usatf tf level ii coaching education cvphysiologynotes
TRANSCRIPT

1
USA Track and Field Level II Coaching Education: Physiology
Part 2 – Cardiovascular physiology
The opening screen. The ability of the cells to exchange
materials with their immediate environment is an absolute
requirement of life. Oxygen is particularly important – cells rely
in a continuous supply of oxygen for their energy supply. They
do have other means for covering their energy needs in the
absence of oxygen, but as you now know these are rather
inefficient and in the long run they all eventually require support
by mitochondrial ATP production – and this energy production
method demands oxygen. Mitochondria are fundamental
constituents of all living cells beyond bacteria and are specially
designed for the ATP energy production task.
Cells of the body are located far away from the source of oxygen
supply –which is the atmosphere. The process by which a flow of
oxygen to the tissues can be maintained involves a method of first extracting the oxygen from the atmosphere – and this
is done through the lungs, and a way of moving that oxygen to the cells needing it – and this is done by the blood
vessels, the blood and a pumping mechanism – the heart, Fuel supplies are also needed – and, like oxygen has to be
moved from outside the body to the cells located inside the body. Together, the lungs, heart, blood and blood vessels
permit amazing physical feats such as running a marathon. Elite athletes are blessed with lungs, heart, blood vessels and
blood that has an extremely efficient capacity to deliver oxygen and nutrients to working cells. Some of this capacity is
inherited, and some of it is acquired through training.
Probably the most amazing organ we have is the heart. It is a muscular organ whose function it is to generate the force
that propels blood through the blood vessels. It can adjust its pumping capacity depending on the oxygen demands of the
mitochondria located in the working muscle. The relevant structural parameter of the pump is the size of the heart, which
determines the amount of blood pumped with each contraction. On average, the heart is approximately .58% of body
mass and this size holds true over a wide range of mammals from mice to cows. The thickness of the heart muscle is
proportional to the work required. It is interesting to note that maximal beating capacity of the heart is no different
between trained and untrained individuals. However, the heart size can be up to twice as large in elite athletes. When
compared to the non-athlete. It is still unclear though, if these elite athletes have larger hearts to begin with or whether
trainability of their hearts is better.
Click the Start Button: Remember that five physiological
systems work together. So, while we are now going to discuss
the cardiovascular and respiratory systems as if they work
independently, keep in mind that these systems are intricately
linked to the energy needs of the working muscle cells.

2
Go to the next screen: This screen overviews the interaction
between the cardiovascular and respiratory systems. Even the
very mild exercise like walking demands substantial ATP energy
and it is the task of the cardiovascular and respiratory systems to
provide the cells with the oxygen and fuel supplies so that they
can produce their ATP supplies. Let’s just talk about the pathway
for oxygen at the moment. Oxygen enters the lungs from the
atmosphere (A) where it diffuses from the small air sacs in the
lungs called alveoli into the bloodstream (this is depicted as the
white gas). Carbon dioxide diffuses from the bloodstream into the
alveoli – depicted as the purple gas.
The next component of the system is the heart that is actually two
pumps sitting side by side (B). The right pump sends the blood off to the lungs to be oxygenated and for the elimination
of carbon dioxide. The left pump sends the oxygenated blood off to the rest of the body.
Oxygen poor blood returns to the heart after circulating through the body. The right side of the heart is composed of the
right atrium and right ventricle and collects the blood and pumps it to the lungs through the pulmonary arteries. The
lungs refresh the blood with a new supply of oxygen. Oxygen rich blood then enters the left side of the heart that’s
composed of the left atrium and ventricle and is pumped through the aorta to supply the body tissues with oxygen.
Once the circulating blood reaches working tissues oxygen diffuses from the capillaries into the working cells and
carbon dioxide diffuses out of the cell and into the bloodstream where it then travels to the right heart and then to the
lungs. (C). As oxygen enters the cell it goes directly to the mitochondria (D) to the inner membrane where the electron
transport chain is located. Here, the electron transport chain uses the oxygen to resynthesize ATP from ADP and free
phosphate. The ATP is then used by the sarcomere of the muscle cell so that muscle contraction and relaxation can occur
(E). We will come back and talk about how the muscle cell uses ATP in Part 3.
The diagram in the middle also shows the fuel supplies. Fuel enters through the gut as food, is processed into the type of
fuel the cells can use, and whatever is not used right away is stored in the liver and muscle as glycogen and in the fat
cells as triglycerides for future use.
