update on gestational diabetes: controversies, changes and challenges james r. scott, md i have no...
TRANSCRIPT

UPDATE ON GESTATIONAL DIABETES: CONTROVERSIES, CHANGES AND CHALLENGES
JAMES R. SCOTT, MD
I HAVE NO CONFLICT OF INTEREST TO DISCLOSE
OBJECTIVES
• TO DEFINE GESTATIONAL DIABETES, ITS PREVALENCE AND DIAGNOSIS • TO RECOGNIZE THE COMPLICATIONS FOR MOTHER AND BABY• TO APPLY THE FINDINGS OF THE NIH CONFERENCE TO YOUR PATIENTS

DEFINITIONS
• TYPE 1 DIABETES (JUVENILE, INSULIN DEPENDENT)COMPLETE FAILURE OF PANCREAS TO SECRETE
INSULIN • TYPE 2 DIABETES (ADULT ONSET)
INSULIN SECRETORY DEFICIENCY & INSULIN RESISTANCE IN VARIOUS ORGANS• GESTATIONAL DIABETES (GDM, PRE-DIABETES)
• FIRST RECOGNIZED DURING PREGNANCY• PREGNANCY HORMONES CARBOHYDRATE INTOLERANCE

THE PROBLEM
• DIABETES ASSOCIATED WITH OBESITY• 1/3rd OF AMERICANS OBESE & INCREASING• 11% OF ADULT AMERICANS HAVE DIABETES • 35 % HAVE PREDIABETES • Total = ALMOST HALF THE POPULATION• PREVALENCE INCREASING & AT YOUNGER AGE• GDM COMMON COMPLICATION - 6-7 % OF
PREGNANCIES• US COST - $635 MILLION ANNUALLY

BOISE27.9%22.2 – 34.2

SCREENING TEST FOR GDM DIAGNOSIS
• CRITERIA ESTABLISHED 30-40 YEARS AGO• TO IDENTIFY WOMEN AT RISK OF
DEVELOPING DIABETES LATER IN LIFE• 50% DEVELOP DIABETES IN 22-28 YEARS• BASED ON NON-PREGNANT WOMEN• NOT TO IDENTIFY RISK OF ADVERSE
PREGNANCY OUTCOME
Universal vs targeted screening debated• US: Most screen all pregnant women• US Preventive Health Service does not
recommend screening (2008) “Current evidence is insufficient to assess the balance between the benefits and harms of screening women for GDM either before or after 24 wks. Harms of screening include short-term anxiety…and inconvenience to women and medical practices because most positive screening tests are likely false positives.”
GDM SCREENING CONTROVERSIES
CURRENTLY, ALL PREGNANT WOMEN TESTED FOR GDM AT 24-28 WEEKS
SOME TEST WOMEN AT HIGH RISK FOR GDM (AND ALL TYPE 1 DIABETICS SHOULD BE) AT FIRST PRENATAL VISIT
• 50 GM GLUCOSE SCREEN > 140 mg/dl
• HbA1C GDM > 6.5 (Has not been validated)
AT RISK FOR GDM
• OLDER THAN AGE 25• OVERWEIGHT• HAD GDM BEFORE• HAD VERY LARGE BABY• CLOSE RELATIVE WITH DIABETES• PREVIOUS STILLBIRTH• AFRICAN AMERICAN, INDIAN, HISPANIC

U.S. GDM SCREENING/DIAGNOSIS
TWO - STEP TESTING• 1 hr 50 gm oral glucose load @ 24-28 wks
If >140 mg/dl • 3 hr 100 gm oral glucose load [> 2 values]
Fasting 105 mg/dl1 hr 190 mg/dl2 hr 165 mg/dl3 hr 145 mg/dl

Distribution of Blood Sugars in Pregnancy
Blood glucose
Overt DM
Gestational DM

GDM COMPLICATIONS• PREECLAMPSIA• MACROSOMIA• SHOULDER DYSTOCIA, BIRTH INJURY• CESAREAN DELIVERY• NEONATAL
• Hyperbilirubinemia• Hypoglycemia• Respiratory Distress Syndrome

PRIOR TO 2005, NO EVIDENCE THAT TREATMENT OF GDM IMPROVED MATERNAL OR INFANT OUTCOME
• Macrosomia/LGA• Shoulder Dystocia

