vasculopathy and vasculitis• medium-size arteries in classic polyarteritis nodosa • the...
TRANSCRIPT

Vasculopathy and Vasculitis
Danoushka Tememe, MD
Overview
• Fibromuscular Dysplasia• Moyamoya• Snedden’s Syndrome
• Susac’s Syndrome• Systemic Vasculitis• Primary angiitis of the CNS

Fibromuscular Dysplasia

Fibromuscular Dysplasia
• FMD is a noninflammatory, nonatherosclerotic arterial disease of the medium-sized arteries throughout the body, which could lead to arterial stenosis, occlusion, aneurysm, and dissection.
• The renal and carotid/vertebral arteries are most frequently affected
• Iliac, mesenteric, subclavian arteries
• Often multifocal and bilateral.
• Usually involves the mid segment of the vessels and spares origins
• Age 25 to 50 years and affects women more often than men (3:1).

Presentation
Hypertension
TIA/Stroke
Spontaneous dissection
Neck pain
Pulsatile tinnitus
Horner’s syndrome
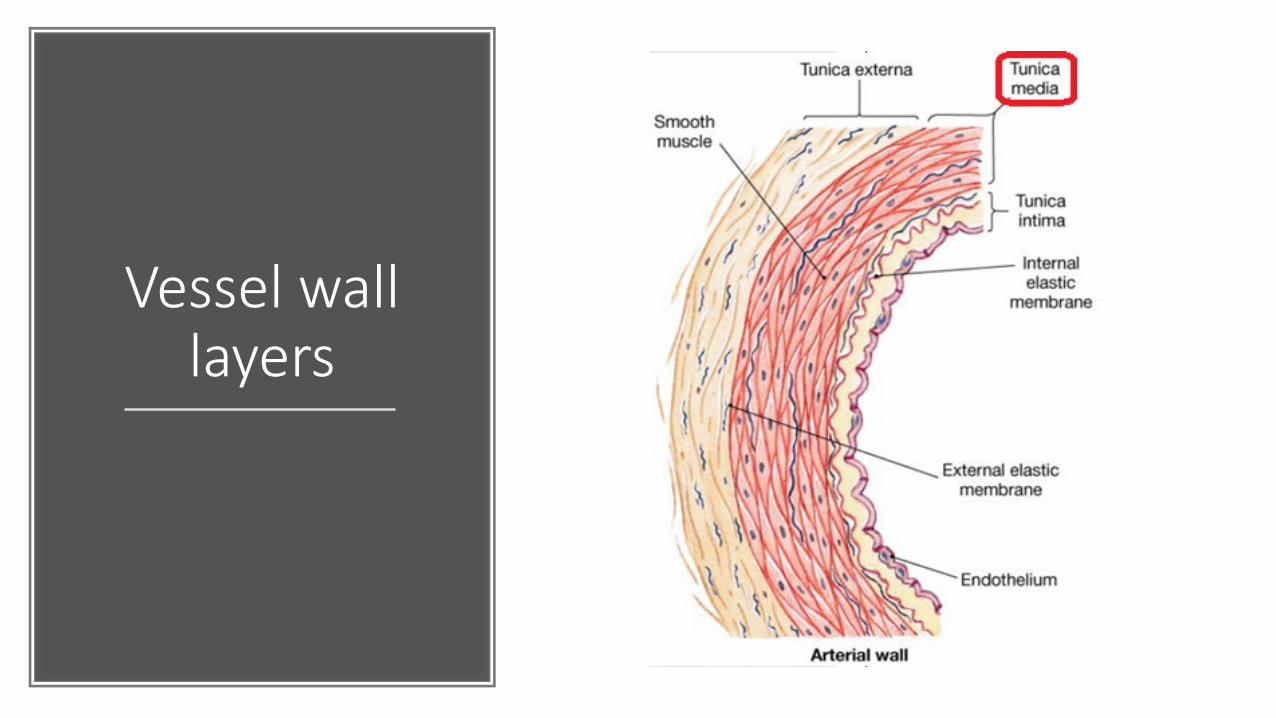
Vessel wall layers

Typical string-of-beadspattern with alternating regions of lumen narrowing and vessel dilatation over a length of 3 – 5 cm
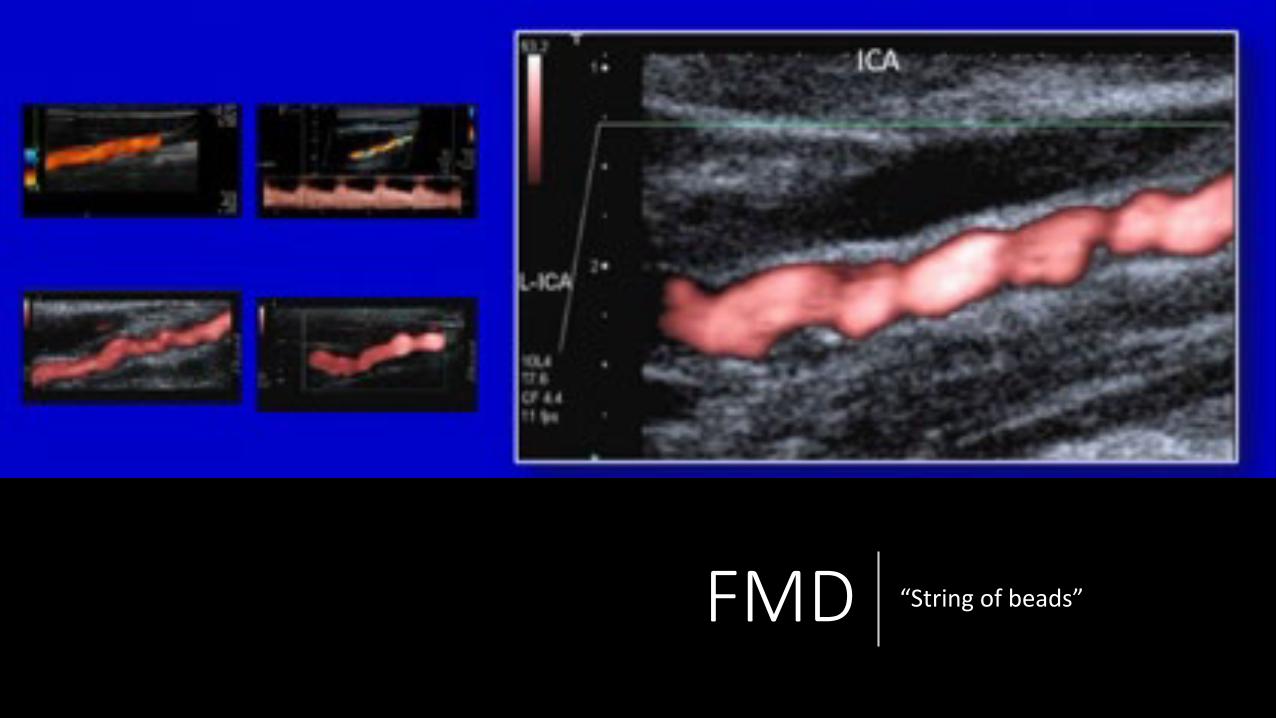
FMD “String of beads”

Extreme tortuosity “S curve”

Treatment
• There is no standard protocol to treat FMD
• Aim of treatment is to improve blood flow and depends on which arteries are affected and the severity
• Balloon angioplasty +/- stent
• The carotid arteries should be imaged if FMD is found elsewhere in the body
• Aspirin daily
• Smoking cessation
Moyamoya

