value experience results - tennessee hfma · ♦ national practice based in chadds ford, ... –...
TRANSCRIPT
EXPERIENCEVA
LU
E
RESULTSDon’t Lose Focus Around
Shadow Billing

Agenda
♦ Welcome and Introduction♦ Background on Medicare Advantage
– Industry Landscape– Rules and Requirements– What is Shadow Billing?
♦ Medicare Advantage Shadow Billing Reimbursement– Why Shadow Bill?– How do Eligible Hospitals get paid?
♦ Shadow Billing Issues– Challenges– Best Practices
IMA Consulting Overview
♦ Established in 1996♦ National practice based in Chadds Ford, Pennsylvania with over 100 professionals♦ Clients range from large for-profit & not-for-profit health systems, to academic medical centers, to
small community hospitals♦ Partners and the leadership team are actively engaged in providing client services♦ Multi-Year awards for “Best Places to Work in Healthcare”♦ Three “Service Sets”
– Revenue Management– Expense Management– Interim Management
♦ Five core lines of business– Finance– Medicare Reimbursement– Revenue Enhancement and Recovery – Revenue Management– Operations Improvement
What is Medicare Advantage?
♦ Dates back to the 1970’s– Balanced Budget Act of 1997– Medicare Modernization Act of 2003
♦ Approved by Medicare; operated by private companies
♦ 31% of all Medicare eligible population (55 Million) are enrolled in a Medicare Advantage plan
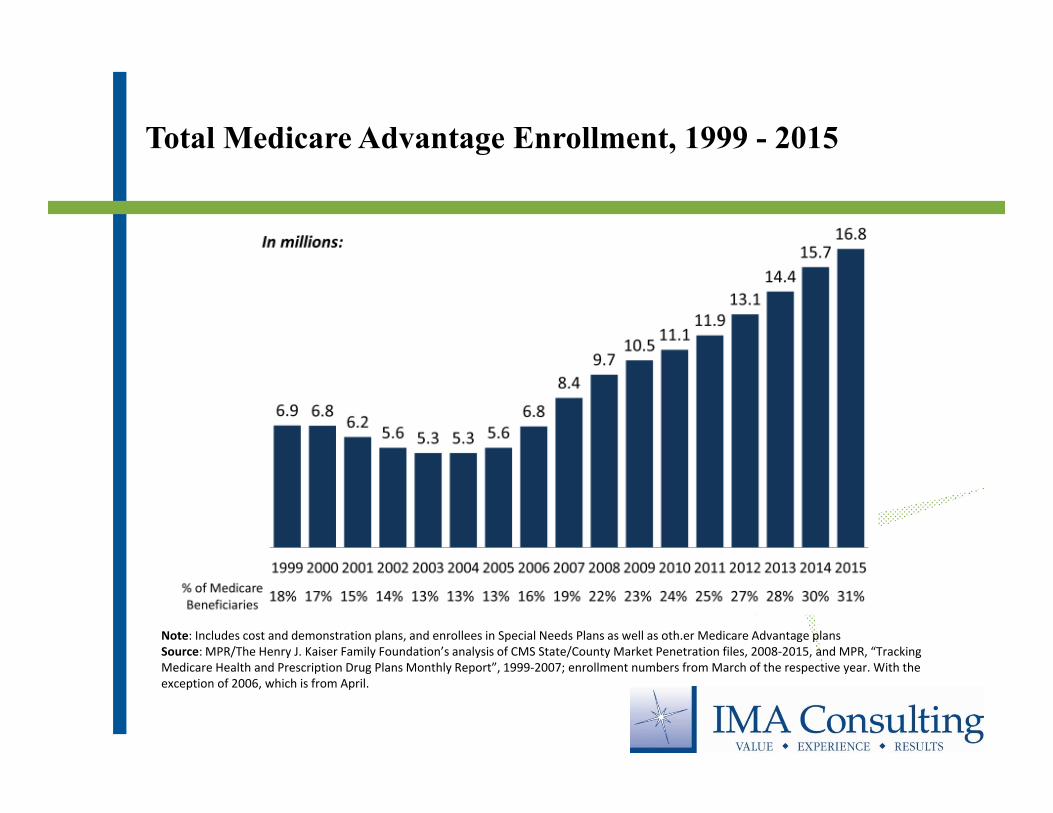
Total Medicare Advantage Enrollment, 1999 - 2015
Note: Includes cost and demonstration plans, and enrollees in Special Needs Plans as well as oth.er Medicare Advantage plansSource: MPR/The Henry J. Kaiser Family Foundation’s analysis of CMS State/County Market Penetration files, 2008‐2015, and MPR, “Tracking Medicare Health and Prescription Drug Plans Monthly Report”, 1999‐2007; enrollment numbers from March of the respective year. With the exception of 2006, which is from April.
