use of ketamine as a fast acting antidepressant for
TRANSCRIPT
USE OF KETAMINE AS A FAST ACTING
ANTIDEPRESSANT FOR TERMINAL CANCER
PATIENTS WITH MAJOR DEPRESSIVE
DISORDER
Claudia Grott Zanicotti
A thesis submitted for the degree of Master of Medical Sciences
of the University of Otago
Dunedin School of Medicine
New Zealand
March 2012

! """!
ACKNOWLEDGEMENTS
After one year of new experiences and a complete change in my lifestyle, I can look back and
see how much I have learned. Obviously, the certainty that there is much more knowledge
ahead is a factor that keeps me motivated, but without the support from my loved friends and
family I would have never achieved one more goal. Thank you all!
It has been a hard year for my family, as we are physically very distant, but emotionally
incredibly close. I hope to see you soon (in New Zealand). I would also like to thank my
husband for being so supportive at all times, I would not be here without you. I love you all!
I would like to thank the staff from the Oncology Department, specially the oncology nurses
and receptionists. Your help with patient’s charts and arranging appointments was essential in
my learning process. I’m also grateful to the Psychological Medicine Department staff,
particularly for been so helpful and welcoming. Roz and Jill: thank you for all your help, for
the arrangements with conferences, and for always clarifying any doubts or questions. I was
also lucky to meet some great people during my stay in the first floor and I really enjoyed our
brief but unforgettable talks, and I sincerely hope these were just the first of many. Sarah was
the best office mate I could have ever found, incredibly friendly and respectful. Also, I am
thankful for the support from Otago Medical Research Foundation Inc. and the Otago
Community Trust.
I am thankful for the help and support of my supervisor and co-supervisor, Professor Paul
Glue and Associate Professor David Perez. Your constant feedback kept me positive during
the toughest times. Professor Paul, I am eternally grateful for your support since the very
beginning, even before I came to New Zealand. Thank you for your constant patience and for
dedicating so much time to this thesis. I definitely met an amazing professional and a person
of incredible character.
My very special thanks goes to the patient who made all of this possible. You are a unique
person, and your patience with the constant assessments was very kind of you. Thank you so
much!

! "#!
ABSTRACT
The objective of this thesis was to investigate the safety and efficacy of single and repeated
administration of ketamine as a fast acting antidepressant in patients with terminal cancer.
Associated with this objective was a comprehensive review of the pathophysiology of major
depressive disorder, existing treatments for major depressive disorder, and a review and meta-
analysis of treatments for depression in patients with cancer. The use of ketamine in
treatment-resistant depression was also reviewed, along with a meta-analysis of mood
responses in placebo-controlled studies, and data from case reports and case series.
The review and meta-analysis of antidepressant treatments for depression in cancer patients
yielded only two small placebo-controlled randomized trials, both for mianserin. No
psychotherapy trials were found that met inclusion criteria for this analysis. The two
mianserin trials showed a benefit in improving mood ratings compared with placebo. The
very limited amount of data on treatment of depression in this population is surprising, and
further research is needed to improve knowledge in this area.
The review and meta-analysis of mood responses to ketamine in three placebo-controlled
randomized crossover studies demonstrated a robust improvement in mood ratings by four
hours, that was sustained up to 72 hours. Uncontrolled data from case series and case reports
showed similar profile to data reported from the placebo-controlled studies.
The study investigates the effect of ketamine on mood ratings in depressed patients with
cancer had three stages; (1) to assess whether a single 1 mg/kg IM dose improved mood; (2)
to assess the effect of repeated 1 mg/kg IM dosing on mood; and (3) to assess the mood
responses to IM doses of 0.1, 0.5 or 1.0 mg/kg IM. This thesis reports the case of a single
patient who participated in Stages 1 and 2. The results in the case presented in this thesis were
positive, with remission of symptoms with single dose and repeated treatment, and
maintenance of remission with weekly injections of ketamine 1 mg/kg.
This thesis supports the possible use of ketamine as a fast acting antidepressant in terminal
cancer patients with Major Depressive Disorder. In a population with short life expectancy,
the existence of a treatment for depressive episodes with rapid onset of action would be
essential, and ketamine might be the option of choice.
! #!
TABLE OF CONTENTS
AUTHOR DECLARATION ........................................................................................... ii
ACKNOWLEDGEMENTS ............................................................................................ iii
ABSTRACT ...................................................................................................................... iv
TABLE OF CONTENTS .................................................................................................. v
LIST OF PUBLICATIONS ............................................................................................ ix
LIST OF FIGURES .......................................................................................................... x
LIST OF TABLES .......................................................................................................... xii
LIST OF ABBREVIATIONS ....................................................................................... xiii
1 INTRODUCTION ............................................................................................... 16
1.1 Introduction ......................................................................................................... 17
1.2 History of depression .......................................................................................... 18
1.3 Epidemiology of depression in Major Depressive Disorder and Bipolar
Disorder ………………………………………...………………………………. 19
1.4 Epidemiology of Major Depressive Disorder in cancer patients .................... 21
2 PATHOPHYSIOLOGY AND TREATMENT OF MAJOR DEPRESSIVE
DISORDER ……………………………………………………..……………… 23
2.1 Pathophysiology of Major Depressive Disorder ............................................... 24
2.1.1 Serotonergic system .............................................................................................. 26
2.1.2 Noradrenergic system ........................................................................................... 26
2.1.3 Dopaminergic system ............................................................................................ 27
2.1.4 HPA axis ............................................................................................................... 27
2.1.5 Gabaergic system .................................................................................................. 29
! #"!
2.1.6 Glutamatergic system ............................................................................................ 29
2.1.7 Cytokines .............................................................................................................. 31
2.2 Current treatments for depressive episodes ..................................................... 32
2.2.1 Psychotherapy ....................................................................................................... 32
2.2.2 Pharmacotherapy .................................................................................................... 32
2.2.3 Electroconvulsive therapy ..................................................................................... 33
2.2.4 Repetitive transcranial magnetic stimulation ........................................................ 34
2.2.5 Vagus nerve stimulation ........................................................................................ 34
2.2.6 Deep brain stimulation .......................................................................................... 35
3 REVIEW AND META-ANALYSIS OF AVAILABLE
TREATMENTS FOR DEPRESSION IN CANCER PATIENTS .................. 36
3.1 Introduction …………………………………………………………………… 37
3.2 Methods ………………………………………………………………….…….. 37
3.2.1 Search strategy ……………………………………………………...…...……… 37
3.2.2 Selection criteria …………………………………………..…………....………. 37
3.2.3 Analysis …………………………………………………..…………...………… 39
3.3 Results …………………….……………………………………………………. 39
3.3.1 Meta-analysis ……………….…………………………………………..……… 39
3.4 Discussion ………………………………………………………………………. 40
3.5 Conclusions …………………………………………………………………….. 41
4 KETAMINE OVERVIEW ………………………………………………...….. 43
4.1 Ketamine .............................................................................................................. 44
4.2 Ketamine as an anesthetic .................................................................................. 44
4.3 Ketamine as a drug of abuse .............................................................................. 44

! #""!
4.4 Ketamine as an analgesic .................................................................................... 45
4.5 Ketamine as a fast acting antidepressant ……………………..……………… 45
4.6 The possible use of ketamine as a fast acting antidepressant for terminal
cancer patients .................................................................................................... 46
5 REVIEW AND META-ANALYSIS OF KETAMINE AS A FAST ACTING
ANTIDEPRESSANT .......................................................................................... 47
5.1 Introduction ......................................................................................................... 48
5.2 Methods ................................................................................................................ 49
5.2.1 Search strategy ...................................................................................................... 49
5.2.2 Selection criteria ................................................................................................... 49
5.2.3 Analyses ................................................................................................................ 51
5.3 Results .................................................................................................................. 51
5.3.1 Randomized clinical trials ..................................................................................... 51
5.3.2 Case reports and case series .................................................................................. 54
5.3.3 Meta-analysis ........................................................................................................ 59
5.4 Discussion ............................................................................................................. 61
5.5 Conclusions .......................................................................................................... 62
6 PROTOCOL FOR TESTING KETAMINE IN MAJOR DEPRESSIVE
DISORDER IN TERMINAL CANCER PATIENTS ...................................... 63
6.1 Introduction ......................................................................................................... 64
6.2 Stages .................................................................................................................... 64
6.2.1 Stage 1 ................................................................................................................... 64
6.2.2 Stage 2 ................................................................................................................... 64
6.2.3 Stage 3 ................................................................................................................... 65

! #"""!
6.3 Inclusion and exclusion criteria ......................................................................... 65
6.3.1 Inclusion criteria ................................................................................................... 65
6.3.2 Exclusion criteria .................................................................................................. 65
6.4 Informed consent ................................................................................................ 69
6.5 Assessments ......................................................................................................... 69
6.6 Statistical analysis ………………………………………………….………….. 72
6.7 Conclusions ……………………………………………………….…………… 72
7 ACUTE AND MAINTENANCE IM KETAMINE FOR A DEPRESSED
PATIENT WITH TERMINAL CANCER ....................................................... 73
7.1 Introduction ......................................................................................................... 74
7.2 Case report ........................................................................................................... 74
7.3 Discussion ............................................................................................................. 81
7.4 Conclusions .......................................................................................................... 82
8 CONCLUSIONS ................................................................................................. 83
8.1 Conclusions …………………………………………………………….………. 84
9 REFERENCES .................................................................................................... 85
9.1 References ……………………………………………………………………… 86
APPENDIXES
Appendix I- Informed consent 103
Appendix II- Case report - in press (page proofs) 109

! "$!
LIST OF PUBLICATIONS
Zanicotti CG, Perez D, Glue P. Acute and maintenance IM ketamine for a depressed patient
with terminal cancer. Oral presentation at: The Royal Australian and New Zealand College of
Psychiatrists (RANZCP) 2011 New Zealand Conference. 2011 Sep 28-30; Queenstown, New
Zealand.
Zanicotti CG, Perez D, Glue P. Effects of low dose intramuscular ketamine on depression
ratings in depressed patients with cancer in palliative care – a case report (Efeitos da
quetamina via intramuscular em baixa dose nos escores de depressão em pacientes deprimidos
e com cancer sob cuidados paliativos – relato de caso). Oral presentation at: 11º Congresso
Brasileiro de Clínica Médica (SBCM). 2011 Oct 27-29. Curitiba, Brazil.
Zanicotti CG, Perez D, Glue P: Mood and pain responses to repeat doses intramuscular
ketamine in a depressed patient with advanced cancer. J Palliat Med 2011 [in press].

! $!
LIST OF FIGURES
Figure 2.1: Anatomical connections and interactions between neuroendocrine system,
BDNF, monoamines, and cytokines in the brain.
Figure 2.2: HPA axis dysfunction in MDD.
Figure 2.3: Tripartide glutamatergic synapse.
Figure 2.4: From inflammation to depressive symptoms.
Figure 3.1: Selection of trials for meta-analysis.
Figure 3.2: Meta-analysis of antidepressant trials in patients with MDD and cancer.
Figure 4.1: Relation between ketamine dosing and its indications.
Figure 5.1: Selection of studies for review and meta-analysis for ketamine as a fast acting
antidepressant.
Figure 5.2: HAM-D mean values for Diazgranados et al., 2010, Zarate et al., 2006, and
Berman et al., 2000.
Figure 5.3: Cases outcomes and Diazgranados et al., 2010 (HAMD).

! $"!
Figure 5.4: Cases outcomes and Diazgranados et al., 2010 (MADRS).
Figure 5.5: Case outcome and Diazgranados et al., 2010 (BDI).
Figure 5.6: Meta-analysis results based on change in HAMD scores.
Figure 6.1: MADRS.
Figure 6.2: HADS.
Figure 6.3: The Demoralization Scale.
Figure 7.1: Antidepressant and analgesic response to IM ketamine 1 mg/kg.
Figure 7.2: Changes in HADS and Demoralization scales with IM ketamine 1 mg/kg.
Figure 7.3: Pearson’s correlation between change in depression and pain scores.
Figure 7.4: Antidepressant response to repeated dosing, at intervals of 7 days and > 7 days.
! $""!
LIST OF TABLES
Table 2.1: Main mechanisms of action of antidepressants.
Table 5.1: Demographic and clinical data for RCT’s.
Table 5.2: Demographic and clinical data for cases.
Table 6.1: ECOG performance status.
Table 6.2: The Comparative Pain Scale.

! $"""!
LIST OF ABBREVIATIONS
ACTH Adrenocorticotropic hormone
ACTRN Australian New Zealand Clinical Trials Registry
AD Alzheimer’s disease
AMPA Alpha-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid
AMPARs AMPA receptors
BD Bipolar disorder
BDI Beck Depression Inventory
BDNF Brain-derived neurotrophic factor
CMI Cell-mediated immune
COPD Chronic obstructive pulmonary disease
CRF Corticotropin-releasing factor
CRH Corticotropin-releasing hormone
CVD Cardiovascular disorder
DBS Deep brain stimulation
DPP IV Dipeptidyl peptidase IV
DS Demoralization scale
DSM Diagnostic and Statistical Manual of Mental Disorders
EAAT Excitatory amino-acid transporter
EC Endocannabinoid
ECOG Eastern Cooperative Oncology Group
ECT Electroconvulsive therapy
GABA Gamma-aminobutyric acid

! $"#!
Gln Glutamine
Glu Glutamate
GluTs Vesicular glutamate transporters
HADS Hospital Anxiety and Depression Scale
HAMD Hamilton Rating Scale for Depression
HD Huntington disease
HIV Human immunodeficiency virus
HPA Hypothalamo-Pituitary-Adrenal
5-HT 5-hydroxytryptamine (serotonin)
HVA Homovanilic acid
IBD Inflammatory bowel disease
ICD International Classification of Diseases
IDO Indoleamine-2,3-dioxygenase
IFN Interferon
IL Interleukin
IM Intramuscular
IV Intravenous
LC Locus coeruleus
MADRS Montgomery-Asberg Depression Rating Scale
MAOI Monoamine oxidase inhibitor
MDD Major Depressive Disorder
MDE Major depressive episode
mGlu Metabotropic glutamate
mGluR Metabotropic glutamate receptor
! $#!
MRS Magnetic Resonance Spectroscopy
MS Multiple sclerosis
mTOR Mammalian target of paramycin
NA Nucleus accumbens
NMDA N-methyl-D-aspartate
NMDARs NMDA receptors
PD Parkinson’s disease
PEP Prolyl endopeptidase
PFC Prefrontal cortex
QIDS-SR 16 The Quick Inventory of Depressive Symptomatology –Self Report (16
items)
RCT Randomized clinical trials
SD Standard deviation
SERT 5-HT transporter
SLE Systemic lupus erythematosus
SNARE Soluble N-ethylmaleimide sensitive factor attachment protein receptor
SNRI Serotonin-norepinephrine reuptake inhibitors
SSRI Selective serotonina reuptake inhibitors
TMS Transcranial magnetic stimulation
TNF Tumor necrosis factor
TRYCATs Tryptophan catabolites
VNS Vagus nerve stimulation
VTA Ventral tegmental area
WHO World health Organization
! %&!
CHAPTER 1
Introduction
!

! %'!
1.1 Introduction!Major Depressive Disorder (MDD) is the most common psychiatric illness, and it affects
more than 120 million people worldwide (more than 27 times the population of New
Zealand). It is characterized by depressed mood and loss of interest and pleasure, but other
signs and symptoms are commonly present, such as: weight loss or gain; sleep disturbance
with insomnia or hypersomnia; fatigue; lack of concentration; feelings of guilt; suicidal
ideation; and psychomotor agitation or retardation (Skolnick et al., 2009; Statistics New
Zealand, Jan 2012; DSM IV). These symptoms must persist for at least 2 weeks, and must be
accompanied by significant distress or impairment. Also, in addition to its high prevalence,
depression presents the greatest proportion of burden due to nonfatal health outcomes (World
Health Organization - World Health Statistics, 2007). !!In patients with cancer, the prevalence of depressive episodes is higher than in general
population (Mitchell et al., 2011). Although it may seem unsurprising, special attention must
be given to this group, as there is a higher risk for depressed patients not to accept proper
cancer treatment (Colleoni et al., 2000). Thus, any depressive symptom should be recorded
and questioned in every follow-up appointment, and adequate treatment should be provided as
fast as possible, in the presence of a depressive episode. Available treatments for depression
will be described further in this chapter.!!Ketamine is an anaesthetic agent that has demonstrated antidepressant properties
(Diazgranados et al.,2010; Berman et al., 2000; Sofia and Harakal, 1975). Its unique quality is
the very fast response relative to dosing, occurring within few hours (Zarate et al., 2006;
Machado-Vieira et al., 2009). Also, the duration of ketamine’s antidepressant effects is of 3
days or more (Zarate et al., 2006; Berman et al., 2000), even though its half-life is of about
2.5 hours (Ketalar® - Medsafe). The reasons for these effects will be partially explained in
this thesis, as the action of ketamine in the brain is not fully understood. Also, the possibility
of using this medication for depressed individuals with short life expectancy, such as terminal
cancer patients, will be discussed.! !In summary, this thesis will cover several topics:
Chapter 1: introduction and epidemiology of depression;
Chapter 2: pathophysiology and treatment of MDD;
Chapter 3: literature review and meta-analyses of effectiveness of antidepressant treatments
in patients with cancer;
! %(!
Chapter 4: ketamine overview;
Chapter 5: literature review and meta-analysis of effectiveness of ketamine in MDD and
depressive episode of bipolar disorder, both case series and randomized clinical trials;
Chapter 6: description of a protocol for treating MDD in cancer patients;
Chapter 7: description of single and repeat dosing for a patient with MDD and terminal
cancer;
Chapter 8: conclusions about the possible use for ketamine as a fast acting antidepressant for
depressive episodes in terminal cancer patients.
!!1.2 History of depression!Depressive symptoms have been described since ancient history, and writings regarding them
were even found in Ancient Egyptian papyri. Also, the Bible presented King Saul with
symptoms of depression (Davison, 2009; Huisman, 2007). In ancient Greece, supernatural
explanations were provided for these symptoms, such as evil spirits and punishment from
gods, but during the 6th century BC, these explanations started losing their impact in Greek
culture.!! The first statement that melancholia (which in ancient times was described by depressive
symptoms, among others) was caused by a dysfunction of the brain was made by Hippocrates
(460- 377 BC). He believed that the excess of “black bile” in individual’s brains was
responsible for melancholic symptoms, giving rise to the humoral theory (first postulated by
Empedocles) for melancholia (Davison, 2009; Bos, 2009). However, centuries latter, the
Christian Church stated again that melancholia was a disease of the soul. This idea brought
back supernatural experiences as a possible cause for depressive symptoms, and many women
were then at risk of being considered witches and condemned to be burnt at the stake (Daly,
2007).!!In the 20th century, more plausible explanations for the symptoms of psychiatric illnesses
were raised. Emil Kraepelin adopted a somatic approach, while Sigmund Freud emphasized
psychological factors, although biological factors were also considered in his hypotheses. In
1930’s, the initiation of treatments, such as electroconvulsive therapy and psychosurgery,
raised the need for clinical categories for treatment decisions (Davison, 2009).!!!
! %)!
!1.3 Epidemiology of depression in Major Depressive Disorder and Bipolar Disorder!Patients with Major Depression and Bipolar Depression have depressive symptoms (such as
depressed mood, diminished interest in activities, diminished ability to concentrate, alteration
in appetite, fatigue, feelings of guilt, suicidal thoughts) alternately with euthymia (normal
mood). In patients with BD, episodes of hypomania/mania (usually with grandiosity, reduced
need to sleep, running thoughts, pressure to keep talking, excessive involvement in
pleasurable activities that may be harmful, distractibility and psychomotor agitation) are also
present, at some time in their lives (DSM IV).
!The yearly prevalence of MDD in general population in the United States is around 6.7%. In
New Zealand, according to The New Zealand Mental Health Survey 2003/4, almost the same
prevalence is found, with major depressive episodes (MDE) affecting 6.6% of general
population (Kessler et al., 2005; Scott et al., 2010). In the New Zealand survey, these episodes
were more commonly found in females (8.1% versus 4.9% in males). Fewer than 10% of
MDE episodes were considered mild, with over half being severe or very severe. Also, just
one-third of patients with severe impairment received treatment from mental health services.
This information may help doctors with the awareness of considerably high prevalence of
depression among patients in general population and its severity. !!Besides differences between MDD and BD, in BD depression is the most experienced mood
(Mitchell and Malhi, 2004). In both cases, there is a correlation with cardiovascular disease,
obesity, metabolic syndrome, dementia, low income, marital status, and others (Weiner et al.,
2011; Ko et al., 2010; Keddie, 2011; Fiedorowicz et al., 2008; Byers and Yaffe, 2011;
Kessing and Andersen, 2004; Schofield et al., 2011; Schoeyen et al., 2011; Yan et al., 2011).
Some associations seem to be explainable, such as lack of exercise and eating habits
associated with metabolic syndrome. However, it is hard to analyse these correlations as cause
of depression, its consequence, or as part of a broader syndrome (Kahl et al., 2011). Also,
these individuals have a higher risk of suicide, and there are more deaths from unnatural
causes in the unipolar depression group, when compared to bipolar depression (Osby et al.,
2001; Black et al., 1987). The costs of depression are high, for example, the economic burden
in USA was of almost $44 billions in 1990 (Greenberg et al., 1993). General medical care
costs are much higher than those with general population, even for depressed subjects that are
on treatment (Bosmans et al., 2010). Although this population maintains an intense use of
professional care, they have higher chances of not meeting their needs, and of having a

! *+!
chronic illness, that may be due to inadequate treatment (Bijil et al., 2000; Pincus and Pettit,
2001). Not only mental health professionals should be aware of these facts, but also general
practioners, as according to Bijil et al., 2000 and Lepine et al., 1997, the majority of
individuals with depression look for treatment in primary care. Thus the treatment for
depressive symptoms is of great importance in both mood disorders.
For the estimation of the global burden in patients with MDD (World Health Organization –
WHO), symptoms severity were split in disability weights: 0.14, 0.35, and 0.76 for mild,
moderate and severe, respectively (Ustün et al., 2004). Actually, many individuals suffer from
chronic or recurrent depression, with some of these patients achieving recovery only 6 months
after initial treatment (50% of recovery, according to Pincus and Pettit, 2001). In Major
Depression, there is less chance of recovery over time with symptomatology, and with each
subsequent episode (Lavori et al., 1994; Keller et al., 1992), leading to a high prevalence of
chronically affected patients, who make up 26.8% of patients with MDD (Satyanarayana et
al., 2009). Moreover, according to the WHO, there is an estimative that, in 2030, unipolar
depression will be the second leading cause of disability adjusted for life years. This is similar
to a previous projection made for 2020 sixteen years ago (Mathers and Loncar, 2005; Murray
and Lopez, 1996). The World Health Organization also states that MDD already comprises
10.7% of total global years lived with disability, and BD accounts for other 2.5% (Ustun et
al., 2004; Ayuso-Mateos, 2006).
Antidepressant treatment for MDD is known to be effective, even though remission rates are
considered not optimal (Khawam et al., 2006; Trivedi et al., 2006). However, its use for
depressive episodes in patients with BD is not clearly beneficial, with some authors reporting
response to antidepressants in this group (Pacchiarotti et al., 2011; Ghaemi et al., 2008) and a
recent review (Sidor and Macqueen, 2011) suggesting that antidepressants are of little help for
acute treatment of depressive episode in BD. Also, Sidor and Macqueen, 2011 state that the
risk of mania switch depends on the criteria used to evaluate it. This risk has been
continuously investigated, and includes cycle acceleration, mania, hypomania and mixed
switch (Amsterdan and Shults, 2010; Pacchiarotti et al., 2009; Ghaemi et al., 2008; Goodnick,
2007). Considering the low response in depressive episodes achieved with antidepressant
medications available, treatment alternatives are desirable.

! *%!
1.4 Epidemiology of Major Depressive Disorder in cancer patients
Depression rates in individuals with advanced cancer are very high, affecting approximately
15% of patients (Mitchell et al., 2011), and when considering subsyndromal depression (the
presence of depressive symptoms that do not meet criteria for MDD) the numbers are even
higher (Boyes et al., 2011). Although diagnoses of adjustment disorder and of minor
depression are quite common in cancer patients (Mitchell et al., 2011), initial support and
follow up of depressive symptoms is very important to ensure appropriate treatment.
Psychological support must be considered for cancer patients during their treatment. For
better results, it should start from the time of cancer diagnosis and, in addition, support for
relatives and caregivers should also be provided (McLean et al., 2011; Kang et al., 2012). !
It is important to be aware that recent data demonstrates even higher rates of depression in
patients prior to commencing chemotherapy, with prevalence as high as 25% (Breen et al.,
2009). Furthermore, suicidal ideation has been found in 10% of cancer patients, who were
more frequently females, with worse interpersonal relationships, significant pain, MDD,
dysthymia and panic disorder (Madeira et al., 2011). Therefore, a complete assessment of
previous and actual history of psychiatric illness, together with detailed interpersonal
relationships, is vital to achieving appropriate treatment (Boyes et al., 2011). Very little
information about treatment of depression was found concerning cancer patients, which will
be discussed in detail further, in Chapter 3. This fact raised concerns about the lack of
information concerning the possibility of different responses to treatment of MDD in this
specific population. !!Depressive episodes may initially start with symptoms that meet criteria for adjustment
disorder (a maladaptive reaction to a stressful life event) and early intervention is essential for
a better prognosis (Akechi et al., 2004). This situation is complicated, because many
symptoms due to cancer or its treatment are also part of MDD criteria (for example, weight
loss, fatigue, psychomotor retardation and diminished ability to concentrate). Trying to solve
this problem, many researchers have assessed mood symptoms with the Hospital Anxiety and
Depression Scale (HADS), which is extensively used in palliative care, due to its absence of
physical symptoms on its assessment. HADS is a validated and reliable tool for medically ill
patients’ assessments for anxiety and depression (Guidi et al., 2011; Castelli et al., 2011).
Also, The Demoralization Scale may be a useful instrument, offering an evaluation of non-
specific dysphoria, social disconnectedness, hopelessness, helplessness and suicidal ideation
(Kissane et al., 2004).
! **!
The impact that MDD has on these patients may result in choices that might be different if
they were not affected by the disorder. For example, a study with cancer patients showed that
acceptance of adjuvant chemotherapy in patients with breast cancer and depression was
51.3%, but among patients without MDD, 92.2% accepted the abovementioned treatment
(Colleoni et al., 2000). With this knowledge, there are more chances of considering a possible
diagnosis of depression in this population. . This awareness could also lead patients to MDD
treatment, and probably to acceptance of cancer treatments, increasing their chances of
survival or recovery.!
Considering the high prevalence of depression in this population, studies evaluating
antidepressant treatments are of great importance for the clinical practice. Unfortunately there
are only two randomized clinical trials on this topic (Costa et al., 1985; van Heeringen and
Zivkov, 1996). A number of other studies have been published, however these have combined
patients with subsyndromal depression and MDD, usually neglecting illness severity. For
patients with terminal cancer, there is an even greater lack of studies, directing attention to the
fact that more could be done for this particular group. There are many studies considering
subjects support via telephone and via internet (White et al., 2011; Klemm and Hardie, 2002),
but usually these trials are for cancer survivors and no similar study was found for advanced
cancer patients.
! *,!
CHAPTER 2
Pathophysiology and treatment of Major
Depressive Disorder

! *-!
2.1 Pathophysiology of Major Depressive Disorder
Depression has been recognized since ancient times but is still considered a complex disease
with unknown etiology (Dagyt! et al., 2010). For many years the monoaminergic system was
the focus for depression treatment. However, with available antidepressants (which target
monoamines), patients’ response is very limited. This fact led researchers to consider the
possibility that other alterations in depressed subjects’ brains might be involved in the
pathophysiology of MDD. In the last decades, hippocampal neurogenesis started to be
investigated in depression’s pathophysiology (Dagyt! et al., 2011), and many hypotheses have
been studied as an attempt to better understand it.
The hypotheses described below are interconnected, indicating that depression is a highly
complex illness. For example, the locus coeruleus, which is considered a part of the central
stress system, has noradrenergic innervation, and is usually overexcited and may be defective
in patients with MDD. (Itoi and Sugimito, 2010; Harro and Oreland, 2001). When the locus
coeruleus is activated, it fires the prefrontal cortex (PFC), and triggers the ventral tegmental
area (VTA), releasing dopamine in the nucleus accumbens (NA). The PFC relays to the VTA,
releasing glutamate in the last, leading to increased excitability and more dopamine release in
the NA (Sara, 2009). This illustrates the interaction between different systems. Further,
cytokines (through influences on synaptic plasticity, and on neuroendorine and monoamine
systems) can influence corticotropin-releasing hormone (CRH), brain-derived neurotrophic
factor (BDNF), serotonin, norepinephrine, and dopamine (Miller and Raison, 2008). Figure
2.1 illustrates these interactions. The following sections will discuss some of the hypotheses
that try to explain the neurobiology of depression.

! *.!
Figure 2.1: Anatomical connections and interactions between neuroendocrine system, BDNF,
monoamines, and cytokines in the brain.
Figure modified from: www.antisocial-disorder.com/page/9
VTA
NA
PFC
!!!!!!!! LC

! *&!
2.1.1 Serotonergic system
The monoamine hypothesis of depression, which proposed that decreased levels of serotonin,
noradrenaline and/or dopamine would induce depressive symptoms (Middlemiss et al., 2002),
was previously converged to the serotoninergic system as a possible main alteration in the
brain, leading to depression (Coppen, 1967). Also, serotonin’s precursor tryptophan, proved
to be decreased in subjects with MDD (Anderson et al., 1990). Treatment with tryptophan had
a positive effect on mood when administered to depressed patients (Young et al., 1985;
Shopsin, 1978), suggesting a role for serotonin in depressive symptoms. Also, an immune-
response with consequent depletion of tryptophan has been associated with depression in
cancer patients (Kurz et al., 2011). Another fact that contributes to the association between the
serotonergic system and depression is the fact that many patients with MDD present chronic
pain symptoms. Regarding this fact, as the serotonergic 5-HT1A receptor seems to play a role
in Major Depression and in pain regulation (Ohayon, 2009), serotonin could provide a link
between these symptoms, and explain their frequent coexistence.
2.1.2 Noradrenergic system
This system is considered to be related to several areas that are altered in subjects with MDD,
such as attention, memory, learning, sleep, emotion and response to stress (Sara, 2009;
Berridge and Waterhouse, 2003). It is also implicated in synaptic plasticity in the
hippocampus (Sara, 2009), possibly playing a role in MDD. Its dysfunction has constantly
been pointed as a possible mechanism in depressive symptoms (Goekoop et al., 2011; Itoi and
Sugimoto, 2010). Some antidepressants with action in the noradrenergic system have been
cited as possibly more effective treatments when compared to selective serotonin-reuptake
inhibitors (SSRIs) however, this is still controversial. Besides these medications also act in
the dopaminergic system, some authors correlate their noradrenergic action to a possible
pathway to the treatment of Major Depression (Montgomery and Briley, 2011; Nutt et al.,
2007).
The noradrenergic system is linked to the activation of the hypothalamic-pituitary-adrenal
(HPA) axis, and vasopressin release, which are also implicated in the pathophysiology of
depression (Keller et al., 2006; Goekoop et al., 2011).