Moyamoya
• Moyamoya disease is a progressive occlusive arteriopathy of the bilateral supraclinoid internal carotid arteries
• Moyamoya syndrome: Down syndrome, neurofibromatosis type 1, sickle cell
• Moyamoya-like vasculopathy: radiation, meningitis
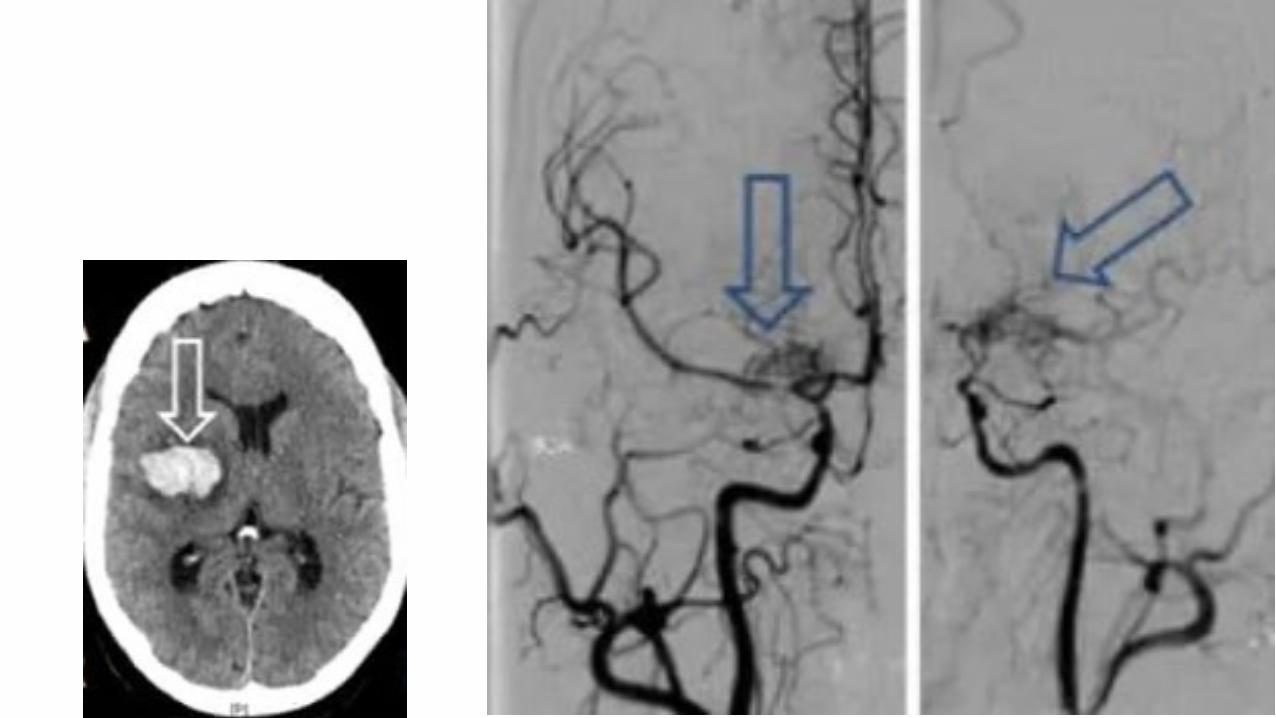
• Abnormal network of fine collateral vessels
• Additional collaterals may develop:• Leptomeningeal collaterals from the posterior cerebral artery• Transdural collaterals from the external carotid artery

Presentation
• Can present with TIA/stroke (50-75%) or intracranial hemorrhage (IPH or SAH).
• Seizures, headache
• Fragile collaterals are prone to hemorrhage and hemodynamic failure.
• Symptomatic episodes of ischemia may be triggered by exercise, crying, coughing, straining, fever, hyperventilation, dehydration, hypotension (e.g., general anesthesia for minor procedures).
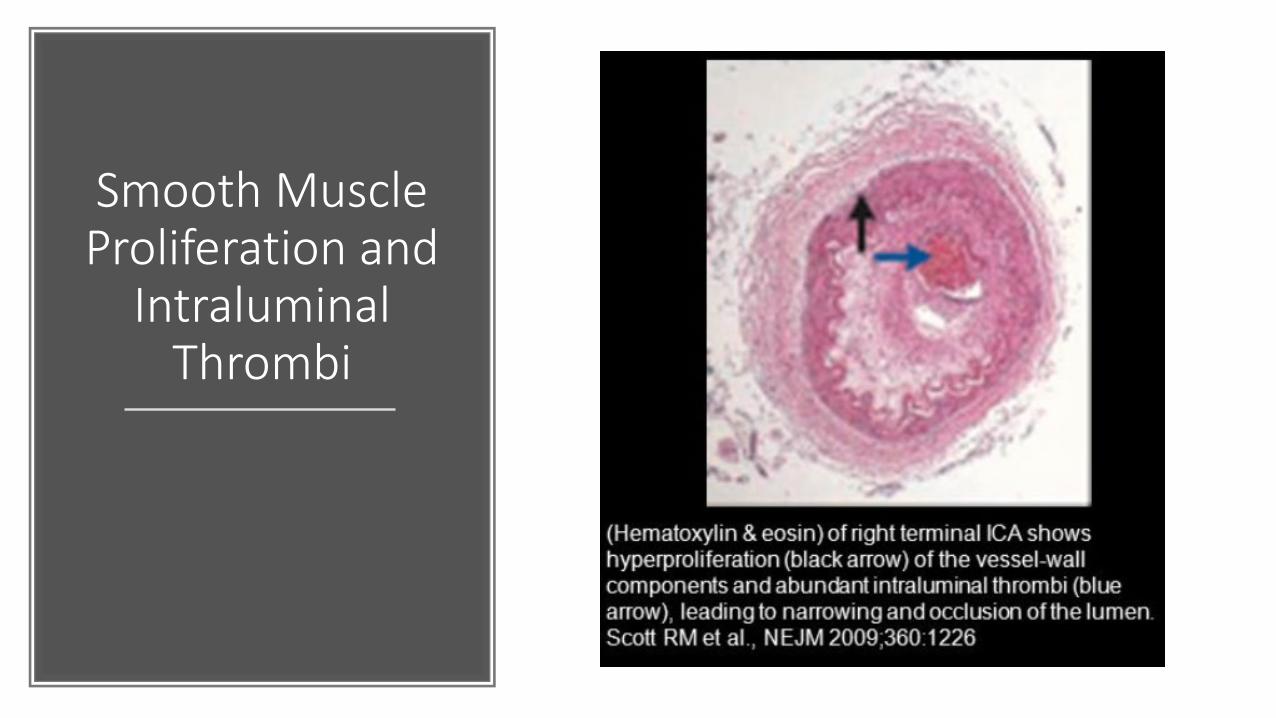
Smooth Muscle Proliferation and
Intraluminal Thrombi
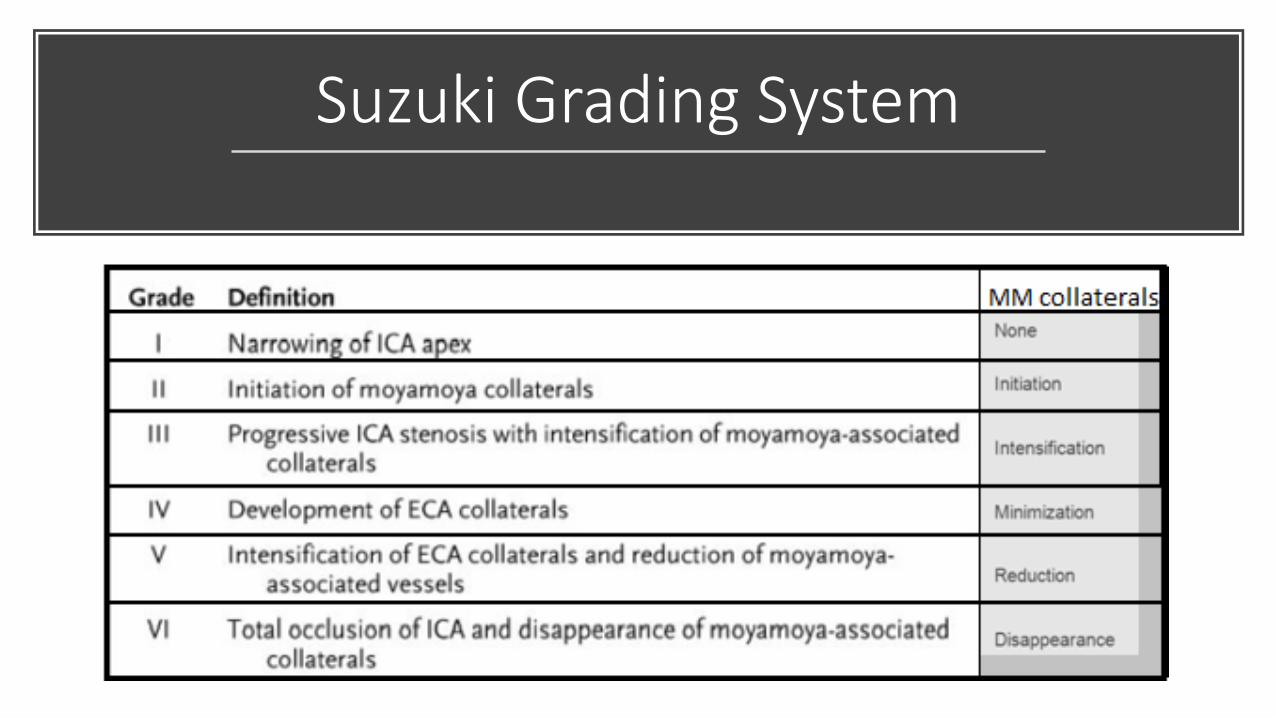
Suzuki Grading System