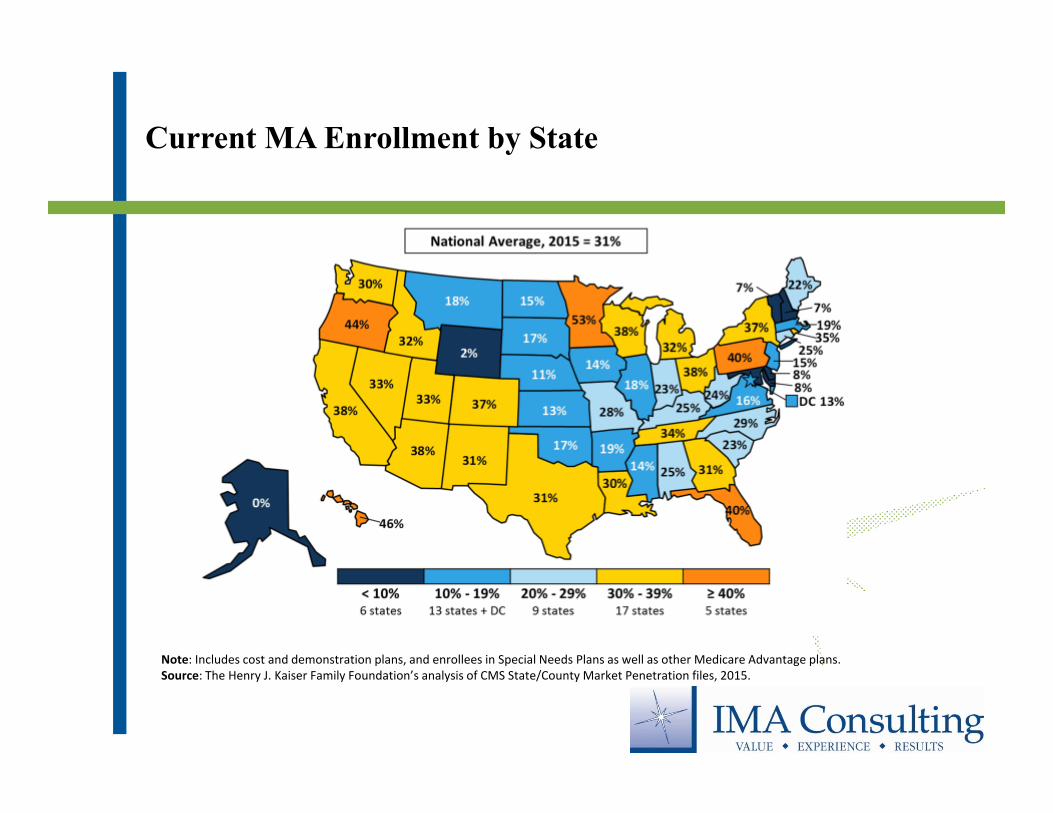
Current MA Enrollment by State
Note: Includes cost and demonstration plans, and enrollees in Special Needs Plans as well as other Medicare Advantage plans.Source: The Henry J. Kaiser Family Foundation’s analysis of CMS State/County Market Penetration files, 2015.
