viral pathogenesis dr. sobia manzoor microbiology & virology ug-7 viral pathogenesis dr. sobia...
TRANSCRIPT
Viral PathogenesisViral PathogenesisDr. Sobia ManzoorDr. Sobia Manzoor
Microbiology & Microbiology & VirologyVirology
UG-7UG-7
Pathogenesis can be describe in 2 ways:Pathogenesis can be describe in 2 ways:
A. Changes within Infected Cell
i. Death (due to inhibition of macromolecular synthesis) ii. Inclusion Bodies (Negri bodies in rabies) iii. Cytopathic Effect (lysis or giant cell formation) iv. Formation of multinucleated cells (fusion of virus infected
cells in herpes & paramyxoviruses) v. Malignant transformation (uncontrolled growth, prolonged
survival, morphological changes) vi. No changes (without morphologic or gross functional
changes, symbiotic relationship)
Process occurs in Process occurs in Infected PatientInfected Patient
Transmission & entry into the host Replication & damage to cells Spread to other cells/organs Immune response Persistence of virus in some instances
STAGES OF TYPICAL VIRAL STAGES OF TYPICAL VIRAL INFECTIONINFECTION
Incubation Period (asymptomatic) Prodromal Period (nonspecific symptoms) Specific illness Period (specific symptoms) Recovery Period (regains good health)

Causes of Persistent viral Causes of Persistent viral InfectionInfection
Integration of viral DNA into host genome Immune tolerance Formation of Viral-Antibody Complex Location within Immunologically sheltered Rapid Antigen variation Spread from cell to cell without an extra cellular
phase Immunosuppression
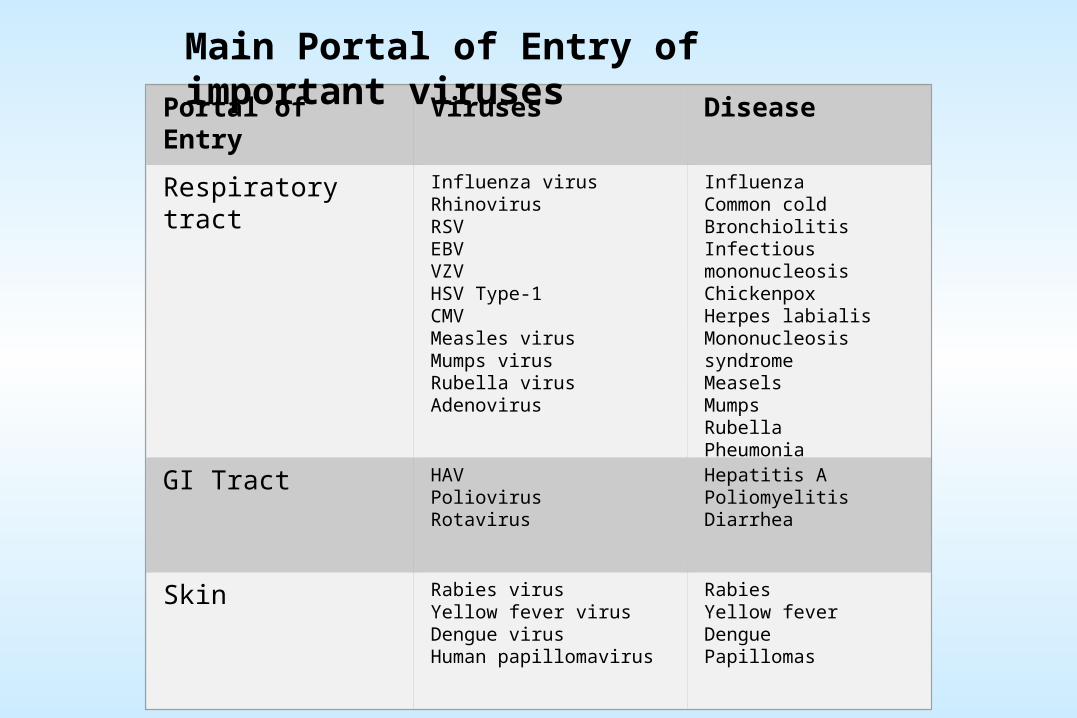
Portal of Entry Viruses Disease
Respiratory tract Influenza virusRhinovirusRSVEBVVZVHSV Type-1CMVMeasles virusMumps virusRubella virusAdenovirus
InfluenzaCommon coldBronchiolitisInfectious mononucleosisChickenpoxHerpes labialisMononucleosis syndromeMeaselsMumpsRubellaPheumonia
GI Tract HAVPoliovirusRotavirus
Hepatitis APoliomyelitisDiarrhea
Skin Rabies virusYellow fever virusDengue virus Human papillomavirus
Rabies Yellow fever Dengue Papillomas
Main Portal of Entry of important viruses

Genital tract HPVHBVHIVHSV Type-2
WartsHepatitis BAIDSHerpes genitalis
Blood HBVHCVHDVHTCLVHIVCMV
Hepatitis BHepatitis CHepatitis DLeukemiaAIDSMononucleosis syndrome
Transplacental CMVRubella virus
Congenital abnormalitiesCongenital abnormalities
Main Portal of Entry of important viruses (Contd….)