! *'!
2.1.3 Dopaminergic system
The role of dopamine in Major Depression seems to be highly linked to attention,
psychomotor activity, and anhedonia (which is the inability of experiencing pleasure in
activities that before were enjoyable). Because many antidepressants do not directly act in the
dopaminergic system, this might contribute to the residual symptoms that many patients
experience during their treatment. Residual symptoms frequently consist of impaired
concentration, motivation and pleasure (Dunlop and Nemeroff, 2007; Nutt, 2006). In the
cerebrospinal fluid of depressed subjects, homovanillic acid (HVA) seems to be decreased.
Some antidepressants are likely to act in the dopaminergic system, such as sertraline,
bupropion and the monoamine oxidase inhibitors (MAOIs), but the magnitude of this action
still requires further studies (Boadie et al., 2007).
2.1.4 HPA axis
The hyperactivity of the hypothalamic- pituitary-adrenal (HPA) axis is the main stress system
in the human body, and is responsible for stress response adaptation. It is related not only to
hormones and peptides, but also to neurotransmitters, such as noradrenaline, dopamine and
serotonin (Joëls and Baram, 2009). The hyperactivity of the HPA axis, which is illustrated in
figure 2.2, induces an exacerbated release of corticotropin-releasing factor (CRF), thus
secreting more ACTH and leading to hypercortisolemia (Keller et al., 2006). Also, HPA axis’
activation is considered to be involved in stress-induced neuronal atrophy. Two types of
neuronal plasticity are impacted by chronic stress, with atrophy of dentrites in the CA3 region
and repressed neurogenesis of granule cells in the dentate gyrus, in which not only
glucocorticoids but also NMDA receptors play a role (McEwen, 1999). Thus, chronic
psychosocial stress may lead to inhibition of neurogenesis and even neuronal loss (McEwen
and Mangarinos, 2001), which may contribute to cognitive impairment in MDD.
! *(!
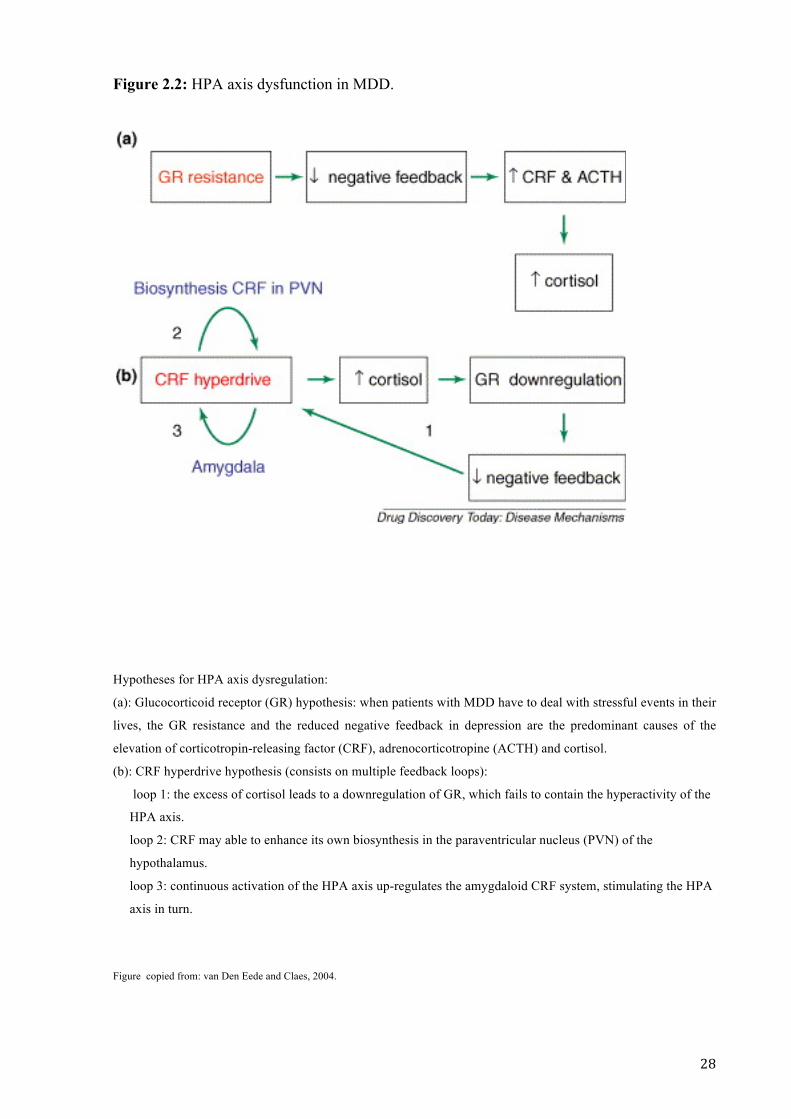
Figure 2.2: HPA axis dysfunction in MDD.
Hypotheses for HPA axis dysregulation:
(a): Glucocorticoid receptor (GR) hypothesis: when patients with MDD have to deal with stressful events in their
lives, the GR resistance and the reduced negative feedback in depression are the predominant causes of the
elevation of corticotropin-releasing factor (CRF), adrenocorticotropine (ACTH) and cortisol.
(b): CRF hyperdrive hypothesis (consists on multiple feedback loops):
loop 1: the excess of cortisol leads to a downregulation of GR, which fails to contain the hyperactivity of the
HPA axis.
loop 2: CRF may able to enhance its own biosynthesis in the paraventricular nucleus (PVN) of the
hypothalamus.
loop 3: continuous activation of the HPA axis up-regulates the amygdaloid CRF system, stimulating the HPA
axis in turn.
Figure copied from: van Den Eede and Claes, 2004.

! *)!
2.1.5 Gabaergic system
Gamma-Aminobutyric acid (GABA) is the most common inhibitory neurotransmitter in the
human brain, and glutamate is involved in GABA’s synthesis. This system is involved in
mood disorders, and increased GABAergic tone may lead to antidepressant effects (Brambilla
et al., 2003). In the cerebrospinal fluid, and in the plasma, depressed patients have lower
levels of GABA (Petty et al., 1992; Berrettini et al., 1983). However, some studies found that,
even after antidepressant treatment, plasma levels of GABA remain low. Another finding was
that level alterations were not associated with depression severity (Petty et al., 1992, 1993).
Different studies suggest that lower GABAergic functioning may be involved in the
pathophysiology of depression (Holland et al., 2010; Zink et al., 2009). With all positive
evidence, the focus on GABAergic system has also contributed to research for new
antidepressant treatments (Mohler, 2012).
2.1.6 Glutamatergic system
Glutamate is the most abundant excitatory neurotransmitter found in the brain, acting in the
“tripartite glutamatergic synapse” (Figure 2.3), involving different glutamate receptors and
other targets with therapeutic potentials (Popoli et al., 2011; Zarate et al. 2010). A number of
studies have used Magnetic Resonance Spectroscopy (MRS) as an attempt to assess activity
of the glutamatergic system in specific regions in the brain (Sanacora et al., 2004; Hasler et
al., 2007; Zarate et al., 2010). These studies have reported that these measures vary
considerably by brain region, type of mood disorder, course, progression and phase of illness
(Sanacora et al., 2012). Glutamate receptors are classified as metabotropic and ionotropic, the
last one includes N-methyl-D-aspartate (NMDA), which is the receptor linked to ketamine
action as a fast acting antidepressant (Paul and Skolnick, 2003).!!!!!!!!!!
! ,+!
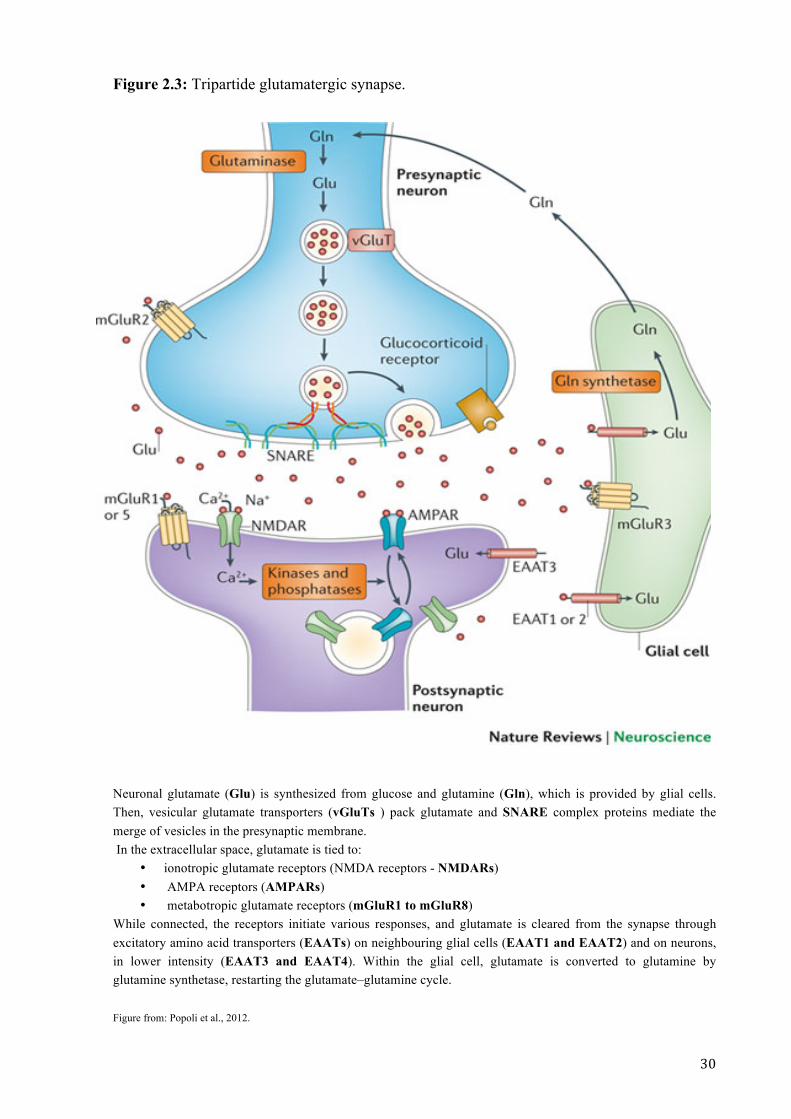
Figure 2.3: Tripartide glutamatergic synapse.!!!
! Neuronal glutamate (Glu) is synthesized from glucose and glutamine (Gln), which is provided by glial cells. Then, vesicular glutamate transporters (vGluTs ) pack glutamate and SNARE complex proteins mediate the merge of vesicles in the presynaptic membrane. In the extracellular space, glutamate is tied to:
• ionotropic glutamate receptors (NMDA receptors - NMDARs) • AMPA receptors (AMPARs) • metabotropic glutamate receptors (mGluR1 to mGluR8)
While connected, the receptors initiate various responses, and glutamate is cleared from the synapse through excitatory amino acid transporters (EAATs) on neighbouring glial cells (EAAT1 and EAAT2) and on neurons, in lower intensity (EAAT3 and EAAT4). Within the glial cell, glutamate is converted to glutamine by glutamine synthetase, restarting the glutamate–glutamine cycle. Figure from: Popoli et al., 2012.

! ,%!
2.1.7 Cytokines
Cytokines are signalling molecules produced by immune cells and are involved in regulating
immune responses. Currently, these molecules have been frequently associated with
depression and have been possibly linked to anorexia, found in several depressed patients
(Schiepers et al., 2005; Anderson, 1996). The communication between the central nervous
system and the immune system has lead to a research focus on cytokines’ relationship with
MDD. Also, several illnesses that present chronic inflammatory response are frequently
known to coexist with MDD. Further, it is well established that there is an association
between depressive symptoms and the use of pro-inflammatory cytokines, which are
frequently used for the treatment of cancer (Yirmiya at al., 1999; O’Connor et al., 2007).
Several factors are related to the role of inflammation in the pathophysiology in depression
(Leonard and Maes, 2012), as demonstrated in Figure 2.4.
Figure 2.4: From inflammation to depressive symptoms.
Peripheral cell-mediated immune activation leads to increased interferon (IFN), interleukin-1 (IL-1), interleukin-2 (IL-2), interleukin-6 (IL) and tumor necrosis factor (TNF). With indoleamine (IDO) activation , a depletion of l-tryptophan occurs, leading to depressive symptoms. Also, the production of tryptophan catabolites (TRYCATs) induces depression.. At the same time, there is the iduction of upregulation of the 5-HT transporter (SERT), diminishing synaptic dopamine (5-HT), which also induces depressive symptoms. !Figure from: Leonard and Maes, 2012.!
!

! ,*!
2.2 Current treatments for depressive episodes
This topic briefly covers the main available treatments for MDD, including some options for
treatment resistant depression.
2.2.1 Psychotherapy
It is widely accepted that psychotherapy is a very important tool in the treatment of several
psychiatric disorders. The most studied are interpersonal, psychodynamic, cognitive and
behavior therapy (Markowitz and Weissman, 2012; Feng et al., 2012; Abbass and Driessen,
2010). Differences found in responses to psychotherapeutic treatments are minor, and overall
these approaches appear to be as effective as antidepressant medications for mild and
moderate depressive episodes (Cuijpers et al., 2011; Härter et al., 2010).
Psychotherapy should be recommended for acute treatment of depression, together with
antidepressant pharmacotherapy, as it may lead to improvement in patients’ quality of life. In
treatment resistant depression results are more varied, nevertheless psychotherapy (cognitive,
interpersonal and behavioral) should be indicated for these individuals (Ishak et al., 2011;
Jakobsen, 2011; Trivedi et al., 2011).
This treatment together with pharmacotherapy usually takes a few weeks to result in
significant response (van Calker et al., 2009). Although psychotherapy is very important for
patients with cancer (Savard et al., 2006), individuals with end-stage cancer may not fully
benefit from this treatment, as their life expectancy is very short.
2.2.2 Pharmacotherapy
Antidepressants are the main treatment for moderate and severe MDD. The selective
serotonin reuptake inhibitors (SSRIs), due to their favorable safety and efficacy profiles, are
usually the first line antidepressants to be indicated for depressive episodes. Also, although
there are several SSRIs, minimal differences can be found amongst them (Souery et al., 2011;
Boulenger et al., 2010). According to some authors, serotonin-norepinephrine reuptake
inhibitors (SNRIs) are broadly similar to SSRIs in terms of efficacy and safety. Their rates of
response and remission are similar, (Weilburg, 2004; Kornstein et al., 2009). Older agents,
such as tricyclic antidepressants and monoamine oxidase inhibitors, despite being effective,
present more side effects. Even, monoamine oxidase inhibitors (MAOIs) present high
! ,,!
toxicity, and these agents, together with tricyclic antidepressants, have higher incidence of
withdrawal when compared to SSRI (Chouinard et al., 1994; Amsterdam and Shults, 2005).
Table 2.1: Main mechanisms of action of antidepressants.
MONOAMINE REUPTAKE INHIBITORS
Serotonin selective SSRIs, Clomipramine
Norepinephrine selective Reboxetine, Maprotiline, Desipramine
Dopamine selective Bupropion
Mixed reuptake inhibitors Venlafaxine, Imipramine, other tryciclics
RECEPTOR ANTAGONISTS
Mianserin, Mirtazapine (5HT2A, 5HT2C, alpha-2)
ENZYME INHIBITORS
Irreversible MAOIs Phenelzine, Tranylcypromine
Reversible MAOIs Moclobemide
2.2.3 Electroconvulsive therapy (ECT)
ECT is a validated treatment for several psychiatric disorders, and consists of
neurostimulation by the induction of a grand mal seizure. ECT’s effects seem to rely in
changes in the monoaminergic system and in the stress response system. It was first described
in 1930’s and over time its efficacy and safety have been extensively studied. ECT’s efficacy
is equally consistent for unipolar and for bipolar depressive episodes. (Trevino et al., 2010;
Nikisch and Mathé, 2008; Coentre et al., 2009; Bailine et al., 2010). It is usually administered
from 1 to 3 times a week, and a meta-analysis with 73 randomized clinical trials showed that
there is no difference in efficacy between these time-points (UK ECT Review group, 2003).
Although cognitive impairment is more significant for bilateral and high dose ECT, when
compared to unilateral and brief pulse, it is also more effective than lower dose treatment.
Also, for continuation electroconvulsive therapy, time between session is increased, which
reduces the chances of cognitive side effects (Lisanby et al., 2000; UK ECT Review group,
2003; Trevino et al, 2010).
! ,-!
2.2.4 Repetitive transcranial magnetic stimulation
Transcranial magnetic stimulation (TMS) was first described in 1985, and consists in an
intense and brief electromagnetic field. It is a noninvasive procedure that is easily tolerated.
(Dell'osso et al., 2011; Gershon et al., 2003).
Repetitive TMS is the most used modality of TMS in psychiatry, providing more prolonged
results than the single-pulse modality. Also, as ECT, it acts on neuroendocrine and
neurotransmitters systems (Baeken and De Raedt, 2011). Treatments are made in a daily basis
for 5 days/week, usually for about 2 to 9 weeks. (Dell'osso et al., 2011; Fitzgerald and
Daskalakis, 2011). Side effects are less significant than those found in ECT, such as memory
impairment, which is usually not present in subjects who received repetitive TMS, except for
those who presented a seizure during treatment, which is not a common side effect
(Wassermann, 2000; Loo et al., 2008).
Comparatively, although repetitive TMS has fewer side effects than ECT, the latter has higher
rates of remission. This fact emphasizes the utility of ECT for treatment resistant patients
(Minichino et al., 2012).
2.2.5 Vagus nerve stimulation (VNS)
VNS was originally developed as a treatment for patients with epilepsy that did not respond to
pharmacological treatment. Recent data has implicated it as a possible treatment for
individuals with depression, although these studies are not controlled. Also, there is the
possibility that it plays a role in serotoninergic and noradrenergic systems as a mechanism for
antidepressant response (Martin and Martín-Sánchez, 2011; Dorr and Debonnel, 2006). A
recent meta-analysis showed that, although several studies demonstrate that VNS may be used
as a possible treatment for depression, its efficacy is still questionable and it may actually
represent a placebo effect (Martin and Martín-Sánchez, 2011). However, a positive aspect of
VNS is the lack of cognitive side effects, specially when compared to ECT. As positive mood
effects were related to subjects who did not have a high degree of resistance to previous
treatments, the use of VNS requires careful consideration (Sackelm et al., 2001).
! ,.!
2.2.6 Deep brain stimulation (DBS)
DBS is an invasive procedure, which involves the insertion of stimulating electrodes in the
brain. Its use is still experimental for depression, although its use for Parkinson’s disease and
refractory obsessive compulsive disorder is approved by the FDA. It consists of a 2 phase
procedure, with the first one performed under local anesthesia and with the patient awake, as
the effects od stimulation must be evaluated. In the second phase, the inserction of a pulse
generator in the subcutaneus fat, under the patient’s subclavian region, is made under general
anesthesia. Then it is connected to cables under the skin, that are connected to the electrodes
in the brain (Bell et al., 2009; Malone, 2010; Blomstedt et al., 2010). Studies show positive
outcomes for patients with treatment resistant depression, however its action in the brain is
not completely clear (Hamani and Nobrega, 2010). In 2005, Mayberg et al. used DBS for
patients with treatment-resistant depression, achieving a sudden and sustained improvement
in mood, in 66% of these patients. The change in mood seems to be related to a fast
deactivation of Broadmann area 25, which is hyperactive in MDD (Mayberg et al., 2005;
1999). However, there are various risks involving this procedure, such as stroke, infection,
paresthesia, and anxiety (Holtzheimer and Mayberg, 2010; Malone, 2010; Blomstedt et al.,
2010). Thus, severity of refractory depression should be carefully evaluated before
considering this treatment.

! ,&!
CHAPTER 3
Review and meta-analysis of available
treatments for depression in cancer patients
! ,'!
3.1 Introduction
As stated in chapter one of this thesis, Major Depressive Disorder (MDD) has a high 12-
month prevalence in general population, and higher rates are seen in patients with advanced
cancer (Scott et al., 2010; Kessler et al., 2005). In addition, depression is the main mental
health complication of cancer (Mitchell et al., 2011).
In patients with cancer, those with past history of Major Depression have a higher probability
of developing depressive episodes after a diagnosis of cancer. As this finding implicates the
possibility of early diagnosis and intervention, depression should be considered a special topic
in psycho-oncology and not be misdiagnosed (Mitchell 2011; Mitchell et al., 2011). More
over, this specific population appears to have a lower level of acceptance of adjuvant
chemotherapy (Colleoni et al., 2000), and in those who will commence chemotherapy,
prevalence rates of MDD may be as high as 25% (Breen et al., 2009). For patients with
cancer, depression can be not only a burden, but also a risk, when considering their
psychological symptoms may affect decisions for accepting treatment options.
Proper attention and treatment should be given to these individuals, as antidepressant drugs
are effective in palliative care settings. However, these medications seem to be
underprescribed for older patients and for those with physical illnesses, despite having MDD
(Rayner et al., 2011). The objective of this chapter is to investigate the safety and
effectiveness of currently available antidepressant treatments in cancer patients.
3.2 Methods
3.2.1 Search strategy
Electronic databases used were: ClinicalTrials.gov, PsychInfo and Pubmed. In all three
databases, search was made with the keywords “treatment” [AND] “depression” [AND]
“cancer”. In Pubmed, the limit “Randomized Controlled Trial” was applied. Articles from
1971 until January 2012 and in English, Portuguese, Spanish and Italian were reviewed. Also,
citations from screened articles were verified.
3.2.2 Selection criteria
For inclusion in the review, studies had to meet the following criteria:
• double-blind Randomized Controlled Trial (RCT),
! ,(!
• placebo controlled,
• presence of at least 20 subjects in each arm,
• patients fulfilling DSM (Diagnostic and Statistical Manual of Mental Disorders) or
ICD (International Classification of Disease) criteria for depressive episode,
• patients with cancer,
• absence of initial antidepressant treatment (or change in current antidepressant
treatment) at the same time of intervention,
• psychopharmacologic or psychotherapeutic treatment for depression.
Any type of psychotherapy was considered in this search.
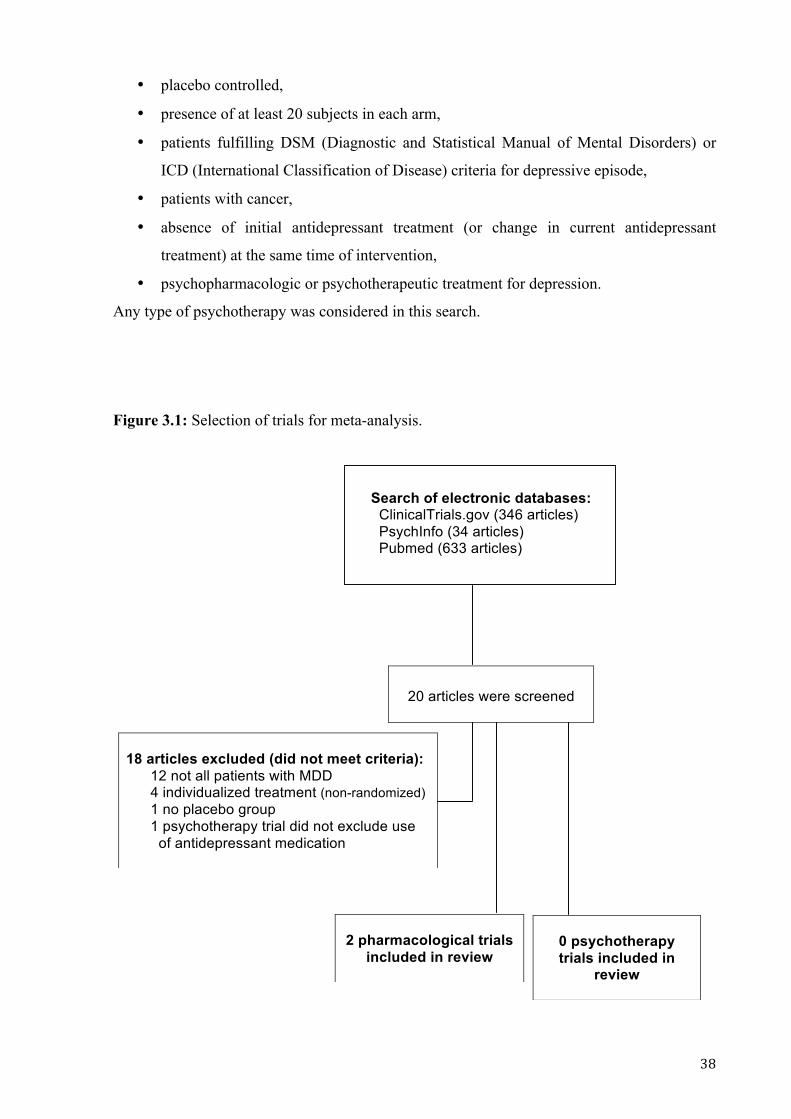
Figure 3.1: Selection of trials for meta-analysis.
!!
20 articles were screened
18 articles excluded (did not meet criteria): 12 not all patients with MDD 4 individualized treatment (non-randomized) 1 no placebo group 1 psychotherapy trial did not exclude use of antidepressant medication
2 pharmacological trials
included in review
0 psychotherapy trials included in
review
Search of electronic databases: ClinicalTrials.gov (346 articles) PsychInfo (34 articles) Pubmed (633 articles) !

! ,)!
3.2.3 Analysis
The selected trials for meta-analysis were analyzed with RevMan 5.1 (Cochrane
Collaboration, 2008). Data for the outcomes for treatment versus placebo were statistically
examined as continuous data, with random effects model, and standardized mean difference
for effect measure. The I2 statistic was used to assess heterogeneity of studies.
3.3 Results
After a systematic search 20 articles were selected for review, of which only 2 met criteria for
meta-analysis (Costa et al., 1985; van Heeringen and Zivkov, 1996). Both trials investigated
the use of pharmacotherapy for depression in cancer patients, and no psychotherapy trial met
criteria for meta-analysis. Among the screened studies, several did not meet criteria for MDD,
although these quoted “depression”, instead of “depressive symptoms” or “adjustment
disorder” in some cases (Bruera et al., 1986; Holland et al., 1998; Roscoe et al., 2005; Savard
et al., 2006; Bar-Sela et al., 2007). In other trials, patients were offered individualized
treatments, thus not appropriate for comparison with other therapies (Ell et al., 2011; Ell et al.,
2008; Strong et al., 2008; Dwight-Johnson et al., 2005). One study compared fluoxetine and
amitriptyline for cancer patients, although it met criteria for MDD according to ICD-10 it was
not included in meta-analysis because of its lack of placebo group (Pezzella et al., 2001). A
psychotherapy trial was excluded because it was not clear if patients could use antidepressant
medications or not (Evans and Connis, 1995).
3.3.1 Meta-analysis
Both of the selected articles compared mianserin (a tetracyclic antidepressant) to placebo,
both evaluated its response in female patients (van Heeringen and Zivkov, 1996; Costa et al.,
1985). Costa et al., 1985 included subjects with general gynecological cancer, and the second
study assessed patients with breast cancer. Another difference between studied populations
was the cancer’s severity, with Costa et al., 1985 including more severely ill patients (several
of them with terminal cancer).
While Costa et al., 1985 showed positive results within 7 days after the initiation of the use of
mianserin, van Heeringen and Zivkov, 1996 reported positive outcome starting on day 14
post-treatment. In the first week patients received 30 mg/day of mianserin, in the following
weeks the dose was increased to 60 mg/day. Mianserin was given to patients three times a day

! -+!
in the trial from Costa et al., 1985 and once a day in van Heeringen and Zivkov, 1996. In
these trials, there were no significant differences in side effects when comparing intervention
and control group. Also, higher rates of premature terminations were observed in controls,
and these were linked to lack of efficacy. Mianserin 60 mg/day was safe when used together
with chemotherapy and with radiotherapy in both trials. The low I2 value (0%) suggests lack
of heterogeneity in these two sets of clinical trial data. The forest plot of these two studies is
shown in figure 3.2, and indicates a moderate statistically significant effect size (SMD= -
0.68), p= 0.0002.
Figure 3.2: Meta-analysis of antidepressant trials in patients with MDD and cancer (HAMD).
3.4 Discussion
Although there are many studies considering depressive symptoms and their treatment in
cancer patients, most of these did not include patients with Major Depression. These studies
frequently included patients with mild symptomatology and/or adjustment disorder (Bruera et
al., 1986; Holland et al., 1998; Roscoe et al., 2005; Savard et al., 2006; Bar-Sela et al., 2007),
making it impossible to analyse treatment response for MDD in this population. After
applying selection criteria, only two studies were suitable for analysis (van Heeringen and
Zivkov, 1996; Costa et al., 1985). This shows a deficit of appropriate research in this area,
which was an unexpected result. Other reviews that presented similar objectives to this
chapter were then assessed, and the included trials in these studies did not meet criteria for
Major Depression (Akechi et al., 2008; Williams and Dale, 2006). All the studies that were
excluded because of individualized treatment addressed patients with MDD, usually with mild
depression. In these trials, treatments included psycho-education, psychotherapy, and the use
of antidepressants (Ell et al., 2011; Ell et al., 2008; Strong et al., 2008; Dwight-Johnson et al.,
2005). Also, the type of treatment offered to the patient varied according to symptomatology,
patient’s choice and level of social support. As provided treatments were different for each

! -%!
individual, it was not possible to make an analysis comparing the results from these studies
with the data available from other research.
The time of onset of MDD plays an important role in the treatment of depression, and chronic
illness and lack of response to previous treatments may occur, resulting in individuals with
more severe symptomatology and lower response to treatment (Rush et al., 2006). In the
selected studies for meta-analysis, Costa et al. analysed subjects with Major Depression
succeeding or paralleling cancer diagnosis, while van Heeringen and Zivkov, 1996 did not
consider the time of onset of depression. Thus, the second trial may have included patients
with chronic or potentially treatment resistant depression as exclusion criteria were not
described. Nevertheless, the statistical analysis shows no heterogeneity in the outcomes of the
compared studies. Both used Hamilton Depression Rating Scale (HAMD), but the numbers of
items used was different in each trial, with 17 items in Costa et al., 1985, and 21 in van
Heeringen and Zivkov, 1996. To manage this, standardized mean differences were used as the
effect measure.
Mianserin was significantly more effective than placebo in both studies, and adverse events
were similar to control group, despite use of cytotoxic drugs. These findings support the use
of mianserin in depressed patients with cancer, even for those who are receiving aggressive
treatment for malignant neoplastic disease. The fact that Costa et al., 1985 prescribed the
medication 3 times a day may reduce patient’s adherence when they are outpatients (Santiago-
Rodriguez et al., 2002). Thus, van Heeringen and Zivkov, 1996 presented a better plan of
administration, with once-a-day dosing, as mianserin’s half-life is 21 to 61 hours and justifies
this posology (Tolvon®-Medsafe). Besides the fact that Costa et al., 1985 reported
statistically significant improvement in the intervention group after 7 days, when evaluating
response of treatment as a reduction in 50% from baseline scores, both trials present response
to mianserin in day 14 after treatment initiation. Neither of the studies presented remission
(HAMD 21 and 17 " 7) of symptoms during treatment (Rudolph and Feiger, 2000;
Zimmerman et al., 2004).
3.5 Conclusions
Depression is a disorder that is common amongst patients with terminal cancer, however there
are only two treatment trials in this population. Mianserin seems to be a safe option for this

! -*!
group, however its efficacy for remission of depressive symptoms is still not clear.
Considerable additional research in this population is required.

