update on nougg guidelines nov 5, 2017 - cloud …€¦ · update on nougg guidelines nov 5, 2017...
TRANSCRIPT
1
Update on NOUGG GuidelinesNov 5, 2017
Sol Stern B.Sc M.Sc. MD MCFPFamily PhysicianOakville, Ontario
Copyright © 2017 by Sea Courses Inc.
All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means – graphic, electronic, or mechanical,
including photocopying, recording, or information storage and retrieval systems without prior written
permission of Sea Courses Inc. except where permitted by law.
Sea Courses is not responsible for any speaker or participant’s statements, materials, acts or omissions.

Faculty/Presenter Disclosure
• Faculty: Sol Stern B.Sc. M.Sc MD MCFP
• Lead Family Physician Argus Medical Centre FHO
• Relationships with commercial interests:• Advisory Boards: Astra Zeneca, BMS, Purdue, J and J, Pfizer, Otsuka, Tribute
• Honoraria: Astra-Zeneca, Bristol Myers Squibb, Ethypharm, , Janssen, J and J, Paladin, Pfizer, Purdue, Sanofi-Aventis
• Consulting Fees: MdBriefcase.com, CTC Consulting, Sea Courses.com
• Grants/Research Support: Hope- 3 Clinical Investigator Astra Zeneca

Disclosure of Commercial Support
Potential for conflict(s) of interest:
• The Speaker will receive an honorarium from Sea Courses
Mitigating Potential Bias
Potential sources of bias identified in the preceding 2 slides have been mitigated as follows:
• Information/recommendations provided in the following program will be evidence- and/or guideline-based and opinions of the speaker will be identified as such.
Learning Objectives
• Review the 10 Recommendations of the 2017 Opioid Guidelines
• Compare the 2017 Guidelines to the 2010 NOUGG Guidelines
Confidential – For Internal Use Only 6
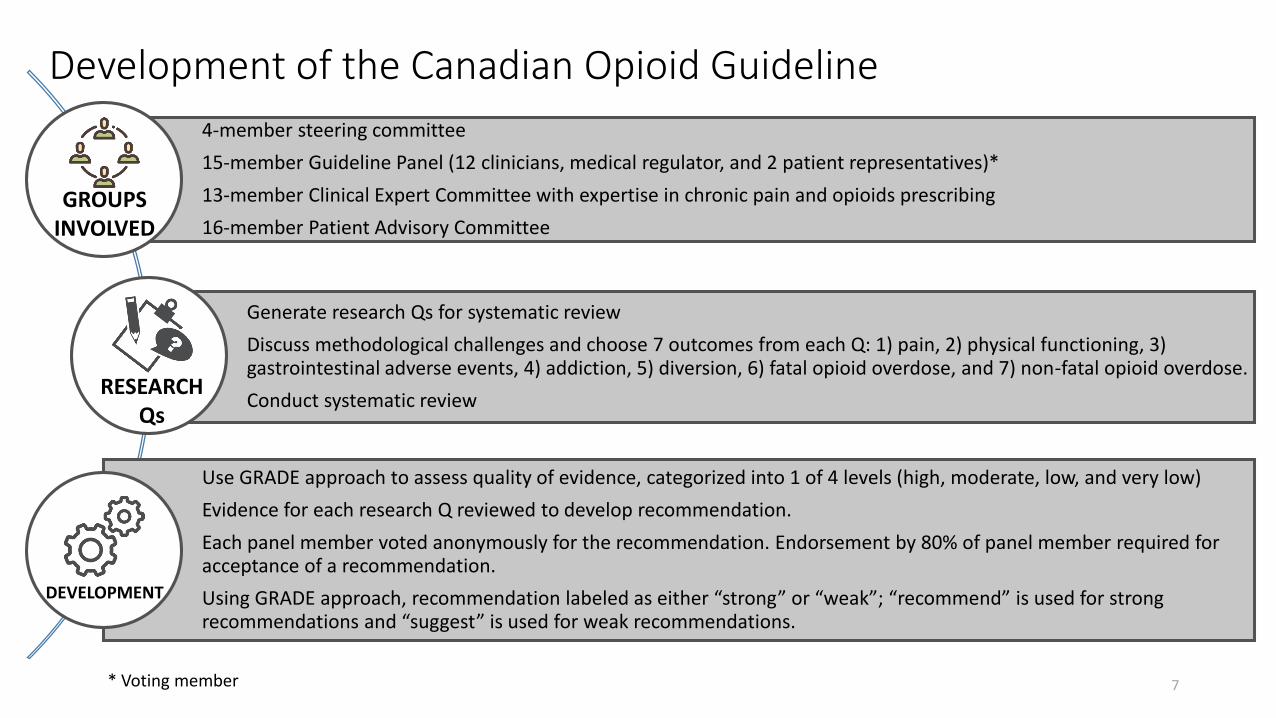
Development of the Canadian Opioid Guideline
7
4-member steering committee
15-member Guideline Panel (12 clinicians, medical regulator, and 2 patient representatives)*
13-member Clinical Expert Committee with expertise in chronic pain and opioids prescribing
16-member Patient Advisory Committee
Generate research Qs for systematic review
Discuss methodological challenges and choose 7 outcomes from each Q: 1) pain, 2) physical functioning, 3) gastrointestinal adverse events, 4) addiction, 5) diversion, 6) fatal opioid overdose, and 7) non-fatal opioid overdose.
Conduct systematic review
Use GRADE approach to assess quality of evidence, categorized into 1 of 4 levels (high, moderate, low, and very low)
Evidence for each research Q reviewed to develop recommendation.
Each panel member voted anonymously for the recommendation. Endorsement by 80% of panel member required for acceptance of a recommendation.
Using GRADE approach, recommendation labeled as either “strong” or “weak”; “recommend” is used for strong recommendations and “suggest” is used for weak recommendations.
GROUPS INVOLVED
RESEARCHQs
* Voting member
DEVELOPMENT