Portal of Entry Viruses Disease
TYPES OF PERSISTANT VIRAL INFECTIONSTYPES OF PERSISTANT VIRAL INFECTIONS 1. Chronic Carrier Infections:
•Infected patients continue to produce significant amount of the virus for long period (carrier state)
•Followed by asymptomatic or chronic illness
•Clinical example is chronic hepatitis, rubella & CMV infections.
2. Latent Infections:
•Patient recovers from initial infection
•Symptoms recur along with viral production
•Clinical examples HSV, VZV infections
Slow Virus Infections:
Prolong period between the initial infection and the onset of disease.
Caused by conventional viruses such as JC viruses (John Cunningham VIRUS) (PML), measles viruses (SSPE), HIV (AIDS) & unconventional agents such as Prions (Kuru, CJD, Scrapie, Visna, BSE).
PML:Progressive Multifocal Leukoencephalopathy SSPE: Subacute Sclerosing Panencephalitis CJD: Creutzfeldt-Jakob Disease, BSE: Bovine Spongiform Encephalopathy
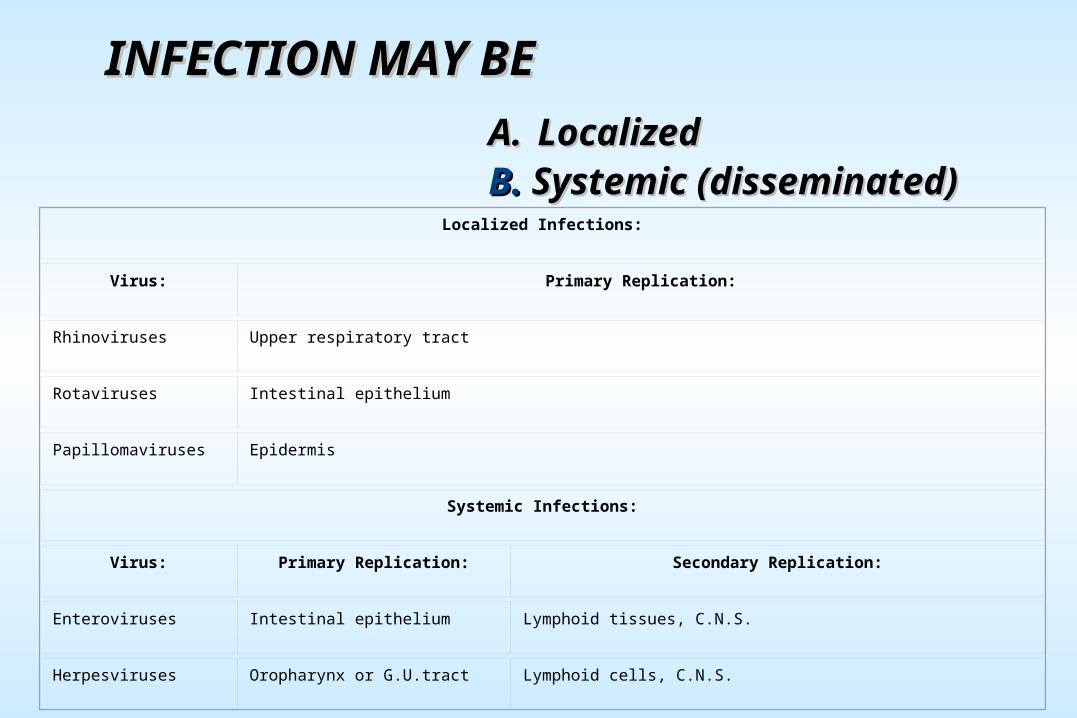
INFECTION MAY BEINFECTION MAY BE A.A. LocalizedLocalizedB.B. Systemic (disseminated)Systemic (disseminated)
Localized Infections:
Virus: Primary Replication:
Rhinoviruses Upper respiratory tract
Rotaviruses Intestinal epithelium
Papillomaviruses Epidermis
Systemic Infections:
Virus: Primary Replication: Secondary Replication:
Enteroviruses Intestinal epithelium Lymphoid tissues, C.N.S.
