenic traumatic cataract. Monitor during week following injection for infections. Patients should be instructed to report symptoms suggestive of any of the above without delay. Transient increases in intraocular pressure (IOP) within 1 hour of injection and sustained IOP increases have been identi� ed. Both IOP and perfusion of the optic nerve head should be monitored and managed appropriately. Concurrent use in both eyes has not been studied and could lead to an increased systemic exposure. There is a potential for immunogenicity with LUCENTIS which may be greater in subjects with DMO. Patients should report an increase in severity of intraocular in� ammation. LUCENTIS should not be administered concurrently with other anti-VEGF agents (systemic or ocular). Withhold dose and do not resume treatment earlier than the next scheduled treatment in the event of the following: a decrease in best corrected visual acuity (BCVA) of ≥30 letters compared with the last assessment of visual acuity; an intraocular pressure of ≥30 mmHg; a retinal break; a subretinal haemorrhage involving the centre of the fovea, or if the size of the haemorrhage is ≥50% of the total lesion area; performed or planned intraocular surgery within the previous or next 28 days. Risk factors associated with the development of a retinal pigment epithelial (RPE) tear after anti-VEGF therapy for wet AMD include a large and/or high pigment epithelial retinal detachment. When initiating LUCENTIS therapy, caution should be used in patients with these risk factors for RPE tears. Discontinue treatment in cases of rhegmatogenous retinal detachment or stage 3 or 4 macular holes. There is only limited experience in the treatment of subjects with DMO due to type I diabetes. LUCENTIS has not been studied in patients who have previously received intravitreal injections, in patients with active systemic infections, proliferative diabetic retinopathy, or in patients with concurrent eye conditions such as retinal detachment or macular hole. There is also no experience of treatment with LUCENTIS in diabetic patients with an HbA1c over 12% and uncontrolled hypertension. In PM patients there are no data on the use of LUCENTIS in patients with extrafoveal lesions and only limited data on its use in those who have had previous unsuccessful therapy with vertepor� n photodynamic therapy. Systemic adverse events including non-ocular haemorrhages and arterial thromboembolic events have been reported following intravitreal injection of VEGF inhibitors. There are limited data on safety in the treatment of DMO, macular oedema due to RVO and CNV secondary to PM patients with prior history of stroke or transient ischaemic attacks. Caution should be exercised when treating such patients. There is limited experience with treatment of patients with prior episodes of RVO and of patients with ischaemic BRVO and CRVO. Treatment is not recommended in RVO patients presenting with clinical signs of irreversible ischaemic visual function loss. Interactions: No formal interaction studies have been performed. In DMO and BRVO adjunctive use of laser therapy and LUCENTIS was not associated with any new ocular or non-ocular safety � ndings. Pregnancy and lactation: Women of
childbearing potential should use e¦ ective contraception during treatment. No clinical data on exposed pregnancies are available. Ranibizumab should not be used during pregnancy unless the expected bene� t outweighs the potential risk to the foetus. For women who wish to become pregnant and have been treated with ranibizumab, it is recommended to wait at least 3 months after the last dose of ranibizumab before conceiving. Breast-feeding is not recommended during the use of LUCENTIS. Driving and using machines: The treatment procedure may induce temporary visual disturbances and patients who experience these signs must not drive or use machines until these disturbances subside. Undesirable e� ects: Most adverse events are related to the injection procedure. Serious adverse events reported include endophthalmitis, blindness, retinal detachment, retinal tear and iatrogenic traumatic cataract. The safety data below include adverse events experienced following the use of LUCENTIS in the entire clinical trial population. Those marked * were only seen in the DMO population. Very Common: Intraocular pressure increased, headache, vitritis, vitreous detachment, retinal haemorrhage, visual disturbance, eye pain, vitreous � oaters, conjunctival haemorrhage, eye irritation, foreign body sensation in eyes, lacrimation increased, blepharitis, dry eye, ocular hyperaemia, eye pruritus, arthralgia, nasopharyngitis. Common: Urinary tract infection*, anaemia, retinal degeneration, retinal disorder, retinal detachment, retinal tear, detachment of the retinal pigment epithelium, retinal pigment epithelium tear, visual acuity reduced, vitreous haemorrhage, vitreous disorder, uveitis, iritis, iridocyclitis, cataract, cataract subcapsular, posterior capsule opaci� cation, punctuate keratitis, corneal abrasion, anterior chamber � are, vision blurred, injection site haemorrhage, eye haemorrhage, conjunctivitis, conjunctivitis allergic, eye discharge, photopsia, photophobia, ocular discomfort, eyelid oedema, eyelid pain, conjunctival hyperaemia, cough, nausea, allergic reactions, hypersensitivity, anxiety. Product-class-related adverse reactions: There is a theoretical risk of arterial thromboembolic events, including stroke and myocardial infarction, following intravitreal use of VEGF inhibitors. A low incidence rate of arterial thromboembolic events was observed in the LUCENTIS clinical trials in patients with AMD, DMO, RVO and PM and there were no major di¦ erences between the groups treated with ranibizumab compared to control. Please refer to the SmPC for full listing of all undesirable e¦ ects.
For UK: Adverse events should be reported. Reporting forms and information can be found at www.mhra.gov.uk/yellowcard. Adverse events should also be reported to Novartis Pharmaceuticals UK Ltd on (01276) 698370 or [email protected]
Legal category: POM, UK Basic NHS cost: £742.17. Marketing authorisation number: EU/1/06/374/001. Marketing authorisation holder: Novartis Europharm Limited, Wimblehurst Road, Horsham, West Sussex, RH12 5AB, United Kingdom. Full prescribing information, including SmPC, is available from: Novartis Pharmaceuticals, Frimley Business Park, Frimley, Camberley, Surrey, GU16 7SR. Telephone: 01276 692255. Fax: 01276 692508. Prepared July 2013.
* Visual impairment due to macular edema secondary to retinal vein occlusion (branch RVO or central RVO)
48198 Eurotimes RVO ad 270x320mm.indd 1 06/08/13 17:26

52
EUROTIMES | Volume 18 | Issue 10
Multifocal IOL implantation appears to provide a safe and viable alternative to monofocal pseudophakia
in selected paediatric cataract patients, according to a recent French study.
Addressing delegates attending the annual meeting of the French Implant and Refractive Surgery Association (SAFIR), Laurence Lesueur MD said that encouraging results had been obtained in a multicentre study of paediatric patients implanted with multifocal implants with up to six years of follow-up.
“The results of the SAFIR 2013 study confirm that hydrophobic multifocal IOLs in selected paediatric cataract patients are a good option if the indications are rigorously respected. The implants offer independence from glasses, limit amblyopia, assist binocular vision, especially in the younger patients, and improve the children’s quality of life without any significant complications to date,” she said.
Dr Lesueur, an ophthalmologist at Centre d’Ophtalmologie Jeanne d’Arc, Toulouse and CHU Toulouse Purpan, France, added, however, that careful monitoring of the IOL positioning is absolutely mandatory in the months and years after implantation.
“We would certainly advise caution in terms of monitoring the stability and centration of the implant over the long term and the patients and their guardians need to be informed of this issue prior to surgery,” she said.
The indications for phaco-refractive surgery are very rare in children, said Dr Lesueur, with all aspects of the surgical process requiring care and attention.
“It is really the huge progress in adult phaco-refractive treatments and technologies in recent years that has enabled us to extend these treatments to selected paediatric cases, with the latest-generation multifocal implants giving us a chance to offer these children spectacle-free vision and an improved quality of life,” she said.
Dr Lesueur noted that the 2013 version of the study is really an updated and enhanced version of the initial trial of 24 eyes of 20 children that had been first presented in 2010, incorporating data from centres in Somain, Bordeaux, Paris, Marseille and Toulouse.
The latest data set presented by Dr Lesueur included 52 eyes of 41 children, with a maximum of six years of follow-up and a mean follow-up of 21 months. Patient ages ranged from nine months to 15 years, with an average of seven years. Of the 41 patients, 30 were treated for unilateral cataracts and 11 were bilateral cases.
Exclusion criteria are very important for paediatric patients, said Dr Lesueur, and need to be scrupulously adhered to.
“We did not operate on any children with corneal anomalies, glaucoma, microphthalmia, pupillary deformation, retinopathies, neuro-ophthalmic anomalies or ocular inflammation,” she said.
In terms of surgical technique, 36 patients underwent straightforward phacoemulsification and multifocal IOL insertion, while 16 patients under the age of five had combined phacoemulsification, posterior capsulorhexis and anterior vitrectomy procedures.
A variety of multifocal IOLs including the AcrySof ReSTOR, AcrySof ReSTOR Toric, Tecnis ZM, Tecnis ZMT, NXG1, Acri.Lisa, and Acri.Lisa Toric were implanted through a 2.2mm to 3.2mm corneal incision.
Dr Lesueur said that the refractive results for the 41 eyes of 33 children with more than one year of follow-up were very good overall, with impressive outcomes for both uncorrected and corrected near and distance visual acuity specially in cases of unilateral cataract operated on after the age of six years.
ShareLearn
Connect.
Join Us On Social Media
• Be sure to check out our social networking sitesand like or follow us to join the conversation
• Get real time access to the latest congress updates,society news and event information
• Our social media sites are a great way tocommunicate and share your congress experiences, connect with members of our team and others inthe ophthalmic community
www.facebook.com/ESCRSwww.facebook.com/eurotimesnews
@ESCRSoffi cial@eurotimestweets
www.linkedin.com/company/eurotimeswww.linkedin.com/company/escrs
Interact with the ESCRS
www.escrs.org www.eurotimes.org
Laurence Lesueur – [email protected]
contact
by Dermot McGrath in Paris
Implants offer independence from glasses, limit amblyopia
MULTIFOCAL IOLS
Update
PAEDIATRIC OPHTHALMOLOGY
The indications for phaco-refractive surgery are very rare in children with all aspects of the surgical process requiring care and attention
“
Laurence Lesueur MD

EUROTIMES | Volume 18 | Issue 10
53
What is the real cataract crisis in 2013? Irregular capsulotomies? Endophthalmitis?
Astigmatism management? Presbyopia?“I don’t think it is any of the above,”
Mark Cherny MD, Melbourne, Australia, told the 2013 American Society of Cataract and Refractive Surgery symposium. The real crisis is 20 million people worldwide blind from cataracts and another 50 million visually impaired, he said.
The cost goes beyond the suffering of those directly afflicted to loss of income, productivity and even educational opportunity for families and communities, Dr Cherny noted. “Many children are taken out of school to care for parents and grandparents who are blind.”
As the ophthalmologists and the eye care industry embrace expensive femtosecond laser technology for cataract surgery, where is global cataract blindness on the agenda? Dr Cherny asked. And what can be done to address the true cataract crisis?
Dr Cherny is hardly a Luddite. An early adopter of femtosecond laser-assisted cataract surgery, he installed a Catalys
system (Optimedica) in July 2012. He now uses it for all his cataract cases.
Cost of technology However, with nearly 1,000 laser-assisted surgeries under his belt, Dr Cherny is also aware that femtosecond technology adds $600 to $1,000 beyond the cost of a conventional phacoemulsification procedure. According to his analysis, the added cost of one femtosecond laser-assisted procedure could fund somewhere between six and 50 entire small incision extracapsular cataract extractions in the developing world.