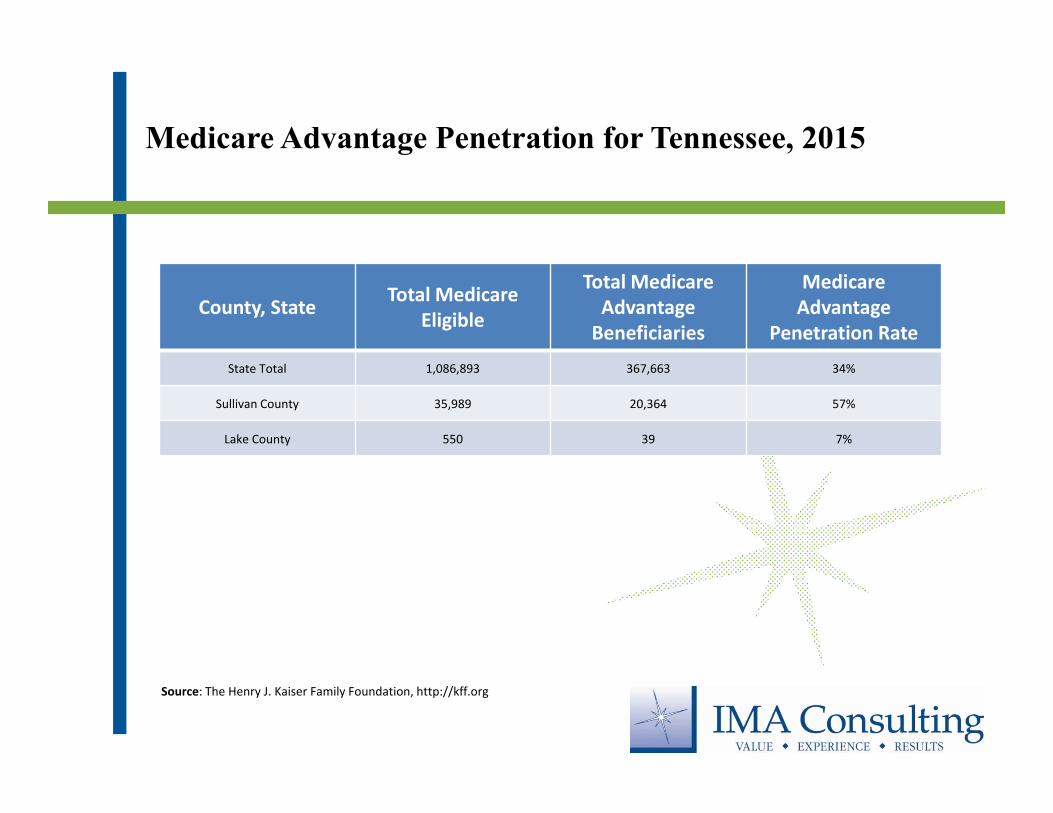
Medicare Advantage Penetration for Tennessee, 2015
County, State Total Medicare Eligible
Total Medicare Advantage Beneficiaries
Medicare Advantage
Penetration RateState Total 1,086,893 367,663 34%
Sullivan County 35,989 20,364 57%
Lake County 550 39 7%
Source: The Henry J. Kaiser Family Foundation, http://kff.org
Types of Medicare Advantage Plans
♦ Local Health Maintenance Organization (HMO)– Plan established network– Beneficiary must choose an in network primary care doctor – Beneficiary must get a referral to see a specialist
