upha anticoagulation therapy update -...
TRANSCRIPT

4/13/15
1
An)coagula)on Therapy Update
Daniel M. Wi>, PharmD, FCCP, BCPS University of Utah College of Pharmacy
Outline
• Review of hemostasis & thrombosis • Overview of available an)coagulants • What to do following an)coagula)on therapy-‐related bleeding
• Choosing between available an)coagulants
J Thromb Haemost. 2003 Feb;1(2):227-‐30

4/13/15
2
Hemosta)c System
• Preserves integrity of circulatory system • A highly complex system
• Vessel wall (endothelial cells) • Soluble plasma proteins (cloZng factors) • Cellular components (platelets) • Micropar)cles ()ssue factor)
• Ac)vated by )ssue injury or changes in the endothelial surface
Overview
• Hemostasis is the arrest of bleeding following blood vessel damage
• Rapid forma)on of impermeable platelet and fibrin plug at site of injury
• Localized to site of injury • Fibrin within clot triggers its own dissolu)on (fibrinolysis)
• Pathologic thrombus = normal regulatory controls overwhelmed
A Clot is Formed
Red = platelets
Green = )ssue factor
White = platelets + fibrin + )ssue factor
Blue = fibrin
Platelet thrombus and fibrin deposi3on occur at the same 3me
N Engl J Med 2008;359:938-‐49

4/13/15
3
Platelet Thrombus Forma)on
• Dynamic process influenced by shear, flow, turbulence and number of platelets in circula)on
• Platelet ac)va)on (by collagen or )ssue factor) results in the release of components cri)cal for thrombus forma)on and platelet-‐platelet interac)on
Thromb Haemost 2013; 110: 859–867
Coagula)on Complexes
(An)coagulant complex)
Co-‐factor
Enzyme
Substrate(s)
Blood Cells, Molecules, and Diseases 36 (2006) 108 – 117
Tissue Factor
• Membrane protein • Present on many cells/has many func)ons
• Present in vessel wall • Can be expressed on monocytes and endothelium • Present in circula)ng blood (micropar)cles)
• Blood-‐borne TF captured in thrombus via interac)ons between P-‐selec)n/PSGL-‐1

4/13/15
4
• TF may circulate in ac)ve and inac)ve forms • Inac)ve TF requires ac)va)on at the site of vascular injury
• Pathologic micropar)cles may bear ac)ve TF • Fibrin is the end product of the coagula)on cascade
The Coagula)on Cascade
X
Xa Va
XII HMK PK
VIIa Tissue Factor
IXa VIIIa IX
XI XIa
Prothrombin (II) Thrombin (IIa)
‘Common Pathway’
‘Extrinsic Pathway’
‘Intrinsic Pathway’
Does NOT explain how blood clots in vivo
The Coagula)on Cascade
X
Xa Va
XII HMK PK
VIIa Tissue Factor
IXa VIIIa IX
XI XIa
Prothrombin (II) Thrombin (IIa)
‘Common Pathway’
‘Extrinsic Pathway’
‘Intrinsic Pathway’ Deficiency results in increased PTT but no bleeding tendency
Deficiency results in increased PTT and
hemophilia
Unable to sustain hemostasis in hemophilia

4/13/15
5
Cellular Model of Clot Forma)on
Thromb Haemost 2013; 109: 569–579
Ini)a)on Phase • Ac)vated )ssue factor is the fuse • TF/VIIa complex ac)vates small
amounts of IX and X • Xa then associates with Va to form
prothrombinase complex • A small amount of thrombin is
produced • Tissue Factor Pathway Inhibitor
• Neutralizes Xa • Feedback inhibi)on on TF/VIIa in
presence of Xa
Thromb Haemost 2013; 109: 569–579
Amplifica)on Phase
• Low concentra)ons of thrombin ac)vate platelets adhering to injury site
• Thrombin ac)vates V, VIII, and XI • Va, VIIIa, and XIa bind to surfaces
of ac)vated platelets
Thromb Haemost 2013; 109: 569–579

4/13/15
6
Propaga)on Phase
• Intrinsic tenase and prothrombinase assemble on surface of ac)vated platelets
• XIa ac)vates IX to form addi)onal intrinsic tenase
• Burst of thrombin • Fibrin generated and stabilized by
XIIIa
Thromb Haemost 2013; 109: 569–579
This is what fibrin looks like…
Thromb Haemost 2010; 104: 1281–1284
Termina)on
• Coagula)on reac)ons are likely terminated when fibrin deposi)on ‘paves over’ the site of injury
• Fresh components of coagula)on reac)ons are no longer able to access the site
• Protein C/S & AT limit thrombus to site of injury