So if femtosecond technology prevents one in 50 patients from a 20/200 outcome – which assumes a failure rate much higher than typical in the developed world – the $30,000 to $50,000 cost could cure blindness in 300 to 2,500 patients receiving small incision procedures. Assuming femtosecond technology “saves” only one in 200 patients from blindness the trade-off is even starker, with as many as 10,000 small incision surgeries potentially done for the same investment.
Surgical perfection “To go from a very good platform, conventional phaco, we have to spend a lot of money to take the next step towards surgical perfection,” Dr Cherny noted. Whether the cost is justified in the face of so much untreated blindness, or if the technology will ultimately benefit developing countries, are questions for which he has no easy answer.
What can be done is to get personally involved, Dr Cherny said.
“I reviewed my own response to global blindness and am embarrassed to say I had done nothing.”
Connecting projects So Dr Cherny set up a web site, SharingVision.org, to help others connect to projects in the developing world. He’s gotten a commitment from Optimedica to donate, and he’s talking to other manufacturers.
Donating a small amount for each procedure he does is another way to help.
Patient awareness Literature in the waiting area helps
increase patient awareness, as do online and social media, Dr Cherny said.
“Many of us have web sites. How many of us have a link to a global aid organisation?”
Dr Cherny sees solving global blindness as a central mission of ophthalmology.
“There are a lot of people who get locked into a little room with a slit lamp and a lot of local patients to treat, and we don’t have the international issue on the agenda. We should all make the global blindness crisis a priority and support and encourage those who are doing something about it.”
by Howard Larkin in San Francisco
With 20 million cataract blind worldwide, cost raises ethical questionsFIGHTING GLOBAL BLINDNESS
Update
GLOBAL OPHTHALMOLOGY
Mark Cherny – [email protected]
cont
act
“We should all make the global blindness crisis a priority and support and encourage those who are doing something about it”
EUROTIMESESC
RS ™
Türkiye
TURKISH LANGUAGE EDITIONNOW ONLINE
Visit: www.eurotimesturkey.org

Dr. Ozana Moraru,Romania
Dr. Gabor Schairoth, Germany
Prof. Dr. Rudy Nuijts, The Netherlands
Host surgeon
surgical Faculty
Dr. Robert Cionni, USA
Preceding the live surgery event!you’re invited to exPerience tHe centurion® vision system
Please join us to celebrate the introduction of the Centurion® Vision System
Introduction: 17:45 – Onyx and Auditorium LoungeJust preceding the Live Surgery telecast!
Celebration:Immediately after the Live Surgery telecast!
Alcon in amsterdam4-9 october 2013
The CaTaraCT refraCTIve SuITe by alCon®The future of cataract surgery is here. Come experience the world premiere of exciting new surgical technologies from global eye care leader, Alcon. Please visit the Alcon Booth #E03.
© 2013 Novartis 9/13 MIX13443JADi
register now! http://escrs.org/alconsatellites
Friday, 4 octoberGlaucoma filtration Surgery: limiting variables and Improving outcomesLevel 1 – G106/107 – RAI Congress Centre.
12:45 – 13:45 (lunch boxes will be provided)Co-Moderators: Dr. Keith Barton, UK Dr. Tarek Shaarawy, Switzerland
Speakers: Dr. Marco Nardi, Italy Dr. Tom Samuelson, USA Dr. Ingeborg Stalmans, Belgium Dr. Carlo Traverso, Italy
Glaucoma Day Symposium! This symposium will focus on the latest efficacy and safety data of the EX-PRESS® Glaucoma Filtration Device, benefits of lumenal control, and advanced pearls and techniques for optimizing your glaucoma filtering surgery procedures.
sunday, 6 octoberadvancements in the Diagnosis and Treatment of Dry eyeElicium 1 – RAI Congress Centre
13:00 – 14:00 (lunch boxes will be provided)Faculty: Dr. James P McCulley, USA Dr. Koray Gumus, Turkey Dr. Eric Donnenfeld, USA
Join experts in the field as they discuss the differential diagnosis, treatment and therapeutic options in the Management of Dry Eye.
sunday, 6 octoberInitial experience with the new alcon Centurion® vision SystemElicium 2 – RAI Congress Centre
13:00 – 14:00 (lunch boxes will be provided)Faculty: Mr. David Allen, UK Dr. Christer Johansson, Sweden Mr. Richard Packard, UK Dr. Khiun Tjia, The Netherlands
Surgeons will share observations, pearls and future possibilities using the new Alcon Centurion® Vision System. Discussion will cover Active Fluidics Technology, Balanced Energy Technology and Applied Integration Technology available with this new system.
sunday, 6 octoberInnovations in Cataract and refractive SurgeryBuers Van Berlage (transportation provided from RAI. Buses depart at 18:00)
19:00 – 20:00 (refreshments will be provided)Moderator: Dr. Rudy Nuijts, The Netherlands
Faculty: Dr. Robert Cionni, USA Dr. Philippe Crozafon, France Dr. Arthur Cummings, Ireland Dr. Theo Seiler, Switzerland
Introducing the Cataract Refractive Suite by Alcon®, a wave of innovation featuring: VERION™ Image Guided System, LenSx® Laser System, LuxOR™ LX3 Ophthalmic Microscope and the new Centurion® Vision System. Come and learn from top industry opinion leaders’ experiences with the CATARACT REFRACTIVE SUITE by Alcon and see the latest advancements in the WaveLight® Refractive Suite.
monday, 7 octoberalcon visionarium – Cataract & refractive Innovations in a 3D video SymposiumThe Forum – RAI Congress Centre
13:00 – 14:00 (lunch boxes will be provided)Faculty: Dr. Phillipe Crozafon, France Prof. Dr. Michael Knorz, Germany Prof. Dr. John Kanellopoulos, Greece Dr. Khiun Tjia, The Netherlands
Join our leading cataract & refractive surgeons in a unique 3D Symposium showcasing Alcon’s newest advanced technologies: the new Centurion® Vision System, VERION™ Image Guided System, LenSx® Laser System, LuxOR™ LX3 Ophthalmic Microscope & WaveLight® Refractive Suite.
These events are for healthcare professionals only. Please present your ESCRS meeting badge for entry into the meeting. For important safety information about the Alcon products discussed in these
programs, please visit the Alcon booth #E03 at ESCRS.
saturday, 5 octoberlive surgery: advancements in techniques and technologies telecast in High definition!The Auditorium – RAI Congress Centre
18:00 – 20:30 (refreshments will be provided)Register now to learn from world-acclaimed surgeons demonstrating their techniques using the latest Alcon® technologies in cataract surgery. Featured technologies will include:• The innovative CENTURION® Vision System, beginning a new era of
cataract removal • VERION™ Image Guided System• LenSx® Laser System• INTREPID® AutoSert® IOL Injector• AcrySof® IQ ReSTOR® family of Multifocal and Multifocal Toric IOLs
Prof. Dr. Michael Knorz, Germany
Dr. Marc Weiser, France
Dr. Robert H. Osher, USA
Dr. Donald N. Serafano, USA
moderator
Dr. Robert Kaufer, Argentina
Faculty Panel
Mr. David Allen, United Kingdom

Dr. Ozana Moraru,Romania
Dr. Gabor Schairoth, Germany
Prof. Dr. Rudy Nuijts, The Netherlands
Host surgeon
surgical Faculty
Dr. Robert Cionni, USA
Preceding the live surgery event!you’re invited to exPerience tHe centurion® vision system
Please join us to celebrate the introduction of the Centurion® Vision System
Introduction: 17:45 – Onyx and Auditorium LoungeJust preceding the Live Surgery telecast!
Celebration:Immediately after the Live Surgery telecast!
Alcon in amsterdam4-9 october 2013
The CaTaraCT refraCTIve SuITe by alCon®The future of cataract surgery is here. Come experience the world premiere of exciting new surgical technologies from global eye care leader, Alcon. Please visit the Alcon Booth #E03.
© 2013 Novartis 9/13 MIX13443JADi
register now! http://escrs.org/alconsatellites
Friday, 4 octoberGlaucoma filtration Surgery: limiting variables and Improving outcomesLevel 1 – G106/107 – RAI Congress Centre.
12:45 – 13:45 (lunch boxes will be provided)Co-Moderators: Dr. Keith Barton, UK Dr. Tarek Shaarawy, Switzerland
Speakers: Dr. Marco Nardi, Italy Dr. Tom Samuelson, USA Dr. Ingeborg Stalmans, Belgium Dr. Carlo Traverso, Italy
Glaucoma Day Symposium! This symposium will focus on the latest efficacy and safety data of the EX-PRESS® Glaucoma Filtration Device, benefits of lumenal control, and advanced pearls and techniques for optimizing your glaucoma filtering surgery procedures.
sunday, 6 octoberadvancements in the Diagnosis and Treatment of Dry eyeElicium 1 – RAI Congress Centre
13:00 – 14:00 (lunch boxes will be provided)Faculty: Dr. James P McCulley, USA Dr. Koray Gumus, Turkey Dr. Eric Donnenfeld, USA
Join experts in the field as they discuss the differential diagnosis, treatment and therapeutic options in the Management of Dry Eye.
sunday, 6 octoberInitial experience with the new alcon Centurion® vision SystemElicium 2 – RAI Congress Centre
13:00 – 14:00 (lunch boxes will be provided)Faculty: Mr. David Allen, UK Dr. Christer Johansson, Sweden Mr. Richard Packard, UK Dr. Khiun Tjia, The Netherlands
Surgeons will share observations, pearls and future possibilities using the new Alcon Centurion® Vision System. Discussion will cover Active Fluidics Technology, Balanced Energy Technology and Applied Integration Technology available with this new system.
sunday, 6 octoberInnovations in Cataract and refractive SurgeryBuers Van Berlage (transportation provided from RAI. Buses depart at 18:00)
19:00 – 20:00 (refreshments will be provided)Moderator: Dr. Rudy Nuijts, The Netherlands
Faculty: Dr. Robert Cionni, USA Dr. Philippe Crozafon, France Dr. Arthur Cummings, Ireland Dr. Theo Seiler, Switzerland
Introducing the Cataract Refractive Suite by Alcon®, a wave of innovation featuring: VERION™ Image Guided System, LenSx® Laser System, LuxOR™ LX3 Ophthalmic Microscope and the new Centurion® Vision System. Come and learn from top industry opinion leaders’ experiences with the CATARACT REFRACTIVE SUITE by Alcon and see the latest advancements in the WaveLight® Refractive Suite.
monday, 7 octoberalcon visionarium – Cataract & refractive Innovations in a 3D video SymposiumThe Forum – RAI Congress Centre
13:00 – 14:00 (lunch boxes will be provided)Faculty: Dr. Phillipe Crozafon, France Prof. Dr. Michael Knorz, Germany Prof. Dr. John Kanellopoulos, Greece Dr. Khiun Tjia, The Netherlands
Join our leading cataract & refractive surgeons in a unique 3D Symposium showcasing Alcon’s newest advanced technologies: the new Centurion® Vision System, VERION™ Image Guided System, LenSx® Laser System, LuxOR™ LX3 Ophthalmic Microscope & WaveLight® Refractive Suite.
