up-pgh competency program for new employee
DESCRIPTION
for newly hired nursesTRANSCRIPT

UP-PGH CBO
Table of Contents
INSTRUCTIONS FOR USE OF COMPETENCY BASED ORIENTATION PATHWAY (CBO) DOCUMENTATION…………………………………………………………………… .2WEEKLY OBJECTIVES……………………………………………………………… 3NURSING COMPETENCY BASED ORIENTATION PATHWAY…………………3
GENERAL ASSESSMENT..........................................................................................3NEUROLOGIC/BEHAVIORAL....................................................................................3PULMONARY SYSTEM..............................................................................................3CARDIOVASCULAR....................................................................................................3GASTROINTESTINAL SYSTEM................................................................................3GENITO-URINARY SYSTEM.....................................................................................3ENDOCRINE & HEMATOLOGIC SYSTEMS...........................................................3MUSCULOSKELETAL SYSTEM................................................................................3SKIN AND WOUND......................................................................................................3PAIN/COMFORT...........................................................................................................3SAFETY PRECAUTIONS............................................................................................3EMERGENCY RESPONSE........................................................................................3INTRAVENOUS THERAPY........................................................................................3BLOOD ADMINISTRATION........................................................................................3AUTO TRANSFUSIONS..............................................................................................3SPIRITUAL CARE/PSYCHOSOCIAL CARE............................................................3FOCUS AREAS.............................................................................................................3
RESTRAINTS AND SECLUSION..........................................................................3COMMUNICATION...................................................................................................3UNIT MANAGEMENT..............................................................................................3PROFESSIONAL NURSE.......................................................................................3
Page 1

UP-PGH CBO
Instructions for Use of Competency Based Orientation Pathway (CBO) Documentation
The purpose of this document is to assist the preceptor in providing a comprehensive and consistent orientation. It is intended to provide a foundation for practice in the area of acute care to promote high standards of nursing practice.
It is the responsibility of individual acute care nurses to identify their practice parameters in accordance with Philippine nurse practice acts, professional codes, professional practice standards, and their own competency.
The CBO guides the orientee in understanding the expectations of the University of the Philippines – Philippine General Hospital Manila and documents the orientation process received by new employees. It is intended to assist with the individualization of the orientation.
Responsibility of the Preceptor: • Obtains document from the preceptee • Reviews document as well as discuss learning needs of the new hire • Develops orientation plan in collaboration with the new hire to meet their learning needs and unit specific competencies• Explain competencies if learning option not available and where to find resources • Complete the CBO document by dating and initialing each statement, full signature at the end of the document• When orientation completed gives CBO document to nurse manager/ Assistant Nurse Manager
Responsibility of the Orientee:• Bring document to all clinical experiences• Review document and complete self assessment before unit based orientation begins 1 = no experience 2 = limited experience 3 = comfortable with experience• Collaborates with preceptor to develop individualized orientation • Remind preceptor to document completion of competencies as learning experiences occur• Recommend keeping CBO document on nursing unit• Communicate with preceptor frequently to ensure learning needs are met
Please Return this Document to the Nurse Manager when Completed.
Page 2

UP-PGH CBOWeekly Objectives for New Graduate Registered Nurse (Goal: 1 – 12 weeks, variable)
WEEK PRIMARY OBJECTIVE PLAN
1Familiarize new employee with Environment of Care and standards/ guidelines
(Limited patient care tasks)
On Unit:Day 1 1. No patient assignment for orientee or preceptor2. Tour of hospital, including library as appropriate, nursing administration,
conference rooms, HR, other units, pharmacy, lab, radiology, operating room, Central supply, cafeteria
3. Preceptor review purpose and function of Competency Based Orientation (CBO) Pathway; orientee complete self assessment
4. Orientee given unit-specific orientation protocols by preceptor5. Meet with supervisory personnel and preceptor
a. Supervisory personnel, preceptor, and orientee review CBO self assessment
i. Identify clinical strengths and weaknesses of orienteeii. Develop orientation plan
b. Align preceptor and orientee schedulesi. To accommodate no more then than two preceptors per orienteeii. Coordinate Continuous Education and necessary classes; e.g.
CVAD, EEG, PTE, temporary pacemakers, et al.iii. Identify off-unit learning opportunities; i.e. OR observation, Infusion
Center, Cath Lab, etc.6. Unit tour including, but not limited to:
a. Medication roomi. Delivery of medsii. Distribution/ location of medsiii. Methods of interface with pharmacyiv. Proper medication labelingv. Proper medication storagevi. Proper medication handling
b. Physical structure of uniti. # Beds and roomsii. Private vs semi private rooms (A&B)iii. Locations:
1. Code blue button 2. crash cart3. med room4. nursing lounge5. physicians lounge6. supply rooms7. dirty utility room
Page 3