4/13/15
7
Modula)on
Prothrombin Thrombin
Fibrinogen Fibrin
FXII
FX
FXI
FIX
FXa
FVIII FV
TFPI
AT
PS PC
FVII
Endogenous An)coagulant Mechanisms
• An)thrombin • Inhibits only free enzymes • Limits coagula)on to site of injury
• Thrombomodulin • Ac)vates protein C
• Protein C • Modulates ac)vity of FVa & VIIIa (even when part of intrinsic tenase and
prothrombinase complexes) • Limits coagula)on to site of injury
• Protein S • Supports ac)vity of protein C
• Tissue Factor Pathway Inhibitor (TFPI) • Inhibits FXa and TF/VIIa complex
Thrombolysis
Fibrinogen (circula3on) Fibrin
(thrombus)
Alpha2 An)plasmin
tPA
Plasmin Plasminogen
Plasminogen Ac)vator Inhibitor (PAI-‐1)
(Binds and inac)vates plasmin)
(Circula)ng inac)ve
precursor)
(Cleaves bonds in fibrin and fibrinogen)
(Binds and inac)vates tPA)
(Physiologic ac)vator of plasminogen)

4/13/15
8
UFH/LMWH/Fondaparinux
Prothrombin Thrombin
Fibrinogen Fibrin
FXII
FX
FXI
FIX
FXa
FVIII FV
TFPI
AT
PS PC
FVII
LMWH
Fondaparinux
Xa
1
AT AT
2 3
AT
4
AT Thrombin
Xa
1
AT AT
2 3
AT
4
AT Thrombin
Xa
1
AT AT
2 3
AT
4
AT Thrombin
Unfrac3onated Heparin
UFH/LMWH/Fondaparinux

