urinary stone disease lecture №2 lecturer – baralo igor vitalievich
TRANSCRIPT

Urinary Stone DiseaseUrinary Stone Disease
LectureLecture № №22LecturerLecturer – – Baralo Igor VitalievichBaralo Igor Vitalievich

Questions of the etiology of stonesQuestions of the etiology of stones Urinary stones have plagued humans since the earliest Urinary stones have plagued humans since the earliest
records of civilization. The etiology of stones remains records of civilization. The etiology of stones remains speculative. speculative.
If urinary constituents are similar from each kidney and if If urinary constituents are similar from each kidney and if there is no evidence of obstruction, why do most there is no evidence of obstruction, why do most stones present in a unilateral fashion? stones present in a unilateral fashion?
Why don't small stones pass uneventfully down the Why don't small stones pass uneventfully down the ureter early in their development? ureter early in their development?
Why do some people form one large stone and others Why do some people form one large stone and others form multiple small calculi? form multiple small calculi?
There is much speculation concerning these and other There is much speculation concerning these and other questions.questions.

PATHOGENESIS OF UPPER URINARY TRACT CALCULIPATHOGENESIS OF UPPER URINARY TRACT CALCULI
•• Urine must be supersaturated for stones to form. Urine must be supersaturated for stones to form.
•• Supersaturation alone is not sufficient for crystallization to occur in Supersaturation alone is not sufficient for crystallization to occur in urine, owing to the presence of urinary inhibitors. urine, owing to the presence of urinary inhibitors.
•• Nephrocalcin, uropontin, and Tamm-Horsfall protein are important Nephrocalcin, uropontin, and Tamm-Horsfall protein are important inhibitors of crystal nucleation, growth, or aggregation. inhibitors of crystal nucleation, growth, or aggregation.
•• Urinary calcium and oxalate are equal contributors to urinary Urinary calcium and oxalate are equal contributors to urinary saturation of calcium oxalate. saturation of calcium oxalate.
•• Calcium stones may originate from subepithelial plaques Calcium stones may originate from subepithelial plaques composed of calcium apatite that serve as an anchor on which composed of calcium apatite that serve as an anchor on which calcium oxalate stones can grow. calcium oxalate stones can grow.
•• The noncrystalline component of stones is matrix, which is The noncrystalline component of stones is matrix, which is composed of a combination of mucoproteins, proteins, composed of a combination of mucoproteins, proteins, carbohydrates, and urinary inhibitorscarbohydrates, and urinary inhibitors


PATHOGENESIS OF UPPER URINARY TRACT CALCULIPATHOGENESIS OF UPPER URINARY TRACT CALCULI
•• Calcium absorption occurs primarily in the small Calcium absorption occurs primarily in the small intestine at a rate that is dependent on calcium intake. intestine at a rate that is dependent on calcium intake.
•• 1,25-Dihydroxyvitamin D3 is the most potent stimulator 1,25-Dihydroxyvitamin D3 is the most potent stimulator of intestinal calcium absorption. of intestinal calcium absorption.
•• PTH stimulates 1α-hydroxylase in the proximal tubule of PTH stimulates 1α-hydroxylase in the proximal tubule of the kidney to convert 25-dihydroxyvitamin D3 to the kidney to convert 25-dihydroxyvitamin D3 to 1,25(OH)2D3. 1,25(OH)2D3.
•• PTH enhances proximal tubular reabsorption of calcium PTH enhances proximal tubular reabsorption of calcium and reduces renal phosphate excretion. and reduces renal phosphate excretion.
•• Intestinal oxalate absorption is influenced by luminal Intestinal oxalate absorption is influenced by luminal calcium, magnesium, and oxalate-degrading bacteriacalcium, magnesium, and oxalate-degrading bacteria

PATHOGENESIS OF UPPER URINARY TRACT CALCULIPATHOGENESIS OF UPPER URINARY TRACT CALCULI
•• Absorptive hypercalciuria is characterized by normal serum calcium, Absorptive hypercalciuria is characterized by normal serum calcium, normal or suppressed PTH, normal fasting urinary calcium, and normal or suppressed PTH, normal fasting urinary calcium, and elevated urinary calcium. elevated urinary calcium.
•• Renal hypercalciuria is due to impaired renal calcium reabsorption, Renal hypercalciuria is due to impaired renal calcium reabsorption, which stimulates PTH secretion and leads to fasting hypercalciuria. which stimulates PTH secretion and leads to fasting hypercalciuria.
•• Resorptive hypercalciuria is primarily due to primary Resorptive hypercalciuria is primarily due to primary hyperparathyroidism but may be seen with granulomatous diseases hyperparathyroidism but may be seen with granulomatous diseases that elaborate 1,25(OH)2D3. that elaborate 1,25(OH)2D3.
•• The most important determinant of uric acid stone formation is low The most important determinant of uric acid stone formation is low urinary pH. urinary pH.
•• Low urine pH seen in uric acid stone formers is likely due to impaired Low urine pH seen in uric acid stone formers is likely due to impaired ammoniagenesis as a result of insulin resistance. ammoniagenesis as a result of insulin resistance.
•• In distal renal tubular acidosis, a defective H+ATPase accounts for In distal renal tubular acidosis, a defective H+ATPase accounts for excretion of excess acid into the distal tubule. excretion of excess acid into the distal tubule.
•• Formation of infection stones requires alkaline urine that can be Formation of infection stones requires alkaline urine that can be achieved only with infection with urease-producing bacteria.achieved only with infection with urease-producing bacteria.

