updates from recent international meeting husain a alawadhi md senior consultant hamad general...
TRANSCRIPT

Updates from Updates from recent recent
International International MeetingMeeting
Husain A Alawadhi MD Husain A Alawadhi MD Senior ConsultantSenior Consultant
Hamad General HospitalHamad General HospitalDoha, QatarDoha, Qatar


Professor Jean-Louis VincentProfessor Jean-Louis Vincent

www.mecriticalcare.netwww.mecriticalcare.net
I HAVE TO SAY:I HAVE TO SAY:
30 MINUTES ≠ 4 DAYS30 MINUTES ≠ 4 DAYS MANY ALREADY PRESENTEDMANY ALREADY PRESENTED NO SLIDES AVAILABLE NO SLIDES AVAILABLE NEWNEW A flower from each “bustan”A flower from each “bustan”


What is the main language in What is the main language in Belgium? One or more than one Belgium? One or more than one
answeranswer . .
1.1. Belgish (Belgium) language?Belgish (Belgium) language?
2.2. English language ?English language ?
3.3. Euro language ?Euro language ?

Diamond Diamond ChocoltaeChocoltae
STREPTOCOCCAL STREPTOCOCCAL INFECTION and XYGRIS INFECTION and XYGRIS UpdateUpdate

KIDNEYKIDNEYThank youThank you
Prevention of AKIPrevention of AKI Diagnosis of AKIDiagnosis of AKI Treatment of AKITreatment of AKI

Claudio Ronco is Professor Claudio Ronco is Professor of Clinical Nephrology of Clinical Nephrology

Still using RIFLE criteriaStill using RIFLE criteria
As of 2010 , what can As of 2010 , what can protect the kidney ?protect the kidney ?

Alkaline phosphatase (AP) attenuates inflammatory responses by Alkaline phosphatase (AP) attenuates inflammatory responses by lipopolysaccharide detoxification and may prevent organ damage lipopolysaccharide detoxification and may prevent organ damage
during sepsis.during sepsis. Dr peter PikkersDr peter Pikkers

Results Results
The 28-day overall mortality after The 28-day overall mortality after inclusion in the AP-treated group was inclusion in the AP-treated group was 24%, compared with 36% in the 24%, compared with 36% in the placebo-treated group (placebo-treated group (pp = 0.45). = 0.45).
The mortality rate in patients with AKI The mortality rate in patients with AKI tended to be tended to be lowerlower in the AP group in the AP group relative to the placebo group (AP = relative to the placebo group (AP = 27%; placebo = 60%; 27%; placebo = 60%; pp = 0.21). = 0.21).


