vitamin d status among emirati students - dr. a haq€¦ · vitamin d status among emirati students...
TRANSCRIPT
Vitamin D Status Among Emirati Students“Avoidance of Sunlight Causing Vitamin D Deficiency”
Afrozul Haq, Ph.D. Afrozul Haq, Ph.D. Afrozul Haq, Ph.D. Afrozul Haq, Ph.D. Pathology & Laboratory Medicine,Pathology & Laboratory Medicine,
SKMC, Abu DhabiSKMC, Abu Dhabi
2nd Biennial Pathology & Laboratory Medicine Update March 17,18, 2011

1. Rajah J. , Abdel-Wareth L. and Haq A. (2010).Failure of one alpha vitamin D (alphacalcidol) in treating nutritional rickets and biochemical response to ergocalciferol. J Steroid Biochem Mol Biol 121:273-276.
2. Rajah J., Haq, A. and Pettifor J.(2010) Vitamin D and calcium status in urban ambulatory children in the middle east. BMC Pediatrics(in press).3. Al Anouti F., Thomas J., Abdel-Wareth L., Rajah J, Grant W. and Haq A. (2010) . Vitamin D deficiency and sun avoidance among
university students at Abu Dhabi, United Arab Emirates. DermatoEndocrinology (in press).4. Haq A., Abdel-Wareth L. and Rajah J. (2009). Is there any correlation between 1,25(OH)2D and 25(OH)D in infants with rickets ?.
Bone , 45 Suppl.2: S102. 5. Rajah J., Haq A., Shalash A. and Du Plesis J. (2009). Diagnosis and prevention of vitamin D deficiency in childhood and a case
report of an infant with prolonged QTc interval. Paediatrics. me 14: 71-73.6. Haq A., Rajah J. and Abdel-Wareth L. (2009).Vitamin D: measurement, deficiency,and its health consequences. Middle East Lab.12(1): 6-10.7. Rajah J., Jamal A., Amani S., Howard P. and Haq A. (2008) . Nutritional rickets and Z scores for hight in the United Arab Emirates.
To D or not to D. Pediatrics International (Japan) 50: 424-428.8. Haq A., Rajah J. and Abdel-Wareth L. (2007). Routine HPLC analysis of vitamin D3 and D2 . DIALOG (Germany) 2: 1-2.
9. Haq A. (2007) Measurement of Vitamin D by HPLC and its role in Health and Diseases: First Clin. Chem. Forum, Abu Dhabi, UAE,1: 4-5.10. Al Anouti F., Thomas J., Ahmad B., Al Hasani S., Abdel-Wareth L., KhaliliAD. And Haq A. (2010) High prevalence of
List of Publications & Abstracts During 2007 to 2011
Vitamin D deficiency among young Emiratis in a sunny country. 28th Intl Symp Diabetes and Nutrition, Oslo, Norway. July1-4. 11. Haq, A. (2010)Vitamin D, metabolism, deficiency and cardiovascular disease. Pathology & Laboratory Medicine Update,
UKAS-SKMC Conference, Abu Dhabi, UAE, March 20. 12. Rajah J., Haq A., Abdel-Wareth L. and Al Jubeh J. (2010).Biochemical differences in nutritional rickets at different ages.
26th Intl. Pediatric Assoc . Cong. Johannesburg, South Africa, August 4-9.13. Haq A., Abdel-Wareth L. and Rajah J.(2009)Failure of one alpha vitamin D (alphacalcidol) in treating nutritional rickets and biochemical
response to ergocalciferol. 14th Workshop on Vitamin D. Brugge, Belgium, October 4-8.14. Rajah J, Al Jubeh J, Haq A , Shalash A and Parsons H. (2009). Osteopenia in mothers of rachitic infants: A new causal hypothesis for
rickets. Bone, 45 Suppl. 2: S101.15. Rajah J., Shalash A., Haq, A. and Plessis JD.(2007). Severe vitamin D deficiency induced cardiomyopathy. South African
Critical Med Congress, Sun City, Gauteng, South Africa, August 14-17.16. Haq A, Al Anouti F, Thomas J, Abdel-Wareth L and Rajah J.(2010) Avoidance of Sun Causing Vitamin D deficiency among Emirati
students. 2nd SEHA Research Conference, Abu Dhabi, December 12-13.17. Al Anouti F., Thomas J., Abdel-Wareth L., Grant BG and Haq A.(2011).The impact of life style and dietary habits on vitamin D status
among young Emiratis.1st WHO Regional Nutritional Conference, Doha(Qatar),…..18. Haq A. , Al Anouti F, Thomas J, Abdel-Wareth L and Rajah J. (2010). Avoidance of sunlight causing vitamin D deficiency among
Emirati students. 2nd SEHA Annual Research Conference, Abu Dhabi(UAE), December 12-13.19. Al-Anouti, F.,Thomas, J., Al Hasani, S., Abdelwareth, L, Haq A.,(2010). Sun, Sea, Sand and Sadness: Exploring the Links between
Vitamin D deficiency and depressive illness in the United Arab Emirates.The British Psychology Society Meeting, Manchester,UK, December1-3.

