valvular heart disease - seton.net · valvular heart disease mark j. pirwitz, m.d., f.a.c.c....
TRANSCRIPT

ValvularHeartDisease
MarkJ.Pirwitz,M.D.,F.A.C.C.President/C.E.O.,SetonHeartInstitute
PhysicianExecutive,CardiovascularServiceLine,SetonHealthcareFamily
ChiefofDivisionofCardiology,AssistantProfessorDepartmentofMedicine,UniversityofTexasDellMedicalSchool

PrevalenceofValvularHeartDisease
• PrevalenceinU.S.A=2.5%– 0.7%age18-44– 13.3%overage75
• Epidemiologyhaschangedsignificantlyoverpast50years• Declineinrheumaticheartdisease• Steadyincreaseinlifeexpectancyresultinginmore
degenerativevalvedisease

RelativeDistributionofNativeHeartValveDisease
Heart,Lung,B.,Volume94,519–524,©2008

EtiologyofValvularHeartDisease
Iung,B.&Vahanian,ANat.Rev.Cardiol.10.1038/nrcardio.2010.202

AorticStenosis

RiskFactorsforDevelopmentofCalcificAorticStenosis
§ Increasingage§ Malegender
§ Hypertension§ Smoking
§ Elevatedlipoprotein(a)§ ElevatedLDLcholesterol

AorticStenosis-NaturalHistory
OttoCM.Timingofaorticvalvesurgery.Heart.2000;84:211-21.
• Survivalafteronsetofsymptomsis50%at2yearswithoutintervention

5YearSurvivalRates
23
4
12
30 28
3 0
5
10
15
20
25
30
35
BreastCancer
LungCancer
ProstateCancer
OvarianCancer
SevereInoperableAS
ColorectalCancer
NationalInstitutesofHealth.NationalCancerInstitute.SurveillanceEpidemiologyandEndResults.CancerStatFactSheets.
Survival,%

ManagementofAsymptomaticAorticStenosis
• AsymptomaticpatientswithAShaveoutcomessimilartoage-matchednormaladults.
• Treatmentofconcomitanthypertensionandhyperlipidemia• Nospecificmedicaltherapyhasbeenshowntoslowprogressionof
diseaseprocess• PhysicalactivityisnotrestrictedinasymptomaticpatientswithmildAS;
thesepatientscanparticipateincompetitivesports.PatientswithmoderatetosevereASshouldavoidcompetitivesports.
• BaseduponACCguidelines,echocardiographyisrecommendedfor:– re-evaluationofpatientswithknownASandchangingsymptomsorsigns– re-evaluationofasymptomaticpatients:everyyearforsevereAS;every1to2
yearsformoderateAS;andevery3to5yearsformildAS.

AorticStenosis–ProgressiontoSymptomaticDisease
Study,year #ofpatients SeverityofAS Event-freesurvivalwithoutsymptoms
Kelly,etal.1988 51 Vmax>3.6m/s 59%at15months
Rosenhek,etal.2000 128 Vmax>4.0m/s 67%at1year
Das,etal.2005 125 AVA<0.8cm2 46%at1year
Pellikka,etat.2005 622 Vmax>4.0m/s 82%at1y67%at2y33%at5y

SurgicalTreatmentforAorticStenosis
0
10
20
30
40
50
60
70
80
90
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Sur
viva
l, %
AVR, Sx
No AVR, Sx
BrownML,PellikkaPA,SchaffHV,etal.JThoracCardiovascSurg.2008;2:308-315.
• InsymptomaticpatientswithAS,AVRimprovessymptomsandimprovessurvival.• Intheabsenceofseriouscomorbidconditions,AVRisindicatedinvirtuallyallsymptomaticpatients
withsevereAS.• AverageperioperativemortalityintheSTSdatabaseis3.0%to4.0%forisolatedAVRand5.5%to6.8%
forAVRplusCABG

TypesofValveProstheses
• Mechanical– Ballandcage(Starr-Edwards);singletiltingdisc(Medtronic-Hall);bileaflet(St.
Jude,Carbomedics)– Durablewithlowratesofmechanicalfailure– Generallyhemodynamicallyefficientexceptinsmallsizes– Requireslong-termantithrombotictherapy(INR2.5-3.5x3months,then2-3
thereafter)• StentedHeterograft
– Bovinepericardialorporcineaorticvalvetissue– Imperfecthemodynamicefficiency– Lowriskofthromboembolismwithoutcoumadin(<0.7%/yr)
• StentlessHeterograft– Stentlessporcinevalvetissue– Enhancedhemodynamicefficiency– Lowthromboembolicrisk

StructuralDeteriorationofBioprostheticValvesAuthor,Yr ValveType TimeofSVD PatientAge,Yr FreedomfromSVD,
%
Jamieson,1988 Porcine 10 30-59 81
Burr,1992 Porcine 13-15 <65 62
65-69 98
70-79 95
Pelletier,1995 Pericardial 10 <60 86
60-69 95
>70 100
Banbury,2001 Pericardial 15 55 70
65 82
75 91

ProportionofPatientswithSevereAorticStenosisTreatedwithAVR
Only26-57%ofpatientswithsevereASultimatelyundergoAVR
TAVR–TranscatheterAorticValveReplacement
• Forpatientswhoareeitherathigh/prohibitiveorintermediateriskforopen-heartsurgery,TAVRmaybeanalternative
• Thislessinvasiveprocedureallowstheaorticvalvetobereplacedwithanewvalvewhiletheheartisstillbeatingusingcatheter-basedtechniques