! -,!
CHAPTER 4
Ketamine overview
! --!
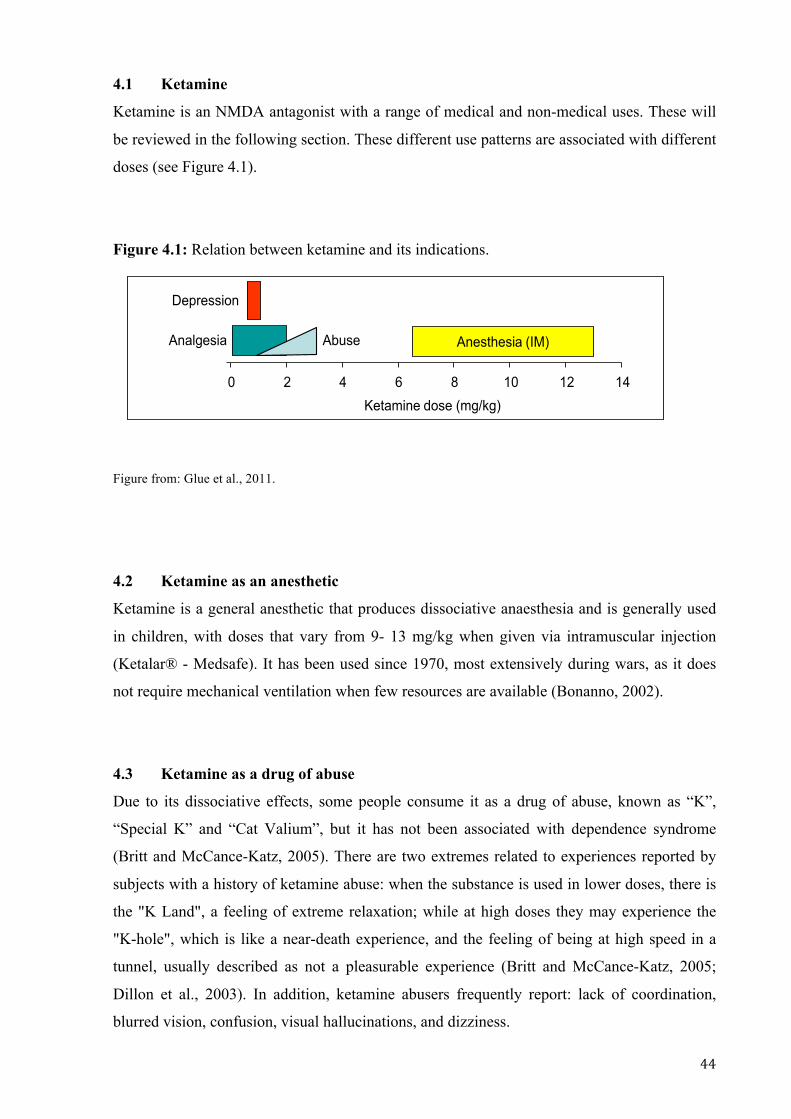
4.1 Ketamine
Ketamine is an NMDA antagonist with a range of medical and non-medical uses. These will
be reviewed in the following section. These different use patterns are associated with different
doses (see Figure 4.1).
Figure 4.1: Relation between ketamine and its indications.
Figure from: Glue et al., 2011.
4.2 Ketamine as an anesthetic
Ketamine is a general anesthetic that produces dissociative anaesthesia and is generally used
in children, with doses that vary from 9- 13 mg/kg when given via intramuscular injection
(Ketalar® - Medsafe). It has been used since 1970, most extensively during wars, as it does
not require mechanical ventilation when few resources are available (Bonanno, 2002).
4.3 Ketamine as a drug of abuse
Due to its dissociative effects, some people consume it as a drug of abuse, known as “K”,
“Special K” and “Cat Valium”, but it has not been associated with dependence syndrome
(Britt and McCance-Katz, 2005). There are two extremes related to experiences reported by
subjects with a history of ketamine abuse: when the substance is used in lower doses, there is
the "K Land", a feeling of extreme relaxation; while at high doses they may experience the
"K-hole", which is like a near-death experience, and the feeling of being at high speed in a
tunnel, usually described as not a pleasurable experience (Britt and McCance-Katz, 2005;
Dillon et al., 2003). In addition, ketamine abusers frequently report: lack of coordination,
blurred vision, confusion, visual hallucinations, and dizziness.!
CORRESPONDENCE
Dose- and Exposure-Response to Ketamine inDepression
To the Editor:
W e read with interest the recent report on the repeated-dose use of ketamine as a rapidly acting antidepressant inpatients with treatment-resistant depression (1). Despite
the promising antidepressant responses to this intervention in thisand other studies (2– 4), several important technical questionsabout administration of ketamine have not yet been explored (5).These include route of administration, dose– exposure relationship,and exposure– and dose–response information. In this letter, wepresent a simulation on projected exposures between intramuscu-lar and intravenous (IV) ketamine to establish comparable dosesand report preliminary dose–response data in patients with treat-ment-refractory bipolar II depression.
Route of Administration and Dose–Exposure Rela-tionship. Most published reports on ketamine used as an anti-depressant are at a dose of .5 mg/kg, given as a slow IV infusion over40 min. This regimen is described as being based on pilot studies inhealthy volunteers (6). An intramuscular (IM) route of administra-tion has the advantage of not requiring an IV infusion pump andfacilitates dosing in patients with poor venous access.
We developed a model for IM and IV pharmacokinetic profilesbased on published reports for racemic ketamine (7,8). The IV pa-rameter values are as reported in Ihmsen et al. (8), and relativebioavailability of IM ketamine to IV was 93% (7). Our model de-scribed similar overall exposures over time based on comparable IMand IV dosing (2-hour area under the concentration-time curvevalues ! 20.9 and 21.7 mg.min/L, respectively); however, peakexposures were higher after IM dosing (Figure 1A). Higher IM or IVketamine doses would be expected to demonstrate dose-propor-tional pharmacokinetics (8). We propose that IM ketamine may bean acceptable alternative route of administration for ketamine inpatients with refractory depression.
Exposure–Response Relationship. There is some sug-gestion that mood response may be related to the early ketamineexposure profile, given the substantial early improvement in de-pression ratings by 40 min after the start of the IV infusion (1– 4).
Therefore, we hypothesize that early exposure is critical to thetherapeutic effect of ketamine, and in this context, the higher peakvalues after IM ketamine may be beneficial (Figure 1A).
Dose–Response Relationship. We have preliminary dose–response data in two female patients with refractory depression,treated with open-label ascending doses of IM ketamine as part ofclinical care. An initial dose of .5 mg/kg produced minimal (10%–20%) reductions in Montgomery–Asberg Depression Rating Scale(MADRS) scores. Higher doses (.7 and 1.0 mg/kg IM) produced pro-portionally greater reductions in MADRS scores, in one case provid-ing scores consistent with remission (" 7; Figure 1B; data are forMADRS ratings 24 hours postinjection). All doses were safe. Re-ported side effects (principally light-headedness, sedation, disso-ciative symptoms) were qualitatively similar to those reported afterIV administration (1– 4). With ascending doses, there was no differ-ence in the time of onset or duration of symptoms; however, sub-jective assessments of symptom intensity indicated greater inten-sity with higher ketamine doses. It is important to note that thedoses used for antidepressant effects are similar to those used foranalgesia (9) and are approximately one tenth of that for anesthesiavia IM administration (10) (Figure 1C). Doses reported in the drugabuse literature fall into an intermediate range (11).
On the basis of published clinical rating data and our simulation,it is clear that early exposure to ketamine is important in its thera-peutic effects, and this can be achieved even more rapidly with IMdosing. Future studies should concentrate on the early exposure–response profile and its relationship with symptom response.
Paul Gluea*Abhishek Gulatib
Martin Le Nedelecc
Stephen Duffullb
Departments of aPsychological Medicine, bPharmacy, and cPharmacology, Universityof Otago, PO Box 913, Dunedin, New Zealand.
*Corresponding author E-mail: [email protected].
None of the authors have any biomedical or financial interests or potential conflicts ofinterest.
Please also see associated correspondence, doi 10.1016/j.biopsych.2011.02.018.
conc
entra
tion
(mg/
L)
time (mins)0 20 40 60 80 100 120
0.0
0.2
0.4
0.6
0.8IV:IM:
Ketamine dose (mg/kg IM)Baseline 0.5 0.7 1.0
MA
DR
S s
core
0
10
20
30
40 Subject 1Subject 2
A
Ketamine dose (mg/kg)0 2 4 6 8 10 12 14
Anesthesia (IM)Analgesia Abuse
DepressionC
B
Figure 1. (A) Simulation of concentration-time profilesup to 120 min for ketamine .5 mg/kg, after intramuscular(IM; dotted line) or intravenous (IV; solid line) administra-tion. (B) Effects of ascending ketamine doses on Mont-gomery-Asberg Depression Rating Scale scores in twodepressed patients, 24 hours postinjection. (C) Ketaminedose–indication relationship.
BIOL PSYCHIATRY 2011;70:e9–e100006-3223/$36.00© 2011 Society of Biological Psychiatry
!

! -.!
Some studies were conduced to assess the effects of this medication when used repeatedly as
a “club drug” on a long-term basis. However, as concomitant use of other drugs and alcohol is
very common, the results of possible cognition impairment may be due to other substances
(Dillon et al., 2003). A finding that is consistent with prolonged ketamine use, is severe lower
urinary tract symptoms, with inflammation and hematuria, many times leading to a diagnosis
of ulcerative cystitis at biopsy, which shows slow response to treatment. Although it is not a
common complication (Mason et al., 2010; Mak et al., 2011), the use of pentosane polysulfate
(Shahani et al., 2007), seems to be the best option as a treatment for ulcerative cystitis,
together with ketamine cessation. Also, ketamine is often prescribed as an analgesic, and has
been studied as a fast acting antidepressant.
4.4 Ketamine as an analgesic
Low doses of ketamine are used for analgesia, commonly between 0.1 and 2 mg/kg. Its use as
an analgesic has been studied in children, patients with chronic pain, patients in Emergency
Departments, and in postoperative settings. (Laskowski et al., 2011; Dadu et al., 2011; Lester
et al., 2010; Deng et al., 2009; Kwok et al., 2004). The duration of analgesic effects closely
follows ketamine plasma concentrations. Thus, most studies have found a significant duration
in early (30 minutes to 4 hours) pain scores, but some authors have also demonstrated pain
relief in late (24 to 72 hours) pain scores (Noppers et al., 2011; Laskowski et al., 2011; Dadu
et al., 2011; Kwok et al., 2004).
A recent meta-analysis concluded that ketamine improves the quality of pain control, and
decreases opioid consumption (Laskowski et al., 2011).
4.5 Ketamine as a fast acting antidepressant
Ketamine, a noncompetitive antagonist of the glutamate receptor NMDA (N-methyl-D-
aspartate), has been suggested as a possible option for treatment resistant Major Depression
(Berman et al., 2000; Zarate et al., 2006; aan het Rot et al., 2010).!
The mechanism of ketamine’s action on mood is not completely clear, but a signaling cascade
leading to synaptogenesis has been studied (Duman et al., 2012). Phelps et al. (2009) have
suggested a better response in patients with familial history of alcohol dependence, because

! -&!
its pathophysiology is also linked to the glutamatergic system. The correlation between
depressive symptoms and pain has not been assessed during ketamine use for depression.
In addition to the rapid onset of antidepressant action, there is a sustained response as well,
for up to one week. This appears to be unrelated to presence of ketamine (half life ~ 3 hours)
or its weakly active metabolite norketamine (half life ~ 2 hours). Recent research suggests
this may be attributable to changes in secondary signaling, and not via receptor blockade.
Therefore, the activation of a protein kinase, mammalian target of rapamycin (mTOR), may
exert the sustained antidepressant effect by the formation of new synapses – synaptogenesis.
Also, mGlu2/3 receptors, seem to activate mTOR signalling, but do not seem to be involved
in ketamine’s acute antidepressant response (Koike et al., 2011).
/01! 21345631! 75! 8179:"61! 5;;<23! within hours or days, usually with maintenance of
response for up to seven days (Zarate et al., 2006; Liebrenz et al., 2009). The doses studied to
treat Major Depressive Disorder (MDD) are low, around 0.5mg/kg, and ketamine’s
administration is usually made with intravenous infusion over 40 to 60 minutes (Machado-
Vieira et al., 2009). Nevertheless, dosage and administration can vary, usually from 0.2mg/kg
to 1.5mg/kg, and administration can also be oral and intramuscular (Goforth and Holsinger,
2007; Irwin and Iglewicz, 2010; Paslakis et al., 2010; Messer et al., 2010; Larkin and
Beautrais, 2011; Glue et al., 2011). Main side effects found with this treatment are dizziness,
psychotomimetic and dissociative effects, which are transient and moderate, dissipating in 80
minutes post infusion (Zarate et al., 2006). !
4.6 The possible use of ketamine as a fast acting antidepressant for terminal cancer
patients
Considering terminal cancer patients are in their last days or months of life, an improvement
in quality of life would mean much, not only for those who are sick, but for their families,
who also suffer greatly. Even, the fact that many people with a diagnosis of cancer present
pain related to their illness, ketamine may be effective for both, depressive symptoms and
pain, as it is frequently used for pain relief in palliative care settings.
!
! -'!
CHAPTER 5
Review and meta-analysis of ketamine as a
fast acting antidepressant

! -(!
5.1 Introduction
Major Depressive Disorder (MDD) is a common disease, with a 12-month prevalence of 6.7%
and a lifetime prevalence of 16.2% (Kessler et al., 2005). A recent study showed that only
around 33% of patients with severe impairment due to MDD receive treatment in mental
health services, indicating that the majority of patients with MDD lack proper treatment and
follow up (Scott et al., 2010). Even more, in 2004, the World Health Organization (WHO)
determined Major Depressive Disorder (MDD) as the main global cause of years lost due to
disability. This data shows that there are major, social and economic, impacts related to MDD
worldwide.
The classical understanding of MDD neurobiology focused on the monoamines, such as
serotonin, norepinephrine and dopamine, and most antidepressants are characterized by
interactions with these systems in the brain. More recently, new treatments for depression that
interact with non-monoamine systems have been studied (Hashimoto, 2009). The
glutamatergic system has been linked to MDD’s pathophysiology in many studies (Hasler et
al., 2007; Hashimoto, 2009; Zarate et al., 2010; Sanacora et al., 2012). This might explain the
lack of remission of depressive symptoms, which occurs in two-third of patients, with
medications that target only monoamine systems (Trivedi et al., 2006).
Ketamine, a noncompetitive antagonist of the glutamate receptor NMDA, is approved in New
Zealand as a general anesthetic (Ketalar® - Medsafe). After been used in Vietnam War, its
use was very extensive in the 1970’s, with the advantage of rarely causing respiratory
depression (Bonanno, 2002). Its applicability is also prominent for analgesia, being widely
used in clinical practice (Sih et al., 2011), however it is not approved in New Zealand for this
indication.
Ketamine was first studied as a possible antidepressant medication in 1975, when it was
compared to imipramine and placebo in rats, and showed positive results with doses of 40 and
80 mg/kg. In this study, ketamine was less effective than imipramine, however it was
significantly more effective than placebo (Sofia and Harakal, 1975). Importantly, this research
presented ketamine as possible treatment for depression. In 2000 the first clinical trial
evaluating ketamine as an antidepressant agent identified a rapid and sustained response, with
depression scores being reduced up to 3 days after a single IV infusion (Berman et al., 2000).
Since then, several studies have addressed the same objective, usually with similar outcomes
(Zarate et al., 2006; aan het Rot et al., 2010).

! -)!
In this review and meta-analysis, changes in depression ratings after dosing, from case reports
and randomized clinical trials, will be analyzed separately. The purpose of this analysis is to
determine the effectiveness, speed of onset, and duration of response, after a single infusion
of ketamine in patients with MDD.
5.2 Methods
5.2.1 Search strategy
Search was made in Pubmed, PsychInfo, Embase and ClinicalTrials.gov with the use of the
keywords “Ketamine” AND “depression”, “bipolar disorder”, OR “mood disorder”. No limits
were added, but only articles in English, Portuguese, Spanish and Italian were reviewed. The
search was made from any 1957 until present (November 2011). Also, citations in screened
articles were checked.
5.2.2 Selection criteria
Studies were required to meet the following criteria:
• patients with a diagnosis of MDD or bipolar disorder (BD) in a depressive episode
according to DSM criteria (DSM III, III-R, or IV, American Psychiatric Association,
1980, 1987, 2000),
• presenting moderate or severe depressive symptoms,
• use of ketamine with IV infusion over 40 to 60 minutes,
• dosage of 0.5mg/kg for racemic ketamine, or 0.25 mg/kg for S-ketamine.
Antidepressant response had to be assessed with reliable validated scales, such as
Mongomery-Asberg Depression Rating Scale (MADRS), Hamilton Rating Scale for
Depression (HAMD), Beck Depression Inventory (BDI), Hospital Anxiety and Depression
Scale (HADS) and/or The Quick Inventory of Depressive Symptomatology (QIDS-SR16).
Studies were analyzed to reach a consensus on what variables could be accepted within the
studies. Thus, patients with no history of ketamine treatment, and patients who had prior
ketamine use (for any treatment) could be included in review and meta-analysis. Current
medication could be suspended or maintained. Four studies used ketamine as an induction
agent for patients with MDD who were treated with electroconvulsive therapy (ECT). These
were not included in the review, as the use of ECT was a complicating factor.

! .+!
Data were included from case series and placebo-controlled randomized clinical trials
(RCTs).
Figure 5.1: Selection of studies for review and meta-analysis for ketamine as a fast acting
antidepressant.
Search of electronic databases:
35- ClinicalTrials.gov (16 selected) 0- Embase 725- Pubmed (36 selected) 8- PsychInfo (0 selected)
!!!!!!!!!!
1 article identified by other
search instruments (not selected)
54 articles were screened
39 articles excluded: 12 did not meet criteria 23 without enough data 3 overlapping studies 1 duplicated
12 case reports/ case series
included in review
3 RCTs included in
meta-analysis

! .%!
5.2.3 Analyses
RCTs were analyzed using RevMan 5.1(Cochrane Collaboration, 2008). Placebo versus
treatment were compared as an intervention review, with continuous data, random effects as
the analysis model and mean difference as effect measure along with 95% confidence
intervals.
Case reports and case series were compared with results from one of the RCTs. The choice of
using Diazgranados et al. data for this comparison was due to this study reporting changes in
three different depression scales. In total, 12 case reports/series results were compared to the
abovementioned RCT. Most of them (7) utilized MADRS for depressive symptoms
assessment, with a minority using HAMD and BDI.
5.3 Results
Fifteen studies were selected for comparison and review. All were published, with the first
one published in 2000 (Berman et al., 2000). There were 3 RCTs that analyzed the outcome
for ketamine as a fast-acting antidepressant.
5.3.1 Randomized clinical trials
Zarate et al. presented a crossover study design with 18 patients, and Diazgranados et al. used
a very similar study design 4 years latter. The primary diagnosis was the main difference
between these studies, as the first included only patients with MDD and the second, patients
with bipolar depression (BD).
Demographic and clinical characteristics of RCTs are presented on Table 5.1, where time to
response and time to relapse are clearly different when comparing the two most recent trials,
although the percentage of response and remission are very similar, 71% and 30%,
respectively. Unfortunately, the Berman et al., 2000 did not provide enough data for this
comparison. A substantial difference while comparing Berman et al., 2000 with the
abovementioned studies is that one of the inclusion criteria was depressive episode, with no
distinction between a diagnosis of MDD or BD, which may lead to different outcomes for
these patients’ subgroups.
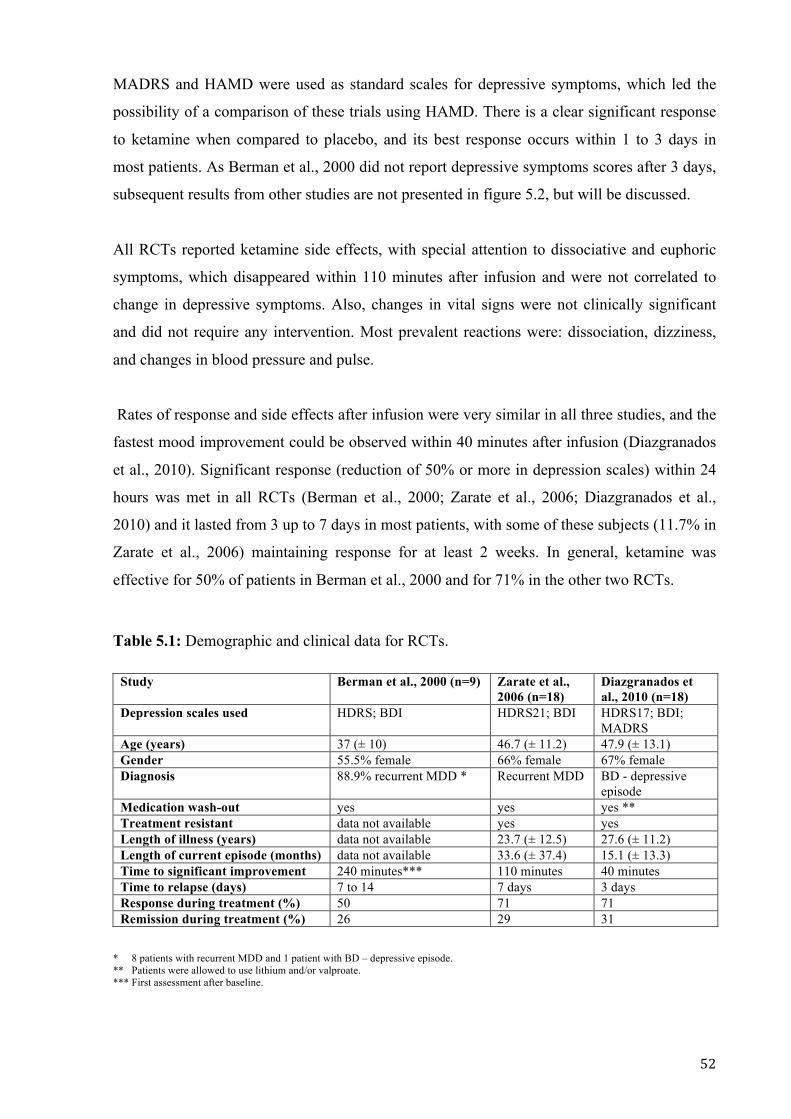
! .*!
MADRS and HAMD were used as standard scales for depressive symptoms, which led the
possibility of a comparison of these trials using HAMD. There is a clear significant response
to ketamine when compared to placebo, and its best response occurs within 1 to 3 days in
most patients. As Berman et al., 2000 did not report depressive symptoms scores after 3 days,
subsequent results from other studies are not presented in figure 5.2, but will be discussed.
All RCTs reported ketamine side effects, with special attention to dissociative and euphoric
symptoms, which disappeared within 110 minutes after infusion and were not correlated to
change in depressive symptoms. Also, changes in vital signs were not clinically significant
and did not require any intervention. Most prevalent reactions were: dissociation, dizziness,
and changes in blood pressure and pulse.
Rates of response and side effects after infusion were very similar in all three studies, and the
fastest mood improvement could be observed within 40 minutes after infusion (Diazgranados
et al., 2010). Significant response (reduction of 50% or more in depression scales) within 24
hours was met in all RCTs (Berman et al., 2000; Zarate et al., 2006; Diazgranados et al.,
2010) and it lasted from 3 up to 7 days in most patients, with some of these subjects (11.7% in
Zarate et al., 2006) maintaining response for at least 2 weeks. In general, ketamine was
effective for 50% of patients in Berman et al., 2000 and for 71% in the other two RCTs. Table 5.1: Demographic and clinical data for RCTs.
* 8 patients with recurrent MDD and 1 patient with BD – depressive episode. ** Patients were allowed to use lithium and/or valproate. *** First assessment after baseline.
Study Berman et al., 2000 (n=9) Zarate et al., 2006 (n=18)
Diazgranados et al., 2010 (n=18)
Depression scales used HDRS; BDI HDRS21; BDI HDRS17; BDI; MADRS
Age (years) 37 (± 10) 46.7 (± 11.2) 47.9 (± 13.1) Gender 55.5% female 66% female 67% female Diagnosis 88.9% recurrent MDD * Recurrent MDD BD - depressive
episode Medication wash-out yes yes yes ** Treatment resistant data not available yes yes Length of illness (years) data not available 23.7 (± 12.5) 27.6 (± 11.2) Length of current episode (months) data not available 33.6 (± 37.4) 15.1 (± 13.3) Time to significant improvement 240 minutes*** 110 minutes 40 minutes Time to relapse (days) 7 to 14 7 days 3 days Response during treatment (%) 50 71 71 Remission during treatment (%) 26 29 31

! .,!
Figure 5.2: HAMD mean values for Diazgranados et al., 2010, Zarate et al., 2006, and Berman et al., 2000. !!
!
10
15
20
25
30
35
baseline 40-60 min 230-240 min day 1 day 2 day 3
placebo - Diazgranados et al., 2010 ketamine - Diazgranados et al., 2010
placebo - Zarate et al., 2006 ketamine - Zarate et al., 2006
placebo - Berman et al., 2000 ketamine - Berman et al., 2000
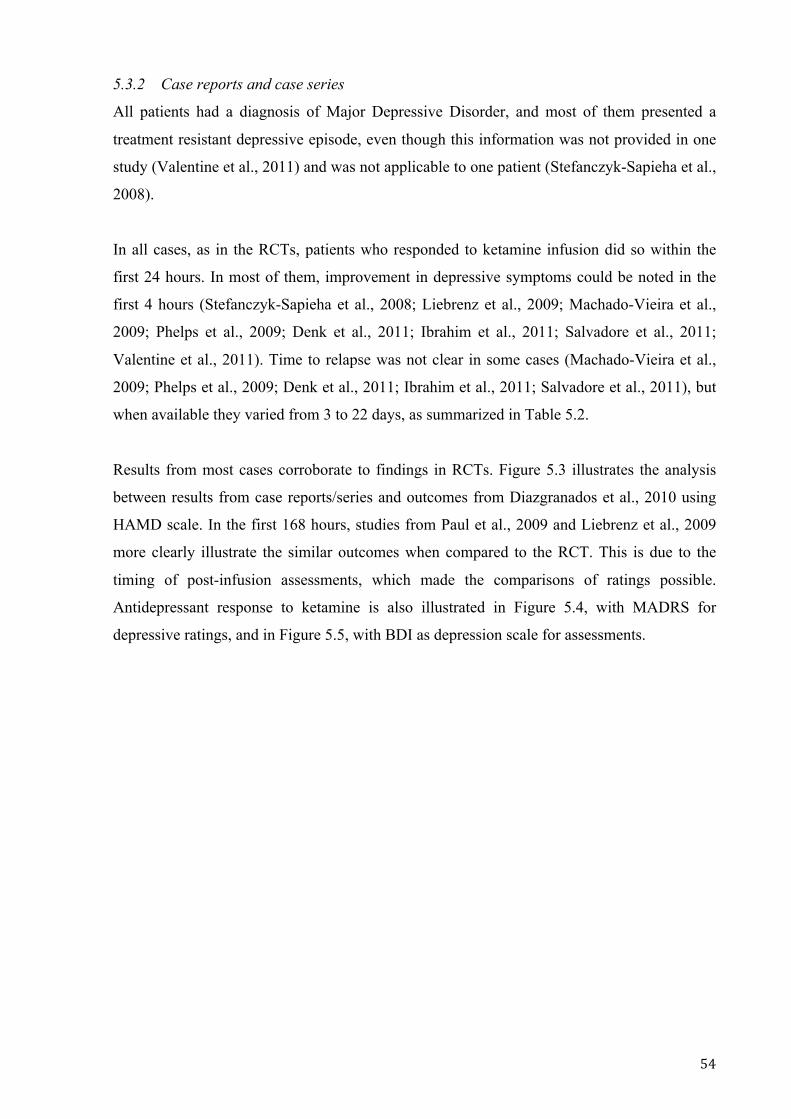
! .-!
5.3.2 Case reports and case series
All patients had a diagnosis of Major Depressive Disorder, and most of them presented a
treatment resistant depressive episode, even though this information was not provided in one
study (Valentine et al., 2011) and was not applicable to one patient (Stefanczyk-Sapieha et al.,
2008).
In all cases, as in the RCTs, patients who responded to ketamine infusion did so within the
first 24 hours. In most of them, improvement in depressive symptoms could be noted in the
first 4 hours (Stefanczyk-Sapieha et al., 2008; Liebrenz et al., 2009; Machado-Vieira et al.,
2009; Phelps et al., 2009; Denk et al., 2011; Ibrahim et al., 2011; Salvadore et al., 2011;
Valentine et al., 2011). Time to relapse was not clear in some cases (Machado-Vieira et al.,
2009; Phelps et al., 2009; Denk et al., 2011; Ibrahim et al., 2011; Salvadore et al., 2011), but
when available they varied from 3 to 22 days, as summarized in Table 5.2.
Results from most cases corroborate to findings in RCTs. Figure 5.3 illustrates the analysis
between results from case reports/series and outcomes from Diazgranados et al., 2010 using
HAMD scale. In the first 168 hours, studies from Paul et al., 2009 and Liebrenz et al., 2009
more clearly illustrate the similar outcomes when compared to the RCT. This is due to the
timing of post-infusion assessments, which made the comparisons of ratings possible.
Antidepressant response to ketamine is also illustrated in Figure 5.4, with MADRS for
depressive ratings, and in Figure 5.5, with BDI as depression scale for assessments.

