value judgment in the oregon medicaid experiment -...
TRANSCRIPT
MEDICAL C,¢REVolume 32- Number 10, pp 975-988(_1994. J.B. L_ppmcott Company
Value Judgment in the Oregon Medicaid Experiment
ROBERTM. KAPLAN,PHD
Oregon proposed a unique social experiment in which combinations ofmedical conditions and treatments were prioritized. Under the proposed pro-gram, providers would not be reimbursed for services relevant to 17% of thecondition-treatment pairs. The program was designed to expand access andallow significantly more residents to qualify for Medicaid. The ori_nal Ore-gon proposal used four levels of human judgmen_ community values as-sessed in town meetings; ratings of the desirability of health states; medicaljudgment of treatment efficacy; and subjective reordering of the list by Ore-gon Health Services Commissioners. In August 1992, the Department ofHealth and Human Services rejected Oregon's application to proceed withthe experiment, objecting to the use of one of the four types of subjectivedata: ratings of the desirability of health states. A revised applicalion thateliminated this one subjective component was approved in March 1993. Thispaper demonstrates that among the four levels of judgment, the ratings ofhealth states were SUl_orted by the most evidence of reliability and validity.Implications for future prioritization experiments are discussed. Key words:Oregon Medicaid Experiment; prioritization; cost-effectiveness; QALY;Medicaid. (Med Care 1994",32:975-988)
The American Health Care system is in a Affordability, Access, and Accountability.serious crisis. Estimated 1994 health care Beyond the problems of excessive expensecosts exceeded $900 billion, whereas access (affordabflity) and limited access, there is anto the system is severely restricted for more accountability problem because the systemthat 37 million uninsured Americans. Medi- is poorly equipped to document what it pro-
c.aid programs in nearly all states are failing duces. In other words, we have no evidencebecause of increasing costs and little poten- that greater expenditures on health caretial to keep up with growing demand. The translate into better health for Americanproblems with the health care system are citizens.threefold and might be described by the 3 A's: In response to these problems, the State
of Oregon proposed an innovative experi-ment that has been the subject of consider-able commentary. 1-7 The Oregon proposal
From the Division of Health Care Sciences, Depart- attempted to address all three issuessimul-ment of Family and Preventive Medi_ne, University ofCa_rni_ SanDiego,LaJolLa.Ca_n_ taneously. The strategy was to rank all medi-
Supportedbya grantfromthe CaliforniaPolicySemi- cal services (excluding long-term care, men-nat andby _ Gram1P60AR40770(M_l.-purlx_ At- tal health, and services for the disabled) bytl'uitis and Musculoskeletoi Disease Center) from theNationa] Instit_t _,_of Health- cost-effectiveness. A substantial proportion
Addresscor_-_nden_ m: RobertM-Kaplan,P.D, of medical procedures have little or no effectProfessorandChief, Divisionof HealthCareScience, on patient outcomes, s Nevertheless, physi-Departmentof FamilyandPreventive_, Un/v_- clans and hospitals are reimbursed for offer-si_yofCa/ifom_ SanDie_, 9500GRmanDrive,LaJona,CA92093-O622. ing these services to Medicaid recipients. At
975

KA]_LAN MEDICAL CARE
the same time, more citizens are uninsured unpublished discussion paper by Davidor significantly underinsu_ed than are coy- Hadom and an analysis by the US Congressered by the Medicaid programs. Because of Office ofTechnologyAssessment OTA _werethe continuing financial difficulties, Medi- Cited to support this statement. A revisedcaid budgets have been unable to keep pace application that eliminated this quality ofwith the rising costs of health care. As a re- life component was approved by the DI-tHSstilt, most Medicaid programs have confinu- in March 1993.ally readjusted eligibility thresholds down- The DHHS decision to exclude quality ofward. Clearly, this has resulted in the life data fails to acknowledge that resourcerationing of health care. Rationing occurs by allocation decisions necessarily require hu-allowing some individuals into Medicaid man judgment. Ultimately, decisions arewhile excluding others who are equally in made by patients, physicians, administra-need. The peculiarities OfMedicaid eligibil- tots, or their surrogates. Oregon clearly rec-it}, force the system to ration by default. 9 ognized this and attempted to separate as-
Oregon's plan used principles of cost-ef- Pects of human judgment. For example,fectiveness that have been endorsed in the when decisions required medical knowl-literature of various academic fields. _=s.l°-n edge, they depended on clinicians. WhenHowever, the proposal to actually use these the decisions required in-depth under-methods for resource allocation was bold and standing of human values, they used disc-us-different, and it generated considerable con- sions held in open forums in Oregon towns.troversyY -13 After detailed study by several When the judgments involved an assess-groups, the plan wasregarded as a reason- ment of quality of life for those with eitherable candidate for social experimentation- 6 symptoms or disabilities, they depended on
the ratings by Oregonians. This exercise wasDepartment of Health and Human unusual because all of these judgments were
Services Rejection of Oregon made publicly using methods that could beApplication replicated by others.
The focus of the DHHS review of the Ore-
Because Oregon intended to revise tracti- gon Experiment was on the use of subjectivetional Medicaid policies, they needed a judgments about quality of life. However,waiver to perform their demonstration ex- there were four types of subjective data inperiment. Such experimentation had been the proposal, not just one. Ultimately, it willwidely promoted by the Bush administra- be argued here, the approved plan is moretion. However, in August 1992, the Depart- subjective than the one rejected. The plandl .
