vi.2 elements for a public summary - lægemiddelstyrelsen 28104976211...this disease incidence and,...
TRANSCRIPT
VI.2 Elements for a Public Summary
VI.2.1 Overview of disease epidemiology
Pertussis Epidemiology
Pertussis (whooping cough) is caused by Bordetella pertussis bacteria, and is an easily spread respiratory tract illness. In 2015, a total of 123210 cases of pertussis cases were reported worldwide with the highest incidence seen in infants and young children. Immunisation of infants against pertussis has greatly reduced the number of infants and young children contracting the illness. However, despite a huge reduction in cases
96

compared to the pre-vaccination era cases have recently begun to increase, and is affecting adolescents and adults in addition to the very young. This is considered to be due to a variety of reasons, particularly that protection against the disease after either natural infection or vaccination is not long lasting, and that doctors and patients are now much more aware of pertussis disease with ability to test for and confirm the illness much improved. In April 2012 the US health authorities declared a pertussis epidemic in response to the increase in pertussis cases being observed. However, despite high uptake of the adolescent booster vaccine (Tdap), pertussis continued to occur in this age group suggesting protection was not long lasting.. Other countries that have also reported outbreaks of pertussis are Australia, UK, New Zealand, Netherlands and some states of Germany.
Tetanus Epidemiology
Tetanus is an infection caused by the bacterium Clostridium tetani. It occurs worldwide and is more common in agricultural regions and areas where contact with soil or animal waste is more likely and immunisation is inadequate. In 2015, a total of 10301 cases of tetanus were reported worldwide. The highest numbers of cases were reported in the African and South-East Asian WHO regions, areas with the lowest numbers of vaccinated people. The widespread use of tetanus toxoid-containing vaccines in pregnant women has resulted in a dramatic reduction in the worldwide number of newborns who suffer from tetanus. In countries with effective vaccination programmes and good standards of hygiene, cases of tetanus in mothers and newborns are very rare with <1 occurring per 1000 live births. Furthermore, in 2015, only 3551 cases of tetanus in newborns were reported, compared with 25 293 cases in 1990.
Whilst vaccination has been used very successfully to protect against the disease, it does not result in lifelong protection. Therefore, booster vaccinations throughout life are important to maintain adequate levels of immunity. A number of countries, including Argentina, Canada, Germany and Portugal, recommend a dT booster dose every 10 years. In addition, natural infection with Clostridium tetani does not lead to immunity afterwards, requiring the vaccination of all survivors of the disease.
Diphtheria Epidemiology
Diphtheria is an infection caused by Corynebacterium diphtheria. It is found worldwide, with 4778 cases reported globally in 2015. The highest number of cases is reported in India (2365). Between 1980 and 2015, India had continuously high numbers of diphtheria cases, with little decline over years. The majority of cases are found in children who are either partially or not vaccinated against the disease. Elsewhere, vaccination programmes have been successful in helping to control diphtheria. Between 1980 and 2015, the total number of reported diphtheria cases worldwide fell by >90%, from 97,511 cases in 1980 to 4778 cases in 2015.
Nevertheless, diphtheria outbreaks still persist. The main causes are the high number of individuals with low levels of immunity (due to incomplete childhood vaccinations and a lack of booster doses), the appearance of a new strain of C. diphtheriae, and poor social conditions (including increased numbers of migrants, crowded living conditions and poor access to healthcare).
CONFIDENTIAL
97