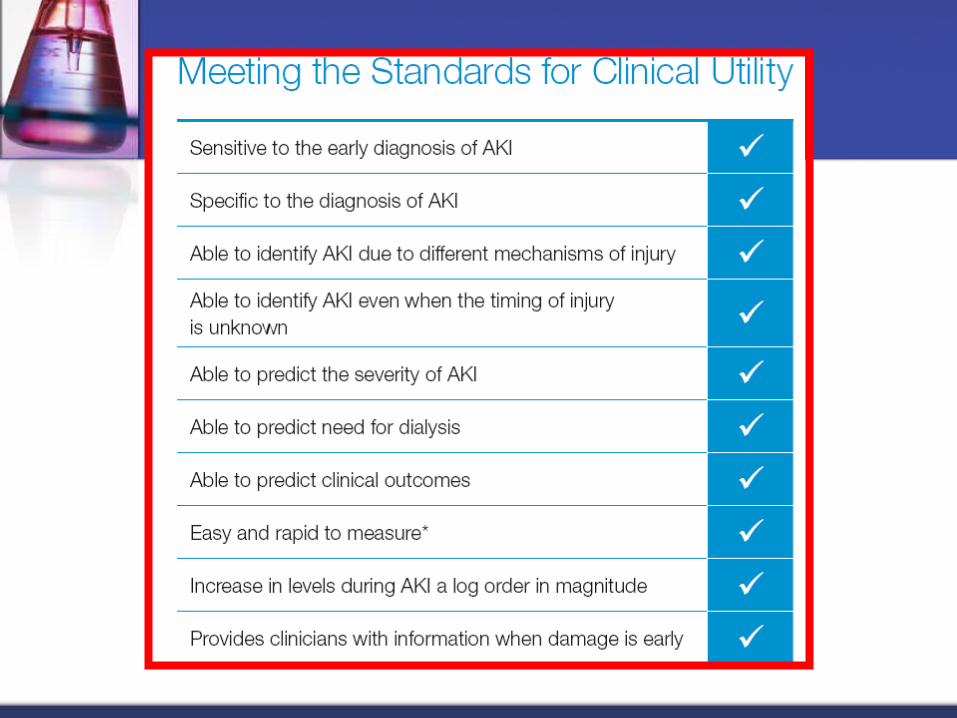
Diagnosis of AKIDiagnosis of AKI




Treatment : Treatment : TIMINGTIMING
We do not know, what is the BEST TIME We do not know, what is the BEST TIME to start hemodialysis .to start hemodialysis .
( ( BESTBEST study ). study ). BBeginning and eginning and EEnding nding SSupportive upportive TTherapy for Kidney. a herapy for Kidney. a multicenter study in 23 countries JAMA multicenter study in 23 countries JAMA 2005: 813-818.2005: 813-818.
Met analysis suggested Early initiation Met analysis suggested Early initiation may have better outcome .Am J Kidney may have better outcome .Am J Kidney Dis 2008 : 52 272-284.Dis 2008 : 52 272-284.
Clin J Am Soc Nephrol 3: 876-880, 2008

Conclusions: 20 ML/KG = 35
ML/KG
ConclusionsIntensive renal support in critically ill patients with acute kidney injury did not decrease
mortality, improve recovery of kidney function, or reduce the rate of nonrenalorgan failure as compared with less-intensive therapy involving a defined dose of
intermittent hemodialysis three times per week and continuous renal-replacement therapyat 20 ml per kilogram per hour.
25 ML/KG = 40 ML/KG25 ML/KG = 40 ML/KG
Conclusions In critically ill patients with acute kidney injury, treatment with higher-intensity continuous renal-replacement
therapy did not reduce mortality at 90 days.
TREATMENT OF AKI : TREATMENT OF AKI :
2010 2010
Haemofiltration Study : Haemofiltration Study : IVOIREIVOIRE (hIgh VOlume in Intensive Care(hIgh VOlume in Intensive Care : :
Early high voume (70 ml/kg/h) VS Early high voume (70 ml/kg/h) VS (35 ml/kg/h) (35 ml/kg/h)

What are the new things for the heart ?
1-learn ECHO
2-External machine
ECHO by Non cardiologist

Intra-Aortic Balloon Pump (IABP).
04/19/2329

Intra-Aortic Balloon Pump (IABP)
-. -. It is inserted into the descending It is inserted into the descending
aorta via the femoral artery either aorta via the femoral artery either percutaneously or by surgical cut-percutaneously or by surgical cut-down.down.
The balloon rapidly deflates just The balloon rapidly deflates just before ventricular systole to reduce before ventricular systole to reduce the impedance (A measure of the the impedance (A measure of the total opposition to current flow in an total opposition to current flow in an alternating current circuit) to left alternating current circuit) to left ventricular ejectionventricular ejection
04/19/2330

No we can do it from No we can do it from outsideoutside

Enhanced External Enhanced External CounterpulsationCounterpulsation
Counterpulsation from outside

Neurohormonal ReleaseIncreases: NO, ANPDeceases: BNP, ET-1, ACE, ANG II
Hemodynamic Effects of EECPIncrease Cardiac Output
Systolic unloading
Increase Venous return
DiastolicRetrograde Flow
Diastolic Augmentation
Increase Shear Stress on endothelium
Increase coronary Perfusion
Pressure Gradients
occlusion
Enhance Collateral capillary sprouting
Improve Diastolic Filling
Remodeling
Release of Growth Factors
Angiogenesis andArteriogenesis
Improve Endothelial Function
Postulated Mechanisms of Action

HOW TO PROTECT HOW TO PROTECT THE LUNG THE LUNG FURTHER FROM FURTHER FROM Ventilator InjuryVentilator Injury
HFOVHFOV
Lung protectiv strategyLung protectiv strategy. . ARDSnet protocolARDSnet protocol
EEnsures oxygenation without causing nsures oxygenation without causing further damage to the lung or other further damage to the lung or other organsorgans. . it's always a priority!it's always a priority!
- - low tidal volumelow tidal volume ( (6 ml/kg in 6 ml/kg in ALI/ARDS)ALI/ARDS)>>permissive Hypercapnea>>permissive Hypercapnea
- - limited alveolar pressurelimited alveolar pressure ( (<< 30-35 30-35 mHmH22O)O) >> permissive hypercapnea >> permissive hypercapnea


