venous thromboembolism (vte) prevention in obstetrics 2013...in obstetrics . objectives ... •...
TRANSCRIPT
Marc Carrier, MD, MSc, FRCP(C) University of Ottawa
Ottawa Hospital Research Institute
Venous Thromboembolism (VTE) Prevention
in Obstetrics
Objectives • Review the incidence and pathophysiology
of venous thromboembolism (VTE) during the ante and post-partum periods
• Review the risk factors for VTE • Previous VTE • Asymptomatic thrombophilia • Pre-pregnancy risk factors (IBD, etc) • Pregnancy-related risk factors
• Review the risk and benefit of pharmacological thromboprophylaxis to prevent VTE
• Ante-partum period • Postpartum period

Population Epidemiology
Retrospective cohort studies
– Antenatal VTE: ~0.5-1.0/1000 maternities1-3
• Daily antenatal risk 3-7.5x higher than non-pregnant women4
– Postpartum VTE: ~0.5/1000 maternities
• Daily postpartum risk 15-35x higher than non-pregnant women4
1-Andersen BS, Acta Obstet Gynecol Scand,1998; 2-Simpson EL, BJOG 2001; 3-Treffers PE, Int J Gynaecol Obstet 1983; 4-Anderson FA, Arch Intern Med 1991

Bourjeily G, Rodger M, Lancet, 2009
Hypercoagulable Blood ↑Procoagulant Factors:↑ Fibrinogen, ↑V, IX, X, XII and VIII ↓Anticoagulant Activity: ↓ Protein S,↑ act. Protein C resistance ↓ Fibrinolytic Activity: ↑ PAI-1 and PAI-2, ↓ t-PA activity = more thrombin generation and less clot dissolution
Stasis Iliac Vein Compression: Right iliac artery compresses left iliac vein Gravid Uterus Venodilation: Hormonally Mediated Bed Rest Immobilization
Pelvic
Calf
Pregnant
DVT1
Non-Pregnant
DVT2
Right Left Right Left
Total 12% 88% 44% 56%
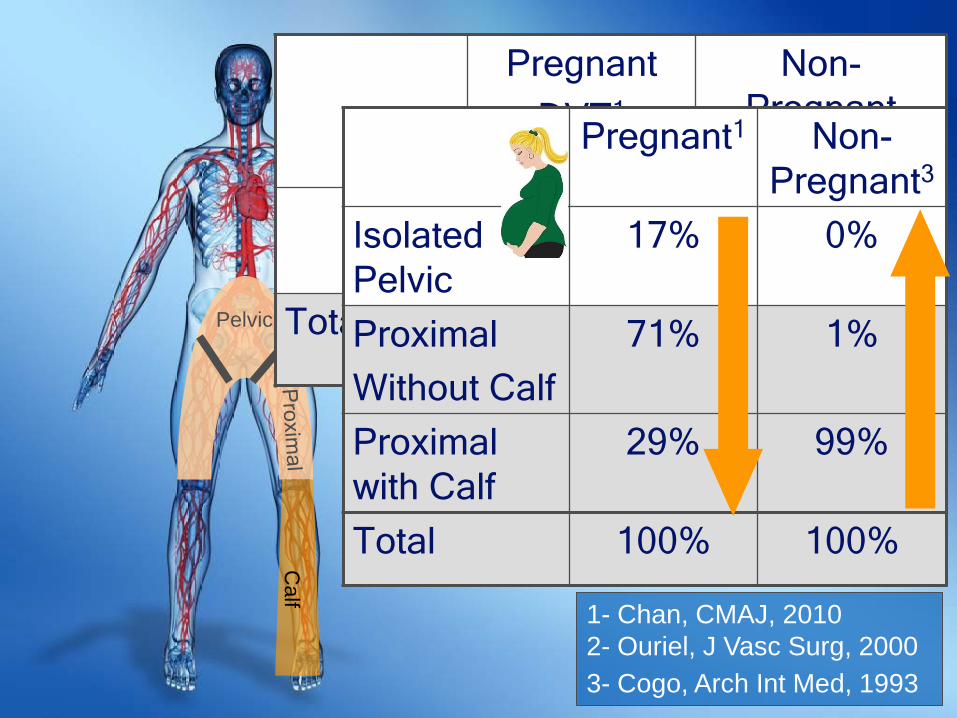
Pregnant1 Non-Pregnant3
Isolated Pelvic
17% 0%
Proximal Without Calf
71% 1%
Proximal with Calf
29% 99%
Total 100% 100%
1- Chan, CMAJ, 2010 2- Ouriel, J Vasc Surg, 2000 3- Cogo, Arch Int Med, 1993