Herpesviruses Oropharynx or G.U.tract Lymphoid cells, C.N.S.
VIRAL PATHOGENESIS
Results from:
Transmission to a new host
Replication and spread within the host(a function of viral tropism)
Cell damage and dysfunction(can be mediated by the virus or by immune defense mechanisms)
Disease symptoms and abnormal laboratory test values
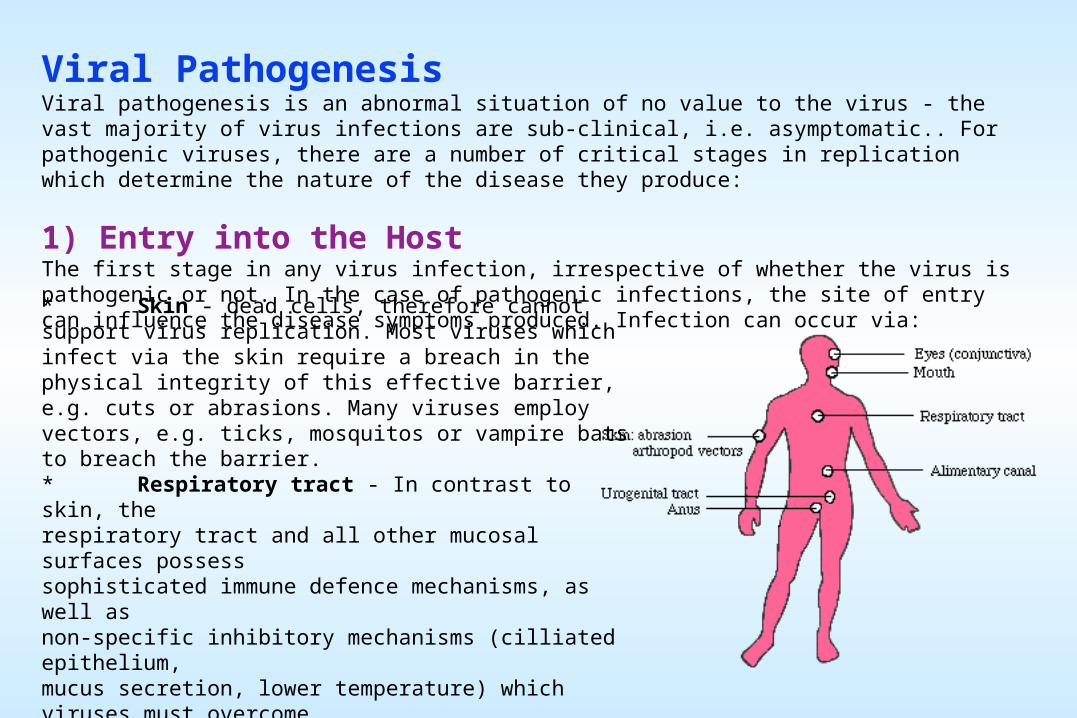
Viral PathogenesisViral pathogenesis is an abnormal situation of no value to the virus - the vast majority of virus infections are sub-clinical, i.e. asymptomatic.. For pathogenic viruses, there are a number of critical stages in replication which determine the nature of the disease they produce:
1) Entry into the HostThe first stage in any virus infection, irrespective of whether the virus is pathogenic or not. In the case of pathogenic infections, the site of entry can influence the disease symptoms produced. Infection can occur via:
* Skin - dead cells, therefore cannot support virus replication. Most viruses which infect via the skin require a breach in the physical integrity of this effective barrier, e.g. cuts or abrasions. Many viruses employ vectors, e.g. ticks, mosquitos or vampire bats to