Go to the next screen: This is the module index screen. You
can navigate anywhere in the module by clicking the buttons of
this screen.
Click the Goals Button: These are the goals for this
module. These topics are all very important background
knowledge for a coach.
Click the Home Menu Button
3
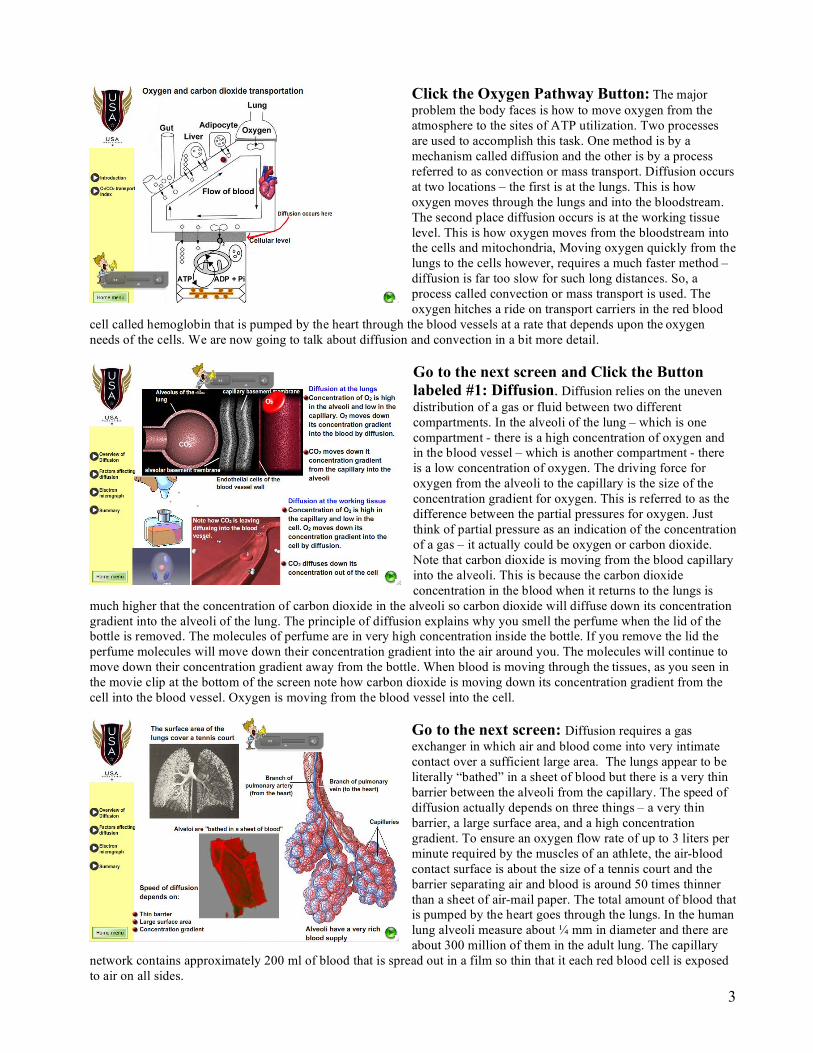
Click the Oxygen Pathway Button: The major
problem the body faces is how to move oxygen from the
atmosphere to the sites of ATP utilization. Two processes
are used to accomplish this task. One method is by a
mechanism called diffusion and the other is by a process
referred to as convection or mass transport. Diffusion occurs
at two locations – the first is at the lungs. This is how
oxygen moves through the lungs and into the bloodstream.
The second place diffusion occurs is at the working tissue
level. This is how oxygen moves from the bloodstream into
the cells and mitochondria, Moving oxygen quickly from the
lungs to the cells however, requires a much faster method –
diffusion is far too slow for such long distances. So, a
process called convection or mass transport is used. The
oxygen hitches a ride on transport carriers in the red blood
cell called hemoglobin that is pumped by the heart through the blood vessels at a rate that depends upon the oxygen
needs of the cells. We are now going to talk about diffusion and convection in a bit more detail.
Go to the next screen and Click the Button
labeled #1: Diffusion. Diffusion relies on the uneven
distribution of a gas or fluid between two different
compartments. In the alveoli of the lung – which is one
compartment - there is a high concentration of oxygen and
in the blood vessel – which is another compartment - there
is a low concentration of oxygen. The driving force for
oxygen from the alveoli to the capillary is the size of the
concentration gradient for oxygen. This is referred to as the
difference between the partial pressures for oxygen. Just
think of partial pressure as an indication of the concentration
of a gas – it actually could be oxygen or carbon dioxide.