Moyamoya

Stage 3/4

Stage 4/5
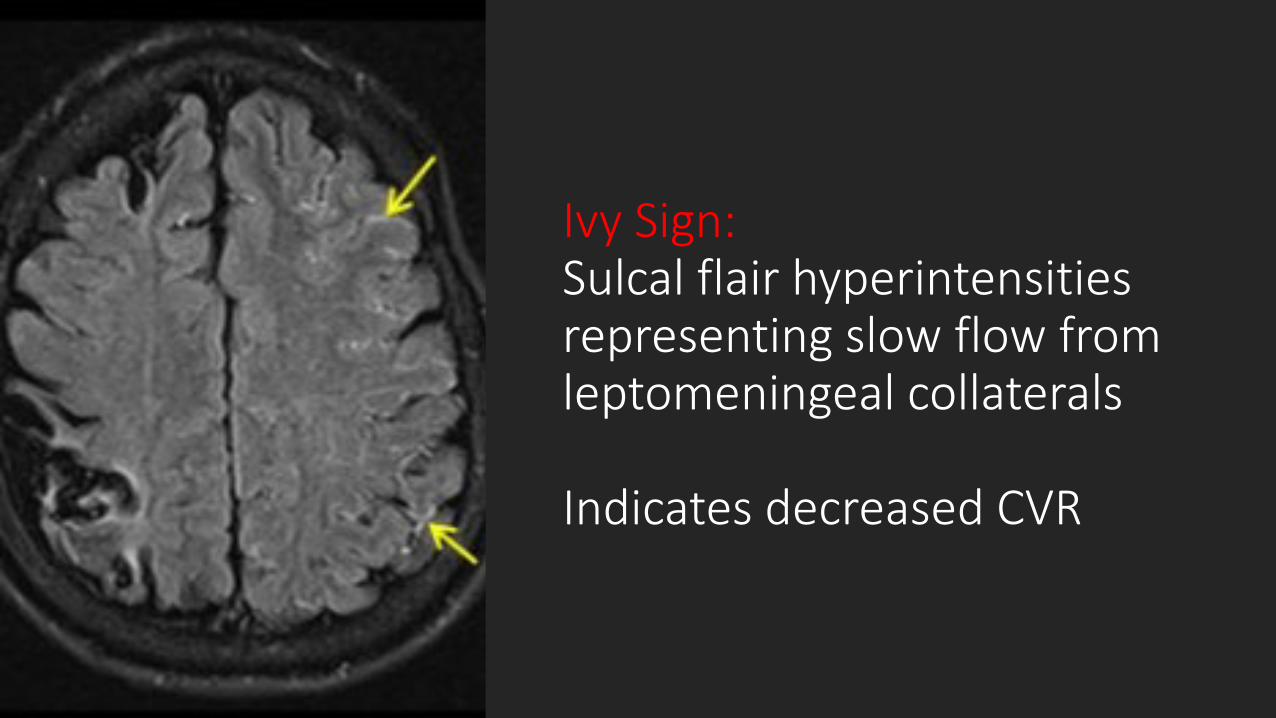
Ivy Sign: Sulcal flair hyperintensities representing slow flow from leptomeningeal collaterals
Indicates decreased CVR