! ""!
Table 5.2: Demographic and clinical data for cases.
!
Study Caric et
al., 2007
(n=1)
Stefanczyk-
Sapieha et al.,
2008 (n=1)
Liebrenz
et al., 2009
(n=1)
Denk
et al., 2011
(n=1)
Paul
et al., 2009
(n=2)
Valentine
et al., 2011
(n=10)
Salvadore
et al., 2011
(n=14)
Machado-
Vieira et al.,
2009 (n=23)
Phelps et al.,
2009 (n=26)
Mathew
et al., 2010
(n=26)
Ibrahim
et al., 2011
(n=40)
Depression scales
used
BDI HDRS21; BDI BDI; HDRS21 MADRS;
BDI
BDI;
HDRS21
HDRS25 MADRS MADRS MADRS;
HDRS17;
BDI
MADRS;
QIDS-SR16
MADRS
Age (years) 32 50 55 56 54.5 41.7 (± 12) 50.1 (± 10.4) 43.9 (± 13.9) 43.5 (± 14.1) 48.2 (± 11.8) 46.5
Gender male male male female 50%
female
60%
female
35.8%
female
39%
female
39%
female
39%
female
40%
female
Diagnosis MDD MDD MDD MDD recurrent
MDD
MDD * MDD MDD MDD MDD MDD
Medication wash-out no no no NA no yes yes yes yes yes yes
Treatment resistant yes no yes yes yes NA yes yes yes yes yes
Length of illness
(years)
NA NA NA NA 7.5 21.2 (±
17.4)
28.9 (± 14.2) 24.8 (± 12.4) 23.7 (± 12.5) 29.7 25.3
Length of current
episode
NA NA NA NA NA 3.3 years
(± 4.3)
13.2 years
(± 15)
1.7 years
(± 2.26)
6.8 years
(± 8.6)
24.3 years
(± 16.3)
8.3 years
Time to significant
improvement
24 hours 2 hours 24 hours NA 24 hours 1 hour 4 hours 3.83 hours 3.83 hours 2 hours 3.83 hours
Time to relapse
(days)
10 3 7 NA 6 7 NA NA NA 22 NA
Response during
treatment
yes yes yes yes 50% yes, % NA yes, % NA 47.8% 43% 73% 50%
Remission during
treatment
yes no not clear yes no NA NA NA 26% 50% NA
NA = data not available Not clear = meets criteria for 1 assessed scale but not for the second applied scale !!!!!#$%&!'()*''(+,!!
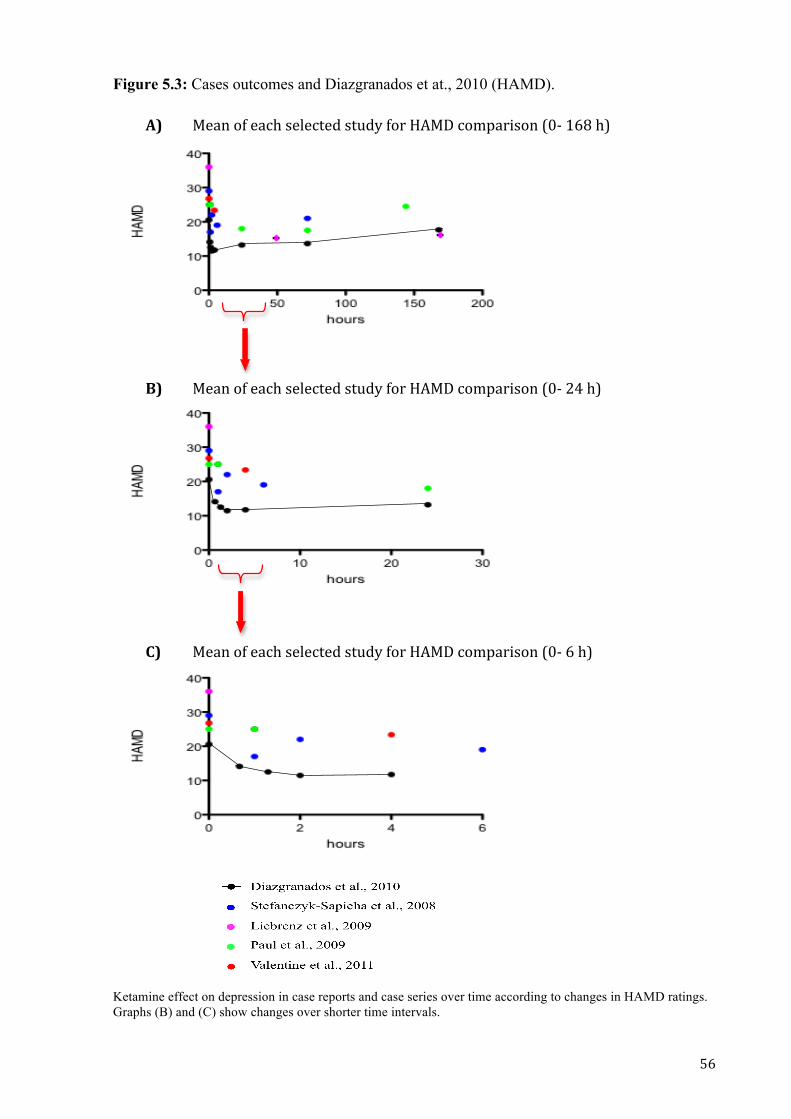
! "#!
Figure 5.3: Cases outcomes and Diazgranados et at., 2010 (HAMD).
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!! !
Ketamine effect on depression in case reports and case series over time according to changes in HAMD ratings. Graphs (B) and (C) show changes over shorter time intervals.!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
$%&'!()!%&*+!,%-%*.%/!,.0/1!)(2!34$5!*(67&28,('!9:;!<#=!+>!
$%&'!()!%&*+!,%-%*.%/!,.0/1!)(2!34$5!*(67&28,('!9:;!?@!+>!
$%&'!()!%&*+!,%-%*.%/!,.0/1!)(2!34$5!*(67&28,('!9:;!#!+>!!"#
$"#
%"#
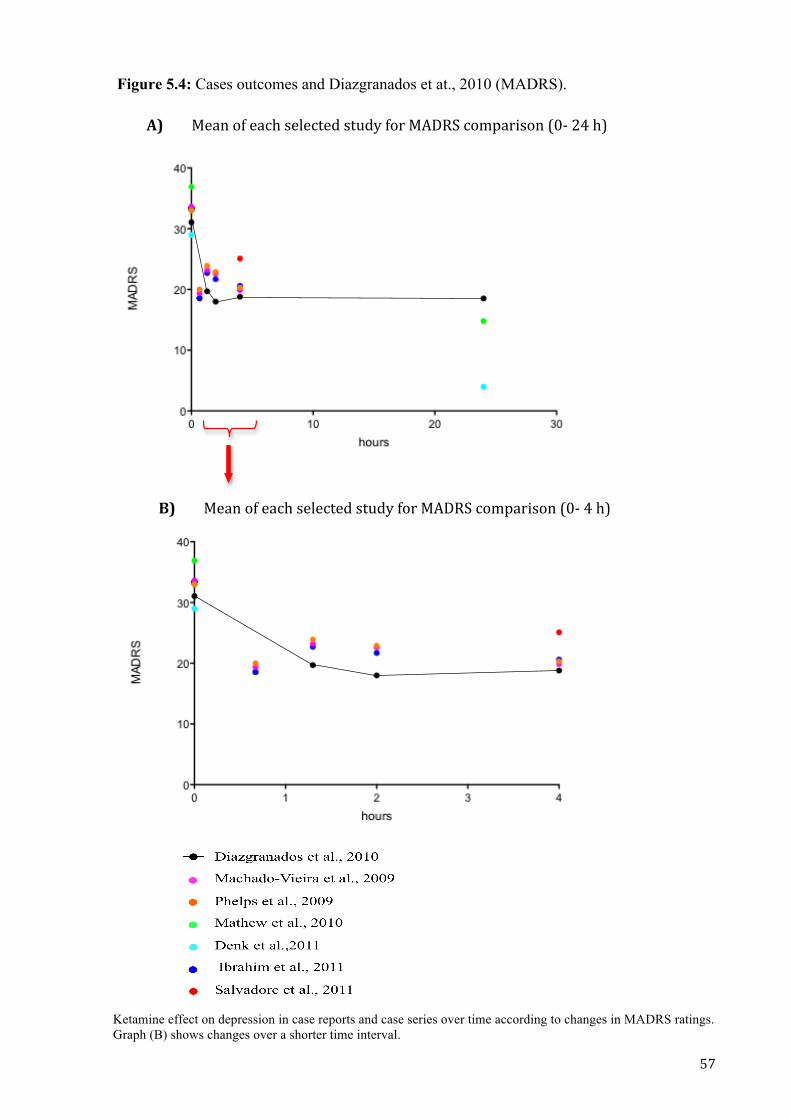
! "A!
Figure 5.4: Cases outcomes and Diazgranados et at., 2010 (MADRS).
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!!!!!!!!!!!!!!!!!!!! !
Ketamine effect on depression in case reports and case series over time according to changes in MADRS ratings. Graph (B) shows changes over a shorter time interval.
!
!
!%"!!!!!!!!$%&'!()!%&*+!,%-%*.%/!,.0/1!)(2!$45BC!*(67&28,('!9:;!?@!+>!!
!
$"!!!!!!!!$%&'!()!%&*+!,%-%*.%/!,.0/1!)(2!$45BC!*(67&28,('!9:;!@!+>!!
!
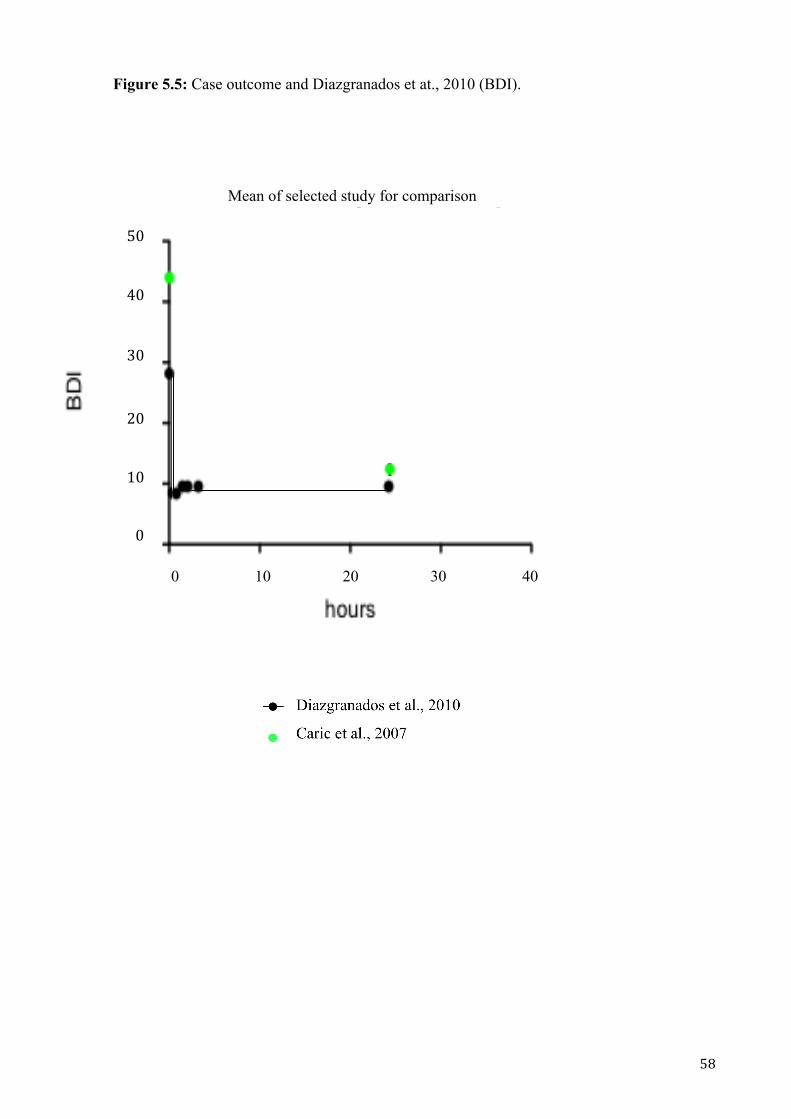
! "=!
Figure 5.5: Case outcome and Diazgranados et at., 2010 (BDI).
!
!
!
0 10 20 30 40
"#!
$#!
%#!
&#!
#!
'#!
0 10 20 30 40
@:!
?:!
<:!
D:!
:!
":!
!
0 10 20 30 40
"#!
$#!
%#!
&#!
#!
'#!
!
0 10 20 30 40
"#!
$#!
%#!
&#!
#!
'#!
!
0 10 20 30 40
"#!
$#!
%#!
&#!
#!
'#!
!
0 10 20 30 40
"#!
$#!
%#!
&#!
#!
'#!
!
0 10 20 30 40
"#!
$#!
%#!
&#!
#!
'#!
!
0 10 20 30 40
"#!
$#!
%#!
&#!
#!
'#!
Mean of selected study for comparison

! "E!
5.3.3 Meta-analysis
In all selected RCTs, a significant antidepressant response was found within 230- 240 minutes
post-infusion. Also, this response was sustained for at least 3 days. HAMD ratings were
relatively stable after 230- 240 minutes post-infusion in the outcomes from Berman et al.,
2000 and Diazgranados et al., 2010. However, Zarate et al., 2006 had a continuous decrease
in depression ratings until day 3 post-infusion (Figure 5.2).
Although Diazgranados et al., 2010 presents a significant treatment effect at 40 minutes after
ketamine infusion, the two other RCTs do not have a significant response within this time.
Thus, the test for overall effect in the meta-analysis results was not statistically significant
(Figure 5.6 A). Diazgranados et al., 2010 presented a faster response than other RCTs and a
shorter duration of ketamine’s antidepressant effects. The possible reasons for this difference
only in Diazgranados et al., 2010 will be discussed further.
At 230 – 240 minutes post-infusion, the three studies are homogeneous and the change in
HAMD scores compared with placebo are substantial and highly statistically significant (5.6
B). At days 1, 2, and 3 post-infusion there are also substantial reductions in HAMD scores
(Figures 5.6 C, D, E). Heterogeneity was evident at days 1, 2, and 3 (highest I2 scores), which
was due to data from Diazgranados et al., 2010.
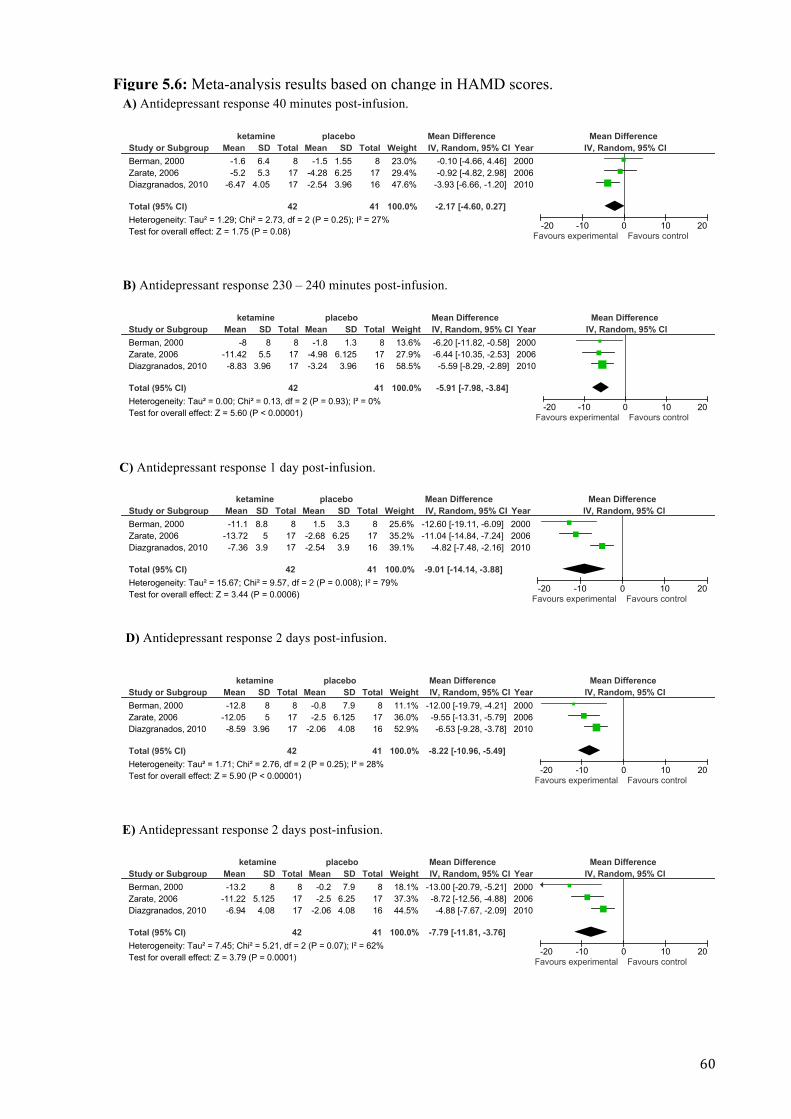
! #:!
Figure 5.6: Meta-analysis results based on change in HAMD scores.
Study or SubgroupBerman, 2000Zarate, 2006Diazgranados, 2010
Total (95% CI)Heterogeneity: Tau! = 1.29; Chi! = 2.73, df = 2 (P = 0.25); I! = 27%Test for overall effect: Z = 1.75 (P = 0.08)
Mean-1.6-5.2
-6.47
SD6.45.3
4.05
Total8
1717
42
Mean-1.5
-4.28-2.54
SD1.556.253.96
Total8
1716
41
Weight23.0%29.4%47.6%
100.0%
IV, Random, 95% CI-0.10 [-4.66, 4.46]-0.92 [-4.82, 2.98]
-3.93 [-6.66, -1.20]
-2.17 [-4.60, 0.27]
Year200020062010
ketamine placebo Mean Difference Mean DifferenceIV, Random, 95% CI
-20 -10 0 10 20Favours experimental Favours control
Study or SubgroupBerman, 2000Zarate, 2006Diazgranados, 2010
Total (95% CI)Heterogeneity: Tau! = 0.00; Chi! = 0.13, df = 2 (P = 0.93); I! = 0%Test for overall effect: Z = 5.60 (P < 0.00001)
Mean-8
-11.42-8.83
SD8
5.53.96
Total8
1717
42
Mean-1.8
-4.98-3.24
SD1.3
6.1253.96
Total8
1716
41
Weight13.6%27.9%58.5%
100.0%
IV, Random, 95% CI-6.20 [-11.82, -0.58]-6.44 [-10.35, -2.53]-5.59 [-8.29, -2.89]
-5.91 [-7.98, -3.84]
Year200020062010
ketamine placebo Mean Difference Mean DifferenceIV, Random, 95% CI
-20 -10 0 10 20Favours experimental Favours control
Study or SubgroupBerman, 2000Zarate, 2006Diazgranados, 2010
Total (95% CI)Heterogeneity: Tau! = 15.67; Chi! = 9.57, df = 2 (P = 0.008); I! = 79%Test for overall effect: Z = 3.44 (P = 0.0006)
Mean-11.1
-13.72-7.36
SD8.8
53.9
Total8
1717
42
Mean1.5
-2.68-2.54
SD3.3
6.253.9
Total8
1716
41
Weight25.6%35.2%39.1%
100.0%
IV, Random, 95% CI-12.60 [-19.11, -6.09]-11.04 [-14.84, -7.24]
-4.82 [-7.48, -2.16]
-9.01 [-14.14, -3.88]
Year200020062010
ketamine placebo Mean Difference Mean DifferenceIV, Random, 95% CI
-20 -10 0 10 20Favours experimental Favours control
Study or SubgroupBerman, 2000Zarate, 2006Diazgranados, 2010
Total (95% CI)Heterogeneity: Tau! = 1.71; Chi! = 2.76, df = 2 (P = 0.25); I! = 28%Test for overall effect: Z = 5.90 (P < 0.00001)
Mean-12.8
-12.05-8.59
SD85
3.96
Total8
1717
42
Mean-0.8-2.5
-2.06
SD7.9
6.1254.08
Total8
1716
41
Weight11.1%36.0%52.9%
100.0%
IV, Random, 95% CI-12.00 [-19.79, -4.21]-9.55 [-13.31, -5.79]-6.53 [-9.28, -3.78]
-8.22 [-10.96, -5.49]
Year200020062010
ketamine placebo Mean Difference Mean DifferenceIV, Random, 95% CI
-20 -10 0 10 20Favours experimental Favours control
Study or SubgroupBerman, 2000Zarate, 2006Diazgranados, 2010
Total (95% CI)Heterogeneity: Tau! = 7.45; Chi! = 5.21, df = 2 (P = 0.07); I! = 62%Test for overall effect: Z = 3.79 (P = 0.0001)
Mean-13.2
-11.22-6.94
SD8
5.1254.08
Total8
1717
42
Mean-0.2-2.5
-2.06
SD7.9
6.254.08
Total8
1716
41
Weight18.1%37.3%44.5%
100.0%
IV, Random, 95% CI-13.00 [-20.79, -5.21]-8.72 [-12.56, -4.88]-4.88 [-7.67, -2.09]
-7.79 [-11.81, -3.76]
Year200020062010
ketamine placebo Mean Difference Mean DifferenceIV, Random, 95% CI
-20 -10 0 10 20Favours experimental Favours control
A) Antidepressant response 40 minutes post-infusion.
B) Antidepressant response 230 – 240 minutes post-infusion.
C) Antidepressant response 1 day post-infusion.
D) Antidepressant response 2 days post-infusion.
E) Antidepressant response 2 days post-infusion.

! #<!
5.4 Discussion
Several RCTs and multiple case reports/series have consistently showed ketamine to be a
rapidly acting antidepressant. Researches with ketamine as a fast acting antidepressant have
not been limited to intravenous administration; some authors have explored alternative routes,
such oral (Irwin and Iglewicz., 2010; Paslaskis et al., 2010) and intramuscular routes (Glue et
al., 2011). The optimal dose and whether it can be used repeatedly, is also not clear. For
example, 0.2mg/kg of ketamine in bolus has demonstrated to be effective for suicidal ideation
(Larkin and Beautrais, 2011). Even more, another study has contributed to these findings,
with promising results for suicidal ideation in treatment resistant MDD, with 0.5mg/kg of
ketamine administered over 40 minutes intravenously (Price et al., 2009). To evaluate dose
response, Glue et al., 2011 compared results for the same patients (n=2) when receiving 0.5,
0.7, and 1mg/kg of intramuscular ketamine. A better outcome was found with the dosage of
1mg/kg, leading us to the question: Would patients, who did not respond to ketamine in other
studies, have a significant response with higher doses? Further investigation is required to
establish how this possible treatment could get to its best results.
In this review, S (+)-ketamine 0.25mg/kg was considered for comparison with racemic
ketamine 0.5mg/kg, as the first is considered to be twice as potent as the racemic mixture
(Hering et al., 1994). According to some studies, S(+) and racemic ketamine do not differ
significantly on hemodynamic changes (White et al., 1985; Ihmsen et al., 2001), being as safe
as racemic ketamine.
The studies analyzed included treatment resistant patients, and their positive outcomes may
indicate an option for this population. Although there were differences in patients’ response
when analyzing MDD and depressive episode in BD (possibly due to the different diagnoses,
use of lithium and valproate in patients with BD, and/or severity of illness) both groups had
generally similar mood responses (Zarate et al., 2006; Diazgranados et al., 2010). Group with
BD may possibly have had faster responses but shorter durations of positive effects
(Diazgranados et al., 2010). This requires future study A similar methodology with a
complete medication washout could exclude the medication factor for analyses. In all studies,
difficulty in maintaining blinding of groups and researchers was clear, as ketamine side
effects (such as euphoria and depersonalization) were easily recognizable. Also, in all RCTs,
depersonalization was not correlated to change in depressive symptoms, indicating that
psychomimetic effects are not required to a positive result.
! #?!
Continuous infusions (with the same methodology used for the first infusion) were present in
3 of the reviewed cases. Stefanczyk-Sapieha et al., 2011 presented a patient who had a shorter
response (24 hours) to ketamine after a second infusion, while the first infusion provided
depression response for up to 3 days. By the other hand, Paul et al., 2009 and Liebrenz et al.,
2009 presented outcomes in a second infusion that were similar to the first ketamine
administration.
Types of rating scales, and timing of ratings, varied across reports. The MADRS and HAMD
were the most commonly used depression scales. Ideally, time points from baseline to 40
minutes, 120 minutes, 240 minutes, 1 day, 3 days, 7 days and more days if response is
maintained may provide important observations for future reviews, as this information was
not reported in many studies. Results were consistent between 4 hours and 3 days post-
infusion, and may be of important consideration for future studies.
5.5 Conclusions
Ketamine has been extensively studied as an antidepressant in the last decade. There are
promising data in terms of rapidity of mood improvement in RCTs involving patients with
refractory unipolar and bipolar depression. Data from case reports and case series are
generally similar to those reported in the RCTs. Significant areas that require clarification
include what the optimal dose and route of administration are, and whether ketamine can be
used in patients with less refractory mood disorders. Although mood responses in unipolar
and bipolar depression appear to be similar, it may be prudent to only include one or other
patient group in future RCTs, and not to combine them. Methodologically, it would be
important for investigators to use similar rating scales and time-points, to maximize
comparisons between studies.

! #D!
CHAPTER 6
Protocol for testing ketamine in Major
Depressive Disorder in terminal cancer
patients
! #@!
6.1 Introduction
This protocol was based on studies that present positive results of ketamine as a fast acting
antidepressant (Diazgranados et al., 2010; Zarate et al, 2006; Berman et al., 2000).
Considering that patients with terminal cancer have a short life expectancy and high rates of
depression, ketamine may be a possible treatment for this population. This trial has been
approved by the Lower South Regional Ethics Committee and is a registered trial -ACTRN
12610001011077. It is one of the first trials of ketamine for depression in patients with
cancer. In particular, this group of patients may benefit from the analgesic effects of
ketamine, as pain rates are also high in this population. Its design addresses a number of key
clinical questions in a scientifically rigorous manner, including:
1- Confirmation that low dose ketamine is an effective antidepressant in a palliative care
cancer population;
2- Demonstration that repeated doses are safe and effective;
3- Characterization of dose-response profile, particularly as this patient group may be
physically debilitated.
The trial consists of 3 stages, each one concerning to the abovementioned objectives, and all
stages take place in a hospital room, with emergency support if needed.
6.2 Stages
6.2.1 Stage 1
Open label characterization of safety and efficacy of 1 mg/kg single dose IM ketamine in 10
depressed patients with cancer. If an antidepressant response can be demonstrated in 5/10
patients, with tolerable side effects, subjects are eligible to proceed to stages 2 and 3. A 50%
improvement in depressive symptoms in MADRS is considered response to treatment
(Zimmerman et al., 2004; Zarate et al., 2006).
6.2.2 Stage 2
Open label characterization of safety and efficacy of 1mg/kg repeat dose IM ketamine in 10
depressed patients with cancer. Subjects that present a sustained response, with tolerable side
effects, are eligible to keep receiving treatment if symptoms recurred. Patients had the option
to drop out of the trial at any time.

! #"!
6.2.3 Stage 3
Double blind, randomized, dose-response assessment of single dose IM ketamine in 30
depressed patients with cancer. Injection dose might be 0.1mg/kg, 0.5mg/kg or 1mg/kg.
Subjects can decide not to participate on Stage 3 at any time.
6.3 Inclusion and exclusion criteria
6.3.1 Inclusion criteria:
• ECOG performance status ! 3 (Table 6.1),
• MADRS >20 (Figure 6.1),
• Comparative Pain Scale ratings ! 5 (Table 6.2),
• presence of terminal (incurable) cancer,
• life expectancy of at least 3 months,
• aged 20 to 65 years-old,
• adequate hematological, renal and hepatic function,
• signed informed consent.
MADRS scores >20 are standard for entry into antidepressant clinical trials (Machado-Vieira
et al., 2009; Diazgranados et al., 2010). Patients with mild to moderate levels of pain were
eligible, but patients with severe pain were excluded, as there might be a bias in patients’
outcomes (as a response in depressive symptoms might be due to pain relief). Subjects could
be confined to bed or chair more than 50% of waking hours and with limited self-care, but not
totally confined to bed or chair or completely disabled, as this would limit data collection.
Further, considering the risk of arrhythmias, slow urinary excretion, and slow hepatic
metabolism, cardiac, renal and hepatic function had to be adequate. Also, patients had to
provide written informed consent.
6.3.2 Exclusion criteria:
• presence of psychosis or delirium,
• presence of cerebral metastasis,
• current use of ketamine,
• current use of another experimental medication,
• any antidepressant treatment started within the last 4 weeks.