ment of Health and Human Sermces re, that was accepted may have more potentialjected Oregon's application for a waiver that for allocation errors and discriminationwould have allowed them to proceed with against persons with disabilities.the demonstration. The rationale for this re-
jection was that the Oregon proposal rio- Four Subjective Judgmentslated the Americans with DisabilityAct " .-
which became law inJuly1992.Specifically, Four differenttypesof subjectivejudg-thedepartmentstatedthattheOregon pref- ment were usedtocreatethe originalOre-
erencesurveyon qualityoflife"quantified gun MedicaidlistThese were:I)valuesas-
stereotypicassumptionsaboutpersonswith sessed in town meetings;2) ratingsfor
disability,"According to the statement, healthstates;3)subjectivejudgments aboutscholarshave found thatpeople without treatmenteffectiveness;and 4)reprioritiza-
disabilitiessystematicallyundervaluethe tionbased on commissionerjudgment.Thequalityoflifeof thosewith disabilities.An followingsectionsreview each of these
976

Voi. 32. No. 10 VALUE JUDGMENT IN OREGON MEDICAID
types of judgments. In the denial of the Ore- gonians, and health care providers. A varietygon Medicaid application in August 1992, of grass roots organizations participated,only preference weights for health states providing publicity for the meeting andwere specifically cited.Amongthe four types door-to-door shuttle service for those whoof judgments, it could be argued that these had disabilities. On the basis of the test-i-were the most scientifically justifiabIe, mony, the commissioners concluded that
the general public wanted coverage for serv-Oregon Town Meetln_ ices that may not be part of standard basic
benefit packages. These services IncludedAs part of the process the commission dental care, prevention, mental health care,
hired a grass roots citizens group that con- and chemical dependency services.ducted 47 community meetings to deter- Critics were quick to point out that thosemine which values were commonly held by who attended the community meetings
I'
members of the Oregon population. The were not representative of all Oregon citi-participants completed a questionnaire con- zens. 12For example, the experiment was de-cerning eight theoretical health situations, signed to impact on those with no medicalThe participants were asked to place _nine insurance and 91% of those who attendedtypes of care into three categories: essential, the meetings were, themselves insured.very important, and important. The nine More than one-third of those who partici-categories ranged from treatment of condi- pated in the meetings had annual incomestions where the health care is likely to ex- in excess of $50,000 and two-thirds hadtend lffe by more than 2 years or to improve graduated from college. Only 1% of thequality of life, and "treatment not likely to meeting participants were black. As a resultextend life or make any big improvement in of this imbalance, there was concern that thequality of life." The partidpants then took process was biased in favor of procedurespart in small group decisions that focused that would benefit the white, educated, andon these issues. On the basis of these dis- wealthy subpopulations of the society.
cussions group, consensus was estimated In response to these concerns, the Healthand results were recorded. 7 Services Commission pointed out that they
The community meetings were well at- made extensive efforts to recruit all mere-tended. Groups ranged in size from small (7 bets of society and engaged in special out-participants) to fairly large (132 participants) reach efforts for the poor. Clearly, the proc-with an average of about 20 participants, ess would have been better if the townOverall, the 47 meetings were attended by meeting participants were more represen-more than 1,000 people. Nearly 64% Of the tative of the general population. However,participants were women and two-thirds public hearings are common components of
were health care workers. On the basis of public policy making. In this respect thethe 47 town meetings, 13 community values meetings in Oregon were not different thanemerged. These 13 values were grouped by " the policy forums in nearly all levels of gov-the commission into three attributes: value ernment. The fact that those who testify at
to society; value to an individual at risk of public hearings are not representative of theneeding service; and essential to basic general population has not stopped local,health care. state, or federal governments from enacting
The commission also held a series of 12 legislation that they perceive to be the willpublic hearings in various parts of the state, of the people. If those participating in theDuring these meetings, testimony was solic- town meetings were reckless in advocatingited from seniors, handicapped persons, policies to support their own self-interest,mental health consumers, low income Ore- we would expect their opinions to be dis-
977
KAPLAN MEDICALCARE