These events are for healthcare professionals only. Please present your ESCRS meeting badge for entry into the meeting. For important safety information about the Alcon products discussed in these
programs, please visit the Alcon booth #E03 at ESCRS.
saturday, 5 octoberlive surgery: advancements in techniques and technologies telecast in High definition!The Auditorium – RAI Congress Centre
18:00 – 20:30 (refreshments will be provided)Register now to learn from world-acclaimed surgeons demonstrating their techniques using the latest Alcon® technologies in cataract surgery. Featured technologies will include:• The innovative CENTURION® Vision System, beginning a new era of
cataract removal • VERION™ Image Guided System• LenSx® Laser System• INTREPID® AutoSert® IOL Injector• AcrySof® IQ ReSTOR® family of Multifocal and Multifocal Toric IOLs
Prof. Dr. Michael Knorz, Germany
Dr. Marc Weiser, France
Dr. Robert H. Osher, USA
Dr. Donald N. Serafano, USA
moderator
Dr. Robert Kaufer, Argentina
Faculty Panel
Mr. David Allen, United Kingdom
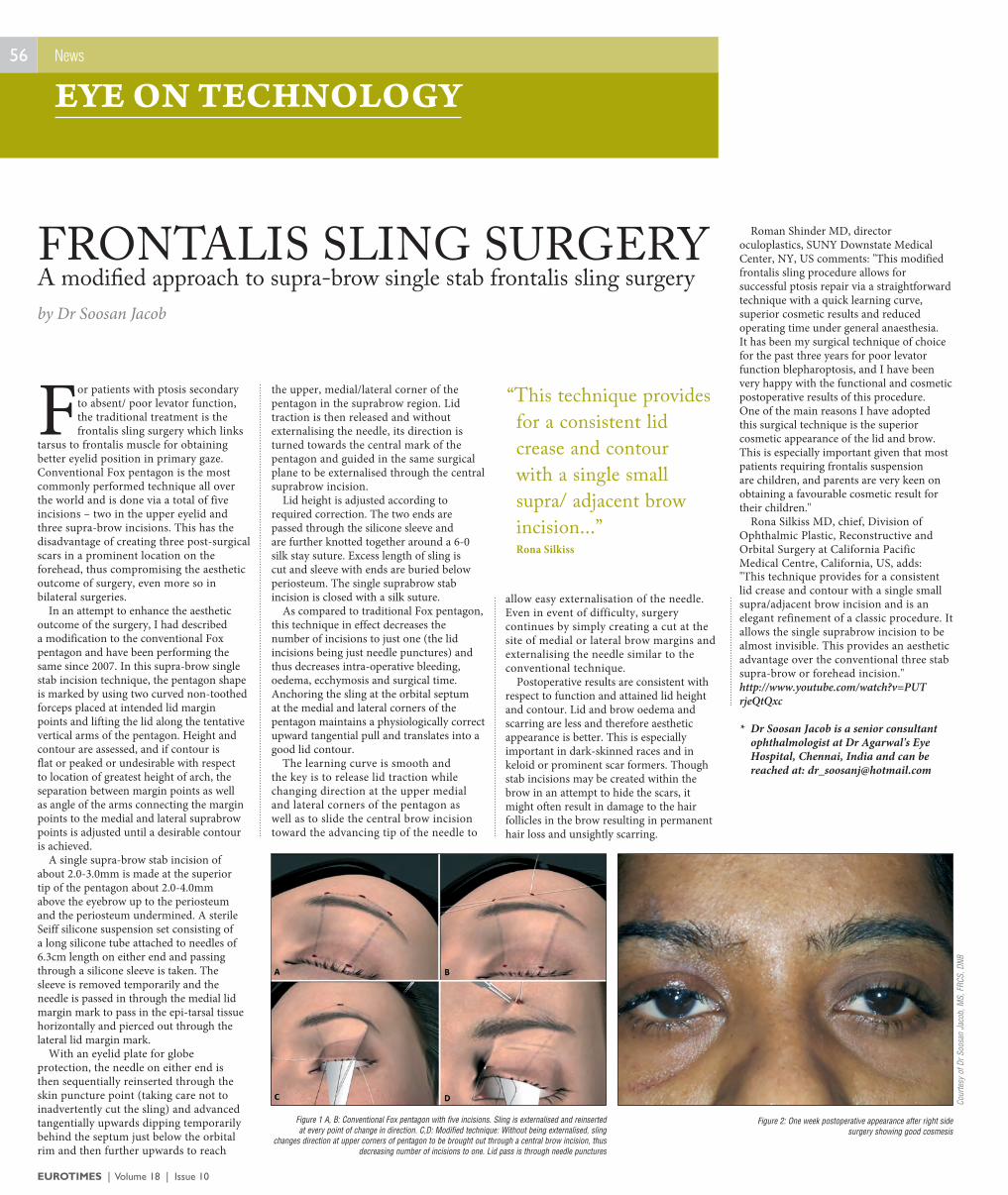
EUROTIMES | Volume 18 | Issue 10
56
For patients with ptosis secondary to absent/ poor levator function, the traditional treatment is the frontalis sling surgery which links
tarsus to frontalis muscle for obtaining better eyelid position in primary gaze. Conventional Fox pentagon is the most commonly performed technique all over the world and is done via a total of five incisions – two in the upper eyelid and three supra-brow incisions. This has the disadvantage of creating three post-surgical scars in a prominent location on the forehead, thus compromising the aesthetic outcome of surgery, even more so in bilateral surgeries.
In an attempt to enhance the aesthetic outcome of the surgery, I had described a modification to the conventional Fox pentagon and have been performing the same since 2007. In this supra-brow single stab incision technique, the pentagon shape is marked by using two curved non-toothed forceps placed at intended lid margin points and lifting the lid along the tentative vertical arms of the pentagon. Height and contour are assessed, and if contour is flat or peaked or undesirable with respect to location of greatest height of arch, the separation between margin points as well as angle of the arms connecting the margin points to the medial and lateral suprabrow points is adjusted until a desirable contour is achieved.
A single supra-brow stab incision of about 2.0-3.0mm is made at the superior tip of the pentagon about 2.0-4.0mm above the eyebrow up to the periosteum and the periosteum undermined. A sterile Seiff silicone suspension set consisting of a long silicone tube attached to needles of 6.3cm length on either end and passing through a silicone sleeve is taken. The sleeve is removed temporarily and the needle is passed in through the medial lid margin mark to pass in the epi-tarsal tissue horizontally and pierced out through the lateral lid margin mark.
With an eyelid plate for globe protection, the needle on either end is then sequentially reinserted through the skin puncture point (taking care not to inadvertently cut the sling) and advanced tangentially upwards dipping temporarily behind the septum just below the orbital rim and then further upwards to reach
the upper, medial/lateral corner of the pentagon in the suprabrow region. Lid traction is then released and without externalising the needle, its direction is turned towards the central mark of the pentagon and guided in the same surgical plane to be externalised through the central suprabrow incision.
Lid height is adjusted according to required correction. The two ends are passed through the silicone sleeve and are further knotted together around a 6-0 silk stay suture. Excess length of sling is cut and sleeve with ends are buried below periosteum. The single suprabrow stab incision is closed with a silk suture.
As compared to traditional Fox pentagon, this technique in effect decreases the number of incisions to just one (the lid incisions being just needle punctures) and thus decreases intra-operative bleeding, oedema, ecchymosis and surgical time. Anchoring the sling at the orbital septum at the medial and lateral corners of the pentagon maintains a physiologically correct upward tangential pull and translates into a good lid contour.
The learning curve is smooth and the key is to release lid traction while changing direction at the upper medial and lateral corners of the pentagon as well as to slide the central brow incision toward the advancing tip of the needle to
allow easy externalisation of the needle. Even in event of difficulty, surgery continues by simply creating a cut at the site of medial or lateral brow margins and externalising the needle similar to the conventional technique.
Postoperative results are consistent with respect to function and attained lid height and contour. Lid and brow oedema and scarring are less and therefore aesthetic appearance is better. This is especially important in dark-skinned races and in keloid or prominent scar formers. Though stab incisions may be created within the brow in an attempt to hide the scars, it might often result in damage to the hair follicles in the brow resulting in permanent hair loss and unsightly scarring.
Roman Shinder MD, director oculoplastics, SUNY Downstate Medical Center, NY, US comments: "This modified frontalis sling procedure allows for successful ptosis repair via a straightforward technique with a quick learning curve, superior cosmetic results and reduced operating time under general anaesthesia. It has been my surgical technique of choice for the past three years for poor levator function blepharoptosis, and I have been very happy with the functional and cosmetic postoperative results of this procedure. One of the main reasons I have adopted this surgical technique is the superior cosmetic appearance of the lid and brow. This is especially important given that most patients requiring frontalis suspension are children, and parents are very keen on obtaining a favourable cosmetic result for their children."
Rona Silkiss MD, chief, Division of Ophthalmic Plastic, Reconstructive and Orbital Surgery at California Pacific Medical Centre, California, US, adds: "This technique provides for a consistent lid crease and contour with a single small supra/adjacent brow incision and is an elegant refinement of a classic procedure. It allows the single suprabrow incision to be almost invisible. This provides an aesthetic advantage over the conventional three stab supra-brow or forehead incision."http://www.youtube.com/watch?v=PUT rjeQtQxc
* Dr Soosan Jacob is a senior consultant ophthalmologist at Dr Agarwal's Eye Hospital, Chennai, India and can be reached at: [email protected]
A modified approach to supra-brow single stab frontalis sling surgeryby Dr Soosan Jacob
FRONTALIS SLING SURGERY
News
EYE ON TECHNOLOGY
Figure 1 A, B: Conventional Fox pentagon with five incisions. Sling is externalised and reinserted at every point of change in direction. C,D: Modified technique: Without being externalised, sling
changes direction at upper corners of pentagon to be brought out through a central brow incision, thus decreasing number of incisions to one. Lid pass is through needle punctures
Figure 2: One week postoperative appearance after right side surgery showing good cosmesis
“This technique provides for a consistent lid crease and contour with a single small supra/ adjacent brow incision...”
Rona Silkiss
Cour
tesy
of D
r Soo
san
Jaco
b, M
S, F
RCS,
DNB

57
EUROTIMES | Volume 18 | Issue 10
After several years of rigorous preparation, the PREvention of Macular EDema after cataract surgery (PREMED) study has
now enrolled its first patients. The ESCRS PREMED study is a European multicentre, randomised trial that could help to transform the current clinical management of cystoid macular edema (CME) after cataract surgery.
Funded by a substantial grant from the ESCRS, the PREMED study is an initiative of the University Eye Clinic Maastricht, the Netherlands, under the supervision of Rudy Nuijts MD, PhD.
“We are pleased that the first patients have now been recruited for this important trial which should prove of immense benefit to all ESCRS members and cataract surgeons,” said Dr Nuijts. “Thanks to the support of the ESCRS, we will hopefully be able to provide more definite evidence-based recommendations for clinical guidelines to prevent the occurrence of CME after cataract surgery in patients with and without diabetes mellitus. Lowering the number of drugs used during postoperative treatment after phacoemulsification may increase cost effectiveness and lower potential side effects,” he added.
The PREMED study aims to enrol a total of 1,350 patients, 300 with diabetes mellitus and 1,050 without, who require cataract surgery in at least one eye. The inclusion period is scheduled to last for 18 months with 12 different centres in Europe and Russia taking part.
The overall aim of the study is to answer some critical questions relating to the prevention of cystoid macular edema after cataract surgery, explained Laura Wielders MD, a researcher who is part of the PREMED study coordinating investigators group.