breach the barrier. * Respiratory tract - In contrast to skin, the respiratory tract and all other mucosal surfaces possess sophisticated immune defence mechanisms, as well as non-specific inhibitory mechanisms (cilliated epithelium, mucus secretion, lower temperature) which viruses must overcome. * Gastrointestinal tract - a hostile environment; gastric acid, bile salts, etc * Genitourinary tract - relatively less hostile than the above, but less frequently exposed to extraneous viruses (?) * Conjunctiva - an exposed site and relatively unprotected
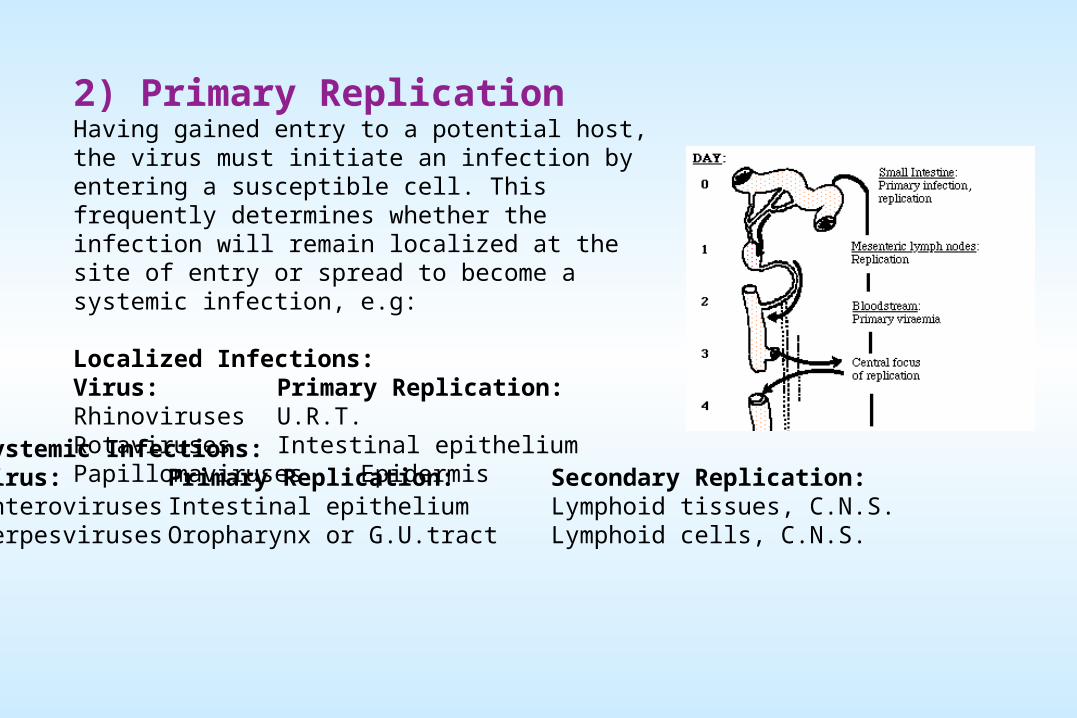
2) Primary ReplicationHaving gained entry to a potential host, the virus must initiate an infection by entering a susceptible cell. This frequently determines whether the infection will remain localized at the site of entry or spread to become a systemic infection, e.g:
Localized Infections:Virus: Primary Replication:Rhinoviruses U.R.T.Rotaviruses Intestinal epitheliumPapillomaviruses Epidermis
Systemic Infections:Virus: Primary Replication: Secondary Replication:Enteroviruses Intestinal epithelium Lymphoid tissues, C.N.S.Herpesviruses Oropharynx or G.U.tract Lymphoid cells, C.N.S.