CMAJ May 8, 2017 8 PAGES
10 Recommendations plus supporting documentation- 4 Strong Recommendations- 6 Weak Recommendations
McMaster Website May 8, 2017105 pages (also available www.magicapp.org)
Additional Information
- 3 Best Practice Statements- 10 Guidance Statements (5 of which are on Risk Mitigation)
8
2017 Canadian Opioid Guideline Overview
Busse JW et al. Guideline for opioid therapy and chronic noncancer pain. CMAJ 2017 May 8;189:E659-66. Michael G. DeGroote National Pain Centre. 2017. http://nationalpaincentre.mcmaster.ca/documents/Opioid%20GL%20for%20CMAJ_01may2017.pdf.
Strong recommendations indicate that all or almost all fully informed patients would choose the recommended course of action, and indicate to clinicians that the recommendation is appropriate for all or almost all individuals.
9
How to use the Guideline
CPNCP, chronic non-cancer pain
Weak recommendations indicate that the majority of informed patients would choose the suggested course of action, but an appreciable minority would not. With weak recommendations, clinicians should recognize that different choices will be appropriate for individual patients, and they should help patients arrive at a decision consistent with their values and preferences.
Weak recommendations should not be used as a basis for standards ofpractice (other than to mandate shared decision-making).
10
How to use the Guideline
CPNCP, chronic non-cancer pain

The guideline also contains best practice statements and clinical expert guidance, which are distinct from recommendations that have been formally categorized using GRADE. Good practice statements represent common-sense practice, are supported by indirect evidence, and are associated with assumed large net benefit.
Clinical expert guidance provides direction in areas for which there is either no published evidence or insufficient evidence to justify a formal recommendation.
11
How to use the Guideline

