varicose vein dr victor jesron nababan spbtkv 160116
TRANSCRIPT

Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam
PENGENALAN CAKUPAN BEDAH
TORAK, KARDIAK DAN VASKULER
TORAK TRAUMA
NON TRAUMA
NEOPLASMA DINDING DADA ORGAN INTRA TORAK
INFEKSI SPESIFIK/NON SPESIFIK
DEGENERASI PARENKIM PARU BLD
KELAINAN DINDING DADA
DIAFRAGMA
LAIN2 PALMAR HIPERHIDROSIS (TORAKAL SIMPATEKTOMI), RAYNAUD, TOS
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

KARDIAK JANTUNG PEDIATRI
KELAIANAN JANTUNG BAWAAN PDA, ASD, VSD, TOF, DORV, TA, DLL
KELAINAN JANTUNG DIDAPAT RHD, IE, DLL
JANTUNG DEWASA KORONER ON PUMP, OFF PUMP KATUB ARYTMIA SURGERY MAZE PACE MAKER PERMANENT ASSIST DEVICE IABP, ECMO, LVAD, RVAD, BIVAD AORTA TORAKAL DHCA NEOPLASMA MYXOMA EMBOLI PARU PENYAKIT PERICARD TRAUMA
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

VASKULER TRAUMA
NON TRAUMA VENA CVD (VARICES, CVI), DVT, MAY
TURNER, DLL
ARTERI ANEURISMA, PSEUDOANEURISMA, PAPO, DIABETIC FOOT ULCER
AORTA TAA, AAA
MALFORMASI ARTERIO VENOUS
AKSES VAKULER CENTRAL, PERIFER, HD AKSES (AV SHUNT, HD CATHETER), CHEMOPORT
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

VICTOR JESRON NABABAN,MDCARDIOTHORACIC AND VASCULAR SURGEON

Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

Background Chronic venous disorders include a spectrum of
clinical manifestations extending from telangiectasias & varicose veins to lipodermatosclerosis & ulceration.
Varicose veins are the most common manifestation of primary chronic venous disease.
varicose veins are usually differentiated from reticular veins and telangiectasias
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

Terminology & New definition CVD, chronic venous disorders: embraces C1–C6.
CVI, chronic venous insufficiency: limited to C3–C6.
Telangiectasias:a confluence of dilated intradermal venules of less than 1 mm in caliber. Synonyms include spider veins, hyphen webs, and thread vein
Reticular veins: dilated bluish subdermal veins usually from 1 mm in diameter to less than 3 mm in diameter. They are usually tortuous.
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

Definition
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

Epidemiology Varicose veins are present in 25% - 33% & chronic venous
insufficiency, with skin changes and ulceration, in 2% -5% of Western populations.
The prevalence of VV increases markedly with age and they are an almost universal finding in individuals over the age of 60 years.
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

Valvular Function in V V’sHealthy Diseased
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

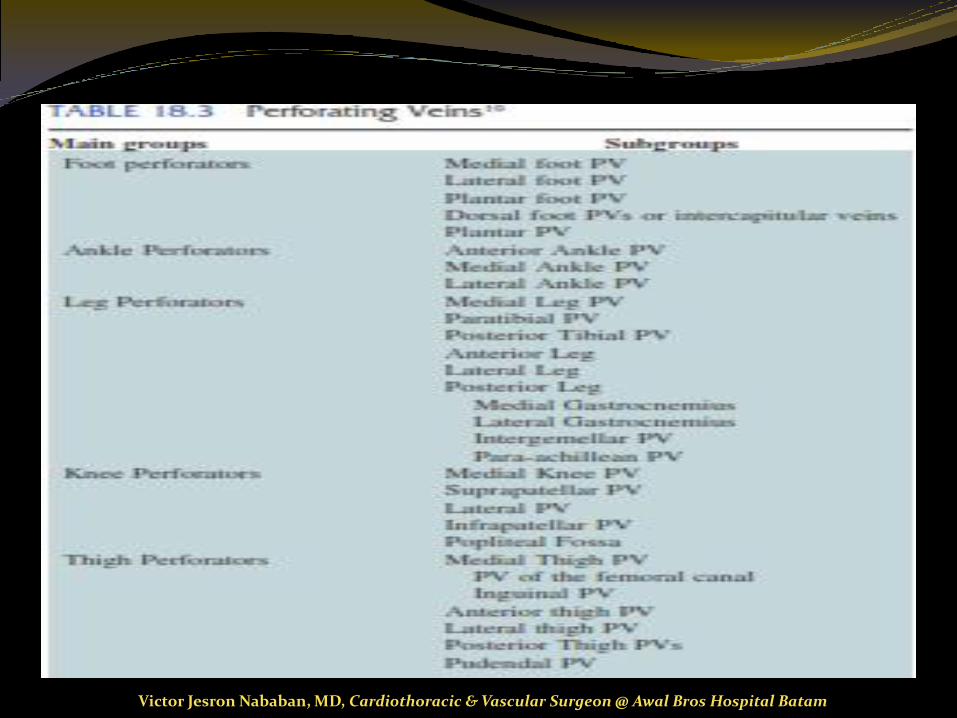
2 venous drainage systems: deep and superficial
Superficial: long and short saphenous veins
Superficial connects to deep system via perforators
Saphenofemoral junction 2-4cm inferolateral to pubic tubercle
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