Figure 2. The normal alveolus compared with the injured alveolus in the early phase of ALI and ARDS. Under the influence of proinflammatory cytokines such as IL-8, IL-1, and TNF, neutrophils initially undergo sequestration in the pulmonary microvasculature, followed by margination and egress into the alveolar space, where they undergo activation. Activated neutrophils release a variety of factors(leukotrienes, oxidants, proteases, and PAF) which contribute to local tissue damage, accumulation of edema fluid in the airspaces, surfactant inactivation, and hyaline membrane formation. Macrophage inhibitory factor (MIF) released into the local milieu sustains the ongoing pro-inflammatory response. Subsequently, the release of macrophage-derived fibrogenic cytokines (TGF-β and PDGF) stimulate fibroblast growth and collagen deposition a/w the healing phase of injury.

Giving oxygen = OxygenationGiving oxygen = Oxygenation Washing Co2 = ventilationWashing Co2 = ventilation
Can we wash Co2 without ventilator??Can we wash Co2 without ventilator?? Since the word capnograpghy = Since the word capnograpghy =
monitoring Co2, we can make a new monitoring Co2, we can make a new word in medical terminology .word in medical terminology .

Washing Co2 from Washing Co2 from inside IVCinside IVC

Prof Welte TobiasProf Welte Tobias

20082008


LUNG ASSISTANT DEVICELUNG ASSISTANT DEVICE iLA Membrane Ventilator®iLA Membrane Ventilator®


INDICATION ( as per INDICATION ( as per company)company)
1.1. COPDCOPD
2.2. VENTILATOR WEANINGVENTILATOR WEANING
3.3. ARDS/ALIARDS/ALI
4.4. BRIDGE TO TRANSPLANATTIONBRIDGE TO TRANSPLANATTION
5.5. INCREASED ICPINCREASED ICP
6.6. BRONCHOPLEURAL FISTULASBRONCHOPLEURAL FISTULAS
7.7. INTENSIVE CARE TRANSPORATIONINTENSIVE CARE TRANSPORATION


Decapneization, in Decapneization, in summarysummary
Lung assistant deviceLung assistant device Extracorporeal Ventilation( NOT ECMO)Extracorporeal Ventilation( NOT ECMO) Rest lungRest lung No ventilator induced Lung InjuryNo ventilator induced Lung Injury Can be used to prevent INTUBATIONCan be used to prevent INTUBATION Can be used during VENTILATIONCan be used during VENTILATION Can be used during Weaning Can be used during Weaning Can be used Post EXTUBATION , to avoid re-Can be used Post EXTUBATION , to avoid re-
intubationintubation Less intubation =Less sedation= less infectionLess intubation =Less sedation= less infection

What is good for the What is good for the brain ? brain ?

Cool the brain after cardiac arrest or severe raised ICP


Hypertonic Saline 23.4%
Improves CPP and brain tissue O2 levels
Decreased ICP by 35% (8-10 mm HG) CPP increased by 14% MAP remained stable Greatest benefit in those with higher
ICP and lower CPP Repeated doses were not associated
with rebound, hypovolemia or HTN 30 mL of 23.4% over 15 minutes

DEAD SEA :33.7% salinity
On comparison, seawater in the world's oceans has a salinity of about 3.5%.
H1 N1 influenza virus H1 N1 influenza virus
Invasive Streptococcal Invasive Streptococcal DiseaseDisease

H1N1 peak is coming H1N1 peak is coming down.down.
Literature is full Literature is full about this outbreak.about this outbreak.
Some publications Some publications suggested a benefit suggested a benefit role of role of HFOVHFOV..
We have to look We have to look gain in depth to gain in depth to HFOV HFOV in our ARDS in our ARDS patients. patients.
IF YOU NEED MORE IF YOU NEED MORE INFORMATION ABOUT H1N1INFORMATION ABOUT H1N1