crepant from those of the general public. The the same score to all those alive.Thus, a per-results of the town meetings indicated that son in a coma is scored as alive (1.0) as is athe public wanted programs that benefit person who is completely functional with nomany, those that emphasize prevention, and symptoms. The Oregon approach assignedthose that improve quality of life. Is the sug- value to these states in recognition that neargestion that poor people are opposed to pre- death and wellness cannot be consideredvention and to equity in health care? Public equivalent. This is accomplished by obtain-opinion polls that include random samples ing descriptions of health states and ratingfrom the general population show that the the desirability for each. In Oregon thesevalues expressed in the town meetings axe ratings were obtained form random samplesconsistent with those of the general popula- of Oregon citizens. These ratings representtion. TM utilities for health states and are described
Perhaps the strongest rebuttal is that as utility weights, preferences, or ratings. Wenearly all states are currently rationing use these terms interchangeably. Once rat-health care by changing the Medicaid eligi- ings are obtained, they can be used tobility criteria and excluding categories of weight or "quality adjust" years of life. Twopeople. These rationing decisions are made years in a state rated as 0.5 (mid way be-with little or no public input. The attempt in tween optimum health and death) areOregon to gain public input represents a equivalent to 1 year of wellness. Theoreti-significant, although imperfect improve- call),,treatments that improve quality of lifemerit over the current system, is by 10%, (for example from 0.5 to 0.6) pro-
duce the equivalent of 1 year of life for eachWeiohts for I-W_ltl'lb-'lnt_ 10 people they affect over the course of 2
year (10 people x 0.1 x 1.0 year = 1.0 QALY).The Oregon experiment used a model for The Oregon commission did not calculate
valuing health states developed at the Uni-- QALYs because it did not consider howversity of California, San Diego .a°'a6"2°This many people would be affected.general health policy model estimates the Criticisms on the use of de_-ability rat-impact of any illness or medical treatment in ings abound. The most common criticisma unit that is equivalent to a year of life. stems from the assumption that mean rat-These units are necessary to make direct ings vary across patient or demographiccomparisons between medical interventions groups. For example, in most areas of pref-that have different specific objectives. Tradi- erence assessment, it is easy to identify dif-tional outcome measures that tare disease ferences between different groups of differ-specific cannot be used for these compari- ent individuals. Judgments about net healthsons. For example, a treatment for diabetes benefits for white Anglo-Saxon men po_-mellitus might be evaluated in terms of bly should not be applied to Hispanic menblood glucose while a treatment for hyper- who may give different weight to sometension might be evaluated in terms of symptoms. Soeial groulrsmay have differentblood pressure. Blood sugar and blood pres- utilities formovies, dothin& or political can-sure outcomes cannot be compared directly didates, and these same differences are as-to one another, roamed to extend to health states. Thus, the
The common denominator for many ill- entire analysis may be highly dependent onnesses has been life expectancy which is the particular group that provided the ratingtypically analyzed through survival analysis, data. In Oregon, for example, critics declaredIn survival analysis those that are alive are the whole process meaningless because thecoded as 1.0, and those who are dead program was aimed at Medicaid recipientsare coded as 0.0. This coding scheme assigns when the ratings came form both Medicaid
978
Vol. 32. No. 10 VALUEJUDGMENTIN OREGONMEDICAID
recipients and nonrecipients. 12 Other ana- the evidence. A study of California prefer-lysts have suggested that ratings from the ence weights demonstrated some signifi-_neral population cannot be applied to any cant, but very small differences, betweenparticular patient group. Rather, patient utili- social and ethnic groups on preferences. TM
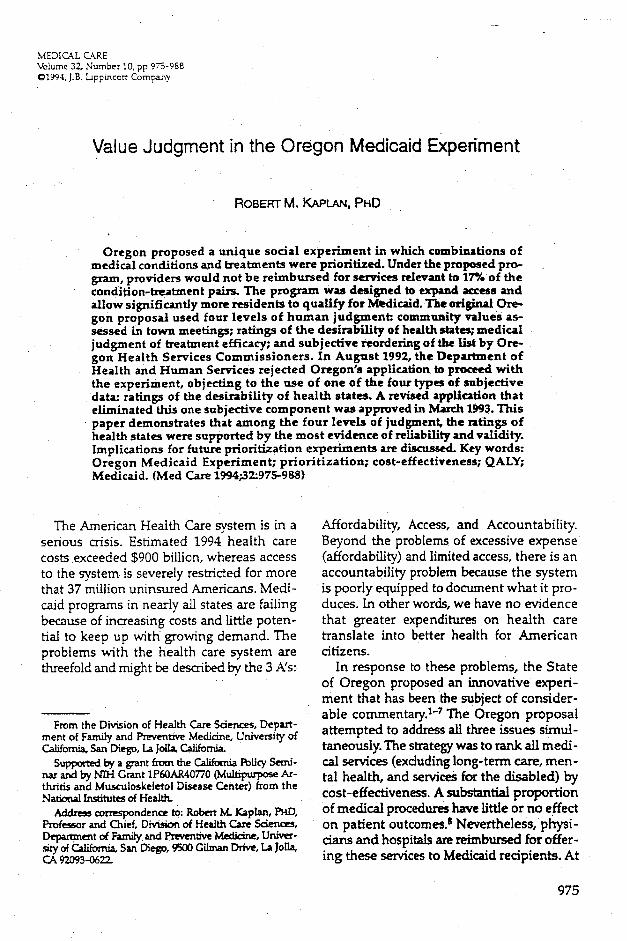
ties from every individual group must be ob- Studies have found little evidence for prefer-rained. The August 1992 rejection of the ence difference between patients andwaiver application was based on the assump- the general population. For example, Bala-tion that people with disabilities have differ- ban and colleagues compared preferenceent utilities than those without disabilities, weights obtained from arthritis patients