4/13/15
9
UFH/LMWH/Fondaparinux
UFH LMWH Fondaparinux
Monitoring aPTT
Platelet count Platelet count Renal func)on
Platelet count Renal func)on
Variability of response Yes Rela)vely low Rela)vely low
Primary Route of Elimina3on
1. Saturable binding
2. Renal Renal Renal
Reversal Agent Yes Par)al No
HIT Postop: <1% -‐ 5% Med/OB: <1%
Postop: <1% Med/OB: <0.1%
No
Warfarin
Prothrombin Thrombin
Fibrinogen Fibrin
FXII
FX
FXI
FIX
FXa
FVIII FV
TFPI
AT
PS PC
FVII
Warfarin Pharmacokine)cs
Half-‐life ≈ 36 hrs
Time to steady state ≈
3-‐5 half-‐lives
108-‐180 hrs OR 4.5-‐7.5 days
4/13/15
10
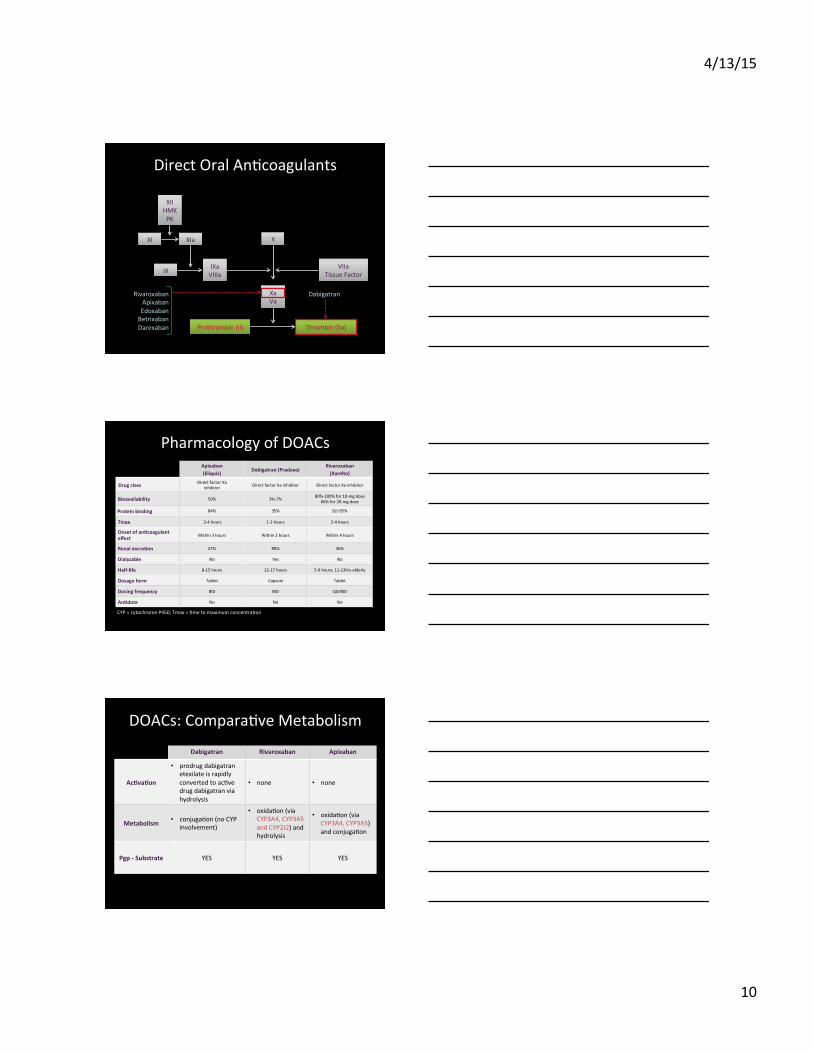
Direct Oral An)coagulants
X
Xa Va
XII HMK PK
VIIa Tissue Factor
IXa VIIIa IX
XI XIa
Prothrombin (II) Thrombin (IIa)
Rivaroxaban Apixaban Edoxaban Betrixaban Darexaban
Dabigatran
Pharmacology of DOACs
CYP = cytochrome P450; Tmax = )me to maximum concentra)on
Apixaban (Eliquis)
Dabigatran (Pradaxa) Rivaroxaban (Xarelto)
Drug class Direct factor Xa inhibitor Direct factor IIa inhibitor Direct factor Xa inhibitor
Bioavailability 50% 3%-‐7% 80%-‐100% for 10-‐mg dose 66% for 20-‐mg dose
Protein binding 84% 35% 92–95%
Tmax 3-‐4 hours 1-‐2 hours 2-‐4 hours
Onset of an3coagulant effect Within 3 hours Within 2 hours Within 4 hours
Renal excre3on 27% 80% 36%
Dialyzable No Yes No
Half-‐life 8-‐15 hours 12-‐17 hours 5-‐9 hours; 11-‐13hrs elderly
Dosage form Tablet Capsule Tablet
Dosing frequency BID BID QD/BID
An3dote No No No
DOACs: Compara)ve Metabolism
Dabigatran Rivaroxaban Apixaban
Ac3va3on
• prodrug dabigatran etexilate is rapidly converted to ac)ve drug dabigatran via hydrolysis
• none • none
Metabolism • conjuga)on (no CYP involvement)
• oxida)on (via CYP3A4, CYP3A5 and CYP2J2) and hydrolysis
• oxida)on (via CYP3A4, CYP3A5) and conjuga)on
Pgp -‐ Substrate YES YES YES