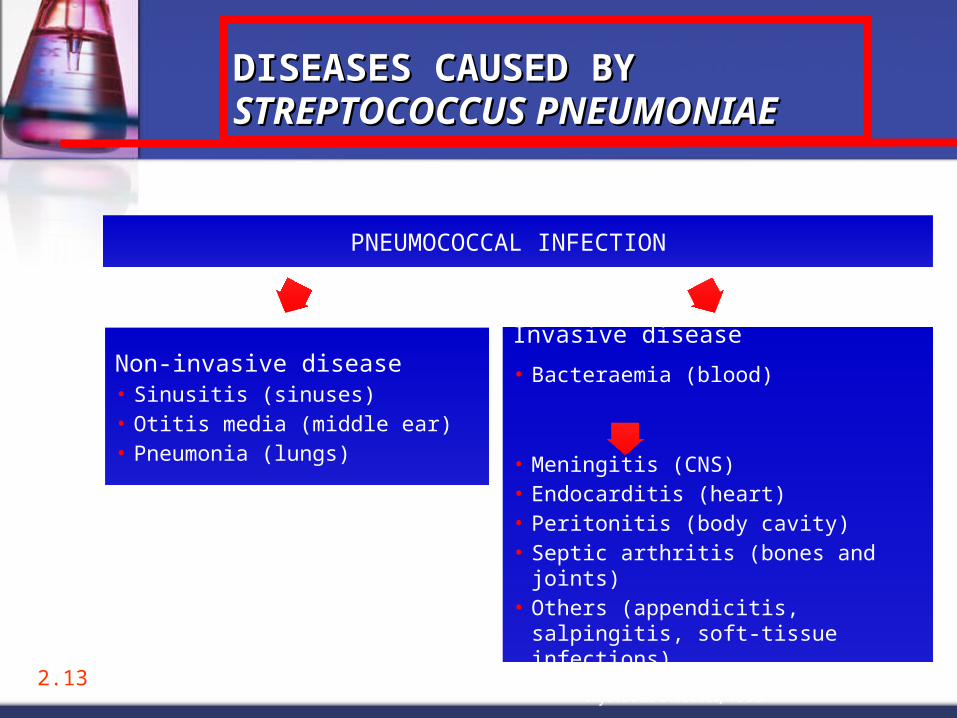
DISEASES CAUSED BY DISEASES CAUSED BY STREPTOCOCCUS STREPTOCOCCUS PNEUMONIAEPNEUMONIAE
Non-invasive disease• Sinusitis (sinuses)• Otitis media (middle ear)• Pneumonia (lungs)
Musher, in Principles and Practice of Infectious Diseases, 1995
Invasive disease
• Bacteraemia (blood)
• Meningitis (CNS)• Endocarditis (heart)• Peritonitis (body cavity)• Septic arthritis (bones and joints)• Others (appendicitis, salpingitis,
soft-tissue infections)
PNEUMOCOCCAL INFECTION
2.13

Michael Michael Niederman MDNiederman MD
: 448 pages 636 pages

Start combination Start combination Antistreptoccocal Antistreptoccocal antibiotics.antibiotics.Michael nidermanMichael niderman “ “
REASON one : The REASON one : The streptococcus may be streptococcus may be PCN resistant. So dual PCN resistant. So dual therapy will overcome therapy will overcome this , in the first 72 this , in the first 72 critical hours.critical hours.
REASON two : IPD fatality REASON two : IPD fatality is high in the first few is high in the first few days, so combination days, so combination therapy is recommended therapy is recommended for for SHORTSHORT period of time period of time ,until pt improves ,until pt improves clinically .clinically .

Treatment outcome Treatment outcome
Overall mortality rates for patients with Overall mortality rates for patients with pneumococcal Bacteremia have pneumococcal Bacteremia have consistently ranged from consistently ranged from 15 to 20 %15 to 20 % in the in the antibiotic era.antibiotic era.
Death mainly in the first three days.Death mainly in the first three days. More death More death
if age >65 ( 15%-35%)if age >65 ( 15%-35%) severity if illness, severity if illness, underlying immunosuppressant.underlying immunosuppressant.
MONITORING YOUR MONITORING YOUR PATINTPATINT


Monitoring ISSUESMonitoring ISSUES
PA>>>> out if fashionPA>>>> out if fashion Noninvasive Technology >>>in Noninvasive Technology >>>in
fashionfashion Simple and non sophisticated>> Simple and non sophisticated>>
coming into fashioncoming into fashion LACTATELACTATE SVO2SVO2 TISSUE IS THE ISSUE TISSUE IS THE ISSUE



