ventilator – acquired pneumonia by prof. adel salah professor of respiratory medicine
DESCRIPTION
VENTILATOR – ACQUIRED PNEUMONIA By Prof. Adel Salah Professor of Respiratory Medicine Zagazig University . Definition. VAP refers to pneumonia that arises more than 48 hours after intubation of trachea and initiation of M. ventilation . - PowerPoint PPT PresentationTRANSCRIPT

VENTILATOR – ACQUIRED PNEUMONIA
By
Prof. Adel Salah Professor of Respiratory Medicine
Zagazig University

Definition
VAP refers to pneumonia that arises more than 48 hours
after intubation of trachea and initiation of M.
ventilation.
According to the microbial pattern and the clinical
outcome, VAP can be divided into:
1. Early onset VAP.
2. Late onset VAP.

Determinants of the microbiologic spectrum of VAP:
Prior use of antibiotics.
Duration of time on mechanical ventilation
Risk Factors for MDR Pathogens Causing VAP and HAP (Am J Respir Crit Care Med , 2005)

PathogenesisColonization of aero-digestive tract .Aspiration of infected secretions .Insertion of an ETT:
I. comprises the natural barrier.
II. facilitates pooling and leakage of contaminated secretions.
III. eliminates the cough reflex.
IV. impair mucociliary clearance.
V. bacterial biofilm .
VI. injure the epithelial surface .Other factors: supine position, frequency of ventilator circuit changes, tracheal suctioning, and contaminated respiratory care equipment .Compromise of the normal host defense mechanisms.
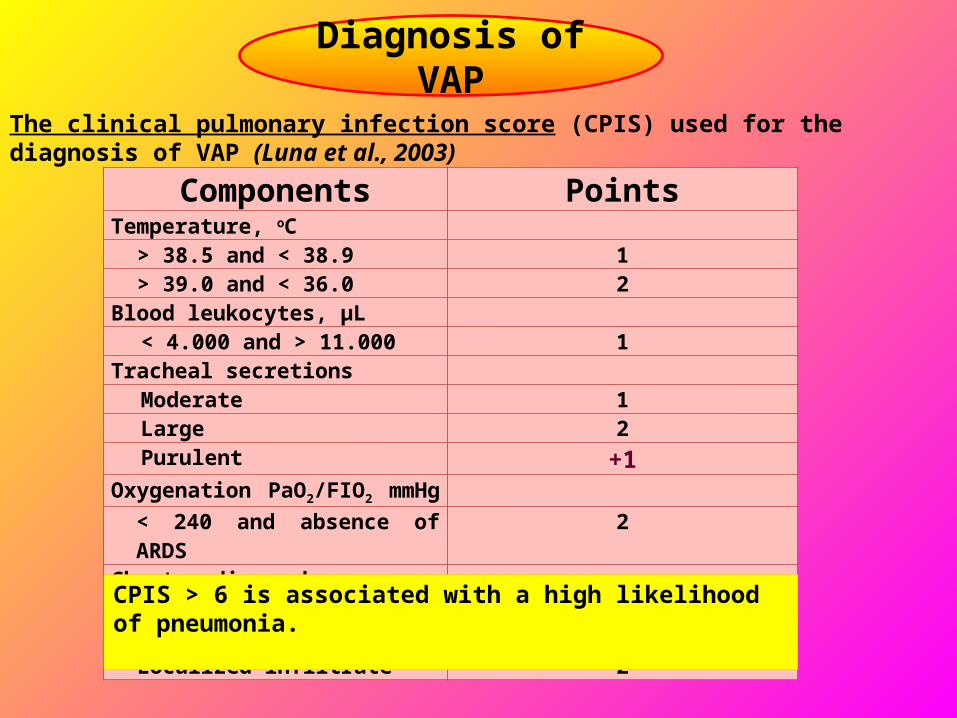
Components PointsTemperature, oC
> 38.5 and < 38.9 1> 39.0 and < 36.0 2
Blood leukocytes, µL< 4.000 and > 11.000 1
Tracheal secretions Moderate 1Large 2Purulent +1
Oxygenation PaO2/FIO2 mmHg < 240 and absence of ARDS 2
Chest radiograph Patchy or diffuse infiltrate 1Localized infiltrate 2
Diagnosis of VAPThe clinical pulmonary infection score (CPIS) used for the diagnosis of VAP (Luna et al., 2003)
CPIS > 6 is associated with a high likelihood of pneumonia.