Vitamin D and its metabolites have many actions in the body not just those required to prevent rickets and osteomalacia.
These newly discovered actions include cancer prevention
WHY IS AN OLD “VITAMIN” SUDDENLY
IN THE NEWS?
These newly discovered actions include cancer prevention and treatment; regulation of hormone secretion; increased resistance to infections; protection against autoimmune diseases; prolonged survival of transplanted organs.
These newly discovered actions require vitamin D levels greater that those found in most people.
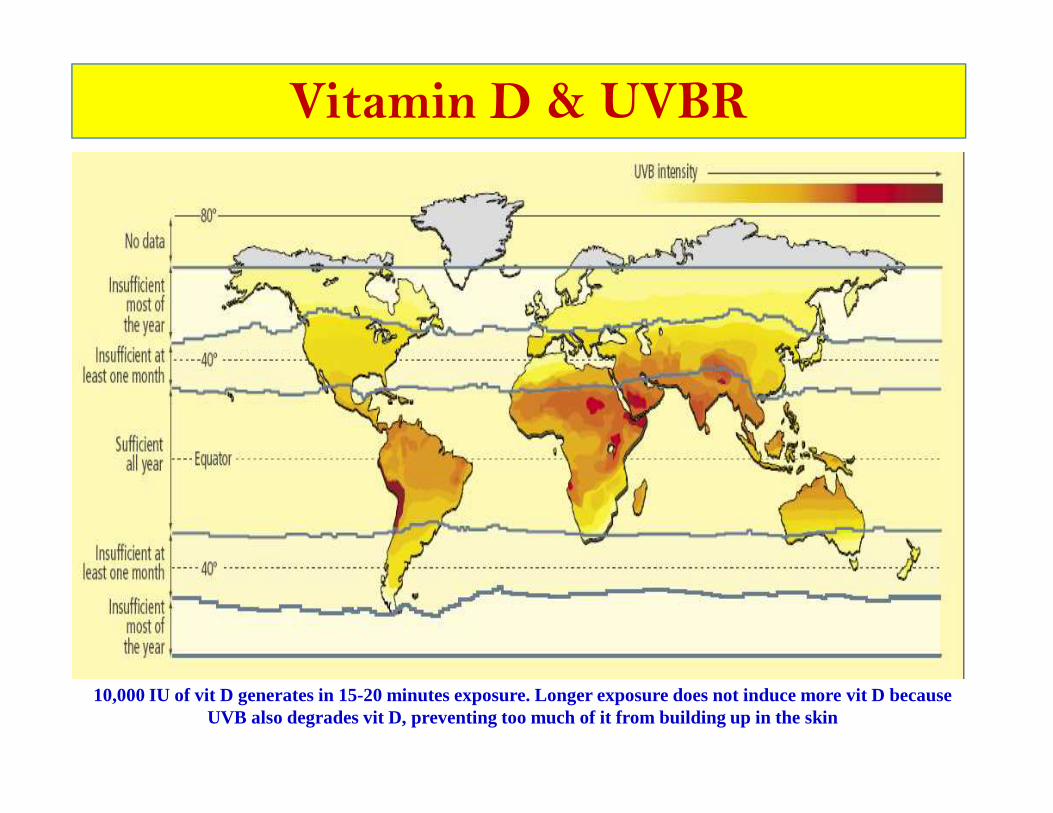
Vitamin D & UVBR
10,000 IU of vit D generates in 15-20 minutes exposure. Longer exposure does not induce more vit D because UVB also degrades vit D, preventing too much of it from building up in the skin

� All studies, in virtually all nations, irrespective of latitude, show that the majority of the world’s population haspopulation hasinadequate vitamin D status

� Vitamin D2 (Ergocalciferol)Ergo sterol from plants/mushrooms/yeast
leads to the formation of Vitamin D2
(calciferol).
Biologically inert
Conversion (OH) in the liver and then in
kidneys produces active form .
D2 is less potent than vitamin D3
MW: 396
Types & Sources of Vitamin D
Asclepius
Mushrooms
� Vitamin D3 (Cholecalciferol)Naturally occurring form in humans,
formed by the action of ultraviolet light
(UVB) on Vitamin D precursors in the skin
(7-DHC).
Lanolin is often used as a raw material
for producing vitamin D3.
Present in fish(salmon), other sea food.
Biologically inert
Conversion(OH) in the liver and then in
kidneys produces active form .
MW: 384
Lanolin
A. Haq, 2010