♦ Local Preferred Provider Organization (PPO)– Plan established network– Beneficiary does not need to choose an in network primary care doctor – Beneficiary does not need a referral to see a specialist
Types of Medicare Advantage Plans – cont’d
♦ Medicare Private Fee-for-Service (PFFS)– Plan established network– The plan decides how much the beneficiary must pay for services
♦ Regional Preferred Provider Organization (RPPO)– Similar to Local PPO– Established to expand Medicare Advantage access to rural beneficiaries
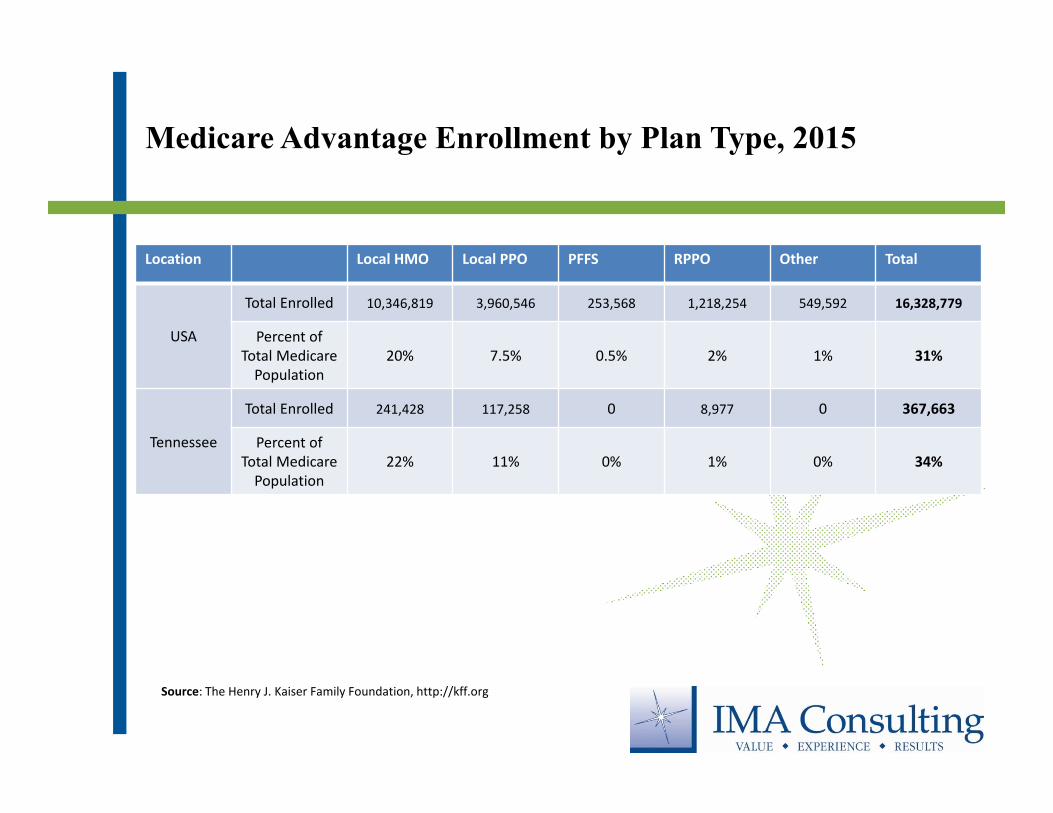
Medicare Advantage Enrollment by Plan Type, 2015
Location Local HMO Local PPO PFFS RPPO Other Total
USA