Brush Sign

Brush Sign on SWI Correlates with Severity of Moyamoya
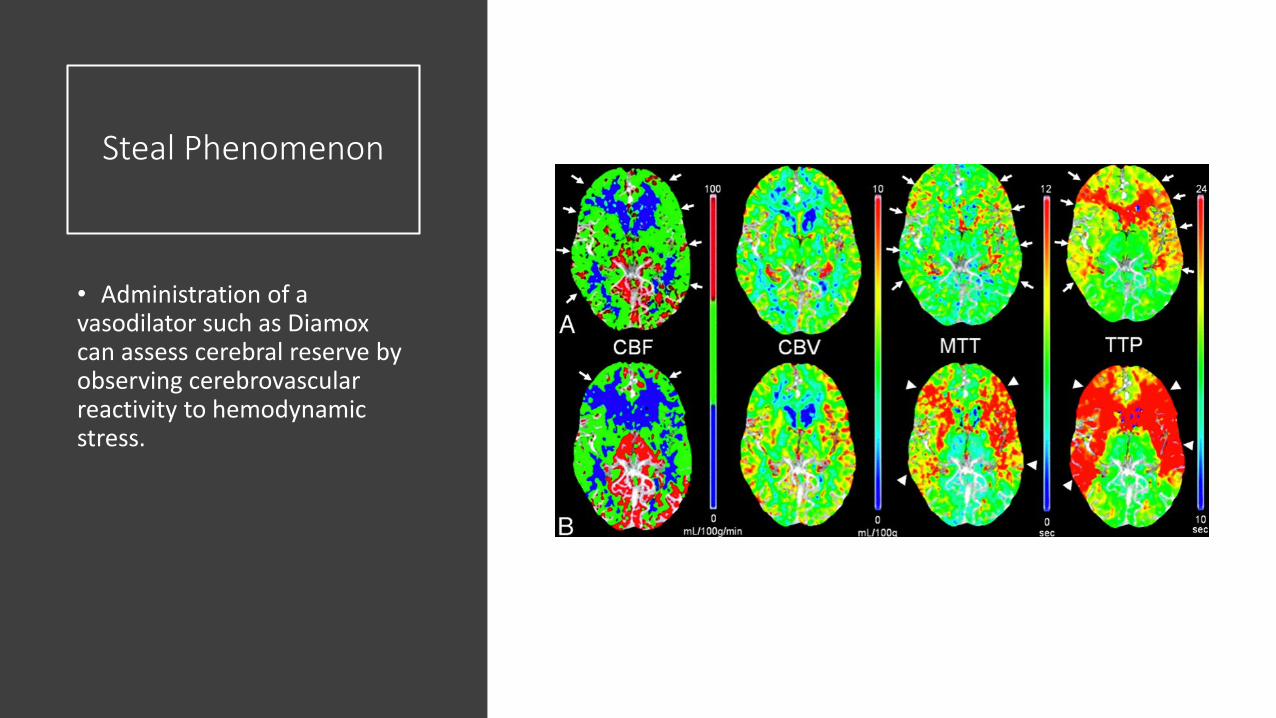
Steal Phenomenon
• Administration of a vasodilator such as Diamox can assess cerebral reserve by observing cerebrovascular reactivity to hemodynamic stress.
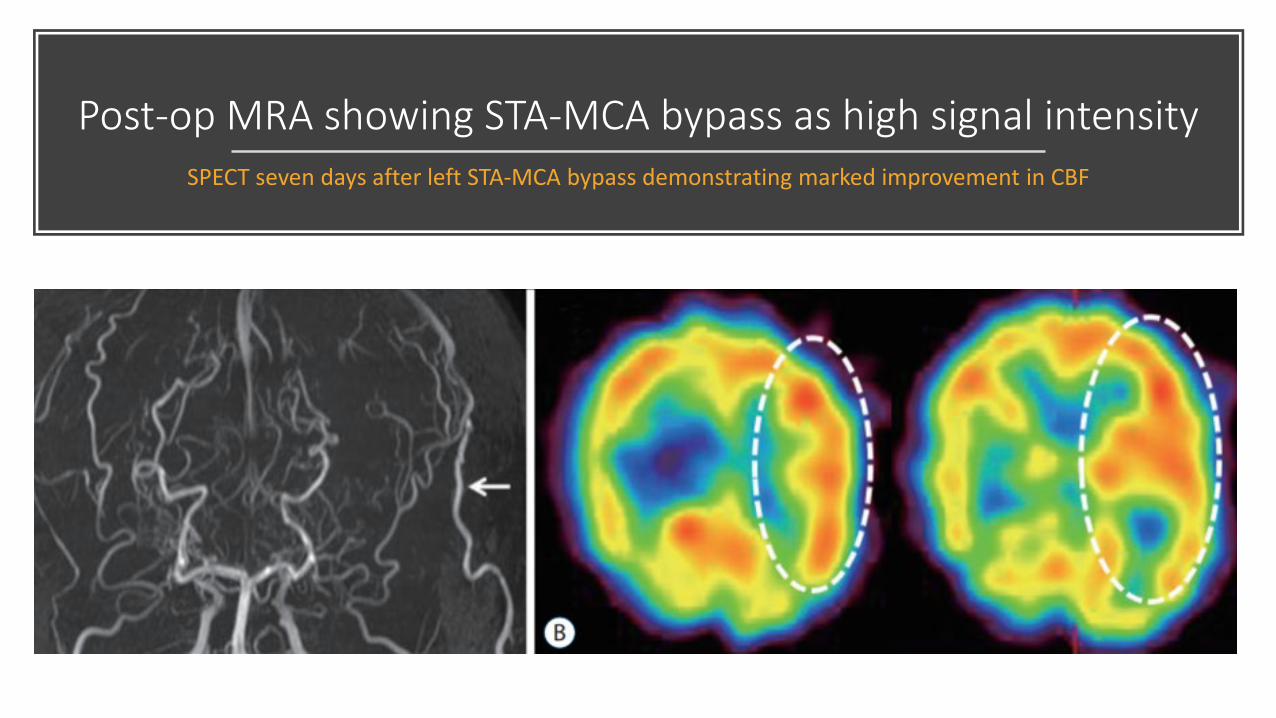
Post-op MRA showing STA-MCA bypass as high signal intensitySPECT seven days after left STA-MCA bypass demonstrating marked improvement in CBF

Post-treatment
changes following STA-
MCA bypass
• Moyamoya vessels start regressing 1 month after bypass surgery.
• STA caliber increases 3 months after surgery.
• ICAT steno-occlusion quickly progresses after surgery.

Sneddon Syndrome

Sneddon Syndrome
• Progressive disorder affecting small- and medium-sized blood vessels.
• Cerebral, ocular, renal, and cardiac involvement
• Characterized by livedo racemosa (net-like patterns of discoloration on the skin) and neurological abnormalities.
• More common in women• Onset of neuro symptoms in the 3rd to 4th decade• The livedo generally occurs up to 10 years earlier

Livedo Racemosa
• Persistent, erythematous or violaceous discoloration of the skin, in a broken, branched, discontinuous and irregular pattern.
• Located on limbs (100%), trunk (84–89%), buttocks (68–74%), or the hands or feet (53–59%)
• Results from persistent impairment of peripheral blood flow caused by occlusion of small or medium-sized arteries
• Does not disappear with rewarming• vs livedo reticularis, which is caused by temporary
vasoconstriction

Diagnosis
• Skin biopsy: occlusion without inflammation of the small to medium-sized arteries at the border between dermis and subcutis.
• May reveal thrombosis of subcutaneous arterioles and compensatory capillary dilation with blood stagnation.
• Can also see intimal endothelial proliferation and proliferation of medial smooth muscle cells
• Blood tests: check for antiphospholipid antibodies (40-50% of patients are aPL+) and rule out other autoimmune conditions (including lupus)
• CECR1 gene implicated given its role in producing adenosine deaminase 2, which is an enzyme that helps support the lining of blood vessel walls.
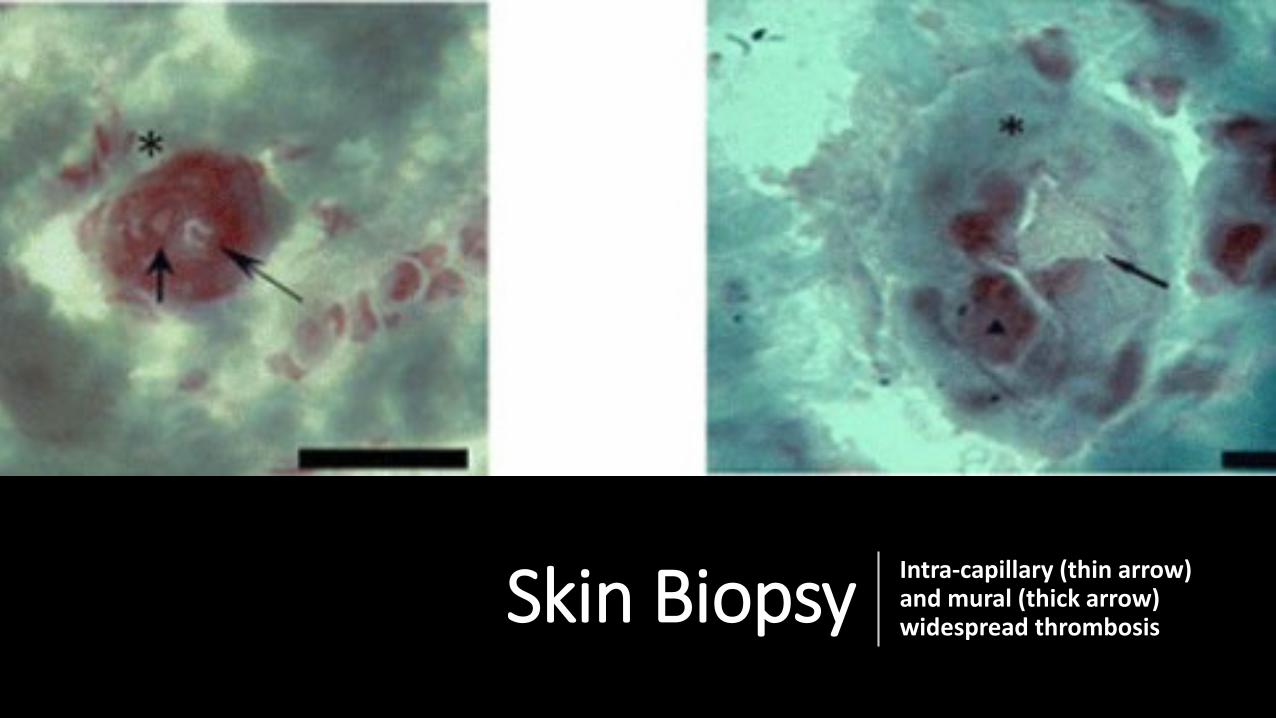
Skin Biopsy Intra-capillary (thin arrow) and mural (thick arrow) widespread thrombosis

Biopsy
• Biopsy site should be in the center of the lesions, where the skin seems to be untouched.
• Multiple biopsies increase the diagnostic yield.
• The goal of a biopsy is to obtain samples of the medium vessel found in the deep reticular dermis and subcutaneous fat, which may require a wedge or large punch biopsy for increased yield.