PATHOGENESIS OF UPPER URINARY TRACT CALCULI PATHOGENESIS OF UPPER URINARY TRACT CALCULI ((Randall’s theoryRandall’s theory))


Radiation of pain Radiation of pain

NAUSEA AND VOMITINGNAUSEA AND VOMITING
Upper-tract obstruction is frequently associated Upper-tract obstruction is frequently associated with nausea and vomiting. with nausea and vomiting. Intravenous fluids are required to restore a Intravenous fluids are required to restore a euvolemic state. Intravenous fluids should not be euvolemic state. Intravenous fluids should not be used to force a diuresis in an attempt to push a used to force a diuresis in an attempt to push a ureteral stone down the ureter. ureteral stone down the ureter. Effective ureteral peristalsis requires coaptation Effective ureteral peristalsis requires coaptation of the ureteral walls and is most effective in a of the ureteral walls and is most effective in a euvolemic stateeuvolemic state

HEMATURIAHEMATURIA
A complete urinalysis helps to confirm the A complete urinalysis helps to confirm the diagnosis of diagnosis of І І urinary stone by assessing for urinary stone by assessing for hematuria and crystaluria and documenting hematuria and crystaluria and documenting urinary pH. Patients frequently admit to urinary pH. Patients frequently admit to intermittent gross hematuria or occasional tea-intermittent gross hematuria or occasional tea-colored urine (old blood). Most patients will have colored urine (old blood). Most patients will have at least microhematuria. Rarely (in at least microhematuria. Rarely (in 10-15% 10-15% of of cases), complete ureteral obstruction presents cases), complete ureteral obstruction presents without micro hematuria.without micro hematuria.

ASSOCIATED FEVERASSOCIATED FEVER
The association of urinary stones with fever is a relative The association of urinary stones with fever is a relative medical emergency. medical emergency. Signs of clinical sepsis are variable and include fever, Signs of clinical sepsis are variable and include fever, tachycardia, hypotension, and cutaneous vasodilation. tachycardia, hypotension, and cutaneous vasodilation. Costovertebral angle tenderness may be marked with Costovertebral angle tenderness may be marked with acute upper-tract obstruction; however, it cannot be acute upper-tract obstruction; however, it cannot be relied on to be present in in stances of long-term relied on to be present in in stances of long-term obstruction. obstruction. In such instances a mass may be palpable resulting from In such instances a mass may be palpable resulting from a grossly hy-dronephrotic kidney. a grossly hy-dronephrotic kidney. Fever associated with urinary tract obstruction requires Fever associated with urinary tract obstruction requires prompt decompression. prompt decompression.

PHYSICAL EXAMINATIONPHYSICAL EXAMINATION
A thorough abdominal examination should exclude other A thorough abdominal examination should exclude other causes of abdominal pain. Abdominal tumors, ab dominal causes of abdominal pain. Abdominal tumors, ab dominal aortic aneurysms, herniated lumbar disks, and aortic aneurysms, herniated lumbar disks, and pregnancy may mimic renal colic. Referred pain may be pregnancy may mimic renal colic. Referred pain may be similar owing to common afferent neural pathways. similar owing to common afferent neural pathways. Intestinal ileus may be associated with renal colic or Intestinal ileus may be associated with renal colic or other intraperitoneal or retroperitoneal processes. other intraperitoneal or retroperitoneal processes. Bladder palpation should be performed because urinary Bladder palpation should be performed because urinary retention may present with pain similar to renal colic. retention may present with pain similar to renal colic. Incarcerated inguinal hernias, epididymitis, orchitis, and Incarcerated inguinal hernias, epididymitis, orchitis, and female pelvic pathologic states may mimic urinary stone female pelvic pathologic states may mimic urinary stone disease. A rectal examination helps exclude other disease. A rectal examination helps exclude other pathologic conditions.pathologic conditions.