Total Enrolled 10,346,819 3,960,546 253,568 1,218,254 549,592 16,328,779
Percent of Total Medicare Population
20% 7.5% 0.5% 2% 1% 31%
Tennessee
Total Enrolled 241,428 117,258 0 8,977 0 367,663
Percent of Total Medicare Population
22% 11% 0% 1% 0% 34%
Source: The Henry J. Kaiser Family Foundation, http://kff.org
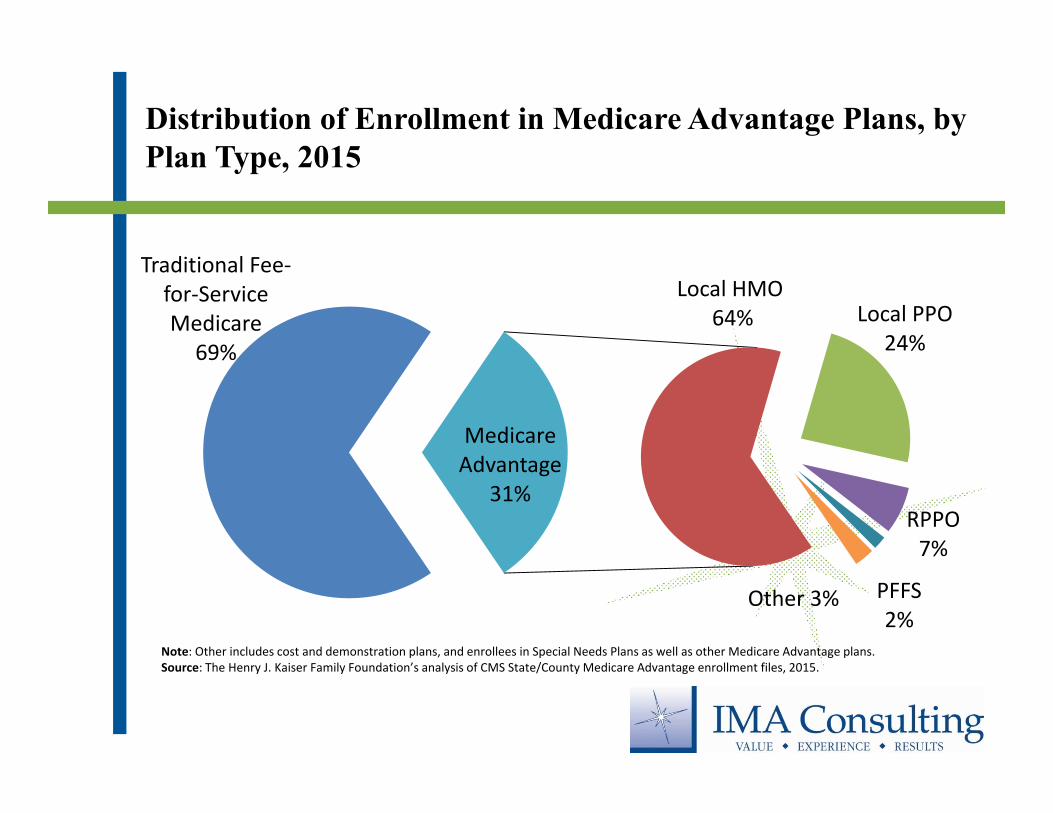
Distribution of Enrollment in Medicare Advantage Plans, by Plan Type, 2015
Traditional Fee‐for‐Service Medicare
69%
Local HMO64% Local PPO
24%
PFFS2%
Other 3%
RPPO7%
Medicare Advantage
31%
Note: Other includes cost and demonstration plans, and enrollees in Special Needs Plans as well