NEW DATA DEMONSTRATED HYPERGLYCEMIA IS A CONTINUUM
• 2008 HAPO Study: 25,505 women• Continuous association between glucose
levels and adverse pregnancy outcomes• Increasing fasting, 1 and 2 hr glucose
glucose • Birth weight >90%tile• No clear cut-point

• Criteria based on pregnancy outcomes• Cut-offs defined from adverse outcomes• Most of world uses 2hr 75 gm OGTT• Endorsed by American Diabetes Association
NEW CRITERIA FOR DIAGNOSING GDM PROPOSED

LOWER THRESHOLDS
• Recommended IADPS thresholds
correspond to 1.75-fold risk for large
and/or “hyperinsulinemic” infants
• 70 – 80% of overgrown infants born to women without diabetes
Metzger et al NEJM 2008

• SINGLE STEP 75 g 2 hr OGTT - One abnormal value for GDM diagnosis:
Fasting 92 mg/dl
1 hr180 mg/dl
2hr153 mg/dl• Lowers thresholds more women
diagnosed as GDM
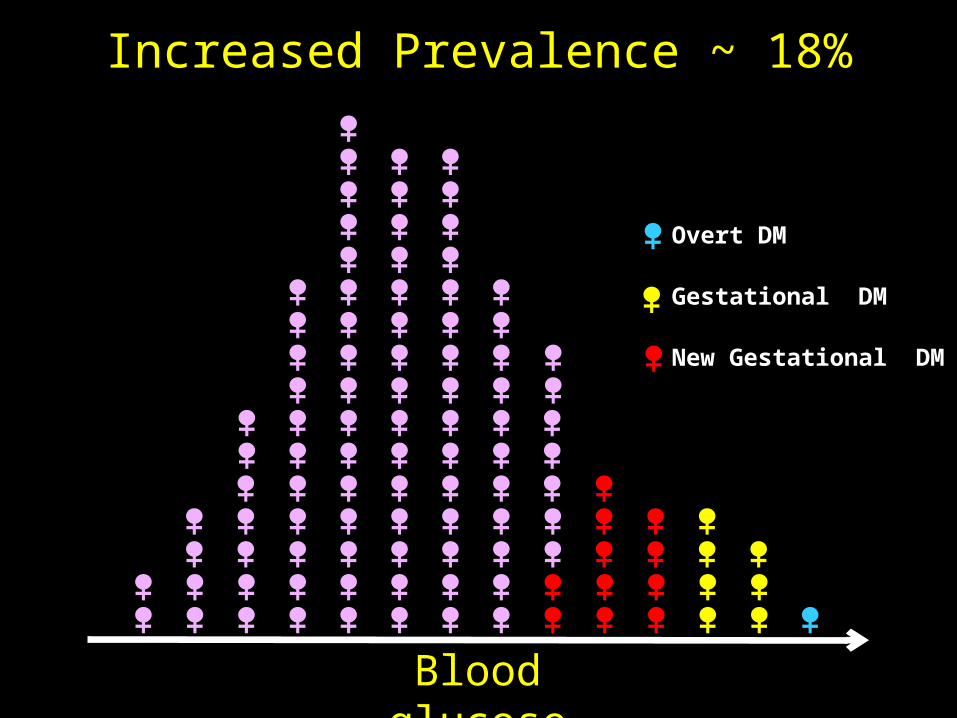
Blood glucose
Increased Prevalence ~ 18%
Overt DM
Gestational DM
New Gestational DM

MAY BE EVEN HIGHER
• GDM tripled from 10.3% to 30.1%
using IADPSG thresholds.
Reyes-Munoz et al Endocrine Practice 2012
• GDM rate increased to 27.5 %Bodmer-Roy et al Obstet Gynecol 2012


Rationale for Consensus Conference
• To Address this complicated issue• To clarify diagnostic thresholds• Rigorous evaluation of existing evidence• Implications of new proposed thresholds • Develop Recommendations


•Produce consensus statements on important, controversial topics in medicine
•Began in 1977•Goal: evaluate available scientific information and develop a statement that advances understanding of the issue useful to health professionals and the public at large
http://prevention.nih.gov/cdp/about.aspx