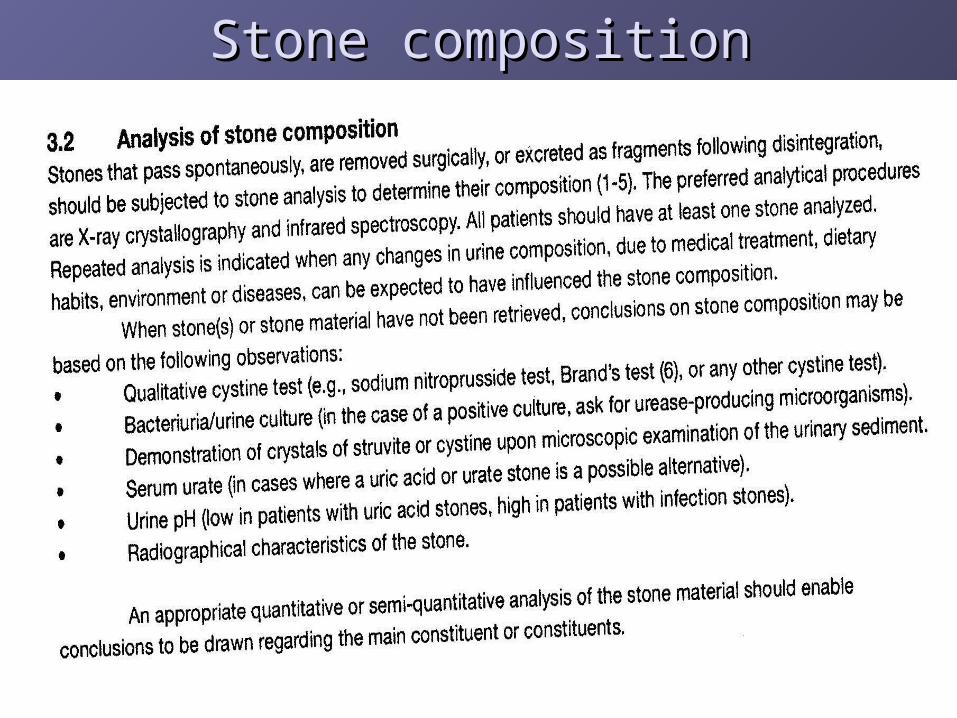
Stone compositionStone composition

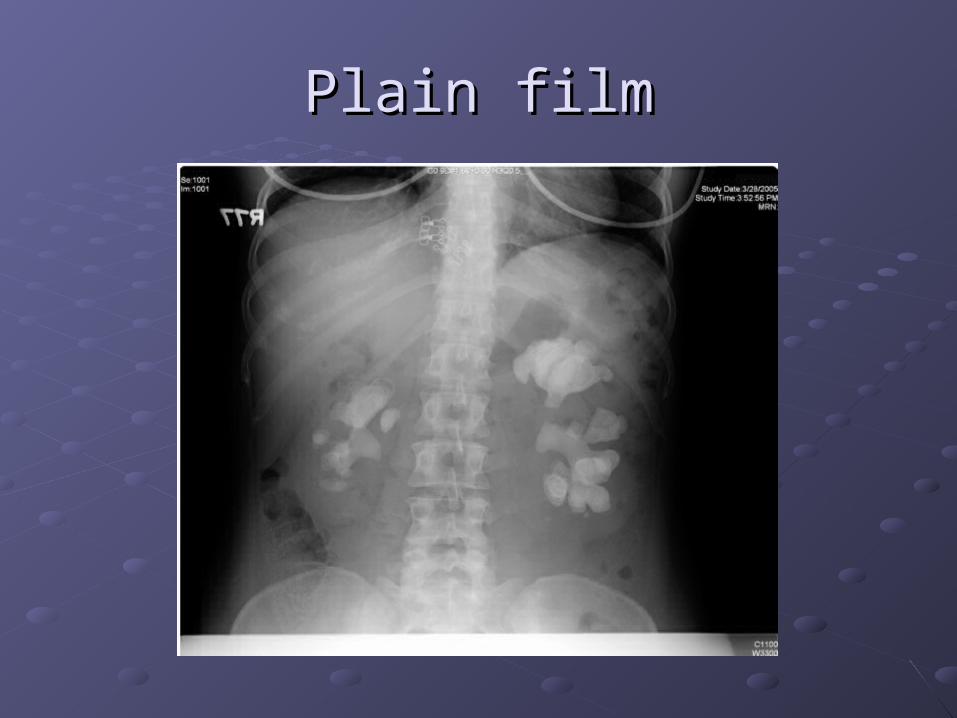
Plain filmPlain film

Intavenous urografy (stone in ureterocele )Intavenous urografy (stone in ureterocele )

Computer tomografy (CT)Computer tomografy (CT)