Note that carbon dioxide is moving from the blood capillary
into the alveoli. This is because the carbon dioxide
concentration in the blood when it returns to the lungs is
much higher that the concentration of carbon dioxide in the alveoli so carbon dioxide will diffuse down its concentration
gradient into the alveoli of the lung. The principle of diffusion explains why you smell the perfume when the lid of the
bottle is removed. The molecules of perfume are in very high concentration inside the bottle. If you remove the lid the
perfume molecules will move down their concentration gradient into the air around you. The molecules will continue to
move down their concentration gradient away from the bottle. When blood is moving through the tissues, as you seen in
the movie clip at the bottom of the screen note how carbon dioxide is moving down its concentration gradient from the
cell into the blood vessel. Oxygen is moving from the blood vessel into the cell.
Go to the next screen: Diffusion requires a gas
exchanger in which air and blood come into very intimate
contact over a sufficient large area. The lungs appear to be
literally “bathed” in a sheet of blood but there is a very thin
barrier between the alveoli from the capillary. The speed of
diffusion actually depends on three things – a very thin
barrier, a large surface area, and a high concentration
gradient. To ensure an oxygen flow rate of up to 3 liters per
minute required by the muscles of an athlete, the air-blood
contact surface is about the size of a tennis court and the
barrier separating air and blood is around 50 times thinner
than a sheet of air-mail paper. The total amount of blood that
is pumped by the heart goes through the lungs. In the human
lung alveoli measure about ! mm in diameter and there are
about 300 million of them in the adult lung. The capillary
network contains approximately 200 ml of blood that is spread out in a film so thin that it each red blood cell is exposed
to air on all sides.

4
Go to the next screen. Here’s an electron micrograph
of the alveolar wall and a thin capillary. To prevent damage
to these very thin cellular barriers the blood pressure is very
low – in fact the pulmonary vascular bed has 1 fifth the
pressure of the systemic circuit but the blood flows at the
same rate of speed. Each capillary is about the long as a
single alveolus – in other words they are very short. The
blood flows through the capillaries in the lungs at a high
rate of speed. It is estimated that at rest the red blood cell
spends less than 1 second in the alveolar capillary. The
hemoglobin of that red blood cell will be completely
saturated with oxygen by the time it is one third along the
capillary – in a minute we’ll talk about what we mean that
the hemoglobin is saturated with oxygen. During exercise
the entire capillary may be needed for hemoglobin
saturation because the velocity of blood flow is much faster – in this situation the red blood cell will only spend about
0.3 seconds in the capillary. At rest the lung has a considerable diffusion reserve, but this reserve can be completely
exploited when the gas exchanger is stressed to the limit in strenuous exercise. As well, at high altitude we need most of
the capillary length for saturating the blood with oxygen.
Go to the next screen: Here’s a summary of the factors
affecting gas exchange. Remember that diffusion is a
passive process that depends on the surface area, the
thinness of the barrier and the concentration gradient.
Oxygen and carbon dioxide molecules easily slip through
the cellular barrier separating the air in the alveolus from the
red blood cell. For the most part the lung volume is limited
by the space available in the chest cavity. The gas exchanger
has an appreciable excess capacity that is not used by non-
athletes except when they are at altitude. Athletes, however,
can reach the limit of the gas exchange mechanism during
strenuous exercise. Some very elite athletes have shown
some hypoxemia, which simple means that the hemoglobin
does not become completely saturate with oxygen after
passing past the alveoli. This is some evidence that elite
athletes tend to have larger lungs than non-athletes that gives them a diffusion surface advantage. As well, chronic
exercise can enable the athlete to use more of their available lung volume due to the training effect on the respiratory
muscles making them stronger allowing them to expand the chest. This permits more alveoli in the lung to fill with air.
There is also an endurance training effect on the respiratory muscles that permits them to work for longer periods of time
before showing the effects of fatigue. There is no evidence that training increases the actual size of the lung, or the
number of capillaries after adulthood. The jury is still out about the training effect during on the size of the lung during
childhood.