Process:• Independent systematic review by AHRQ Evidence-based Practice Center•Provided to panel 6 wks prior to conference
• Conference•2.5 days of expert presentations and open public discussion
•Panel drafts statement for presentation on 3rd day

Consensus Conference Panelists:•Knowledgeable about topic but have no published or known opinion on subject
•No financial or career interest in topic
•Represent a variety of perspectives
“independent assessment of available knowledge”

CHARGE – EVALUATE EVIDENCE AND IMPLICATIONS IF NEW GDM SCREENING PROPOSAL INSTITUTED1. Evidence that additional patients identified
have increased frequency of maternal/ perinatal morbidities
2. Evidence that these morbidities can be prevented or decreased by intervention
3. Evidence that benefits outweigh harms incurred

Potential Benefits

ACCEPTED
• WOULD HAVE UNIFORM WORLDWIDE SCREENING SYSTEM
• BASED ON PREGNANCY OUTCOMES• CUT-OFFS BASED ON ADVERSE EVENTS• ABLE TO COMPARE RESEARCH & CLINICAL OUTCOMES

HAPO STUDY
• Showed increased maternal and perinatal risks at thresholds lower than currently used, but…..
• Maternal BMI and weight gain major confounders
Metzger et al NEJM 2008

ACHOIS RCT ON Rx vs No Rx
• Reduced preeclampsia from 18% to 12%
• Reduced LGA from 22% to 13%• Reduced birth wt > 4000 gm
from 21% to 13%
Crowther et al. NEJM 2005
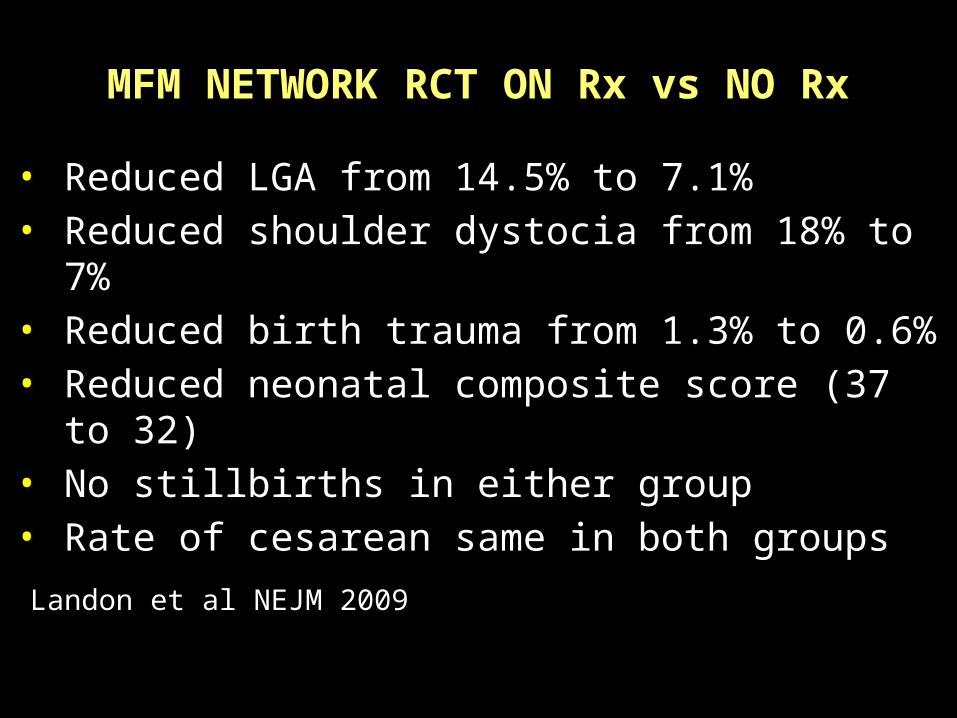
MFM NETWORK RCT ON Rx vs NO Rx
• Reduced LGA from 14.5% to 7.1%• Reduced shoulder dystocia from 18% to 7%• Reduced birth trauma from 1.3% to 0.6% • Reduced neonatal composite score (37 to 32)• No stillbirths in either group• Rate of cesarean same in both groups
Landon et al NEJM 2009

CAUTION IN INTERPRETATION
1. Trial participants highly motivated - ? Generalizable to practice
2. Not all treatments were same (not studied)
3. Different thresholds for criteria to diagnose GDM