EdwardsSAPIENTranscatheterHeartValve
Bovinepericardialtissue
PETskirtStainlesssteelframe
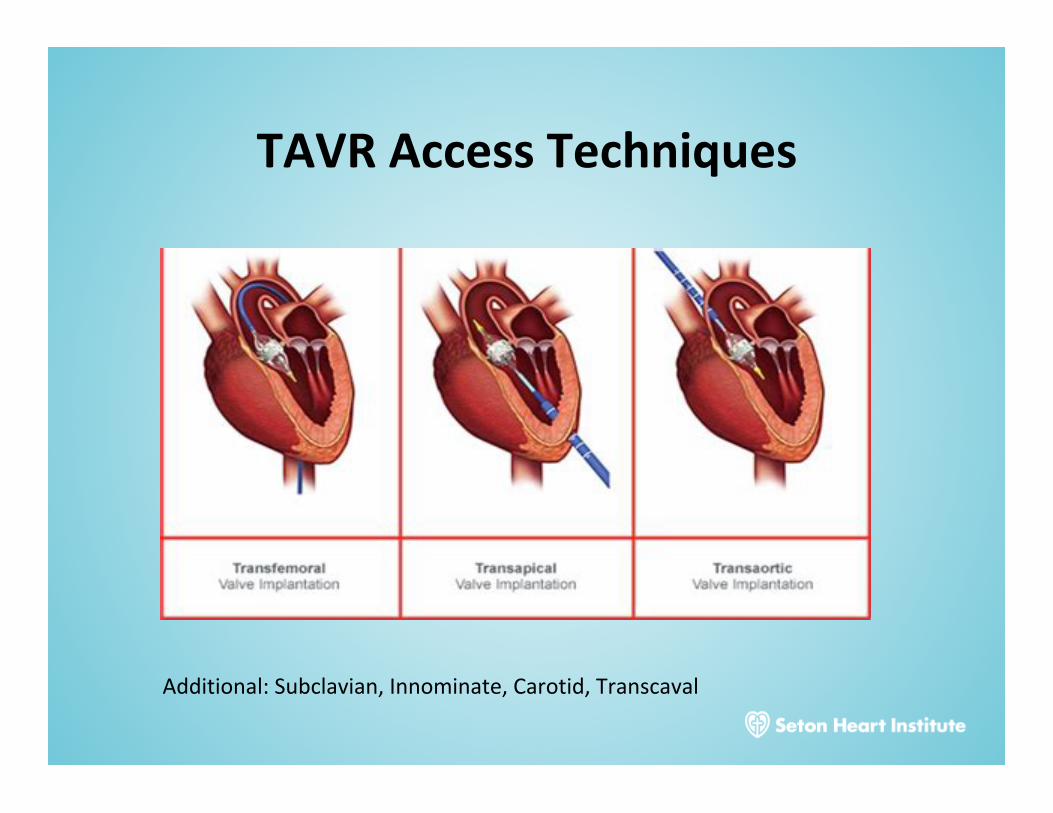
TAVRAccessTechniques
Additional:Subclavian,Innominate,Carotid,Transcaval
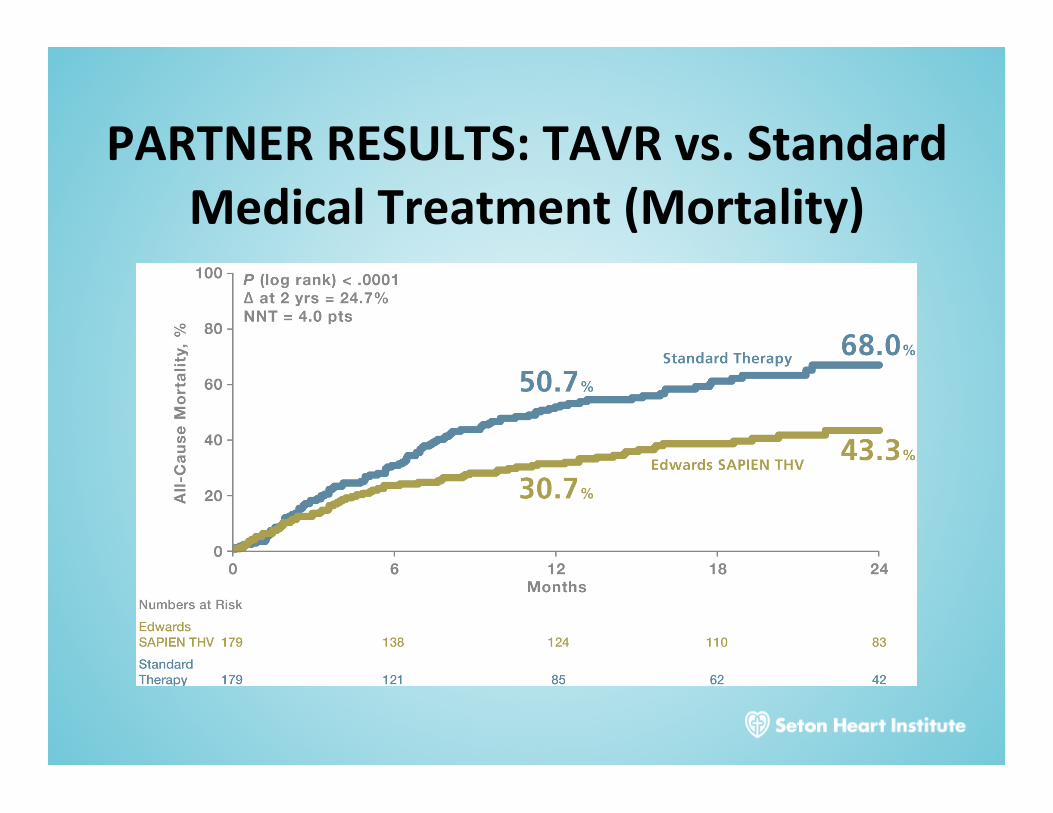
PARTNERRESULTS:TAVRvs.StandardMedicalTreatment(Mortality)
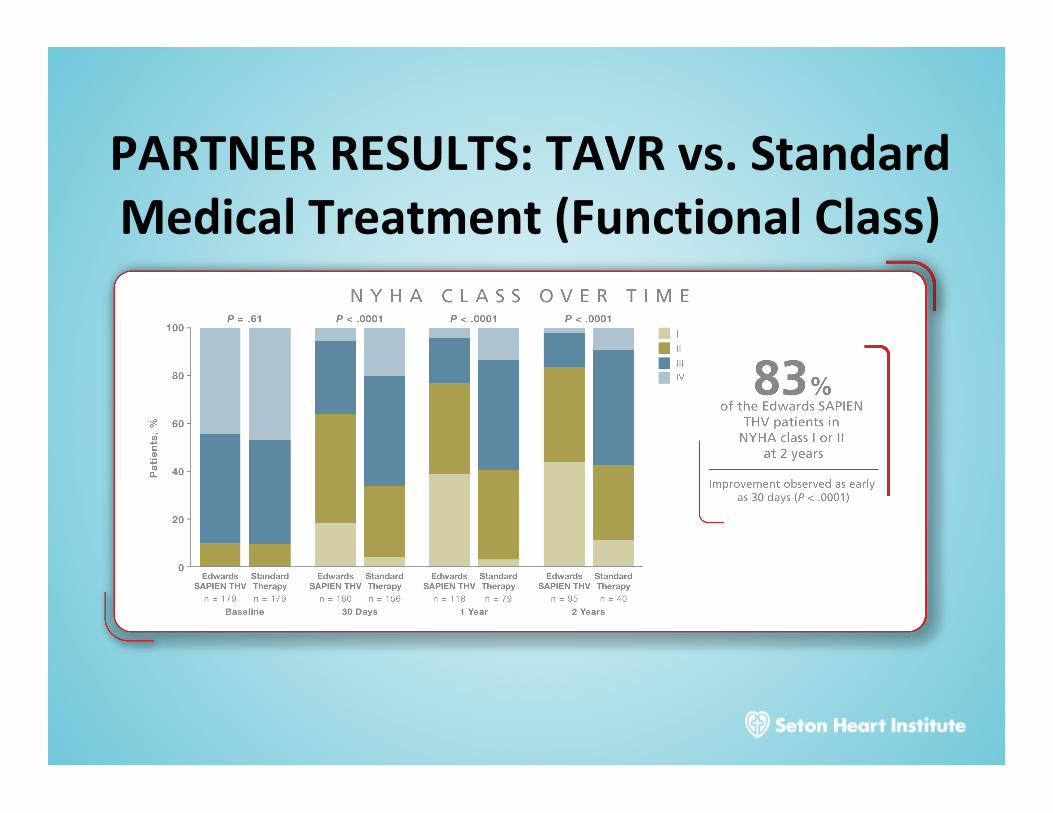
PARTNERRESULTS:TAVRvs.StandardMedicalTreatment(FunctionalClass)
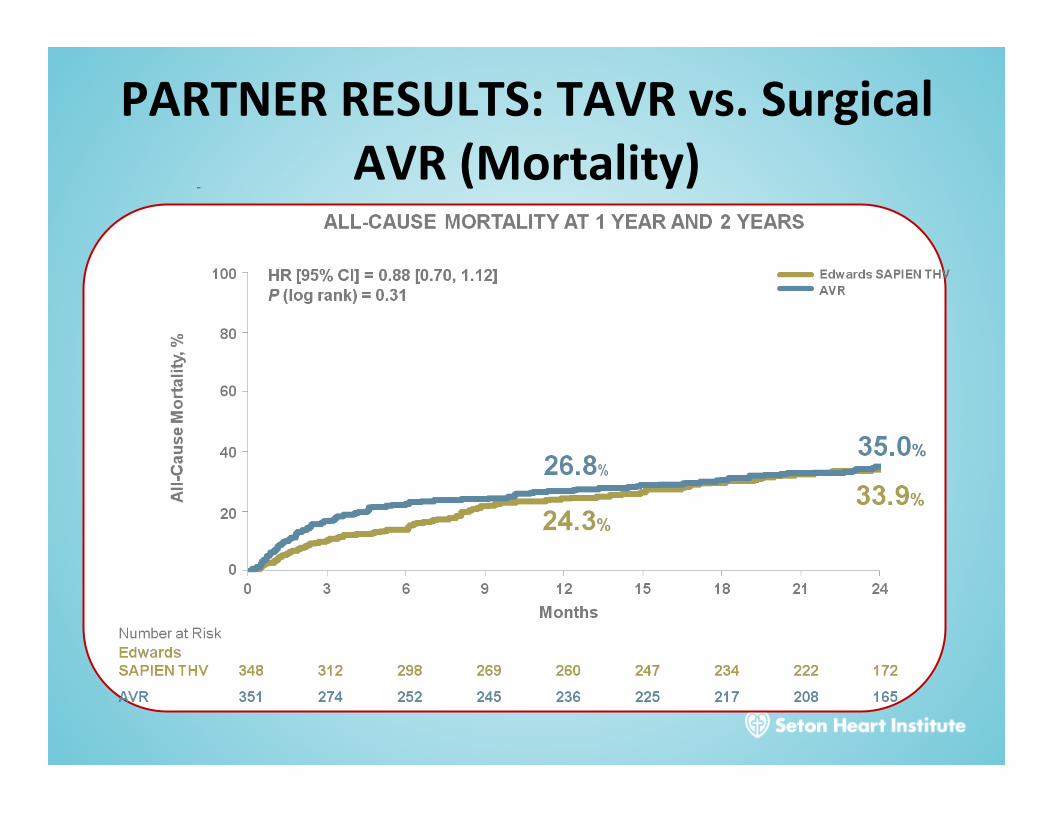
PARTNERRESULTS:TAVRvs.SurgicalAVR(Mortality)