Ante-partum Thromboprophylaxis

Case 1 • 30 yo woman
– 8 weeks GA – Known Factor V Leiden (FLV) found
on family screening
• ? Ante-partum thromboprophylaxis
• She also had a DVT post trauma 5 years ago…? Thromboprophylaxis

When should we consider thromboprophylaxis?
• Assess risk benefit ratio • Risks associated with prophylactic LMWH
• Ante-partum bleeding: 0.42% • Postpartum bleeding: 0.95% • Wound hematoma, HIT: 0% • Major skin reaction/allergy: 0.96% • Osteoporosis: 0.26%
Greer IA, Blood 2005;106:401-407

When should we consider thromboprophylaxis?
• Benefits of prophylactic LMWH – Risk of VTE > 10% - Thromboprophylaxis – Risk of VTE < 1% - No thromboprophylaxis – Risk ≥1 but ≤ 10% - Controversial (preferences, etc)
• SOGC panel consensus Risk of VTE ≥1 %= consider thromboprophylaxis

Ante-Partum Risk Factors Previous VTE
Risk of VTE < 1% ≥1 to ≤ 10% > 10% •Provoked VTE (Not OCP or pregnancy related)
•Unprovoked VTE •Pregnancy related VTE •OCP related VTE
•OCP related VTE
Brill-Edwards P et al. NEJM 2000;343:1439-1444; Pabinger I et al. J Thromb Heamost 2005;3: 949-954; De Stephano V, Br J Haematol 2006;135:386-391.

Ante-Partum Risk Factors Aymptomatic thrombophilia
Risk of VTE < 1% ≥1 to ≤ 10% > 10% •Hetero FVL •Hetero PTG •PC deficiency •PS deficiency
•Combined hetero FVL + PTG
•AT III •Homo FVL •Homo PTG
Pabinger I et al. Hematol J 2000;1:37-41; van Boven HH et al. Blood 1999;94:2590-2594; Tormene D et al. Haematologica 2001;86: 1305-1309; Middeldorp S et al. Ann Intern Med 1998;128:15-20. Zotz RB et al. Clinical Haemotalogy 2003; 16:243-259; McColl MD et al. Thromb Haemost 1997;78:1183-8; Gerhardt A et al. NEJM 2000; 342:374-80;

Ante-Partum Risk Factors Pre-pregnancy risk factors
Risk of VTE < 1% ≥1 to ≤ 10% > 10% •Diabetes •IBD •Cancer •Varicose veins •Weight/BMI •Age •Smoking
Sultan AA et al. Blood 2013;121:3953-3961; Simpson EL et al. BJOG 2001;108:56-60; Larsen TB et al. Thromb Res 2007;120:505-509; Knight M BJOG 2008;115:453-461; Jacobsen AF et al. J Thromb Haemost 2008;6:905-912.
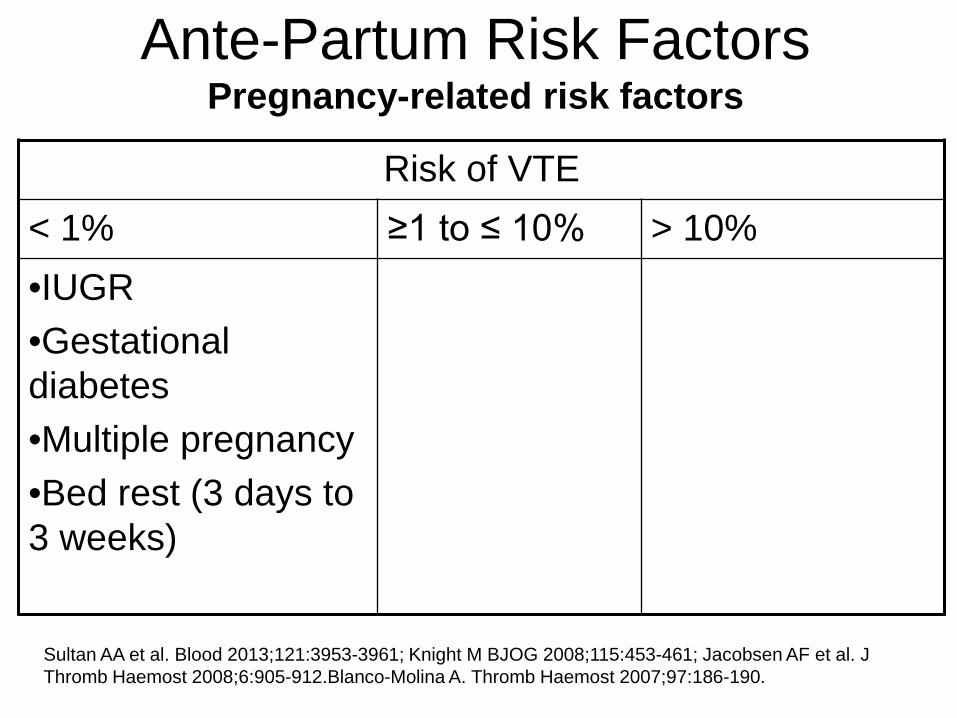
Ante-Partum Risk Factors Pregnancy-related risk factors
Risk of VTE < 1% ≥1 to ≤ 10% > 10% •IUGR •Gestational diabetes •Multiple pregnancy •Bed rest (3 days to 3 weeks)
Sultan AA et al. Blood 2013;121:3953-3961; Knight M BJOG 2008;115:453-461; Jacobsen AF et al. J Thromb Haemost 2008;6:905-912.Blanco-Molina A. Thromb Haemost 2007;97:186-190.