Cerebral Angiogram
• Shows peripheral small-vessel and medium-vessel vasculopathy resulting in pruning of the distal cortical vessels and tortuous irregular distal collaterals.

Treatment
• No specific treatment for underlying condition
• Antiplatelet therapy • Can use anticoagulants if +antiphospholipid antibodies
• ACE inhibitors may reduce endothelial proliferation
• Nifedipine may reduce skin symptoms• No effect on cerebrovascular complications
• Smoking cessation and avoidance of estrogen oral contraceptives

Susac’s Syndrome
Susac’s Syndrome
• Autoimmune disease characterized by retinal, cochlear, and brain microangiopathy
• Clinical triad of subacute encephalopathy, branched retinal artery occlusion, and sensorineural hearing loss
• More common in women • Age of onset between 20-50 years of age
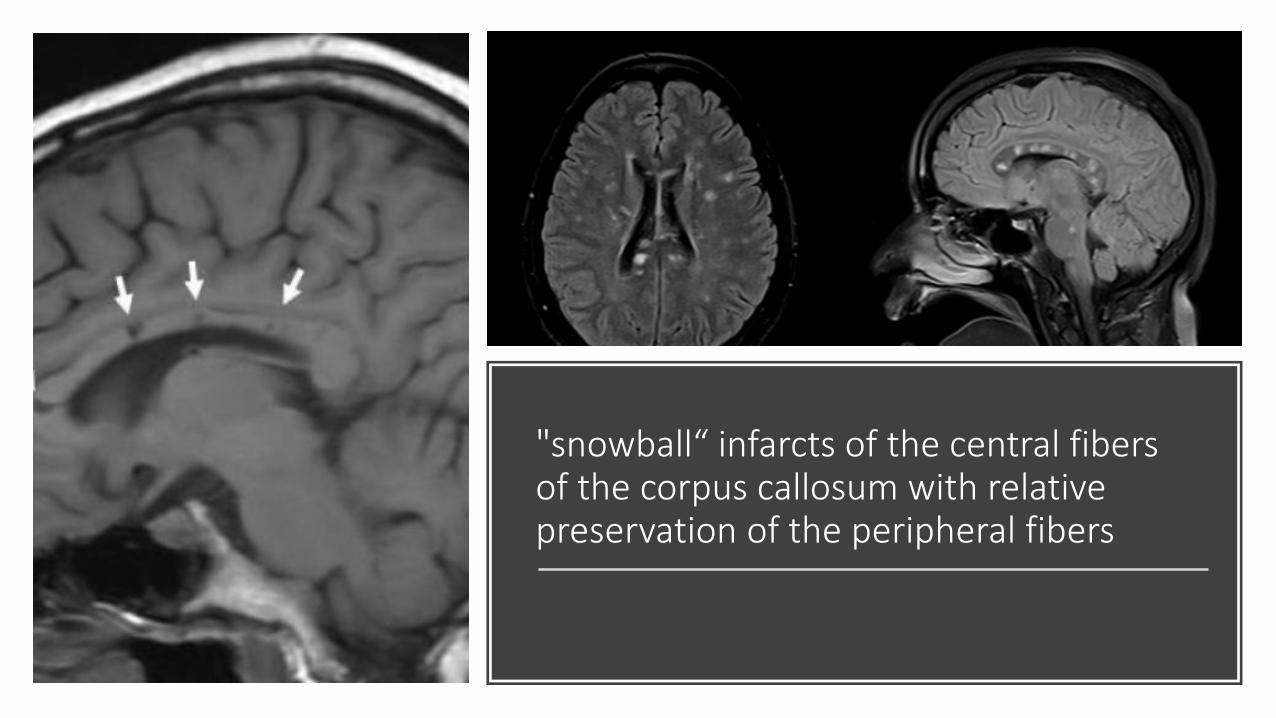
"snowball“ infarcts of the central fibers of the corpus callosum with relative preservation of the peripheral fibers
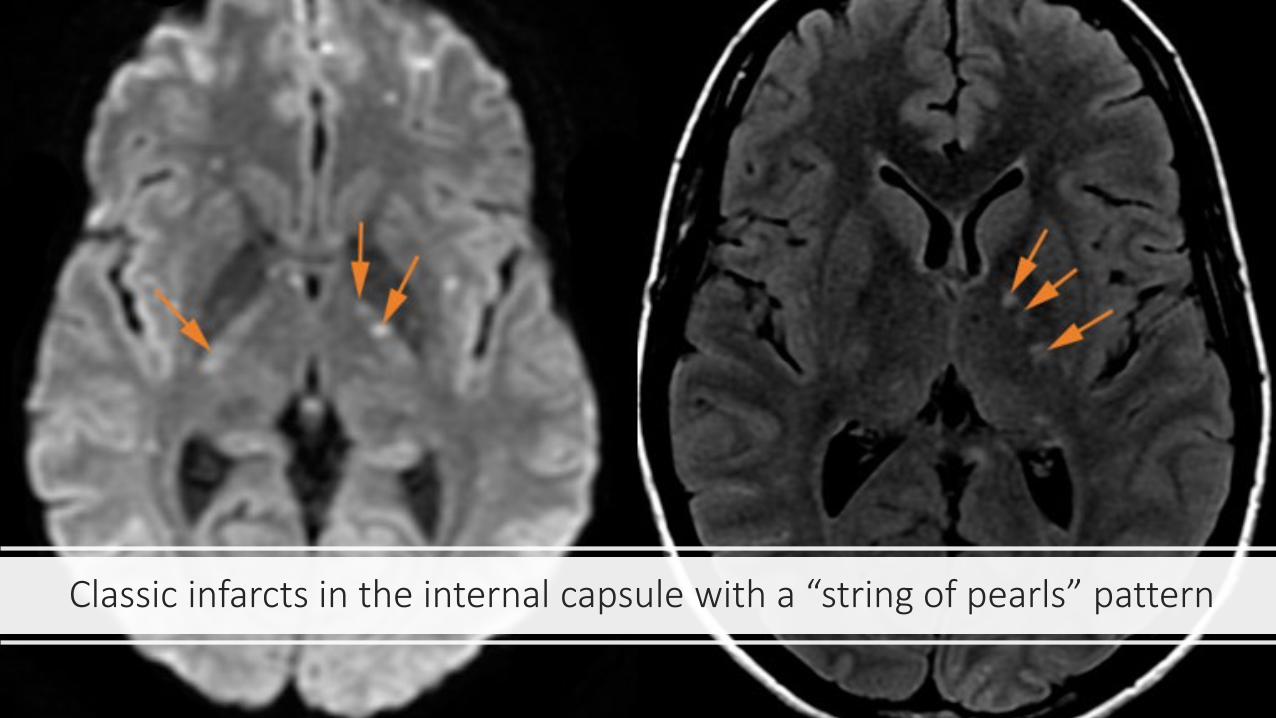
Classic infarcts in the internal capsule with a “string of pearls” pattern
Vasculitides
Vasculitides
• Characterized by inflammation and necrosis of the blood vessel wall
• Primary CNS vasculitis vs systemic vasculitis with involvement of the CNS
• Systemic vasculitis can be separated into 3 main groups based on if they affect predominantly large-sized vessels, medium-sized, or small-sized vessels
• Large vessels including the aorta are affected in giant-cell arteritis• Medium-size arteries in classic polyarteritis nodosa• The small-vessel vasculitides are separated in those with antineutrophil
cytoplasm antibodies (ANCA) and those without.
• Primary angiitis of the central nervous system (PACNS) affect both medium-and small-sized vessels
• Major symptoms of cerebral vasculitis are stroke, headache and encephalopathy
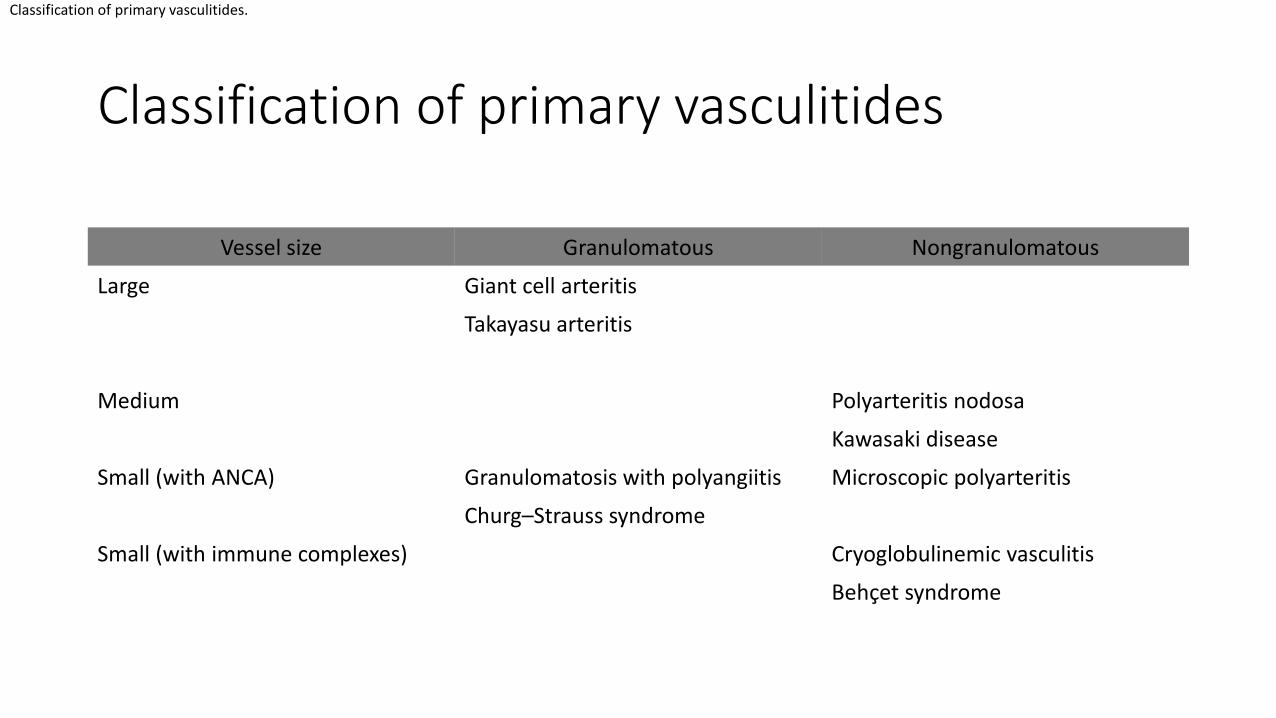
Classification of primary vasculitides
Vessel size Granulomatous Nongranulomatous
Large Giant cell arteritis
Takayasu arteritis
Medium Polyarteritis nodosa
Kawasaki disease
Small (with ANCA) Granulomatosis with polyangiitis Microscopic polyarteritis
Churg–Strauss syndrome
Small (with immune complexes) Cryoglobulinemic vasculitis
Behçet syndrome
Classification of primary vasculitides.