as other Medicare Advantage plans.Source: The Henry J. Kaiser Family Foundation’s analysis of CMS State/County Medicare Advantage enrollment files, 2015.
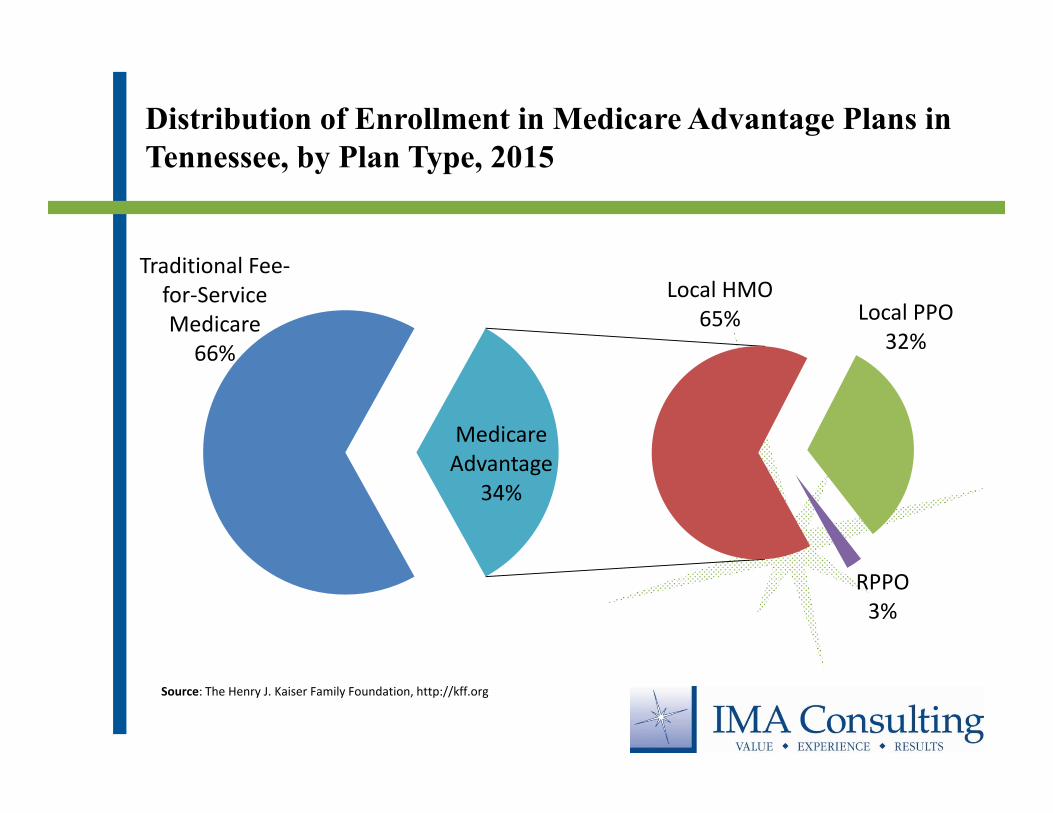
Distribution of Enrollment in Medicare Advantage Plans in Tennessee, by Plan Type, 2015
Traditional Fee‐for‐Service Medicare
66%
Local HMO65% Local PPO
32%
RPPO3%
Medicare Advantage
34%
Source: The Henry J. Kaiser Family Foundation, http://kff.org
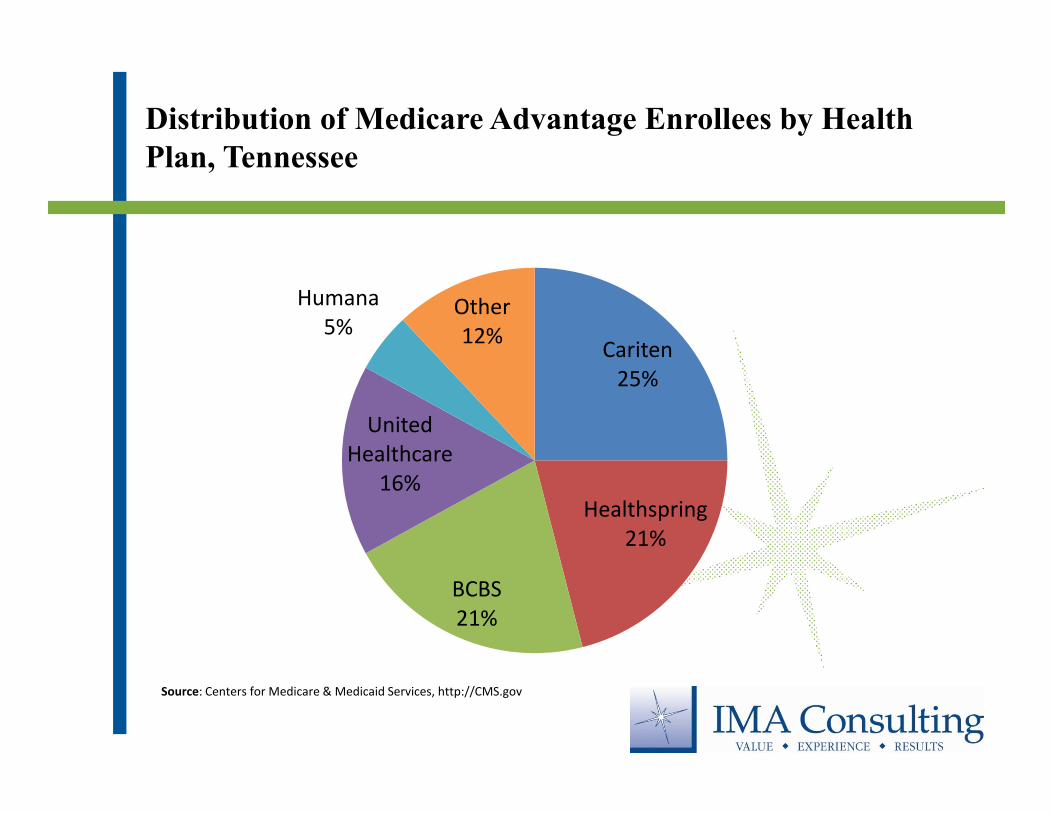
Distribution of Medicare Advantage Enrollees by Health Plan, Tennessee
Cariten25%
Healthspring21%
BCBS21%
United Healthcare
16%
Humana5%
