update on medicines management programme: safe and ...€¦ · update on medicines management...
TRANSCRIPT

Update on Medicines Management Programme: Safe and Effective Use of
Medicines
HSE West RNP Continuing Professional Development Day
Friday November 18th 2016
Maria Daly, Senior Pharmacist, Medicines Management [email protected] www.hse.ie/yourmedicines

� Multi‐disciplinary Team – including the National Medicines Information Centre (NMIC) and the National Centre for Pharmacoeconomics (NCPE) in collaboration with the HSE‐Primary Care.
� Aim ‐ sustained national leadership relating to� Safe� Effective � Cost‐effective prescribing
The Medicines Management Programme (MMP)

0
500
1000
1500
2000
2500
Mill
ions
(€)
The Medicines Management Programme (MMP) was established in January 2013
The Medicines Management Programme (MMP)
Drug expenditure under the Community Drugs Schemes 1991 - 2014

Overview� Medication errors
� Preferred Drugs
� Inhaled medicines for asthma and COPD
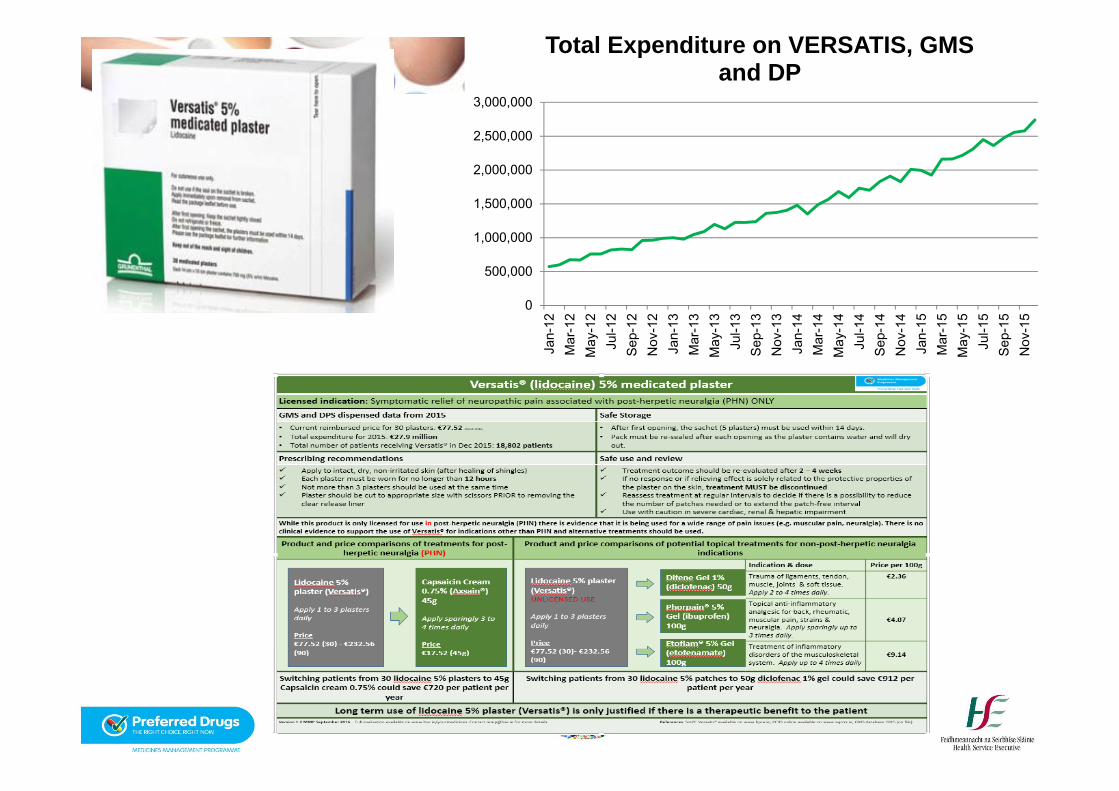
� Versatis 5% medicated plaster
� Projects in collaboration with other NCP- Blood glucose strips, antibiotics, lithium and valproate
� www.hse.ie/yourmedicines