Symptoms
• Major symptoms of cerebral angiitis are stroke, headache, and encephalopathy.
• Other symptoms include seizures, cranial nerve palsies, or myelopathies.
• Elevated ESR/CRP is seen in systemic vasculitis • May include anemia, thrombocytosis, elevated liver
enzymes, and low complement • Complement consumption is seen in vasculitis with
immune complexes.
• In PACNS, serum findings usually are normal, but CSF studies reveal inflammatory findings (ie mild lymphomonocytic pleocytosis or protein elevation)
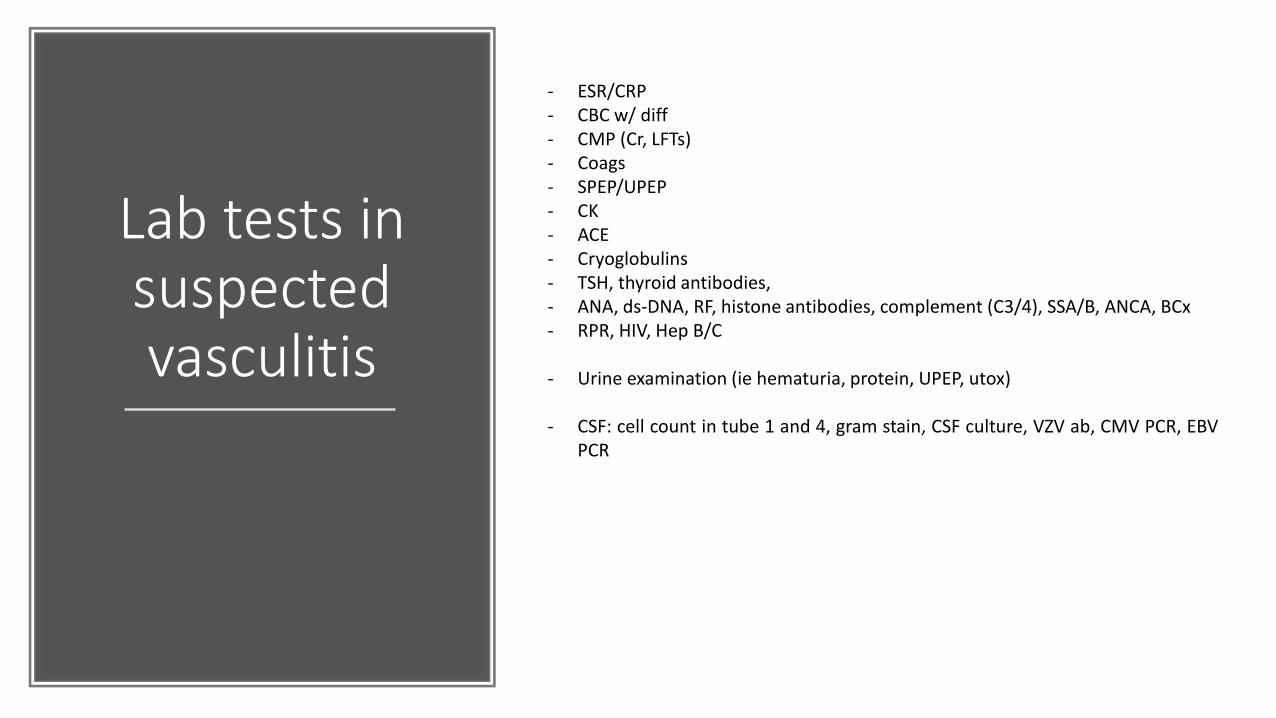
Lab tests in suspected vasculitis
- ESR/CRP- CBC w/ diff- CMP (Cr, LFTs)- Coags- SPEP/UPEP- CK- ACE- Cryoglobulins- TSH, thyroid antibodies,- ANA, ds-DNA, RF, histone antibodies, complement (C3/4), SSA/B, ANCA, BCx- RPR, HIV, Hep B/C
- Urine examination (ie hematuria, protein, UPEP, utox)
- CSF: cell count in tube 1 and 4, gram stain, CSF culture, VZV ab, CMV PCR, EBVPCR