TAVRinIntermediateRiskAorticStenosisPatients
• PARTNER2ATrialrandomized2032intermediateriskpatientstoTAVRorSAVR
• TAVRnon-inferiortoSAVRwithregardtomortalityordisablingCVAat2years(19.3%vs.21.1%)
• LowerratesofAKI,Afib;largerAVA;shorterlengthofstaywithTAVRvsSAVR
MBLeon,etal;NEJM4/2/16

SetonHeartInstituteValveProgramYear Volume
2014 11
2015 29
2016 47
2017 79
24
InHospitalMortality 1.3%(1.5%)
MajorBleeding 1.3%(1.7%)
LOS 1.9d(1.9)(6din2015)
CVAat30d 1.3%(2.0%)
>mildPVLat30d 0%(1.2%)
30dReadmission 11.4%(7.7%)
Rolling4QuarterClinicalOutcomes

AorticInsufficiency-Etiology
• idiopathicdilatationoftheaorta• congenitalabnormalitiesoftheaorticvalve(mostnotablybicuspidvalves)• calcificdegeneration• rheumaticdisease• infectiveendocarditis• systemichypertension• myxomatousdegeneration• dissectionoftheascendingaorta• Marfansyndrome• traumaticinjuriestotheaorticvalve• ankylosingspondylitis• syphiliticaortitis• rheumatoidarthritis

AcuteAorticInsufficiency
• Diagnosis– Newdiastolicmurmur,tachycardia,rales– Pulsepressuremaynotbeincreasedbecausesystolicpressureis
reducedandtheaorticdiastolicpressureequilibrateswiththeelevatedLVdiastolicpressure
– LVsizeisusuallynormalonexam,CXR,echo– Echocardiographyisindispensableinconfirmingthepresenceand
severityofthevalvularregurgitationanddeterminingitscause– Ifdissectionissuspected,TEE/CT/MRIisindicated
SuddenLargeRegurgitantVolume
Tachycardia,Hypotension,PulmonaryEdema
AbruptIncreaseinLVEDPwithDecreased
ForwardStrokeVolume

AcuteAorticInsufficiency-Treatment
• Deathduetopulmonaryedema,ventriculararrhythmias,electromechanicaldissociation,orcirculatorycollapseiscommoninacutesevereAI
• Urgentsurgicalintervention• Nitroprussideforacuteafterloadreduction• Dopamine,dobutaminetoaugmentforwardflow• IABPiscontraindicated• CareshouldbetakenifB-blockersusedinthesettingof
dissectionasthismayblockcompensatorytachycardia