The difference between instrumental and with those obtained from the general popu-terminal preferences is important to under- lation in San Diego. z2They found remark-standing this debate. 21The difference between able correspondence for ratings of cases in-instrumental and terminal preference is volving a_,'daritispatients (Figure 1). Nerenzanalogous to the difference between a and colleagues performed a similar studymeans and an ends. Instrumental prefer- with cancer patients. Again; they found thatences describe the means by which various preference weights for these patients andassets are attained. For instance, socialists the cognitive strategies used to evaluateand capitalists hold different instrumental these descriptions were remarkably similarvalues with regard to the methods for to those from the general population, z3achieving a fully functioning society. Differ- There are few differences by location. Pat-ent individuals may have different prefer- rick and his colleagues found essentially noences for how they would like to achieve differences between utilities for anotherhappiness and evidence suggests that sodal health status measure among those who liveand demographic groups vary considerably in the UK and those who live in Seattle. 24on instrumental values. We have compared residents of the Navaho
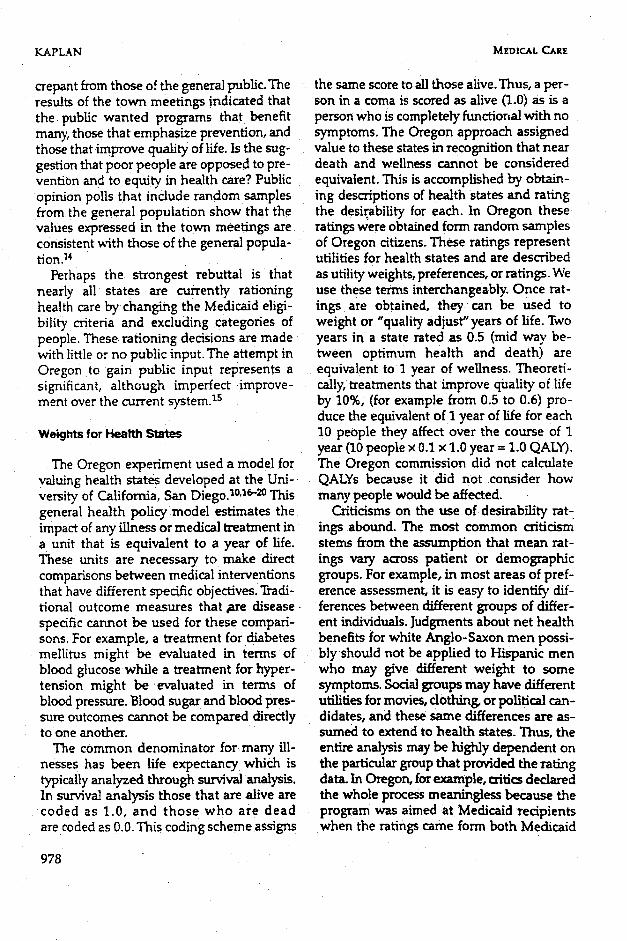
Terminal values are the ends, or general nation living in rural Arizona with the gen-states of being that individuals seek to eral population in San Diego and found fewachieve. The classic Rokeach study of val- differences. One of the crucial comparisonsues demonstrated that there is very little was between Oregon citizens with disabili-variability among social groups for termi- ties and those without these problems.nal preferences. Within health states, there Among respondents to the Oregon survey,is less reason to believe that different so- 76 had used a wheelchair or walker at some
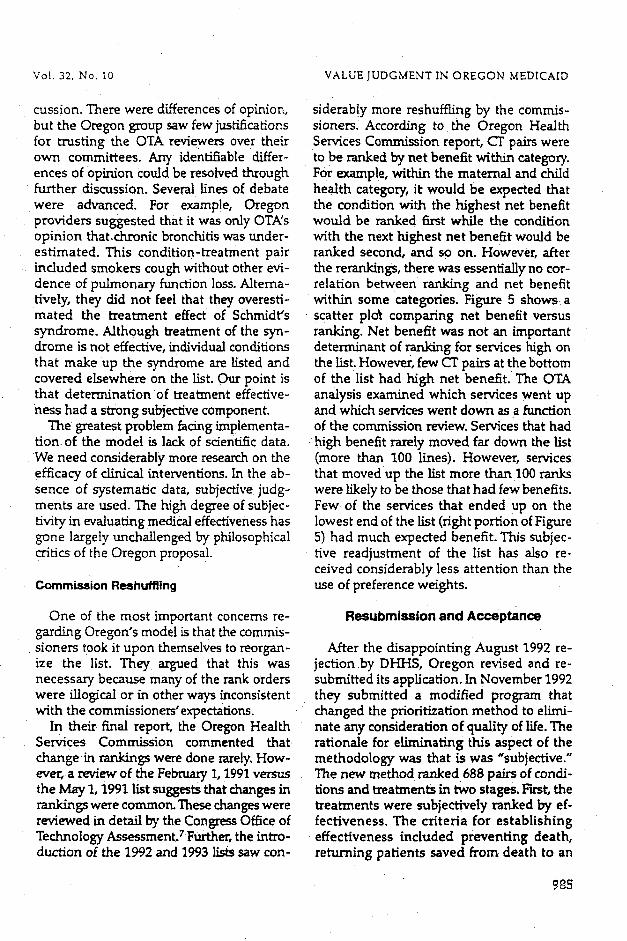
cial or ethnic groups will have different point in their life. In comparison to peopleutilities for health outcomes. All groups who had not experienced these conditions,agree that it is better to live free of pain those who had used a wheelchair or walkerthan to experience pain. Freedom from rated 7 of 31 cases significantly higher. Dif-disability is universally preferred over dis- ferences for the other 24 cases were not sig-ability states. Although it often is sug- nificant. However, the seven statisticallygested that individuals adapt to disabili- significant differences were typically smallties, studies have consistently shown that (less than 0.05 on a scale from 0.0 to 1.0) andthose with disabilities rate being disabled rarely were the rank orders different. Figureas less desirable than being disability 2 shows that the ratings from those with andfreefla If disability states were preferred to without the experience of these problemsnondisability states there would be no mo- were strongly linear and highly correlated.tivation to develop interventions to help The utility judgments obtained by thethose with problems causing the disabilities. Oregon Health Services Commission used a
The common assumption that utilities different scaling methodology and differentvary across social groups is challenged by wording in the case descriptions than in
979
KAPLAN MEDICAL CARE
O 1
_Dm
e"
CD
_" 0.60
n 0.4 ,.0n
•- 0.2G)r-.
0.00.0 0.2 0.4 0.6 0.8 1.0 1.2
Rheumatoid Arthritis PatientsFro, 1. Comparison of rheumatoid arthritis patients v_m,_ general pop-I* 'tlon (aft_ _ _ _ 19_).
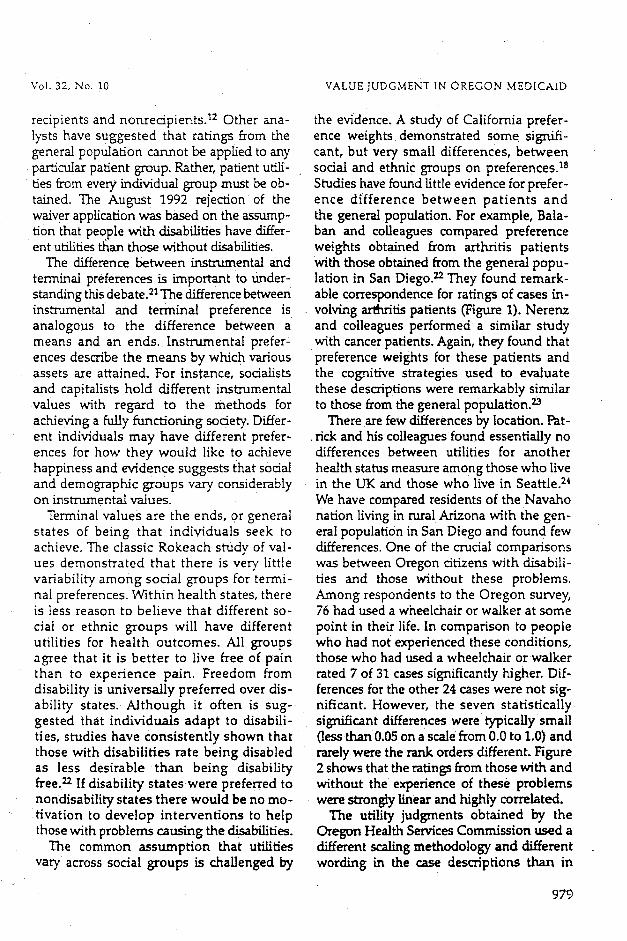
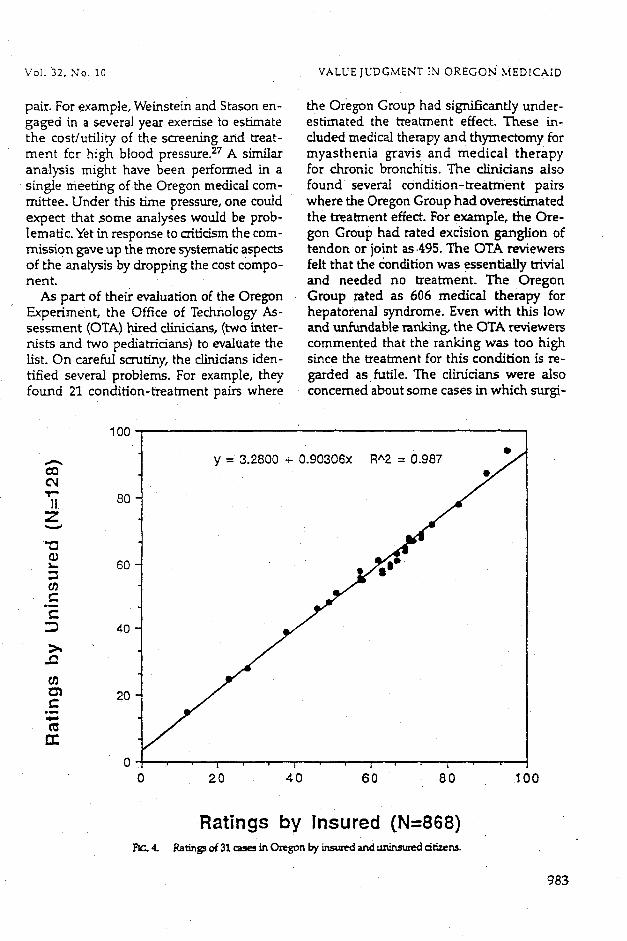
other studies. Nevertheless, differences be- small and typically not significant, z4 Wetween San Diego citizens evaluated in the have used EuroQol scenarios and estimatedmid 1970s and Oregon citizens evaluated in approximate San Diego preferences forthe 1990s were small 19With _e exception these cases. The results suggest that prefer-of three outliers, the relationship was linear ences are similar.We do recognize that thereand strong (r = 0.92). Figure 3 compares is considerable variability in estimating pref-Oregon women and Oregon men, whereas erences for a particular case. z5 However, av-Figure 4 compares Oregon citizens with eraged across individuals, the mean prefer-health _ce with those without insur- ence for different_mses in different groups isance. Neither gender nor insurance status remarkably similar.has substantial impact. A similar scaling We should not leave the impression thatmethodology was used by the EuroQol there are never any mean differences inGroup in a series of European communities, preference. For example, our original studyThe data from those studies suggest that dif- identified some significant differences be-ferences in preference among citizens in the tween social groups, is Further, the Oregonthree different European communities are Health Services Commission identified
980

Vol. 32, No. 10 VALUE JUDGMENT IN OREGON MEDICAID