Ante-Partum Risk Factors Multiple pregnancy-related risk factors
Risk of VTE < 1% ≥1 to ≤ 10% > 10% •IUGR + preeclampsia
•Bed rest (≥ 7 days) and BMI (≥ 25 Kg/m2)
Jacobsen AF et al. J Thromb Haemost 2008;6:905-912.

Dosing of thromboprophylaxis
• Unfractionated heparin: 5000 IU sc BID • Dalteparin 5000 IU sc daily • Enoxaparin 40 mg sc daily • Tinzaparin 4500 IU sc daily • Nadroparin 2850 IU sc daily • Consider decreasing dose if < 50 kg • Consider increasing dose if > 100 kg
Neuraxial anesthesia
• Hold anticoagulation at the onset of labor – or day prior of planned delivery
• UFH: – Neuraxial anesthesia: No delay up to 4 hours
• LMWH: – Neuraxial anesthesia: Min of 10 to 12 hours – ? Switch from LMWH to UFH at 37 weeks
• Depends on local practices and logistics

Take Home Message • Individual risk assessment
– If higher risk: Discuss signs and symptoms of VTE
• Consider prophylactic doses of LMWH: – Previous unprovoked or OCP or pregnancy
related VTE – Asymptomatic homo FVL or PTG, ATIII – Asymptomatic combined thrombophilia – In presence of multiple risk factors where the
overall absolute risk > 1% • e.g. Previous provoked VTE and thrombophilia

Take Home Message • Routine thromboprophylaxis is not
recommended for single pregnancy-related risk factors
• Any indication for intermediate or therapeutic doses of LMWH? – If already on long-term anticoagulation – Multiple previous VTE – Previous VTE with high risk thrombophilia
(ATIII, APLA, etc)

Post-partum Thromboprophylaxis

Case 1 • 30 yo woman
– 8 weeks GA – Known Factor V Leiden (FLV) found
on family screening – Uncomplicated vaginal delivery – No placeta-mediated complications
• Postpartum thromboprophylaxis
• She also add a DVT post trauma 5
years ago…? Thromboprophylaxis