Click the Return Button
Click the Button labeled #2: Transport of
oxygen. Oxygen does not dissolve very well in water. One
liter of blood can only hold about 3 mls of oxygen and the
heart would have to pump over 1000 liters of blood per
minute to deliver the 3 liters of oxygen that the muscles of
an athlete may need to cover the demands of their muscles
during a strenuous run. The strategy used to improve the
situation is to add an oxygen carrier to the blood that
appreciably increases its oxygen carrying capacity that
reduces the blood flow requirements. Let’s take a brief look
at how the oxygen carrier works.

5
Click the continue button: The oxygen carriers used
in all vertebrates and many other animals is hemoglobin.
The structure of hemoglobin includes four heme sites for
oxygen to attach. This improves the oxygen carrying
capacity of blood by about 30 times higher than a solution of
water. This makes the oxygen capacity of blood similar to
that of air. Oxygen that diffuses into the red blood cells
combines chemically with hemoglobin to form
oxyhemoglobin. So, while there is a little bit of oxygen
dissolved in the plasma most of the oxygen is transported by
the red blood cells. In fact, the red blood cells owe their
intense red color to their high hemoglobin content.
Hemoglobin fills about a quarter of the red blood cell’s
internal space. Most other structures you see in other cells
are eliminated in the mature red blood cell. There is no
nucleus and none of the structures that are needed to repair the cell and there are no mitochondria. The red blood cell
makes all its ATP through glycolysis. The life span of the red blood cell is about 140 days on average.
Go to the next screen: What you see here is the
oxyhemoglobin curve. During rest when the red blood cells
leave the lungs the hemoglobin is 98% saturated with
oxygen and at this level of hemoglobin saturation the partial
pressure of oxygen or PO2 is 100 mmHg. Remember that
the partial pressure of a gas simply gives you a measure of
the concentration of the gas dissolved in the plasma. After
passing through the tissues the red blood cells return to the
lungs with hemoglobin that is 75% saturated with oxygen.
The PO2 of blood in the veins is around 40 mm Hg so, you
can see that the amount of oxygen that is dissolved in the
plasma is much lower in venous blood. The PO2 is related
to the amount of oxygen left on the hemoglobin. The
difference between the hemoglobin oxygen saturation
before entering the tissues and the hemoglobin oxygen saturation after leaving the tissues is called the arteriovenous
oxygen difference or a-v O2 difference) and represents how much oxygen is consumed by the tissues. Every time the red
blood cells passes through the lungs it is replenished with oxygen and the hemoglobin becomes 98 percent saturated with
oxygen again. The conditions in the tissues during exercise stimulate the red blood cells to release more oxygen and the
PO2 of blood can drop to around 20 mmHg depending on how much oxygen the cells extract from the blood – note that
the hemoglobin when the PO2 is 20 mmHg is still around 35% saturated with oxygen. Elite athlete can extract a little
more oxygen at the working tissue level– perhaps leaving the hemoglobin about 30% saturated with oxygen - but the
driving force for oxygen into the cell at these low PO2 levels becomes quite weak due to the diminished concentration
gradient for oxygen into the mitochondria. The key point is that the a-vO2 difference represents how much oxygen is
extracted or consumed by the tissues.
Click the Return Button
Click the Button labeled #3: Transport of
carbon dioxide. Carbon dioxide or CO2 is the gaseous
waste produced by the Krebs cycle. As fast as the CO2 is
produced the gas diffuses out of the cell, and into the
capillary. As the blood is passing through the tissues it is
dumping off the oxygen the cells need and at the same time
it will pick up the carbon dioxide. The PCO2 or partial
pressure of carbon dioxide in the cells is higher than it is in
the blood that is entering the tissue bed. At rest, the PCO2 of
cells is around 46 mmHg but it can get a lot higher than this
during exercise. The PCO2 entering the tissue capillaries is
around 40mmHg. As a result, the CO2 diffuses down its

6
concentration gradient out of the cell and into the capillary. Now we will take brief look at how CO2 is transported back
to the lungs where it is expelled into the atmosphere.
Go to the next screen: Carbon dioxide is transported
in the blood in three forms. A small amount –less than 10%
dissolves in the plasma and will be transported that way.