ChronicAorticInsufficiency
• Diagnosis– Diastolicmurmur,displaceLVimpulse,widepulsepressure,S3– LVsizeisusuallyenlargedonexam,CXR,echo– Echocardiographytoconfirmthepresenceanddeterminetheseverity
ofthevalvularregurgitation,assessaorticrootsize,andevaluateLVfunction
SlowIncreaseinRegurgitantVolume
Initially,MaintenanceofForward
StrokeVolumeandLVEDP
IncreaseinEnd-DiastolicVolumeand
LVCompliance
IncreasedAfterloadResults
inImpairedContractility,
ElevatedLVEDP
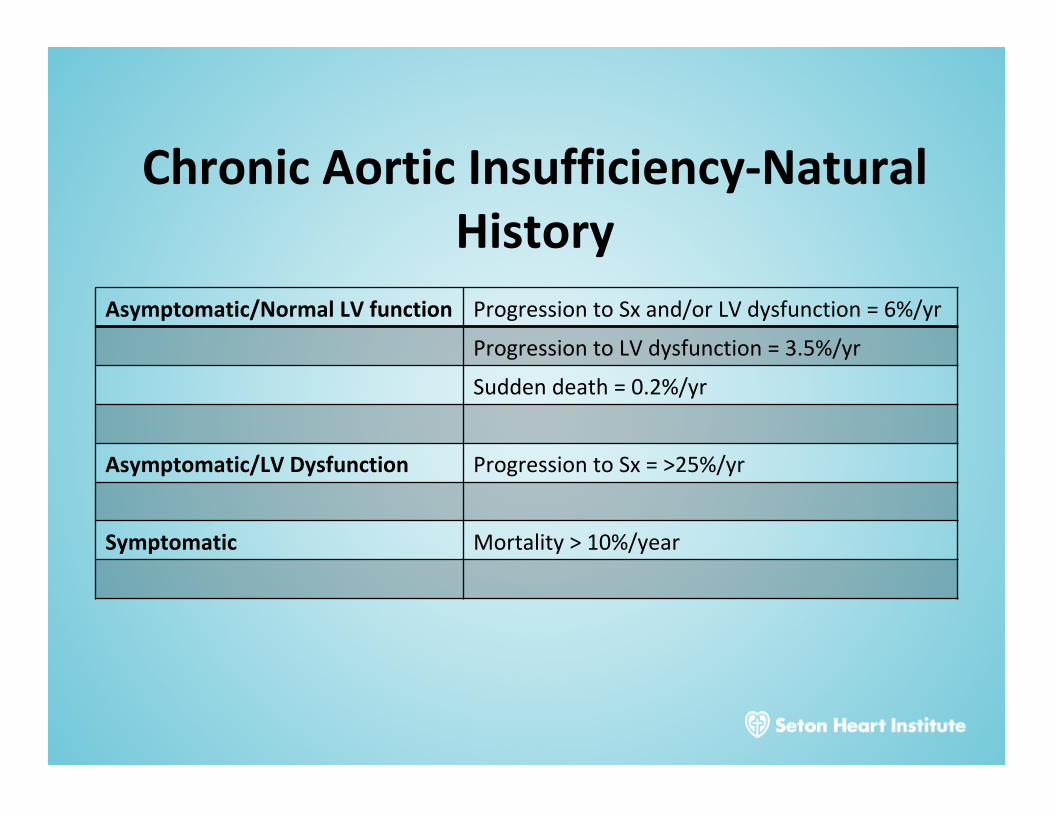
ChronicAorticInsufficiency-NaturalHistory
Asymptomatic/NormalLVfunction ProgressiontoSxand/orLVdysfunction=6%/yr
ProgressiontoLVdysfunction=3.5%/yr
Suddendeath=0.2%/yr
Asymptomatic/LVDysfunction ProgressiontoSx=>25%/yr
Symptomatic Mortality>10%/year


ChronicAorticInsufficiency-MedicalTherapy
• VasodilatortherapyisindicatedforchronictherapyinpatientswithsevereARwhohavesymptomsorLVdysfunctionwhensurgeryisnotrecommendedbecauseofadditionalcardiacornoncardiacfactors.
• Vasodilatortherapyisreasonableforshort-termtherapytoimprovethehemodynamicprofileofpatientswithsevereheartfailuresymptomsandsevereLVdysfunctionbeforeproceedingwithAVR
• Maybeconsideredforlong-termtherapyinasymptomaticpatientswithsevereARwhohaveLVdilatationbutnormalsystolicfunction– 2smallstudies(Nifedipinevs.Digoxin;Nifedipinevs.Enalaprilvs.placebo)
• Vasodilatortherapyisnotindicatedfor:– asymptomaticpatientswithmildtomoderateARandnormalLVsystolic
function– asymptomaticpatientswithLVsystolicdysfunctionwhoareotherwise
candidatesforAVR– SymptomaticpatientswitheithernormalLVfunctionormildtomoderateLV
systolicdysfunctionwhoareotherwisecandidatesforAVR
MitralStenosis
• Etiology– Predominatelyduetorheumaticcarditis.Lesscommonlycongenitaloraquired(LAmyxoma,severeannularcalcification)
• 2:1female:male

MitralStenosis• Pathophysiology
– ReductioninvalveareacausesincreasedtransmitralgradientresultinginelevatedLApressure,pulmonaryedema,diminishedcardiacoutput.
– Valveareas>1.5cm2usuallydonotcausesymptoms,butdecreasesindiastolicfillingtimefromtachycardia(infection,Afib,pregnancy,etc.)increasesMVgradientandmayprovokesymptoms.
– Progressive,indolentprocesswithlonglatentperiod(20-40years)• Diagnosis
– Maypresentwithnosymptoms,fatigue,ordyspnea/pulmonaryedema.– AccentuatedS1,openingsnap,diastolicrumble– EchocardiographyshouldbeperformedtodeterminethediagnosisofMS,
assesshemodynamicseverity(meangradient,MVarea,andpulmonaryarterypressure),assessforconcomitantvalvularlesions,andassessvalvemorphology.
MitralStenosis-NaturalHistory
• Annuallossofvalvearea0.1-0.3cm2peryear• Overall10-yearsurvivalofpatientswithMSis50-60%dependinguponsymptomsatpresentation.– Asymptomatic:80%– Significant,limitingsymptoms:0-15%
• Mortalityduetoprogressivesystemiccongestion,systemicembolization,infection

MitralStenosis-MedicalTherapy
• Nomedicaltherapywillspecificallyrelieveobstructiontoinflowatthemitralvalve.
• Avoidanceofunusualphysicalstressandtachycardia.Negativechronotropicdrugs(BBlockers,Ca-Channelblockers)maybebeneficialinpatientswithexertionalsymptoms.
• Saltrestriction,diureticsinpatientswithcongestivesymptoms
• Treatmentofatrialfibrillation(occursin30-40%ofsymptomaticMSpatients)