Signs and symptoms are very nonspecific and lead to overdiagnosis of pneumonia.
So why it is difficult to accurately diagnose VAP?
Fever and leucocytosis.
Increased tracheal secretion.
Oropharyngeal colonization.
Chest radiographic changes.
Blood or pleural fluid culture.
How can pneumonia be differentiated from all these other diseases?
Confirmation of VAP usually relies on a lower respiratory tract
quantitative cultures

What is the rationale for QCs
Infection is more likely the higher the density of microorganisms in a
particular space.
A critical density must be reached in order to cause clinical infection.
A certain threshold is therefore used in order to separate true
infection from colonization.
B.PSB > 100-1000 CFU/ml
B.BAL > 1000-10000 CFU/ml
Deep endotrahceal aspirates > 105-106 CFU/ml
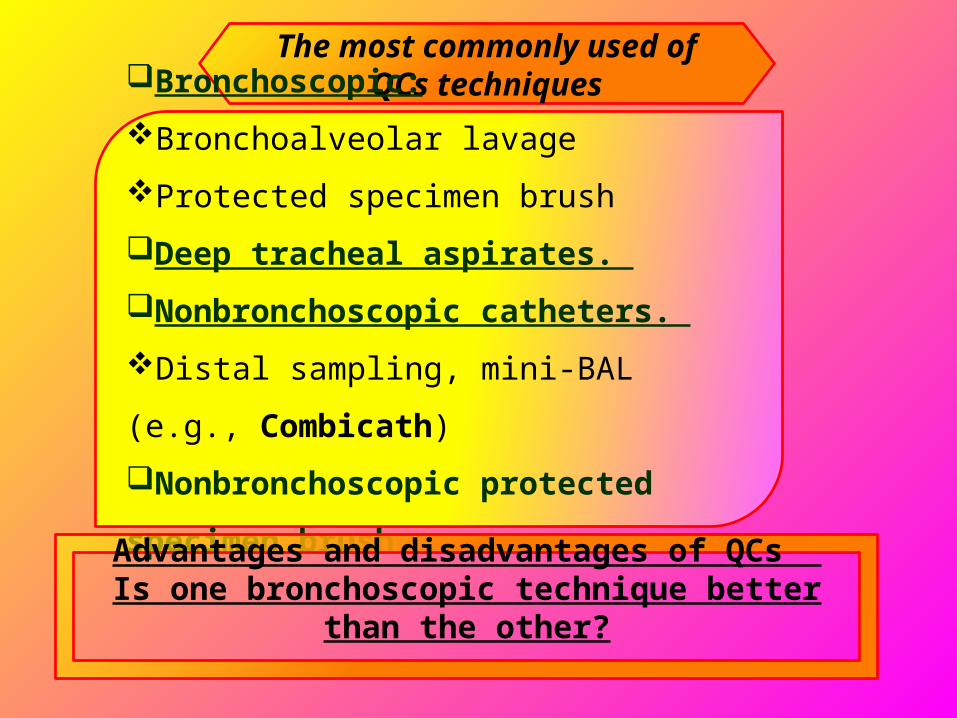
The most commonly used of QCs techniques
Bronchoscopic:Bronchoalveolar lavage
Protected specimen brush
Deep tracheal aspirates. Nonbronchoscopic catheters. Distal sampling, mini-BAL (e.g., Combicath)
Nonbronchoscopic protected specimen brush
Advantages and disadvantages of QCs Is one bronchoscopic technique better than the other?

Role of biomarkers as diagnostic and prognostic markers of VAP
Procalcitonin (PCT): ►Low PCT levels (< 0.25 µg/l) in patients with no clinical signs of severe illness suggest safe withdrawal of antibiotics, thereby limiting the use of unnecessary antibiotics. ►Alternatively PCT > 0.5 µg/ml strongly recommends antibiotic treatment as it is indicative of active bacterial infection. ►PCT was shown to be elevated on an average 2 days prior to the clinical diagnosis of VAP and therefore can be used as an early marker for diagnosis of VAP.
The other biomarkers: like natriuretic peptides, copeptin and CRP levels are useful prognostic markers and may be of great help in the risk stratification of patients.