Reflection� Medication use has become increasingly complex
� Multimorbidity means different clinicians looking after different elements of patient care
� Medication error is a major cause of preventable patient harm
� As prescribers, you will have an important role in making medication use safe

Risk of ErrorsWhen can medication errors occur:� When a patient is admitted and/or discharged from
hospital
� When a drug chart is re-written
� When therapy is being changed- add-on or replacement
� When dosing, frequency or time is unclear and leads to wrong administration
� SALADs – Sound Alike Look Alike Drugs


Sound Alike Look Alike Drugs- SALADs
� Keral 25mg vs Keppra 250mg
� Humulin S vs Humulin I vs Humulin M3
� Lamictal vs Lamisil
Dexketoprofen versus Levetiracetam
Short-acting versus intermediate-acting insulin versus combination of both
Lamotrigine versus Terbinafine

Generic Prescribing� International Non-proprietary Names (INN)
facilitate the identification of pharmaceutical substances or active pharmaceutical ingredients. Each INN is a unique name that is globally recognized and is public property. A non-proprietary name is also known as a generic name.
� Reduced risk of dispensing and administration errors if medicines are prescribed by the INN/generic name

Combination ProductsPerindopril/Amlodipine
Amlodipine/Valsartan
Amlodipine/Valsartan/Hydrochlorothiazide
Sitagliptin/Metformin
Naproxen/Esomeprazole
Ezetimibe/Simvastatin

PPI- LANSOPRAZOLEStatin- SIMVASTATINACE Inhibitor- RAMIPRILARB- CANDESARTANB-Blocker- BISOPROLOLCCB- AMLODIPINESSRI- CITALOPRAMSNRI- VENLAFAXINEAntimuscarinic- TOLTERADINEOral Anticoagulant- WARFARINNOAC- APIXABAN (second line)

Selection of a Preferred Drug
� Factors considered when making a recommendation for a “preferred drug”:
� Range of therapeutic indication(s)� Clinical evidence base� Clinical guidelines ( National & International )� Patient related factors� Cost� Current prescribing practice

MMP Preferred DrugsEvaluation Report Tips and Tools

Statins – April 2013
Simvastatin is recommended as the statin of first choice
• Over 310,000 patients receive a statin each month
• Approx. 4.2 million statin prescriptions issued/annum
• Total expenditure exceeds € 50 million/annum
• The calculated ingredient cost per prescription item for simvastatin remains the lowest in the therapeutic class
Phase 1Statins and PPIs

Statins – still opportunities to prescribe more safely and to reduce expenditure
There are still almost 100,000 prescriptions issued for rosuvastatin each month
If we prescribed any other statin in preference to rosuvastatin savings of over € 4 million/year could be made
Most risk of side-effects with rosuvastatin
Calculated Ingredient cost per statin prescription after reference pricing

Proton pump inhibitors (PPIs ) – April 2013
Lansoprazole is recommended as the PPI of first choice
• Over 265,000 patients receive a PPI each month
• Approx. 3.6 million PPI prescriptions issued/annum
• Total expenditure exceeds € 55 million/annum
• Esomeprazole is one of the most expensive PPIs and accounts for over 32% of all PPI prescriptions

Esomeprazole is still the most commonly prescribed PPI.
If we prescribed any other PPI in preference to Esomeprazole (Nexium) or rabeprazole savings of over € 1.7 million/year could be made.
Reducing doses and stopping inappropriate prescribing is also required.Most patients should be on reduced dose PPI (Lansoprazole 15mg)
Calculated Ingredient cost per PPI prescription after reference pricing
PPIs – potential to improve prescribing and further reduce expenditure


PPI- LANSOPRAZOLEStatin- SIMVASTATINACE Inhibitor- RAMIPRILARB- CANDESARTANB-Blocker- BISOPROLOLCCB- AMLODIPINESSRI- CITALOPRAMSNRI- VENLAFAXINEAntimuscarinic- TOLTERADINEOral Anticoagulant- WARFARINNOAC- APIXABAN (second line)
Ramipril is the ACE inhibitor of choice(>130,000 ACE prescriptions/month & > €14.7 million/annum)
Candesartan is the Preferred ARB (>115,000 ARB prescriptions/month & > €24.5 million/annum)
Phase 2ACE inhibitors and Angiotensin II receptor blockers (ARBs)