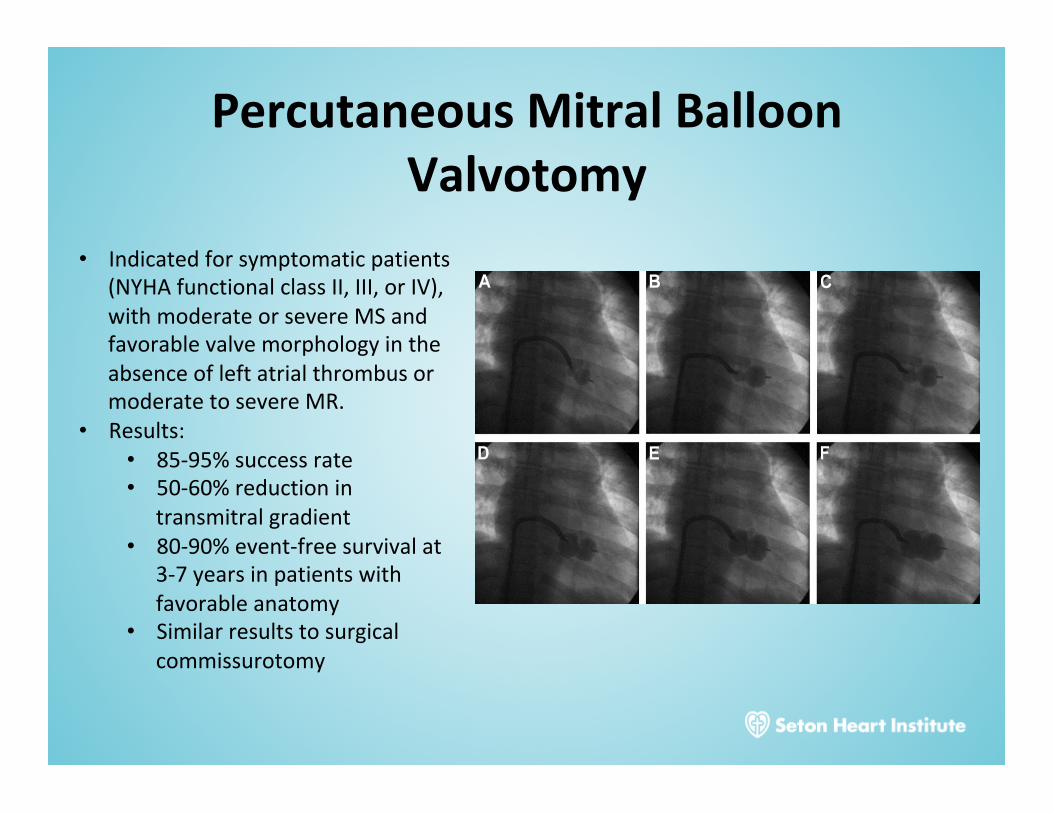
PercutaneousMitralBalloonValvotomy
• Indicatedforsymptomaticpatients(NYHAfunctionalclassII,III,orIV),withmoderateorsevereMSandfavorablevalvemorphologyintheabsenceofleftatrialthrombusormoderatetosevereMR.
• Results:• 85-95%successrate• 50-60%reductionin
transmitralgradient• 80-90%event-freesurvivalat
3-7yearsinpatientswithfavorableanatomy
• Similarresultstosurgicalcommissurotomy

MitralRegurgitation
• Morethan2millionpersonsintheU.S.havemoderateorsevereMR
• Etiologies:degenerative(mitralvalveprolapse),rheumaticheartdisease,CAD,endocarditis,collagenvasculardisease,annulardilatation

DegenerativevsFunctionalMitralRegurgitation
NormalDegenerative:ProlapseDegenerative:FlailFunctional
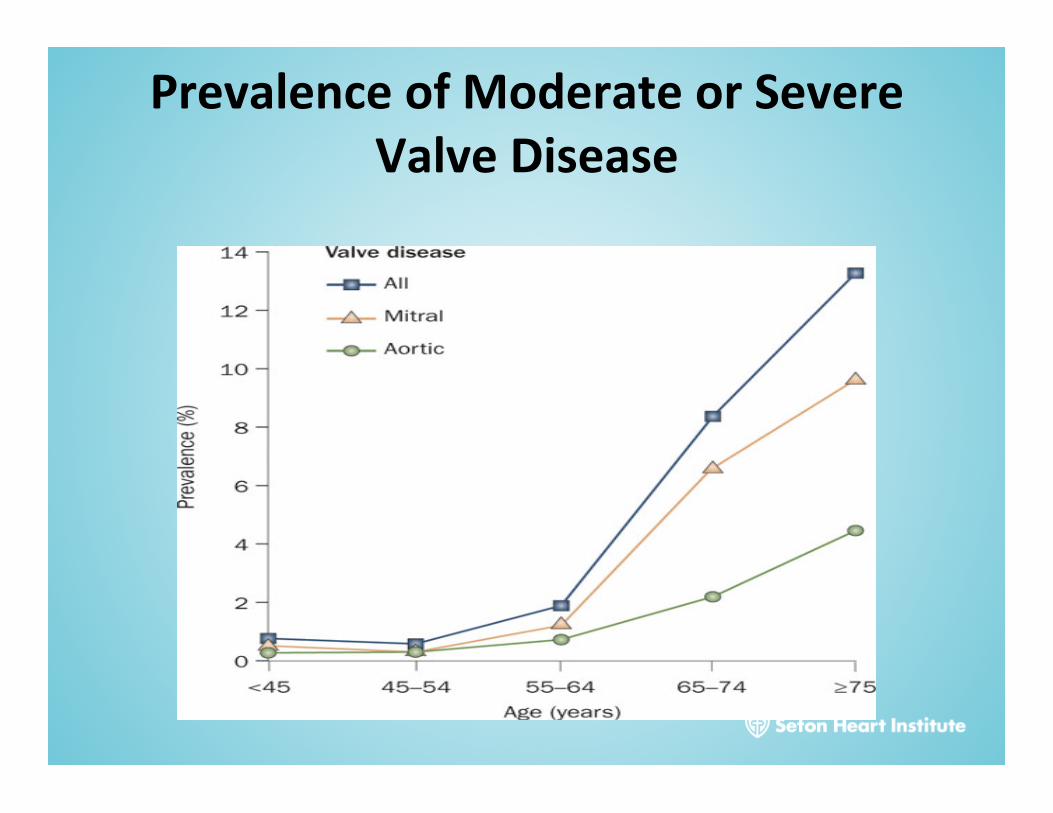
PrevalenceofModerateorSevereValveDisease

MitralRegurgitation-Acute
• Presentation– RapidLA,LVvolumeoverloadresultinginpulmonarycongestionand
decreasedstrokevolume/forwardcardiacoutput– Almostalwaysseverelysymptomatic– Rales,S3,normalheartsize,early/holosystolicmurmur– Confirmedbyechocardiography
• Treatment– Afterloadreduction(nitroprusside)toreduceafterloadandimproveforward
cardiacoutput– Diureticstorelievecongestionanddecreasepreload– Inotopes(dobutamine)– IABP– Surgicalintervention