“In the past few years, several new treatments have been tried to address the problem of CME after cataract surgery in diabetic and non-diabetic patients. However, no well-designed randomised controlled clinical trial has compared all the currently existing preventive strategies. This lack of well-designed trials and the large variety of treatments used in clinical practice was our major reason for starting the PREMED study,” she said.
The study protocol has now been finalised, said Laura Wielders, with all
patients undergoing phacoemulsification for cataract removal and placement of a posterior chamber intraocular lens. In the non-diabetic population, patients will receive either bromfenac 0.09 per cent eye drops twice daily starting two days before surgery and continuing two weeks postoperatively; dexamethasone disodium phosphate 0.1 per cent eye drops four times daily starting two days before surgery and continuing four times daily during the first postoperative week and one drop less per day every following week, or a combination of both drugs. These strategies will be compared for their efficacy in preventing central subfield mean macular thickening.
Four Treatment Groups In the diabetic population, patients will be randomised into four treatment groups: (1) topical bromfenac 0.09 per cent and dexamethasone disodium phosphate 0.1 per cent; (2) topical bromfenac and dexamethasone and a subconjunctival injection of 40mg preservative-free triamcinolone acetonide (TA); (3) topical bromfenac and dexamethasone and an intravitreal injection of 1.25mg bevacizumab; (4) topical bromfenac and dexamethasone, a subconjunctival injection of 40mg preservative-free TA and an intravitreal injection of 1.25mg bevacizumab.
The primary endpoint of the study is the change in central subfield mean macular thickness (CSMT) as compared to baseline at six weeks postoperatively. The secondary endpoint is the occurrence of clinically significant macular edema (CSME) within 12 weeks postoperatively.
In case of CSME, treatment will be initiated and its effect will be part of the evaluation at 12 weeks. Medical data of all patients who develop CSME during the study will be checked at the end of the study and at least six months after surgery.
At the end of the study, the hope is that clinicians will have a much clearer picture as to the optimum postoperative treatment regimen for cataract patients with and without diabetes mellitus.
OASIS name and logo are registered trademarks of OASIS Medical, Inc.514 S. Vermont Ave, Glendora, CA 91741.
800-528-9786 (USA Toll Free) 909-305-5400
[email protected] www.oasismedical.com
Find out more about how we can help your practice. Contact OASIS® for a surgical demonstration.
Oasis is dedicated to equipping eye care providers with cost effective solutions to ensure quality patient care,
improve practice management, and support practice growth.
More than expected
Patent No. 8,439,833 B2
The Oasis Iris Expander®
is a single-use 7.0mm or
6.25mm polypropylene
ring provided in sterile
condition and packaged
five units per box.
SUSTAIN YOUR ACCESS.
Unimpeded view during complicated small pupil surgeries
Four pockets gently cradle the ocular tissue without pinching or clamping
Once removed, iris returns to its normal shape and function
Also used to manage Floppy Iris Syndrome (IFIS)
Easy removal without potential tearing
THE OASIS IRIS EXPANDER®
EXPAND YOUR VIEW.
Visit us at ESCRS Booth #J24
by Dermot McGrath
European multicentre trial could transform understanding of CME after cataract surgery
PREMED STUDY
News
RESEARCH
Rudy Nuijts – [email protected]
contact

58
EUROTIMES | Volume 18 | Issue 1008_1309_15 ESASO_Anz_EUT_120x300_RZ.indd 1 02.09.13 12:33
The International AMD and Retina Congress plays a pivotal role in establishing the standards of ophthalmology training and
practice. The 2013 meeting, which takes place in Dublin, Ireland on October 25 and 26, will offer another platform for over 1,000 specialised ophthalmologists from 44 countries to come together and learn from each other in the fields of medical and surgical retina.
In light of the increasing therapeutic options for treating retinal diseases such as age-related macular degeneration (AMD), diabetic macular edema (DME), retinal vascular occlusion (RVO) and disorders of the vitreomacular interface, the programme will examine the appropriate use of available therapies in the context of evidence from clinical trials and long-term clinical experience.
“The meeting will provide an educational forum for ophthalmologists to discuss the management of retinal diseases with a view to maximising outcomes for patients,” says Francesco Bandello, chairman of the Scientific Committee.
Innovative approaches In addition, innovative approaches to the management of patients with vision impairment, including the use of stem cells and retinal transplantation as well as gene therapy and artificial vision, will be discussed. Delegates will participate in sessions on diabetic retinopathy and on retinal vascular occlusion. The sessions will start with brief introductions of clinical cases on the state-of-the-art treatment and then leading experts will discuss these cases with the audience. There are sessions planned where the problems of the long-term treatment of wet AMD is faced and the three anti-VEGFs in use will be compared.
Spread over two days, the scientific programme includes several sessions, master classes, debates and posters. Master classes will provide delegates with the opportunity to obtain in-depth tuition on practical aspects of OCT and other imaging modalities, in addition to the use of sub-threshold laser. The emphasis will be on education through sharing of practical experience and expertise. “Expect the 13th international AMD and Retina Congress to be even more interactive and instructive,” said Prof Bandello.
New ideas During the meeting of the Scientific Committee in Budapest in April, new ideas and activities were discussed which will be implemented during the upcoming meeting. For the first time, the congress will include selected experiences of specialised ophthalmologists within the main plenary sessions. These case studies will serve to share invaluable insights from the clinic with the ESASO audience, and will form part of the discussions during Session 4 of the main programme. Thus, critical discussions on comparative clinical cases will fire up the debates with the final aim to learn how to best use medications.
Needless to say, each congress stands and falls with its scientific programme. Still, it is important to mention that ESASO will be proud to welcome its delegates at the wonderful, friendly and warm Irish capital where they will not only discuss latest state-of-the-art technology, medicine and improvements, but where people from all over the world will gather to meet friends and enjoy a memorable Gathering.
ESASO looks forward to welcoming you in Dublin!
International AMD and Retina Congress convenes in Dublin, Ireland on October 25-26
ESASO GATHERING
News
ESASO
ESCRS
FREE
3 YEAR
MEMBERSHIP
FOR TRAINEES
ESCR
S M
EMBE
RSH
IP
NO
W IN
CLU
DES
ACC
ESS
TO
A
ND
ESCRS
ET double page.indd 1 14/02/2012 16:04:35
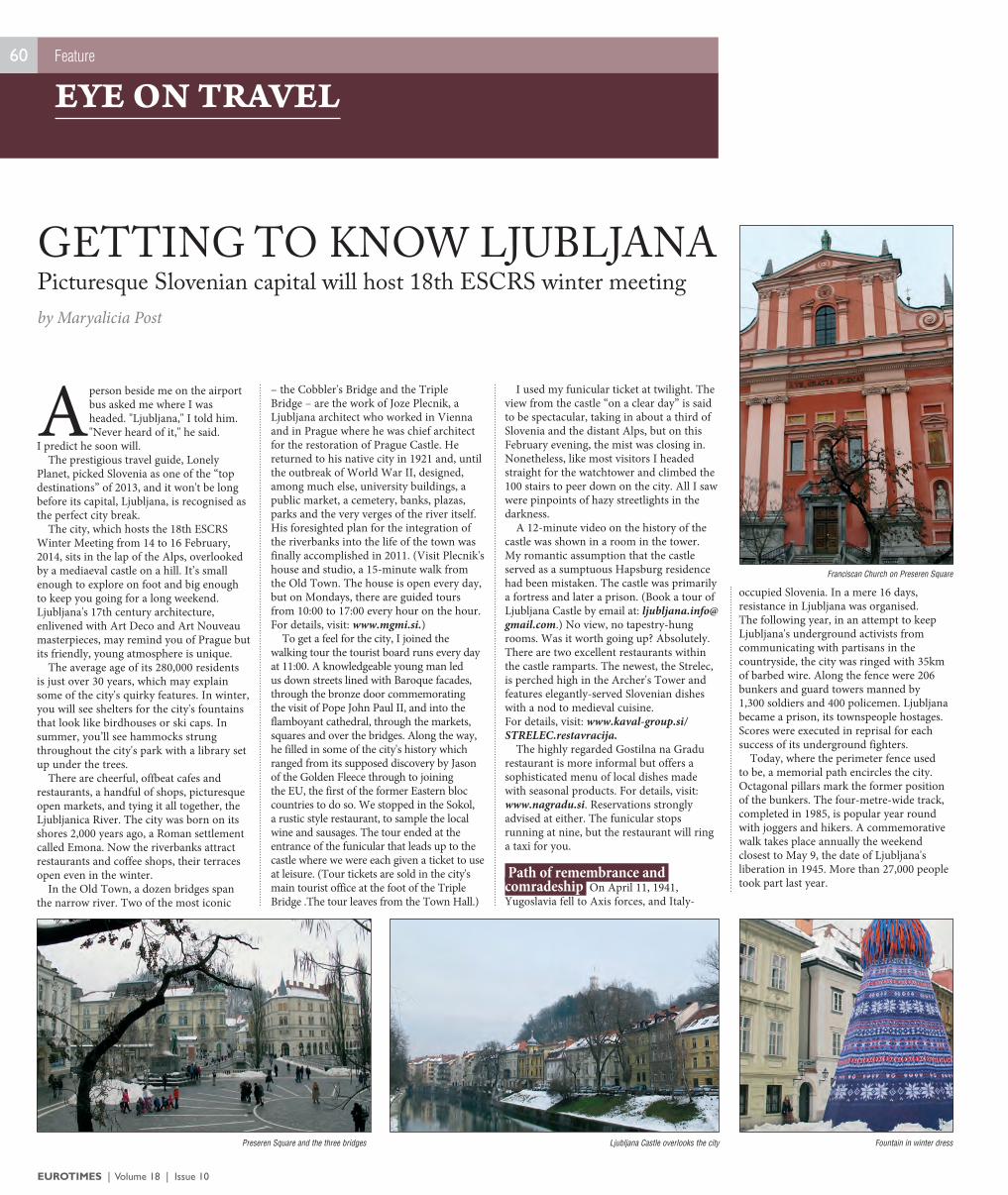
EUROTIMES | Volume 18 | Issue 10
60
A person beside me on the airport bus asked me where I was headed. "Ljubljana," I told him. "Never heard of it," he said.
I predict he soon will. The prestigious travel guide, Lonely
Planet, picked Slovenia as one of the “top destinations” of 2013, and it won't be long before its capital, Ljubljana, is recognised as the perfect city break.
The city, which hosts the 18th ESCRS Winter Meeting from 14 to 16 February, 2014, sits in the lap of the Alps, overlooked by a mediaeval castle on a hill. It’s small enough to explore on foot and big enough to keep you going for a long weekend. Ljubljana's 17th century architecture, enlivened with Art Deco and Art Nouveau masterpieces, may remind you of Prague but its friendly, young atmosphere is unique.
The average age of its 280,000 residents is just over 30 years, which may explain some of the city's quirky features. In winter, you will see shelters for the city's fountains that look like birdhouses or ski caps. In summer, you’ll see hammocks strung throughout the city's park with a library set up under the trees.
There are cheerful, offbeat cafes and restaurants, a handful of shops, picturesque open markets, and tying it all together, the Ljubljanica River. The city was born on its shores 2,000 years ago, a Roman settlement called Emona. Now the riverbanks attract restaurants and coffee shops, their terraces open even in the winter.