4/13/15
11
DOACs: A New Drug Interac)on Mindset
• Warfarin • Drug interac)ons can be managed through increased monitoring and dose adjustment
• Interac)ng drugs are not contraindicated
• DOACs • Drug interac)ons are contraindica)ons or precau)ons
• No ability to monitor and adjust dose based on response
DOACs: Formula)on Issues, Food Effects
Apixaban Dabigatran Rivaroxaban
Formula3on • No informa)on
• Capsules cannot be: crushed (no feeding tube), broken, or chewed
• Expires 4 mo awer bo>le is opened
• May be crushed and mixed with applesauce in a feeding tube (G-‐tube)
Food Effects • Bioavailability not affected by food
• May be taken with or without food
• 10-‐mg tablet: may be taken with/without food
• 15-‐mg and 20-‐mg tablets: should take with largest meal of the day
Case 1
A 77 year old man receiving warfarin for AF is admi>ed with a bleeding duodenal ulcer. He has a history of HTN and DM. He is discharged on omeprazole 20 mg daily. Should his warfarin be resumed? If yes, when?
4/13/15
12
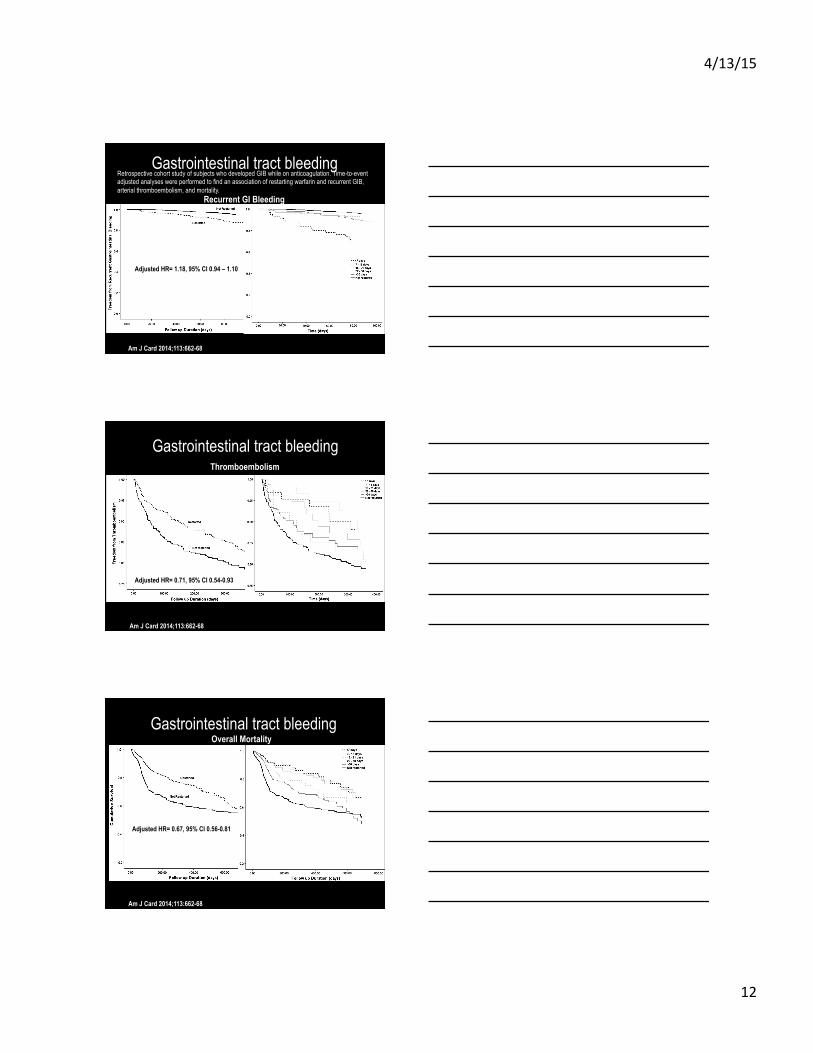
Gastrointestinal tract bleeding
Adjusted HR= 1.18, 95% CI 0.94 – 1.10
Recurrent GI Bleeding
Am J Card 2014;113:662-68
Retrospective cohort study of subjects who developed GIB while on anticoagulation. Time-to-event adjusted analyses were performed to find an association of restarting warfarin and recurrent GIB, arterial thromboembolism, and mortality.
Gastrointestinal tract bleeding
Am J Card 2014;113:662-68
Adjusted HR= 0.71, 95% CI 0.54-0.93
Thromboembolism
Gastrointestinal tract bleeding Overall Mortality
Am J Card 2014;113:662-68