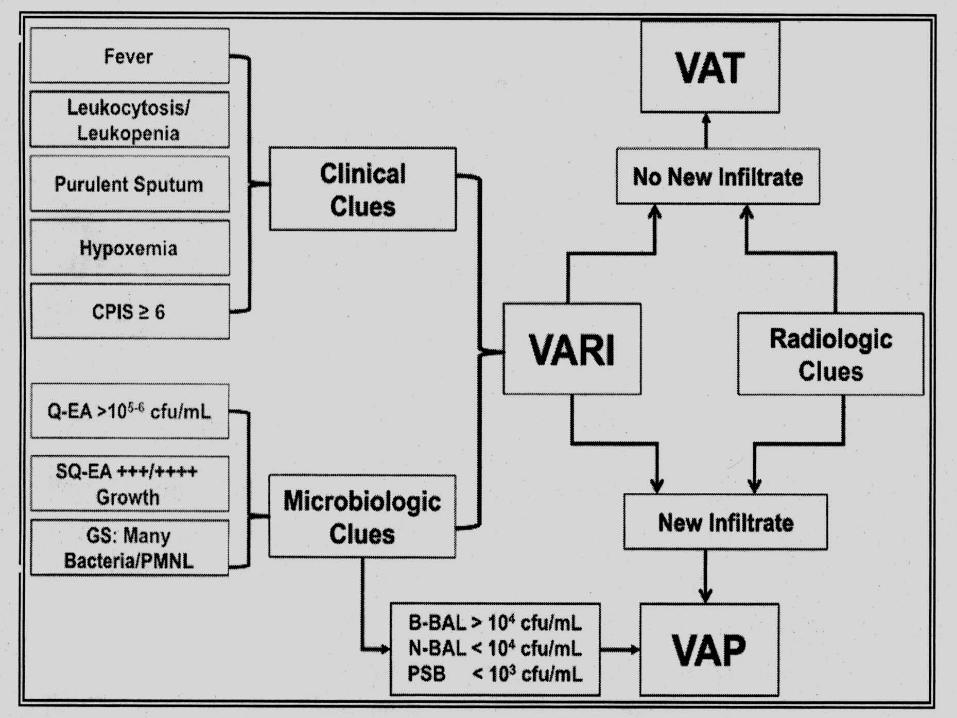
The algorithm for
the diagnosis of
VAP
Differential diagnosis
Other diagnoses should be considered in a patients without typical
signs and symptoms or those who do not respond to empirical
antibiotic therapy.
The differential diagnosis of VAP includes: congestive heart failure.Atelectasis.Acute respiratory distress syndrome (ARDS).pulmonary embolism with infarction. chemical pneumonitis from aspiration. alveolar hemorrhage.Lung contusion in trauma patient.
Complications►Patients who remain ill after initiation of appropriate antibiotic therapy may have
developed complications of pneumonia.
►Common complications include :
complicated parapneumonic effusions, frank empyema.
ARDS.
Spreading of infection to other organs.
sepsis, with multiple organ dysfunction, Renal failure hepatic failure,
disseminated intravascular coagulation, hemodynamic instability, and coma may all
occur in this setting.
Antibiotic treatment of VAP
2 overriding principles
Adequate initial empiric
antibiotic therapy.
Avoiding unnecessary antibiotics.
Duration of therapy Antibiotic class rotation
Treatment Failure criteria indicate treatment failure: (usually after 3 days from AB initiation):failure to improve the PaO2/FiO2 ratio after antibiotic initiation.
persistence of fever or hypothermia plus purulent respiratory secretions.
worsening of the pulmonary infiltrate by 50%.
development of septic shock or multiple organ failure syndrome.
causesWrong diagnosis.Host factors: underlying diseases (e.g., endobronchial malignancy or foreign body), superinfections with organisms that are not sensitive to the antibiotics given, or any of a variety of types of immunosuppression.Bacterial factors : associated with failure of initial therapy include primary or acquired resistance to the initial antibiotic.Complications of the initial infection: (e.g., empyema, abscess formation).

PCT < 0.25 µg/L

Prevention strategies
Guard against Bacterial colonization :►Effective hand washing by hospital personnel. ►Protective gowns and gloves. ►Oral (nonnasal) intubation. ►Limiting stress ulcer prophylaxis to high risk critically ill patients such as those who require mechanical ventilation or have a coagulopathy. ►Avoiding unnecessary antibiotics. ►Adequate initial empiric antibiotic therapy. ►Antibiotic class rotation. ►Chlorhexidine oral rinse. ►Selective digestive decontamination ►Probiotics.►Antimicrobial coating of tracheal tubes.

Guard against aspiration of contaminated secretions:Keeping mechanically ventilated patients
semirecumbent. Reducing excessive use of narcotics. Continuous subglottic suctioning. Use of a closed endotracheal suctioning system.Use of weaning protocols to shorten duration of
mechanical ventilation. Do not routinely change the ventilator circuit. Only
change when visibly soiled or malfunctioning.Consider non invasive ventilation Drain circuit condensate. Use only sterile fluid for humidification or nebulization.Avoiding large gastric volumes. Avoid patient transport. Reduce accidental extubations.