CONCLUSIONS
• GDM Risks present but mild and relatively low even without Rx • Maternal Rx reduces some maternal and infant adverse outcomes•Overall reduction in adverse events relatively small

Potential Harms

PROBLEMS IN REAL WORLD
PATIENTS•MEDICALIZATION OF PREGNANCY• INCONVENIENCE – MUST SCHEDULE OGTT (REQUIRES FASTING) FOR ALL OB PATIENTS
•MONITORING OF GLUCOSE •MORE VISITS, TRAVEL, TIME, BABYSITTERS •EMOTIONAL IMPACT

IMPLICATIONS FOR PROVIDERS
•MANPOWER – MORE PERSONNEL NEEDED FOR 30% INCREASED WORKLOAD
•MORE EDUCATION VISITS, CLINIC VISITS, TESTING VISITS
•MORE ULTRASOUNDS, NSTs AND OTHER MONITORING
•MORE INDUCTONS•PROBABLY MORE CESEAREAN DELIVERIES•HIGHER RATES OF NBICU ADMISSIONS

IMPLICATIONS FOR U.S. HEALTH CARE SYSTEM
• INSTITUTING CHANGE• SIGNIFICANT IMPACT ON CAPACITY• DRAMATIC INCREASE IN WOMEN WITH MILDER GDM DIAGNOSIS WILL LEAD TO SIGNIFICANT HEALTH CARE COSTS

Annual Cost of Gestational Diabetes
Status Quo
$2 Billion
$636 Million
IADPSG
Chen et al, Population Health Management, 2009

• No evidence that identification and treatment of this new large group of “Borderline GDM” women is beneficial
• Improvement in short-term outcomes in women with mild GDM less likely
MOST IMPORTANT

CONCLUSION
• Not sufficient evidence to adopt one-step approach• Would increase prevalence of GDM, costs, and interventions without improvements in most clinically important patient outcomes• Given potential benefits of one-step approach, further research and reconsideration warranted

Panel supports maintaining current U.S. diagnostic approach for gestational diabetes mellitus
http://www.nih.gov/news/health/mar2013/od-06.htm
http://www.nih.gov/news/health/mar2013/od-06.htm

BOTTOM LINE: • Disadvantages outweigh advantages• Keep present two-step approach• Screen with 1 hr OGTT followed by
3 hr OGTT prn

MY PERSPECTIVE
• NIH CONFERENCE GOT IT RIGHT • DON’T OVERDIAGNOSE OR OVERTREAT GESTATIONAL DIABETES • OBESITY BIGGER PROBLEM AND DIFFICULT TO MANAGE • TYPE 1 DIABETES MUCH MORE SERIOUS FOR MOTHER AND BABY – NEED EXPERT CARE AND “WATCH HER LIKE A HAWK”

REFERENCES 1. VanDorsten JP, DODSON W, Espeland MA et al. Diagnosing gestational
diabetes mellitus. NIH Consensus Development Conference Statement. NIH Consens State Sci Statements 2013;29(1):1-30. Available at: http://prevention.nih.gov/cdp/conference/2013/gdm/files/Gestional_ Diabetes_Mellitus.508.pdf
2. Gestational Diabetes Mellitus. ACOG Practice Bulletin 2013;137:1-11. 3. Crowther CA, Hiller JE, Moss JR et al. Effect of treatment of gestational
diabetes mellitus on pregnancy outcomes. Australian Carbohydrate Intolerance study (ACHOIS) Trial Group. N Engl J Med 2005;352:2477-86
4. Metzger BE, Lowe LP, Dyer AR et al. Hyperglycemia and adverse pregnancy outcomes. HAPO Study Cooperative Research Group . N Engl J Med 2008;358:1991-2002.
5. Landon MB, Spong CY, Thom E et al. A multicenter, randomized trial of treatment for mild gestational diabetes. Eunice Kennedy Shriver NICHD Maternal-Fetal Medicine Units Network. N Engl J Med 2009;361;1339-48
6. Metzger BE, Gabbe SG, Person B et al. International association of diabetes and pregnancy study groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. International Association of Diabetes and Pregnancy Study Groups Consensus Panel. Diabetes Care 2010;33;676-82.