Carbon dioxide is about 20 times more soluble in water than
oxygen so there is much more CO2 than O2 in simple
solution. The remaining CO2 enters the red blood cell. Once
in the red blood cell a small amount will bind to hemoglobin
forming carbaminohemoglobin. Up to around 20% can be
transported this way. The bulk of the CO2 however will be
converted to bicarbonate ions. The red blood cell contains a
very high level of carbonic anhydrase that is an enzyme that
accelerates the conversion of CO2 into bicarbonate. As the
CO2 enters the red blood cell carbonic anhydrase combines
it with water to make carbonic acid or in H2CO3. Carbonic
acid rapidly breaks up into a bicarbonate ion and a hydrogen
ion. The bicarbonate moves into the plasma while the hydrogen ion is buffered by the hemoglobin.
Go to the next screen: Now the blood has reached the
lung. As it passes by the alveolus the carbon dioxide will
once again move down its concentration barrier out of the
blood vessel and into the alveolus. Note the partial pressure
differences for carbon dioxide between the blood vessel and
the alveolus. The first carbon dioxide to diffuse out in the
alveolus is the CO2 that is dissolved in the plasma. Now let’s
take a look at what happens to the bicarbonate ion and how
it is converted back to carbon dioxide.
Go to the next screen: When the CO2 that is dissolved
in the plasma this creates a concentration gradient for the
CO2 that is attached to the hemoglobin and it will be
released from the hemoglobin, diffuse out of the red blood
cell and then into the alveolus. Once this happens there is
now a low concentration of CO2 in the red blood cell and
bicarbonate ions will move back into the red blood cell
where it will spontaneously combine with the hydrogen that
are released from the hemoglobin to from carbonic acid.
The enzyme carbonic anhydrase converts the carbonic acid
into CO2 and water. The CO2 then moves out of the red
blood cell into the plasma and then down its concentration
gradient into the alveolus.

7
Go to the next screen: You now understand that
oxygen and carbon dioxide diffuse down their concentration
barriers. At the lung oxygen will diffuse into the blood
stream and carbon dioxide will diffuse from the bloodstream
into the lung. Once in the capillaries passing through the
lung oxygen is then moved to the left side of the heart where
it will be pumped to the working tissues.
When the blood moves into the working tissue capillary bed
there are a number of factors that change hemoglobin’s
affinity for oxygen and carbon dioxide. At the working
muscle level the temperature of the blood increases. As
well, the acidity or pH causes a change due to the CO2 that
is being produced. Another organic compound called 2.3
DPG or diphosphoglycerate that is a side product of
glycolysis of the red blood cells also increases. All these will decrease the affinity hemoglobin has for oxygen. The O2 is
more easily dumped from the hemoglobin. Just as a side comment 2,3 DPG also increases during an ascent to high
altitude and this is one of the arguments for altitude training. However, the 2,3 DPG effect seems to be fairly small
compared with the temperature and acidity effect. As the hemoglobin loses it affinity for oxygen it increases its affinity
for CO2 and as the blood moves along the capillary in the tissue bed it picks up the CO2 from the cells dropping the pH
from around 7.4 to 7.2 – or lower when the athlete is exercising very strenuously.
When the blood passes through the lung capillaries the reverse occurs as CO2 is discharged into the air. The pH rises
again and the temperature of the blood cools as it moves towards the lungs. This causes the hemoglobin to weaken its
affinity for CO2 and increases its affinity for oxygen.
Click the Return Button
Click the Important Terminology Button: The
normal heart is a muscle about the size of a fist. When the
athlete is at rest every beat it drives about 3 ounces of blood
through its chambers. Inside it is divided into two parts.
Blood enters the heart on the right side which contracts
sending it from the upper right chamber – the right atrium –
into the lower chamber – the right ventricle. Another beat
pushes the blood again into the lungs where it picks up
oxygen before moving into the left atrium which pumps it
into the left ventricle. The left ventricle has to pump blood
to the brain and to the most distant cells in the toes. When an
athlete starts running the working muscle cells need more
oxygen. To meet this demand two things happen – 1) the
heart speeds up its delivery of blood and 2) there is a
redistribution of blood flow from inactive organs to the
active skeletal muscles. In this section we will overview the important terminology used to describe amount of blood
leaving the heart – such as cardiac output, stroke volume and heart rate and how exercise and training affects these in the
immediate and long term. Getting the blood back to the heart is the job of the venous system and we have three
“pumping” mechanisms that helps accomplish this task. We will briefly overview these three mechanisms. And, we will
finish this section by taking a look at how the body redistributes blood flow from organs that are not essential to the
exercise to the working muscles that are in desperate need of the oxygen.