! ##!
Considering psychosis and delirium, as there is a lack of reasoning and judgment, patients
would not be able to give informed consent, and the use of ketamine in these population,
might cause a worsening in their symptoms (Ketalar- Medsafe). The presence of cerebral
metastasis may cause neurologic and psychiatric symptoms and change the permeability of
the blood-brain barrier (Chakrabarti et al., 2011; Lee 2010; Abbott et al., 2006). The last
might lead to a different dosage of the medication acting in the brain. Current use of ketamine
was not allowed because it might be already impacting patient’s mood, and experimental
medication because of possible unknown influence in depressive symptoms. Subjects could
not be receiving any new treatment for depression in the last 4 weeks (including
psychotherapy), to avoid positive results that might not be linked to ketamine administration.
Entry criteria assessment sheets can be found in attachments.
Table 6.1: ECOG performance status.
Table from: Oken et al., 1982.
Grade ECOG 0 Fully active, able to carry on all pre-disease performance without restriction 1 Restricted in physically strenuous activity but ambulatory and able to carry out
work of a light or sedentary nature, e.g., light house work, office work 2 Ambulatory and capable of all selfcare but unable to carry out any work
activities. Up and about more than 50% of waking hours 3 Capable of only limited selfcare, confined to bed or chair more than 50% of
waking hours 4 Completely disabled. Cannot carry on any selfcare. Totally confined to bed or
chair 5 Dead
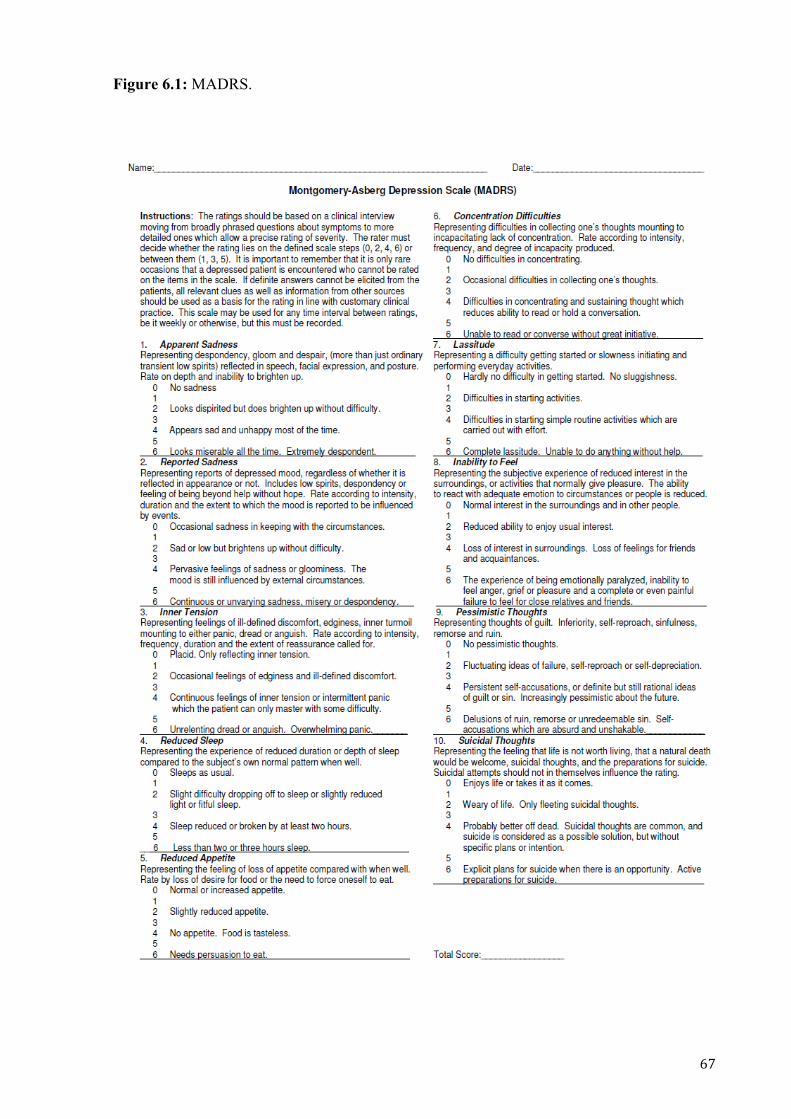
! #A!
Figure 6.1: MADRS.

! #=!
Table 6.2: The Comparative Pain Scale.
0
No pain. Feeling perfectly normal.
Minor
Does not interfere with most activities. Able to adapt to pain psychologically and with medication or devices such as cushions.
1
Very Mild
Very light barely noticeable pain, like a mosquito bite or a poison ivy itch. Most of the time you never think about the pain.
2
Discomforting
Minor pain, like lightly pinching the fold of skin between the thumb and first finger with the other hand, using the fingernails. Note that people react differently to this self-test.
3 Tolerable
Very noticeable pain, like an accidental cut, a blow to the nose causing a bloody nose, or a doctor giving you an injection. The pain is not so strong that you cannot get used to it. Eventually, most of the time you don't notice the pain. You have adapted to it.
Moderate
Interferes with many activities. Requires lifestyle changes but patient remains independent. Unable to adapt to pain.
4 Distressing
Strong, deep pain, like an average toothache, the initial pain from a bee sting, or minor trauma to part of the body, such as stubbing your toe real hard. So strong you notice the pain all the time and cannot completely adapt. This pain level can be simulated by pinching the fold of skin between the thumb and first finger with the other hand, using the fingernails, and squeezing real hard. Note how the simulated pain is initially piercing but becomes dull after that.
5
Very Distressing
Strong, deep, piercing pain, such as a sprained ankle when you stand on it wrong, or mild back pain. Not only do you notice the pain all the time, you are now so preoccupied with managing it that you normal lifestyle is curtailed. Temporary personality disorders are frequent.
6 Intense
Strong, deep, piercing pain so strong it seems to partially dominate your senses, causing you to think somewhat unclearly. At this point you begin to have trouble holding a job or maintaining normal social relationships. Comparable to a bad non-migraine headache combined with several bee stings, or a bad back pain.
Severe
Unable to engage in normal activities. Patient is disabled and unable to function independently.
7
Very Intense
Same as 6 except the pain completely dominates your senses, causing you to think unclearly about half the time. At this point you are effectively disabled and frequently cannot live alone. Comparable to an average migraine headache.
8
Utterly Horrible
Pain so intense you can no longer think clearly at all, and have often undergone severe personality change if the pain has been present for a long time. Suicide is frequently contemplated and sometimes tried. Comparable to childbirth or a real bad migraine headache.
9
Excruciating Unbearable
Pain so intense you cannot tolerate it and demand pain killers or surgery, no matter what the side effects or risk. If this doesn't work, suicide is frequent since there is no more joy in life whatsoever. Comparable to throat cancer.
10
Unimaginable Unspeakable
Pain so intense you will go unconscious shortly. Most people have never experienced this level of pain. Those who have suffered a severe accident, such as a crushed hand, and lost consciousness as a result of the pain and not blood loss, have experienced level 10.!

! #E!
6.4 Informed consent
For each subject, a consent form, which was written in lay terms, was given and thoroughly
explained. After having complete understanding of the trial, patients had up to 2 days to think,
talk to friends, family, other doctors, etc. Further, individuals were reassured that they could
withdraw their consent at anytime, without needing to explain or giving a reason for it. It was
also emphasized that withdrawing would not affect their health treatment in any way. A copy
of the informed consent is attached to this thesis (Appendix I).
6.5 Assessments
In all three stages, two main scales were used to access depression ratings (MADRS; Figure
6.1) and pain (The Comparative Pain Scale; Table 6.2). These were performed at screening
(20 minutes before injection) and 1, 2, 4, 24, 48, 72, and 120 hours post-injection. Other
scales used in the study were: Hospital Anxiety and Depression Scale (HADS; Figure 6.2)
and Demoralization Scale (Figure 6.3), which were performed at baseline and 24 hours post-
injection.
MADRS is a well known and validated scale to access depression (Phelps et al., 2009;
Diazgranados et al., 2010). Also, it includes all DSM-IV criteria for MDD (Montgomery and
Asberg, 1979). Its main difference when compared to HADS is that the last one does not
include physical symptoms in its rating. Therefore, HADS is often used in patients with
cancer and other somatic diseases (Zigmond and Snaith, 1983; Bjelland et al., 2002).
Demoralization Scale consists of 24 questions with a total score ranging from 0 to 96, and a
score > 30 is considered high. This suggests the presence of adjustment disorder or even a
depressive episode (Kissane et al., 2004). Considering the fact that cancer patients usually
experience pain, Comparative Pain Scale was used to assess its intensity. This scale consists
of scores that range from 0 to 10, considering 0 as “no pain” and 10 as “unspeakable pain”.
Also, it is going to be useful to check correlation between pain and depression, as many
studies report their high correlation, even though its neural basis is not yet elucidated (Bair et
al., 2003; Strigo et al., 2008).
Vital signs were assessed on baseline, 1, 2, 3, and 4 hours post-injection on stage 1 and 3. At
stage 2, if patients maintain a stable and normal blood pressure, after 3 repeat dosing,
assessments are made on baseline, 1, and 2 hours post-injection. Vital signs assessments are
repeated at any time if patients present distressing side effects or report possible cardiac
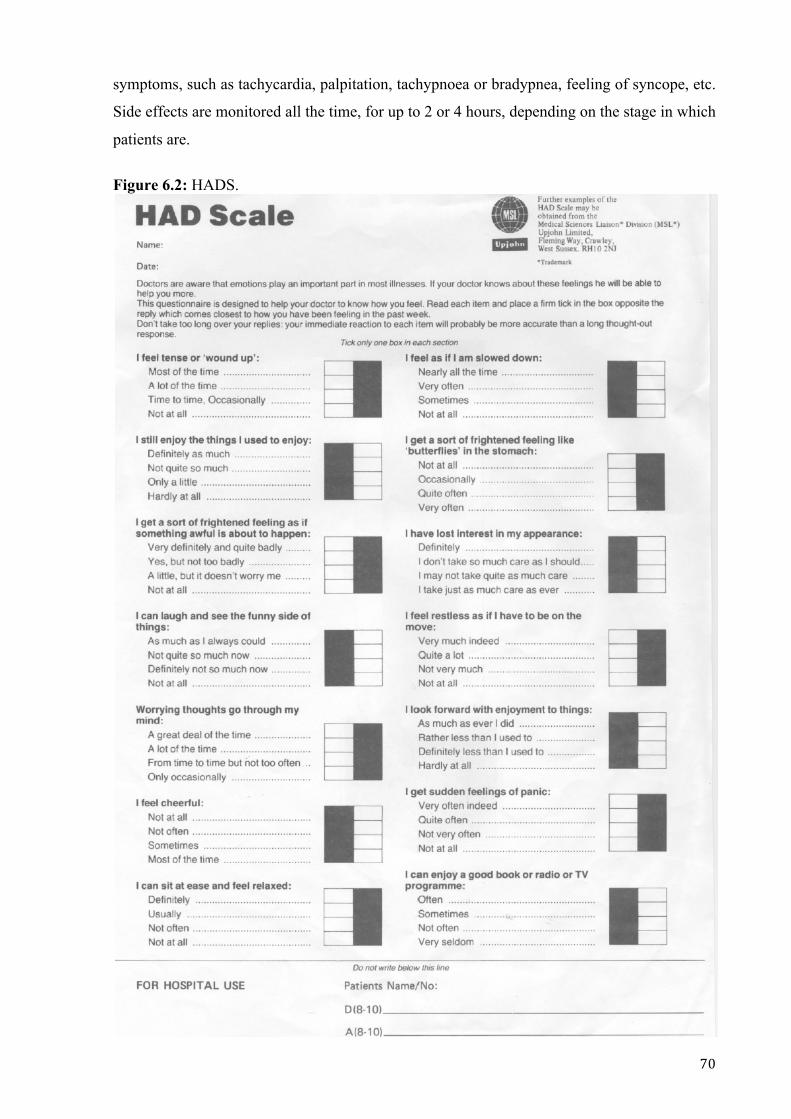
! A:!
symptoms, such as tachycardia, palpitation, tachypnoea or bradypnea, feeling of syncope, etc.
Side effects are monitored all the time, for up to 2 or 4 hours, depending on the stage in which
patients are.
Figure 6.2: HADS.

! A<!
Figure 6.3: The Demoralization Scale. F(2!%&*+!,.&.%6%'.!G%-(HI!1(0!&2%!&,J%/!.(!8'/8*&.%!+(H!,.2('K-1!.+%!,.&.%6%'.!+&,!&77-8%/!.(!1(0!(L%2!
.+%!-&,.!.H(!H%%J,!G1!*82*-8'K!.+%!*(22%,7('/8'K!'06G%2M!NL%2!.+%!7&,.!.H(!H%%J,!+(H!().%'!+&L%!1(0!
)%-.O!
# &'(')# *'+,-.# *-.'/01.'2# 340'5# %++#06'#
71.'#
<M!!!P+%2%!8,!&!-(.!()!L&-0%!8'!H+&.!Q!*&'!())%2!
(.+%2,M!:! <! ?! D! @!
?M!!!!$1!-8)%!,%%6,!.(!G%!7(8'.-%,,M! :! <! ?! D! @!
DM!!!!P+%2%!8,!'(!7027(,%!.(!.+%!&*.8L8.8%,!8'!61!-8)%M!! :! <! ?! D! @!
@M!!!!$1!2(-%!8'!-8)%!+&,!G%%'!-(,.M! :! <! ?! D! @!
"M!!!!Q!'(!-('K%2!)%%-!%6(.8('&--1!8'!*('.2(-M! :! <! ?! D! @!
#M!!!!Q!&6!8'!K((/!,7828.,M! :! <! ?! D! @!
AM!!!!R(!('%!*&'!+%-7!6%M!!! :! <! ?! D! @!
=M!!!!Q!)%%-!.+&.!Q!*&''(.!+%-7!61,%-)M! :! <! ?! D! @!
EM!!!!Q!)%%-!+(7%-%,,M! :! <! ?! D! @!
<:M!!Q!)%%-!K08-.1M! :! <! ?! D! @!
<<M!!Q!)%%-!8228.&G-%M! :! <! ?! D! @!
<?M!!Q!*(7%!)&82-1!H%--!H8.+!-8)%M! :! <! ?! D! @!
<DM!!Q!+&L%!&!-(.!()!2%K2%.!&G(0.!61!-8)%M! :! <! ?! D! @!
<@M!!S8)%!8,!'(!-('K%2!H(2.+!-8L8'KM!!! :! <! ?! D! @!
<"M!!Q!.%'/!.(!)%%-!+02.!%&,8-1M! :! <! ?! D! @!
<#M!!Q!&6!&'K21!&G(0.!&!-(.!()!.+8'K,M! :! <! ?! D! @!
<AM!!Q!&6!72(0/!()!61!&**(67-8,+6%'.,M! :! <! ?! D! @!
<=M!!Q!)%%-!/8,.2%,,%/!&G(0.!H+&.!8,!+&77%'8'K!.(!
6%M!:! <! ?! D! @!
<EM!!Q!&6!&!H(2.+H+8-%!7%2,('M! :! <! ?! D! @!
?:M!!Q!H(0-/!2&.+%2!'(.!G%!&-8L%M! :! <! ?! D! @!
?<M!!Q!)%%-!,&/!&'/!68,%2&G-%M! :! <! ?! D! @!
??M!!Q!)%%-!/8,*(02&K%/!&G(0.!-8)%M! :! <! ?! D! @!
?DM!!Q!)%%-!T08.%!8,(-&.%/!(2!&-('%M! :! <! ?! D! @!
?@M!!Q!)%%-!.2&77%/!G1!H+&.!8,!+&77%'8'K!.(!6%M! :! <! ?! D! @!
!"#$%&'()*&&&&&&&&&&&&&&&&&&&&&&&&&&&&&&&&&&&&&&&&&&&&&&&&&&&&&&R(.%!H+%'!,*(28'KU!8.%6,!<I!#I!<?I!<A!&'/!<E!&2%!2%L%2,%!,*(2%/M&

! A?!
6.6 Statistical Analysis
All data were listed, and summary statistic (mean, SD) calculated. Change scoring in MADRS
and pain ratings were calculated by subtracting scores post-dosing from baseline values.
Correlation of change in pain and depression scores was made using Pearson’s method.
6.7 Conclusions
This protocol presents similarities with previous studies, however it adds pain scores.
Ketamine has analgesic properties, thus correlation between pain and depression responses
can be assessed. Results found with this methodology may shed light to the relationship
between pain and depression as they are frequently coexistent and some authors claim their
interdependence (Mongini et al., 2007; Waters et al., 2004). Also, another aspect of this
protocol is the possibility of repeated ketamine injections for Major Depression.
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
! AD!
CHAPTER 7
Acute and maintenance IM ketamine for a
depressed patient with terminal cancer

! A@!
7.1 Introduction
This chapter describes a patient enrolled in a clinical trial to assess the effects of Ketamine in
MDD in patients with terminal cancer. The trial was approved by the Lower South Regional
Ethics Committee, Southern Health District Board and Dunedin School of Medicine,
University of Otago, New Zealand (ACTRN 12610001011077). The patient participated in
Stages 1 and 2 of this trial.
7.2 Case Report
A. is a 37-year-old patient with metastatic ovarian carcinoma. She has a diagnosis of Major
Depressive Disorder (MDD) and Dysthymic Disorder since she was 18 years old. Although
she has used various antidepressants, A. reports her mood was never fully improved. For the
past 10 years she presented a worsening of her depressive symptoms, which persisted at the
time of her entrance in the study, including: irritability, low mood, lack of energy, easy
crying, sleep disturbance, poor concentration, intense and excessive feelings of guilt and
suicidal ideation. Her domestic circumstances were very stressful, due to concern about the
future of her 11-year-old daughter and the lack of support from her friends and family.
The most distressing symptoms of her metastatic ovarian carcinoma, was visceral pain in the
right iliac fossa, which started 4 months after her diagnosis of cancer. Her diagnosis was
made in January of 2010, and her pain was in the same location as a metastatic tumor, which
was about 7cm in diameter on palpation in November of 2011. For pain intensity assessment,
The Comparative Pain Scale, with a range from 0 to 10 was used (Harich- online resource).
She also has a previous history of drug abuse, which started when she was 17 years old, with
the use of cannabis. At 21 years old, she used cocaine, heroin and methamphetamine. With
time, her drug of choice was methamphetamine. In 2004 she was able to quit the use of drugs
after starting methadone for opioid substitution therapy. A. has been abstinent since then.
There is also a family history of alcoholism (both grandfathers and one uncle).
When first assessed for this ketamine trial, A. was taking venlafaxine 150 mg/day, quetiapine
50 mg/day, and methadone 95 mg/day. All her medications were continued during her
ketamine treatment with doses unchanged. She was also receiving chemotherapy once a week
(a combination of carboplatin and gemcitabine). After informed consent was given, she
received ketamine 1 mg/kg IM open-label, and her dosing was performed on an outpatient
basis in a hospital clinic.

! A"!
The Montgomery-Asberg Scale (MADRS) was used as the main scale to assess her
depression severity. This scale consists of 10 items, each one scored from 0 to 6 (total range
from 0 to 60). Scores > 20 are standard for entry into antidepressant clinical trials
(Diazgranados et al., 2010; Machado-Vieira et al., 2009). Mood and pain assessments were
obtained at baseline (20 minutes before injection), 1, 2, 4, 24, 48, 72 and 168 hours post-
injection. The Hospital Anxiety and Depression Scale (HADS) is often used in patients with
cancer or other somatic diseases, and its optimal cut off scores are > 7 on both HADS-A and
HADS-D for anxiety and depression respectively (Zigmond and Snaith, 1983; Bjelland et al.,
2002). No physical symptoms are included in this scale, permitting a focus on affective and
behavioral symptoms (Zigmond and Snaith, 1983). The Demoralization Scale (DS) consists
of 24 questions (with a total score range from 0 to 96), and a score > 30 is considered high
(Kissane et al., 2004). HADS and DS were assessed at baseline and 24 hours.
The patient’s initial MADRS score was 24, dropping to 7 one hour after the first dose of
ketamine (Figure 7.1 A). For the next 2 days her MADRS remained low (lowest score was 5
points), with improvement in all MADRS items. Depressive symptoms returned after 6 - 7
days post-injection. Also, her pain score was reduced within 15 to 20 minutes after the first
ketamine dose, however her scores for pain returned to baseline within 24 hours (Figure 7.1
A). A. reported moderate but tolerable dissociative side effects, such as depersonalization and
immobility, starting 5 minutes post-injection and resolving within 45 to 60 minutes. Vital
signs were unchanged.
The patient subsequently received repeat ketamine doses at intervals of 8 to 10 days, based on
return of her depressive symptoms, initially receiving treatment when her depressive scores
were higher than 20. Her mood response to repeat injections has been identical each time, in
terms of speed, magnitude of response and duration (Figure 7.1 B). Onset of pain relief
continued to be fast, nevertheless the durability of analgesic response was much more variable
(Figure 7.1 C). Reported side effects were similar in timing of onset and intensity to those
noted after the first dose of ketamine. Scores on HADS and DS demonstrated consistent
improvement in her mood symptoms (Figure 7.2). Correlation between changes in depression
and pain scores over time were initially robust, but decreased over the next 168 hours (Figure
7.3).

! A#!
Figure 7.1: Antidepressant and analgesic response to IM ketamine 1mg/kg.
!
A) Antidepressant and analgesic effects after first IM injection of ketamine 1 mg/kg – Stage 1. B) Consistency of antidepressant response after 6 injections. C) Inconsistency in pain response after 24 hours after 6 injections.
V&8'!9!!>!
:!!!!!!!!!!!!!?@!!!!!!!!!!!!@=!!!!!!!!!!!!A?!!!!!!!!!!!!!E#!!!!!!!!!!!<?:!!!!!!!!!<@@!!!!!!!!!!<#=!!!!!!!!!!<E?!
!
?"!
?:!
D:!
<:!
!!"!
!:!
<"!
D!
?!
<!
:!
@!
"!
$45BC!9!!>!
V&8'!2&.8'K!9!!>!
.86%!9+>!!
!!$45BC!
!!!!!.86%!9+>!
:!!!!!!!!!!!!!?@!!!!!!!!!!!!@=!!!!!!!!!!!!A?!!!!!!!!!!!!!E#!!!!!!!!!!!<?:!!!!!!!!!<@@!!!!!!!!!!<#=!!!!!!!!!!<E?!
?"!
?:!
D:!
<:!
!!"!
!:!
<"!
$45BC!
time (h) 0 24 48 72 96
!
120 144 168 192
V&8'!2&.8'K!
0
1 !
2
3
4
5
6
7
! !
!
! !
!
!
! !
!
! ! ! ! !
! !
! ! !
!
!
! ! !
!
!
!
!
! !
! !
!
!
! !
! ! ! !
! !
! !
! ! !
!
!
! !
!
! !
! Dose 1 Dose 2 Dose 3 Dose 4 Dose 5 Dose 6
! ! ! ! ! !
!!
!
!!
!
!
!!
!
! ! ! !!
!!
! ! !
!
!
!!!
!
!
!
!
!!
! !
!
!
!!
!!! !
! !
!!
!!!
!
!
!!
!
! !
A)
B)
C)
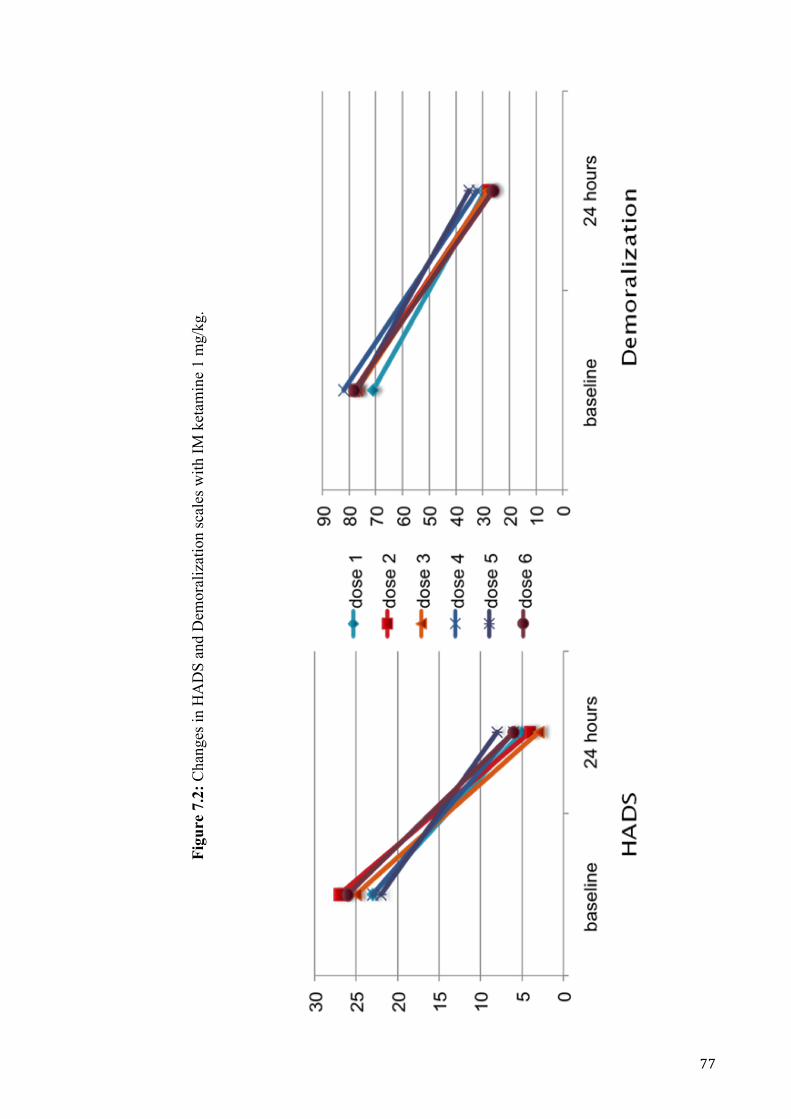
! AA!
Figu
re 7
.2: C
hang
es in
HA
DS
and
Dem
oral
izat
ion
scal
es w
ith IM
ket
amin
e 1
mg/
kg.
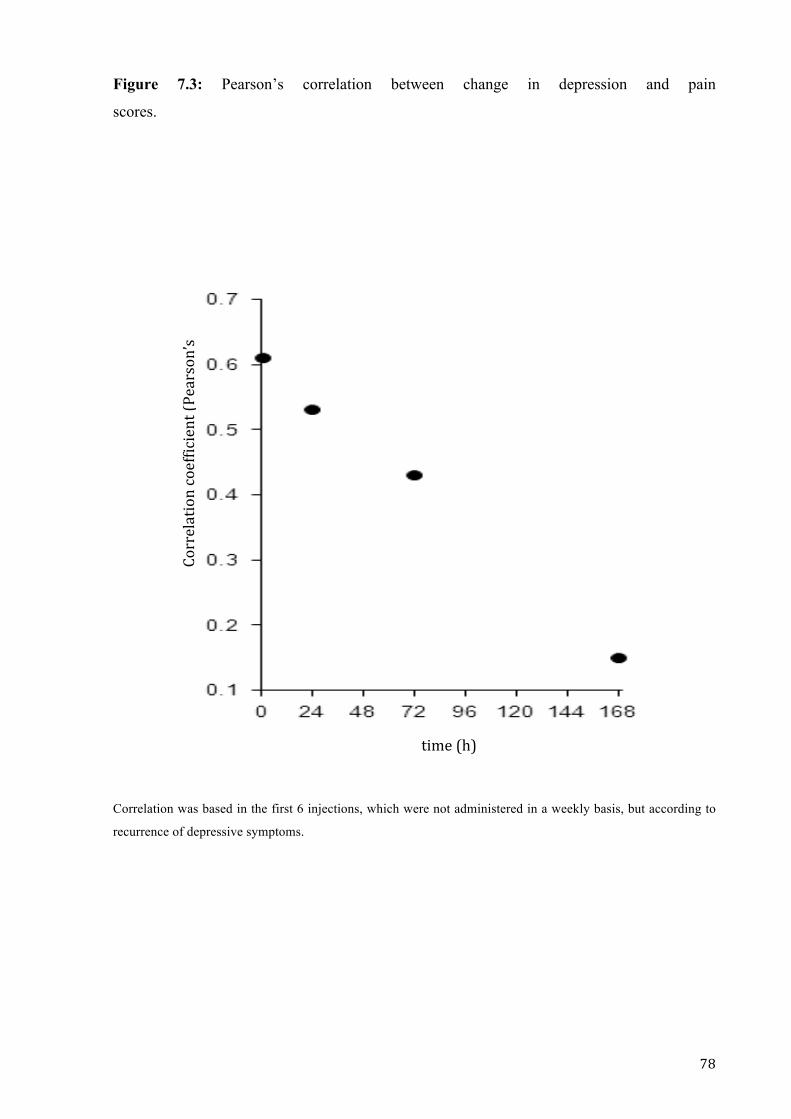
! A=!
Figure 7.3: Pearson’s correlation between change in depression and pain
scores.
Correlation was based in the first 6 injections, which were not administered in a weekly basis, but according to
recurrence of depressive symptoms.
!!!!!!!!!!!!!!!W(22%-&.8('!*(%))8*8%'.!9V%&2,('X,!
B>!
!!!!!!!!!!!.86%!9+>!!
! AE!
The improvement in the patient’s mood was noticed by her family, even on the phone when
talking to her sister. Also, her daughter noted she was calmer and more patient. In visits to
A.’s house to collect mood assessments these reported comments were verified.
After a total of 7 injections, A. asked for dosing before recurrence of her depressive
symptoms. As her depression was in remission for 7 days, with MADRS starting to increase 8
to 10 days post-injection, the patient started to receive ketamine on a weekly basis. With the
treatment at every 7 days, following the same protocol for the previous injections, she
obtained remission of MDD. There were two occasions, when her MADRS scores increased
to > 10, when she was unable to attend the clinic appointments, with delays between dosings
of 8 and 9 days respectively. Using this method of administration, her depression has
continued to respond to weekly ketamine dosing over 8 months (Figure 7.4). During this time,
the patient had changes in her cancer treatment, without demonstrating changes in her
response to ketamine injections for her depression. Except for the two time-points
abovementioned, the patient has maintained remission, with no complaints of cognitive
impairment. Also, side effects (such as depersonalization, inability to move, and dizziness)
were less notable with this dosage regimen.
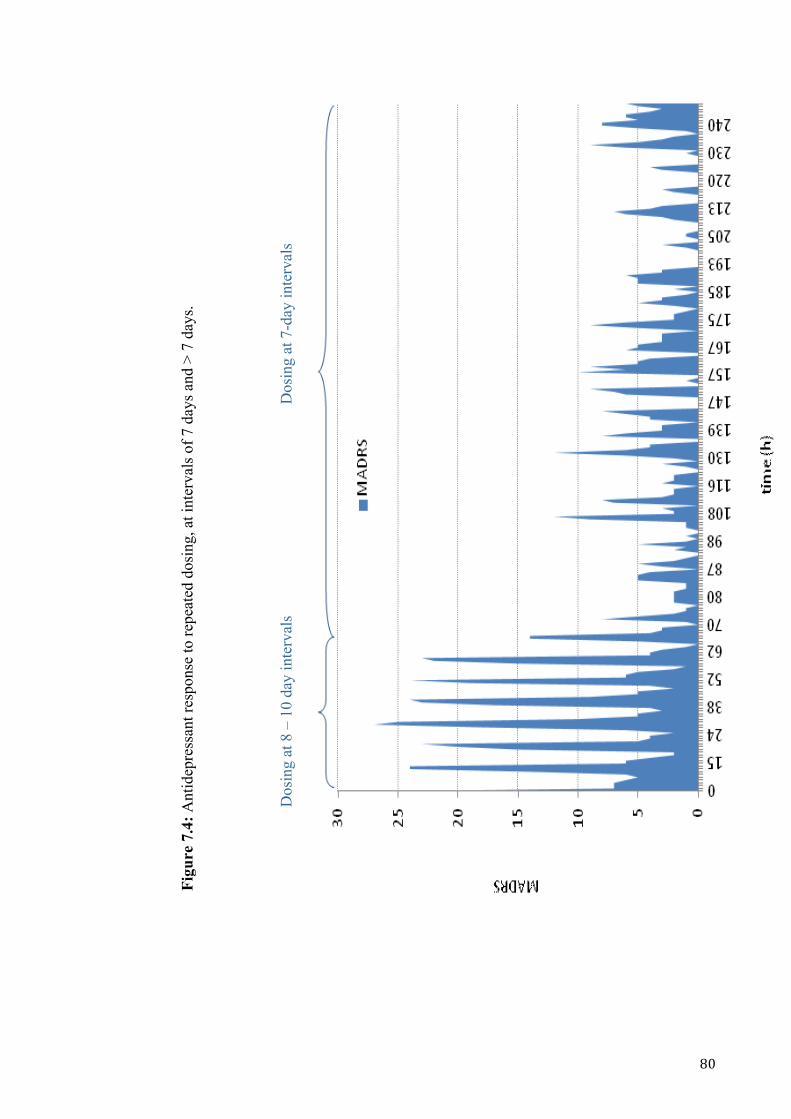
! =:!
Figu
re 7
.4: A
ntid
epre
ssan
t res
pons
e to
repe
ated
dos
ing,
at i
nter
vals
of 7
day
s and
> 7
day
s.
!
D
osin
g at
8 –
10
day
inte
rval
s
Dos
ing
at 7
-day
inte
rval
s