6%3%1%
SUN

Vitamin D3
Vitamin D3 & D2
25(OH)D Prostate,skin, lung, breast,
colon, macrophages,monocytes , other cells
& tissues
Vitamin D Endocrine, Autocrine / ParacrineSystems
1,25(OH)2D
1,25(OH)2D
Calcium homeostasis, muscle health, bone health, neurodevelopment
Immunomodulation, gene transcription, cardiovascular health, & cancer prevention
Haq A et al. (2009) Middle East Laboratory, 12:6-10.
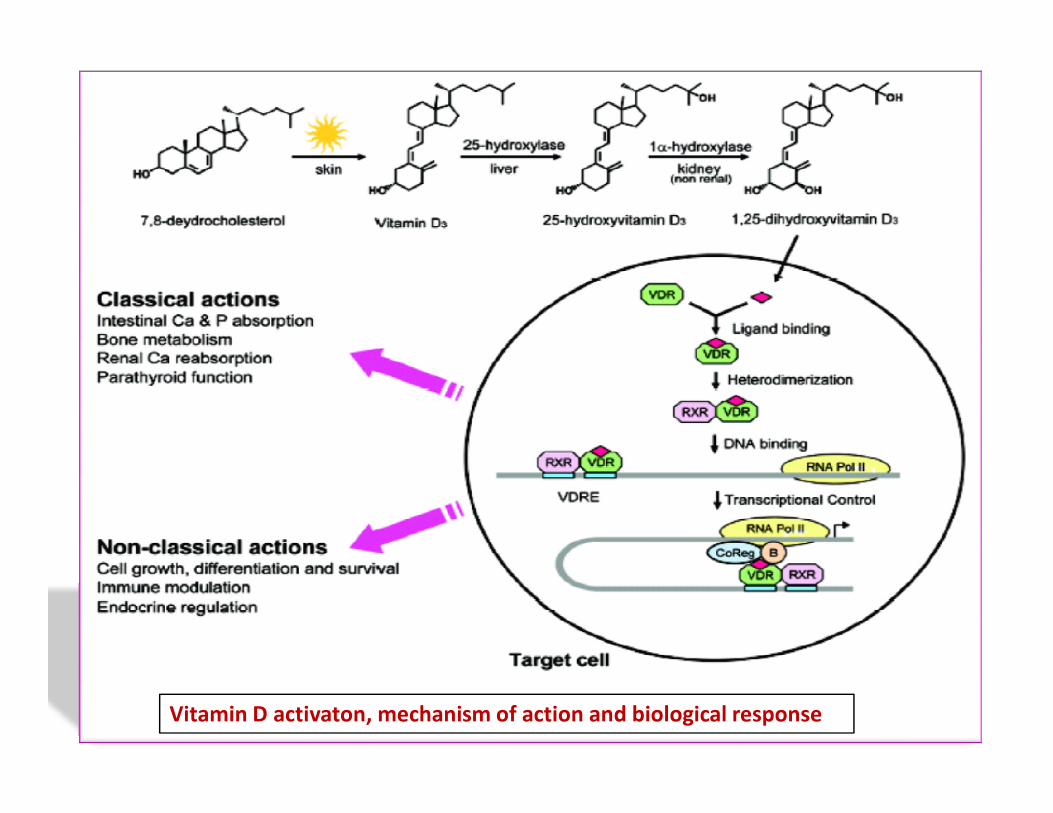
Vitamin D activaton, mechanism of action and biological response