69 of 25
What is StOWhat is StO22? ?
SaO2 and SpO2
measure O2saturation in the arteries.
ScvO2 measures O2 saturation in
the superior vena cava. SvO2
measures O2 saturation in the
pulmonary artery.
StO2 measures O2 saturation in themicrocirculation where O2 diffuses to tissue cells. StO2 is a measure of tissue oxygenation and is a sensitive
indicator of tissue perfusion status.
InSpectra StO2
StO2 = hemoglobin oxygen saturation of the microcirculation
SaO2SpO2
ScvO2SvO2

InSpectra™ StO2 below 75% indicates serious hypoperfusion associated with MODS and death in trauma patients.1
InSpectra StO2 above 75% indicates adequate perfusion.1
InSpectra StO2 functions as well as base deficit1 and lactate2 in indicating hypoperfusion in trauma patients.
Reduced O2 Consumption??8
Clinical Range of StOClinical Range of StO22
1Cohn SM, Nathens AB, Moore FA, Rhee P, Puyana JC, Moore EE, Beilman GJ. Tissue Oxygen Saturation Predicts the Development of Organ Dysfunction During Traumatic Shock Resuscitation.
J Trauma. 2007:62(1):44-55.

71 of 25
The InSpectraThe InSpectraTMTM StO StO2 2
Tissue Oxygenation Tissue Oxygenation SystemSystem
NoninvasiveNoninvasive Easy to useEasy to use Fast responseFast response Readings unaffected byReadings unaffected by
AgeAge GenderGender EdemaEdema Skin pigmentationSkin pigmentation AdiposeAdipose
Operates in presence of Operates in presence of hypothermiahypothermia