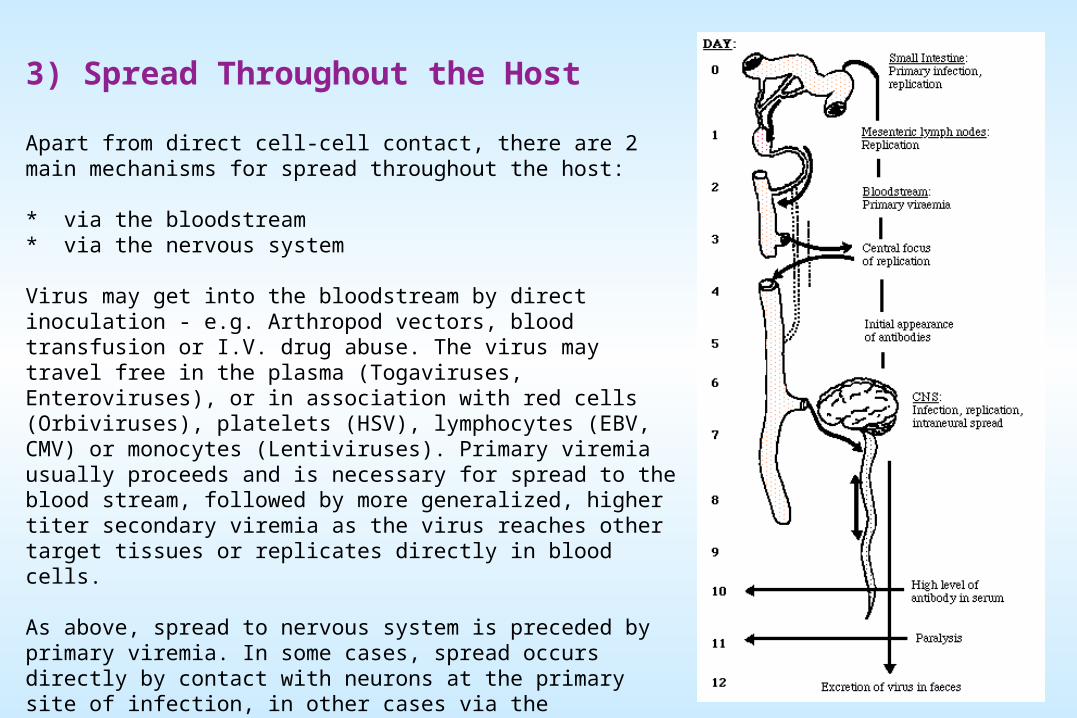
3) Spread Throughout the Host
Apart from direct cell-cell contact, there are 2 main mechanisms for spread throughout the host:
* via the bloodstream * via the nervous system
Virus may get into the bloodstream by direct inoculation - e.g. Arthropod vectors, blood transfusion or I.V. drug abuse. The virus may travel free in the plasma (Togaviruses, Enteroviruses), or in association with red cells (Orbiviruses), platelets (HSV), lymphocytes (EBV, CMV) or monocytes (Lentiviruses). Primary viremia usually proceeds and is necessary for spread to the blood stream, followed by more generalized, higher titer secondary viremia as the virus reaches other target tissues or replicates directly in blood cells.
As above, spread to nervous system is preceded by primary viremia. In some cases, spread occurs directly by contact with neurons at the primary site of infection, in other cases via the bloodstream. Once in peripheral nerves, the virus can spread to the CNS by axonal transport along neurons (classic - HSV). Viruses can cross synaptic junctions since these frequently contain virus receptors, allowing the virus to jump from one cell to another.
4) Cell/Tissue DamageViruses may replicate widely throughout the body without any disease symptoms if they do not cause significant cell damage or death.
Retroviruses do not generally cause cell death, being released from the cell by budding rather than by cell lysis, and cause persistent infections, even being passed vertically to offspring if they infect the germ line.
Conversely, Picornaviruses cause lysis and death of the cells in which they replicate, leading to fever and increased mucus secretion in the case of Rhinoviruses, paralysis or death (usually due to respiratory failure) for Poliovirus.
5) Cell/Tissue TropismTropism - the ability of a virus to replicate in particular cells or tissues - is controlled partly by the route of infection but largely by the interaction of a virus attachment protein (V.A.P.) with a specific receptor molecule on the surface of a cell, and has considerable effect on pathogenesis. Many V.A.P.'s and virus receptors are now known.
6) Persistence vs. ClearanceThe eventual outcome of any virus infection depends on a balance between two processes:
i) Persistence:Long term persistence of virus results from two main mechanisms:
a) Regulation of lytic potentialThe strategy followed is the continued survival of a critical number of virus infected cells - sufficient to continue the infection without killing the host.