WHY DOES VITAMIN D AFFECT SO MANY
BIOLOGIC PROCESSES?
Vitamin D controls (directly or indirectly) more than 3000 genes that regulate calcium and bone metabolism, modulate innate immunity, control cell growth and maturation, regulate the production of insulin and renin, induce apoptosis and inhibit angiogenesis.
Many tissues are able to make their own 1,25(OH)2D.
�When vitamin D is in short supply, the various tissues and cells of our bodies cannot make enough calcitriolto open up their DNA libraries adequately
Vitamin D Shortage
to open up their DNA libraries adequately
� Their functioning is thus impaired
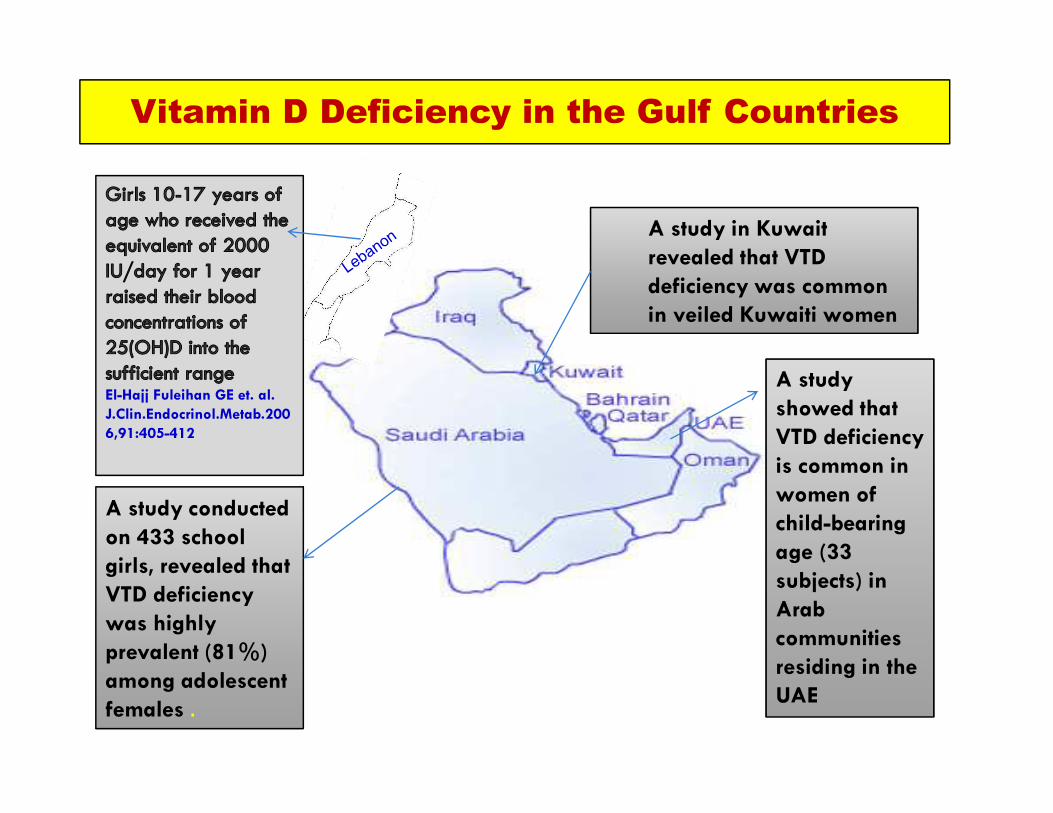
Vitamin D Deficiency in the Gulf Countries
A study in Kuwait
revealed that VTD
deficiency was common
in veiled Kuwaiti women
A study
showed that El-Hajj Fuleihan GE et. al.
J.Clin.Endocrinol.Metab.200
A study conducted
on 433 school
girls, revealed that
VTD deficiency
was highly
prevalent (81%)
among adolescent
females .
showed that
VTD deficiency
is common in
women of
child-bearing
age (33
subjects) in
Arab
communities
residing in the
UAE
J.Clin.Endocrinol.Metab.200
6,91:405-412

The D-lemma: To Screen or Not to
Screen for 25(OH)D Concentrations?
�With the recognition of widespread vitamin D deficiency/insufficiency in children and adults, there is no need to measure everybody's blood 25(OH)D. It would be much more cost-effective to implement a vitamin D supplementation program for all children and adults until there is higher fortification of vitamin D in foods and drinks
Michael F. Holick , Clinical Chemistry, 56:729-731(2010)

Causes and Consequences of Vitamin D
Deficiency
Holick MF, Nat Rev Endocrinol 7: 73-75 (2011)

� Sun exposure obtaining 10 to 15 minutes per day, with 40% of the skin exposed without sunscreen, can help prevent vitamin D deficiency
� Consuming vitamin D rich foods also can help to maintain the beneficial (75 nM) to optimal
Three Ways to Obtain Vitamin D
to maintain the beneficial (75 nM) to optimallevels (90 to150 nM) of 25-hydroxyvitamin D in the blood
� Vitamin D supplementation with vitamin D3(Cholecalciferol) or D2 (get blood levels of 25(OH)D tested first)
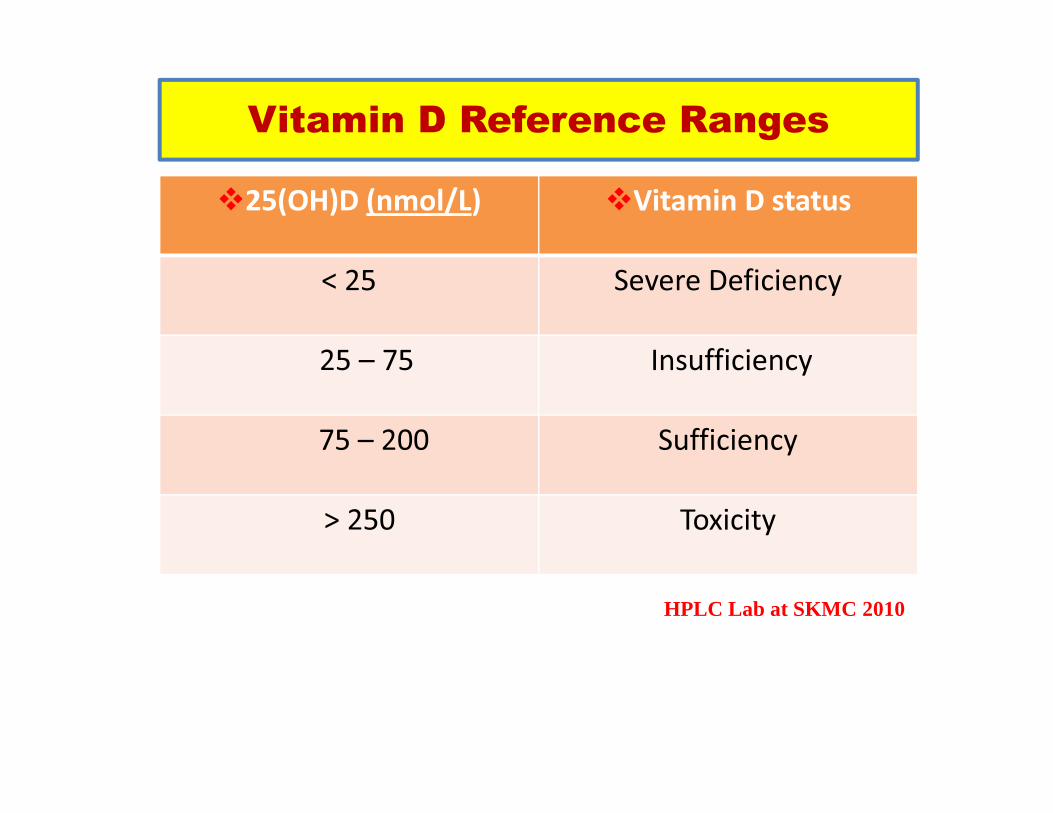
Vitamin D Reference Ranges
�25(OH)D (nmol/L) �Vitamin D status
< 25 Severe Deficiency
25 – 75 Insufficiency
HPLC Lab at SKMC 2010
75 – 200 Sufficiency
> 250 Toxicity