Adjusted HR= 0.67, 95% CI 0.56-0.81
4/13/15
13
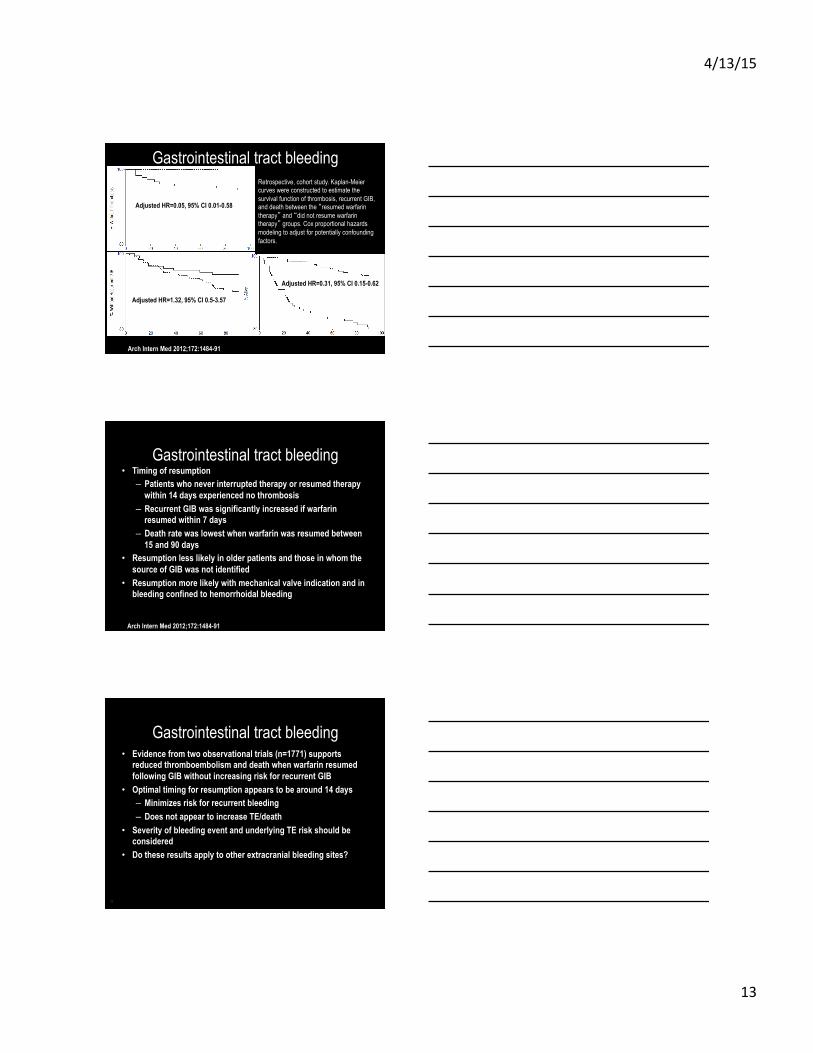
Gastrointestinal tract bleeding
Adjusted HR=0.31, 95% CI 0.15-0.62
Adjusted HR=1.32, 95% CI 0.5-3.57
Adjusted HR=0.05, 95% CI 0.01-0.58
Arch Intern Med 2012;172:1484-91
Retrospective, cohort study. Kaplan-Meier curves were constructed to estimate the survival function of thrombosis, recurrent GIB, and death between the “resumed warfarin therapy” and “did not resume warfarin therapy” groups. Cox proportional hazards modeling to adjust for potentially confounding factors.
Gastrointestinal tract bleeding • Timing of resumption
– Patients who never interrupted therapy or resumed therapy within 14 days experienced no thrombosis
– Recurrent GIB was significantly increased if warfarin resumed within 7 days
– Death rate was lowest when warfarin was resumed between 15 and 90 days
• Resumption less likely in older patients and those in whom the source of GIB was not identified
• Resumption more likely with mechanical valve indication and in bleeding confined to hemorrhoidal bleeding
Arch Intern Med 2012;172:1484-91
Gastrointestinal tract bleeding • Evidence from two observational trials (n=1771) supports
reduced thromboembolism and death when warfarin resumed following GIB without increasing risk for recurrent GIB
• Optimal timing for resumption appears to be around 14 days – Minimizes risk for recurrent bleeding – Does not appear to increase TE/death
• Severity of bleeding event and underlying TE risk should be considered
• Do these results apply to other extracranial bleeding sites?
39