UP-PGH CBO8. nurses mailboxes9. nurses station
c. Bed functionsi. Call lightsii. Bed lightsiii. Positioning (trendelenberg, reverse trendelenbeg), degree of
elevationiv. Special bed indications and resources
d. Document storage (paper)e. Patient medical recordf. Medication Administration Records (paper and electronic)g. Nursing unit white boards
7. Safety proceduresa. Fireb. Gas shut off valvesc. Evacuation routed. Yellow name badge card e. Codesf. Evacuation devices
8. Administrative functionsa. Telephone etiquette b. How to transfer a callc. Red phonesd. Nondisclosure statuse. Work schedule: location and proceduref. Process for vacation request, missed break or meal
9. Communicationa. Chain of Commandb. Paging protocolc. Physician privilegesd. CPARe. Elements of Nursing Reportf. Who to Call/ MD coverageg. Paging via WebRefh. Primary vs consulting physician servicesi. Physician ID numbers (PID)j. UP-PGH phone book
i. Paperii. WebRefiii. Blink
10. PCIS a. Printing of PCARSb. Charting assessments
Page 4

UP-PGH CBOc. Charting Point of Care testingd. Charting Care Plane. Charting PADBf. Review report/results (lab, procedures, consults)
11. Resources a. Nursing colleagues
i. Nurse Managerii. Assistant Nurse Manageriii. Charge Nurseiv. Preceptor v. Interdisciplinary teamvi. Co-workers vii. Superusersviii. Nursing Education, Development, and Researchix. Case Managersx. Wound and ostomy nursesxi. Vascular access nurses
b. Interdisciplinary colleaguesi. PTii. OTiii. MD, NA, MWiv. Nutritionv. Speechvi. RT
c. Pocket Reference Cardsi. Patient Safety Goalsii. Phone numbersiii. Core Valuesiv. Pillars of Excellencev. Clinical resources
d. Unit-specific resource binderse. WebRef
i. MCPs (have new hire find blood administration MCP)ii. Care Notesiii. CP onlineiv. Infection Controlv. Library
f. Lift team and/or lift devices12. Equipment
a. Vital sign machinesb. Sequential Compression Devices (SCDs)c. Bladder scannerd. Camera and printer
Page 5

UP-PGH CBO
Focus on acquisition of nursing skills and basic patient care per CBO
e. IV pumpsf. Vein finder ultrasound g. Enteral feeding pumpsh. Patient transfer devicesi. Unit specific equipmentj. Overhead frame and trapezek. Skin cart- Hillcrest, Supplies- Thorntonl. Crash cartm. Oxygen
i. Tanksii. Regulatorsiii. Flow meters
n. Wall suctiono. Crash Cart
Day 2 Three patient preceptor/orientee assignment1. Identify unit assignment board
a. Patient nameb. Nurse assignmentc. Physiciand. Fall precautionse. Infection precautions
2. Participate in shift rounds if appropriate 3. Receive report per unit standard4. Review medical record5. Demonstrate ability to use paging system6. Document in PCIS
Day 3 Three patient preceptor/orientee assignmentIn addition to day two activities, recommend the following: 1. Obtain and give shift report
a. 3 day trendb. Expectations for next shift
2. Participate in shift change routinesa. Walking roundsb. Unit specificc. Confirm Plan of Care with MD, HN, CN
3. Develop/ update plan of care with preceptor4. If you haven’t already, introduce orientee to Educator
Page 6