small, but significant, preference differences judgment. For each pair of medical condi-among those who had previously expert- tionand treatment (referred to as condition-enced a condition and those who had not. treatment or CT pair), clinicians estimatedHowever, these differences were typically the Quality of Well-Being (QWB) change forsmall and it is unlikely that these smatl dif- the average patient. A clinician panel placedferences could affect which services would patients into defined categories of mobility,be funded under the program. Although the physical activity,and social activity. In addi-OTA analysis showed that it was hypotheti- l-ion,clinicians were asked to identify whichcally possible for condition-treatment pairs of 23 symptoms or problems would be mostto move from the fundable to the unfund- likely at the beginning of treatment. Then,able range on the list, such shifts were very the clinicianswere asked to repeat the exer-improbable and could only happen for serv- cise with _eir expectations for their averageices that already had marginal placements, patient following treatment. The time frame
for these judgments was 5 years.PhysicianJudgmentof Effectiveness The initial task for providers was enor-
mous. In their first attempt at prioritizadonThe health outcomes for people in differ- the group examined more than 1,600 condi-
ent treatments was estimated using clinical tion treatment pairs and several groups of
100
,_ y = 5.0641 + 0.89249x R^2=_
80L0
co 60 •
__,0 • •ID
.,C: 40-
r'-"-- 20
0
Z 0 • i , , ,0 20 40 60 80 O0
Ever in Wheelchair or WalkerFie,. 2. Co_q,,a_._on b_h_,_n ev_ and nev_ in _ or w.alker for 31 item._
D_m fromOregon I-i_d__ _ Oregon State U_ty.
981

KAPLAN MEDZCAL CARE
100
y = 0.49906 + 1.0125×
80
60 m
g 40
I_ 20
0 I ' 1 1 ' ' ' ; ' ' !
0 20 40 60 80 100
Ratings by Men (N=391)FIG.3. Comparisonof_ ratingsby men and women in
providers were needed. Ultimately, 54 pro- replacement of some condition-treatmentvider groups and over 200 individual provid- pairs were, m the opinion of the commis-ers from many specialty groups participated, sioners, counter-intuitive. Almost certainly,The groups included essentially all licensed these peculiar placements were based onpractitioner associations in the state of Ore- faulty analysis. For example, treatment forgon and represented most mediEal subspe- thumb-sucking and acute headaches re-cialties. In addition, the practitioner panels ceived higher rankings than treatment for
included chiropractors, .acupuncturists, and AIDS or cystic fibrosis. The problem was notmassage therapists, the method but rather the way data were
The major difficulty with the initial Ore- generated by the medical committees. We
gon exercise was the attempt to prioritize a should not fault the committees for doing alarge number of services in a relatively short poor •job. Indeed, tremendous personal ef-period of time. The first *trial run_'release of fort went into estimation of treatment effec-the lis t used both cost and effectiveness in- tiveness. The difficulty was that the commit-formation to form a cost-utility ratio for tee attempted to do several decades of workeach of nearly 1,600 condition-treatment within the confinement of a few months.pairs. Although the list was never published, Health policy analystssometimes take 2 to 3it was widely circulated. Early inspection of : years to thoroughly analyze the expectedthe list revealed many inconsistencies. The benefits of a single condition-treatment
982
Vol. 32, N'o. 10 VALUEJUDGMENT IN OREGON MEDICAID
pair. For example, Weinstein and Stason en- the Oregon Group had significantly under-gaged in a several year exercise to estimate estimated the treatment effect. These in-the cosdutility of the screening and treat- cludecl medical therapy and thymectomy forment for high blood pressure. 27 A similar myasthenia gravi s and medical therapyanalysis might have been performed in a for chronic bronchitis. The clinicians alsosingle meeting of the Oregon medical corn- found several condition-treatment pairsmittee. Under this time pressure, one could where the Oregon Group had overestimatedexpect that .some analyses would be prob- the treatment effect. For example, the Ore-lematic. Yet in response to criticism the corn- gon Group had rated excision ganglion ofmission g'ave up the more systematic aspects tendon or joint as .495. The OTA reviewersof the analysis by dropping the cost compo- felt that the conclition was essentially trivialnent. and needed no treatment. The Oregon
As part of their evaluation of the Oregon Group rated as 606 medical therapy forExperiment, the Office of Technology As- hepatorenal syndrome. Even with this lowsessment (OTA) hired clinicians, (two inter- and unfundable ranking, the OTA reviewers
nists and two pediatridans) to evaluate the commented that the ranking was too highList. On careful scrutiny, the clinicians iden- since the treatment for this condition is re-tiffed several problems. For example, they garded as futile. The clinicians were alsofound 21 condition-treatment pairs where concerned about some cases in which surgi-
100
y = 3.2800 + 0.90306x R/'2 = 0.987
"1""
11 80Z
•- 60
o"t
:3 40
20I:
.a,.I,,.Ic_
00 20 40 60 80 100
Ratings by Insured (N=868)FIC.4. Ratingsof31ca..qesinCh'egonI:__ and_ citizen.