Other12%
Source: Centers for Medicare & Medicaid Services, http://CMS.gov
Balance Budget Act of 1997 (105th Congress)
♦ Signed on August 5, 1997
♦ Additional payments for IME and GME costs of patients enrolled in a Medicare managed care program
♦ Created Shadow Billing (IME/GME payments) for teaching hospitals
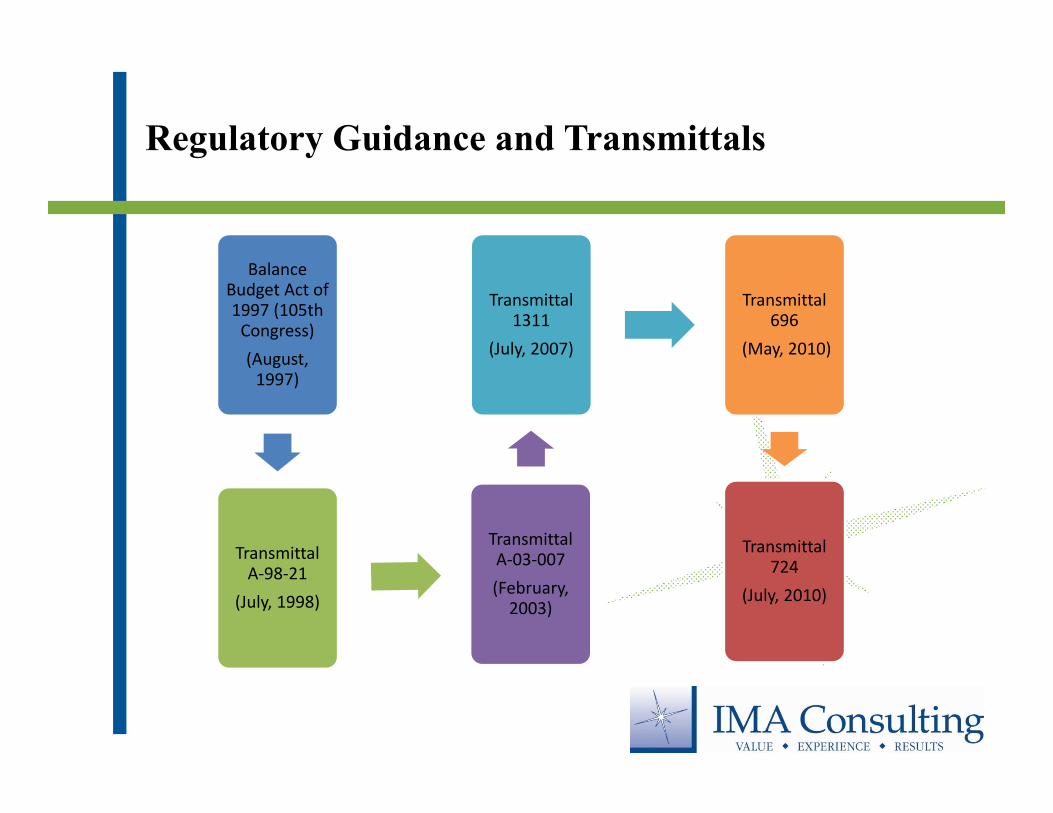
Regulatory Guidance and Transmittals
Balance Budget Act of 1997 (105th Congress) (August, 1997)
Transmittal A‐98‐21
(July, 1998)
Transmittal A‐03‐007 (February, 2003)
Transmittal 1311
(July, 2007)
Transmittal 696
(May, 2010)
Transmittal 724
(July, 2010)
What is Shadow Billing?