UreterolithoextractionUreterolithoextraction

Extracorporeal shock wave lithotripsyExtracorporeal shock wave lithotripsy

A. Supersonic shock wave emission from a spark gap electrodeA. Supersonic shock wave emission from a spark gap electrode
B. Reflecting the shock wave from focus B. Reflecting the shock wave from focus 1 1 to focus to focus 2 2 allows for stone fragmentationallows for stone fragmentation..
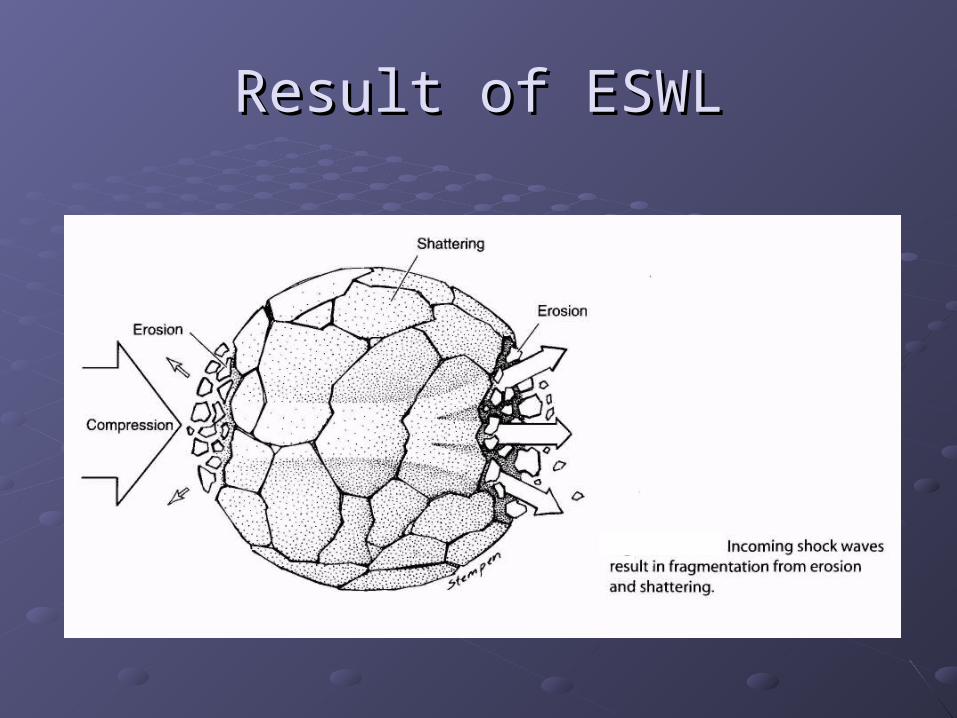
Result of ESWLResult of ESWL

URETEROSCOPIC STONE EXTRACTIONURETEROSCOPIC STONE EXTRACTION
Ureteroscopic stone extraction is highly efficacious for lower ureteral calculi. The use of Ureteroscopic stone extraction is highly efficacious for lower ureteral calculi. The use of smallcaliber ureteroscopes and the advent of balloon dilation or ureteral access smallcaliber ureteroscopes and the advent of balloon dilation or ureteral access sheaths have increased stone-free rates dramatically. Even relatively largecaliber sheaths have increased stone-free rates dramatically. Even relatively largecaliber endoscopes without balloon dilation are effective in lower ureteral stone retrieval. endoscopes without balloon dilation are effective in lower ureteral stone retrieval. Stone-free rates range from Stone-free rates range from 66% 66% to to 100% 100% and are dependent on stone burden and and are dependent on stone burden and location, length of time the stone has been impacted, history of retroperitoneal location, length of time the stone has been impacted, history of retroperitoneal surgery, and the experience of the operator. Complication rates range from surgery, and the experience of the operator. Complication rates range from 5% 5% to to 30%; 30%; the rates increase when manipulations venture into the proximal ureter. the rates increase when manipulations venture into the proximal ureter. Ureteral stricture rates are less than Ureteral stricture rates are less than 5%. 5%. Postoperative vesicoureteral reflux is Postoperative vesicoureteral reflux is extremely rare. Calculi that measure less than extremely rare. Calculi that measure less than 8 8 mm are frequently removed intact. mm are frequently removed intact. Round wire stone baskets can be torqued to help entrap stone or stone fragments. Round wire stone baskets can be torqued to help entrap stone or stone fragments. Flat wire baskets should be used with caution; if twisted, they can de velop sharp, Flat wire baskets should be used with caution; if twisted, they can de velop sharp, knifelike edges resulting in ureteral injury. Excessive force with any instrument in the knifelike edges resulting in ureteral injury. Excessive force with any instrument in the ureter may result in ureteral injury.ureter may result in ureteral injury.
A variety of lithotrites can be placed through an ureteroscope, including electrohydraulic; A variety of lithotrites can be placed through an ureteroscope, including electrohydraulic; solid, and hollow-core ultrasonic probes; a variety of laser systems; and pneumatic solid, and hollow-core ultrasonic probes; a variety of laser systems; and pneumatic systems such as the Swiss lithoclast. Electrohydraulic lithotrites have power settings systems such as the Swiss lithoclast. Electrohydraulic lithotrites have power settings as high as as high as 120 120 V that result in a cavitation bubble, followed by collapse of this bubble V that result in a cavitation bubble, followed by collapse of this bubble causing subsequent shock waves. Care should be taken to keep the tip of the causing subsequent shock waves. Care should be taken to keep the tip of the electrode away from surrounding tissue and the tip of the endoscope. Ultrasonic electrode away from surrounding tissue and the tip of the endoscope. Ultrasonic lithotrites have a piezoceramic energy source that converts electrical energy into lithotrites have a piezoceramic energy source that converts electrical energy into ultrasonic waves in the range of ultrasonic waves in the range of 25,000 25,000 Hz. This vibratory action is effective in Hz. This vibratory action is effective in fragmenting calculi. Hollow probes can suction stone fragments and debris fragmenting calculi. Hollow probes can suction stone fragments and debris simultaneously. Laser systems are discussed elsewhere in this book. The simultaneously. Laser systems are discussed elsewhere in this book. The electromechanical impactors are similar to jackhammers with a movable pistonlike tip electromechanical impactors are similar to jackhammers with a movable pistonlike tip that fragments calculi.that fragments calculi.