4/13/15
14
Case 1
A 77 year old man receiving warfarin for AF is admi>ed with a bleeding duodenal ulcer. He has a history of HTN and DM. He is discharged on omeprazole 20 mg daily. Should his warfarin be resumed? If yes, when?
Case 2
A 55 year old man taking apixaban for treatment of a DVT sustained following knee replacement surgery 4 months ago is admi>ed with bloody stools and a hematocrit of 27%. He receives 2 units of packed RBCs. No source of bleeding is iden)fied. Should an)coagula)on therapy be resumed following discharge?
Case 3
A 62-year-old man who presents with an intracerebral hemorrhage (ICH) while taking warfarin for atrial fibrillation. His INR is 2.5. His CHADS score is 3. Should warfarin be restarted to decrease the risk of future thromboembolism?

4/13/15
15
Intracranial hemorrhage • The ‘BRAIN’ Study • Cohort of consecutive patients with warfarin-related ICH (intracerebral
[~1/3 lobar] or subarachnoid) • Among the 284 patients studied (mean age 74 ±12 years), warfarin was
restarted in-hospital in 91 patients (32%) • Mortality rates lower in those who restarted warfarin in-hospital: 31.9%
vs 54.4% (30-day, P < 0.001) and 48% vs 61% (1-year, P = 0.04), and bleeding not increased
• Multivariable predictors of mortality: – Restarted warfarin in-hospital (30-day OR 0.49, 95% CI 0.26-0.93) – Intraventricular hemorrhage (30-day OR 2.19, 95% CI 1.09-4.40) – CNS <7 (more severe stroke) (30-day OR 6.04, 95% CI 3.32-10.97) – INR >3.0 at presentation (30-day OR 3.28, 95% CI 1.66-6.49)
Can J Card 2012;28:33–39
Intracranial Hemorrhage
Intracranial hemorrhage Factors arguing for and against resuming anticoagulation after ICH FACTOR FOR AGAINST Etiology HTN-related ICH (deep), BP adequately controlled Cerebral amyloid angiopathy (lobar) Microvascular risk Microbleeds on gradient-echo MRI Indication for anticoagulation Secondary prevention Primary prevention Atrial fibrillation, CHADS2 ≥ 4 or CHA2DS2-VASc ≥ 5 Atrial fibrillation, low CHADS2 < 4 or CHA2DS2-VASc < 5 Mechanical heart valve Thrombophilia (protein S/C/antithrombin deficiency; APLA) Anticipated difficulty managing anticoagulation
X X X X X
X X X X X
CCJM 2010;77:791-99