♦ Synonymous for “No Pay” or “Information Only” claim
♦ Claim is submitted to the Medicare Administrative Contractor (MAC) for Medicare Part A services provided to Medicare Advantage beneficiaries
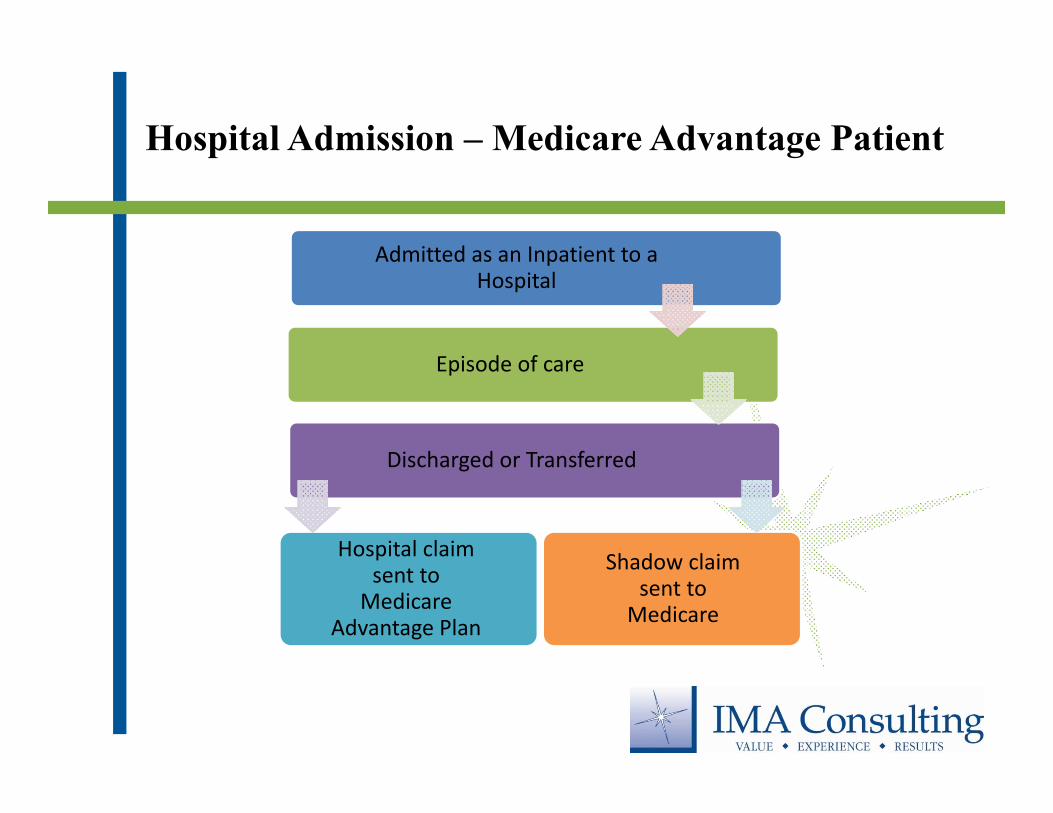
Hospital Admission – Medicare Advantage Patient
Admitted as an Inpatient to a Hospital
Episode of care
Discharged or Transferred
Hospital claim sent to
Medicare Advantage Plan
Shadow claim sent to
Medicare
Why Shadow Bill?
♦ Submitted for the purpose of receiving supplemental payments– Indirect Medical Education (IME)– Graduate Medical Education (GME)– Electronic Health Record (EHR) Meaningful Users
♦ Compliance
Indirect Medical Education (IME)
♦ Covers the indirect costs of teaching interns/residents
♦ Based on the ratio of the number of interns and residents per hospital bed
♦ Determined by inserting it’s individual intern/resident to bed ratio (IRB) into a formula established under Medicare statue
♦ Will typically receive their IME payment two weeks after submitting a Shadow Bill
♦ IME payments will appear on the PS&R report as a type 118 Report
Graduate Medical Education (GME)
♦ Covers the direct cost of a teaching program
♦ Based on the number of residents, the costs associated with training the residents and the hospitals Medicare patient load
♦ Additional GME dollars for each additional inpatient day
♦ Payments via Medicare Cost Report settlements
♦ Days associated with GME payments appear on PS&R report as a type 118 report
Electronic Health Record (EHR) Meaningful Users
♦ Incentive payments to eligible hospitals
♦ Rewards the adoption and meaningful use of:– Health Information Technology (HIT)– Electronic Health Records (EHR)
♦ Began receiving payments in any year from FY 2011 – FY 2015
♦ FY 2016 is the last year for incentive payments for Medicare purposes
Additional Reasons to Shadow Bill
♦ Medicare fraction of the Disproportionate Share Hospital (DSH) calculation
♦ Nursing Allied Health Education (NAHE) payments
♦ Compliance
Shadow Billing Challenges
♦ Day-to-day challenges
♦ Niche part of revenue cycle
♦ Missing information
♦ Follow up
Shadow Billing Challenges – Cont’d
♦ May not be top priority for non-teaching facilities
♦ System conversions
♦ Medicare timely filing guidelines
Shadow Billing Best Practices
♦ Understand
♦ Reconcile
♦ Review
♦ Communicate
♦ Be creative

Conclusion
Don’t Lose Sight
Mario Feher, Director6 Hillman Drive, Suite 100
Chadds Ford, PA 19317
215-514-0951
www.ima-consulting.com
Contact Information
27