Postpartum VTE
• Leading cause of death in Canada • 17 maternal deaths per year • 15 to 35 fold increase in the 6 weeks following the
delivery (highest during the first 3 weeks)
• Different risk factors for postpartum vs. ante-partum VTE
• Again: – Consensus: Risk of VTE ≥1 =
Thromboprophylaxis
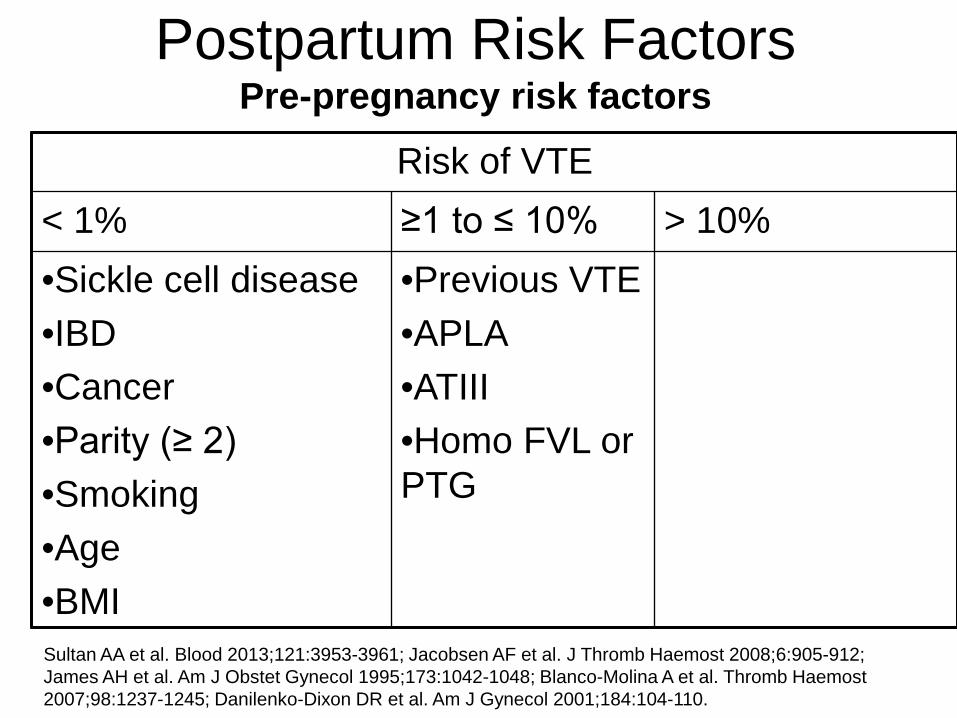
Postpartum Risk Factors Pre-pregnancy risk factors
Risk of VTE < 1% ≥1 to ≤ 10% > 10% •Sickle cell disease •IBD •Cancer •Parity (≥ 2) •Smoking •Age •BMI
•Previous VTE •APLA •ATIII •Homo FVL or PTG
Sultan AA et al. Blood 2013;121:3953-3961; Jacobsen AF et al. J Thromb Haemost 2008;6:905-912; James AH et al. Am J Obstet Gynecol 1995;173:1042-1048; Blanco-Molina A et al. Thromb Haemost 2007;98:1237-1245; Danilenko-Dixon DR et al. Am J Gynecol 2001;184:104-110.

Postpartum Risk Factors Pregnancy-related risk factors
Risk of VTE < 1% ≥1 to ≤ 10%
•Gestational DM •IUGR •Placenta previa •Abruption •PROM •Preterm birth •Stillbirth
•Any C-section •Elective C-section •ER C-section
Sultan AA et al. Blood 2013;121:3953-3961; Jacobsen AF et al. J Thromb Haemost 2008;6:905-912; Jacobsen AF et al. Obstet Gynecolo 2008;198:233. e1-233; Blanco-Molina A et al. Thromb Haemost 2007;98:1237-1245; Danilenko-Dixon DR et al. Am J Obstet Gynecol 2001; 2001;184:104-110.

Postpartum Risk Factors Multiple risk factors
Risk of VTE < 1% ≥1 to ≤ 10% > 10% •IUGR + preeclampsia •C-section with infection postpartum
•> 1 liter hemorrhage + post-partum surgery •Vaginal delivery + infection postpartum •Bed rest (> 7days) + BMI ≥ 25 kg/m2
Jacobsen AF et al. J Thromb Haemost 2008;6:905-912.

Duration of thromboprophylaxis
• Persistent risk factors – Prior VTE (highest), high risk thrombophilia, etc – 6 weeks post-partum
• Transient risk factors
– Until discharged from hospital or up to 2 weeks

Neuraxial anesthesia
• Removal of neuraxial anesthesia: – UFH:
• 4 hours after last dose – LMWH:
• 10 to 12 hours after last dose (or before next dose) • May resume LMWH 2 hours post removal

Take Home Message • Individual risk assessment
– If higher risk: Discuss signs and symptoms of VTE – Close clinical follow-up
• Consider prophylactic doses of LMWH:
– Previous VTE – ATIII def, Homo FVL or PTG, combined
thrombophilia, APLA – Strict bed rest prior to delivery (> 7 days)
• >90% of the time in bed – Peri or postpartum blood loss (> 1L) or transfusion
and concurrent postpartum surgery – Vaginal delivery and peripartum sepsis