! =<!
7.3 Discussion
This is the second case report with ketamine being used as a fast acting antidepressant in
patients with a diagnosis of cancer (Stefanczyk-Sapieha et al., 2008). The present report
extends information on ketamine use by assessing simultaneous effects on mood and pain
ratings, and by demonstrating the reproducibility of the antidepressant response with multiple
repeated doses.
The patient had remission (MADRS < 10; Hawley et al., 2002) of her depressive symptoms
within one hour after receiving the first injection of IM ketamine at a dose of 1mg/kg. This
finding is consistent with previous research, which noted a rapid mood response for more than
70% of patients within 24 hours (aan het Rot et al., 2010; Zarate et al., 2006). A.’s
improvement was sustained for 6 to 7 days, with depression scores gradually returning to
baseline, which was also consistent with recent studies (aan het Rot et al., 2010; Berman et
al., 2000). Some authors have reported the fact that some patients present a sustained mood
response for even longer periods of time (aan het Rot et al., 2010; Messer and Haller, 2010).
Most previous researchers used ketamine intravenously (usually over 40 minutes) rather than
IM injections, as used in this case. In a recent study, pharmacokinetic simulations suggested
comparable exposures after IV infusion and IM injection (Glue et al., 2011). In the present
case, the dose used (1mg/kg) was higher than those administered in most published cases,
which used 0.5mg/kg of Ketamine (aan het Rot et al., 2010; Zarate et al., 2006; Berman et al.,
2000), and the optimal dose for MDD treatment is still unclear. Changes in the
Demoralization Scale and HADS ratings were consistent with the MADRS data.
The analgesic effects of ketamine were also fast in onset, however its durability was variable
after 24 hours post-injection. Changes in pain scores and depression ratings were most closely
correlated 1 hour post-dosing (Pearson’s r = 0.61) with progressively weaker correlations over
the next 168 hours. This finding suggests that the sustained antidepressant effects of ketamine
are mediated differently from the mechanisms associated with immediate changes in pain and
mood. One possible mechanism may be via stimulation of mTOR signaling and via synaptic
protein synthesis (Duman et al., 2012).
A. did not experience tachyphylaxis to repeated ketamine injections, as demonstrated by the
consistent improvement in her mood scores at every injection and by her sustained remission
with weekly dosages. Messer et al., 2010 reported similar findings, with maintenance of
remission in one patient for more than 15 months, with ketamine infusions given every 3
weeks. In contrast, it should be noted that Liebrenz et al., 2009 reported a different response
! =?!
to a second ketamine infusion, with the same route of administration and dose for both, in one
patient. The subject in their study had worsening of depressive symptoms 2 days after the
second infusion, while after the first dosage the patient had presented a response sustained for
7 days. This data suggests that individual differences may influence mood responses to
repeated doses of ketamine.
According to Phelps et al., 2009 the patient’s positive mood response to ketamine might be
related to her family history of alcoholism, affecting 2 of her second-degree relatives. In the
abovementioned study, ketamine response was compared between 2 groups of depressed
subjects, one with family histories of alcoholism and the second without. Their results suggest
that a family history of alcohol dependence may be a marker for mood response to an NMDA
antagonist but, as this was the first study analyzing family history of alcohol dependence in
patients with MDD, it requires confirmation.
Administration by IM injection may have benefits when compared to IV infusion, such as:
• faster administration,
• less discomfort to patients,
• reduced costs, without the need of a pump for the infusion.
These aspects, together with her positive outcome, support the use of IM injections in future
research.
7.4 Conclusions
The use of a 1 mg/kg IM dose was well tolerated and achieved remission of depressive
symptoms. The optimal dose for the treatment of MDD has not yet been established (Glue et
al., 2011), and further data are required to define this. Considering that standard oral
antidepressants have a delay in their response of usually 4 to 6 weeks, these findings may
justify the use of IM ketamine as an antidepressant agent for a population with a short life
expectancy, as described in this case report. Also, this case illustrates the potential for
repeated use of ketamine, with maintenance of response and no complications during the
treatment. Future research is also needed to clarify the role of ketamine as a long-term
treatment option.
!
!
!

! =D!
CHAPTER 8!
!
!
Conclusions!!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
! =@!
8.1 Conclusions!
Ketamine, administered intramuscularly in a dose of 1mg/kg was effective as an
antidepressant agent. In the patient presented in this thesis, there was an improvement in
mood within 1 hour post-injection, which was maintained for up to one week, consistent with
results from published data from RCTs and case reports/ case series (Chapter 5).
!
Although most studies used intravenous administration of ketamine, intramuscular injections
have also been used successfully. This route of administration was chosen due to its simpler
and more convenient administration, with no need of an infusion pump. This choice made its
administration easy and well accepted by the patient. Side effects, such as depersonalization,
dizziness, and elevation in blood pressure, were reported, but none of them required treatment
in the previous studies reviewed in this thesis, nor in the case report presented here. Also, side
effects disappeared within two hours post-administration. This indicates that ketamine
administration should be done in a hospital, but patients might be safely discharged after side
effects are gone and vital signs are stable. The patient’s antidepressant response was
consistent after repeated injections, with no evidence of tolerance. Although this may be an
inconvenient treatment method for long term use, the observation that tolerance was not
developed means that long-term use can be considered if no other treatments are effective or
tolerated. The positive outcome with injections on a weekly basis, with maintenance of
remission of symptoms (which means the patient did not meet criteria for MDD with
continuous injections) is very promising.!
!
Although other studies must be done in this population, the promising results for ketamine has
indicate that it can be a useful medication for terminal cancer patients with depression. One
unexpected finding from this thesis was the very limited number of high quality treatment
trials from depression in cancer patients (Chapter 3). Potentially, the availability of a new
drug treatment may stimulate research in this area. For patients with terminal cancer, time is
probably the most pressing factor when they have depressive episodes, as current
antidepressant treatments take a relatively long time for therapeutic effect to occur. Then, a
fast acting antidepressant would be important to improve quality of life in terminal cancer
individuals with depression, and provide their family more positive memories after their loved
ones are gone. !
!
!
!

! ="!
CHAPTER 9
References
! =#!
9.1 References
1- aan het Rot M, Collins KA, Murrough JW, Perez AM, Reich DL, Charney DS,
Mathew SJ: Safety and efficacy of repeated-dose intravenous ketamine for treatment-resistant
depression. Biol Psychiatry 2010;67:139-145.
2- Abbass A, Driessen E: The efficacy of short-term psychodynamic psychotherapy for
depression: a summary of recent findings. Acta Psychiatr Scand 2010;121:398-399.
3- Abbott NJ, Rönnbäck L, Hansson E: Astrcyte-endothelial interactions at the blood-
brain barrier. 2006;7:41-53.
4- Akechi T, Okuyama T, Onishi J, Morita T, Furukawa TA: Psychotherapy for
depression among incurable cancer patients. Cochrane Database Syst Rev 2008 [in press].
5- Akechi T, Okuyama T, Sugawara Y, Nakano T, Shima Y, Uchitomi Y: Major
depression, adjustment disorders, and post-traumatic stress disorder in terminally ill cancer
patients: associated and predictive factors. J Clin Oncol 2004;22:1957-1965.
6- American Psychiatric Association (1980). Diagnostic and statistical manual of mental
disorders (3rd ed). Washington, DC: Author.
7- American Psychiatric Association (1987). Diagnostic and statistical manual of mental
disorders (3rd ed., Revised). Washington, DC: Author.
8- American Psychiatric Association (2000). Diagnostic and statistical manual of mental
disorders (4th ed., Text Revision). Washington, DC: Author.
9- Amsterdam JD, Shults J: Efficacy and mood conversion rate of short-term fluoxetine
monotherapy of bipolar II major depressive episode. J Clin Psychopharmacol 2010;30:306-
311.
10- Amsterdam JD, Shults J: MAOI efficacy and safety in advanced stage treatment-
resistant depression: a retrospective study. J Affect Disord 2005;89:183-188.
11- Anderson IM, Parry-Billings M, Newsholme EA, Poortmans JR, Cowen PJ:
Decreased plasma tryptophan concentration in major depression: relationship to melancholia
and weight loss. J Affect Disord 1990;20:185-191.
12- Anderson JL: The immune system and major depression. Adv Neuroimmunol
1996;6:119-129.
13- Ayuso-Mateos JL: Global burden of bipolar disorder in the year 2000. Global Program
on Evidence for Health Policy. World Health Organization 2006. In
www.who.int/healthinfo/statistics/bod_bipolar.pdf Accessed on 03 January 2012.
14- Baeken C, De Raedt R: Neurobiological mechanisms of repetitive transcranial
magnetic stimulation on the underlying neurocircuitry in unipolar depression. Dialogues Clin
Neurosci 2011;13:139-145.

! =A!
15- Bailine S, Fink M, Knapp R, Petrides G, Hussain MM, Rasmussen K, Sampson S,
Mueller M, McClintock SM, Tobias KG, Kellner CH: Electroconvulsive therapy is equally
effective in unipolar and bipolar depression. Acta Psychiatr Scand 2010;121:431-436.
16- Bair MJ, Robinson RL, Katon W, Kroenke K: Depression and pain comorbidity: a
literature review. Arch Intern Med 2003;163:2433-2445.
17- Bar-Sela G, Atid L, Danos S, Gabay N, Epelbaum R: Art therapy improved depression
and influenced fatigue levels in cancer patients on chemotherapy. Psychooncology
2007;16:980-984.
18- Bell E, Mathieu G, Racine E: Preparing the ethical future of deep brain stimulation.
Surg Neurol 2009;72:577-786.
19- Berman RM, Cappiello A, Anand A, Oren DA, Heninger GR, Charney DS, Krystal
JH: Antidepressant effects of ketamine in depressed patients. Biol Psychiatry 2000;47:351-
354.
20- Berrettini WH, Nurnberger Jr JI, Hare TA, Simmons-Alling S, Gershon ES, Post RM:
Reduced plasma and CSF gamma-aminobutyric acid in affective illness: effect of lithium
carbonate. Biol Psychiatry 1983;18:185-194.
21- Berridge CW, Waterhouse BD: The locus coeruleus-noradrenergic system:
modulation of behavioral state and state-dependent cognitive process. Brain Res Rev
2003;42:33-84.
22- Bijl RV, Ravelli A: Psychiatric morbidity, service use, and need for care in the general
population: results of The Netherlands Mental Health Survey and Incidence Study. Am J
Public Health 2000;90:602-607.
23- Bjelland I, Dahl AA, Haug TT, Neckelmann D: The validity of the Hospital Anxiety
and Depression Scale. An updated literature review. J Psychosom Res 2002;52:69-77.
24- Black DW, Winokur G, Nasrallah A: Mortality in patients with primary unipolar
depression, secondary unipolar depression, and bipolar affective disorder: a comparison with
general population mortality. Int J Psychiatry Med 1987;17:351-360.
25- Blomstedt P, Sjöberg RL, Hansson M, Bodlund O, Hariz MI: Deep brain stimulation
in the treatment of depression. Acta Psychiatr Scand 2011;123:4-11.
26- Bonanno FG: Ketamine in war/ tropical surgery (a final tribute to the racemic
mixture). Injury 2002;33:323-327.
27- Bos J: The rise and decline of character: humoral psychology in ancient and early
modern medical theory. Hist Human Sci 2009;22:1-27.
! ==!
28- Bosmans JE, de Bruijne MC, de Boer MR, van Hout H, van Steenwijk P, van Tulder
MW: Health care costs of depression in primary care patients in The Netherlands. Fam Pract
2010;27:542-548.
29- Boulenger JP, Hermes A, Huusom AK, Weiller E: Baseline anxiety effect on outcome
of SSRI treatment in patients with severe depression: escitalopram vs paroxetine. Curr Med
Res Opin 2010;26:605-614.
30- Boyes AW, Girgis A, D'Este C, Zucca AC: Flourishing or floundering? Prevalence
and correlates of anxiety and depression among a population-based sample of adult cancer
survivors 6months after diagnosis. J Affect Disord 2011;135:184-192.
31- Brambilla P, Perez J, Barale F, Schettini G, Soares JC: GABAergic dysfunction in
mood disorders. Mol Psychiatry 2003;8:721-737.
32- Breen SJ, Baravelli CM, Schofield PE, Jefford M, Yates PM, Aranda SK: Is symptom
burden a predictor of anxiety and depression in patients with cancer about to commence
chemotherapy? Med J Aust. 2009;190:99-104.
33- Britt GC, McCance-Katz EF: A brief overview of the clinical pharmacology of “club
drugs”. Subst Use Misuse 2005;40:1189-1201.
34- Bruera E, Carraro S, Roca E, Barugel M, Chacon R: Double-blind evaluation of the
effects of mazindol on pain, depression, anxiety, appetite, and activity in terminal cancer
patients. Cancer Treat Rep 1986;70:295-298.
35- Byers AL, Yaffe K: Depression and risk of developing dementia. Nat Rev Neurol
2011;7:323-331.
36- Caric D, Kaithackachalil S, Kim J, Nickell PV, Nathan S: A case study of a patient
with a medication-resistant major depression treated with ketamine infusion followed by
pharmacotherapy alone vs combined ECT and pharmacotherapy. J ECT 2007;23:51.
37- Castelli L, Binaschi L, Caldera P, Mussa A, Torta R: Fast screening of depression in
cancer patients: the effectiveness of the HADS. Eur J Cancer Care (Engl) 2011;20:528-533.
38- Chakrabarti I, Giri A, Majumdar K, DE A: An unusual case of thyroid papillary
carcinoma with solitary cerebral metastasis presenting with neurological symptoms. Turk
Patoloji Derg 2011;27:154-156.
39- Chouinard G, Saxena BM, Nair NP, Kutcher SP, Bakish D, Bradwejn J, Kennedy SH,
Sharma V, Remick RA, Kukha-Mohamad SA, et al. A Canadian multicentre placebo-
controlled study of a fixed dose of brofaromine, a reversible selective MAO-A inhibitor, in
the treatment of major depression. J Affect Disord 1994;32:105-114.
40- Coentre R, Barrocas D, Chendo I, Abreu M, Lvy P, Maltez J, Figueira ML:
Electroconvulsive therapy: myths and evidences. Acta Med Port 2009;22:275-280.

! =E!
41- Colleoni M, Mandala M, Peruzzotti G, Robertson C, Bredart A, Goldhirsch A:
Depression and degree of acceptance of adjuvant cytotoxic drugs. Lancet 2000;356:1326-
1327.
42- Coppen AJ: The biochemistry of affective disorders. Br J Psychiatry 1967;113:1237-
1264.
43- Costa D, Mogos I, Toma T: Efficacy and safety of mianserin in the treatment of
depression of women with cancer. Acta Psychiatr Scand Suppl 1985;320:85-92.
44- Cuijpers P, Andersson G, Donker T, van Straten A: Psychological treatment of
depression: results of a series of meta-analyses. Nord J Psychiatry 2011;65:354-3.64.
45- Dadu S, Mishra LS, Agrasal M, Chandola HC: Comparative clinical study of effect of
neostigmine and ketamine for postoperative analgesia. J Indian Med Assoc 2011;109:308-
311.
46- Dagyt" G, Den Boer JA, Trentani A: The cholinergic system and depression. Behav
Brain Res 2011;221:574-582.
47- Daly RW: Before depression: the medieval vice of acedia. Psychiatry 2007;70:30-51.
48- Davison K: Historical aspects of mood disorders. Psychiatry 2009;8:47-51.
49- Dell'osso B, Camuri G, Castellano F, Vecchi V, Benedetti M, Bortolussi S, Altamura
AC: Meta-Review of Metanalytic Studies with Repetitive Transcranial Magnetic Stimulation
(rTMS) for the Treatment of Major Depression. Clin Pract Epidemiol Ment Health
2011;7:167-177.
50- Deng GF, Zheng JP, Wang S, Tian B, Zhang SG: Remifentanil combined with low-
dose ketamine for postoperative analgesia of lower limb fracture: a double-blind, controlled
study. Chin J Traumatol 2009;12:223-227.
51- Denk MC, Rewerts C, Holsboer F, Erhardt-Lehmann A, Turck CW: Monitoring
ketamine treatment response in a depressed patient via peripheral mammalian target of
rapamycin activation. Am J Psychiatry 2011;168:751-752.
52- Diazgranados N, Ibrahim L, Britsche NE, Newberg A, Kronstein P, Khalife S,
Kammerer WA, Quezado Z, Luckenbaugh DA, Salvadore G, Machado-Vieira R, Manji HK,
Zarate CA Jr: A randomized add-on trial of an N-methyl-D-aspartate antagonist in treatment-
resistant bipolar depression. Arch Gen Psychiatry 2010;67:793-802.
53- Dillon P, Copeland J, JansenK: Patterns of use and harms associated with non-medical
ketamine use. Drug Alcohol Depend 2003;69:23-28.
54- Dorr AE, Debonnel G: Effect of vagus nerve stimulation on serotonergic and
noradrenergic transmission. J Pharmacol Exp Ther 2006;318:890-898.
! E:!
55- Duman RS, Li N, Liu RJ, Duric V, Aghajanian G: Signaling pathways underlying the
rapid antidepressant actions of ketamine. Neuropharmacology 2012;62:35-41.
56- Dunlop BW, Nemeroff CB: The role of dopamine in the pathophysiology of
depression. Arch Gen Psychiatry 2007;64:327-337.
57- Dwight-Johnson M, Ell K, Lee P: Can collaborative care address the needs of low-
income latinas with comorbid depression and cancer? Results from a randomized pilot study.
Psychosomatics 2005;46:224-232.
58- Ell K, Xie B, Kapetanovic S, Quinn DI, Lee P, Wells A, Chou C: One-year follow-up
of collaborative depression care for low-income, predominantly Hispanic patients with
cancer. Psychiatr Serv 2011;62:162-170.
59- Ell K, Xie B, Quon B, Quinn DI, Dwight-Johnson M, Lee P: Randomized controlled
trial of collaborative care management of depression among low-income patients with cancer.
J Clin Oncol 2008;26:4488-4496.
60- Evans RL, Connis RT: Comparison of brief group therapies for depressed cancer
patients receiving radiation treatment. Public Health Rep 1995;110:306-311.
61- Feng CY, Chu H, Chen CH, Chang YS, Chen TH, Chou YH, Chang YC, Chou KR:
The Effect of Cognitive Behavioral Group Therapy for Depression: A Meta-Analysis 2000-
2010. Worldviews Evid Based Nurs 2012;9:2-17.
62- Fiedorowicz JG, Palagummi NM, Forman-Hoffman VL, Miller DD, Haynes WG:
Elevated prevalence of obesity metabolic syndrome, and cardiovascular risk factors in bipolar
disorder. Ann Clin Psychiatry 2008;20:131-137.
63- Fitzgerald PB, Daskalakis ZJ: A practical guide to the use of repetitive transcranial
magnetic stimulation in the treatment of depression. Brain Stimul 2011 [in press].
64- Gershon AA, Dannon PN, Grunhaus L: Transcranial magnetic stimulation in the
treatment of depression. Am J Psychiatry 2003;160:835-45.
65- Ghaemi SN: Treatment of rapid-cycling bipolar disorder: are antidepressants mood
destabilizers? Am J Psychiatry 2008;165:300-302.
66- Glue P, Gulati A, Le Nedelec M, Duffull S: Dose and exposure response to Ketamine
in depression. Biol Psychiatry 2011;70:e9-10.
67- Goekoop JG, de Winter RF, Wolterbeek R, van Kempen GM, Wiegant VM: Evidence
of vasopressinergic-noradrenergic mechanisms in depression with above-normal plasma
vasopressin concentration with and without psychotic features. J Psychopharmacol
2011;25:345-352.
68- Goforth HW, Holsinger T: Rapid relief of severe major depressive disorder by the use
of preoperative Ketamine and electroconvulsive therapy. J ECT 2007;23:23-25.

! E<!
69- Goodnick PJ: Bipolar depression: a review of randomized clinical trials. Expert Opin
Pharmacother 2007;8:13-21.
70- Greenberg PE, Stiglin LE, Finkelstein SN, Berndt ER: The economic burden of
depression in 1990. J Clin Psychiatry 1993;54:405-418.
71- Guidi J, Fava GA, Picardi A, Porcelli P, Bellomo A, Grandi S, Grassi L, Pasquini P,
Quartesan R, Rafanelli C, Rigatelli M, Sonino N: Subtyping depression in the medically ill by
cluster analysis. J Affect Disord 2011;132:383-388.
72- Hamilton M: Development of a rating scale for primary depressive illness. Br J Soc
Clin Psychol 1967;6:278-296.
73- Hamani C, Nóbrega JN: Deep brain stimulation in clinical trials and animal models of
depression. Eur J Neurosci 2010;32:1109-1117.
74- Harich, J. The comparative pain scale. In: http://www.tipna.org/info/documents/
ComparativePainScale.htm. Accessed on 10/03/2011.
75- Harro J, Oreland L: Depression as a spreading adjustment disorder of monoaminergic
neurons: a case for primary implication of the locus coeruleus. Brain Res Brain Res Rev
2001;38:79-128.
76- Härter M, Klesse C, Bermejo I, Schneider F, Berger M: Unipolar depression:
diagnostic and therapeutic recommendations from the current S3/National Clinical Practice
Guideline. Dtsch Arztebl Int 2010;107:700-708.
77- Hashimoto K: Emerging role of glutamate in the pathophysiology on major depressive
disorder. Brain Res Rev 2009; 61: 105-123.
78- Hasler G, van der Veen JW, Tumonis T, Meyers N, Shen J, Drevets WC: Reduced
prefrontal glutamate/glutamine and gamma-aminobutyric acid levels in major depression
determined using proton magnetic resonance spectroscopy. Arch Gen Psychiatry
2007;64:193-200.
79- Hawley CJ, Gale TM, Sivakumaran T: Defining remission by cut off score on the
MADRS: selecting the optimal value. J Affect Disord 2002;72:177-184.
80- Holland JC, Romano SJ, Heiligenstein JH, Tepner RG, Wilson MG: A controlled trial
of fluoxetine and desipramine in depressed women with advanced cancer. Psychooncology
1998;7:291-300.
81- Holland PR, Akerman S, Goadsby PJ: Cortical spreading depression-associated
cerebral blood flow changes induced by mechanical stimulation are modulated by AMPA and
GABA receptors. Cephalalgia 2010;30:519-527.
82- Holtzheimer PE 3rd, Mayberg HS: Deep brain stimulation for treatment-resistant
depression. Am J Psychiatry 2010;167:1437-1444.
! E?!
83- Huisman M: King Saul, work-related stress and depression. J Epidemiol Community
Health 2007;61:890.
84- Ibrahim L, Diazgranados N, Luckenbaugh DA, Machado-Vieira R, Baumann J,
Mallinger AG, Zarate CA Jr: Rapid decrease in depressive symptoms with an N-methyl-d-
aspartate antagonist in ECT-resistant major depression. Arch Gen Psychiatry 2010;67:793-
802.
85- Ihmsen H, Geisslinger G, Schuttler J: Stereoselective pharmacokinetics of ketamine:
R(-)-ketamine inhibits the elimination of S(+)-ketamine. Clin Pharmacol Ther 2001;70:431-
438.
86- Irwin SA, Iglewicz A: Oral ketamine for the rapid treatment of depression and anxiety
in patients receiving hospice care. J Palliat Med 2010;13:903-908.
87- Ishak WW, Ha K, Kapitanski N, Bagot K, Fathy H, Swanson B, Vilhauer J, Balayan
K, Bolotaulo NI, Rapaport MH: The impact of psychotherapy, pharmacotherapy, and their
combination on quality of life in depression. Harv Rev Psychiatry 2011;19:277-289.
88- Itoi K, Sugimoto N: The brainstem noradrenergic systems in stress, anxiety and
depression. J Neuroendocrinol 2010;22:355-361.
89- Jakobsen JC: Review: interpersonal psychotherapy is effective as an acute or
maintenance treatment for unipolar depression. Evid Based Ment Health 2011;14:108.
90- Joels M, Baram TZ: The neuro-symphony of stress. Nat Rev Neurosci 2009;10:459-
466.
91- Kahl KG, Greggersen W, Schweiger U, Cordes J, Balijepalli C, Lösch C, Moebus S:
Prevalence of the metabolic syndrome in unipolar major depression. Eur Arch Psychiatry Clin
Neurosci 2011 [in press].
92- Keddie AM: Associations between severe obesity and depression: results from the
National Health and Nutrition Examination Survey, 2005-2006. Prev Chronic Dis 2011;8:57.
93- Keller MB, Lavori PW, Mueller TI, Endicott J, Coryell W, Hirschfeld RM, Shea T:
Time to recovery, chronicity, and levels of psychopathology in major depression. A 5-year
prospective follow-up of 431 subjects. Arch Gen Psychiatry 1992;49:809-816.
94- Keller PA, McCluskey A, Morgan J, O’connor SM: The role of the HPA axis in
psychiatric disorders and CRF antagonists as potential treatments. Arch Pharm (Weinheim)
2006;339:346-355.
95- Kessing L, Andersen P: Does the risk of developing dementia increase with the
number of episodes in patients with depressive disorder and in patients with bipolar disorder?
J Neurol Neurosurg Psychiatry 2004;75:1662-1666.
! ED!
96- Kessler RC, Chiu WT, Demler O, Walters EE: Prevalence, severity and co-morbidity
of twelve-month DSM-IV disorders in the National Comorbidity Survey Replication (NCS-
R). Arch Gen Psychiatry 2005;62:617-627.
97- Ketalar- Medsafe. (date of preparation: 19 July 2010). In
www.medsafe.govt.nz/profs/datasheet/k/ketalarinj.pdf. Assessed on 11 November 2011.
98- Khawam EA, Laurencic G, Malone DA Jr: Side effects of antidepressants: an
overview. Cleve Clin J Med 2006;73:351-353, 356-361.
99- Kissane DW, Wein S, Love A, Lee XQ, Kee PL, Clarke DM: The Demoralization
Scale: a report of its development and preliminary validation. J Palliat Care 2004;20:269-276.
100- Klemm R, Hardie T: Depression in Internet and face-to-face cancer support groups: a
pilot study. Oncol Nurs Forum 2002;29:45-51.
101- Ko GJ, Kim MG, Yu YM, Jo SK, Cho WY, Kim HK: Association between depression
symptoms with inflammation and cardiovascular risk factors in patients undergoing peritoneal
dialysis. Nephron Clin Pract 2010;116:29-35.
102- Koike H, Lijima M, Chaki S: Involvement of the mammalian target of rapamycin
signaling in the antidepressant-like effect of group II metabotropic glutamate receptor
antagonists. 2011;61:1419-1423.
103- Kornstein SG, Li D, Mao Y, Larsson S, Andersen HF, Papakostas GI: Escitalopram
versus SNRI antidepressants in the acute treatment of major depressive disorder: integrative
analysis of four double-blind, randomized clinical trials. CNS Spectr 2009;14:326-333.
104- Kurz K, Schroecksnadel S, Weiss G, Fuchs D: Association between increased
tryptophan degradation and depression in cancer patients. Curr Opin Clin Nutr Metab Care
2011;14:49-56.
105- Kwok RFK, Lin J, Chan MTV, Gin T, Chiu WKY: Preoperative ketamine improves
postoperative analgesia after gynecologic laparoscopic surgery. Anesth Analg 2004;98:1044-
1049.
106- Larkin GL, Beautrais AL: A preliminary naturalistic study of low dose ketamine for
depression and suicide ideation in the emergency department. Int J Neuropsychopharmacol
2011;14:1127-1131.
107- Laskowski K, Stirling A, Mckay WP, Lim HJ: A systematic review of intravenous
ketamine for postoperative analgesia. Can J Anaesth 2011;58:911-923.
108- Lavori PW, Keller MB, Mueller TI, Scheftner W, Fawcett J, Coryell W: Recurrence
after recovery in unipolar MDD: an observational follow-up study of clinical predictors and
somatic treatment as a mediating factor. Int J Methods Psychiatr Res 1994;4:211-229.