PERCUTANEOUS NEPHROLITHOTOMYPERCUTANEOUS NEPHROLITHOTOMY
Percutaneous removal of renal and proximal ureteral cal culi is the treatment of Percutaneous removal of renal and proximal ureteral cal culi is the treatment of choice for large choice for large (> 2.5 (> 2.5 cm) cal culi, those resistant to ESWL, select lower pole cm) cal culi, those resistant to ESWL, select lower pole calyceal stones with a narrow, long infundibulum and an acute infundibulo-pelvic calyceal stones with a narrow, long infundibulum and an acute infundibulo-pelvic angle, and instances with evidence of obstruction; the method can rapidly establish a angle, and instances with evidence of obstruction; the method can rapidly establish a stone-free status. Needle puncture is directed by fluoroscopy, ultrasound, or both, stone-free status. Needle puncture is directed by fluoroscopy, ultrasound, or both, and is routinely placed from the posterior axillary line into a posterior inferior calyx. and is routinely placed from the posterior axillary line into a posterior inferior calyx. Su perior caliceal puncture may be required, and in such situations care should be Su perior caliceal puncture may be required, and in such situations care should be taken to avoid injury to the pleura, lungs, spleen, and liver. Tract dilation is per formed taken to avoid injury to the pleura, lungs, spleen, and liver. Tract dilation is per formed by sequential plastic dilators (Amplatz system),by sequential plastic dilators (Amplatz system),telescoping metal dilators (Alken), or balloon dilation with a backloaded Amplatz telescoping metal dilators (Alken), or balloon dilation with a backloaded Amplatz sheath. Tracts placed during open renal procedures are frequently tortuous and sub-sheath. Tracts placed during open renal procedures are frequently tortuous and sub-optimal for subsequent endourologic procedures.optimal for subsequent endourologic procedures.Percutaneous extraction of calculi requires patience and perseverance. Hardcopy Percutaneous extraction of calculi requires patience and perseverance. Hardcopy radiographs help to confirm a stone-free status. Remaining calculi can be retrieved radiographs help to confirm a stone-free status. Remaining calculi can be retrieved with the aid of flexible endoscopes, additional percutaneous puncture access, follow-with the aid of flexible endoscopes, additional percutaneous puncture access, follow-up irrigations, ESWL, or additional percutaneous sessions. Realistic goals should be up irrigations, ESWL, or additional percutaneous sessions. Realistic goals should be established. Patients should be informed that complex calculi frequently require established. Patients should be informed that complex calculi frequently require numer ous procedures.numer ous procedures.Maintenance of body temperature with appropriate blankets during preoperative Maintenance of body temperature with appropriate blankets during preoperative patient positioning and with warmed irrigation fluids helps to prevent bleeding patient positioning and with warmed irrigation fluids helps to prevent bleeding diatheses associated with hypothermia. The average blood loss during a diatheses associated with hypothermia. The average blood loss during a percutaneous nephrolithotomy is percutaneous nephrolithotomy is 2.0—2.8 2.0—2.8 g/dL of hemoglobin. Multiple percutaneous g/dL of hemoglobin. Multiple percutaneous punctures and renal pelvic perforations are associated with a greater blood loss. punctures and renal pelvic perforations are associated with a greater blood loss. Overall, such procedures are safe and effective and have a transfusion rate well Overall, such procedures are safe and effective and have a transfusion rate well below below 10%.10%.

OPEN STONE SURGERYOPEN STONE SURGERY
PYELOLITHOTOMYPYELOLITHOTOMY
ANATROPHIC NEPHROLITHOTOMYANATROPHIC NEPHROLITHOTOMY
RADIAL NEPHROTOMYRADIAL NEPHROTOMY
OTHER RENAL PROCEDURESOTHER RENAL PROCEDURES
URETEROLITHOTOMYURETEROLITHOTOMY