UP-PGH CBOdocument
Week 2 through
4
Demonstrates increasing responsibility and competence in providing total patient care
At the end of each week, review progress and establish goals for the next week.
Two patient assignment with direct preceptor oversight. May assist with admit or discharge, transportation of patient, administer blood etc
1. Perform general assessment 2. Completes system focused assessment (neuro, CV, GI per patient diagnosis,
needs assessment as correlated with vital signs, I&O, labs, signs & symptoms)3. Follow clinical pathways4. Develop/ revise plan of care5. Document with preceptor auditA midpoint meeting should be scheduled at the end of week four.
Participants: 1) Nurse Manager, 2) Preceptor, 3) Educator, 4) Orientee
Focus: Review progress and accomplishments of the orientee toward orientation goals.
Bring to the meeting: 1) Nursing Competency Based Orientation Pathway and 2) Planning Guide
Objectives: Review orientee strengths and accomplishments Establish plan to support and encourage the orientee to achieve independent
and interdependent practitioner roles Determine if orientation is meeting orientee’s needs Realign orientation plan to meet orientee’s needs Discuss orientee’s integration into unit culture
Insure that CBO document is up to date, identify elements for follow up on the CBO document
Page 7

UP-PGH CBOWeek 5 Identify patterns associated with
common illnesses on the unit. Trend changes in patient assessment. Begin developing formalized plan of care.
Develop system for prioritizing daily care and managing the day.
Continue with previous bedside objectives and skill acquisition and expand per CBO Pathway and as patient assignment allows.
At the end of each week, review progress and establish goals for the next week.
Two to three patient assignment in collaboration with preceptor.1.
2.
3.
4.
5.
Week 6 Continue goals from week five, focus on organization/ prioritizing/ achieving autonomy.
Continue with previous bedside objectives and skill acquisition and expand per CBO Pathway and as patient assignment allows.
At the end of each week, review progress and establish goals for the next week.
Three to four patient assignment in collaboration with preceptor.1.
2.
3.
4.
5.
Week 7 Continue with previous goals. Preceptor assumes “observer” role (orientee informing preceptor of plan of care). Orientee demonstrating increased autonomy.
Proactively develop the plan of care for assigned patients with minimal assistance from preceptor.
Continue with previous bedside objectives and skill acquisition and expand per CBO Pathway and as patient assignment allows.
Orientee to assume responsibility for a patient assignment with preceptor observation.1.
2.
3.
4.
5.
Page 8

UP-PGH CBO
Identify what duties can be appropriately delegated to other members of the healthcare team.
At the end of each week, review progress and establish goals for the next week.
Week 8 Continue with previous bedside objectives and skill acquisition and expand per CBO Pathway and as patient assignment allows.At the end of each week, review progress and establish goals for the next week.
Full assignment with backup by preceptor. 1.
2.
3.
4.
5.Schedule a meeting at the end of week eight, including: 1) Nurse Manager, 2) Preceptor, 3) Educator, 4) Orientee
Focus: Determine readiness of orientee. Identify orientee’s professional goals. Establish short and long term plans. Introduce career choices.
Bring to meeting: 1) Patient assessment, 2) plan of care, 3) vital signs, etc. for a full day of patient care and the 4) CBO document. Objectives:
Review orientee strengths and accomplishments Establish plan to support and encourage the orientee to achieve independent
and interdependent practitioner roles Determine if orientation is meeting orientee’s needs Realign orientation plan to meet orientee’s needs Discuss orientee’s integration into unit culture Insure that CBO document is up to date, identify elements for follow up on the
CBO document Evaluate documentation consistency within UP-PGH guidelines. If
documentation issues are identified, they will be shared with the orientee Evaluate readiness to complete orientation, determine future planning Develop mechanism for ongoing support, e.g. mentor, buddy
Week 9 Continue with previous bedside objectives and skill acquisition and expand per CBO Pathway and as patient assignment allows.
1.
2.
Page 9

UP-PGH CBO
Refine practice to incorporate the Nursing Process
At the end of each week, review progress and establish goals for the next week.
3.
4.
5.
Week 10
Continue with previous bedside objectives and skill acquisition and expand per CBO Pathway and as patient assignment allows.
Refine practice to incorporate the Nursing Process.
At the end of each week, review progress and establish goals for the next week.
1.
2.
3.
4.
5.
Week 11
Continue with previous bedside objectives and skill acquisition and expand per CBO Pathway and as patient assignment allows.
Refine practice to incorporate the Nursing Process.
At the end of each week, review progress and establish goals for the next week.
1.
2.
3.
4.
5.
Week 12
Continue with previous bedside objectives and skill acquisition and expand per CBO Pathway and as patient assignment allows.
Refine practice to incorporate the Nursing Process.
At the end of each week, review progress and establish goals for the next week.
1.
2.
3.
4.
5.
Page 10