The CEAP Classification C linical Classification
E tiological Classification
A natomical segmental localization
P athophysiological classification
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

Revisi CEAP tahun 2004
Class-0
...kalau periksa jangan lama lama.....
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

CEAP Class 1
Hanya nampak
varises kapilaris
atau retikularis saja
Class-1
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam
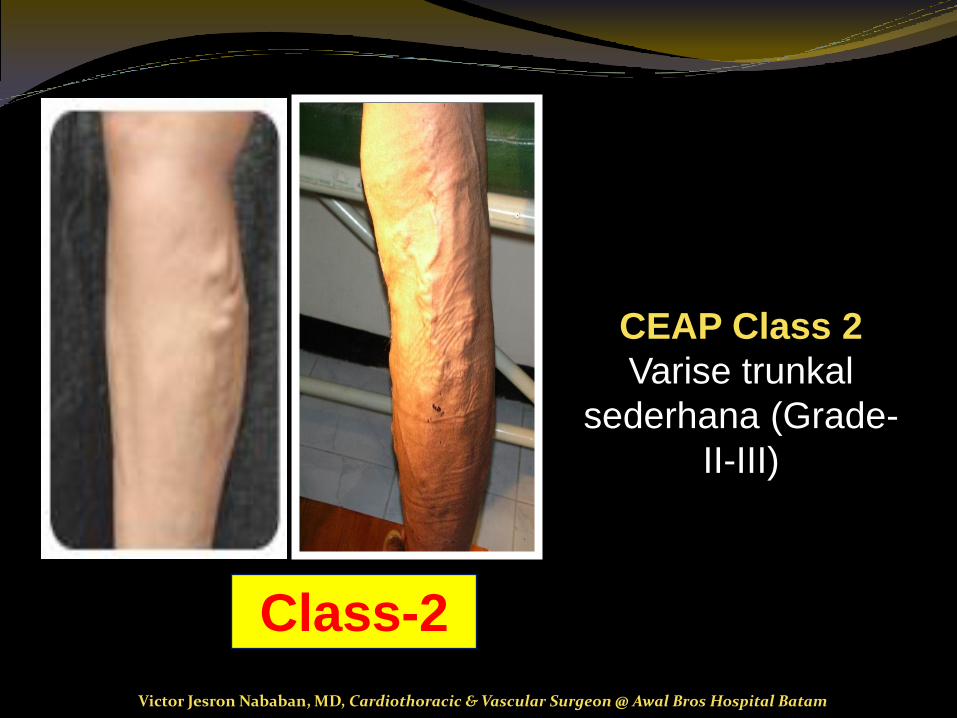
CEAP Class 2
Varise trunkal
sederhana (Grade-
II-III)
Class-2
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

CEAP Class 3Edema ankle/ malelolus
kearah proksimal .
Kongesti venous
karena inkompetensi
vena safena dapat
menyebabkan edema
ortostatik.
Class-3
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

CEAP Class 4
Pigmentasi kulit
tungkai bawah medial
(lipodermatosklerosis).
Deposit hemosiderin
menentukan warna
perubahan kulit dan
bisa menjadi tanda
keradangan kronis
yang menyebabkan
proses fibrosis
Class-4
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

CEAP Class 5Ulkus venous yang
MENYEMBUH .
Kenaikan tekanan vena
menyebabkan hipoksia
jaringan yang
menyebabkan
kerapuhan kulit dan
terjadi ulserasi.
Class-5
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

CEAP Class 6Ulkus venous
terbuka/ aktif. ulcer.
Hipertensi venous
menyebabkan
periubahan gradien
tekanan yang
menyebabkan
ulkus.
Class-6
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

Beware : CEAP-6 in a diabetic
patientTreated (personally) with
diabetic wound dressing....
(more than 2 months)
Then treated with Pasta-Unna
wound dressing.... (2 weeks)
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

Risk Factors
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

Symptoms Great majority of individuals with VV are
asymptomatic
A wide variety of lower limb symptoms have been attributed to VV. These include: 1. aching
2. heaviness and tension
3. a feeling of swelling
4. tiredness
5. restless legs
6. nocturnal cramps
7. itching.
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