ANATROPHIC NEPHROLITHOTOMYANATROPHIC NEPHROLITHOTOMY

ANATROPHIC NEPHROLITHOTOMYANATROPHIC NEPHROLITHOTOMY
ORAL MEDICATIONSORAL MEDICATIONS1. 1. Alkalinizing pH agentsAlkalinizing pH agents——Potassium citrate is an oral agent that elevates urinary pH Potassium citrate is an oral agent that elevates urinary pH effectively by effectively by 0.7-0.8 0.7-0.8 pH units. Typical dosing is pH units. Typical dosing is 60 60 mEq in mEq in 3 3 or or 4 4 divided doses daily. It is divided doses daily. It is available in wax-matrix available in wax-matrix 10-10-mEq tablets, liquid preparations, and crystals that must be mixed mEq tablets, liquid preparations, and crystals that must be mixed with fluids. The effect is maintained over many years. Care should be taken in patients suscepti with fluids. The effect is maintained over many years. Care should be taken in patients suscepti ble to hyperkalemia, those with renal failure, and those taking potassium-sparing diuretics. ble to hyperkalemia, those with renal failure, and those taking potassium-sparing diuretics. Although the med ication is usually well tolerated, some patients may complain of abdominal Although the med ication is usually well tolerated, some patients may complain of abdominal discomfort, especially with tablet preparations. It is indicated in those with calcium oxalate discomfort, especially with tablet preparations. It is indicated in those with calcium oxalate calculi secondary to hypocitraturia calculi secondary to hypocitraturia (< 320 (< 320 mg/d), including those with renal tubular acidosis. mg/d), including those with renal tubular acidosis. Potassium citrate also may be used effectively to treat uric acid lithiasis and nonsevere forms of Potassium citrate also may be used effectively to treat uric acid lithiasis and nonsevere forms of hyperurico-suric calcium nephrolithiasis.hyperurico-suric calcium nephrolithiasis.Sodium and potassium bicarbonate, orange juice, and lemonade are alternative alkalinizing Sodium and potassium bicarbonate, orange juice, and lemonade are alternative alkalinizing agents. There are no effective long-term urinary acidifying agents.agents. There are no effective long-term urinary acidifying agents.2. 2. Gastrointestinal absorption inhibitorGastrointestinal absorption inhibitor——Cellulose phosphate binds calcium in the gut and Cellulose phosphate binds calcium in the gut and thereby in hibits calcium absorption and urinary excretion. It is a popular drug in the treatment of thereby in hibits calcium absorption and urinary excretion. It is a popular drug in the treatment of absorptive hypercalciuria type I with recurrent calcium nephrolithiasis, al though it only prevents absorptive hypercalciuria type I with recurrent calcium nephrolithiasis, al though it only prevents new stone formation. Patients should have normal parathyroid hormone values, nor mal serum new stone formation. Patients should have normal parathyroid hormone values, nor mal serum calcium and phosphate values, no evidence of bone disease, and evidence of increased calcium and phosphate values, no evidence of bone disease, and evidence of increased intestinal cal cium absorption. The drug decreases the urinary satura tion of calcium phosphate intestinal cal cium absorption. The drug decreases the urinary satura tion of calcium phosphate and calcium oxalate. It may increase urinary oxalate and urinary phosphate levels. A typical and calcium oxalate. It may increase urinary oxalate and urinary phosphate levels. A typical starting dosage is starting dosage is 5 5 g g 3 3 times daily with meals; the dosage may be titrated by following 24-h times daily with meals; the dosage may be titrated by following 24-h urinary calcium levels. Urinary magnesium, calcium, oxalate, and sodium levels and serum urinary calcium levels. Urinary magnesium, calcium, oxalate, and sodium levels and serum parathyroid hormone should be monitored parathyroid hormone should be monitored 1—2 1—2 times yearly. Magnesium supplements are times yearly. Magnesium supplements are frequently required and should be taken at least frequently required and should be taken at least 1 1 h before or after cellulose phosphate is h before or after cellulose phosphate is taken. Cellulose phosphate is associated with a. sodium load and should be used with caution taken. Cellulose phosphate is associated with a. sodium load and should be used with caution in those with congestive heart failure. Gastrointestinal side effects are infrequent; they include in those with congestive heart failure. Gastrointestinal side effects are infrequent; they include dyspepsia and loose bowel movements.dyspepsia and loose bowel movements.Cellulose phosphate may be suboptimal treatment for postmenopausal women who are at risk Cellulose phosphate may be suboptimal treatment for postmenopausal women who are at risk for bone disease. An alternative treatment for such patients would be hydrochlorothiazides for bone disease. An alternative treatment for such patients would be hydrochlorothiazides supplemented with potassium citrate to offset the potential hypokalemia and hypocitraturia.supplemented with potassium citrate to offset the potential hypokalemia and hypocitraturia.