UP-PGH CBOWeekly Objectives for Experienced Registered Nurse (Goal: 2 – 4 weeks orientation, variable)
WEEK PRIMARY OBJECTIVE PLAN
1
2
Familiarize new employee with Environment of Care and standards/ guidelines
(Limited patient care tasks)
On Unit:Day 1 No patient assignment for orientee the first 4 hours. Can be spent with preceptor or charge.1. Complete CBO self assessment2. Schedule weekly CBO Pathway progress meeting/ review reports3. Tour of hospital4. Scavenger hunt5. Co-assignment with preceptor
a. Blood draws6. Orientee to locate and review protocols for a. Central line b. Falls c. Restraints
7. Patient co-assignment with preceptor for remaining 8 hours of shift. a. Communication i. CPAR ii. Chain of command
Day 2Full assignment between orientee and preceptor.
a. Expand skill acquisition including documentation per CBO Pathway and as patient assignment allows
b. At the end of each day, review progress and establish goals for the next day
Day 3Full assignment between orientee and preceptor.
a. Mid-day # 3, schedule time for weekly progress evaluationb. Completion of CBO documentationc. Proactively develop the plan of care for assigned patients with minimal
assistance from preceptor
Week 2 next page
Day 4, 5, 6Orientee takes full assignment with preceptor.
a. Preceptor oversight seeking out learning experiences, commensurate with
Page 11

UP-PGH CBO
3 - 4 Focus on acquisition of nursing skills and basic patient care per CBO document
orientee’s assignment. b. Identify what duties can be appropriately delegated to other members of
the healthcare team.Mid-day, day 6
a. Weekly progress evaluationb. Meet with Nurse Manager to make competency recommendationc. Complete CBO Pathway documentation
Week 3 – 4Take full assignment.
a. Continue with previous bedside objectives and skill acquisitionb. Expand per CBO Pathway and as patient assignment allows
Meet with Nurse Manager, Educator to make competency recommendation, unit fitness
U
Page 12

UP-PGH CBO
UP-PGH NURSING Competency Based Orientation PathwayAcute Care Nursing Units
Name:____________________________________ Annual Evaluation Date:________________
( )RN
Codes for Self Assessment: 0 = No prior experience 1 = Limited experience 2=Performs independently
Code for Method O = Observation S = Simulation/Demo CR = Chart Review V = Verbalization
RESOURCES
Follow up:
FOLLOW UP EVALUATOR'S
INITIALS
Enter Name of Supervisor/ Manager for follow up
PROCEDURE OR SKILL
Self
Ass
ess EVALUATOR
ASSESSMENT METHODFOLLOW UP FOR "DOES NOT MEET"
ASSESSMENT
Met Date Initials Date Initials
GENERAL ASSESSMENT
Obtains head to toe assessment every shift (q12h) and prn changes in patient condition or per MD order Reviews history and physical, medical record, and pertinent nursing documentation on admission Assesses overall general appearance Obtains, assesses and trends vital signs per routine, prn changes in patient condition or per MD order Assesses patient response to illness and treatment: changes in body image, self concept, role performance Identifies problems from the assessment and formulates a plan of care Collaborates with patient/family to identify expected outcomes
NEUROLOGIC/BEHAVIORAL Assesses mental status, orientation using Glacow Coma Scale (GCS)
Identifies abnormal findings:anxiety, agitation, Page 13

UP-PGH CBOcombativiness,seizures, CSF drainage, s/s of increased ICP (blurred vision, slurred speech, weakness, progressive sleepiness, vomiting, worsening headache, unequal pupils, changes in respiratory pattern) Assesses patient for warning signs of stroke: sudden onset of the following weakness, speech difficulty or confusion, visual difficulty, dizziness, trouble walking or loss of balance, severe headache with no known cause Verbalizes how and when to call a Stroke Code Demonstrates computer resources and education materials located on stroke center website Inspects head and neck for sutures, dressings, drains Assesses sensory impairments (visual,hearing, smell and sensation) Performs bedside water swallow screening test Performs Interventions Modifies nursing care related to sensory impairments Teaches patient warning signs of stroke Monitors and maintains dressings/drains Documents assessment, problems & interventions Identifies and describes seizure activity Initiates and manitains spinal precautions as needed Performs neuromuscular assessment Performs focused neurological assessment in patient with neurological deficits: pupil checks, motor strength and sensory function, gait and balance Intiates aspiration precautions as indicated Collaborates with MD and speech pathology for dysphasia evaluation Follows spinal precautions (neuro/trauma/ ortho) Documents assessment, problems & interventions Verbalizes neurologic changes associated with aging: decreased reaction time, decreased response to painful stimuli, changes in speech and mobility, changes in sense of smell, taste,sensation. Verbalizes likelihood for intracranial bleed in geriatric trauma victims PULMONARY SYSTEM Performs Assessment
Page 14