R01. Optimize non-opioid pharmacotherapy (NORx) and non-pharmacological therapy (NPTx). Strong Recommendation Against
Consider the evidence for the specific treatment.
Opioids may have similar effects on pain relief and similar improvements in physical function when compared to NSAIDs, tricyclic antidepressants, or nabilone.
Opioid are associated with risks for addiction, overdose, diversion.
Confidential – For Internal Use Only 12
2017
CPNCP, chronic non-cancer pain
PRACTICAL INFO
Michael G. DeGroote National Pain Centre. 2017. http://nationalpaincentre.mcmaster.ca/documents/Opioid%20GL%20for%20CMAJ_01may2017.pdf. Accessed 05/15/2017.
R02. Add a trial of opioids to CNCP patients without current or past SUD and without other current serious psychiatric disorders, who experience persistent pain despite optimized NORx. Weak Recommendation
Initiation, titration, and monitoring of response, with discontinuation if important improvement in pain or function is not achieved.
Prescribe for no more than 28 days at a time. Intervals may be shorter in some cases.
Reasonable trial should be accomplished within 3-6 months.
Confidential – For Internal Use Only 13
2017
CNCP, chronic non-cancer pain; NORx, Non-opioid pharmacologic therapy; SUD, substance use disorder
PRACTICAL INFO
Michael G. DeGroote National Pain Centre. 2017. http://nationalpaincentre.mcmaster.ca/documents/Opioid%20GL%20for%20CMAJ_01may2017.pdf. Accessed 05/15/2017.
R03. Opioids should not be used in CNCP patients with an active SUD. Strong Recommendation Against
Screen for SUD using validated substance abuse/misuse tools. Effectiveness of UDS and PDMP in reducing OUD not clearly demonstrated; suggested initially and periodically thereafter.
Facilitate treatment of underlying SUD, if not yet addressed
Confidential – For Internal Use Only 14
2017
CNCP, chronic non-cancer pain; OUD, opioid use disorder; PDMP, prescription drug monitoring program; SUD, substance use disorder, UDS, urine drug screening
PRACTICAL INFO
National Opioid Use Guideline Group (NOUGG), 2010. http://nationalpaincentre.mcmaster.ca/documents/opioid_guideline_part_b_v5_6.pdf. Accessed 03/31/2017.

R04. Stabilize the psychiatric disorder before considering a trial of opioid in CNCP patients with an active serious psychiatric disorder whose NORx has been optimized, and who have persistent problematic pain. Weak Recommendation
Psychiatric comorbidity and emotional distress are common among patients CNCP.
Patients with psychiatric disorders report more severe pain. Patients should be screened for psychiatric disorder with appropriate tools.
Stabilize the disease first before considering an opioid trial.
15
2017
CNCP, chronic non-cancer pain; NORx, non-opioid pharmacologic therapy
PRACTICAL INFO
Michael G. DeGroote National Pain Centre. 2017. http://nationalpaincentre.mcmaster.ca/documents/Opioid%20GL%20for%20CMAJ_01may2017.pdf. Accessed 05/15/2017