PPI- LANSOPRAZOLEStatin- SIMVASTATINACE Inhibitor- RAMIPRILARB- CANDESARTANB-Blocker- BISOPROLOLCCB- AMLODIPINESSRI- CITALOPRAMSNRI- VENLAFAXINEAntimuscarinic- TOLTERADINEOral Anticoagulant- WARFARINNOAC- APIXABAN (second line)

� Over 150,000 patients are being treated with an SSRI (112,419) or an SNRI (40,266)
� Each year over 2.29 million prescription items are issued ( SSRI=1,613,479 & SNRI=677,718 )
� Total expenditure exceeds € 55.7 million per annum ( SSRI = €36.06 m & SNRI = € 19.68 m )
Community Drugs Schemes SSRI & SNRI prescribing

� Each month approximately 50,000 patients discontinue an SSRI or SNRI only to be replaced by a similar number commencing treatment
Community Drugs Schemes SSRI & SNRI prescribing
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
35.00%
Duration of antidepressant use - percentage of patients
1 2 3 4 5 6 7 8 9 10 11 12

SSRI Preferred Drug: Citalopram� Use appropriate dosing� Antidepressant effect usually seen
by 2 weeks. If no effect seen by week 4 then a change in dose or drug is indicated.
� A single episode of depression is treated for a minimum of 6 months after recovery.
� If antidepressant therapy is stopped immediately on recovery, 50% of patients may experience a return of their depressive symptoms.

Preferred SNRI - Venlafaxine� Use appropriate
doses and formulations: immediate release and XL formulations
� Abrupt discontinuation should be avoided.
� When discontinuing phase out over several weeks (minimum 2 weeks).

Inhaled medicines for Asthma and COPD
� There are over 50 licensed inhalers for asthma and over 35 licensed inhalers for COPD
� Expenditure on inhalers for asthma and COPD in 2015‐exceeded €91.6 million/annum on GMS scheme alone
� It is estimated that COPD accounts for 84% of this expenditure ( €77 million/annum )

ICS and LABA inhalers for Asthma & COPD
� €50 million on ICS and LABA combination inhalers� €2.4 million/month Seretide® (GMS only)� €1.3 million/month Symbicort® (GMS only)New products in this group including hybrid (“generic”) inhalers offer opportunity to reduce expenditure
� Used in GOLD Category 3-4 for COPD� Step 4 in Asthma therapy guidelines
Bufomix® (budesonide 160µg + formoterol 4.5 µg) are dose equivalent to ‘Symbicort’ (budesonide
200µg + formoterol 6µg) and are up to 22% cheaper
Therefore the most cost-effective inhaled corticosteroid + long acting beta 2 agonist combination product is Bufomix®

Inhaler technique guide videos and checklists available on: www.asthma.iewww.COPD.ie
0
500,000
1,000,000
1,500,000
2,000,000
2,500,000
3,000,000
Jan-
12M
ar-1
2M
ay-1
2Ju
l-12
Sep
-12
Nov
-12
Jan-
13M
ar-1
3M
ay-1
3Ju
l-13
Sep
-13
Nov
-13
Jan-
14M
ar-1
4M
ay-1
4Ju
l-14
Sep
-14
Nov
-14
Jan-
15M
ar-1
5M
ay-1
5Ju
l-15
Sep
-15
Nov
-15
Total Expenditure on VERSATIS, GMS and DP

CollaborationsRheumatology
Diabetes
Epilepsy/ Neurology
Mental health
HCAI/AMR

Blood Glucose Test Strips� Total expenditure in 2014: €46.8million� 26 individual test strips reimbursed� NCPD published new guidelines in 2015� MMP recommendations published in April 2016

Drug groupsDrug Class Example Hypoglycaemic
riskBiguanides Metformin (Glucophage®) Low
DPP4-Inhibitors Sitagliptin (Januvia®)Linagliptin (Trajenta®)
Low
GLP-1 Agonists Canagliflozin (Invokana®) Dapagliflozin (Forxiga®)
Low
Thiazolidinediones Pioglitazone (Actos®)Rosiglitazone (Avandia®)
Low
SGLT2 Inhibitors Repaglinide (Novonorm®) Low
Sulphonyureas Gliclazide (Diamicron®) Higher
Meglitinide Repaglinide (Prandin®) Higher