In the Old Town, a dozen bridges span the narrow river. Two of the most iconic
– the Cobbler's Bridge and the Triple Bridge – are the work of Joze Plecnik, a Ljubljana architect who worked in Vienna and in Prague where he was chief architect for the restoration of Prague Castle. He returned to his native city in 1921 and, until the outbreak of World War II, designed, among much else, university buildings, a public market, a cemetery, banks, plazas, parks and the very verges of the river itself. His foresighted plan for the integration of the riverbanks into the life of the town was finally accomplished in 2011. (Visit Plecnik's house and studio, a 15-minute walk from the Old Town. The house is open every day, but on Mondays, there are guided tours from 10:00 to 17:00 every hour on the hour. For details, visit: www.mgmi.si.)
To get a feel for the city, I joined the walking tour the tourist board runs every day at 11:00. A knowledgeable young man led us down streets lined with Baroque facades, through the bronze door commemorating the visit of Pope John Paul II, and into the flamboyant cathedral, through the markets, squares and over the bridges. Along the way, he filled in some of the city's history which ranged from its supposed discovery by Jason of the Golden Fleece through to joining the EU, the first of the former Eastern bloc countries to do so. We stopped in the Sokol, a rustic style restaurant, to sample the local wine and sausages. The tour ended at the entrance of the funicular that leads up to the castle where we were each given a ticket to use at leisure. (Tour tickets are sold in the city's main tourist office at the foot of the Triple Bridge .The tour leaves from the Town Hall.)
I used my funicular ticket at twilight. The view from the castle “on a clear day” is said to be spectacular, taking in about a third of Slovenia and the distant Alps, but on this February evening, the mist was closing in. Nonetheless, like most visitors I headed straight for the watchtower and climbed the 100 stairs to peer down on the city. All I saw were pinpoints of hazy streetlights in the darkness.
A 12-minute video on the history of the castle was shown in a room in the tower. My romantic assumption that the castle served as a sumptuous Hapsburg residence had been mistaken. The castle was primarily a fortress and later a prison. (Book a tour of Ljubljana Castle by email at: [email protected].) No view, no tapestry-hung rooms. Was it worth going up? Absolutely. There are two excellent restaurants within the castle ramparts. The newest, the Strelec, is perched high in the Archer's Tower and features elegantly-served Slovenian dishes with a nod to medieval cuisine. For details, visit: www.kaval-group.si/STRELEC.restavracija.
The highly regarded Gostilna na Gradu restaurant is more informal but offers a sophisticated menu of local dishes made with seasonal products. For details, visit: www.nagradu.si. Reservations strongly advised at either. The funicular stops running at nine, but the restaurant will ring a taxi for you.
Path of remembrance and comradeship On April 11, 1941, Yugoslavia fell to Axis forces, and Italy-
occupied Slovenia. In a mere 16 days, resistance in Ljubljana was organised. The following year, in an attempt to keep Ljubljana's underground activists from communicating with partisans in the countryside, the city was ringed with 35km of barbed wire. Along the fence were 206 bunkers and guard towers manned by 1,300 soldiers and 400 policemen. Ljubljana became a prison, its townspeople hostages. Scores were executed in reprisal for each success of its underground fighters.
Today, where the perimeter fence used to be, a memorial path encircles the city. Octagonal pillars mark the former position of the bunkers. The four-metre-wide track, completed in 1985, is popular year round with joggers and hikers. A commemorative walk takes place annually the weekend closest to May 9, the date of Ljubljana's liberation in 1945. More than 27,000 people took part last year.
by Maryalicia Post
Picturesque Slovenian capital will host 18th ESCRS winter meetingGETTING TO KNOW LJUBLJANA
Feature
EYE ON TRAVEL
Franciscan Church on Preseren Square
Fountain in winter dressLjubljana Castle overlooks the cityPreseren Square and the three bridges
ESCRSWinter Meeting
In conjunction with the Slovenian Society of Cataract & Refractive Surgery
Ljubljana, Slovenia14-16 February 2014
EuropEan SociEty of cataract & rEfractivE SurgEonS
th18Preliminary Programme Available
www.escrs.org
Abstract Submission Deadline:
31 October 2013

EUROTIMES | Volume 18 | Issue 10
62
“I keep tripping and falling over my children, so now they know not to run right in front of me,” a young mother of three told me
in the retinal genetics clinic. “I just don’t see them until it’s too late.”
That’s it, I thought! Finally, I’ve found a clear indication that someone had real visual field loss. Only someone with a serious constriction of their visual field would ever fall over their own children.
Before I developed my retinal observation skills enough to make sense of my funduscopic examination, I relied heavily on my history-taking to come to a useful differential diagnosis. I hadn’t yet learned to evaluate abnormalities in so many locations and in so many layers. So, I tried to get as far as possible just speaking with the patients: Age at onset? Family members with the same problems? Consanguinity? Night blindness?
I realised that asking about night blindness was too vague for most patients, and very few people notice a constriction of their visual field until very late in the disease. So instead I began to ask, “Do you frequently fall over your young children because you don’t see them?”
A comprehensive history, however, can only get you so far. At a certain point, you have to look at what’s going on in the retina. And that’s when it gets really difficult!
Some abnormalities are obvious, but some signs are so subtle. And the overlap between various hereditary retinal diseases is enormous. The genetics specialist in our hospital, Dr van den Born, receives all the “I have no idea what this is” referrals. She is completely familiar with an entire group of diseases that most ophthalmologists read about during their residencies but probably haven’t seen since.
But the medical retina rotation isn’t limited to exotic retinal dystrophies and ERGs. Working in the fluorescein angiography clinic is an adventure full of unusual and unsettling juxtapositions. The fantastic feeling of making a correct diagnosis, like an unusual chorioretinitis, is often immediately followed by the shame of an unsuccessful venous cannulation for fluorescein injection.
One moment you feel like an advanced subspecialist, and the next moment like a struggling first-year medical student.
It’s a humbling experience. The FA clinic keeps you sharp, because the pathologies themselves are so varied. Vascular, inflammatory, neoplastic, degenerative and traumatic come one after the other. Yes, they’re all (chorio) retinal, but no, they have nothing else in common.
Wednesday afternoons in the macular degeneration clinic offer a few hours of intellectual relaxation. For most of the patients seen here, the diagnosis has usually already been established and the treatment initiated. We simply have to decide, based on visual acuity and OCT scans, how to proceed with treatment.
This isn’t to say it’s easy, but really, the options are pretty limited. More injections, fewer injections, no injections. More difficult is managing patients’ expectations, particularly those in whom the macula of their best eye is progressively worsening. You can feel these patients’ worlds shrinking as they sit before you. Driving a car has long been abandoned. The bicycle has been sold. Visits to the museum have stopped. But until recently they could at least identify their family and friends. No longer. They now pass old friends on the street without recognising them. They can no longer distinguish the faces of their grandchildren. The computer skills that they worked so hard to develop have become irrelevant, as they can no longer read what is written on the screen nor enjoy the photographs that they have been sent. It seems as though every macular degeneration sufferer has always loved to read or knit. No longer. Joining them on their emotional journey can be quite intense.
The diabetic & vascular (“Diva”) retinopathy is a different story. “I know you absolutely want to initiate treatment of this early diabetic macular edema,” said my supervisor about a new patient. “But I’d suggest you wait a few months until her vision decreases. Her visual acuity will decrease during the next few months, even with early treatment. But if we treat now, she’s likely to blame the vision loss on your treatment. That will lead to distrust, poor treatment compliance, and worse outcomes.”
The diabetic patient is for us a difficult one to decipher. We ophthalmologists, as compulsive, detail-obsessed individuals for whom vision is so crucial, cannot
comprehend the seemingly careless attitude that some at-risk patients have. But then a quick reminder of these patients’ daily schedules – dietary sacrifices, fingertip pricks, insulin injections and the constant threat of hypoglycaemic misery, not to mention the sword of Damocles perpetually hanging over their heads and hearts – allows us to understand their occasional deviation from all their doctors’ recommendations. It remains difficult to accept the fact that some patients will continue to miss important laser appointments and won’t return for treatment until they develop a vitreous haemorrhage or worse.
Of course, when it comes to sheer complexity, uveitis is king. Just when the diagnosis seems clear, when the treatment plan appears logical, when you think
you’ve got the inflammation more or less under control, it takes a surprising turn. Recurrences, complications, referrals, masquerade syndromes. It seems uveitis can always stay one step ahead.
In this case, we take refuge in the intravitreal injection clinic. Twenty-five consecutive injections, simple as can be. Left eye or right? Do you have your antibiotic drops? Great, see you next month!
by Leigh Spielberg
Unusual juxtapositions make for exhilarating – and sometimes humbling – adventure
RETINAL ROTATION
Feature
RESIDENT’S DIARY
Illus
tratio
n: E
oin
Cove
ney
Leigh Spielberg is an ophthalmology resident at the Rotterdam Eye Hospital in The Netherlands

New Orleans 2013
Save the DateSaturday, November 16 -Monday, November 18, 2013
Make the most of your time while in New Orleans and attend the EyeWorld programs for an educational opportunity to network with your colleagues.
Check often for program updates:
www.EyeWorld.org
Registration opens August 2013
Oct ESCRS - EW at AAO 2013-revDL_Layout 1 8/28/13 2:39 PM Page 1

64
EUROTIMES | Volume 18 | Issue 10
At the heart of EVA is a revolutionary fluid control system called VacuFlow VTi using Valve Timing intelligence technology. It just effortlessly delivers the precise flow and fast vacuum required by you, the surgeon.
Put simply, EVA VacuFlow VTi technology puts you in absolute control, all of the time.
• ESCRS booth #A20
• Symposium: DORC goes Anterior October 6, 2013 • Room D203/204 • 13:00-14:00 h
Visit our DuTCh mASTERpiECE
109-1104 ADV-masterpieces-120x300-2.indd 1 8/30/13 3:15 PM
Ready-to-use air gas mixtureGeuder has announced the launch of EasyGas, a ready-to-use air-gas mixture in syringes. "The sterile pre-filled syringe system is immediately applicable and easy to use," said a Geuder spokeswoman.
"The precise mixture ratio of the non-expanding concentration guarantees a safe use.
Furthermore, the colour coding avoids a mix-up of the gases.Three gases will be available: EasyGas SF6 (Sulfurhexafluoride 20%), EasyGas C2F6 (Hexafluorethane 16%) as well as EasyGas C3F8 (Octafluorpropane 12%)," said the spokeswoman nwww.geuder.com/easygastamponade!
Femto splitter
Katena says its new produce the Donnenfeld Femto Splitter, designed by Eric D Donnenfeld MD of Rockville Centre, will complement modern cataract femtosecond ablation techniques. "The paracentral curve in the shaft exactly matches the shape of a laser created central nuclear bowl, providing optimal surface contact for efficiently splitting the lens out to the periphery and down to the posterior plate," said a company spokeswoman. "The Donnenfeld Femto Splitter improves post-
ablation nuclear chopping with minimal manipulation," she said.nwww.katena.com
Abbott acquires OptiMedicaAbbott has completed its acquisition of OptiMedica Corporation.
"OptiMedica's Catalys system enhances Abbott's leadership position in vision care with the addition of a state-of-the-art laser cataract technology to our portfolio," said Murthy Simhambhatla, senior vice-president, medical optics, Abbott.