R05: Continue NORx in CNCP patient with a history of SUD, whose NORx has been optimized, and who experience persistent pain. Weak Recommendation
Screen for SUD using validated tools for substance abuse/misuse and alcohol use.
Effectiveness of UDS and PDMP in reducing OUD not clearly demonstrated; suggested initially and periodically thereafter.
16
2017
CNCP, chronic non-cancer pain; NORx, non-opioid pharmacologic therapy; OUD, opioid use disorder PDMP, prescription drug monitoring program; UDS, urine drug screening
PRACTICAL INFO
Michael G. DeGroote National Pain Centre. 2017. http://nationalpaincentre.mcmaster.ca/documents/Opioid%20GL%20for%20CMAJ_01may2017.pdf. Accessed 05/15/2017
R06: When starting opioid therapy, prescribe a dose <90 MME/d rather than no upper or a higher limit on dosing. Strong Recommendation
R07: When starting opioid therapy, prescribe a dose <50 MME/d for CNCP patients. Weak Recommendation
When beginning opioid therapy, restrict the dose to less than 50 MME/d.
Opioid dose should not be increased to ≥ 90 MME/d without careful justification based on diagnosis and on individualized assessment of risks and benefits.
Refer to a colleague for a 2nd opinion regarding the possibility of increasing dose >90 MME/d.
17
GUIDELINE
PRACTICAL INFO
Michael G. DeGroote National Pain Centre. 2017. http://nationalpaincentre.mcmaster.ca/documents/Opioid%20GL%20for%20CMAJ_01may2017.pdf. Accessed 05/15/2017.
MME/d, morphine milligram equivalent/day
R08: Rotate to other opioids in CNCP patients who are currently using opioids and experiencing persistent pain and/or side effects. Weak Recommendation
Calculate equianalgesic dose* of new opioid and reduce calculated dose by 25-50% to minimize risk of inadvertent OD.
Rotation as strategy to ↓ dose:
1. ↓ TDD of current opioid by 10-30%/week while starting new opioid at lowest TDD.
2. ↓ TDD of current opioid by 10-25%/week while titrating TDD of new opioid weekly by 10-20%, with goal of switching over in 3-4 weeks
Confidential – For Internal Use Only 18Michael G. DeGroote National Pain Centre. 2017. http://nationalpaincentre.mcmaster.ca/documents/Opioid%20GL%20for%20CMAJ_01may2017.pdf. Accessed 05/15/2017
* Opioid conversion table provides only a rough approximation of equivalent opioid potency and does not account for cross tolerance from one opioid to another.TDD, total daily dose; OD, overdose
GUIDELINE
PRACTICAL INFO
R09: For CNCP patients currently using ≥90 MME/d, taper to the lowest effective dose, potentially including discontinuation rather than no change in opioid therapy. Weak Recommendation
Regularly evaluate and counsel patients about benefits and harms with LTOT and potential benefits of tapering
Actively engage patient in a discussion about merits of gradual dose reduction. Collaborate with patient to create a tapering plan.
Gradual dose reduction of 5-10% MME every 2-4 weeks with frequent follow-up is reasonable rate of opioid tapering.
Alternative methods include ↓ dose rapidly over few days/weeks or immediately; taper with methadone or buprenorphine.
Pause tapering in patients struggling with tapering plan and re-evaluate patient’s pain/clinical status/coping mechanism and the approach tapering can help formulate a go-forward plan (R10).
Encourage to taper to lowest opioid dose without loss of previously achieved function.
Confidential – For Internal Use Only 19
GUIDELINE
PRACTICAL INFO
Michael G. DeGroote National Pain Centre. 2017. http://nationalpaincentre.mcmaster.ca/documents/Opioid%20GL%20for%20CMAJ_01may2017.pdf. Accessed 05/15/2017

R10. A formal multidisciplinary program should be used for CNCP patients using opioids and experiencing tapering challenges. Strong Recommendation
Serious challenges in tapering could include re-emergence of or new functional or psychological impairment, aberrant behaviours around opioid use, or behaviours indicative of emerging or overt SUD
20
CNCP, chronic non-cancer pain
GUIDELINE
PRACTICAL INFO
Michael G. DeGroote National Pain Centre. 2017. http://nationalpaincentre.mcmaster.ca/documents/Opioid%20GL%20for%20CMAJ_01may2017.pdf. Accessed 05/15/2017

1) Acquire informed consent prior to initiating opioid use for chronic non-cancer pain. A discussion about potential benefits, adverse effects, and complications will facilitate shared-care decision making regarding whether to proceed with opioid therapy.
2) Clinicians should monitor their chronic non-cancer pain patients using opioid therapy for their response to treatment, and adjusttreatment accordingly.
3) Clinicians with chronic non-cancer pain patients prescribed opioids should address any potential contraindications and exchange relevant information with the patient’s general practitioner (if they are not the general practitioner) and/or pharmacists
21
Best Practice Statements
Restriction in amounts of opioids prescribedImmediate vs Controlled Release OpioidsCo-prescribing with opioidsSleep apneaHypogonadism
Urine drug screeningTreatment agreementsTamper-resistant formulationsFentanyl patch exchangeNaloxone
22
Expert Guidance
• Patients with CNCP may be offered a trial of opioids only after they have been optimized on non-opioid therapy, including nondrug measures.
• They suggest avoiding opioid therapy for patients with a history of substance use disorder (including alcohol) or active mental illness, and opioid therapy should be avoided in cases of active substance use disorder.
• For patients beginning opioid therapy, they recommend restricting to less than 90 mg morphine equivalents daily (MED) and suggest restricting the maximum prescribed dose to less than 50 mg MED.
• Patients already receiving high-dose opioid therapy (≥ 90 mg MED) should be encouraged to embark on a gradual dose taper, and multidisciplinary support should be offered where available
23
Key Points