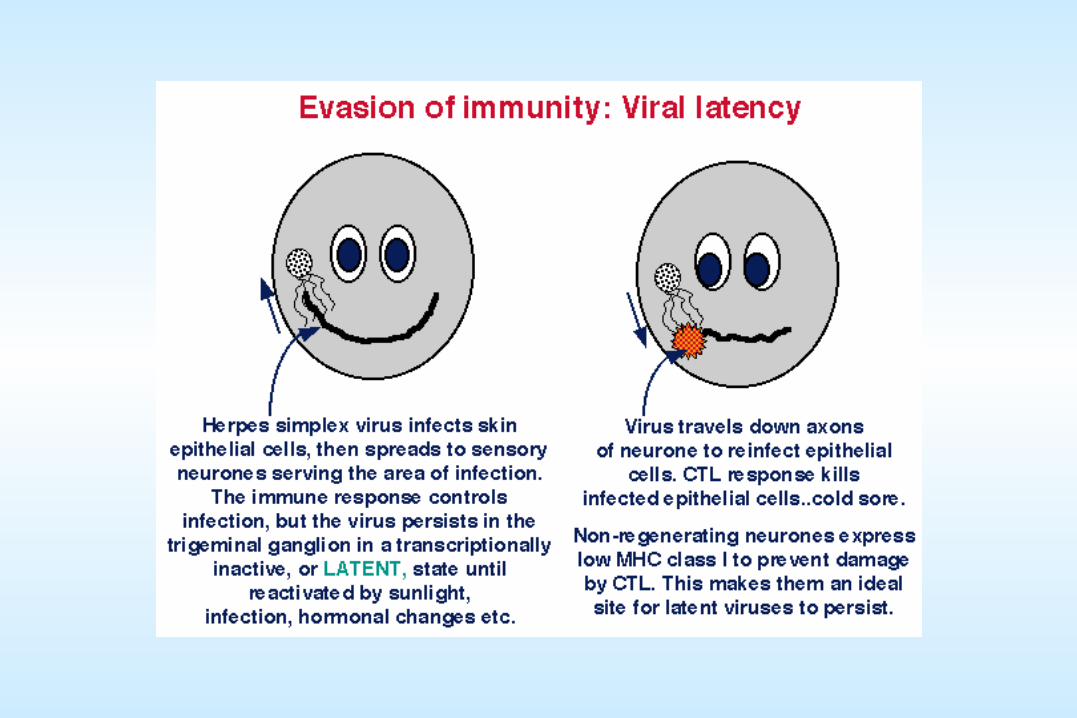
* For viruses which do not usually kill the cells in which they replicate, this is not usually a problem, hence these viruses tend naturally to cause persistent infections, e.g. Retroviruses. * For viruses which undergo lytic infection, e.g. Herpesviruses, it is necessary to develop mechanisms which restrict virus gene expression, and consequently, cell damage.
b) Evasion of immune surveillance - Includes:
* antigenic variation * immune tolerance, causing a reduced response to an antigen, may be due to genetic factors, pre-natal infection, * restricted gene expression * down-regulation of MHC class I expression, resulting in lack of recognition of infected cells e.g. Adenoviruses * down-regulation of accessory molecules involved in immune recognition e.g. LFA-3 and ICAM-1 by EBV. * infection of immunocompromised sites within the body e.g. HSV in sensory ganglia in the CNS * direct infection of the cells of the immune system itself e.g. Herpes viruses, Retroviruses (HIV) - often resulting in immunosuppression.
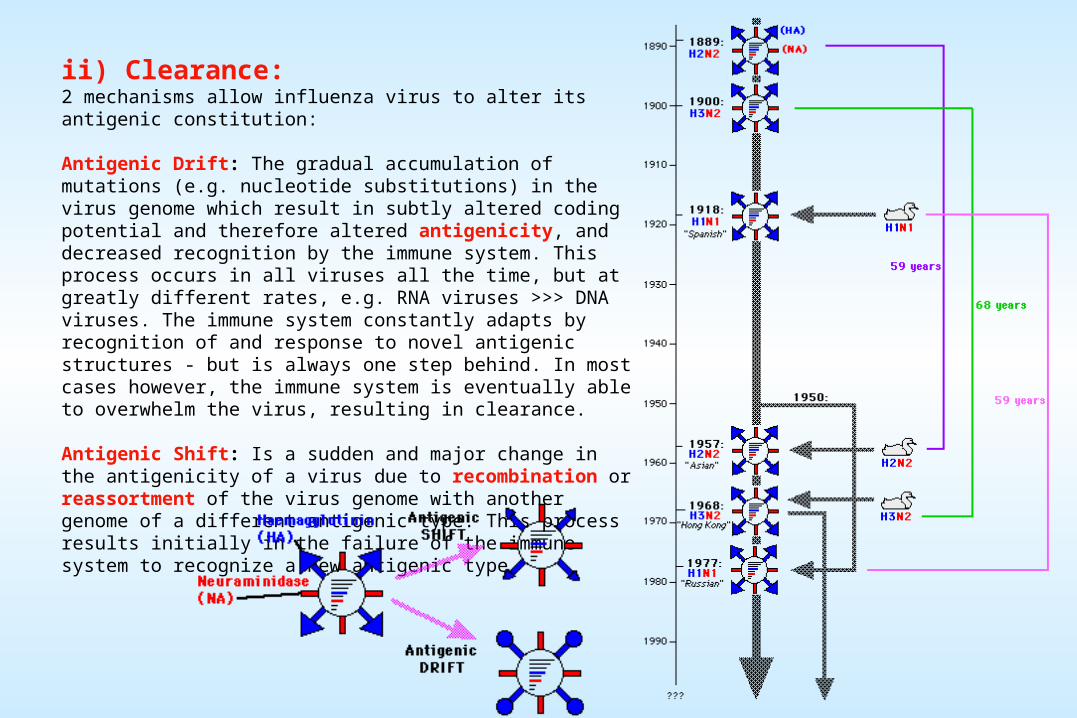
ii) Clearance:2 mechanisms allow influenza virus to alter its antigenic constitution:
Antigenic Drift: The gradual accumulation of mutations (e.g. nucleotide substitutions) in the virus genome which result in subtly altered coding potential and therefore altered antigenicity, and decreased recognition by the immune system. This process occurs in all viruses all the time, but at greatly different rates, e.g. RNA viruses >>> DNA viruses. The immune system constantly adapts by recognition of and response to novel antigenic structures - but is always one step behind. In most cases however, the immune system is eventually able to overwhelm the virus, resulting in clearance.