! E@!
109- Lee TS: Transient and spontaneously-remitting complex hallucinations in a patient
with melanoma and brain metastases. 2010;51:267-270.
110- Leonard B, Maes M: Mechanistic explanations how cell-mediated immune activation,
inflammation and oxidative and nitrosative stress pathways and their sequels and
concomitants play a role in the pathophysiology of unipolar depression. Neurosci Biobehav
Rev 2012;36:764-785.
111- Lester L, Braude DA, Niles C, Crandall CS: Low-dose ketamine for analgesia in the
ED: a retrospective case series. Am J Emerg Med 2010;28:820-827.
112- Liebrenz M, Stohler R, Borgeat A: Repeated intravenous ketamine therapy in a patient
with treatment-resistant major depression. World J Biol Psychiatry 2009;10:640-643.
113- Lisanby SH, Maddox JH, Prudic J, Devanand DP, Sackeim HA: The effects of
electroconvulsive therapy on memory of autobiographical and public events. Arch Gen
Psychiatry 2000;57:581-590.
114- Loo CK, McFarquhar TF, Mitchell PB: A review of the safety of repetitive
transcranial magnetic stimulation as a clinical treatment for depression. Int J
Neuropsychopharmacol 2008;11:131-147.
115- Machado-Vieira R, Yuan P, Brutsche N, Diazgranados N, Luckenbaugh D, Manji HK,
Zarate CA Jr: Brain-derived neurotrophic factor and initial antidepressant response to an N-
methyl-D-aspartate antagonist. J Clin Psychiatry 2009;70:1662-1666.
116- Mak SK, Chan MT, Bower WF, Yip SK, Hou SS, Wu BB, Man CY: Lower urinary
tract changes in young adults using ketamine. J Urol 2011;186:610-614.
117- Malone DA Jr: Use of deep brain stimulation in treatment-resistant depression. Cleve
Clin J Med 2010;77:77-80.
118- Markowitz JC, Weissman MM: Interpersonal Psychotherapy: Past, Present and
Future. Clin Psychol Psychother 2012 Feb [in press].
119- Martin JL, Martin-Sanchez E: Systematic review and meta-analysis of vagus nerve
stimulation in the treatment of depression: Variable results based on study designs. Eur
Psychiatry 2012;27:147-155.
120- Mason K, Cottrell AM, Corrigan AG, Gillatt DA, Mitchelmore AE: Ketamine-
associated lower urinary tract destruction: a new radiological challenge. Clin Radiol
2010;65:795-800.
121- Mathers CD, Loncar D: Updated projections of global mortality and burden of disease,
2001- 2030: data sources, methods and results. Evidence and information for policy. World
Health Organization 2005. In

! E"!
http://www.who.int/healthinfo/statistics/bodprojectionspaper.pdf. Accessed on 03 January
2012.
122- Mathew SJ, Murrough JW, aan het Rot M, Collins KA, Reich DL, Charney DS:
Riluzole for relapse prevention following intravenous ketamine in treatment-resistant
depression: a pilot randomized, placebo-controlled continuation trial. Int J
Neuropsychopharmacol 2010 ;13:71-82.
123- Mayberg HS, Liotti M, Brannan SK, McGinnis S, Mahurin RK, Jerabek PA, Silva JA,
Tekell JL, Martin CC, Lancaster JL, Fox PT: Reciprocal limbic-cortical function and negative
mood: converging PET findings in depression and normal sadness. Am J Psychiatry
1999;156:675-682.
124- Mayberg HS, Lozano AM, Voon V, McNeely HE, Seminowicz D, Hamani C,
Schwalb JM, Kennedy SH: Deep brain stimulation for treatment-resistant depression. Neuron
2005;45:651-660.
125- McEwen BS: Stress and hippocampal plasticity. Annu Rev Neurosci 1999;22:105-
122.
126- McEwen BS, Magarinos AM: Stress and hippocampal plasticity: implications for the
pathophysiology of affective disorders. Hum Psychopharmacol 2001;16:7-19.
127- Mercadante S, Porzio G, Gebbia V: Spinal analgesia for advanced cancer patients: An
update. Crit Rev Oncol Hematol 2011;16:in press.
128- Messer MM, Haller IV: Maintenance ketamine treatment produces long-term recovery
from depression. Primary Psychiatry 2010;17:48-50.
129- Messer M, Haller IV, Larson P, Pattison-Crisostomo J, Gessert CE: The use of a series
of ketamine infusions in two patients with treatment-resistant depression. J Neuropsychiatry
Clin Neurosci 2010;22:442-444.
130- Middlemiss DN, Price GW, Watson JM: Serotonergic targets in depression. Curr Opin
Pharmachol 2002;2:18-22.
131- Miller AH, Raison CL: Immune system contributions to the pathophysiology of
depression. FOCUS 2008;6:36-45.
132- Minichino A, Bersani FS, Capra E, Pannese R, Bonanno C, Salviati M, Delle Chiaie
R, Biondi M: ECT, rTMS, and deepTMS in pharmacoresistant drug-free patients with
unipolar depression: a comparative review. Neuropsychiatr Dis Treat 2012;8:55-64.
133- Mitchell AJ: New developments in the detection and treatment of depression in cancer
settings. Prog Neurol Psychiatry 2011;10: in press.
134- Mitchell AJ, Chan M, Bhatti H, Halton M, Grassi L, Johansen C, Meader N:
Prevalence of depression, anxiety, and adjustment disorder in oncological, haematological,
! E#!
and palliative-care settings: a meta-analysis of 94 interview-based studies. Lancet Oncol
2011;12:160-174.
135- Mitchell PB, Malhi GS: Bipolar depression: phenomenological overview and clinical
characteristics. Bipolar Disord 2004;6:530-539.
136- Mohler H: The GABA system in anxiety and depression and its therapeutic potential.
Neuropharmacology 2012;62:42-53.
137- Mongini F, Ciccone G, Ceccarelli M, Baldi I, Ferrero L: Muscle tenderness in
different types of facial pain and its relation to anxiety and depression: A cross-sectional
study on 649 patients. Pain 2007;131:106-111.
138- Montgomery SA, Asberg M: A new depression scale designed to be sensitive to
change. Br J Psychiatry 1979;134:382-389.
139- Montgomery A, Briley M: Noradrenergic symptom cluster in depression.
Neuropsychiatr Dis Treat 2011;7:1-2.
140- Murray CJL, Lopez AD: The global burden of disease: a comprehensive assessment of
mortality and disability from diseases, injuries, and risk factors in 1990 and projected to 2020.
Harvard School of Public Health 1996.
141- Nikish G, Mathe AA: CSF monoamine metabolites and neuropeptides in depressed
patients before and after electroconvulsive therapy. Eur Psychiatry 2008;23:356-359.
142- Noppers I, Niesters M, Swartjes M, Bauer M, Aarts L, Geleijnse N, Mooren R, Dahan
A, Sarton E: Absence of long-term analgesic effect from a short-term S-ketamine infusion on
fibromyalgia pain: a randomized, prospective, double blind, active placebo-controlled trial.
Eur J Pain 2011;15:942-949.
143- Nutt DJ: The role of dopamine and norepinephrine in depression and antidepressant
treatment. J Clin Psychiatry 2006;67:3-8.
144- Nutt D, Demyttenaere K, Janka Z, Aarre T, Bourin M, Canonico PL, Carrasco JL,
Stahl S: The other face of depression, reduced positive affect: the role of catecholamines in
causation and cure. J Psychopharmacol 2007;21:461-471.
145- O’Connor MF, Irwin MR, Seldon J, Kwan L, Ganz PA: Pro-inflammatory cytokines
and depression in a familial cancer registry. Psychooncology 2007;16:499-501.
146- Ohayon MM: Pain sensitivity, depression, and sleep deprivation: Links with
serotoninergic disfunction. J Psychiatr Res 2009;43:1243-1245.
147- Oken MM, Creech RH, Tormey DC, Horton J, Davis TE, McFadden ET, Carbone PP:
Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol
1982;5:649-655.

! EA!
148- Osby U, Brandt L, Correia N, Ekbom A, Sparén P: Excess mortality in bipolar and
unipolar disorder in Sweden. Arch Gen Psychiatry 2001;58:844-850.
149- Pacchiarotti I, Mazzarini L, Colom F, Sanchez-Moreno J, Girardi P, Kotzalidis GD,
Vieta E: Treatment-resistant bipolar depression: towards a new definition. Acta Psychiatr
Scand 2009;120:429-440.
150- Pacchiarotti I, Valentí M, Bonnin CM, Rosa AR, Murru A, Kotzalidis GD, Nivoli
AM, Sánchez-Moreno J, Vieta E, Colom F: Factors associated with initial treatment response
with antidepressants in bipolar disorder. Eur Neuropsychopharmacol 2011;21:362-369.
151- Paslakis G, Gilles M, Meyer-Lindenberg A, Deuschle M: Oral administration of the
NMDA receptor antagonist S-ketamine as add-on therapy of depression: a case series.
Pharmacopsychiatry 2010;43:33-35.
152- Paul IA, Skolnick P: Glutamate and depression: clinical and preclinical studies. Ann
NY Acad Sci 2003;1003:250-272.
153- Paul R, Schaaff N, Padberg F, Möller HJ, Frodl T: Comparison of racemic ketamine
and S-ketamine in treatment-resistant major depression: report of two cases. World J Biol
Psychiatry 2009;10:241-244.
154- Petty F, Kramer GL, Gullion CM, Rush AJ: Low plasma gamma-aminobutyric acid
levels in male patients with depression. Biol Psychiatry 1992;32:354-363.
155- Petty F, Steinberg J, Kramer GL, Fulton M, Moeller FG: Desipramine does not alter
plasma GABA in patients with major depression. J Affect Disord 1993;29:53-56.
156- Pezzella G, Moslinger-Gehmayr R, Contu A: Treatment of depression in patients with
breast cancer: a comparison between paroxetine and amitriptyline. Breast Cancer Res Treat
2001;70:1-10.
157- Phelps LE, Brutsche N, Moral JR, Luckenbaugh DA, Manji HK, Zarate CA Jr: Family
history of alcohol dependence and initial antidepressant response to an M-methyl-D-aspartate
antagonist. Biol Psychiatry 2009;65:181-184.
158- Pincus HA, Pettit AR: The societal costs of chronic major depression. J Clin
Psychiatry 2001;62:5-9.
159- Popoli M, Yan Z, McEwen BS, Sanacora G: The stressed synapse: the impact of stress
and glucocorticoids on glutamate transmission. Nat Rev Neurosci 2011;13:22-37.
160- Price RB, Nock MK, Charney DS, Mathew SJ: Effects of intravenous ketamine on
explicit and implicit measures of suicidality in treatment-resistant depression. Biol Psychiatry
2009;66:522-526.

! E=!
161- Rayner L, Price A, Evans A, Valsraj K, Hotopf M, Higginson IJ: Antidepressants for
the treatment of depression in palliative care: systematic review and meta-analysis. Palliat
Med 2011;25:36-51.
162- RevMan 5.1. Cochrane Collaboration 2008. In: www.cc-ims.net/RevMan. Accessed
on 19 December 2011.
163- Roscoe JA, Morrow GR, Hickok JT, Mustian KM, Griggs JJ, Matteson SE, Bushunow
P, Qazi R, Smith B: Effect of paroxetine hydrochloride (Paxil ®) on fatigue and depression in
breast cancer patients receiving chemotherapy. Breast Cancer Res Treat 2005;89:243-249.
164- Rudolph RL, Feiger AD: A double-blind, randomized, placebo-controlled trial of
once-daily venlafaxine extended release (XR) and fluoxetine for the treatment of depression. J
Affect Disord 2000;56:171-181.
165- Rush AJ, Trivedi MH, Wisniewski SR, Nierenberg AA, Stewart JW, Warden D,
Niederehe G, Thase ME, Lavori PW, Lebowitz BD, McGrath PJ: Acute and long-term
outcomes in depressed outpatients requiring one or several treatment steps: a STAR*D report.
Am J Psychiatry 2006;163:1905-1917.
166- Sackeim HA, Rush AJ, George MS, Marangell LB, Husain MM, Nahas Z, Johnson
CR, Seidman S, Giller C, Haines S, Simpson RK Jr, Goodman RR: Vagus nerve stimulation
(VNS) for treatment-resistant depression: efficacy, side effects, and predictors of outcome.
Neuropsychopharmacology 2001;25:713-728.
167- Salvadore G, van der Veen JW, Zhang Y, Marenco S, Machado-Vieira R, Baumann J,
Ibrahim LA, Luckenbaugh DA, Shen J, Drevets WC, Zarate CA: An investigation of amino-
acid neurotransmitters as potential predictors of clinical improvement to ketamine in
depression. Int J Neuropsychopharmacol 2011; 1:1-10.
168- Sanacora G, Gueorguieva R, Epperson CN, Wu YT, Appel M, Rothman DL, Krystal
JH, Mason GF: Subtype-specific alterations of gamma-aminobutyric acid and glutamate in
patients with major depression. Arch Gen Psychiatry 2004;61:705-713.
169- Sanacora G, Treccani G, Popoli M: Towards a glutamate hypothesis of depression: An
emerging frontier of neuropsychopharmacology for mood disorders. Neuropharmacology
2012;62:63-77.
170- Santiago-Rodriguez E, Sales-Carmona V, Ramos-Ramirez R: Risk factors for
therapeutic noncompliance of patients with epilepsies. Gac Med Mex 2002;138:241-246.
171- Sara SJ: The locus coeruleus and noradrenergic modulation of cognition. Nat Rev
Neurosci 2009;10:211-223.
! EE!
172- Satyanarayana S, Enns MW, Cox BJ, Sareen J: Prevalence and correlates of chronic
depression in the Canadian community health survey: mental health and well-being. Can J
Psychiatry 2009;54:389-398.
173- Savard J, Simard S, Giguere I, Ivers H, Morin CM, Maunsell E, Gagnon P, Robert J,
Marceau D: Randomized clinical trial on cognitive therapy for depression in women with
metastatic breast cancer: psychological and immunological effects. Palliat Support Care
2006;4:219-237.
174- Schiepers OJ, Wichers MC, Maes M: Citokines and major depression. Prog
Neuropsychopharmacol Biol Psychiatry 2005;29:637-638.
175- Schoeyen HK, Birkenaes AB, Vaaler AE, Auestad BH, Malt UF, Andreassen OA,
Morken G: Bipolar disorder patients have similar levels of education but lower socio-
economic status than the general population. J Affect Disord 2011;129:68-78.
176- Schofield DJ, Kelly SJ, Shrestha RN, Callander EJ, Percival R, Passey ME: How
depression and other mental health problems can affect future living standards of those out of
the labor force. Aging Ment Health 2011;15:654-662.
177- Scott KM, Browne MAO, Wells JE: Prevalence, impairment and severity of 12-month
DSM-IV major depressive episodes in Te Rau Hinengaro: New Zealand Mental Health
Survey 2003/4. Aust N Z Psychiatry 2010;44:750-758.
178- Shahani R, Streutker C, Dickson B, Stewart RJ: Ketamine-associated ulcerative
cystitis: a new clinical entity. Urology 2007;69:810-812.
179- Shopsin B: Enhancement of the antidepressant response to L-tryptophan by a liver
pyrrolase inhibitor: a rational treatment. Neuropsychobiology 1978;4:188-192.
180- Sidor MM, Macqueen GM: Antidepressants for the acute treatment of bipolar
depression: a systematic review and meta-analysis. J Clin Psychiatry 2011;72:156-167.
181- Sih K, Campbell SG, Tallon JM, Magee K, Zed PJ. Ketamine in adult emergency
medicine: controversies and recent advances. Ann Pharmacother. 2011 Dec;45(12):1525-34.
182- Skolnick P, Popik P, Trullas R: Glutamate based antidepressants: 20 years on. Trends
Pharmacol Sci 2009; 30: 563-569.
183- Sofia RD, Harakal JJ: Evaluation of ketamine HCl for anti-depressant activity. Arch
Int Pharmacodyn Ther 1975;214:68-74.
184- Souery D, Serretti A, Calati R, Oswald P, Massat I, Konstantinidis A, Linotte S,
Bollen J, Demyttenaere K, Kasper S, Lecrubier Y, Montgomery S, Zohar J, Mendlewicz J:
Switching antidepressant class does not improve response or remission in treatment-resistant
depression. J Clin Psychopharmacol 2011;31:512-516.
185- Statistics New Zealand. In: www.stats.govt.nz. Accessed on 20 January 2012.
! <::!
186- Stefanczyk-Sapieha L, Oneschuk D, Demas M: Intravenous ketamine “burst” for
refractory depression in a patient with advanced cancer. J Palliat Med 2008;11:1268-1271.
187- Strigo IA, Simmons AN, Matthews SC, Craig AD, Paulus MP: Association of major
depressive disorder with altered functional brain response during anticipation and processing
of heat pain. Arch Gen Psychiatry 2008;65:1275-1284.
188- Strong V, Waters R, Hibberd C, Murray G, Wall L, Walker J, McHugh G, Walker A,
Sharpe M: Management of depression for people with cancer (SmaRT oncology 1): a
randomized trial. Lancet 2008;372:40-48.
189- Tolvon- Medsafe. In www.medsafe.govt.nz/profs/datasheet/t/Tolvontab.pdf. Assessed
on 1 February 2012.
190- Trevino K, McClintock SM, Husain MM: A review of continuation electroconvulsive
therapy: application, safety and efficacy. J ECT 2010;26:186-195.
191- Trivedi M, Rush AJ, Wisniewski SR, Nierenberg AA, Warden D, Ritz L, Norquist G,
Howland RH, Lebowitz B, McGrath PJ, Shores-Wilson K, Biggs MM, Balasubramani GK,
Fava M: Evaluation of outcomes with citalopram for depression using measurement-based
care in STAR*D: implications for clinical practice. Am J Psych 2006;163:28-40.
192- Trivedi RB, Nieuwsma JA, Williams JW Jr: Examination of the utility of
psychotherapy for patients with treatment resistant depression: a systematic review. J Gen
Intern Med 2011;26:643-650.
193- UK ECT Review group: Efficacy and safety of electroconvulsive therapy in
depressive disorders: a systematic review and meta-analysis. Lancet 2003;361:799-808.
194- Ustün TB, Ayuso-Mateos JL, Chatterji S, Mathers C, Murray CJ: Global burden of
depressive disorders in the year 2000. Br J Psychiatry 2004;184:386-392.
195- Valentine GW, Mason GF, Gomez R, Fasula M, Watzl J, Pittman B, Krystal JH,
Sanacora G: The antidepressant effect of ketamine is not associated with changes in occipital
amino acid neurotransmitter content as measured by [(1)H]-MRS. Psychiatry Res
2011;191:122-127.
196- van Calker D, Zobel I, Dykierek P, Deimel CM, Kech S, Lieb K, Berger M, Schramm
E: Time course of response to antidepressants: predictive value of early improvement and
effect of additional psychotherapy. J Affect Disord 2009;114:243-253.
197- van Den Eede F, Claes S: Mechanisms of depression: role of the HPA axis. Drug
Discov Today Dis Mech 2004;1:413-418.
198- van Heeringen K, Zivkov M: Pharmacological treatment of depression in cancer
patients. A placebo-controlled study of mianserin. Br J Psychiatry 1996;169:440-443.

! <:<!
199- Wassermann EM: Side effects of repetitive transcranial magnetic stimulation. Depress
Anxiety 2000;12:124-129.
200- Waters SJ, Keefe FJ, Strauman TJ: Self-discrepancy in chronic low back pain: relation
to pain, depression, and psychological distress. J Pain Symptom Manage 2004 Mar;27:251-9.
201- Weilburg JB: An overview of SSRI and SNRI therapies for depression. Manag care
2004;13:25-33.
202- Weiner M, Warren L, Fiedorowicz JG: Cardiovascular morbidity and mortality in
bipolar disorder. Ann Clin Psychiatry 2011;23:40-47.
203- White PF, Schüttler J, Shafer A, Stanski DR, Horai Y, Trevor AJ: Comparative
pharmacology of the ketamine isomers. Studies in volunteers. Br J Anaesth 1985;57:197-203.
204- White VM, Macvean ML, Grogan S, D'Este C, Akkerman D, Ieropoli S, Hill DJ,
Sanson-Fisher R: Can a tailored telephone intervention delivered by volunteers reduce the
supportive care needs, anxiety and depression of people with colorectal cancer? A randomised
controlled trial. Psychooncology 2011 [in press].
205- Williams JBW: A structured interview guide for the Hamilton Depression Rating
Scale. Arch Gen Psychiatry 1988;45:742-747.
206- Williams S, Dale J: The effectiveness of treatment for depression/depressive
symptoms in adults with cancer: a systematic review. Br J Cancer 2006;94:372-390.
207- World Health Statistics 2007.
www.who.int/entity/whosis/whostat2007_10highlights.pdf. Assessed on 22 November 2011.
208- Yan XY, Huang SM, Huang CQ, Wu WH,Qin Y: Marital status and risk for late life
depression: a meta-analysis of the published literature. J Int Med Res 2011;39:1142-1154.
209- Yirmiya R, Weidenfeld J, Pollak Y, Morag M, Morag A, Avitsur R, Barak O,
Reichenberg A, Cohen E, Shavit Y, Ovadia H: Cytokines, "depression due to a general
medical condition," and antidepressant drugs. Adv Exp Med Biol 1999;461:283-316.
210- Young SN, Smith SE, Pihl RO, Ervin FR: Tryptophan depletion causes a rapid
lowering of mood in normal males. Psychopharmacology 1985;87:173-177.
211- Zarate CA Jr, Singh JB, Carlson PJ, Brutsche NE, Ameli R, Luckenbaugh DA,
Charney DS, Manji H: A randomized trial of an N-methyl-D-aspartate antagonist in
treatment-resistant major depression. Arch Gen Psychiatry 2006;63:856-864.
212- Zarate C Jr, Machado-Vieira R, HenterI, Ibrahim L, Diazgranados N, Salvadore G:
Glutamatergic modulators: the future of treating mood disorders? Harv Rev Psychiatry
2010;18:293-303.
213- Zigmond AS, Snaith RP: The hospital anxiety and depression scale. Acta Psychiatr
Scand 1983;67:361-370.

! <:?!
214- Zimmerman M, Posternak MA, Chelminski I: Derivation of a definition of remission
on the Montgomery-Asberg depression rating scale corresponding to the definition of
remission on the Hamilton rating scale for depression. J Psychiatr Res 2004;38:577-582.
215- Zink M, Vollmayr B, Gebicke-Haerter PJ, Henn FA: Reduced expression of GABA
transporter GAT3 in helpless rats, an animal model of depression. Neurochem Res
2009;34:1584-1593.
! <:D!
Appendix I
Informed consent

5%7&2.6%'.,!()!$%/8*8'%!&'/!V,1*+(-(K8*&-!$%/8*8'%I!Y'8L%2,8.1!()!N.&K(!
!
Rapid depression treatment in cancer patients/Information Sheet, Consent Form Ver 20/12/10
!
RAPID DEPRESSION TREATMENT IN PATIENTS WITH CANCER– INFORMATION SHEET FOR INTERESTED INDIVIDUALS
#
P+&'J! 1(0! )(2! ,+(H8'K! &'! 8'.%2%,.! 8'! .+8,! 72(Z%*.M! V-%&,%! 2%&/! .+8,! 8')(26&.8('! ,+%%.!
*&2%)0--1! G%)(2%! /%*8/8'K! H+%.+%2! (2! '(.! 8.! 8,! &772(728&.%! )(2! 1(0! .(! .&J%! 7&2.M! [(02!
7&2.8*87&.8('! 8,!%'.82%-1!L(-0'.&21M! Q)! 1(0!/%*8/%!'(.! .(! .&J%!7&2.I! 8.!H8--!'(.!&))%*.!&'1!
)0.02%! *&2%! (2! .2%&.6%'.M! Q)! 1(0! /(! &K2%%! .(! .&J%! 7&2.! 8'! .+%! ,.0/1I! 1(0! &2%! )2%%! .(!
H8.+/2&H!&.!&'1!.86%!H8.+(0.!+&L8'K!.(!K8L%!&!2%&,('!&'/!.+8,!H8--!8'!'(!H&1!&))%*.!&'1!
)0.02%!+%&-.+!*&2%M!P+%!)(--(H8'K!,+%%.!%\7-&8',!H+&.!.+%!,.0/1!H8--!8'L(-L%M!!
V-%&,%!2%&/!.+%!8')(26&.8('!8'!.+%!2%,.!()!.+8,!8')(26&.8('!,+%%.!*&2%)0--1M!
!
8690#12#06'#%1.#-4#06'#:)-;'<0=#
Rates of depression in patients with terminal cancer are high - up to 70% have clinically significant symptoms of depression, and up to 25% may meet criteria for major depression. Although antidepressant drugs can be effective in patients with terminal cancer, they are slow to work (there can be a delay of up to 6-8 weeks between starting dosing and mood improvement), and are therefore not that helpful to patients needing rapid relief. Having an antidepressant that lifts mood fast might be very helpful, especially to improve quality of life for patients with cancer and their families. Low doses of ketamine, a drug that blocks the brain chemical glutamate, can improve symptoms of depression rapidly (within 2 hours), for up to 7 days (see Figure). This effect can be sustained by use of repeated doses. Ketamine is commonly used to treat pain. The doses we plan to use in this study are similar to doses used for treating pain, and are safe and well tolerated. Ketamine has been used extensively in man for over 40 years. Ketamine was originally developed as an anaesthetic drug, and is also commonly used to treat pain. The doses used for anaesthesia are about 10 times greater that the doses used for treating pain. The doses we plan to use in this study are similar to those used to treat pain. We have local experience with ketamine in major depression and can report similar positive outcomes to those described above. !
]%!7-&'!.(!.%,.!.+%!&'.8/%72%,,&'.!%))%*.,!()!J%.&68'%!8'!D!,.&K%,U!!
C.&K%!<U!V&2.8*87&'.,!H8--!2%*%8L%!&!,8'K-%!8'.2&60,*0-&2!8'Z%*.8('!()!J%.&68'%!9<6K^JK>M!
]%!H8--!&,,%,,!*+&'K%,!8'!1(02!6((/!(L%2!.+%!'%\.!A!/&1,!
!
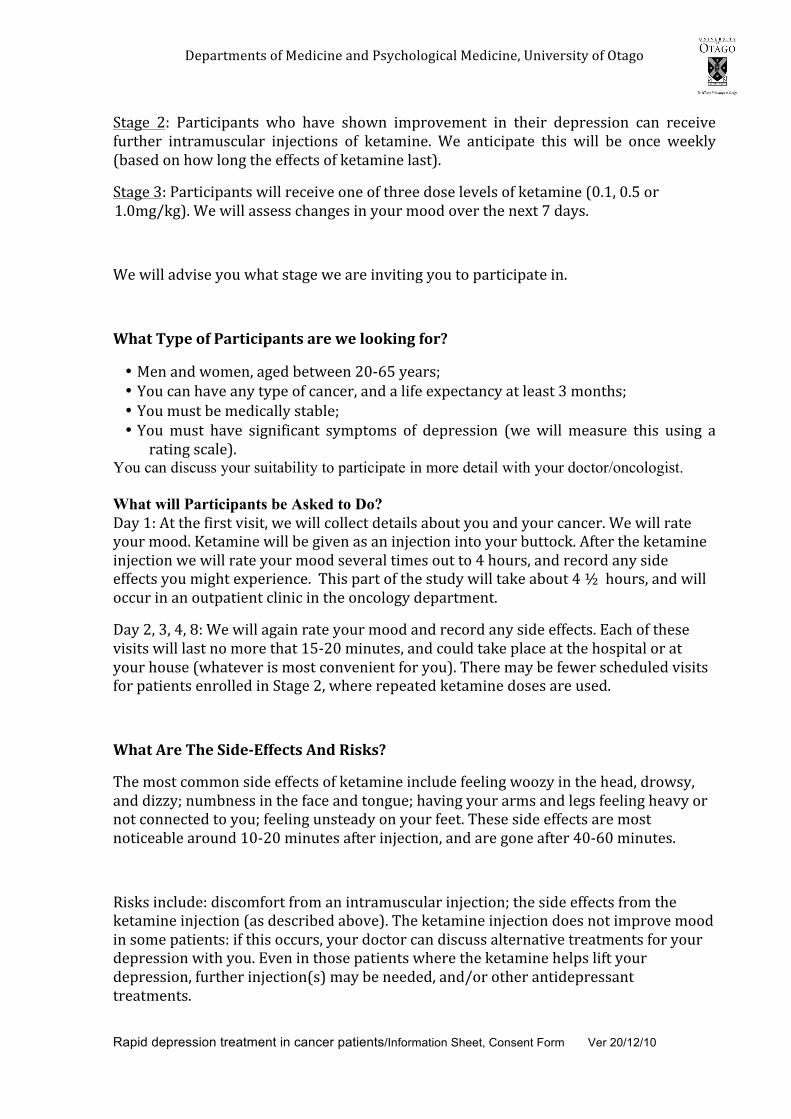
5%7&2.6%'.,!()!$%/8*8'%!&'/!V,1*+(-(K8*&-!$%/8*8'%I!Y'8L%2,8.1!()!N.&K(!
!
Rapid depression treatment in cancer patients/Information Sheet, Consent Form Ver 20/12/10
!
!
C.&K%! ?U! V&2.8*87&'.,! H+(! +&L%! ,+(H'! 8672(L%6%'.! 8'! .+%82! /%72%,,8('! *&'! 2%*%8L%!
)02.+%2! 8'.2&60,*0-&2! 8'Z%*.8(',! ()! J%.&68'%M! ]%! &'.8*87&.%! .+8,! H8--! G%! ('*%! H%%J-1!
9G&,%/!('!+(H!-('K!.+%!%))%*.,!()!J%.&68'%!-&,.>M!
C.&K%!DU!V&2.8*87&'.,!H8--!2%*%8L%!('%!()!.+2%%!/(,%!-%L%-,!()!J%.&68'%!9:M<I!:M"!(2!
<M:6K^JK>M!]%!H8--!&,,%,,!*+&'K%,!8'!1(02!6((/!(L%2!.+%!'%\.!A!/&1,M!
!
]%!H8--!&/L8,%!1(0!H+&.!,.&K%!H%!&2%!8'L8.8'K!1(0!.(!7&2.8*87&.%!8'M!
!
8690#7>?'#-4#:9)01<1?9502#9)'#@'#+--A15B#4-)=#
• $%'!&'/!H(6%'I!&K%/!G%.H%%'!?:;#"!1%&2,_!• [(0!*&'!+&L%!&'1!.17%!()!*&'*%2I!&'/!&!-8)%!%\7%*.&'*1!&.!-%&,.!D!6('.+,_!• [(0!60,.!G%!6%/8*&--1!,.&G-%_!• [(0!60,.! +&L%! ,8K'8)8*&'.! ,167.(6,! ()! /%72%,,8('! 9H%!H8--! 6%&,02%! .+8,! 0,8'K! &!
2&.8'K!,*&-%>M!
You can discuss your suitability to participate in more detail with your doctor/oncologist. What will Participants be Asked to Do? 5&1!<U!4.!.+%!)82,.!L8,8.I!H%!H8--!*(--%*.!/%.&8-,!&G(0.!1(0!&'/!1(02!*&'*%2M!]%!H8--!2&.%!
1(02!6((/M!`%.&68'%!H8--!G%!K8L%'!&,!&'!8'Z%*.8('!8'.(!1(02!G0..(*JM!4).%2!.+%!J%.&68'%!
8'Z%*.8('!H%!H8--!2&.%!1(02!6((/!,%L%2&-!.86%,!(0.!.(!@!+(02,I!&'/!2%*(2/!&'1!,8/%!
%))%*.,!1(0!68K+.!%\7%28%'*%M!!P+8,!7&2.!()!.+%!,.0/1!H8--!.&J%!&G(0.!@!a!!+(02,I!&'/!H8--!
(**02!8'!&'!(0.7&.8%'.!*-8'8*!8'!.+%!('*(-(K1!/%7&2.6%'.M!!
5&1!?I!DI!@I!=U!]%!H8--!&K&8'!2&.%!1(02!6((/!&'/!2%*(2/!&'1!,8/%!%))%*.,M!b&*+!()!.+%,%!
L8,8.,!H8--!-&,.!'(!6(2%!.+&.!<";?:!68'0.%,I!&'/!*(0-/!.&J%!7-&*%!&.!.+%!+(,78.&-!(2!&.!
1(02!+(0,%!9H+&.%L%2!8,!6(,.!*('L%'8%'.!)(2!1(0>M!P+%2%!6&1!G%!)%H%2!,*+%/0-%/!L8,8.,!
)(2!7&.8%'.,!%'2(--%/!8'!C.&K%!?I!H+%2%!2%7%&.%/!J%.&68'%!/(,%,!&2%!0,%/M!!
!
8690#%)'#76'#*1,'/C44'<02#%5,#D12A2=##
P+%!6(,.!*(66('!,8/%!%))%*.,!()!J%.&68'%!8'*-0/%!)%%-8'K!H((c1!8'!.+%!+%&/I!/2(H,1I!
&'/!/8cc1_!'06G'%,,!8'!.+%!)&*%!&'/!.('K0%_!+&L8'K!1(02!&26,!&'/!-%K,!)%%-8'K!+%&L1!(2!
'(.!*(''%*.%/!.(!1(0_!)%%-8'K!0',.%&/1!('!1(02!)%%.M!P+%,%!,8/%!%))%*.,!&2%!6(,.!
'(.8*%&G-%!&2(0'/!<:;?:!68'0.%,!&).%2!8'Z%*.8('I!&'/!&2%!K('%!&).%2!@:;#:!68'0.%,M!
!
B8,J,!8'*-0/%U!/8,*(6)(2.!)2(6!&'!8'.2&60,*0-&2!8'Z%*.8('_!.+%!,8/%!%))%*.,!)2(6!.+%!
J%.&68'%!8'Z%*.8('!9&,!/%,*28G%/!&G(L%>M!P+%!J%.&68'%!8'Z%*.8('!/(%,!'(.!8672(L%!6((/!
8'!,(6%!7&.8%'.,U!8)!.+8,!(**02,I!1(02!/(*.(2!*&'!/8,*0,,!&-.%2'&.8L%!.2%&.6%'.,!)(2!1(02!
/%72%,,8('!H8.+!1(0M!bL%'!8'!.+(,%!7&.8%'.,!H+%2%!.+%!J%.&68'%!+%-7,!-8).!1(02!
/%72%,,8('I!)02.+%2!8'Z%*.8('9,>!6&1!G%!'%%/%/I!&'/^(2!(.+%2!&'.8/%72%,,&'.!
.2%&.6%'.,M!