ORAL MEDICATIONSORAL MEDICATIONS
3. 3. Phosphate supplementationPhosphate supplementation——Renal phosphate leak is best treated by replacing phosphate. Renal phosphate leak is best treated by replacing phosphate. Phosphate absorption may be inhibited in the presence of alu minum-, magnesium-, or calcium-Phosphate absorption may be inhibited in the presence of alu minum-, magnesium-, or calcium-containing antacids. This treatment should be used with caution in digital-ized patients and in containing antacids. This treatment should be used with caution in digital-ized patients and in those with severe renal failure, Ad-dison disease, or severe hepatic dysfunction. It is gener ally those with severe renal failure, Ad-dison disease, or severe hepatic dysfunction. It is gener ally well tolerated. Dosing can begin with well tolerated. Dosing can begin with 250 250 mg mg 3-4 3-4 times daily and may be doubled depending on times daily and may be doubled depending on follow-up serum electrolyte, calcium, and phosphorus levels.follow-up serum electrolyte, calcium, and phosphorus levels.4. 4. DiureticsDiuretics——Thiazides can correct the renal calcium leak associated with renal hypercalciuria. Thiazides can correct the renal calcium leak associated with renal hypercalciuria. This prevents a secondary hyperparathyroid state and its associated el evated vitamin D This prevents a secondary hyperparathyroid state and its associated el evated vitamin D synthesis and intestinal calcium ab sorption. A rapid decrease in urinary calcium excretion is synthesis and intestinal calcium ab sorption. A rapid decrease in urinary calcium excretion is appreciated and is sustained long-term appreciated and is sustained long-term (> 10 (> 10 years). A starting dose of years). A starting dose of 25 25 mg may be titrated mg may be titrated based on urinary calcium levels. Side effects are usually well tolerated. Potassium levels should based on urinary calcium levels. Side effects are usually well tolerated. Potassium levels should be monitored. Hypokalemia induces a hypocitraturic state; potassium replacement corrects the be monitored. Hypokalemia induces a hypocitraturic state; potassium replacement corrects the hypokalemia and its associated hypocitra turia.hypokalemia and its associated hypocitra turia.Thiazides result in a transient decrease in urinary calcium excretion in absorptive hypercalciurics. Thiazides result in a transient decrease in urinary calcium excretion in absorptive hypercalciurics. Urinary calcium excretion rebounds to pretreatment values in Urinary calcium excretion rebounds to pretreatment values in 50% 50% of such patients after of such patients after 4-5 4-5 years of therapy. Dietary changes are not believed to be responsible for this phenomenon. years of therapy. Dietary changes are not believed to be responsible for this phenomenon. Thiazides do not restore normal intestinal absorption of calcium.Thiazides do not restore normal intestinal absorption of calcium.5. 5. Calcium supplementationCalcium supplementation——Enteric hyperoxaluric calcium nephrolithiasis is effectively treated Enteric hyperoxaluric calcium nephrolithiasis is effectively treated with cal cium supplements. Calcium gluconate and calcium cit rate are better absorbed and are with cal cium supplements. Calcium gluconate and calcium cit rate are better absorbed and are more effective in increasing serum calcium availability than are other forms of calcium. Calcium more effective in increasing serum calcium availability than are other forms of calcium. Calcium carbonate, calcium phosphate, and oyster shell are forms of calcium that are less efficiently carbonate, calcium phosphate, and oyster shell are forms of calcium that are less efficiently absorbed; they remain in the intestinal lumen, available to bind oxalate, thus reducing its absorbed; they remain in the intestinal lumen, available to bind oxalate, thus reducing its absorption. These less efficiently absorbed forms of calcium are optimal to treat enteric absorption. These less efficiently absorbed forms of calcium are optimal to treat enteric hyperoxaluric calcium nephrolithiasis and must be given with meals to be effective.hyperoxaluric calcium nephrolithiasis and must be given with meals to be effective.

ORAL MEDICATIONSORAL MEDICATIONS
6. 6. Uric acid-lowering medicationsUric acid-lowering medications——Allopurinol is used to treat hyperuricosuric Allopurinol is used to treat hyperuricosuric calcium nephrolithiasis with or without hyperuricemia. Unlike uricosuric agents calcium nephrolithiasis with or without hyperuricemia. Unlike uricosuric agents that reduce serum uric acid levels by increasing urinary uric acid excretion, allopurinol that reduce serum uric acid levels by increasing urinary uric acid excretion, allopurinol is a xanthineoxidase inhibitor and reduces both serum and urinary levels of uric acid. is a xanthineoxidase inhibitor and reduces both serum and urinary levels of uric acid. It has no impact on the biosynthesis of purines; rather, it acts exclusively on purine It has no impact on the biosynthesis of purines; rather, it acts exclusively on purine catabolism. Elevated levels of xanthine and hypoxanthine in the urine secondary to catabolism. Elevated levels of xanthine and hypoxanthine in the urine secondary to allopurinol have not been associated with nephrolithiasis. Allopurinol is a potentially allopurinol have not been associated with nephrolithiasis. Allopurinol is a potentially dan gerous drug and should be discontinued at the first ap pearance of a skin rash, dan gerous drug and should be discontinued at the first ap pearance of a skin rash, which infrequently may be fatal. Therapy can start at which infrequently may be fatal. Therapy can start at 300 300 mg per day. It is toler ated mg per day. It is toler ated best when taken after meals.best when taken after meals.7. 7. Urease inhibitorUrease inhibitor——Acetohydroxamic acid is an ef fective adjunctive treatment in Acetohydroxamic acid is an ef fective adjunctive treatment in those with chronic urea-splitting urinary tract infections associated with struvite those with chronic urea-splitting urinary tract infections associated with struvite stones. Acetohydroxamic acid reversibly inhibits bacter ial urease, decreasing urinary stones. Acetohydroxamic acid reversibly inhibits bacter ial urease, decreasing urinary ammonia levels, and will subsequently acidify urine. It is best used as prophylaxis ammonia levels, and will subsequently acidify urine. It is best used as prophylaxis after removal of struvite stones. It also may be used after unsuccessful attempts at after removal of struvite stones. It also may be used after unsuccessful attempts at curative surgical removal of calculi or culture-specific antibiotic therapy. Patients with curative surgical removal of calculi or culture-specific antibiotic therapy. Patients with serum creatinine serum creatinine > 2.5 > 2.5 mg/dL are unable to achieve therapeutic urinary levels. mg/dL are unable to achieve therapeutic urinary levels. Acetohydroxamic acid is not effective with nonurease-producing bacteria. Long-term Acetohydroxamic acid is not effective with nonurease-producing bacteria. Long-term data data (> 7 (> 7 years) are unavailable. A signif icant number of patients complain of side years) are unavailable. A signif icant number of patients complain of side effects, in cluding headaches that are usually short-lived and responsive to aspirin effects, in cluding headaches that are usually short-lived and responsive to aspirin compounds. Other frequent com plaints include nausea, vomiting, anorexia, compounds. Other frequent com plaints include nausea, vomiting, anorexia, nervousness, and depression. A typical dosing regimen is one nervousness, and depression. A typical dosing regimen is one 250 250 mg tablet mg tablet 3 3 or or 4 4 times daily (total dosage: times daily (total dosage: 10-15 10-15 mg/kg/d).mg/kg/d).