"OptiMedica's technology combined with Abbott's global market presence, offer the potential to provide advanced cataract treatment options to more patients around the world," he said.
In a press release announcing the acquisition, Abbott stated that it had acquired OptiMedica for $250m, net of cash. Additional amounts totaling up to $150m will be payable upon completion of certain development, regulatory and sales milestones.nwww.abbott.com
Symptomatic vitreomascular adhesion (VMA)Health Canada has approved JETREA (ocriplasmin) for the treatment of symptomatic vitreomacular adhesion (VMA). Canada is the first market where JETREA is approved outside the US and Europe. ThromboGenics’ partner Alcon holds the commercialisation rights to JETREA outside the US and will be responsible for the launch of the drug in Canada.
Alcon, a division of Novartis, acquired the rights to commercialise JETREA outside the US in March 2012. It launched the drug in the UK, its first European market, in April, followed by launches in Germany, Denmark, Finland, Norway and Sweden. ThromboGenics is commercialising the drug in the US and launched JETREA® in the US in mid-January 2013 where it is approved for the treatment of patients with symptomatic VMA.
Dr Patrik De Haes, CEO of ThromboGenics, said: “The Priority Review approval of JETREA in Canada, the first market outside the US and Europe, is further evidence that all stakeholders are committed to making this first pharmacological drug available quickly to as many patients as possible."nwww.thrombogenics.com
Feature
INDUSTRY NEWSRecent developments in the vision care industry
Don’t Miss Eye on History, see page 70

65
EUROTIMES | Volume 18 | Issue 10
Review
BOOK REVIEW
If you have a book you would like to have reviewed please send it to: EuroTimes, Temple House, Temple Road, Blackrock, Co Dublin, Ireland
“Never underestimate a ‘simple’ cataract operation,” a senior cataract surgeon and corneal transplant specialist told me during my cataract surgery rotation. “It can go wrong very quickly if you’re not careful.”
This was quite a revelation, coming from someone who was well experienced in dealing with penetrating keratoplasty, DSAEK, and all the other complicated ocular surface procedures.
Once I started operating myself, I came to realise how many different types of complications could occur. From the initial corneal incisions to the final hydration of the wounds, essentially everything can go wrong. It is these problems that are addressed in a new book from Slack Incorporated, Cataract Surgery Complications.
“All surgeons have complications… we hope you only have a few… and that this book will help to resolve them very well,” the authors write. Within 150 pages, Lucio Buratto, Stephen F Brint, and Mario R Romano have produced a concise manual with well-illustrated text for the beginning and intermediate-level cataract surgeon.
Indeed, despite our specialty’s total familiarity with cataract surgery, the concept of inserting a highly energetic tool and many sharp instruments into one of the body’s most delicate organs remains vaguely disconcerting. So, we should be highly prepared, both for the operation itself and the potential pitfalls during and after surgery.
Chapter 1, “Anesthesia by Injection,” covers a topic frequently skipped in cataract surgery texts. In fact, it is frequently overlooked in residency training, due to the widespread adoption of topical anaesthesia and the presence of anaesthesiologists who administer the occasional retrobulbar injection. Chapter 2 covers the corneal incision, concentrating on the optimal techniques to ensure watertight closure and thus minimise endophthalmitis risk.
Chapters 3 and 14 discuss the capsulorrhexis and the seemingly endless ways that this step can ruin an entire procedure. “Since the anterior capsule cannot be mended once a complication has occurred, management must be prompt and principles of prevention are paramount.” The rhexis can be too big, too small, decentred and irregularly shaped. This book provides advice on how to cope with these and other problems.
The text is not limited to cataract surgery, per se. In case of posterior capsular rupture,
posterior segment manoeuvres must be undertaken. “The surgeon’s primary concern with capsular rupture is to prevent nuclear dislocation into the vitreous.” Chapters 9 and 10 cover anterior and posterior vitrectomy, respectively.
A posterior vitrectomy is beyond the reach of most cataract surgeons, but it’s nonetheless good to know how to prepare an eye for transfer to the vitreoretinal specialist and to read, in simple terms, what happens once the patient’s care has been assumed by the posterior segment surgeon. The same applies for endophthalmitis, which is covered in Chapter 11. CME, or Ivine Gass syndrome, the treatment of which is usually the responsibility of the cataract surgeon, is the topic of Chapter 12.
Besides the classic complications, more modern concerns are also discussed, such as those associated with the femtosecond laser, and the avoidance of posterior capsular opacification with the endocapsular ring. Further, advanced complication management techniques, like using the intraocular lens as a scaffold to prevent dropped nuclei after posterior capsule rupture, are introduced to the reader.
“Cataract Surgery Complications” is intended for the beginning and intermediate-level cataract surgeon, which includes ophthalmology residents during their surgical rotations and ophthalmologists who are considering or completing a cataract surgery fellowship.
www.oculus.de
The Power ofColour ToPograPhy
experience the Keratograph 5M Topographer!
Visit booth no. e02 at eSCrS, amsterdam
OCULUS presents the future in
corneal topography and dry eye
diagnosis! Find out what the new
Keratograph 5M with colour camera
and magnification changer can do
for you and your patients!
Oc Eurotimes K5M bunt 120x300 4c1 1 21.08.2013 13:04:52
BOOKS EDITORLeigh Spielberg
PUBLICATIONCATARACT SURGERY COMPLICATIONS
EDITORS IN CHIEFLUCIO BURATTO, STEPHEN F BRINT, AND MARIO R ROMANO
PUBLISHED BY SLACK INCORPORATED
Be prepared
SYMPOSIUM & CONGRESS
2014 APRIL 25–29B O S T O N
Additional Programming
Cornea DayASCRS Glaucoma Day
ASOA WorkshopsTechnicians & Nurses Program
REGISTRATION OPENSOCTOBER 16, 2013
www.ascrs.orgwww.asoa.org
The Only U.S. Meeting Dedicated to the Anterior Segment Specialist
&The Leading Practice Management
Program in Ophthalmology
Follow @ASCRStweets on Twitter.#ASCRSASOA2014
AMER
ICAN
SOC
IETY OF CATARACT AND REFRACTIVE SURGERY
Y E A R S
19742014

67
EUROTIMES | Volume 18 | Issue 10
Frankfurt is one of the great business centres of the world which is one of the reasons why the ESCRS Practice Development
Committee has decided to hold its third Practice Management Weekend in this great German city.
Frankfurt is the largest financial centre in continental Europe and ranks among the world's leading financial centres. It is home to the European Central Bank, Deutsche Bundesbank, Frankfurt Stock Exchange and several large commercial banks.
It is also a city steeped in culture and history and is home to the Johann Wolfgang Goethe University and Frankfurt University of Applied Sciences, many museums (eg, Städel, Naturmuseum Senckenberg, Schirn Kunsthalle Frankfurt, Goethe House). The city also has two major botanical gardens, the Palmengarten, which is Germany's largest, and the Botanical Garden of the Goethe University.
One of the major goals of the ESCRS Practice Management programme is to teach ophthalmologists that running a successful ophthalmological practice requires both clinical excellence and also business skills.
The Practice Management meeting in Frankfurt will be held from Friday November 1 to Sunday November 3.
The committee has chosen excellent speakers for what promises to be a very interesting programme. As well as learning from some of the key opinion leaders in Europe, the weekend will offer the opportunity to network in an informal and relaxed setting.
Assumptions and truths The theme of this year’s meeting is “Building your own Practice – Assumptions and Truths” and it is hoped that the programme will allow delegates a unique opportunity to get
advice from top ophthalmologists and also marketing and management consultants on how to grow and improve their practices.
So why Assumptions and Truths? As one of our keynote speakers Manfred Tetz will explain, what ophthalmologists assume they know and what they actually know are two different things.
Personal voyage In his talk "From Small to Big – A Personal Voyage" Prof Tetz will explain that when he opened his private practice in Berlin in May 2003, he saw one patient during the whole day. Today, Eye Centre Spreebogen is staffed by two full-time ophthalmologists in addition to Prof Tetz. There are also three part-time colleagues for specialised work such as retina and strabismus, and a few affiliated surgeons who use the clinic’s facilities for private patients. Despite an uneven economy, practice volume has grown steadily at about 10 per cent annually, says Prof Tetz, who will discuss his personal voyage at the Frankfurt meeting.
ESCRS is also honoured to have as another keynote speaker Prof Thomas Kohnen. There was a time when work as a university-based ophthalmologist ensured a steady stream of private patients who arrived based on the reputation of institution alone and the assurance that the best doctors worked there. But, times have changed, and today university-based ophthalmology practices compete head-to-head with private practices with the newest technology and excellent surgeons.
In his lecture, Prof Kohnen will talk about his work to re-invent his university-based department in order to make it competitive with private clinics, while ensuring the highest standards of care for patients. The workshop will explore all aspects of running a successful practice – from staffing to acquiring the newest technology.
The full programme for the Practice Management Weekend is at: http://pmfrankfurt.escrs.org.
* Colin Kerr is executive editor of EuroTimes and project manager for the ESCRS Practice Development Programme.
The moment twice the speed puts the finishing touch on proven experience.This is the moment we work for.
// MEL 90 MADE BY ZEISS
The excimer laser that intelligently combines experience and advancement –
that is the MEL® 90 from ZEISS. Refractive surgeons will be fascinated by its
practical flexibility. With the FLEXIQUENCE switch function, they can easily
choose between 250 Hz or 500 Hz operation as their personal or individual
practice situation requires. The innovative Triple-A profile and intra-operative
ablation speed of 1.3 seconds per diopter enable fast, safe and tissue-saving
treatments. These along with many other performance features make the
MEL 90 a customized, success-oriented power package.
MEL 90 – your preferences, your workflow, your expectations precisely.
Visit us at ESCRS at hall 1 booth G02 to explore the new landmark of the ZEISS Refractive Laser Scenerywww.meditec.zeiss.com/escrs
MEL
90
is no
t app
rove
d fo
r sal
e in
the
U.S.
by Colin Kerr
Third Practice Management Weekend to be held in Frankfurt, Germany
PERSONAL VOYAGE
Feature
PRACTICE DEVELOPMENT
“What ophthalmologists assume they know and what they actually know are two different things”
Manfred Tetz
EL CONQUISTADORa Waldorf Astoria Property
The Premier Innovative Educational Retreat for
Anterior Segment Surgeons and Administrators
REGISTER TODAYAND BOOK HOUSING
www.WinterUpdate.org
• Accessible faculty leads an open exchange of techniques and solutions• Strategize in a relaxing environment on the “Island of Enchantment”
• High-energy sessions for physicians and practice managers
• A family-friendly setting with a private beach, golf, horseback riding, water park, all near the El Yunque rainforest

Review
JCRS HIGHLIGHTSJournal of Cataract and Refractive Surgery
Collagen crosslinking: New hope for more advanced ectatic disease?JCRS provides an issue featuring a collection of papers on collagen crosslinking (CXL). Eight full-length articles highlight the evolution of the understanding of this treatment for corneal ectatic disease. In a lead editorial William Dupps MD notes that investigators are grappling for evidence-based answers to questions such as who can benefit most from CXL and which treatment modalities are most effective. Several of the studies in this issue incorporate prospective designs, documentation of pretreatment disease progression and contralateral controls to elevate the level of clinical evidence and the likelihood that valid answers will emerge. The papers reflect some of the most pressing and elusive questions in clinical CXL and add more voices, some dissenting, to key controversies, he notes.
n WJ Dupps et al., JCRS, “Effective corneal collagen crosslinking in advanced cases of progressive keratoconus”, Volume 39, Issue 8, 1131-1132.