X on the x drug ?Most likely No

Critical Care Med.Critical Care Med. 2008 Jan;36(1):296-327 2008 Jan;36(1):296-327
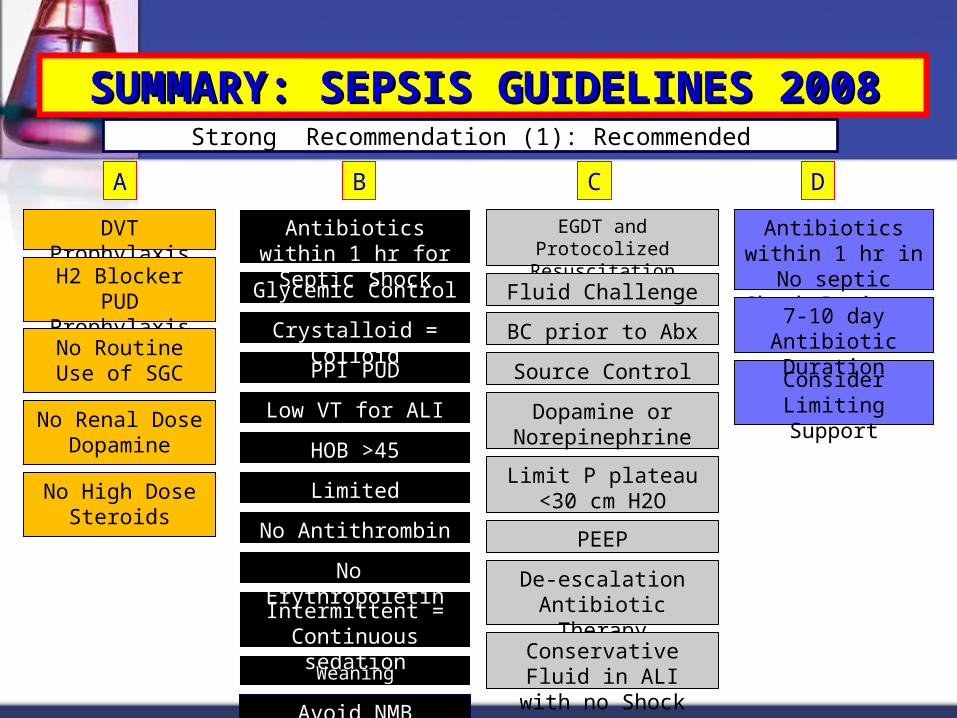
SUMMARY: SEPSIS GUIDELINES SUMMARY: SEPSIS GUIDELINES 20082008
Strong Recommendation (1): Recommended
DVT Prophylaxis
H2 Blocker PUD Prophylaxis
No Routine Use of SGC
A DCB
Glycemic Control
Consider Limiting Support
BC prior to Abx
Antibiotics within 1 hr for Septic Shock
EGDT and Protocolized Resuscitation
Antibiotics within 1 hr in No septic Shock Patients
De-escalation Antibiotic Therapy
7-10 day Antibiotic Duration
Source Control
Fluid Challenge
Dopamine or Norepinephrine
Limit P plateau <30 cm H2O
PEEP
Conservative Fluid in ALI with no Shock
No Renal Dose Dopamine
No High Dose Steroids
Weaning Protocol/SBT
Avoid NMB
PPI PUD Prophylaxis
Crystalloid = Colloid
Limited Transfusion
Low VT for ALI
HOB >45
Intermittent = Continuous sedation
No Antithrombin II
No Erythropoietin