Updated Vitamin D Status
Serum 25(OH)D Vitamin D Clinical/Biochemical (nmol/L) Status Alterations
� < 25 Severely Severely Deficient Deficient Rickets, osteomalacia, myopathy, calcium malabsorption, severe hyperparathyroidism, impaired immune and cardiac function.
� 25 – 49 Deficient Deficient Reduced bone mineral density, impaired muscle function, low intestinal calcium absorption rate, elevated PTH.
Zittermann A et al. Current Opin Clin Nutr & Metabolic Care 2009,12: 634–639
muscle function, low intestinal calcium absorption rate, elevated PTH.
� 50 – 74 Insufficient Insufficient Low bodily stores of 25(OH)D, elevated PTH
� 75 - 374 SufficientSufficient No disturbances of D-dependent functions
� > 375 Toxic Toxic Soft tissue calcification, hypercalcemia

150160
200
150
200
250
25
(OH
)D (
nm
ol/
L)
The Upper Limit of Possible 25(OH)D is
150 - 200 nmol/L
0
50
100
HI/WI Farmers Outdoor
Workers
25
(OH
)D (
nm
ol/
L)Am J Clin Nutr 80,1645-1649, 2004;
J Clin Endocrinol Metab 87,4952- 4956,2002
savannah

Research Project
�Small Scale Study (Target: ZU male/female students) & Larger population based study (Target: Adult Emirati population residing in Abu Dhabi)
Objectives and rationale of the study
�Assess the Prevalence of Vitamin D deficiency among the target population (274/ZU students and 500/general
2nd Biennial Pathology & Laboratory Medicine UpdateMarch 17,18, 2011
the target population (274/ZU students and 500/general population)
� Evaluate the influence of sun avoidance attitude, diet and life style/depression (psychosocial factors) on Vitamin D status

Methodology
�Vitamin D blood testing by HPLC (modified method)
�Sun Avoidance Inventory/Sun Academic Initiative (SAI) to assess attitude towards sun avoidance in (SAI) to assess attitude towards sun avoidance in the context of Vitamin D deficiency
�BDI (Beck Depression Inventory)
� FFQ (Food Consumption and Diet)

Choose an assay that measures both 25(OH)D2 and 25(OH)D3
If using an assay that separates 25(OH)D2 and 25(OH)D3 (i.e. HPLC or LC/MS-MS) indicate the sum of the 2 compounds (25(OH)D2+25(OH)D3) as the main results in your results sheet.
Participate to an external quality control scheme that provides materials with a documented commutability with human sera (e.g. the CAP or the UK based DEQAS)
Requirements for 25(OH)D Assays
An internal quality control program has to be carried out in every laboratory by using different levels samples and valuable criteria for rejecting or accepting “the analytical run“
Do not use population-based reference values (i.e. the concentrations of an apparently healthy population) in addition to a recommended range for 25(OH)D.
We recommend serum as the sample of choice. Express results in nmol/L