Imaging
DSA
Carotid doppler
CTA
MRA
18-FDG PET is very sensitive in revealing inflamed vessels

Diagnostic criteria for the diagnosis of Primary Angiitis of the CNS
1 Acquired neurological deficit unexplained after complete evaluation
2 Diagnostic cerebral angiogram with narrowing of vessels, areas of dilationand/or beaded vessel appearance, displacement of vessels or vesselocclusions
3 No evidence of systemic vasculitis or any other condition that could mimicthe angiogram findings

Primary Angiitis of the CNS
• PACNS is more common in males (2:1)
• Onset most often occurs after 40 years of age
• ESR not helpful
• CSF inflammation is observed in ~90% of patients
• Histological findings are characterized by infiltrations of the vascular walls with mononuclear cells including lymphocytes, macrophages, and histiocytes

Large vessel vasculitidesTemporal ArteritisTakayasu Arteritis
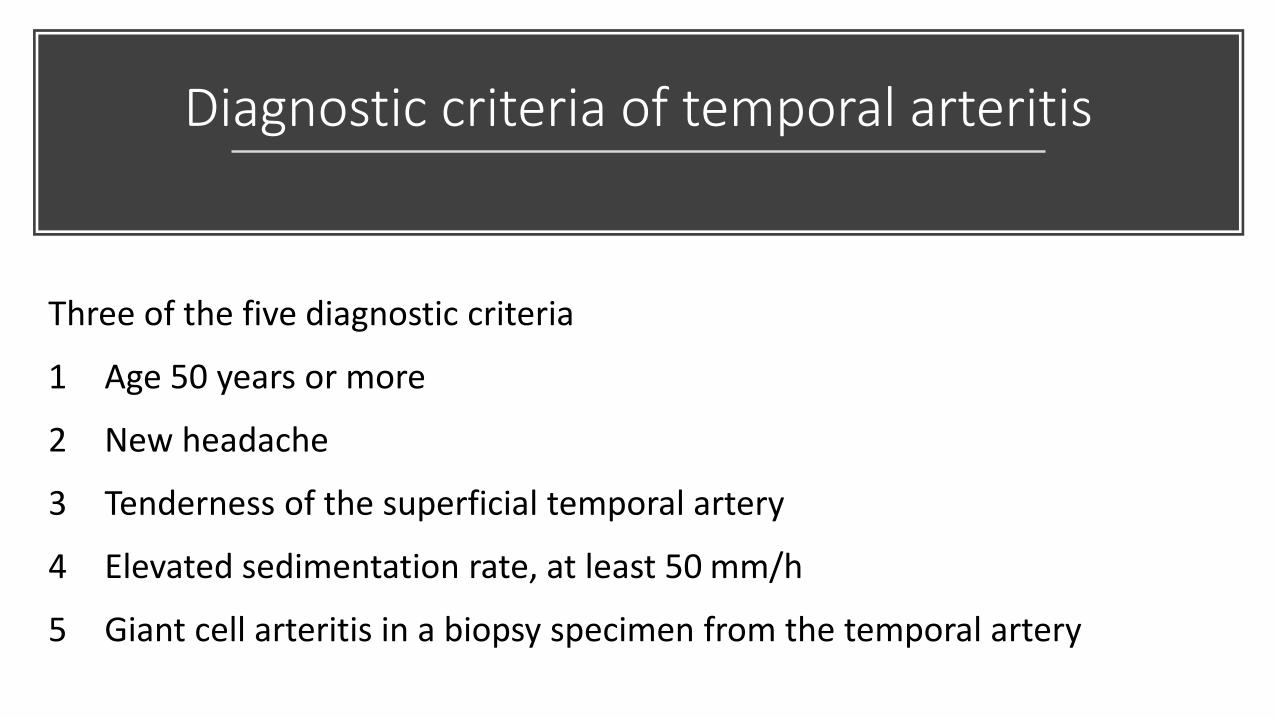
Diagnostic criteria of temporal arteritis
Three of the five diagnostic criteria
1 Age 50 years or more
2 New headache
3 Tenderness of the superficial temporal artery
4 Elevated sedimentation rate, at least 50 mm/h
5 Giant cell arteritis in a biopsy specimen from the temporal artery
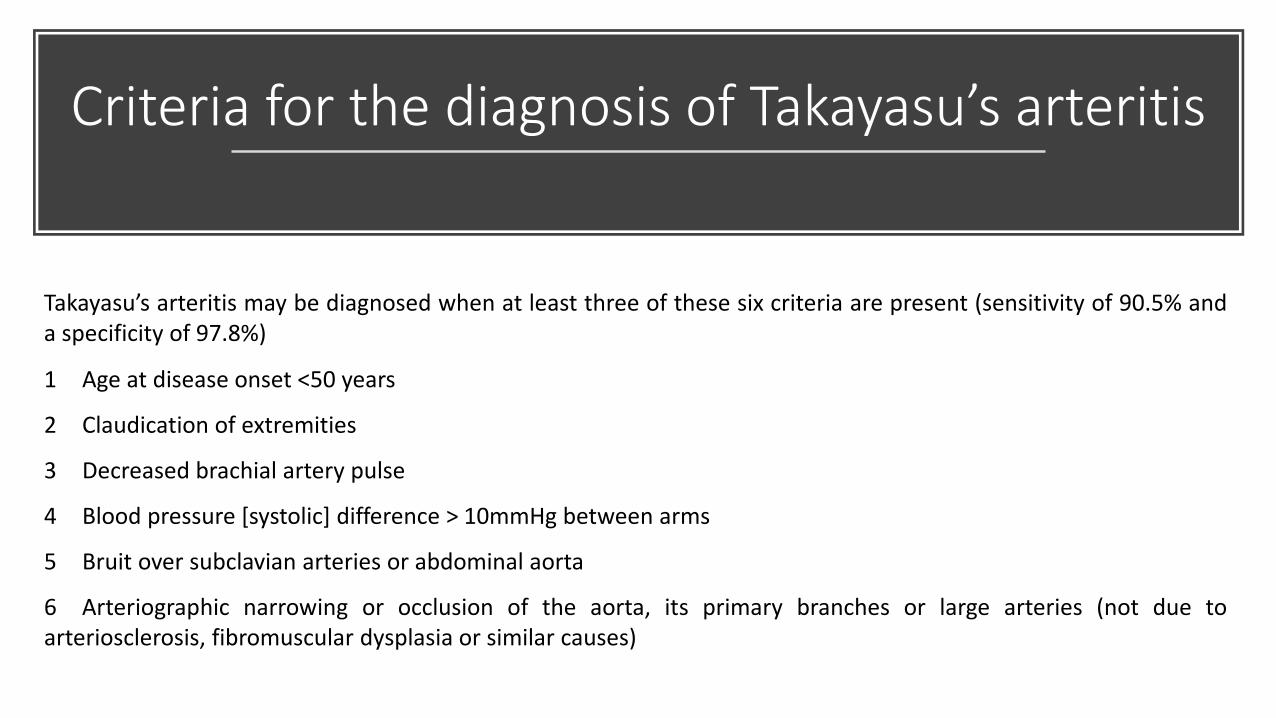
Criteria for the diagnosis of Takayasu’s arteritis
Takayasu’s arteritis may be diagnosed when at least three of these six criteria are present (sensitivity of 90.5% anda specificity of 97.8%)
1 Age at disease onset <50 years
2 Claudication of extremities
3 Decreased brachial artery pulse
4 Blood pressure [systolic] difference > 10mmHg between arms
5 Bruit over subclavian arteries or abdominal aorta
6 Arteriographic narrowing or occlusion of the aorta, its primary branches or large arteries (not due toarteriosclerosis, fibromuscular dysplasia or similar causes)