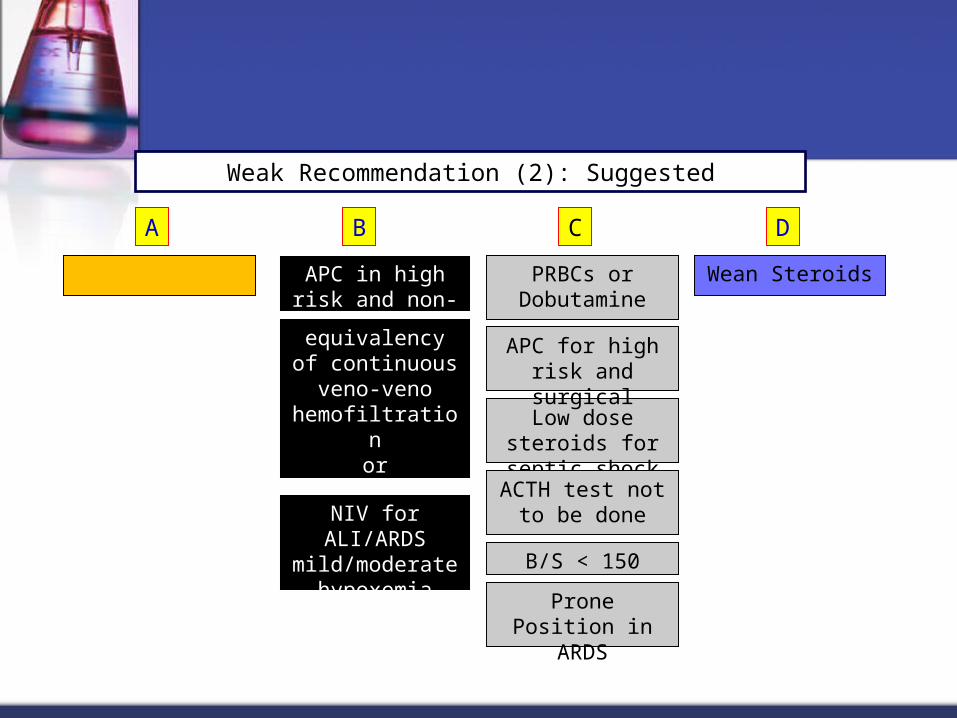
Weak Recommendation (2): Suggested
APC in high risk and non-surgical
A DCB
equivalencyof continuous
veno-veno hemofiltrationor intermittent hemodialysis
Wean Steroids
Low dose steroids for septic shock
B/S < 150
APC for high risk and surgical
PRBCs or Dobutamine
ACTH test not to be done
Prone Position in ARDS
NIV for ALI/ARDS mild/moderate
hypoxemia
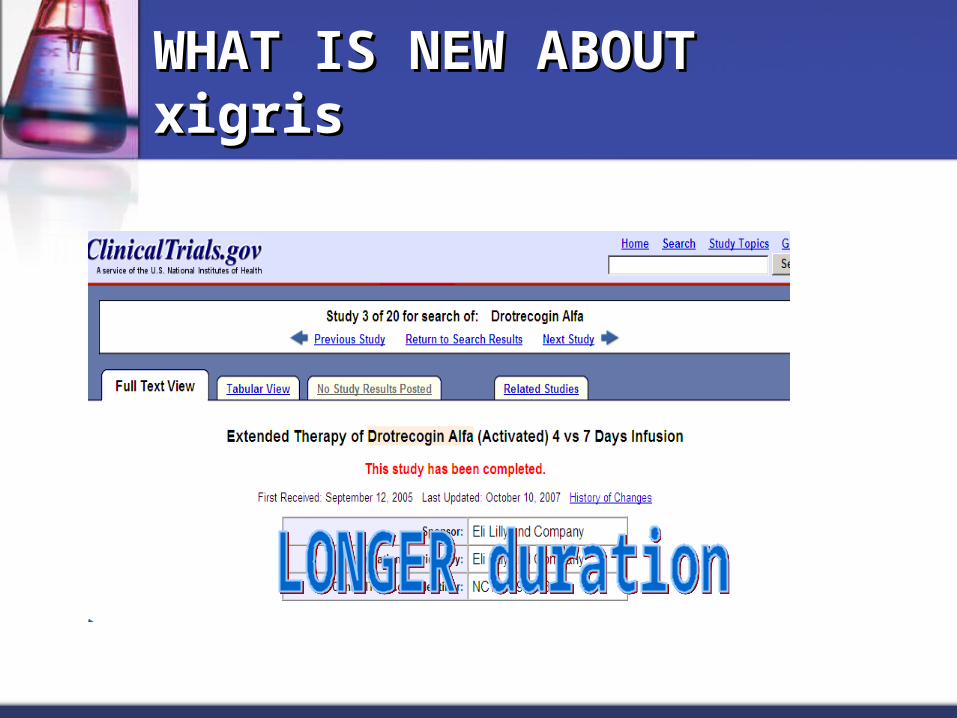
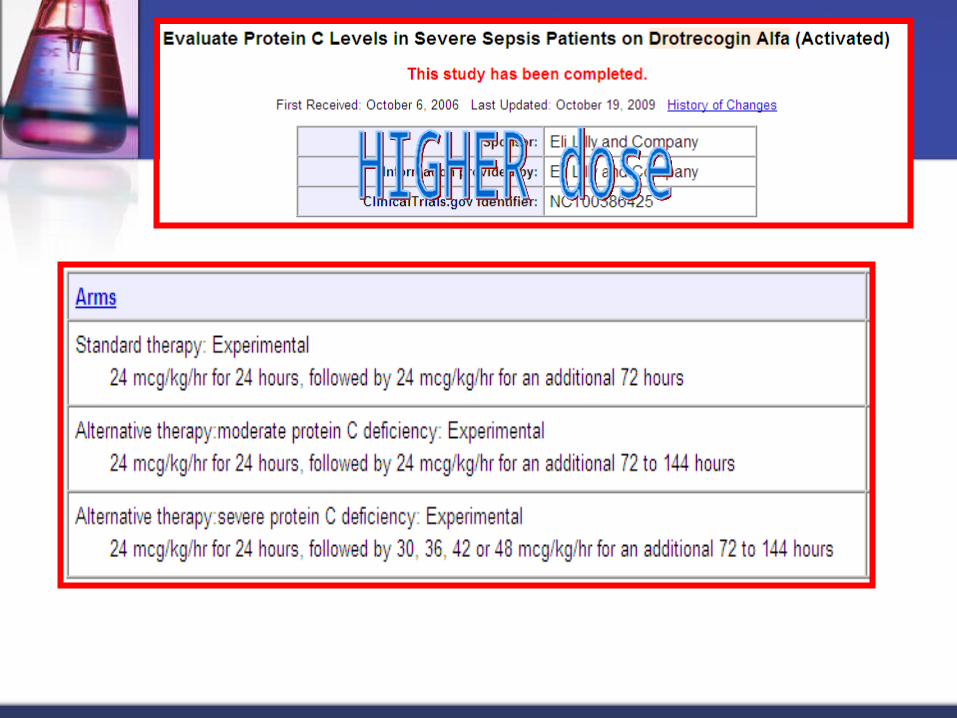
WHAT IS NEW ABOUT xigrisWHAT IS NEW ABOUT xigris
Questions for 2010Questions for 2010
Is larger dose Is larger dose better? ( and still better? ( and still safe ).safe ).
Is longer duration is Is longer duration is better? ( and still better? ( and still safe )safe )
Dose it correlate Dose it correlate with Protein C with Protein C deficiency level ?deficiency level ?
Would we put X on Would we put X on the Xigris drugthe Xigris drug

THANKS , ANY QUESTIONS ?