MitralRegurgitation-Chronic
• PatientswithmildtomoderateMRmayremainasymptomaticwithlittleornohemodynamiccompromiseformanyyears
• NaturalhistoryofsevereMR– 6-7%mortality/year– 90%ofpatientsaredeadorhaveMVsurgeryby10years
• Follow-upofAsymptomaticMR– Mild:Annualfollow-up.Yearlyechonotindicatedunlesschangeinsymptoms– Moderate:Annualclinicalfollow-upwithechocardiography– Severe:Clinicalfollow-upwithechoevery6-12monthstoassessforsymptomsor
asymptomaticLVdysfunction
ChronicLA,LVVolumeOverload
LVDysfunction,ElevatedFilling
Pressures,Congestion,DiminishedOutput
LA,LVDilatationMaintainingForwardOutputatLowerFillingPressures
CompensatoryPhase Decompensation

ChronicMitralRegurgitation-MedicalTherapy
• IntheasymptomaticpatientwithchronicMR,thereisnogenerallyacceptedmedicaltherapy
• Nolarge,long-termstudiestoindicatethatACE/ARBarebeneficialinimprovingmortalityordelayingsurgicalintervention.
• Intheabsenceofsystemichypertension,thereisnoknownindicationfortheuseofvasodilatingdrugsorACEinhibitorsinasymptomaticpatientswithMRandpreservedLVfunction.
• ACE/ARB,B-BlockersshouldbeusedinsettingofLVdysfunctionorsymptomaticCHF

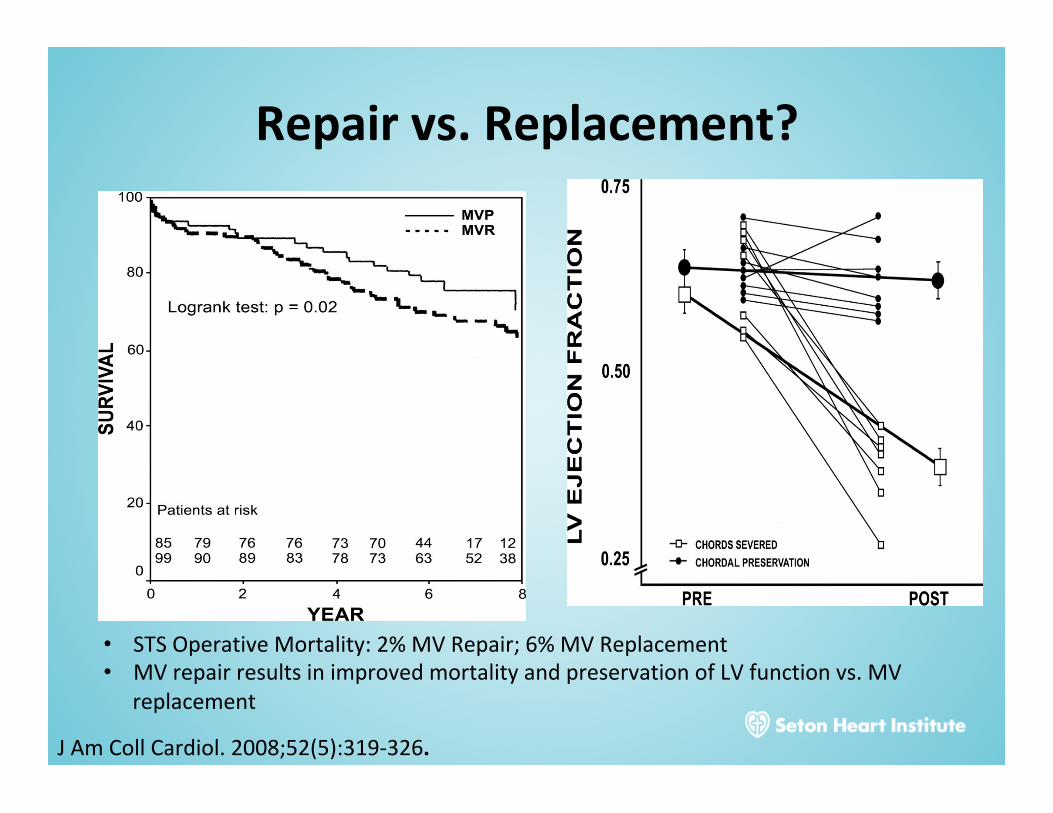
Repairvs.Replacement?
• STSOperativeMortality:2%MVRepair;6%MVReplacement• MVrepairresultsinimprovedmortalityandpreservationofLVfunctionvs.MV
replacement
JAmCollCardiol.2008;52(5):319-326.