Take Home Message • Consider prophylactic doses of LMWH if 2 or
more of the following: – Any C-section – Smoking (> 10 cigarettes/day antepartum) – BMI ≥30 kg/m2 at first antepartum visit – IUGR – Preeclampsia – Placenta previa or abruption – Peri or postpartum infection (vaginal or c-section) – Low risk thrombophilia (PC, PS, hetero FV or PT) – IBD, DM, sickle cell disease – Multiple pregnancy – Pre-term delivery
Take Home Messages
• DVT in pregnancy is likely a north (proximal) to south (distal) disease
• Individual risk assessment – If higher risk: Discuss signs and symptoms of
VTE + Close follow-up
• Consider ante and/or postpartum thromboprophylaxis in patients with risk of VTE ≥1%

Diagnosis of DVT and PE in Pregnancy

Case 1
• 30 yo woman presents at 8 weeks GA with a tender swollen left leg/buttock

Exam: left thigh/calf are >5 cm bigger than her right leg

Case 1
How would you exclude DVT? 1. Negative D-dimer alone 2. Low Wells model and negative D-Dimer 3. Single negative compression US (CUS) 4. Negative serial compression US (CUS) on
Day 1 and day 7 5. Negative compression ultrasound (CUS)
and negative MRV

Wells Clinical Model for DVT Wells P, et al. Value of Assessment of Pre-test Probability of Deep-Vein Thrombosis in Clinical Management. Lancet Vol. 350, Dec 1997, 1795-1798.
Active cancer (treatment ongoing or within past 6 months or palliative) 1
Recent paresis, paralysis or cast immobilization of lower limb (within past 4 weeks) 1
Recently bedridden for more than 3 days or major surgery within the past four weeks 1
Localized tenderness of the deep venous system 1
Oedema of entire leg 1
Calf swelling > 3 cm when compared with contralateral calf (measured 10 cm under the tibial tuberosity) 1
Pitting oedema more marked on suspected side 1
Collateral vein network (non-varicose) (replaced by previous VTE in recent versions) 1
Another diagnosis as likely or more likely than DVT -2
Total Score:
Probability is: High Intermediate Low
if total is equal to or greater than 3 if total is 1 or 2 if total is 0
Probability is: Likely Unlikely
if total is >1 if total is ≤1
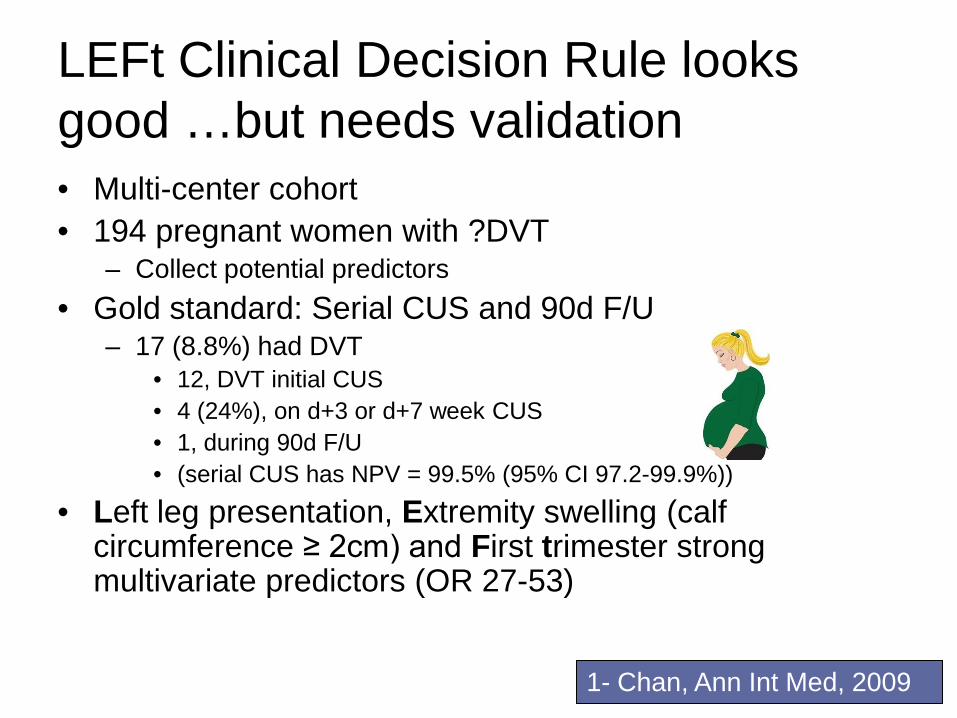
LEFt Clinical Decision Rule looks good …but needs validation • Multi-center cohort • 194 pregnant women with ?DVT
– Collect potential predictors • Gold standard: Serial CUS and 90d F/U
– 17 (8.8%) had DVT • 12, DVT initial CUS • 4 (24%), on d+3 or d+7 week CUS • 1, during 90d F/U • (serial CUS has NPV = 99.5% (95% CI 97.2-99.9%))
• Left leg presentation, Extremity swelling (calf circumference ≥ 2cm) and First trimester strong multivariate predictors (OR 27-53)
1- Chan, Ann Int Med, 2009