983

!_AFLAN MEDICAL CARE
"i°O I I I I I I I I I
I " " eal... a I
[- . ?0.9 • •• • Ill
• _ IRow m m
°" F-- ._ • 1
L'" • .,- 4• e _il • •
O.7 I o" " I." == - l_:'.;.- ._ . . . J
0 • 6 | .=_. "-a • 'I, II,"'". "'..• " "-- I.C: o.s r :_ " "---" "'.-_ ,. ,', - "I| g'm._a sdit m. _ • • /
• • _0.4L ..:' _ _wa _.-_; ." . J
| __I Is • tl • • I = _ • Ms _ • I ,_]I" ",, w= • • -dr q, --,%-,-1, .",w--re /" /
la - _'I_ It" _'' :. ml, u,,_# = I0"2 -- s " "" " .,= • "I " --
'nil • l isis/.. ,, . ...e , • .,_'k,:..- /r, =.'' • - [".= ._" "=_. /
0 3.00 200 300 400 SO0 600 700 800
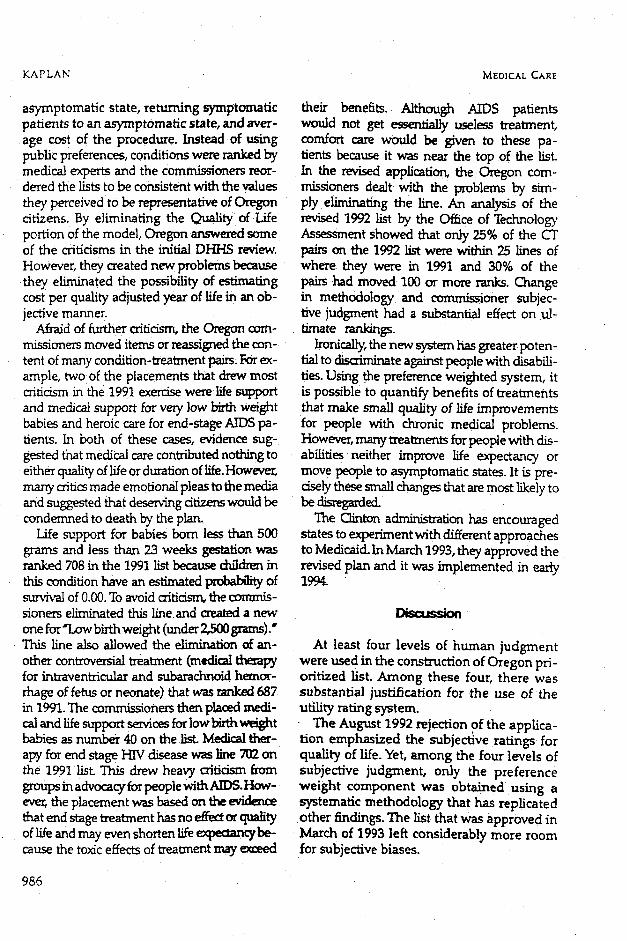
Rank of CT PairF_.5. Net benefits in QWB units versus rank of CT pair.
cal therapy was higher on the list then that go along with it. For example, medicalmedical therapy. The reviewers argued thempy for problems in bloocl clotting is dif-that medical therapy should always be tried ficult tO evaluate because it depends onbefore surgery is employed. Thus, medical whether the problem is caused by a tran-therapy should rank higher than surgery, sient infection or by a serious disease such
One of the most serious concerns raised as cancer. Sometimes, it was difficult for the
by the clinical reviewers was the inexpli- . consultants to evaluate thecondition-treat-cable grouping of some concl/tion-treat- ment pairs since identification of the prob-merit pairs. For example, line 264 was for lem requires treatment. An example in-diseases of white blood ceils. However, eludes surgery forperitoneal adhesions (linethis category groups together some condi- 508). The difficulty is that the diagnosis oftions which are quite trivial with others this problem requires a surgical procedure orthat are life threatening. Line 640 (testicu- laparotomy. In addition to these problems,far hyperfunction) combines a condition the consultants identified several problemswhich may require no treatment, with of apparent miscoding or of mismatches be-Schmidt's syndrome, which is likely to be tween the international classification offatal without treatment, disease (IC'D-9)and the CFT code matches. 7
Another medical concern was the prob- Advocates from Oregonargued that theirlem of comorbidity. It is often difficult to as- medical committeeincluded clinicians withsess the importance of a condition without at least equal experience and that their ownknowing the other •diseases or disabilities judgments arose from detailed group dis-
984
Vol 32, No. 10 VALUEJUDGMENTINOREGONMEDICAID
cussion. There were differences of opinion, siderab!y more reshuffling by the commis-but the Oregon group saw fewjustificaC/ons sioners. According to the Oregon Healthfor trusting the OTA reviewers over their Services Commission report, CT pairs wereown committees. Any identifiable differ- to be ranked by net benefit within category.ences of opinion could be resolved through For example, within the maternal and child
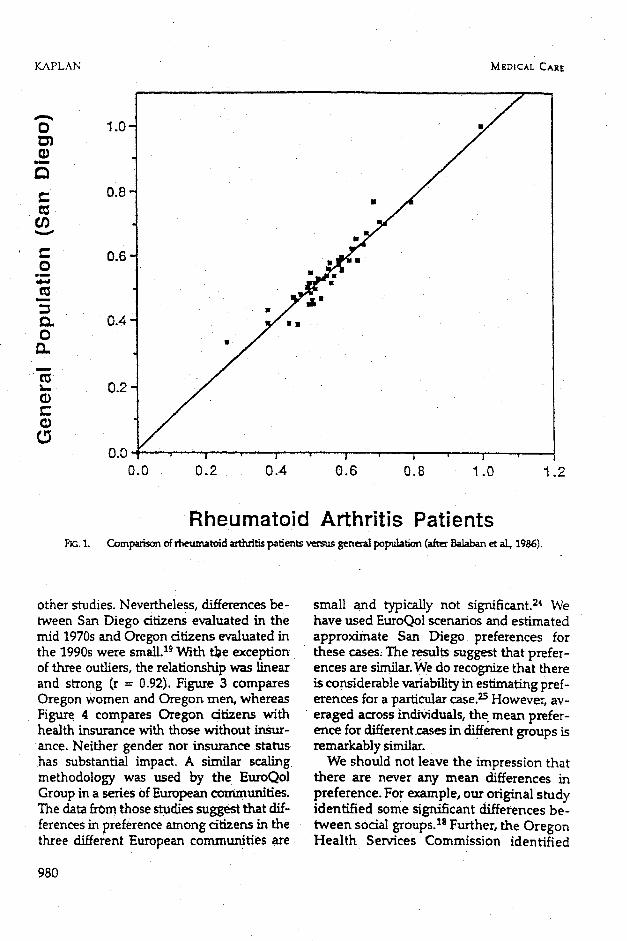
further discussion. Several lines of debate health category, it would be expected thatwere advanced. For example, Oregon the condition with the highest net benefitproviders suggested that it was only OTA's would be ranked fn'st while the conditionopinion that.chronic bronchitis was under- with the next highest net benefit would beestimated. This condition-treatment pair ranked second, and so on. However, afterincluded smokers cough without other evi- the rerankings, there was essentially no cor-dence of pulmonary function loss. Klterna- relation between ranking and net benefittively, they did not feel that they overesti- within some categories. Figure 5 shows amated the treatment effect of Schmidt's scatter pldt comparing net benefit versussyndrome. Although treatment of the syn- ranking. Net benefit was not an important
drome is not effective, individual conditions determinant of ranking for services high onthat make up the syndrome are listed and the list. However, few cr pairs at the bottomcovered elsewhere on the list. Our point is of the list had high net benefit. The OTAthat determination of treatment effective- analysis examined which services went uphesshad a strongsubjectivecomponent, and which serviceswent down asafunction
The greatestproblemfacingimplementa- ofthecommissionreview.Servicesthathad
tionof the model islackofscientificdata. high benefitrarelymoved fardown thelistWe need considerablymore researchon the (more than 100 lines).However, services
efficacyofclinicalinterventions.Intheab- thatmoved up the listmore than 100ranks
sence of systematicdata,subjectivejudg- were likelytobethosethathad few benefits.