Medium vessel Vasculitides
Polyarteritis nodosa
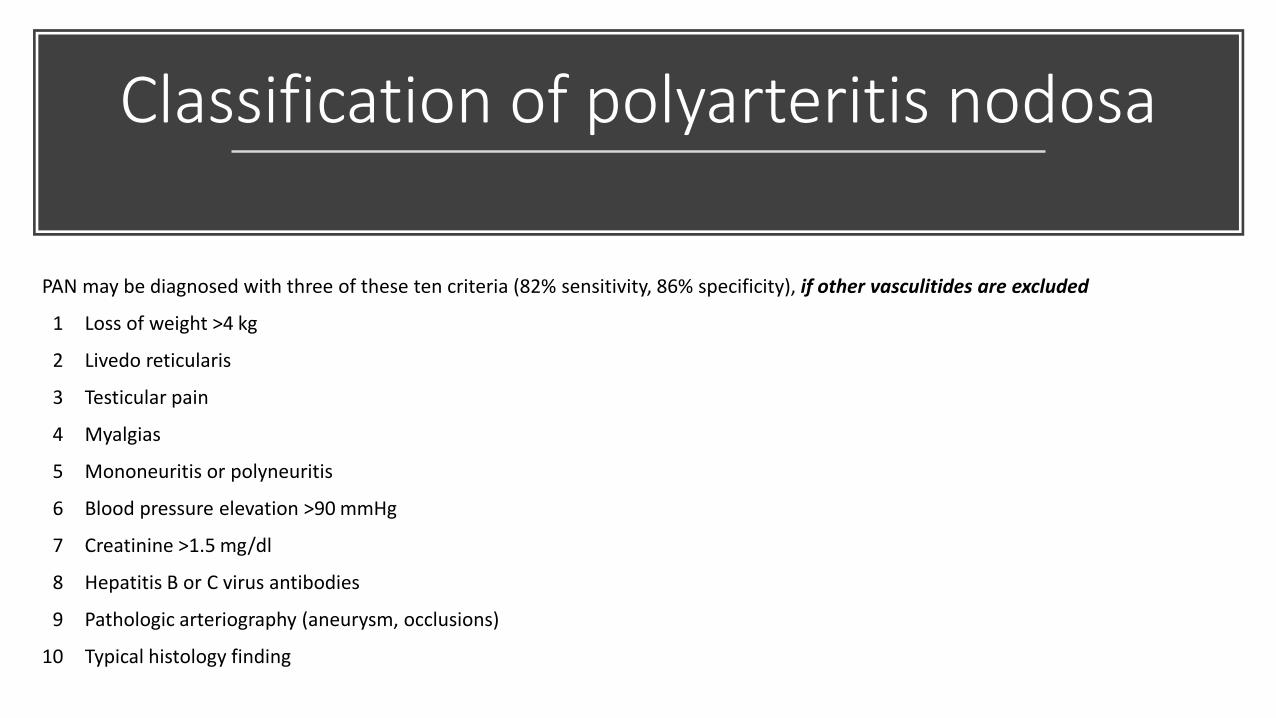
Classification of polyarteritis nodosa
PAN may be diagnosed with three of these ten criteria (82% sensitivity, 86% specificity), if other vasculitides are excluded
1 Loss of weight >4 kg
2 Livedo reticularis
3 Testicular pain
4 Myalgias
5 Mononeuritis or polyneuritis
6 Blood pressure elevation >90 mmHg
7 Creatinine >1.5 mg/dl
8 Hepatitis B or C virus antibodies
9 Pathologic arteriography (aneurysm, occlusions)
10 Typical histology finding

Small vessel vasculitidesGranulomatosis with
polyangiitisChurg–Strauss syndrome
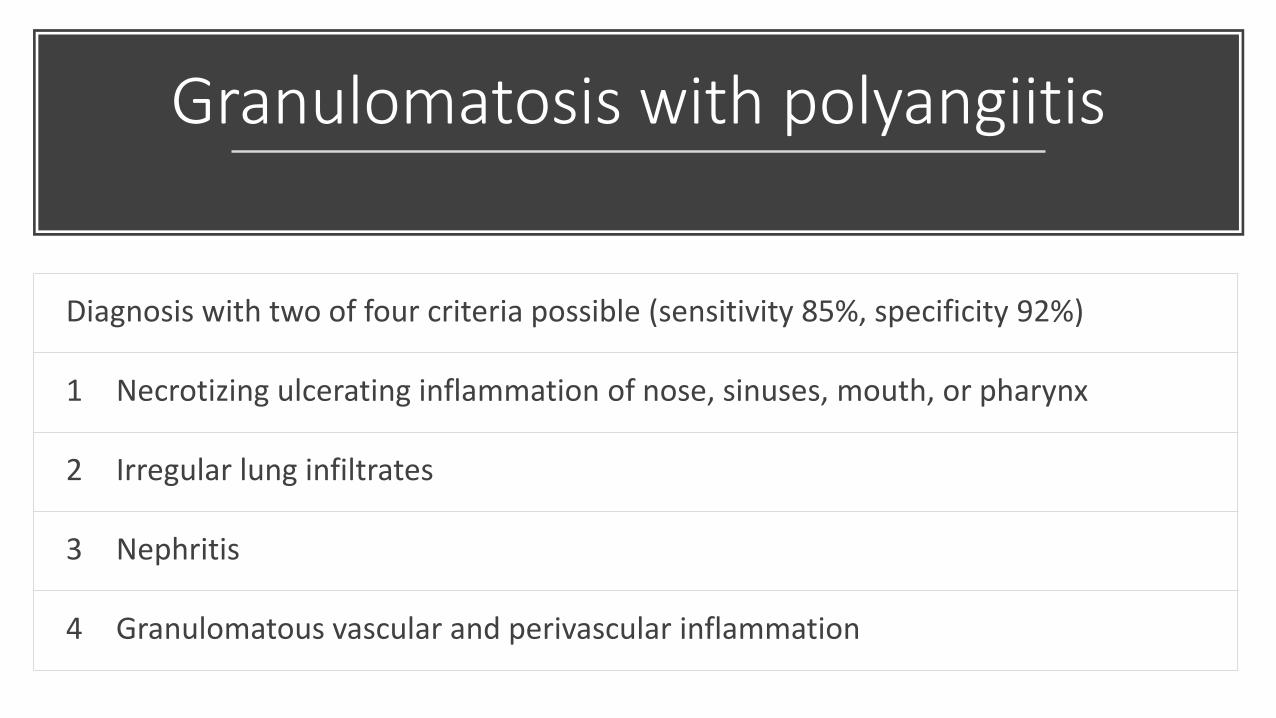
Granulomatosis with polyangiitis
Diagnosis with two of four criteria possible (sensitivity 85%, specificity 92%)
1 Necrotizing ulcerating inflammation of nose, sinuses, mouth, or pharynx
2 Irregular lung infiltrates
3 Nephritis
4 Granulomatous vascular and perivascular inflammation

Behçet’s disease
• Multisystem, chronic-relapsing vasculitis
• Recurrent oral ulcerations must be present with at least two of the following:
• recurrent genital ulceration, eye lesions (uveitis, cells in the vitreous on slit lamp examination or retinal vasculitis), erythema nodosum
• Diagnosis is purely clinical
• Recurrent oral and genital ulcers are frequently the only symptoms at the onset of the disease.
• CNS involvement (Neuro–Behçet) occurs in about 30% of patients after an average of 5 years.
• Brainstem is predominantly involved• Stroke, CN, and headache