8
Click the Cardiac Output, stroke volume and
heart rate button: Cardiac output is the amount of blood
pumped per minute by the heart. Increases in cardiac output
are closely related to how hard the athlete is working – which,
in turn is related to how much oxygen the working muscles are
demanding. The cardiac output is the most important
descriptor of heart function because it determines the quantity
of oxygen that can be transported by the blood. At rest cardiac
output is around 5 liters per minute and increase to around 30
liters per minute during exercise. Blood flowing into the right
atrium and ventricle must equal the flow through the lung and
flow into the left atrium and ventricle. If you roll the cursor
along the red bar under the graph you will see how cardiac
output increases. Cardiac output depends on two variables –
the stroke volume and the heart rate
Go to the next screen: Note that at rest there is hardly
any difference in cardiac output between the trained and
untrained. However, a trained runner has a higher cardiac
output capacity. The question is how is this higher cardiac
output accomplished. Remember that cardiac output
depends on two things – the heart rate and the stroke
volume. Stroke volume is the amount of blood the heart can
pump per beat. Let’s take a look at stroke volume and see
what happens to that under exercising conditions.
Go to the next screen: Maximal stroke volume can
exceed 200 mL per beat during exercise – at rest it typically
ranges from 50 to 110 mL/beat. Slide the cursor along the
red bar and watch what happens to both cardiac output and
stroke volume. Note how stroke volume reaches it’s highest
value about half way along the red bar. It turns out that
stroke volume reaches its highest value at around 40 to 60%
of VO2max. Also note, that cardiac output continues to
increase despite the fact that stroke volume does not change
any more as the athlete runs faster. When the athlete reaches
anaerobic threshold – or the point at which the aerobic
energy system can’t keep up with the energy demands and
the muscle cells can’t clear the hydrogen ions or lactate. The
athlete can still run a bit faster but the build up of hydrogen
ions will eventually cause the athlete to stop and recover.
There’s only one variable left – the heart rate. This variable is responsible for the increasing cardiac output even though
stroke volume does not increase after about 40 to 60% of VO2max.

9
Go to the next screen: Maximum stroke volume can
be double in the athlete. Women generally have a lower
stroke volume than men do because they have smaller
hearts. The larger stroke volume is the result of the increase
in heart size that can be achieved through training. However,
there is also a genetic factor involved here – elite athletes
appear to have the genetically larger heart and this, in
addition to the training effect, provides them with an athletic
advantage. Keep in mind that any adjustment in structure of
the heart is a slow process that typically takes months – even
years to be completed and there is a genetic limit to its
stroke volume capacity.
Go to the next screen. Now let’s talk about heart rate
or the beating frequency of the heart. Heart rate increases
linearly with increasing workload or the volume of oxygen
consumed. Slide the cursor along the red bar to see the
relationship of heart rate to stroke volume and cardiac
output. Note that while stroke volume reaches its maximum
about half way along the red bar the heart rate keeps
increasing up to the anaerobic threshold. Cardiac output
stops increasing at this point as well. So, after about 40 to
60% of VO2 max the increase in cardiac output is due to the
increasing heart rate. Stroke volume is related to the size of
the heart and this is fixed depending on genetics and its
structural changes that can occur with training over a long
period of time. But heart rate is capable of instantly
changing over a wide range according to the oxygen needs
of the muscle cell. The beating frequency depends on the autonomic nervous system and hormone level – especially the
amount of adrenalin or epinephrine in the blood.
Go to the next screen: Heart rate is what is known as
its functional capacity. It allows rapid adjustment to the
needs of the moment and these adjustments occur in
milliseconds to seconds. The structural capacity of the heart
sets the maximal amount of blood it can pump in one beat.
The body can adjust this capacity to higher levels if needed
and does this by enlarging the heart size but this adjustment
occurs very, very slowly. This structural adjustment is an
important feature because it allows the heart to be kept at the
smaller size until the need for enlargement arises. Indeed the
heart will shrink back to its normal size once the athlete
stops high performance training.
However, the maximal beating frequency of the heart does
not change with training. This is fixed and depends on the
age of the athlete – the older the athlete the lower the maximal heart rate. Training does reduce the heart rate at sub
maximal workloads, though, because the heart becomes stronger and can pump out more blood per beat. Indeed, a slow
heart rate in a healthy individual indicates an efficient circulatory system.