ments areused.The highdegreeofsubjec- Few of the servicesthatended UP on the
tivityinevaluatingmedicaleffectivenesshas lowestend ofthelist(rightportionofFigure
gone largelyunchallengedby philosophical 5)had much expectedbenefit.Thissubjec-
criticsoftheOregon proposal, rivereadjustmentof the listhas alsore-
ceivedconsiderablylessattentionthanthe
Commission Reehuffling use of preference weights.
One ofthe most importantconcernsre- Resubmi_ion and Acceptancegarding Oregon's model is that the commis-sioners took it upon themselves to reorgan- After the disappointing August 1992 re-ize the list. They argued that this was jection by DHHS, Oregon revised and re-necessary because many of the rank orders submitted its application. In November 1992were illogical or in other ways inconsistent they submitted a modified program thatwith the commissioners" expectations, changed the prioritization method to elimi-
In their final report, the Oregon Health nate any consideration of quality of life. TheServices Commission commented that rationale for eliminating this aspect of thechange in rankings were done rarely. How- methodology was that is was "subjective."ever, a review of the February 1, 1991 versus The new method ranked 688 pairs of condi-the May 1, 1991 list suggests that changes in tions and treatments in two stages. First, therankings were common. These changes were treatments were subjectively ranked by el-reviewed in detail by the Congress Office of fectiveness. The criteria for establishingTechnology Assessment. 7Further, the intro- effectiveness included preventing death,duction of the 1992 and 1993 lists saw con- returning patients saved from death to an
995
KAPLAN MED]CAL CARE
asyrnptomaticstate, retumingsymptomatic their benefits. Although AIDS patientspatients to an asyraptomatic state, and aver- would not get essentially useless treaiment,age cost of the procedure. Instead of using comfort care would be given to these pa-public preferences, conditions were ranked by tients because it was near the top of the list.medical experts and the commissioners reor- In the revised application, the Oregon com-dered the lists to be consistent with the values missioners dealt with the problems by sire-they perceived to be representativeof Oregon ply eliminaKng the line. An analysis of thecitizens. By eliminating the Quality of Life revised 1992 list by the Office of Technologyportion of the model, Oregon answered some Assessment showed that only 25% of the CTof the criticisms in the initial DHHS review, pairs on the 1992 list were within 25 lines ofHowever, they created new problems because where they were in 1991 and 30% of the
they eliminated the possibility of estimating pairs had moved 100 or more ranks. Changecost per quality adjusted year of life in an oh- in methodology and commissioner sub]ec-jective manner, five judgment had a substantial effect on ul.
Afraid of further criticism, the Oregon corn- fimate rankings.rmssioners moved items or reassigned the con- Ironically, the new system has greater poten-tent of many condition-treatment pairs. Forex- tial to discriminate against people with disabili-ample, two of the placements that drew most ties. Using the preference weighted system, itcrifidsm in the 1991 exercise were life support is possible to quantify benefits of treatmentsand medical support for very low birth weight that make small quality of life improvementsbabies and heroic care for end-stage AIDS pa- for people with chronic medical problems.tients. In both of these cases, evidence sug- However, many treatments fur people with dis-gested that medical care contributed nothing to abilities neither improve life expectancy oreither quality oflife or duration of tife.However, move people to asymptomatic states. It is pre-ma_ critics made emotional pleas to the media dsely these small changes that are most likely toand suggested that deserving citizens would be be disregarded.
condemned to death by the plan. The C_'¢on adminLCaation has encouragedLife support for babies born less than 5(30 states to experiment with different approaches
grams and less than 23 weeks gestation was to Medicaid. In March 1993, they approved theranked 708 in the 1991 list because chi1&_ in revised plan and it was implemented in earlythis condition have an estimated pmbahlity of 1994.
of 0.00. To avoid criti_wu the commis-sioners eliminated this line.and created a new
one for q.ow birth weight (under 7,_500grams)."This line also allowed the elimination of an- At least four levels of human judgment
other controversial treatment (m_lical ttr_r'apy were used in the construction of Oregon pri-for ir_traventriollar and subarachnoid hereof- ofitized list. Am ong these four, there wasrhage of fetus or neonate) that was ranked 687 substantial justification for the use of thein 1991. The commissioners then placed medi- utility rating system.
cal and life support services for low birth v_ight The August 1992 rejection of the applica-babies as number 40 on the list. Medical ther- tion emphasized the subjective ratings foraW for end stage HW disease was line 702 on quality of life. Yet, among the four levels of
the 1991 list This drew heavy criticism from subjective judgment, only the preferencegroupsinadvocacyforpeoplewithAIDS.How- weight component was obtained using aever,theplacementwas basedon theevidence systematicmethodology thathas replicatedthat end stage treatment has no _ or quality other findings. The list that was approved inofl/.fe and may even shortenlife expemmcybe- March of 1993 left considerably more roomcause the toxic effects of treatment may ex_ed for subjective biases.