Poliomyelitis Epidemiology
Poliomyelitis used to cause paralysis and permanent physical disability in thousands of children every year. The introduction of effective vaccines in the late 1950s (inactivated poliovirus vaccine- IPV) and early 1960s (oral poliovirus vaccine - OPV) greatly reduced this disease incidence and, following the implementation of the Global Polio Eradication Initiative (GPEI) in 1988, poliomyelitis cases further declined and became extremely rare(414 cases in 2015). However, sporadic cases still continue to occur in a small number of countries where there is reduced access to healthcare and immunization, particularly those in conflict zones.
Consequently, the potential for imported poliovirus to cause outbreaks and possibly re-establish transmission in countries which were previously polio-free remains a threat until global eradication of polio is achieved, with immunization needing to be maintained. Today, poliomyelitis remains endemic in Pakistan, Afghanistan and Nigeria.
VI.2.2 Summary of treatment benefits
Vaccination with the Boostrix Polio (Tdap-IPV) vaccine results in teaching the immune system in defending to each of the components of the vaccine. A booster dose of Boostrix Polio will enhance protection against diphtheria, tetanus, poliomyelitis, and pertussis disease. Boostrix Polio is to be used for booster vaccination against diphtheria, tetanus, poliomyelitis and pertussis in individuals from the age of four years onwards. Boostrix Polio may be administered to adolescents and adults with unknown vaccination status or incomplete vaccination against diphtheria, tetanus and pertussis as part of an initial immunisation series against diphtheria, tetanus, pertussis and poliomyelitis (Annex 2). The variation to sections 4.2 and 4.6 of the EU SmPC proposed by the Company has beenaccepted and it reads as follow:
Section 4.2 of the EU SmPC (Annex 2):
The use of Boostrix Polio may be considered during the third trimester of pregnancy. For the use of the vaccine before the third trimester of pregnancy, see section 4.6.
Section 4.6 of the EU SmPC (Annex 2):
Safety data from a prospective observational study where Boostrix (dTpa component of Boostrix Polio) was administered to pregnant women during the third trimester (793 pregnancy outcomes) as well as data from passive surveillance where pregnant women were exposed to Boostrix Polio or to Boostrix in the 3rd and 2nd trimester have shown no vaccine related adverse effect on pregnancy or on the health of the foetus/newborn child.
The use of Boostrix Polio may be considered during the third trimester of pregnancy.
Human data from prospective clinical studies on the use of Boostrix Polio during the first and second trimester of pregnancy are not available. However, as with other inactivated vaccines, it is not expected that vaccination with Boostrix Polio harms the
CONFIDENTIAL
98

foetus at any trimester of pregnancy. The benefits versus the risks of administering Boostrix during pregnancy should be carefully evaluated.
Animal studies do not indicate direct or indirect harmful effects with respect to pregnancy, embryonal/foetal development, parturition or post-natal development (see section 5.3).
Limited data indicate that maternal antibodies may reduce the magnitude of the immune response to some vaccines in infants born from mothers vaccinated with Boostrix Polio during pregnancy. The clinical relevance of this observation is unknown.
In addition, the company recently proposed the following wording to be included in the product information (EU SmPC) for Boostrix Polio (Annex 2 bis):
Section 4.2 of the EU SmPC:
Boostrix Polio may be administered from the age of three years onwards.Section 4.5 of the EU SmPC:
Boostrix Polio may be administered concomitantly with any of the following monovalent or combination vaccines: measles, mumps, rubella, varicella and human papilloma virus vaccine with no clinically relevant interference with antibody response to any of the components of either vaccine (section 4.8).
The protection against these four diseases has greatly reduced the number of people with tetanus, poliomyelitis, diphtheria and pertussis. For pertussis, vaccination remains as the only protection against the disease. The focus of prevention and control efforts is the protection of infants and others at greatest risk for severe disease and increasing the number of immunized adolescents and adults, with a special focus on pregnant women. Pertussis vaccination remains the single most effective way to prevent infection.
Vaccination against tetanus has been important worldwide, as the number of newborns who get tetanus has been greatly reduced. In countries where there are not adequate places for women to give birth or they give birth at home with non-sterile tools, these are risk factors for the newborn to develop tetanus infection. Booster vaccination against tetanus should be given every ten years, and this has reduced the number of cases of tetanus worldwide.
Diphtheria is a serious disease that can cause severe difficulty in breathing and, in some cases, death. In the last twenty years, only through vaccination, it has been possible to reduce the number of cases worldwide by more than 80% .Booster vaccination programs need to be started and maintained to control this disease.
Poliomyelitis is a serious disease that can produce permanent paralysis and death. It is imperative to have all children vaccinated against poliomyelitis, as this disease can be out of control if there is no appropriate vaccine coverage. Countries who have reduced their vaccination coverage in recent years, have had serious poliomyelitis outbreaks, affecting younger children overall.
CONFIDENTIAL
99