Antigenic Shift: Is a sudden and major change in the antigenicity of a virus due to recombination or reassortment of the virus genome with another genome of a different antigenic type. This process results initially in the failure of the immune system to recognize a new antigenic type.
Determinants of cell damage and dysfunction
1. Direct destruction of cells by virusPoliovirus - poliomyelitis Herpes simplex - cold soresRotavirus - diarrhea HIV - AIDS
2. Immune mediated destruction of virus-infected cells (CTL and Ab)Hepatitis B - hepatitis Dengue - Dengue shockMeasles - post-measles encephalitis & SSPE
3. Indirect effector mechanismsInfluenza - interleukins and interferons releasedRhinovirus - kinin release, vascular changesRespiratory syncytial - IgE Ab-mediated effectsHepatitis B and C - Ab:Ag complex deposition
4. Virus-encoded immune alterationAdenovirus - E3 alters class I MHC expressionVaccinia (and other poxviruses) - TNF analogueEpstein-Barr - Interleukin 10
5. Allow access to other pathogens
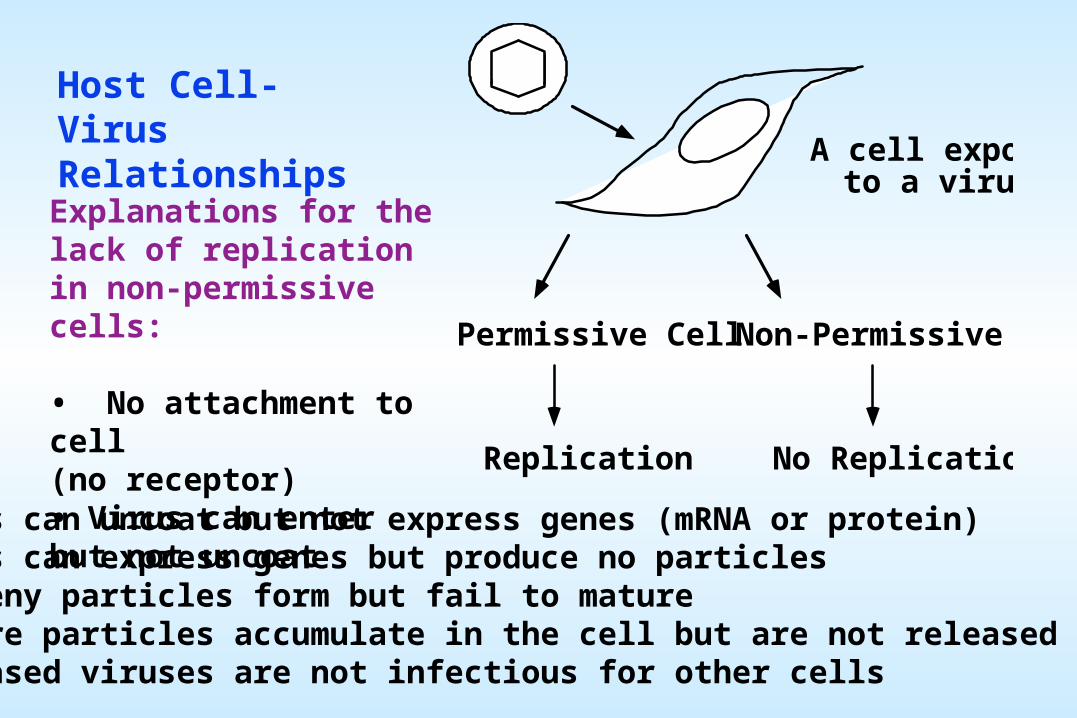
A cell exposedto a virus
Permissive Cell Non-Permissive Cell
Replication No Replication
Host Cell-Virus Relationships
Explanations for the lack of replication in non-permissive cells:
• No attachment to cell(no receptor)• Virus can enter but not uncoat• Virus can uncoat but not express genes (mRNA or protein)• Virus can express genes but produce no particles• Progeny particles form but fail to mature• Mature particles accumulate in the cell but are not released• Released viruses are not infectious for other cells
LATENCY
When virus infection fails to result in an immediate production of progeny. Rather, the virus enters a latent state in which the viral genome may become incorporated into the host's genome or maintained as an extrachromosomal element.