986

Vol. 32, No. 10 VALUEJUDGMENTIN OREGONMEDICAID
Cost-effectiveness analysis is receiving in- dictory with the notion that people with dis-creasing attention as a approach to resolving abilities need medical services. People whohealth care problems. For example, both the are at optimum health (1.0 on the QWBprovince of Ontario, Canada and the Aus- scale) may need fewer services than thoseitalian government have endorsed prioriti- who occupy lower levels. Quantifying thesezation schemes to make formulary deci- differences allows us to set priorities for fu-
sions. Application of these methods should ture resource allocation. If, for the sake of at-rely on the strongest methodologies avail- gument, we decide to score people with dis-able. Consumer utilities for health states are abilities 1.0 and they with stay there withoutan important part of health status and can treatment, it would follow that we shouldbe measured reliably, not provide any services for these individu-
Elimination of preferences from the Ore- ads because they have already achieved theoptimum level of weUness. Scores lower thatgon resource allocation model was not only " '
misinformed, it was incorrect. It assumed 1.0 suggest that resources should be used tothat there would be discrimination against improve these conditions. This in no waypersons with disabilities because treatment implies that the lives of people with disabili-could not improve theiz chronic problems, ties are valued less that those of peopleHowever, this analysis makes a serious con- without disabilities. The most importantceptual error. Effectiveness of treatment is point is that judgment was not made on thebased on estimated course of the illness basis of rating of disability, but rather onwith and Without treatment A treatment the basis of expected improvement as a
that sustains life, even without improve- result of treatment. The only referencemerits in quality of life, produces very sub- cited when former Secretary of Healthstantial benefits. For example, suppose a and Human Services Louis Sullivan rejectedperson is an acddent that leaves him or her the Oregon application in 1992, was anin a state rated 0.5 on a 0 to 1.0 scale. Fur- unpublished paper by Hadorn. zs However,
ther suppose that a treatment will maintain Hadorn's conclusion was ignored. He notedthem at this level while absence of treat- that"Itis the changein qualityoflife, ornetment wiU result in death. According to the benefit realized fi'om treatment that mat-Oregon model, the treatment will produce ters, not the point-in-time quality of life of0.50 (calculated as 0.50--0) for each year the the patient".person remains in that state. That is a pow- Because of the DH]-IS challenge, Oregonerful treatment effect in comparison to eliminated the quantitative utility data andmost alternatives. The crucial element is developed a prioritized list that excludedthat the treatment works. The system does quality of life decisions. In doing so theyattempt to exclude treatments that neither gave up the most replicable part of theirextend life nor make patients better in con- methodology. Subjective, judgments are antrast to those not receiving treatment. In unavoidable part of priority setting. Policy-other words, the targets for elimination are makers must acknowledge what aspects ofonly treatments that use resources and do their decisions depend on human judgmentnot make a difference, and they must use the most reliable and
The August 1992 DHHS decision also valid methods to capture them.misrepresented the meaning of quality of
life scores. They assumed that having a low Acknowledgmentsquality of life score was discriminatory be-
cause people with disabilitiesand those TheauthorthanksMariaHewi_Paig_Spies-lv_Itz_withoutdisabilitieswould notbe ratedthe Dan-en_ Lu_Lotd-LippincottandBobDiPTetesame. AIternatively, the statement is contra- for_ commentsonanearlierdraftof this paper.
987

KAPLAN MEDICAL CARE
References 16. Kaplan RM. The Hippocratic Predicament: Af-fordability, access, and a_ountab_ity in American medi-
1. HadomDC.Settinghealthcare_ inOre- cine.SanDiego:AcademicPress,1993.gon: Cost-effectiveness meets the rule of n_cxm. JAMA 17. Kaplan RM. Health-related quality of life in pa-19'91;265".2218. tient decision making. Journal of Social Issues
2. Hadorn DC. Reply to doctors GdZette and 1991;47:69.MacLean. JAMA 1991; 266:1081.
18. Kapl_n RM, Bush JVV,Berry CC. The reliability,
3. Hadom DC. The problem of dis_iminafion in _,ability, and generMiTability of a health s_atus index:health care priority set, rig. JAMA 1992;268:1454. American Statistical Amociation, Proceedings of the 5o-
4. Eddy DM. What care is "e_,ential'? W'hat services cial Status Section 1978:704.
are"basic"? JAMA1991;265:782- 19. Kaplan RM, DeBon M, Anderson BF. Effects of5. Eddy DM. Oregon's methoc_. Did co_e- number of rating scale points upon utilities in a Quality
ne_ anab_is fail? JAMA 1991",266'.2135. of Well-being scale. _ Care 1991;29:.1061.
6. Strosberg MA, Wiener JM, Baker R. Rationing 20. Kaplan P.M. Value for money in management ofAmerica's Medical Care: The Oregon Plan and Bey_ad, HIV: Health-related quality of life. In: Maynard A, ed.Washington, DC: Brookings, 1992. Economic as'peers of HIV management. London: Col-
T. Office of Technology Assessment, Un_ed States wood, 1991:19.Congress. Evaluation of the Oregon Mediraiel p_ 21. Rokeach M. The nature of human values. NewWashingt or_ D C: U-S. Gov_rnm ent Printing Off_'_e,1992. York: Free Press, 1973.
8. Brook R.H, Lohr IC _ we need to ration effective 22. Balaban DJ, Fagi PC, Goldfarb _ et al. Weightshealth care? Issues in Science and Technology 1986;3:68. for scoring the Quality of WeB-being in._rmnent among
9. Kitzhabar J. The Oregon Basic Health Services rheumatoid acthritics. Med Care 1986;24:973.
A_. Salem, OR: Oregon State Senate, 1990. 23. Nerenz DR. Golob K. Trump DL. Preference10. Kaplan RM, Anderson ]E The general health po]- weights for the Quality of Well-being Scale as obtained
icy model: An integrated approach. In."Spilker B, ed. fi'om oncology pafier_. Unpublished Paper, Henry FordQuality of Life Assessments in Clinical Txiats. New York: Hospital, Detroit, Michigan: 1990.
Raven. 1990;131. 24. EuroQol Group. Eu.roQol: A new facility for the11. Torrance GW. Measurement of health state utili- measurement of health-related quality of fife. Health
ties for economic appraisal: A review. Journal of Health Policy 1990;16:199.
_cs 1986;5:1. 2.5. Patrick D, Sittanpalam Y, Somerville S, et al. A
1Z Daniels N. Is the Oregon rationing plan fair? cax_ss-cultural comparison of health status values. Am JJAMA 1_: 2232. PublicHealth 1985; 75:1402.
13. LaPuma J,Lawior F_Quality-adjusted life years: 26. Mulley AJ. As_g patient'sutilities: Can the
implications for clinicians and poliO, ends justify the means? Med Cam 1989;27".,$269.
JAMA 1990",263'.2917. 27. Weinstein MC, St_on W'B. Hypertension= A pol-l4. Jajich-Toch C, Roper BW. Americans' views on icy perspective. Cambridge, MA: Harvard University,
health care: A study in contradictions. H_.Mth Aft" 1976.
1990=9=.149. 28. Hadorr_ DC. The Oregon priority-setting exer-15. V_ener yM, Oregon's plan for health care ration- ci._: Quality of life and public policy. Hastings Center
ing. Brookings Review 1992;Winter.26. Report 1991;21(Supp13):S11.#
988