VI.2.3 Unknowns relating to treatment benefits
Boostrix Polio has not been extensively studied in pregnant women, breastfeeding women, and children less than four years old. These particular groups of people have been part of very limited clinical trials up till the DLP. Boostrix Polio is not meant to be used for primary immunisation in infants. Recent pertussis outbreaks in the United States, United Kingdom, Australia, New Zealand, and other countries, have led to pregnant woman being now vaccinated in order to protect their infants. This will also be reflected accordingly within Boostrix Polio leaflet. Tests on animals’ suggest that there is no safety concern in providing Boostrix or Boostrix Polio during pregnancy. GSK is continuously monitoring adverse events and outcomes of pregnant woman who received Tdap vaccine to better understand the safety of the vaccine. Additionally, the results of study dTpa-IPV-009 (111763) demonstrate that Boostrix Polio, when given as a booster dose co-administered with MMR vaccine (Priorix) to children of 3 to 4 years of age, can confer an immune response in children 3 years onwards that is as effective as the currently authorized vaccines (see Annex 12).
VI.2.4 Summary of safety concerns
Important identified risks: None
Important potential risks
Risk What is known (Including reason why it is considered a potential risk)
Possible immune interference in babies born from mothers vaccinated with Boostrix and Boostrix Polio during pregnancy.
Limited data on the safety or immunogenicity of Boostrix line vaccines during pregnancy or lactation are available. Maternal antibodies mounted in response to Boostrix vaccines shot may later on reduce the immune response to some vaccines in infants born from mothers vaccinated with Boostrix vaccinesduring pregnancy. The potential consequences of this observation are unknown at present.
Missing information
Risk What is knownTdap waning of immunity Due to the sharing of antigens between Boostrix and Boostrix
Polio, the following information is also relevant to consider for Boostrix Polio: data with the Boostrix formulation licensed in US, containing less adjuvant as compared to the formulation registered in Europe, indicate that Boostrix has a moderate protection in the first year postvaccination, and the protection wanes considerably from the second year (this was observed in the last pertussis epidemic in the US).
CONFIDENTIAL
100