5%7&2.6%'.,!()!$%/8*8'%!&'/!V,1*+(-(K8*&-!$%/8*8'%I!Y'8L%2,8.1!()!N.&K(!
!
Rapid depression treatment in cancer patients/Information Sheet, Consent Form Ver 20/12/10
!
!
81++#E#F'#?91,#4-)#.>#?9)01<1?901-5#-5#0612#?)-;'<0=#
R(M!P+%!G%'%)8.,!H8--!*(6%!)2(6!.+%!.2%&.6%'.!72(L8/%/!G1!.+%!6%/8*8'%!0,%/!8'!.+%!
,.0/1M!
!
81++#10#F'#95>#<-202#4-)#.>#?9)01<1?901-5#-5#0612#?)-;'<0=##
R(M!Q.!H8--!G%!'(!*(,.,!)(2!1(02,%-)!(2!)&68-1!2%K&2/8'K!.+8,!72(Z%*.M!!
!
!95#:9)01<1?9502#!695B'#06'1)#G15,#95,#8106,)9@#4)-.#06'#:)-;'<0=#
[(0!6&1!H8.+/2&H!)2(6!.+8,!72(Z%*.!&.!&'1!.86%!&'/!H8.+(0.!&'1!/8,&/L&'.&K%!()!&'1!
J8'/M!!
!
8690#H909#-)#E54-).901-5#@1++#F'#!-++'<0',#95,#8690#I2'#@1++#F'#G9,'#-4#10=#
]%! &2%! *(--%*.8'K! 8')(26&.8('! &G(0.! *+&'K%,! 8'! 1(02!6((/! &).%2! J%.&68'%I! 8'*-0/8'K!
+(H!T08*J-1! .+8,!(**02,I!&'/!+(H! -('K! 8.! -&,.,! )(2M!]%!H8--! 2%*(2/!&'1!,8/%!%))%*.,!1(0!
2%7(2.I! &'/! (.+%2! ,&)%.1! 6%&,02%,! 9G-((/! 72%,,02%I! %.*>M! ]%! H8--! &'&-1,%! .+8,!
8')(26&.8('!,.&.8,.8*&--1!.(!/%.%268'%!.+%!)(--(H8'KU!!
• +(H!%))%*.8L%!J%.&68'%!8,!&,!&'!&'.8/%72%,,&'.I!!
• +(H!)&,.!8.!H(2J,I!!
• +(H!-('K!.+%!%))%*.,!-&,.!)(2I!&'/!
• H+&.!8,!.+%!G%,.!/(,%!.(!0,%M!
!
P+%!2%,0-.,!H8--!G%!70G-8,+%/!8'!&'!8'.%2'&.8('&-!,*8%'.8)8*!Z(02'&-M!P+%!/&.&!8'*-0/%/!8'!
.+8,!70G-8*&.8('!H8--!8'!'(!H&1!G%!-8'J%/!.(!&'1!,7%*8)8*!7&2.8*87&'.!&'/!1(02!8/%'.8.1!H8--!
'(.!G%!2%*(2/%/!H8.+! .+%!/&.&M! Q)!1(0!H&'.!&**%,,! .(!1(02!7%2,('&-!/&.&! -&.%2!1(0!H8--!
'%%/! .(! 2%*(2/! .+%! 8/%'.8)8*&.8('!'06G%2!0,%/! )(2! 1(02!7&2.8*0-&2! .%,.,M! [(0!&2%!6(,.!
H%-*(6%!.(!2%T0%,.!&!*(71!()!.+%!2%,0-.,!()!.+%!72(Z%*.!,+(0-/!1(0!H8,+M!
!
P+%!/&.&!*(--%*.%/!H8--!G%!,%*02%-1!,.(2%/!8'!,0*+!&!H&1!.+&.!('-1!.+(,%!8'L(-L%/!8'!.+%!
2%,%&2*+!72(K2&6!H8--!G%!&G-%!.(!K&8'!&**%,,!.(!8.M!!4.!.+%!%'/!()!.+%!72(Z%*.!&'1!7%2,('&-!
8')(26&.8('!H8--!G%!/%,.2(1%/!866%/8&.%-1!%\*%7.!.+&.I!&,!2%T082%/!G1!.+%!Y'8L%2,8.1d,!
2%,%&2*+!7(-8*1I!&'1!2&H!/&.&!('!H+8*+!.+%!2%,0-.,!()!.+%!72(Z%*.!/%7%'/!H8--!G%!2%.&8'%/!
8'!,%*02%!,.(2&K%!)(2!.%'!1%&2,I!&).%2!H+8*+!8.!H8--!G%!/%,.2(1%/M!
#
8690#14#>-J#69('#95>#KJ'201-52=#
Q)!1(0!+&L%!&'1!T0%,.8(',!&G(0.!(02!72(Z%*.I!%8.+%2!'(H!(2!8'!.+%!)0.02%I!7-%&,%!)%%-!)2%%!
.(!*('.&*.!0,!L8&!.+%!/%.&8-,!K8L%'!G%-(HM!

5%7&2.6%'.,!()!$%/8*8'%!&'/!V,1*+(-(K8*&-!$%/8*8'%I!Y'8L%2,8.1!()!N.&K(!
!
Rapid depression treatment in cancer patients/Information Sheet, Consent Form Ver 20/12/10
!
!-509<0#H'091+2U!!
V2()%,,(2!V&0-!e-0%I!5%7.!()!V,1*+(-(K8*&-!$%/8*8'%_!.%-!:D!@A:!D=#A_!%6&8-U!
7&0-MK-0%f(.&K(M&*M'c!
4,,(*8&.%!V2()%,,(2!5&L8/!V%2%cI!50'%/8'!V0G-8*!3(,78.&-_!.%-!:D@A@!:EEE_!%6&8-U!
/&L8/M7%2%cf,(0.+%2'/+GMK(L.M'c!
52!W-&0/8&!g&'8*(..8I!5%7.!()!V,1*+(-(K8*&-!$%/8*8'%_!.%-!:D!@A:!E@"<_!%6&8-U!
*-&0/8&K2(..f+(.6&8-M*(6!
%!!#2090'.'50L##
Q'!.+%!0'-8J%-1!%L%'.!()!&!7+1,8*&-!8'Z021!&,!&!2%,0-.!()!1(02!7&2.8*87&.8('!8'!.+8,!,.0/1I!
1(0!H8--!G%!*(L%2%/!G1!.+%!&**8/%'.!*(67%',&.8('!-%K8,-&.8('!H8.+!8.,!-868.&.8(',M!Q)!1(0!
+&L%!&'1!T0%,.8(',!&G(0.!4WW!7-%&,%!)%%-!)2%%!.(!&,J!.+%!2%,%&2*+%2!)(2!6(2%!
8')(26&.8('!G%)(2%!1(0!&K2%%!.(!.&J%!7&2.!8'!.+8,!.28&-M!
!
M'9+06#95,#,129F1+10>#2090'.'50L#
Q)!1(0!+&L%!&'1!T0%28%,!(2!*('*%2',!&G(0.!1(02!28K+.,!&,!&!7&2.8*87&'.!8'!.+8,!,.0/1!1(0!
6&1!H8,+!.(!*('.&*.!&!3%&-.+!&'/!58,&G8-8.1!C%2L8*%,!W(',06%2!4/L(*&.%I!.%-%7+('%U!
9:D>!@AE!:?#"!(2!)2%%7+('%!:=::!DA!AA!##!(2!)2%%)&\!:=::!?A=A!A#A=!9:=::!?!
CYVVNBP>!(2!%6&8-!&/L(*&*1f+/*M(2KM'c!Q)!.+%2%!8,!&!,7%*8)8*!$&(28!8,,0%^*('*%2'!
7-%&,%!*('.&*.!S8'/&!e2%''%--!&.!:=::!DAA!A##M!
!
P+8,!72(Z%*.!+&,!G%%'!2%L8%H%/!&'/!&772(L%/!G1!.+%!S(H%2!C(0.+!B%K8('&-!b.+8*,!
W(668..%%!9SBC^<:^<<^:":>M!

5%7&2.6%'.,!()!$%/8*8'%!&'/!V,1*+(-(K8*&-!$%/8*8'%I!Y'8L%2,8.1!()!N.&K(!
!
Rapid depression treatment in cancer patients/Information Sheet, Consent Form Ver 20/12/10
!
!
RAPID DEPRESSION TREATMENT IN PATIENTS WITH CANCER– #
!3&*C&7#N3DG#N3D#:%D7E!E:%&7*#
#
I have read the “RAPID DEPRESSION TREATMENT IN PATIENTS WITH CANCER” Information Sheet concerning this project. All my questions have been answered to my satisfaction. I understand that I am free to request further information at any stage. !
Q!J'(H!.+&.U!
1. I am free to withdraw from testing at any time without any disadvantage; ?M Q!0'/%2,.&'/!.+%!/&.&!H8--!G%!/%,.2(1%/!&.!.+%!*('*-0,8('!()!.+%!72(Z%*.!G0.!&'1!
2&H!/&.&!('!H+8*+!.+%!2%,0-.,!()!.+%!72(Z%*.!/%7%'/!H8--!G%!2%.&8'%/!8'!,%*02%!
,.(2&K%!)(2!.%'!1%&2,I!&).%2!H+8*+!8.!H8--!G%!/%,.2(1%/_!
3. I understand the results of the project may be published but my anonymity will be preserved.
I agree to take part in this project. ………………………………………………… (Full name) ............................................................................ ............................... (Signature) (Date) ………………………………………………. (Full name) ……………………………………………….. ……………………. (Doctor’s / Researcher Signature) (Date) P+8,!72(Z%*.!+&,!G%%'!2%L8%H%/!&'/!&772(L%/!G1!.+%!S(H%2!C(0.+!B%K8('&-!b.+8*,!W(668..%%!
9SBC^<:^<<^:":

!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
!!
!!!!!<:E!
!
Appendix II
Case report – in press (page proofs)

!
!
Brief Reports
Mood and Pain Responses to Repeat Dose IntramuscularKetamine in a Depressed Patient with Advanced Cancer
Claudia G. Zanicotti, M.D.,1 David Perez, M.D., FRACP,2 and Paul Glue, M.D., FRCPsych1
Abstract
Depression is highly prevalent in patients with advanced cancer, commonly affecting quality of life. Consideringthe response delay with conventional antidepressants and the short life expectancy for these patients, treatmentsfor Major Depressive Disorder (MDD) with faster onset of action are desirable. In this case report, a femalepatient with metastatic ovarian cancer reported rapid and sustained response to intramuscular (IM) injections ofketamine (1mg/kg). Over a course of six treatments, her mood response was identical on each occasion andprovided remission of her depressive symptoms. Pain was also improved, although for a shorter duration. Thesefindings support the use of IM ketamine as a possible antidepressant option for this population.
Introduction
The prevalence ofMajor Depressive Disorder (MDD) inadult patients with cancer is high. In those receiving
palliative care the rate is considered approximately 15%,1,2
and the rate of severe depression in advanced cancer patientsis around 11%.3
Current antidepressants target the monoaminergic systemand typically have a slow onset of action. More recently, therehas been an awareness of the role of the glutamatergic systemin the pathophysiology of mood disorders.4 Ketamine – anoncompetitive NMDA (N-Methyl-D-Aspartate) antagonist –has recently been identified as a possible fast-acting treatmentfor MDD.5,6 Moreover, the use of ketamine for pain in ad-vanced cancer patients might also pose an extra benefit as anadjuvant therapy.7
The following case report describes a patient enrolled inan ongoing clinical trial, which was approved by theLower South Regional Ethics Committee, Southern HealthDistrict Board and Dunedin School of Medicine, Universityof Otago, New Zealand. This trial is registered (ACTRN12610001011077).
The patient participated in Stages 1 and 2 of this trial. Stage1 consists of a single open label injection of IM ketamine 1mg/kg. Patients whose mood improved, with Montgomery-Asberg Depression Rating Scale (MADRS)8 score reduced by50% or more, could proceed to Stage 2. This stage consists ofopen label characterization of safety and efficacy of repeatdose IM ketamine, administered at approximately weeklyintervals.
Inclusion criteria are diagnosis of MDD (DSM IV-TR);9
MADRS > 20; presence of incurable cancer; written informedconsent; life expectancy > 3 months; age between 20 and 65years old; ECOG bAU1status < 4; and adequate hepatic, renal, andhematological function. Exclusion criteria are current use ofketamine; presence of psychosis or delirium; presence of ce-rebral metastases; Comparative Pain Scale10 score of > 5; andany antidepressant treatment started within the previous4 weeks.
Case Report
A. is a 36-year-old female patient with metastatic ovariancarcinoma. She has had MDD and Dysthymic Disorder di-agnosed since she was 18 years old. Even though she has triedvarious antidepressants, the patient reports that her moodwas never completely improved. For the past 10 years she hada worsening of her depressive symptoms, which persisted atthe time of her first assessment, and included low mood, lackof energy, irritability, easy crying, sleep disturbance, lack ofconcentration, excessive feelings of guilt, and passive deathwish. Her domestic circumstances were stressful, due toconcern about the future of her 11-year-old daughter and thelack of support from her ex-boyfriend (the child’s father) andher family.
Along with depression, A. has had visceral pain for *8months in the right iliac fossa, in the same location as a met-astatic tumor, which is about 7cm in diameter on palpation.For pain intensity assessment, The Comparative Pain Scale,10
with a range from 0 (no pain) to 10 (short unconsciousness),
1Department of Psychological Medicine, Dunedin School of Medicine, University of Otago, Dunedin, New Zealand.2Department of Oncology, Dunedin School of Medicine, University of Otago, Dunedin, New Zealand.Accepted: November 18, 2011.
JOURNAL OF PALLIATIVE MEDICINEVolume 15, Number 4, 2012ª Mary Ann Liebert, Inc.DOI: 10.1089/jpm.2011.0314
1
JPM-2011-0314-ver9-Zanicotti_1P.3d 03/26/12 2:04pm Page 1
JPM-2011-0314-ver9-Zanicotti_1P

!
!
was used. She also has a previous history of drug abuse(methamphetamine), being abstinent for more than six years,and a family history of alcoholism (both grandfathers andone uncle).
When first assessed for ketamine treatment, A. was takingvenlafaxine 150mg/day, quetiapine 50mg/day, and metha-done 95mg/day. All her medications were continued duringthe ketamine treatment with doses unchanged. She was alsoreceiving weekly chemotherapy (combination of carboplatinand gemcitabine). After informed consent was given, she re-ceived ketamine 1mg/kg IM open-label. Dosing was per-formed on an outpatient basis in a hospital clinic.
MADRS was used as the main scale to assess her depres-sion scores. This is a validated scale that includes most DSM-IV criteria for MDD.8 It consists of 10 items, each one scoredfrom 0 to 6 (total range from 0 to 60). Scores > 20 are standardfor entry into antidepressant clinical trials.6,11 Mood and painassessments were obtained at baseline (20 minutes before in-jection), 1, 2, 4, 24, 48, 72, and 168 hours post-injection. TheHospital Anxiety and Depression Scale (HADS)12,13 is oftenused in patients with cancer or other somatic diseases, and itsoptimal cut-off scores are > 7 on both HADS-A and HADS-Dfor anxiety and depression respectively. There are no physicalsymptoms in its assessment, lessening the effects of physicalillness over depression and anxiety symptoms.13 The De-moralization Scale (DS)14 consists of 24 questions (total scorerange = 0 to 96), and a score > 30 is considered high. HADSand DS were assessed at baseline and 24 hours.
The patient’s initial MADRS score was 24, which droppedto 7 one hour after the first dose of ketamine. For the next twodays herMADRS remained low (5 points), with improvementin all MADRS scale items. Her depressive symptoms returnedafter 6 to 7 days post-injection. Also, her pain score was re-duced within a few minutes after the first ketamine dose,however returned to baselinewithin 24 hours (F1c Figure 1A). Shereported moderate but tolerable dissociative side effects, suchas depersonalization and immobility, that started 5 minutespost-injection and which resolved within 45 to 60 minutes.Vital signs were unchanged.
The patient has subsequently received repeat ketaminedoses at intervals of 7 to 8 days, based on return of her de-pressive symptoms. Her mood response to repeat injectionshas been identical each time, in terms of speed andmagnitudeof response (Figure 1B). Onset of pain relief continued to berapid, however the durability of analgesic response has beenmuch more variable (Figure 1C). Reported side effects weresimilar in timing of onset and intensity to those noted after thefirst dose. Scores on HADS and DS showed consistent im-provement in her mood symptoms ( bT1Table 1).
The improvement in the patient’s mood was noticed by herfamily, even on the phone while talking to her sister. Also, herdaughter said she was calmer and more patient. In visits toA.’s house to collect mood assessments these reported find-ings were verified.
Discussion
This is the second case report of ketamine being used as afast acting antidepressant in patients with cancer.15 Thepresent report extends information on ketamine use by as-sessing simultaneous effects on mood and pain ratings, andby demonstrating the reproducibility of the antidepressantresponse with repeated dosing.
The patient had remission of her depressive symptomswithin one hour after receiving the first injection of IM keta-mine (MADRS < 10).16 This is consistent with previous re-search that noted a rapidmood response for more than 70% ofpatients within 24 hours.17,18 The patient’s improvement wassustained for 6 to 7 days, with a gradual return to baseline inher depression scores, which is also consistent with the liter-ature.18,19 Some authors have noticed that there are patientswith a mood response sustained for even longer periods oftime.18,20 Most previous studies have used an IV infusion over40 minutes rather than IM injections, as used in this case.Pharmacokinetic simulations suggest comparable exposuresafter IM injection and IV infusion.21 The dose used in this case(1mg/kg) is higher than the dose used in most publishedcases (0.5mg/kg),17,18,19 and the optimal dose for treating
FIG. 1A. Change in depression ratings (!) and pain score (r) after first dose of IM ketamine. 1B: Reproducible changes indepression ratings after repeated ketamine administration - doses 1(!), 2(;), 3(-), 4(r), 5(:), 6( ). 1C: Variable changes inpain ratings after repeated administration (legend as for 1(B)). 1D: Correlation of change from baseline in MADRS and painratings (Pearson’s r) by time post dose.
JPM-2011-0314-ver9-Zanicotti_1P.3d 03/26/12 2:04pm Page 2
2 ZANICOTTI ET AL.

!
!
depression is still unclear. Changes in the DS and HADSratings were consistent with the MADRS data.
The analgesic effects were also fast in onset, however thedurability was variable after day one. Changes in pain scoresand depression ratings were most closely correlated 1 hourpost-dosing (Pearson’s r = 0.61) with progressively weakercorrelations over the next 168 hours (Figure 1D). This suggeststhat the sustained antidepressant effects of ketamine are me-diated differently from the mechanisms associated with im-mediate changes in pain and mood. One possible mechanismmay be via stimulation of mTOR signaling and via synapticprotein synthesis.22
Our patient had no tachyphylaxis, as demonstrated by theconsistent improvement in her mood scores at every injection.Messer and colleagues20 reported similar findings, withmaintenance of remission in one patient for more than 15months, with ketamine infusions given every three weeks. Itshould be noted that Liebrenz and colleagues23 reported adifferent response to a second ketamine infusion in one pa-tient, with worsening of depressive symptoms two days aftera second injection. This suggests that there may be individualdifferences in mood responses to repeated doses of ketamine.
According to Phelps and colleagues,24 the patient’s positivemood response might be related to her family history of al-coholism, affecting two of her second-degree relatives. In theabove mentioned study the authors compared ketamine re-sponse in two groups of depressed patients, one with familyhistories of alcoholism and the second without. Their resultssuggest that a family history of alcohol dependence may be amarker for mood response to an NMDA antagonist but, asthis was the first study with depressed patients, it requiresfurther studies for confirmation.
Administration by IM injection may have benefits whencompared to IV infusion, such as faster administration, withless discomfort to the patient; and reduced costs, without theneed of a pump for the infusion. These aspects, together withher positive outcome, support the use of IM injections in fu-ture research.
The use of a 1mg/kg IM dose was well tolerated andachieved remission of MDD. However, the optimal dose hasnot yet been established.21 Further data are required to de-termine optimal use of ketamine as a fast-acting antidepres-
sant. Considering that antidepressants available today have adelay in their response of usually 4 to 6 weeks, these findingsmay justify the use of IM ketamine as an antidepressant agentfor a population with a short life expectancy, as described inthis case report.
Acknowledgments
This research was supported by Otago Medical ResearchFoundation Inc. and the Otago Community Trust.
Authors Disclosure Statement
All authors state no competing financial interests exist.
References
1. Hotopf M, Chidgey J, Addington-Hall J, Ly KL: Depressionin advanced disease: A systematic review. Part 1. Prevalenceand case finding. J Palliat Med 2002;16:81–97.
2. Mitchell AJ, Chan M, Bhatti H, Halton M, Grassi L, JohansenC, Meader N: Prevalence of depression, anxiety, and ad-justment disorder in oncological, haematological, andpalliative-care settings: A meta-analysis of 94 interview-based studies. Lancet Oncol 2011;12:160–174.
3. Salvo N, Zeng L, Zhang L, Leung M, Khan L, Presutti R,Nguyen J, Holden L, Culleton S, Chow E: Frequency of re-porting and predictive factors for anxiety and depression inpatients with advanced cancer. Clin Oncol (R Coll Radiol)2011;6:in press.
4. Hashimoto K: Emerging role of glutamate in the patho-physiology of major depressive disorder. Brain Res Rev2009;61:105–123.
5. Zarate C Jr, Machado-Vieira R, Henter I, Ibrahim L, Dia-zgranados N, Salvadore G: Glutamatergic modulators: Thefuture of treating mood disorders? Harv Rev Psychiatry2010;18:293–303.
6. Machado-Vieira R, Yuan P, Brutsche N, Diazgranados N,Luckenbaugh D, Manji HK, Zarate CA Jr: Brain-derivedneurotrophic factor and initial antidepressant response to anN-methyl-D-aspartate antagonist. J Clin Psychiatry 2009;70:1662–1666.
7. Mercadante S, Porzio G, Gebbia V: Spinal analgesia for ad-vanced cancer patients: An update. Crit Rev Oncol Hematol2011;16:in press.
8. Montgomery SA, Asberg M: A new depression scale de-signed to be sensitive to change. Br J Psychiatry 1979;134:382–389.
9. American Psychiatric Association: Diagnostic and StatisticalManual of Mental Disorders (4th ed). Washington, DC,2000..
10. Harich, J: The comparative pain scale. www.tipna.org/info/documents/ComparativePainScale.htm. (Last acessed 10/03/2011.)
11. Diazgranados N, Ibrahim L, Brutsche NE, Newberg A,Kronstein P, Khalife S, Kammerer WA, Quezado Z, Luck-enbaugh DA, Salvadore G, Machado-Vieira R, Manji HK,Zarate CA Jr: A randomized add-on trial of an N-methyl-D-aspartate antagonist in treatment-resistant bipolar depres-sion. Arch Gen Psychiatry 2010;67:793–802.
12. Bjelland I, Dahl AA, Haug TT, Neckelmann D: The validityof the Hospital Anxiety and Depression Scale. An updatedliterature review. J Psychosom Res 2002;52:69–77.
13. Zigmond AS, Snaith RP: The hospital anxiety and depres-sion scale. Acta Psychiatr Scand 1983;67:361–370.
Table 1: Assessment of HADSand Demoralization Scale
Dose Assessments Baseline24 hours
post-injection
Dose 1 HADS 23 (D:14 A:9) 5 (D:3 A:2)DS 71 29
Dose 2 HADS 27 (D:17 A:10) 4 (D:2 A:2)DS 78 28
Dose 3 HADS 25 (D:18 A:7) 3 (D:2 A:1)DS 77 28
Dose 4 HADS 23 (D:15 A:8) 6 (D:6 A:0)DS 82 32
Dose 5 HADS 22 (D:16 A:6) 8 (D:6 A:2)DS 77 35
Dose 6 HADS 26 (D:15 A:11) 6 (D:5 A:1)DS 78 26
DS, Demoralization Scale; D, HADS depression scores; A, HADSanxiety scores.
JPM-2011-0314-ver9-Zanicotti_1P.3d 03/26/12 2:04pm Page 3
KETAMINE FOR DEPRESSION IN A CANCER PATIENT 3

!
!
14. Kissane DW, Wein S, Love A, Lee XQ, Kee PL, Clarke DM:The Demoralization Scale: A report of its development andpreliminary validation. J Palliat Care 2004;20:269–276.
15. Stefanczyk-Sapieha L, Oneschuk D, Demas M: Intravenousketamine ‘‘burst’’ for refractory depression in a patient withadvanced cancer. J Palliat Med 2008;11:1268–1271.
16. Hawley CJ, Gale TM, Sivakumaran T: Defining remission bycut off score on the MADRS: Selecting the optimal value. JAffect Disord 2002;72:177–184.
17. Zarate CA Jr, Singh JB, Carlson PJ, Brutsche NE, Ameli R,Luckenbaugh DA, Charney DS, Manji HK: A randomized trialof an N-methyl-D-aspartate antagonist in treatment-resistantmajor depression. Arch Gen Psychiatry 2006;63:856–864.
18. Aan het Rot M, Collins KA, Murrough JW, Perez AM, ReichDL, Charney DS, Mathew SJ: Safety and efficacy of repeated-dose intravenous ketamine for treatment-resistant depres-sion. Biol Psychiatry 2010;67:139–145.
19. Berman RM, Cappiello A, Anand A, Oren DA, Heninger GR,Charney DS, Krystal JH: Antidepressant effects of ketaminein depressed patients. Biol Psychiatry 2000;47:351–354.
20. Messer MM, Haller IV: Maintenance ketamine treatment pro-duces long-term recovery from depression. Primary Psychiatry2010;17:48–50.
21. Glue P, Gulati A, Le Nedelec M, Duffull F: Dose- andexposure-response to ketamine in depression. Biol Psy-chiatry 2011;7:in press.
22. Duman RS, Li N, Liu RJ, Duric V, Aghajanian G: Signalingpathways underlying the rapid antidepressan actions ofketamine. Neuropharmacology 2012;62:35–41.
23. Liebrenz M, Stohler R, Borgeat A: Repeated intravenousketamine therapy in a patient with treatment-resistant majordepression. World J Biol Psychiatry 2009;10:640–643.
24. Phelps LE, Brutsche N, Moral JR, Luckenbaugh DA, ManjiHK, Zarate CA Jr: Family history of alcohol dependence andinitial antidepressant response to an NMDA antagonist. BiolPsychiatry 2009;65:181–184.
Address correspondence to:Claudia Grott Zanicotti
Department of Psychological MedicineUniversity of Otago
PO Box 913Dunedin, New Zealand
E-mail: [email protected]
JPM-2011-0314-ver9-Zanicotti_1P.3d 03/26/12 2:04pm Page 4
4 ZANICOTTI ET AL.