Corneal ring segments plus CXLOne open question in keratoconus treatment concerns the potential benefit of combining corneal ring segments and ultraviolet-A and riboflavin collagen crosslinking (CXL). Accordingly, researchers conducted a retrospective comparative case series study to evaluate the efficacy of single or paired intrastromal corneal ring segments combined with CXL in 74 patients with keratoconus. Consecutive patients with keratoconus had femtosecond laser-assisted ring segment implantation combined with same-day CXL between 2008 and 2011. Some 47 eyes of 40 patients received paired segments while 38 eyes of 34 patients received single rings segments. The uncorrected distance visual acuity was significantly improved after single ICRS (3.4 lines; P=.04) and paired ring segment (2.7 lines; P=.01) implantation combined with CXL. Corrected distance visual acuity remained stable. The single and paired ICRS groups had a significant reduction in mean cylinder at one year (single ICRS: −3.84 dioptres [D] ± 1.72 [SD] versus −2.19 ± 1.54 D, P=.02; paired ICRS: −3.91 ± 1.45 D versus −2.96 ± 1.92 D) (P=.02). There
was no significant difference in total higher order aberrations. No patient lost lines of CDVA.
n Sonia N. Yeung et al., JCRS, “Efficacy of single or paired intrastromal corneal ring segment implantation combined with collagen cross linking in keratoconus”, Volume 39, Issue 8, Pages 1146-1151.
Femto laser retreatmentLASIK has evolved into a predictable refractive surgery technique with reports of good long-term stability. Nonetheless, a significant number of patients require a second surgery, referred to as a retreatment or enhancement, to correct residual refractive errors after LASIK. Investigators studied the utility of creating an additional side cut within the old laser LASIK flap using a femtosecond laser to reduce the incidence of epithelial ingrowth in patients having retreatments for residual refractive errors after LASIK. In a comparative case series 24 eyes of 18 patients had femtosecond laser-assisted retreatment with side cut only, while 103 eyes of 80 patients had a flap-lift LASIK enhancement. Twenty-seven cases of epithelial ingrowth were identified in the two groups, four cases (17 per cent) in the side-cut group and 23 cases (22 per cent) in the flap-lift group. There was a statistically significant difference between the two groups in the incidence of epithelial ingrowth in patients in which the microkeratome was used as the initial method of flap creation.
n PK Vaddavalli et al., JCRS, “Femtosecond laser-assisted retreatment for residual refractive errors after laser in-situ keratomileusis”, Volume 39, Issue 8, 1241-1247.
69
EUROTIMES | Volume 18 | Issue 10
Thomas KohnenASSOCIATE EDITOR OF JCRS
FURTHER STUDYBecome a member of ESCRS to receive a copy of EuroTimes and JCRS journal
Address: Hermann-Burkhardt-Straße 3 72793 Pfullingen • GermanyTel: +49 (0) 7121-69 065-20 Email: [email protected]
LOOKING FOR A NEW PREMIUM OFFER?ALSANZA, German manufacturer of medical and pharmaceutical liquids, extends its activities to Surgical Ophthalmology, focusing on:
IOLs OVDs Knives BSS Phaco
www.alsatoriscan.com
LSIOLMonofocal
ALSANZA family of IOLs:
TORIC LSIOL
Monofocal Toric
3D toric LSIOL
Multifocal Toric
3D LSIOL
Multifocal
ESCRS
Booth K05
Hall 1
alsanza_uk_120_300_mm 2.indd 1 08/07/13 17:43
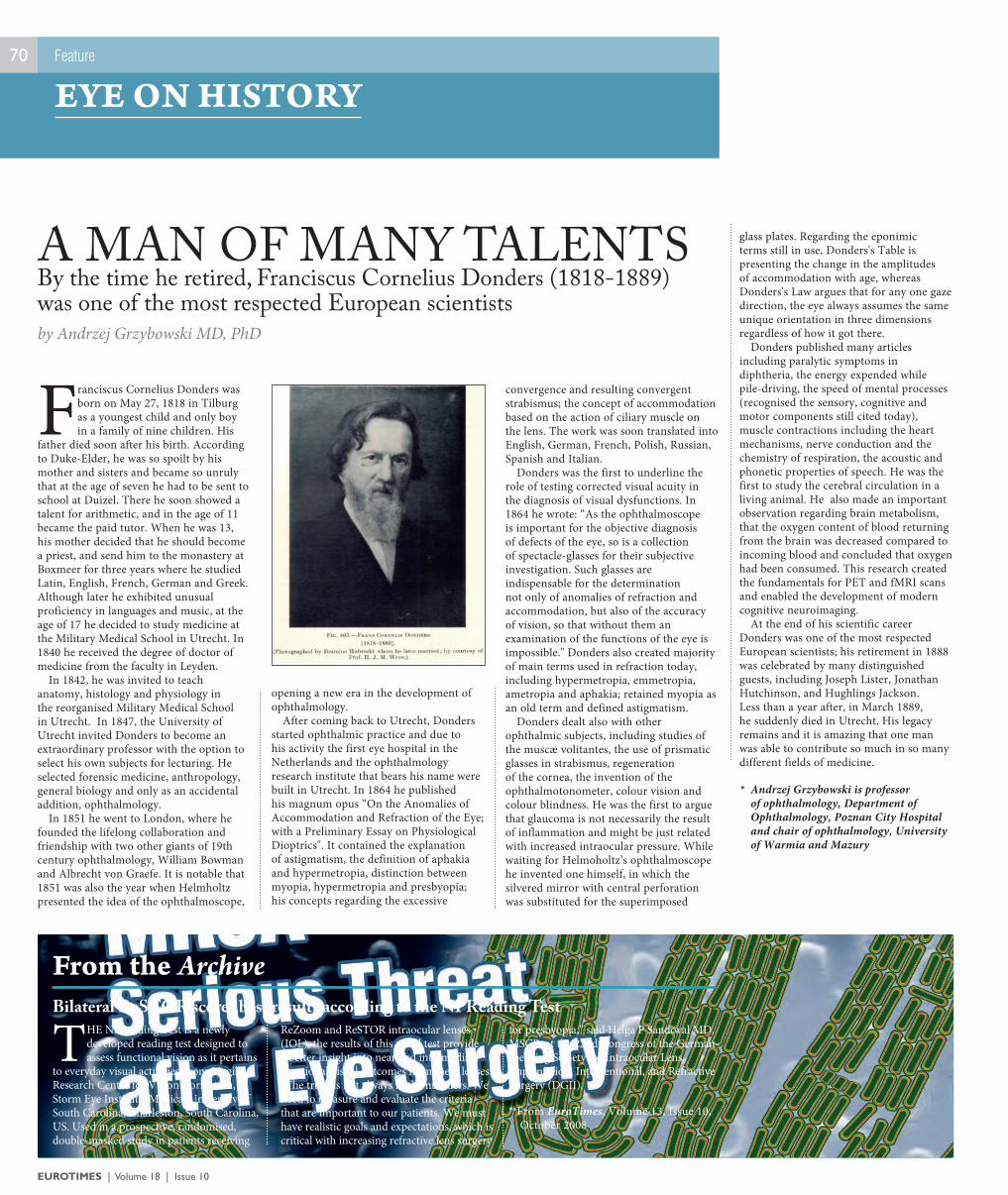
EUROTIMES | Volume 18 | Issue 10
70
Franciscus Cornelius Donders was born on May 27, 1818 in Tilburg as a youngest child and only boy in a family of nine children. His
father died soon after his birth. According to Duke-Elder, he was so spoilt by his mother and sisters and became so unruly that at the age of seven he had to be sent to school at Duizel. There he soon showed a talent for arithmetic, and in the age of 11 became the paid tutor. When he was 13, his mother decided that he should become a priest, and send him to the monastery at Boxmeer for three years where he studied Latin, English, French, German and Greek. Although later he exhibited unusual proficiency in languages and music, at the age of 17 he decided to study medicine at the Military Medical School in Utrecht. In 1840 he received the degree of doctor of medicine from the faculty in Leyden.
In 1842, he was invited to teach anatomy, histology and physiology in the reorganised Military Medical School in Utrecht. In 1847, the University of Utrecht invited Donders to become an extraordinary professor with the option to select his own subjects for lecturing. He selected forensic medicine, anthropology, general biology and only as an accidental addition, ophthalmology.
In 1851 he went to London, where he founded the lifelong collaboration and friendship with two other giants of 19th century ophthalmology, William Bowman and Albrecht von Graefe. It is notable that 1851 was also the year when Helmholtz presented the idea of the ophthalmoscope,
opening a new era in the development of ophthalmology.
After coming back to Utrecht, Donders started ophthalmic practice and due to his activity the first eye hospital in the Netherlands and the ophthalmology research institute that bears his name were built in Utrecht. In 1864 he published his magnum opus “On the Anomalies of Accommodation and Refraction of the Eye; with a Preliminary Essay on Physiological Dioptrics". It contained the explanation of astigmatism, the definition of aphakia and hypermetropia, distinction between myopia, hypermetropia and presbyopia; his concepts regarding the excessive
convergence and resulting convergent strabismus; the concept of accommodation based on the action of ciliary muscle on the lens. The work was soon translated into English, German, French, Polish, Russian, Spanish and Italian.
Donders was the first to underline the role of testing corrected visual acuity in the diagnosis of visual dysfunctions. In 1864 he wrote: “As the ophthalmoscope is important for the objective diagnosis of defects of the eye, so is a collection of spectacle-glasses for their subjective investigation. Such glasses are indispensable for the determination not only of anomalies of refraction and accommodation, but also of the accuracy of vision, so that without them an examination of the functions of the eye is impossible." Donders also created majority of main terms used in refraction today, including hypermetropia, emmetropia, ametropia and aphakia; retained myopia as an old term and defined astigmatism.
Donders dealt also with other ophthalmic subjects, including studies of the muscæ volitantes, the use of prismatic glasses in strabismus, regeneration of the cornea, the invention of the ophthalmotonometer, colour vision and colour blindness. He was the first to argue that glaucoma is not necessarily the result of inflammation and might be just related with increased intraocular pressure. While waiting for Helmoholtz’s ophthalmoscope he invented one himself, in which the silvered mirror with central perforation was substituted for the superimposed
glass plates. Regarding the eponimic terms still in use, Donders's Table is presenting the change in the amplitudes of accommodation with age, whereas Donders's Law argues that for any one gaze direction, the eye always assumes the same unique orientation in three dimensions regardless of how it got there.
Donders published many articles including paralytic symptoms in diphtheria, the energy expended while pile-driving, the speed of mental processes (recognised the sensory, cognitive and motor components still cited today), muscle contractions including the heart mechanisms, nerve conduction and the chemistry of respiration, the acoustic and phonetic properties of speech. He was the first to study the cerebral circulation in a living animal. He also made an important observation regarding brain metabolism, that the oxygen content of blood returning from the brain was decreased compared to incoming blood and concluded that oxygen had been consumed. This research created the fundamentals for PET and fMRI scans and enabled the development of modern cognitive neuroimaging.