PercutaneousMitralValveRepair:MitraClip
• Byapproximatingtheanteriorandposteriormitralleafletsandformingadouble-orificevalve,theMitraClipdevicereducesMR
• Currentlyapprovedforuseinpatientswithdegenerativemitralregurgitationwhoarehighriskforconventionalmitralvalvesurgery
0
20
40
60
80
100
Perc
ent o
f Pat
ients
(%)
Baseline(N = 124)
01+2+3+4+
Discharge(N = 123)
1 Year(N = 84)
2 Years(N = 40)
MITRAL REGURGITATION GRADE
0
20
40
60
80
100
Perc
ent o
f Pat
ients
(%)
Baseline(N = 127)
30 Days(n = 113)
lllllllV
1 Year(n =84)
NYHA FUNCTIONAL CLASS
82%MR≤ 2+
9.7%MR ≤ 2+
83%MR≤ 2+
87%Class
l/ll
82%Class
l/ll
82.5%MR≤ 2+
13.4%Class I/II
0
20
40
60
80
100
Perc
ent o
f Pat
ients
(%)
Baseline(N = 124)
01+2+3+4+
Discharge(N = 123)
1 Year(N = 84)
2 Years(N = 40)
MITRAL REGURGITATION GRADE
0
20
40
60
80
100
Perc
ent o
f Pat
ients
(%)
Baseline(N = 127)
30 Days(n = 113)
lllllllV
1 Year(n =84)
NYHA FUNCTIONAL CLASS
82%MR≤ 2+
9.7%MR ≤ 2+
83%MR≤ 2+
87%Class
l/ll
82%Class
l/ll
82.5%MR≤ 2+
13.4%Class I/II
Reduction in MR Severity Improvement in Heart Failure Symptoms
30-day MR severity was used if discharge MR was unavailable.
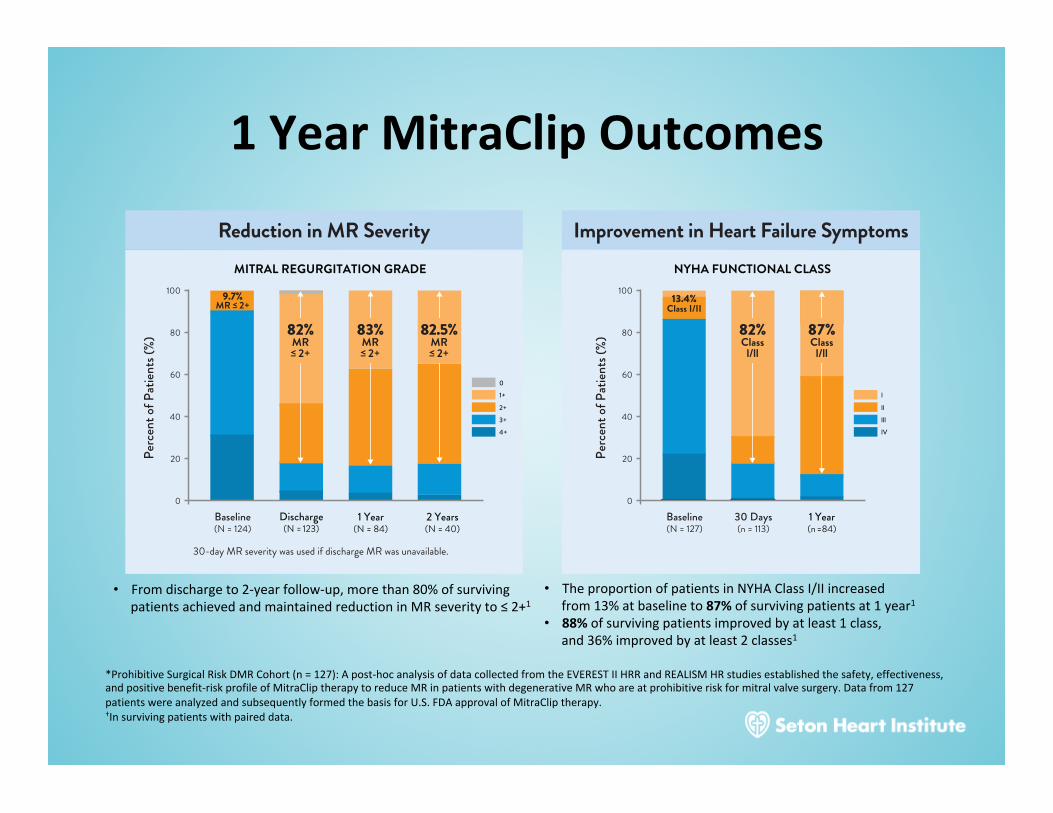
1YearMitraClipOutcomes
*ProhibitiveSurgicalRiskDMRCohort(n=127):Apost-hocanalysisofdatacollectedfromtheEVERESTIIHRRandREALISMHRstudiesestablishedthesafety,effectiveness,andpositivebenefit-riskprofileofMitraCliptherapytoreduceMRinpatientswithdegenerativeMRwhoareatprohibitiveriskformitralvalvesurgery.Datafrom127patientswereanalyzedandsubsequentlyformedthebasisforU.S.FDAapprovalofMitraCliptherapy.†Insurvivingpatientswithpaireddata.
• Fromdischargeto2-yearfollow-up,morethan80%ofsurvivingpatientsachievedandmaintainedreductioninMRseverityto≤2+1
• TheproportionofpatientsinNYHAClassI/IIincreasedfrom13%atbaselineto87%ofsurvivingpatientsat1year1
• 88%ofsurvivingpatientsimprovedbyatleast1class,and36%improvedbyatleast2classes1
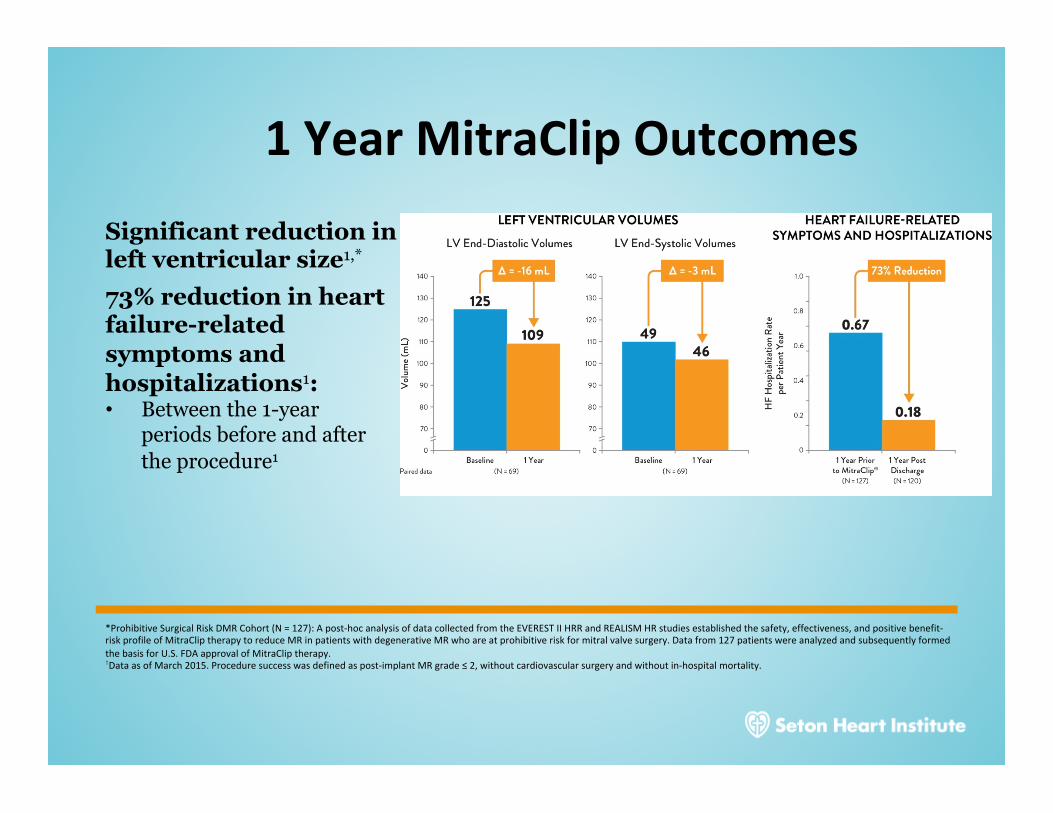
1YearMitraClipOutcomes
Significant reduction in left ventricular size1,* 73% reduction in heart failure-related symptoms and hospitalizations1: • Between the 1-year
periods before and after the procedure1
*ProhibitiveSurgicalRiskDMRCohort(N=127):Apost-hocanalysisofdatacollectedfromtheEVERESTIIHRRandREALISMHRstudiesestablishedthesafety,effectiveness,andpositivebenefit-riskprofileofMitraCliptherapytoreduceMRinpatientswithdegenerativeMRwhoareatprohibitiveriskformitralvalvesurgery.Datafrom127patientswereanalyzedandsubsequentlyformedthebasisforU.S.FDAapprovalofMitraCliptherapy. †DataasofMarch2015.Proceduresuccesswasdefinedaspost-implantMRgrade≤2,withoutcardiovascularsurgeryandwithoutin-hospitalmortality.