4/13/15
16
Case 3
A 62-year-old man who presents with an intracerebral hemorrhage (ICH) while taking warfarin for atrial fibrillation. His INR is 2.5. His CHADS score is 3. Should warfarin be restarted to decrease the risk of future thromboembolism?
Case 4
A 66 year old woman with history of HTN and CAD is diagnosed with symptoma)c atrial fibrilla)on. Her ventricular rate is controlled with verapamil and amiodarone is started for rhythm control. She takes ASA 81 mg daily for her stable CAD. Is an)coagula)on therapy indicated? If yes, which agent should be selected?
Beyond INR-‐based Dose Adjustment
• Is an)coagulant therapy appropriate for my pa)ent? • Does the benefit outweigh the bleeding risk? • Are the financial and lifestyle costs jus)fied?
• Is my pa)ent on the CORRECT an)coagulant? • Can I make an)coagulant therapy safer for my pa)ent?

4/13/15
17
Atrial Fibrilla)on
• Assess stroke and bleeding risk • Withhold/discon)nue AC therapy in the rare pa)ent for whom it would not be beneficial
• Reduce bleeding risk • Be familiar with all therapeu)c op)ons
Lew Atrial Appendage (LAA)
CHADS2: Risk of Stroke Na)onal Registry of Atrial Fibrilla)on Par)cipants (NRAF)
Scoring: 1 point: Conges)ve heart failure, HTN, ≥ 75 years, and DM 2 points: Stroke history or transient ischemic a>ack † Expected stroke rate per 100 pt-‐yrs from the exponen)al survival model, assuming aspirin not taken
CHADS2 Score # Pa3ents (n = 1733)
# Strokes (n = 94)
NRAF Crude Stroke Rate per 100 Pa3ent-‐yrs
NRAF Adjusted Stroke Rate (95%
CI)†
0 120 2 1.2 1.9 (1.2-‐3.0)
1 463 17 2.8 2.8 (2.0-‐3.8)
2 523 23 3.6 4.0 (3.1-‐5.1)
3 337 25 6.4 5.9 (4.6-‐7.3)
4 220 19 8.0 8.5 (6.3-‐11.1)
5 65 6 7.7 12.5 (8.2-‐17.5)
6 5 2 44.0 18.2 (10.5-‐27.4)
Gage BF, Waterman AD, Shannon W, Boechler M, Rich MW, Radford MJ. JAMA. 2001 Jun 13;285(22):2864-‐70. Pub Med PMID: 11401607.
4/13/15
18
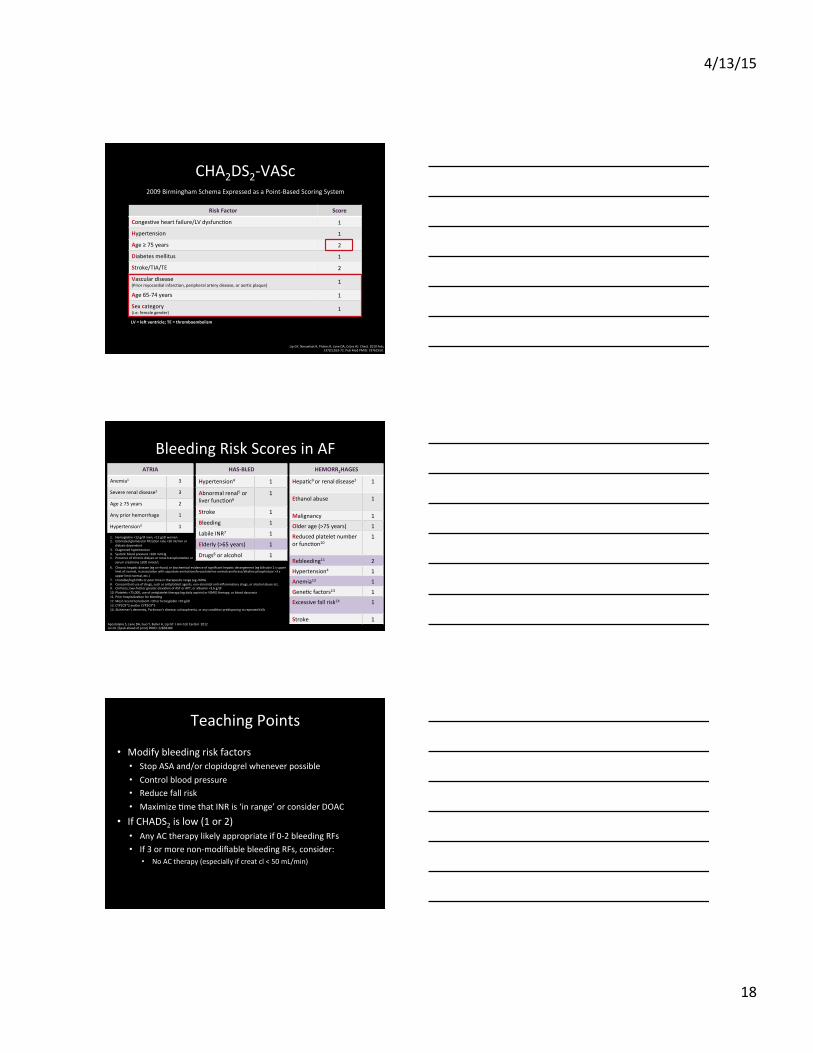
Risk Factor Score
Conges)ve heart failure/LV dysfunc)on 1
Hypertension 1
Age ≥ 75 years 2
Diabetes mellitus 1
Stroke/TIA/TE 2
Vascular disease (Prior myocardial infarc)on, peripheral artery disease, or aor)c plaque)
1
Age 65-‐74 years 1
Sex category (i.e. female gender)
1
CHA2DS2-‐VASc 2009 Birmingham Schema Expressed as a Point-‐Based Scoring System
LV = leh ventricle; TE = thromboembolism
Lip GY, Nieuwlaat R, Pisters R, Lane DA, Crijns HJ. Chest. 2010 Feb;137(2):263-‐72. Pub Med PMID: 19762550.
Bleeding Risk Scores in AF
1. Hemoglobin <13 g/dl men; <12 g/dl women 2. Es)mated glomerular filtra)on rate <30 ml/min or
dialysis-‐dependent 3. Diagnosed hypertension 4. Systolic blood pressure >160 mmHg 5. Presence of chronic dialysis or renal transplanta)on or
serum crea)nine ≥200 mmol/L 6. Chronic hepa)c disease (eg cirrhosis) or biochemical evidence of significant hepa)c derangement (eg bilirubin 2 x upper
limit of normal, in associa)on with aspartate aminotransferase/alanine aminotransferase/alkaline phosphatase >3 x upper limit normal, etc.)
7. Unstable/high INRs or poor )me in therapeu)c range (eg <60%) 8. Concomitant use of drugs, such as an)platelet agents, non-‐steroidal an)-‐inflammatory drugs, or alcohol abuse etc. 9. Cirrhosis, two-‐fold or greater eleva)on of AST or APT, or albumin <3.6 g/dl 10. Platelets <75,000, use of an)platelet therapy (eg daily aspirin) or NSAID therapy; or blood dyscrasia 11. Prior hospitaliza)on for bleeding 12. Most recent hematocrit <30 or hemoglobin <10 g/dl 13. CYP2C9*2 and/or CYP2C9*3 14. Alzheimer's demen)a, Parkinson's disease, schizophrenia, or any condi)on predisposing to repeated falls
ATRIA
Anemia1 3
Severe renal disease2 3
Age ≥ 75 years 2
Any prior hemorrhage 1
Hypertension3 1
HAS-‐BLED
Hypertension4 1
Abnormal renal5 or liver func)on6
1
Stroke 1
Bleeding 1
Labile INR7 1
Elderly (>65 years) 1
Drugs8 or alcohol 1
HEMORR2HAGES
Hepa)c9 or renal disease2 1
Ethanol abuse 1
Malignancy 1
Older age (>75 years) 1
Reduced platelet number or func)on10
1
Rebleeding11 2
Hypertension4 1
Anemia12 1
Gene)c factors13 1
Excessive fall risk14 1
Stroke 1 Apostolakis S, Lane DA, Guo Y, Buller H, Lip GY. J Am Coll Cardiol. 2012 Jul 24. [Epub ahead of print] PMID: 22858389
Teaching Points
• Modify bleeding risk factors • Stop ASA and/or clopidogrel whenever possible • Control blood pressure • Reduce fall risk • Maximize )me that INR is ‘in range’ or consider DOAC
• If CHADS2 is low (1 or 2) • Any AC therapy likely appropriate if 0-‐2 bleeding RFs • If 3 or more non-‐modifiable bleeding RFs, consider:
• No AC therapy (especially if creat cl < 50 mL/min)