Physical Examination
Position
The patient should be examined standing in a good light in a warm room.
Inspection
dilated, elongated, tortuous, and sacculated vein
signs of CVI include
corona phlebectatica,
lipodermatosclerosis, and
open ulceration
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

Physical Examination (1)
Palpation
Percussion over a varix while palpating with the other hand at a higher or lower level will help trace out the pattern (the “tap” test of Chevrier).
Particularly helpful in the obese.
There may be a cough impulse, even a thrill over a large varix, particularly a saphena varix in the groin.
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

Physical Examination (2)
Tredelenburg Test
Purpose: to identify the level and location of deep to superficial reflux.
Value in circumstances in which duplex scanning is not readily available.
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

Physical Examination (3)
Tredelenburg Test The test comprises two parts : Part 1:
The patient lying down the leg is elevated to 45° and
A tourniquet or the examiner’s hand compresses the GSV in the high thigh.
With compression in place, the patient stands in a well-lit room.
Previously noted superficial veins are then carefully observed for filling with blood
Part 2:
The compression is then released.
The superficial veins are then carefully observed for increased filling with blood.
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

Physical Examination (4)
Interpretation of Tredelenburg Test
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam
Physical Examination (3) Ulcer Examination
This should include
1. a description of the ulcer, concentrating on the
2. pulse status and ankle–brachial index
3. gait and, in particular, ankle mobility
4. general physical examination
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

Diagnostic Tools
Diagnostic Vascular Laboratory Non invasive test
Indirect : Plethysmography is used in the assessment of the amount of reflux, the efficiency of the calf muscle
pump, and obstruction.
Direct: Duplex scan can determine the presence of anatomic obstruction with a sensitivity and specificity
of over 90%
Radiologic Imaging Computed tomography or (MRI)
Invasive Phlebography
IVUS
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

RULE # 1
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

RULE # 2
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

Sign of the egyptian EYE
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

Management
Medical Ablation
Compression
Sclerotherapy
Drugs
Surgery
Percutaneous Laser
RF ablation
Stripping
Babcock excision
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

Medical Management Compression tx standard first-line treatment for CVI and venous ulcer
Goal: to facilitate ulcer healing, provide rapid ulcer healing, and prevent recurrence
Including: elastic compression stockings,
paste gauze boots (Unna’s boot),
and multilayer wraps,dressings, and bandages.
Pneumatic compression devices
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

Medical Management Drugs treatment No drug will cure varicose veins, although some drugs benefit
venous edema & ulceration.
Some phlebotonic drugs improve the symptoms and edema associated with venous disease. These could be used in association with compression for the management of troublesome symptoms.
Drugs for venous ulcer: Fibrinolytic tx
Drugs that modify Leukocyte metabolism
Platelet inhibitors
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam
Medical Management Sclerotheraphy Indication: Superficial venules, “venous spiders” (veins < 1 mm of internal
diameter), venous lakes, and other venous blemishes.
Varicosities 1–3 mm in diameter in the absence of detectable valvularreflux as evidenced by duplex examination.
Postoperative residual veins are those < 3 mm in Ø that the surgeon chose not to excise in order to limit the number of incisions.
Incompetent perforating veins (< 4 mm)
Bleeding varicosities (varicorrhage)
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

Medical Management Sclerotheraphy
Contraindication:
Pregnancy
Elderly and sedentary patients
Generalized, severe systemic disease
Advanced rheumatic disease, osteoarthritis or any disease of the musculoskeletal system that interferes with the patient’s mobility.
Arterial insufficiency of the lower extremities
Patients with history of severe allergic disease or bronchial asthma
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

Medical Management Sclerotheraphy
Contraindication:
Febrile illnesses
Acute superficial thrombophlebitis or deep vein thrombosis
Obesity.
Varicose veins in communication with a source of venous reflux, demonstrated by duplex ultrasound,
Patients on anticoagulants
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

Medical Compression Stockings
CLINICAL
SITUATIONS
COMPRESSION in mmHg
10-20 20-30 30-40
C0s, C1s
C1 Post-Injections
C2s Pregnancy
C3 Prevention
C4b
C5
C6
The efficacy of MCS have been proved in a lot of
clinical situations, even leg ulcers
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

Surgical Management 3 principle goals The varicosities must be permanently removed and the
underlying cause of venous hypertension treated the repair must be done in as cosmetic a fashion as possible complications must be minimized.
Indication: Truncal varicose vein gr III-IV
Contraindication Pts with VTE Pts with anesthetic complication
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