Risk What is knownLimited information on the use of Boostrix and Boostrix Polio in pregnant women
Limited data on the safety or immunogenicity of Boostrix and Boostrix Polio during pregnancy or lactation are available. It is generally accepted that inactivated vaccines pose no risk to the pregnant or lactating women and their child.
VI.2.5 Summary of additional risk minimisation measures by safety concern
All medicines have a Summary of Product Characteristics (SmPC) which provides physicians, pharmacists and other health care professionals with details on how to use the medicine, the risks and recommendations for minimising them. An abbreviated version of this in lay language is provided in the form of the package leaflet (PL). The measures in these documents are known as routine risk minimisation measures.
The latest approved version of the Summary of Product Characteristics and the Package leaflet for Boostrix Polio can be found in the Annex 2. Included as well, is the proposed SmPC for the ongoing labelling variation for Boostrix Polio (age lowering & co-administration with MMR/V vaccine) as Annex 2bis.
There are no additional risk minimisation measures specifically developed for Boostrix Polio only. Pharmacovigilance activities such as clinical studies on the use of Boostrix in pregnancy and close monitoring of spontaneous cases in pregnant women exposed to Boostrix are already described in the Boostrix Risk Management Plan. Careful and immediate evaluation of spontaneous cases and new literature data when available is ensured.
VI.2.6 Planned post authorisation development plan
Not applicable with only Boostrix Polio. As mentioned there are epidemiological and clinical studies recently proposed with Boostrix that will provide additional safety information of the impact of acellular pertussis antigen used in pregnancy as nowadays, Boostrix line vaccines are being recommended during pregnancy.
There are currently no Boostrix Polio studies which are specific obligations and/or conditions of the MA. All the other clinical studies with Boostrix Polio are already concluded at data lock point of this report. Study 111763 [DTPA-IPV (BOOSTRIX-IPV)-009], as presented below in the table, has been recently completed.
CONFIDENTIAL
101
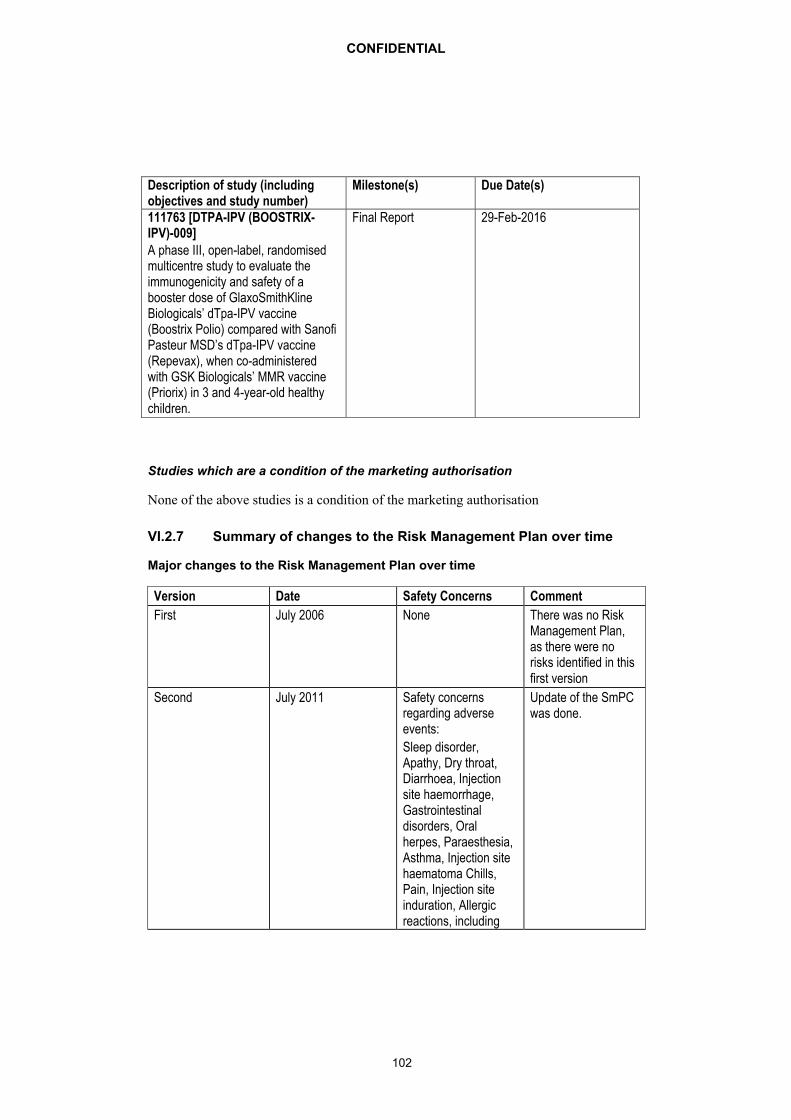
Description of study (including objectives and study number)
Milestone(s) Due Date(s)
111763 [DTPA-IPV (BOOSTRIX-IPV)-009]A phase III, open-label, randomised multicentre study to evaluate the immunogenicity and safety of a booster dose of GlaxoSmithKline Biologicals’ dTpa-IPV vaccine (Boostrix Polio) compared with Sanofi Pasteur MSD’s dTpa-IPV vaccine (Repevax), when co-administered with GSK Biologicals’ MMR vaccine (Priorix) in 3 and 4-year-old healthy children.
Final Report 29-Feb-2016
Studies which are a condition of the marketing authorisation
None of the above studies is a condition of the marketing authorisation
VI.2.7 Summary of changes to the Risk Management Plan over time
Major changes to the Risk Management Plan over time
Version Date Safety Concerns Comment
First July 2006 None There was no Risk Management Plan, as there were no risks identified in this first version
Second July 2011 Safety concerns regarding adverse events:
Sleep disorder,Apathy, Dry throat, Diarrhoea, Injection site haemorrhage, Gastrointestinal disorders, Oral herpes, Paraesthesia, Asthma, Injection site haematoma Chills, Pain, Injection site induration, Allergic reactions, including
Update of the SmPC was done.
CONFIDENTIAL
102

Version Date Safety Concerns Comment
anaphylactic and anaphylactoid reactions, Convulsions with or without fever.
Third February 2014 Tdap waning of immunity.
Missing information of the use of Boostrix Polio in pregnant women
Newly risk identified, as well missing information. Routine monitoring of existing cases and literature of vaccination failure and safety of Tdap –IPV in pregnant women is ongoing.
Fourth August 2016 Additional data on the use of Boostrix line vaccines in pregnant women (Missing information) and addition of Blunting as new potential risk
Proposed labelling change with regard to initial immunisation in adolescents and adults with unknown vaccination status or incomplete vaccination against diphtheria, tetanus and pertussis as part of an immunisation series against diphtheria, tetanus and pertussis (and polio).
New potential risk and additional missing information have been considered.
Current November 2016 Accepted Labelling change in regards toMaternal Immunization.
Update on the data on the use of Boostrix during pregnancy and lactation, and update on the available
Update of the SmPCand one labelling variation ongoing(age lowering & co-administration with MMR/V vaccine)
CONFIDENTIAL
103

Version Date Safety Concerns Comment
literature on Blunting
Update on vaccine waning of immunity and vaccine failure from sales data and post marketing surveillance.
Update in regards to the ongoing labelling variation for age lowering and co administration with MMR/Vvaccine
CONFIDENTIAL
104