ImpactofMRonSurvivalinPatientswithCHF
JAmCollCardiol.2008;52(5):319-326.
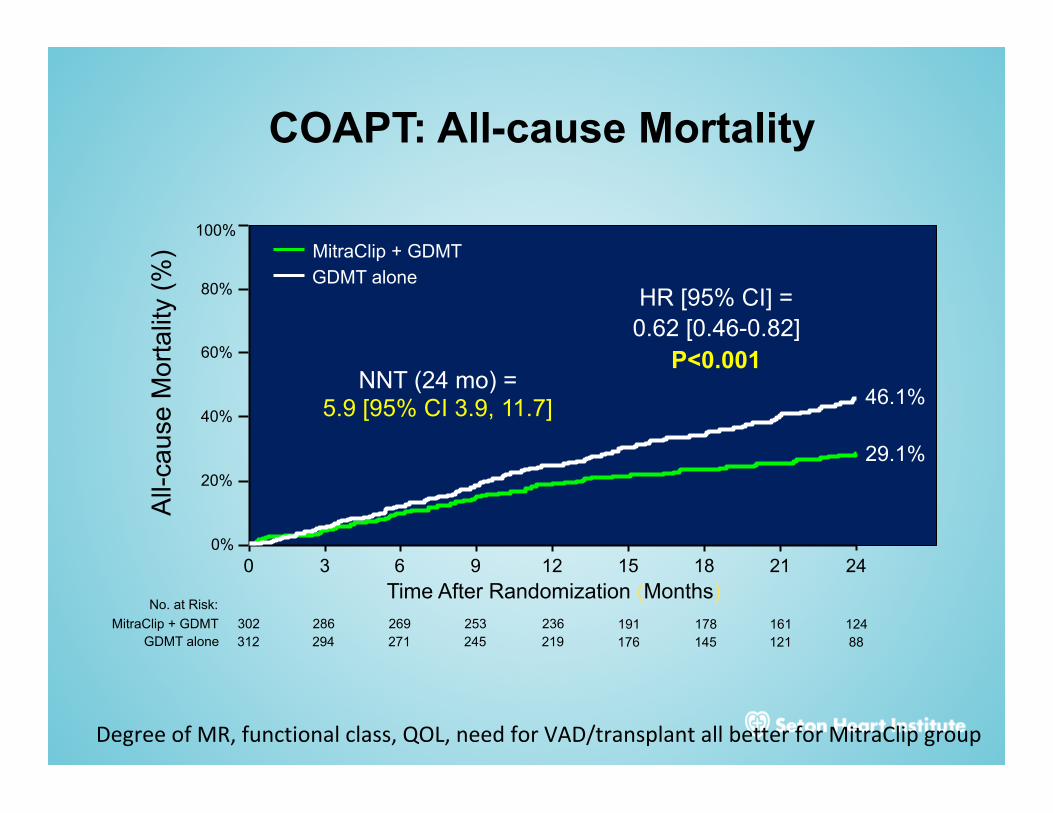
COAPT: All-cause Mortality A
ll-ca
use
Mor
talit
y (%
)
0%
20%
40%
60%
80%
100%
Time After Randomization (Months) 0 3 6 9 12 15 18 21 24
46.1%
29.1%
HR [95% CI] = 0.62 [0.46-0.82]
P<0.001
MitraClip + GDMT GDMT alone
302 286 269 253 236 191 178 161 124 312 294 271 245 219 176 145 121 88
No. at Risk:
MitraClip + GDMT GDMT alone
NNT (24 mo) = 5.9 [95% CI 3.9, 11.7]
DegreeofMR,functionalclass,QOL,needforVAD/transplantallbetterforMitraClipgroup
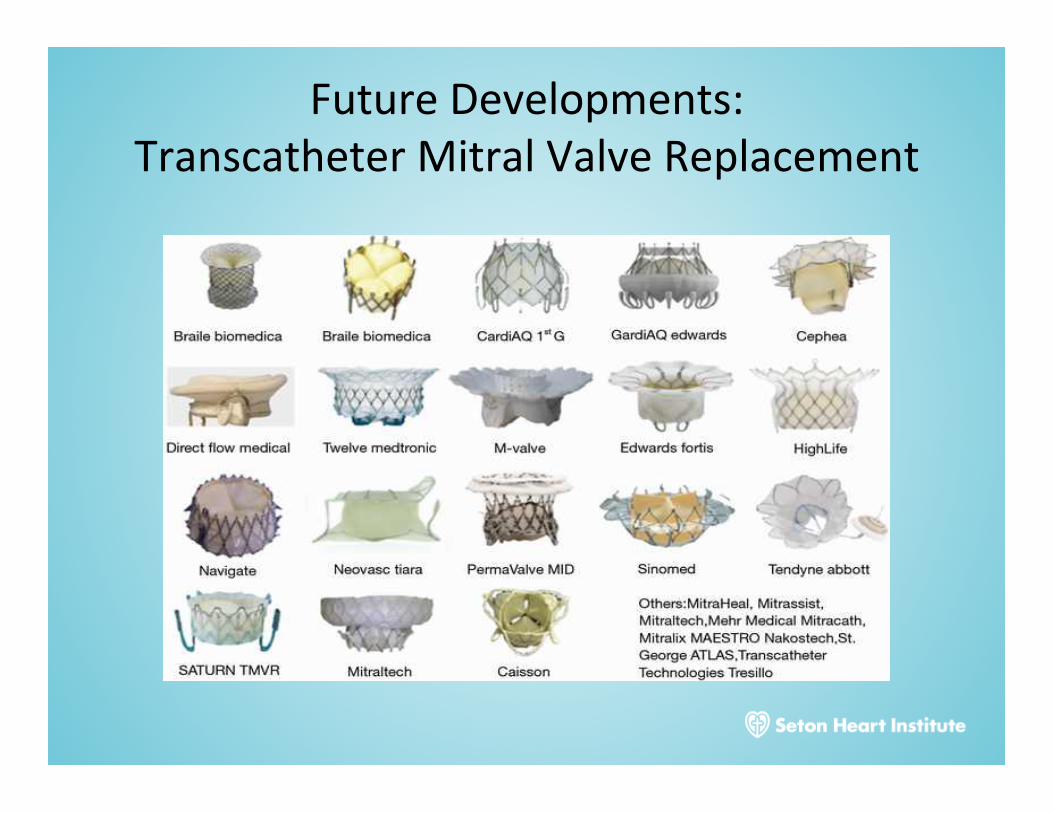
FutureDevelopments:TranscatheterMitralValveReplacement

Conclusions• Valvularheartdiseaseisveryprevalentintheprimarycaresetting,particularlyintheagingpopulation(13.3%overage75)
• Opensurgicalvalvularrepair/replacementhaspreviouslybeentheprimarytherapyforsymptomaticdisease.
• Medicaltherapyisprimarilyusedforstabilizationforacutevalvedysfunction.
• Newer,lessinvasivepercutaneoustechniquesmayallowtreatmentofpatientspreviouslydeemedaspoorsurgicalcandidateswithlessmorbidity