Surgical Management Early Complication:
discomfort
bruising
bleeding
wound infections
deep venous thrombosis
nerve injury
Technique: Stripping GSV or SSV
Phlebectomy
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

PHLEBECTOMY
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

Main RULES Phlebectomy
1. Small incisions (1-2 mm)2. Longitudinal3. Hooks4. Steristrips5. compression
Phlebectomy can replace all the component parts of
the operation except flush ligation
Good practical experience is necessaryCan rescue the operation
Spare wheel
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

• Simplifies Surgery (recurrences)
• Makes it less traumatic
• Goes where surgeon cannot go:
• lympho-nodal networks of the groin
• Deep and long, dystrophic perforators
• Recurrent VV inside the saph. compartment
* Creton D. et Uhl JF EJVES 1998;15:412-5
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

70 incisions
Mean number : 30 incisions per operation
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

Endoluminal radiofrequency/laser ablation of the great saphenous vein: methods
Photograph courtesy of VNUS medical Technologies, San Jose, CA.
Percutaneous access to the greater saphenous vein most commonly at the level of the knee under duplex ultrasound guidance
Bola Pratt P&S MS 4
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

Endoluminal radiofrequency ablation of the great saphenous vein: methods
Photographs courtesy of VNUS medical Technologies, San Jose, CA.
1) A guidewire is then advanced to the saphenofemoral junction over which the closure catheter is passed
2) catheter prongs are extruded tocontact the intimal lining of the vessel wall
3) radiofrequency generator allows the tip of the catheterand the prongs to attain a temperature of 85 degrees C.
CFA = common femoral arteryCFV = common femoral veinSEV= superficial epigastric veinSFJ = saphenofemoral junction
Bola Pratt P&S MS 4
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

FEMORAL BLOCK
EPIDURAL - SPINAL
GENERAL anesthesia
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam
TUMESCENT
anesthesia
The best technique +++++
Only one technique
For varicose veins surgery
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam
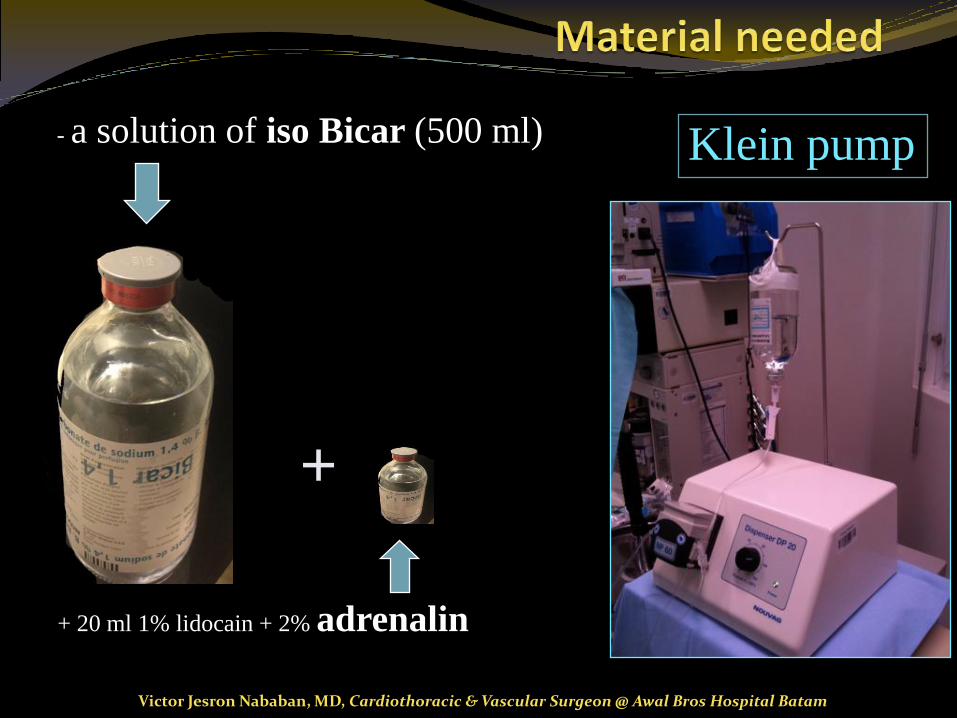
- a solution of iso Bicar (500 ml) Klein pump
+
+ 20 ml 1% lidocain + 2% adrenalin
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

Take home message
Anesthesia by Blocks possible but
Tumescent Anesthesia is the best ++
Avoid general or peridural anesthesia For GSV surgery
risk, bleeding , early walk
quick return to normal activity +++
complication nerve injury
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam

Thank you!Any Questions?
Victor Jesron Nababan, MD, Cardiothoracic & Vascular Surgeon @ Awal Bros Hospital Batam