4/13/15
19
Meta-‐analysis of Efficacy and Safety of Direct Oral An)coagulants
Dabigatran, Rivaroxaban, Apixaban, Edoxaban vs. Warfarin in AF pa)ents
All cause stroke/SE
Ruff et al. Epub.December 4, 2013 hlp://dx.doi.org/10.1016/S0140-‐6736(13)62343-‐0
Meta-‐analysis of Efficacy and Safety of Direct Oral An)coagulants
Dabigatran, Rivaroxaban, Apixaban vs. Warfarin in AF pa)ents
Major Bleeding
Ruff et al. Epub.December 4, 2013 hlp://dx.doi.org/10.1016/S0140-‐6736(13)62343-‐0
Meta-‐analysis of Efficacy and Safety of Direct Oral An)coagulants
Dabigatran, Rivaroxaban, Apixaban, Edoxaban vs. Warfarin in AF pa)ents
Secondary Safety and Efficacy Outcomes
Ruff et al. Epub.December 4, 2013 hlp://dx.doi.org/10.1016/S0140-‐6736(13)62343-‐0

4/13/15
20
Case 4
A 66 year old woman with history of HTN and CAD is diagnosed with symptoma)c atrial fibrilla)on. Her ventricular rate is controlled with verapamil and amiodarone is started for rhythm control. She takes ASA 81 mg daily for her stable CAD. Is an)coagula)on therapy indicated? If yes, which agent should be selected?
Case 5
A 48 year old man is diagnosed with a popliteal DVT. He recently had reconstruc)ve knee surgery following an injury sustained on his job as a roughneck on an offshore oil pla�orm. He has no other health problems and is on no other medica)ons. What would be the best plan for star)ng an)coagula)on therapy for this pa)ent?
DVT/PE: Goals of Therapy
Acute Phase (≥ 5 days)
Chronic Phase (≥ 3 months)
Relieve symptoms Avoid Recurrence (new clot)
Prevent emboliza)on Minimize risk of post-‐thrombo)c syndrome chronic. Pulm HTN Avoid clot extension/
forma)on

4/13/15
21
Tradi)onal/Standard Therapy
• Warfarin target INR 2-‐3 with 5 day overlap using – Heparin – LMWH – Fondaparinux
Acute VTE Treatment: Summary
Trial Name Drug Year Published
Heparin/ LMWH at start
HR or RR: Recurrent VTE vs. warfarin (95% CI)
HR: Major Bleeding vs. warfarin (95% CI)
RE-‐COVER (DVT and/or PE) dabi 2009 Yes 1.10
(0.65 -‐ 1.84) 0.82
(0.45 -‐ 1.48)
RE-‐COVER II dabi 2013 Yes 1.08 (0.64 -‐ 1.80)
0.69 (0.36 to 1.32)
EINSTEIN DVT riva 2010 No 0.68 (0.44 -‐ 1.04)
0.65 (0.33 -‐ 1.30)
EINSTEIN PE riva 2012 No 1.12 (0.75 -‐ 1.68)
0.49 (0.31 -‐ 0.79)
AMPLIFY apix 2013 No 0.84 (0.60 -‐ 1.18)
0.31 (0.17 -‐ 0.55)
HOKUSAI edox 2013 Yes 0.89 (0.70 – 1.13)
0.84 (0.59 – 1.21)
Op)mal Candidates for DOACs
• Pa)ents who: • Have difficulty geZng INR tes)ng or, despite adherence to recommenda)ons, have low ‘)me-‐in-‐range’
• Can afford (or arrange to get) them • Are not taking medica)ons known to interact with the new an)coagulants
• Have normal renal func)on • Do not have cancer, APS • Not pregnant
4/13/15
22
Case 5
A 48 year old man is diagnosed with a popliteal DVT. He recently had reconstruc)ve knee surgery following an injury sustained on his job as a roughneck on an offshore oil pla�orm. He has no other health problems and is on no other medica)ons. What would be the best plan for star)ng an)coagula)on therapy for this pa)ent?
Ques)ons?
Thank you for a>ending!