I want to make one more comment about the max heart rate – while there is no training an athlete can do that will
increase the max heart rate, there is a gradually lowering of the max heart rate with advancing age. The max heart rate
loses about 1 beat per min each year. This becomes a relevant issue for you if you are training older runners and you are
using heart rate as an estimate of training stress.

10
Go to the next screen: Let’s just quickly review what
we just discussed. The amount of blood the heart pumps in
one minute is called the cardiac output. Cardiac output
depends on two variables – the heart rate and the stroke
volume. Stroke volume is the amount of blood pumped out
per beat and the heart rate is the number of beats the heart
makes in 1 minute. Both stroke volume and heart rate
increase during exercise increasing the cardiac output.
Stroke volume increases up to about 40 – 60% of VO2max.
After that it plateaus. Heart rate varies in direct relationship
to the workload – and plays a larger role in increasing
cardiac output.
The stroke volume can increase with training but there is a
genetic limit and it takes a long time for this to occur
because it involves a structural change.
There is an upper limit to the maximum heart rate and this does not change with training. However, during rest and
exercise the trained athlete has a lower heart rate for the same workload than an untrained athlete. And finally, the athlete
has a higher cardiac output than the untrained. Some of this is due to genetics – that is the elite athlete has a naturally
larger heart – and some of it is due to the structural changes that occur with training.
Click the Return Button
Click the Venous Return Button: The left side of
the heart can only pump out as much blood as it receives
from the right side. The venous system is responsible for
keeping pace with the cardiac output needs. The blood in the
venous system is under very low pressure and the walls of
the veins have a very low compliance which simply means
that they easily expand to depending on the amount of blood
they need to hold. If the cells need a higher cardiac output
the blood must be sent back to the heart at a higher rate of
speed. There are three mechanisms that increase the venous
return to the heart.
One mechanism is a muscle pump and a respiratory pump
and the veins will constrict. This reduces the amount of
blood that is in the veins forcing it out of the veins towards
the heart. As the muscle contract their veins are compressed and the blood within them is forced toward the heart. Note
the valves in the veins that stop the backflow of blood until the next muscle contraction.
The second mechanism is the respiratory pump, As the chest wall expands due to the brain signals to the respiratory
muscles to contract this lowers the pressure in the chest cavity allowing the veins in the chest cavity to fill with blood.
When the athlete breathes out the pressure in the chest cavity increases sending the venous blood towards the heart.
And finally, the veins will constrict and this reduces the volume of the venous system squeezing the blood toward the
heart.
Click the Return Button

11
Click the Redistribution of Blood Flow Button: Another important adjustment the body makes to ensure that
there is adequate blood flow to the working muscles is to
redistribute the blood flow from organs that don’t need it to
the working muscles. The redistribution of blood flow is due
to a constriction of the muscles surrounding the arterioles
supplying the capillary beds organs that are not essential and
a vasodilation of arterioles of the capillary beds supplying
the active muscles.
Let’s take a look at the result of the vasoconstriction and
vasodilation phenomenons. At rest, for example, the heart
pumps around 5 to 6 liters of blood through the bloods
vessels. This is all that is needed to deliver the necessary
oxygen and nutrients to the cells.
As you analyze how that blood flow or 5 to 6 liters is distributed to the organs note that 24% of it or about 1.5 liters goes
to the liver and gut, 19% or 1.1 liters goes to the kidneys and around 20% goes to the muscles. The brain needs at least 2
liters of blood and at rest this represent 35% of the cardiac output.
During exercise, things changes quite a bit – because cardiac output increases dramatically in order to meet the oxygen
demands of the working muscles. In this example cardiac output is 25 liters per minute. 100% of that goes through the
lungs and then 100% of the blood passing through the lungs it is sent to the from the left ventricle where it is then sent
out to the body’s organs. But note that the blood flow through the gut, liver and kidney has dropped dramatically. The
muscles are now receiving around 90% of the blood flow or 22 liters per minute – the brain still needs its 2 liters – in fact
under exercising conditions it needs a bit more – around 2.5 liters. When the weather is hot then more blood will be
diverted to the skin for cooling purposes. This blood flow to the skin is drawn away from the working muscles and this
explains why athletic performances are often lower in hotter weather.
All these factors – the muscle pump, the respiratory pump, venoconstriction and the redistribution of blood flow, in
conjunction with the increased extraction of oxygen under exercising conditions all increase blood circulation.
Click the Return Button
Click the Home Menu Button
You have now completed this module