At the end of his scientific career Donders was one of the most respected European scientists; his retirement in 1888 was celebrated by many distinguished guests, including Joseph Lister, Jonathan Hutchinson, and Hughlings Jackson. Less than a year after, in March 1889, he suddenly died in Utrecht. His legacy remains and it is amazing that one man was able to contribute so much in so many different fields of medicine.
* Andrzej Grzybowski is professor of ophthalmology, Department of Ophthalmology, Poznan City Hospital and chair of ophthalmology, University of Warmia and Mazury
by Andrzej Grzybowski MD, PhD
By the time he retired, Franciscus Cornelius Donders (1818-1889) was one of the most respected European scientists
A MAN OF MANY TALENTS
Feature
EYE ON HISTORY
From the ArchiveBilateral ReSTOR scores best results according to the NPReading Test
THE NPReading Test is a newly developed reading test designed to assess functional vision as it pertains
to everyday visual activities, from Magill Research Center for Vision Correction, Storm Eye Institute, Medical University of South Carolina, Charleston, South Carolina, US. Used in a prospective, randomised, double-masked study in patients receiving
ReZoom and ReSTOR intraocular lenses (IOL), the results of this novel test provide a better insight into near and intermediate functional visual outcomes from these lenses.“The truth is not always in the numbers. We need to measure and evaluate the criteria that are important to our patients. We must have realistic goals and expectations, which is critical with increasing refractive lens surgery
for presbyopia,” said Helga P Sandoval MD, MSCR, at the 22nd Congress of the German-speaking Society for Intraocular Lens Implantation, Interventional, and Refractive Surgery (DGII).
* From EuroTimes, Volume 13, Issue 10, October 2008
71
EUROTIMES | Volume 18 | Issue 10
Review
OPHTHALMOLOGICA
José Cunha-VazEDITOR OF OPHTHALMOLOGICA,The peer-reviewed journal of EURETINA
– William Butler Yeats
EDUCATION
FILLINGLIGHTING
F I R E
IS NOT THE
OF A
OF A PAIL, BUT THE
http://elearning.escrs.orgGain access to all of this and more online at
Learn and explore key aspects of modern anterior segment surgery
Prepared by ESCRS in partnership with Society opinion-leaders
Earn CME points
36 hours of interactive, assessed and accredited eLearning
Refractive Surgery Didactic Course
Cataract Surgery Didactic Course
Workshop on Visual Optics
Cornea Didactic Course
Basic Phaco Instructional Course
Surface Ablation Techniques Instructional Course
Endophthalmitis Instructional Course
Rituximab effective in refractory non-infectious ocular inflammation A growing body of evidence suggests that the monoclonal antibody, rituximab, can reduce both external and internal non-infectious ocular inflammation, according to a review of the literature. Numerous series have been published demonstrating that a single course of rituximab reduced the inflammation to a state of quiescence without the need for other immunosuppressive agents for periods ranging from 18 months to several years in eyes with refractory autoimmune disease with ocular involvement and eyes with intraocular lymphoma .
nO.Tomkins-Netzer et al Ophthalmologica “Can Rituximab Induce Long-Term Disease Remission in Patients with Intra-Ocular Non-Infectious Inflammation” 2013 October; Vol 230, Issue 4, DOI:10.1159/000351426.
MS thins retinal nerve fibre layerMeasurements carried out with spectral domain OCT indicate that multiple sclerosis (MS) may have a significant thinning effect on patients’ retinal nerve fibre layer (RNFL), especially in cases where there is also optic neuritis, according to the results of a retrospective study. In 24 eyes of 12 MS patients the average peripapillary RNFL thickness, as measured by OCT was 81.9 µm, compared to the control value of 102.1 µm (p = 0.001). In MS patients with a history of optic neuritis, RNFL was thinner than that of MS patients without optic neuritis (71.8 µm vs. 92.0 µm, p = 0.001).
nL Feng ey al . Ophthalmologica • The Evaluation of the Retinal Nerve Fiber Layer in Multiple Sclerosis with Special-Domain Optical Coherence Tomography 2013 October; Vol 230, Issue 4, DOI:10.1159/000351862.
Triple therapy stabilises refractory AMDTriple therapy with ranibizumab, triamcinolone and reduced fluence PDT can stabilise vision in eyes with exudative AMD that has not responded to anti-VEGF therapy alone, according to the results of a prospective study involving 30
patients. Three groups of 10 patients each received one of three variations of triple therapy. At six months follow-up, the groups that underwent PDT with reduced fluence and either reduced or standard irradiance had slight but insignificant improvements in visual acuity, but in the group that underwent standard fluence PDT the visual acuity decreased by 0.29 (p < 0.05) logMAR.
nVeritti D. • Ophthalmologica Triple Therapy for Anti-Vascular Endothelial Growth Factor Nonresponders in Neovascular Age-Related Macular Degeneration: Impact of Different Photodynamic Therapy Parameters 2013 October; Vol 230, Issue 4, DOI:10.1159/000351651.
Indocyanine green slows recovery A retrospective analysis of spectral-domain optical coherence tomography images in 34 eyes of 34 patients who had undergone macular hole surgery with or without indocyanine green staining of the inner limiting membrane showed that the inner segment/ outer segment defect was significantly worse at one and three months in those who underwent surgery with ICG. Moreover, the changes in BCVA were significantly better in the non-ICG group at one and three months, but the groups did not differ significantly at six months.
nShiono A., “Ophthalmologica Effects of Indocyanine Green Staining on the Recovery of Visual Acuity and Macular Morphology after Macular Hole Surgery”, 2013 October; Vol 230, Issue 4, DOI:10.1159/000351661.
WWW.EURETINA.ORG
25 JANUARY 2014ROME CAVALIERI WALDORF ASTORIA HOTEL, ITALY
4TH EURETINAWINTER MEETINGROME
Reference
CALENDAR OF EVENTSDates for your Diary
2013 2014
72
OCTOBER
ESCRS Glaucoma Day4 OctoberAmsterdam, The Netherlandswww.escrs.org
4th EuCornea Congress4-5 OctoberAmsterdam, The Netherlandswww.eucornea.org
XXXI Congress of the ESCRS5-9 OctoberAmsterdam, The Netherlandswww.escrs.org
EPOS/WSPOS Paediatric Sub Speciality Day9 OctoberAmsterdam, The Netherlandswww.wspos.org
43rd ECLSO Congress25-26 OctoberMunich, Germanywww.eclso.eu
NOVEMBER
Queen Victoria Hospital NHS Foundation Trust - Corneoplastic Professional Education Meeting1 NovemberLingfield, UKwww.qvh.nhs.uk
NOVEMBER
Practice Management Weekend1-3 NovemberFrankfurt, Germanyhttp://pmfrankfurt.escrs.org/
AAO Annual Meeting16-19 NovemberNew Orleans, USAwww.aao.org
93rd SOI National Congress27-30 NovemberRome, Italywww.congressisoi.com
The MCLOSA 20th Annual Scientific Meeting29 NovemberLondon, UKwww.mclosa.org.uk
2014 JANUARY
5th International Course on Ophthalmic and Oculoplastic Reconstruction and Trauma Surgery8-10 JanuaryVienna, Austriawww.ophthalmictrainings.com
JANUARY
4th EURETINA Winter Meeting25 JanuaryRome, Italywww.euretina.org
FEBRUARY
18th ESCRS Winter Meeting14-16 FebruaryLjubljana, Sloveniawww.escrs.org
NEW ENTRY12th International Ocular Inflammation Society Congress27 February – 1 MarchValencia, Spainhttp://ioisvalencia.org/
MARCH
Frankfurt Retina Meeting 201415-16 MarchMainz, Germanywww.eckardt-frankfurt.de
The 5th World Congress on Controversies in Ophthalmology (COPHy)20-23 MarchLisbon, Portugalhttp://www.comtecmed.com/cophy
APRIL
ASCRS•ASOA Symposium and Congress25-29 AprilBoston, USAwww.ascrs.org
AUGUST
NEW ENTRYNordic Congress of Ophthalmology (NOK 2014)20-23 AugustStockholm, Swedenhttp://www.nok2014.se/Default.aspx
SEPTEMBER
NEW ENTRY14th EURETINA Congress11-14 SeptemberLondon, UKwww.euretina.org
NEW ENTRY5th EuCornea Congress12-13 SeptemberLondon, UKwww.eucornea.org
NEW ENTRYXXXII Congress of the ESCRS13-17 SeptemberLondon, UKwww.escrs.org
If you would like to see your classified ad here, please contact Mairin Condon: [email protected].
Advertising Directory: Abbott Medical Optics: Pages: 13, IBC; AcuFocus: Page: 7; Alcon: Pages: 54-55, OBC; Alsanza Medizintechnik und Pharma GmbH: Page: 69; ASCRS/Eyeworld: Pages: 63, 66, 68; Bausch + Lomb | Technolas: Pages: 37, 49; Benz Research & Development: Page: 17; Carl Zeiss Meditec: Pages: 6, 67; Croma-Pharma GmbH: Page: 34; D.O.R.C. International BV: Page: 64; ESASO: Page: 58; Geuder: Page: 21; Haag Streit Ag: Pages: 10, 27; Hoya Surgical Optics GmbH: Page: 33; Huvitz: Page: 30; IROC AG: Page: 12; Keeler: Page: 31; Medicontur International SA: Page: 23; Millennium Biomedical Inc. (MBI): Page: 15; Moria: Pages: 19, 46; Nidek: Page: 43; Novartis: Pages: 45, 51; Oasis Medical: Page: 57; Oculus Optikgerate GmbH: Page: 65; Oertli Instruments AG: Page: IFC; Rayner Intraocular Lenses Ltd: Page: 3; S. Karger AG: Page: 38; Schwind Eye-Tech-Solutions: Page: 11; TearScience: Page: 36; The Eyebag Company: Page: 39; VSY Biotechnology: Page: 9; Ziemer Ophthalmic Systems: Page: 35

F A M I L Y O F I O L S
F A M I L Y O F I O L S
F A M I L Y O F I O L S
Multifocal Toric Multifocal Toric MonofocalPreloaded
The TECNIS® family of IOLs: Proven performance and outcomes. Invaluable peace-of-mind.
You deserve some inner peace. And that’s what you get with the broad portfolio of TECNIS® aspheric IOLs. The proven combination of optics, material, and design associated with TECNIS® IOLs continues to help you provide patients with predictable, high-quality outcomes.
When it comes to peace-of-mind, the choice is clear.
Visit www.tecnisiol.com to learn more.TECNIS is a trademark owned by or licensed to Abbott Laboratories, its subsidiaries or affiliates. ©2012 Abbott Medical Optics Inc.www.AbbottMedicalOptics.com / 2012.11.14-CT81
WELCOME TO THE ERA OF CENTURION®
Active Fluidics™
Automatically optimizes chamber stability by allowing surgeons to customize and control IOP throughout the procedure.
Balanced Energy™
Enhances cataract emulsification efficiency using OZil® Intelligent Phaco and the new INTREPID® Balanced Tip design.
Applied Integration™
Designed to work seamlessly with other Alcon technologies for an integrated cataract procedure experience.
Optimize every moment of your cataract removal procedure with the NEW CENTURION® Vision System.
©2013 Novartis 8/13 CNT13017JAD-i
THE CATARACT REFRACTIVE SUITE BY ALCON
Learn more about the new era of cataract procedures. Visit CenturionVisionSystem.com.
81423 CNT13097JAD ET.indd 1 9/11/13 2:07 PM