Vitamin D Status in the UAE
68
50
60
70
80
of S
tud
en
ts
<25
25-49
274 UAE STUDENTS FROM ZAYED UNIVERSITY
26
51
0
10
20
30
40
<25 25-49 50-75 >75
% o
f S
tud
en
ts
Vitamin D (nmol/L)
25-49
50-75
>75
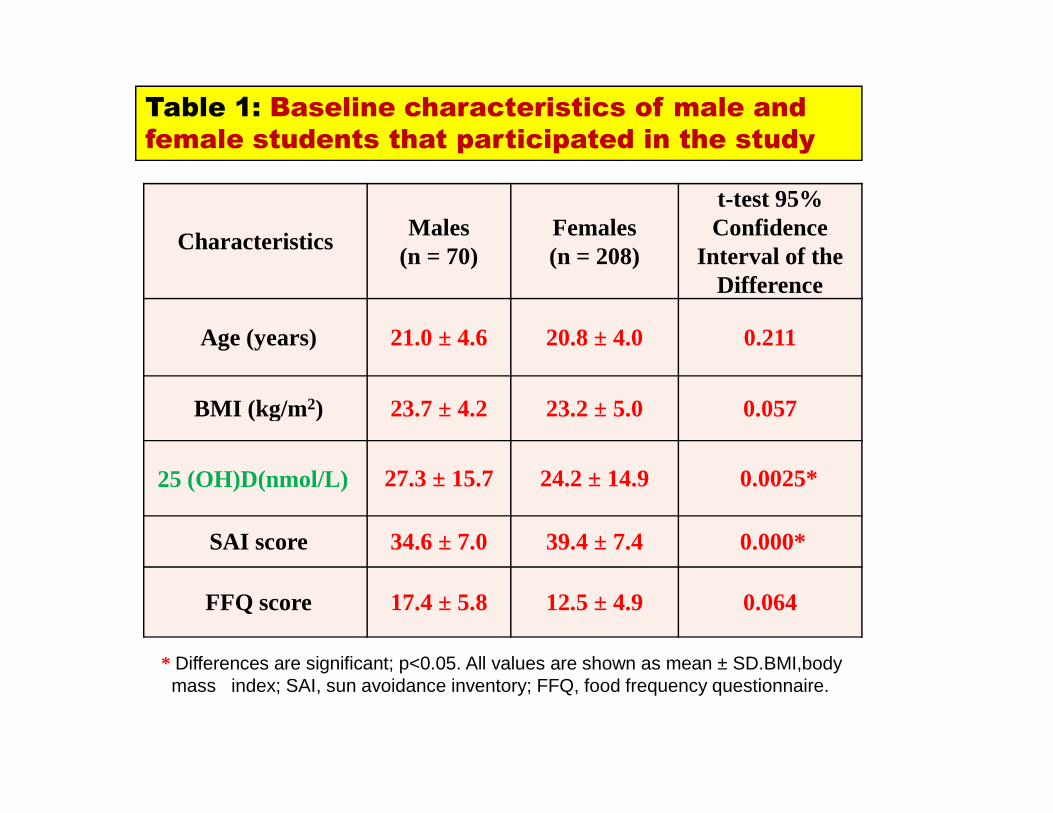
Table 1: Baseline characteristics of male and
female students that participated in the study
CharacteristicsMales
(n = 70)Females(n = 208)
t-test 95% Confidence
Interval of the Difference
Age (years) 21.0 ± 4.6 20.8 ± 4.0 0.211
BMI (kg/m 2) 23.7 ± 4.2 23.2 ± 5.0 0.057
* Differences are significant; p<0.05. All values are shown as mean ± SD.BMI,bodymass index; SAI, sun avoidance inventory; FFQ, food frequency questionnaire.
BMI (kg/m 2) 23.7 ± 4.2 23.2 ± 5.0 0.057
25 (OH)D(nmol/L) 27.3 ± 15.7 24.2 ± 14.9 0.0025*
SAI score 34.6 ± 7.0 39.4 ± 7.4 0.000*
FFQ score 17.4 ± 5.8 12.5 ± 4.9 0.064