Patient group Testing recommendation Limit on yearly dispensingPatients receiving insulin
4 times daily and when required No limit recommended
Test according to specialist recommendations
Patients receiving non‐insulin anti‐diabetic drugs
Patients receiving sulphonylurea or meglitinide drugs: May test 1‐2 times daily or if feeling hypoglycaemic.
1200 test strips per yearTwo boxes (100 test strips) per month will be reimbursed
Patients on oral drugs other than sulphonylurea or meglitinides (i.e.metformin and/or a thiazolidinedione, DPP‐4 inhibitor,GLP‐1 analogue, SGLT2 inhibitor):May test 3 times per week if needed
600 test strips per yearOne box (50 test strips) per month will be reimbursed
Diet alone Not required 100 test strips per yearOne pack per 6 months to allow for periodic testing where recommended

PRESCRIBING TIPS FOR SAFE ANTIBIOTIC USEAntimicrobial resistance is a growing and significant threat to public health that is compromising our ability to treat infections effectively. It is widely acknowledged that antibiotic resistance is driven by high rates of antibiotic prescribing and it is critical that we work to reduce unnecessary antibiotic use.Evidence-based antimicrobial guidelines are a key tool in efforts to improve antibiotic prescribing, reduce the progression of antibiotic resistance and optimise patient outcomes.
www.antibioticprescribing.ieAims to:1 To provide a simple, best guess approach to the treatment of common infections2 To promote the safe and effective use of antibiotics3 To minimise the emergence of bacterial resistance in the communityThis site is provided by the HSE and RCPI Clinical Programme on HCAI and AMR Prevention, working with the ICGP. It aims to provide GPs with a quick reference guide to antibiotic prescribing. Much of what is seen in general practice are self-limiting viral infections . Care is also needed in the use of antifungal ,antiviral and insecticides due to emerging resistance .
The following table summarises our preferred antibiotics for the common conditions seen in Irish General practice and which antibiotics we would prefer to minimise the use of to reduce the emergence of resistance.
“Keeping antibiotics effective for future generations is everyone’s responsibility”Make www.antibioticprescribing.ie one of your favourites


Every time we as healthcare workers consider influencing a decision to use or prescribe an antibiotics need to ask ourselves …….
• Is this antibiotic really necessary?• Is there reasonable certainty of a
bacterial infection?• If so it needs to be the right antibiotic, at
the right dose, to the right patient!

Treatment of Urinary Tract Infections
30 – 50% of frail, elderly long‐term care residents can have a positive urine culture without symptoms of UTI
Dysuria, frequency, urgency, new onset incontinence, fever >38°C, suprapubictenderness, haematuria
Urinary catheter:loin pain, fever >38°C
• Do NOT perform dipstick urinalysis if patients are asymptomatic or if urinary catheter present (false positives)
• A positive urine dipstick result in an asymptomatic patient is not significant and should not be treated
• DO NOT SEND URINE FOR CULTURE IF THERE ARE NO SIGNS AND SYMPTOMS OF UTI
Dipstick urine testing is NOT a reliable way to diagnose UTI
Urinary Tract Infection- must have symptoms and signs

Prescribing of antibiotics (all ages) in the GMS scheme from 2012-2014 inclusive
Total number of items2012 = 2.89million2013 = 2.83million2014 = 2.68million
Ref: Analysis by Dr Kathleen Bennett for HSE Medicines Management Programme, 18th Nov 2014

Lithium� Collaborate with NCP for
Mental Health.
� Safe switching patients from Calcolit to Priadel.
� Report includes- How to switch, appropriate timing of lithium levels, therapeutic range, signs of toxicity.

Sodium Valproate� Collaborate with NCP Epilepsy
& Mental Health
� Valproate should not be prescribed to in girls and women of child-bearing age
� Valproate toolkit
� Safety information for HCP and patients on the risks of valproate
� Includes information booklet and checklist

Find us on:www.hse.ie/yourmedicines
Any Questions?
Useful websites:www.hse.ie/valproatewww.nmic.iewww.ncpe.iewww.antibioticprescribing.iewww.hpra.ie