ORAL MEDICATIONSORAL MEDICATIONS
8. 8. Prevention of cystine calculiPrevention of cystine calculi——Conservative measures, including massive fluid Conservative measures, including massive fluid intake and urinary alkalinization, are frequently inadequate to control cystine stone intake and urinary alkalinization, are frequently inadequate to control cystine stone formation. Penicillamine, the same drug that is used to chelate excess copper in the formation. Penicillamine, the same drug that is used to chelate excess copper in the treatment of Wil son disease, undergoes a thiol-disulfide exchange with cystine. This treatment of Wil son disease, undergoes a thiol-disulfide exchange with cystine. This reduces the amount of urinary cystine that is relatively insoluble. Cystine solubility is reduces the amount of urinary cystine that is relatively insoluble. Cystine solubility is pH-depen-dent (pH pH-depen-dent (pH 5.0: 150-300 5.0: 150-300 mg/L; pH mg/L; pH 7.0: 200-400 7.0: 200-400 mg/L; pH mg/L; pH 7.5: 220-500 7.5: 220-500 mg/L). D-Penicillamine. is associated with numerous and frequent side effects, mg/L). D-Penicillamine. is associated with numerous and frequent side effects, including rashes and hematologic, renal, and hepatic abnormali ties. An initial dosage including rashes and hematologic, renal, and hepatic abnormali ties. An initial dosage of of 250 250 mg daily in mg daily in 3-4 3-4 divided doses may help reduce severe side effects. It may be divided doses may help reduce severe side effects. It may be in creased gradually to in creased gradually to 2 2 g/d. Dosage should be titrated with quantitative urinary g/d. Dosage should be titrated with quantitative urinary cystine values. Penicillamine increases the requirement of pyridoxine (vitamin B6), cystine values. Penicillamine increases the requirement of pyridoxine (vitamin B6), which should be supplemented with which should be supplemented with 25-50 25-50 mg/d.mg/d.Mercaptopropionylglycine (Thiola) is better toler ated by patients than is penicillamine. Mercaptopropionylglycine (Thiola) is better toler ated by patients than is penicillamine. Mercaptopropionylglycine, a reducing agent, binds to the sulfide por tion of cystine, Mercaptopropionylglycine, a reducing agent, binds to the sulfide por tion of cystine, forming a mixed disulfide (Thiolacysteine) water-soluble compound. It may retard the forming a mixed disulfide (Thiolacysteine) water-soluble compound. It may retard the rate of new stone formation. The dosage should be titrated with repeat 24-h urinary rate of new stone formation. The dosage should be titrated with repeat 24-h urinary cystine values. An initial dosage may be cystine values. An initial dosage may be 200-300 200-300 mg mg 3 3 times daily, either times daily, either 1 1 h before h before or or 2 2 h after each meal. Side effects are not in frequent and may include drug fever; h after each meal. Side effects are not in frequent and may include drug fever; nausea, vomiting, and gastrointestinal upset; rash, wrinkling, or friable skin; lupuslike nausea, vomiting, and gastrointestinal upset; rash, wrinkling, or friable skin; lupuslike symptoms, decreased taste perception; and a variety of hematologic disorders.symptoms, decreased taste perception; and a variety of hematologic disorders.

The The pump-room pump-room of of mineralmineral waterswaters in Morshinin Morshin
sanatorium-and-spa treatment