Table 2: Baseline characteristics of
female students in summer and winter
CharacteristicsFemales
(summer)(n = 138)
Females(winter)(n = 70)
t-test 95% Confidence
Interval of the Difference
Age (years) 21.1 ± 4.6 20.3 ± 1.9 0.106
BMI (kg/m 2) 22.6 ± 4.6 24.4 ± 5.6 0.30
25 (OH)D(nmol/L) 20.9 ± 14.9 31.3 ± 12.3 0.0005*
SAI score 41.4 ± 7.4 35.1 ± 5.4 0.000*
FFQ score 13.2 ± 5.4 11.0 ± 3.2 0.003
* Differences are significant; p<0.05. All values are shown as mean ± SD., BMI, bodymass index; SAI, sun avoidance inventory; FFQ, food frequency questionnaire.
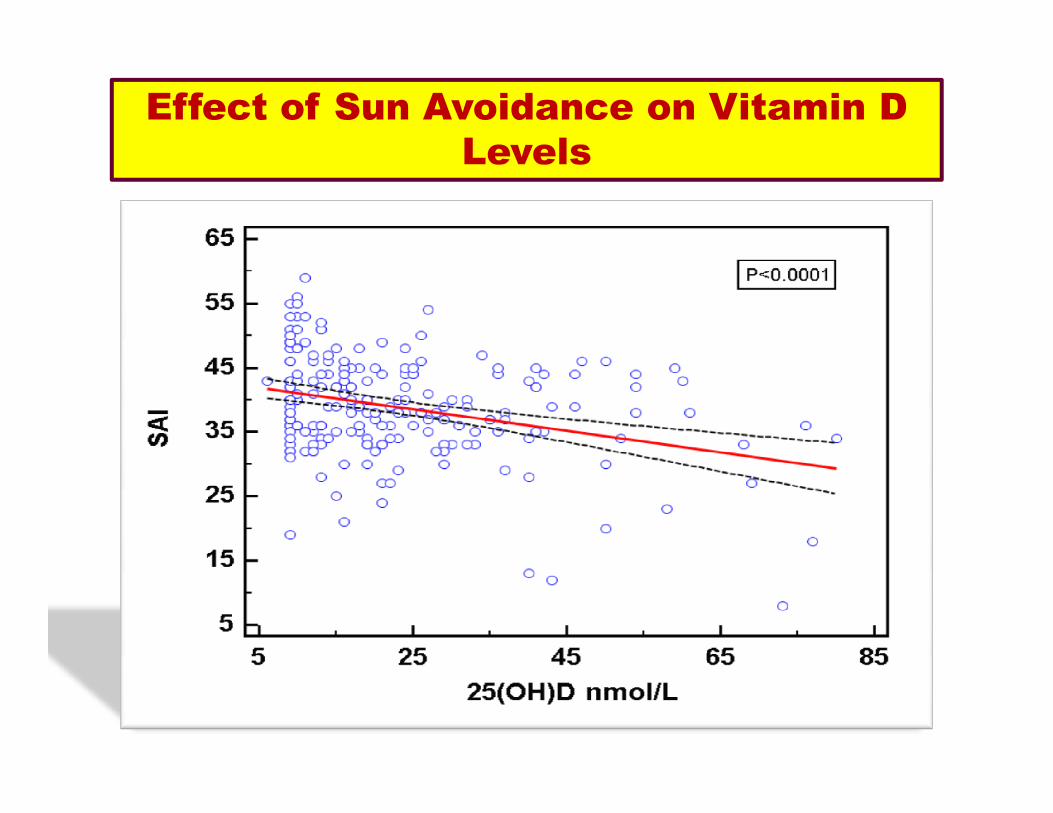
Effect of Sun Avoidance on Vitamin D
Levels


Vitamin D SAI Total BDI-Total Body Mass Index
Vitamin D 1 -0.327** -0.311** 0.030
Significance-1 tailed 0.000 0.000 0.332
n 212 208 211 209
SAI Total -0.327** 1 0.178** 0.099
Significance-1-tailed 000 0.005 0.078
Correlation Between Vitamin D,
SAI, BDI & BMI
Significance-1-tailed 000 0.005 0.078
n 208 208 207 205
BDI Total -0.311** 0.178** 1 -0.005Significance-1 tailed
000 0.005 0.471
n 211 207 211 208
BMI 0.030 0.099 -0.005 1Significance-1 tailed
0.332 0.078 0.471
n 209 205 208 209
** Correlation is significant at the 0.01 level (1-tailed), Pearson Correlation, Significance (1-tailed)

Results
� Significant negative correlation between vitamin D
status and SAI
� Significant negative correlation between vitamin D
status and BDI status and BDI
� Significant positive correlation between BDI
and SAI
X No correlation between vitamin D and FFQ
X No correlation between vitamin D and BMI
Conclusions
� Documents the true picture of Vitamin D deficiency among University students in the UAE
� Guide future intervention studies which would aim at implementing awareness programs to educate people about the beneficial role of Vitamin D (implications from SAI results)SAI results)
� Vitamin D deficiency and insufficiency can be bothcorrected/treated and prevented safely through supplementation, fortification and UVB
� Encourage policy makers to implement a policy in the UAE regarding the need for fortification of drinks and some food items with Vitamin D
Recommendation:
I recommend:
400-1000 IU/day for infants
1000-1500 IU/day for Children 1-10 years
1500-2000 IU/day for teenagers and adults
Michael F. Holick , Clinical Chemistry, 56:729-731(2010)