Latent viral genomes are passively replicated along with host chromosomes. Not all viral genes remain silent during latency and there may be a perceptible change in the phenotype of the cell. The viral genome may become reactivated, potentially up to decades after the initial infection.
Herpes, papilloma, Hepadnaviruses: Latent forms exist as plasmids (nuclear, extrachromosomal element)
Virus: Site of latent infection:Herpes simplex - sensory neuronsVaricella-zoster - dorsal root ganglionEpstein-Barr - B lymphocytesPapilloma - basal epitheliume.g. Development of "cold sores" by herpes viruses after the host is exposed to large doses of unfiltered sunlight.
Retroviruses:Latent forms exist as "proviruses" integrated into the host chromosome
HTLV 1 - T cellsHIV - CD4+ T cells, macrophages
Latency can be associated with tumorigenic transformation of the cell. Infrequently, latent viral nucleic acid may be passed not only to the progeny of the cells within the host, but also through successive generations in the germ line.
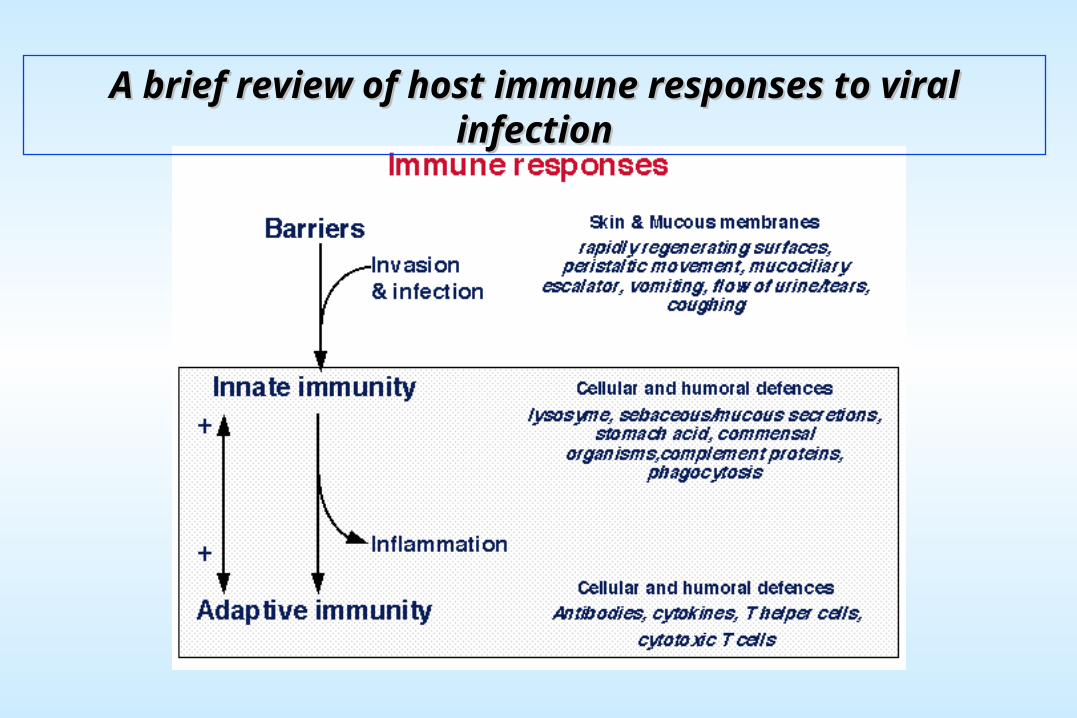
A brief review of host immune responses to viral infectionA brief review of host immune responses to viral infection