D-Dimer alone to exclude DVT in pregnancy looks good …but needs validation • Multi-center cohort • 149 pregnant women with ?DVT
– SimpliRED D-Dimer • Gold standard: Serial CUS and 90d F/U
– 13 (8.7%) had DVT
WS Chan, S Chunilal, A Lee, M. Rodger and JS Ginsberg. Annals Int Med 2007

100% Sensitivity
Specificity
Negative predictive
value …40
50
60 70 80 90 0…
100
Normal D-Dimer to exclude DVT in pregnancy
95% CI: 75-100%
60% 95%CI: 52-68%
95-100% 100%
WS Chan, S Chunilal, A Lee, M. Rodger and JS Ginsberg. Annals Int Med 2007

Case 1
How would you exclude DVT? 1. Negative D-dimer alone 2. Low Wells model and negative D-Dimer 3. Single negative compression US (CUS) 4. Negative serial compression US (CUS) on
Day 1 and day 7 5. Negative compression ultrasound (CUS)
and negative MRV
Case 2
35 yo women 30 wks GA presents with pleuritic CP and SOB and positive D-Dimer.
How would you exclude PE? 1. Low Wells model and negative D-
Dimer 2. Compression US first then if normal do
a V/Q; normal perfusion excludes PE 3. V/Q: normal perfusion excludes PE 4. Negative CT pulmonary angiogram
alone

Wells Clinical Model for PE Points
• Clinical symptoms of DVT 3
• No alternative diagnosis more likely than PE 3
• Heart rate over 100 1.5 • History of immobilization or surgery in previous 4 weeks
1.5
• Previous DVT/PE 1.5
• Hemoptysis 1.0
• Cancer
1.0
Total Score ≤4 = negative, >4 = positive
Return to Question 5

D-Dimer looks good …but needs validation
• Multi-center cohort • 149 pregnant women with ?DVT
– SimpliRed D-Dimer
• Gold standard: Serial CUS and 90d F/U – 13 (8.7%) had DVT
WS Chan, S Chunilal, A Lee, M. Rodger and JS Ginsberg. Annals Int Med 2007

V/Q CXR All 3
CT
0.016
0.032
0.05
0
0.066
0.082
0.1
0.000001 Gy
Radiation Exposure to Fetus G
ray
(Gy)
0.00051 Gy
0.000013 Gy
0.00054 Gy
Possible Teratogenic Threshold 0.1Gy
Possible Oncogenic Threshold 0.01Gy

V/Q Test of Choice in Pregnancy: Disadvantages of CT over V/Q • Higher proportion of inadequate CTs in
pregnancy (up to 1/3rd)1
– Contrast timing/ IVC dilution
• V/Q normal in >70% of patients in pregnancy with ?PE2,3
1- Ridge et al, AJR, 2009; 2- Chan et al, Arch Int Med, 2002; 3-Cahill, Obstet Gynecol, 2009;

V/Q Test of Choice in Pregnancy: Disadvantages of CT over V/Q • Non-Pregnant: High “false positive” rate
with CT in an RCT1 which may worsen with ↑slices in MDCT2
• Increase lifetime risk of malignancy from radiation exposure – 150X ↑ breast radiation than V/Q – 1 in 143 in 20 y.o. non-pregnant ♀3
1- Anderson, JAMA, 2007; 2- Carrier, JTH, 2010; 3-Einstein, JAMA 2007

Case 2
30 wks GA presents with pleuritic CP and SOB and positive D-Dimer.
How would you exclude PE? 1. Low Wells model and Negative D-Dimer
2. Compression US first then if normal do a V/Q; normal excludes PE
3. V/Q: normal excludes PE 4. Negative CT pulmonary angiogram alone

Take Home Messages
• DVT in pregnancy is likely a north (proximal) to south (distal) disease
• Serial ultrasounds are required to exclude DVT in pregnancy
• V/Q scan remains test of choice for ?PE