Treatment Recommendations For Vitamin
D Deficiency
1Tab 1Tab VitaminD3 VitaminD3 50,000 IU50,000 IU/ / monthmonth
Seru
m 2
5(O
H)D
(nm
ol/
L)
90
100
110
Seru
m 2
5(O
H)D
(nm
ol/
L)
90
100
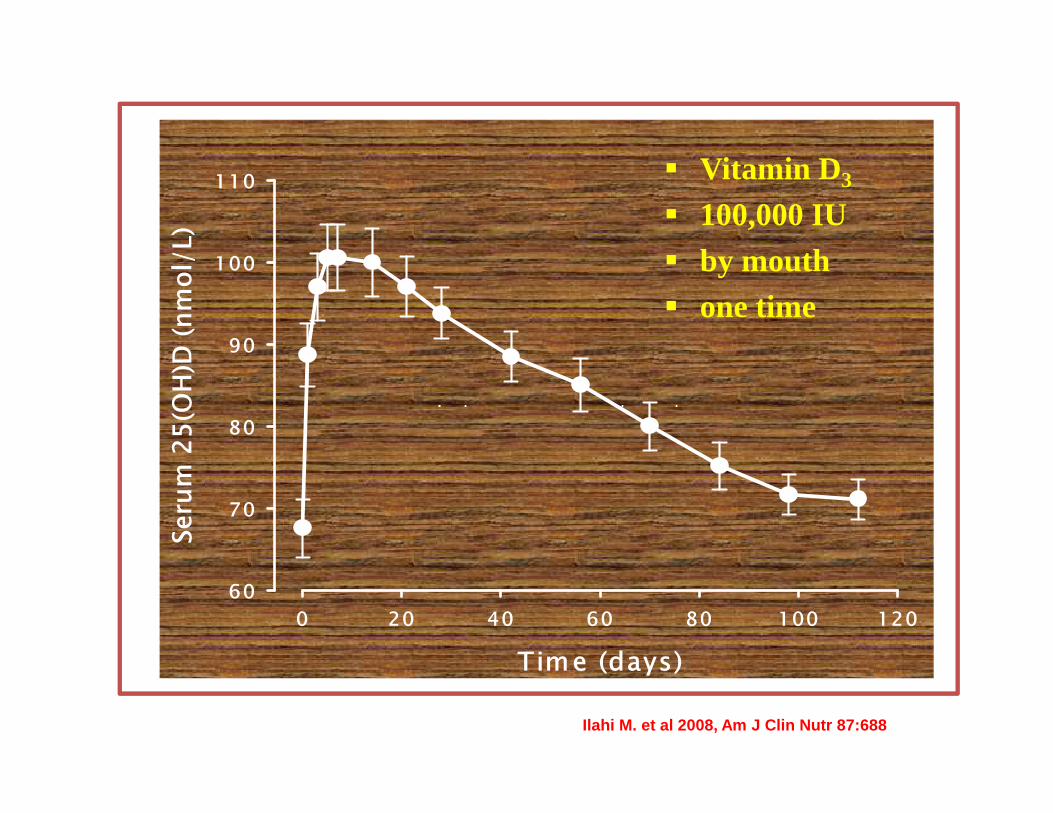
110� Vitamin D 3
� 100,000 IU � by mouth� one time
Time (days)
0 20 40 60 80 100 120
Seru
m 2
5(O
H)D
(nm
ol/
L)
60
70
80
Time (days)
0 20 40 60 80 100 120
Seru
m 2
5(O
H)D
(nm
ol/
L)
60
70
80
Ilahi M. et al 2008, Am J Clin Nutr 87:688
Is Vitamin D Toxic. ?..
� Excessive exposure to sunlight does not lead to overproduction of vitamin D.
� Supplemental vitamin D in certain clinical settings may have toxicity.
� Symptoms are largely hypercalcaemia, high � Symptoms are largely hypercalcaemia, high blood pressure, headache, fatigue, loss of appetite, excessive thrust and polyurea, severe itching, vomiting, diarrhoea, constipation, kidney damage, joints and muscle pain.

Bone 84Calcium 51Osteoporosis 51Kidney 44Renal 28Postmenopausal 25Hyperparathyroidism 20
Chronic Obstructive Pulmonary Disease 7Colon 6Multiple Sclerosis 5Blood Pressure 5Muscle 5Cystic Fibrosis 5Hip 5
1217 Clinical Trials Related to Vitamin D
on Jan 20, 2011
http://clinicaltrials.gov/
Hyperparathyroidism 20Prostate 19Obese 19Breast Cancer 16Fracture 15Diabetes 12HIV 10Elderly 9Tuberculosis 9
Hip 5Rheumatoid Arthritis 5Lung 4Psoriasis 4Lupus 4Crohn's 4Knee 3Heart 9Rickets 7

Outstanding Questions
1. What is the optimal level of vitamin D suppl. and or level of D in the blood to achieve maximal benefits?.
2. Is vitamin D suppl. given orally is equally 2. Is vitamin D suppl. given orally is equally effective to D produced endogenously in the skin?.
3. Do low concentrations of D predispose people to malignancy or inflammatory disease?.

Acknowledgements
� Dr. Fatme Al Anouti
� Dr. Laila Abdel-Wareth� Dr. Jaishen Rajah� Dr. Jaishen Rajah�Mr. Nafiz Nimer