UP-PGH CBOAssesses patency of airway, rate, depth, pattern of respirations, oxygen saturation, skin pallor, sputum production Auscultates breath sounds and identifies adventitious breath sounds
Recognizes signs and symptoms of respiratory distress or airway obstruction: tachypnea, use of accessory muscles, increased respiratory effort on inspiration, forced or protracted expiration, snoring, crowing or stridor, asymmetrical chest movement, cyanosis
Reassesses patient within 30 minutes after changes in oxygen therapy or respiratory treatments
Assesses patient with chest tube for sub q emphysema,dressing is dry, intact and occlusive.
Assesses chest tube/drainage device for patency, integrity, water seal, tidaling, suction water levels, amount, color & consistency of drainage, air leak, device below level of chest tube, secured using nylon bands; tubing is placed in a non dependent position
Evaluates effectiveness of oxygen therapy by checking oxygen saturation, ABGs, and work of breathing
Identifies and reports abnormalities: shallow irregular breathing, hypo/hyper ventilation, dyspnea, apnea, hemoptysis, SOB, use of accessory muscles and abdominal breathing.
Performs Interventions Initiates and maintains oxygen device: nasal cannula, mask, non rebreather mask, oximizer, trach collar
Inserts oral or nasopharyngeal airways per patient condition.
Obtains and verifies accuracy of pulse oximetry values (pulse reading matches actual pulse)
Demonstrates use of bag valve mask Positions patient to maximize oxygenation Performs trach care every shift and prn: suctions patient, inspects and cleanses skin surrounding stoma, applies dressing and changes trach ties as needed. Cleans or inserts new inner cannula every 24 hours.
Page 15

UP-PGH CBOEnsures tracheostomy equipment at bedside: suction canister/set-up, suction catheters, replacement trach of same size, obturator, disposable inner canula,ambu bag,NS, oxygen regulator and delivery system
Ensures chest tube supplies are at bedside: sterile water or NS, Vaseline gauze, 4X4's, clamp, tape
Obtains sputum specimen collection Reviews diagnostics/labs, CXR, sputum, ABG, PFT, culture and sensitivity, angiogram/VQ scan
Describes safety measures when transporting a patient with a chest tube: verifies with MD if okay to be off suction, removes suction port tubing and does not cover or clamp any tubing, and ensures chest drainage device below level of chest tube insertion
Demonstrates chest tube drainage device set up and replacement
Collaborates with Respiratory Therapy (RT) for changes in patient's respiratory effort, BiPAP needs
Assess patient's response to BiPAP therapy and maintains BiPAP supportive therapy(effective seal, skin integrity, comfort, calming measures)
Demonstrates effective airway management: opens airway and removes secretion &/or foreign bodies
Educates and encourages patient to use secretion mobilization devices: incentive spirometer, PEP, and flutter device
Documents assessment, problems and iinterventions CARDIOVASCULAR Performs Assessment Auscultates heart sounds (S1,S2), apical pulse Identifies & reports abnormalities: chest pain, hypo-hypertension, tachycardia > 100 beats /min, bradycardia < 60 beats/min, irregular heart rate. Absent, weak, bounding or thready pulse. Pale, cyanotic or mottled skin color.Capillary refill > 3 seconds, edema, shortness of breath, jugular venous disention.
Assesses vital signs and oxygen saturation. Palpates peripheral pulses for rhythm, amplitude and bilateral equality
Assesses peripheral pulses using a Doppler
Page 16

UP-PGH CBOAssesses peripheral perfusion e.g. skin temp, color,capillary refill
Assesses fluid volume status ( excess versus deficit), daily weight, edema,s/s CHF.
Assesses AV fistula and/or AV graft for bruit, thrill, pulse, and condition of dressing or drainage if present
Monitors cardiac rhythm and analyzes and interprets the following rhythms; normal sinus rhythm, tachycardia, bradycardia, PAC, PVC, atrial fibrillation/flutter, ventricular tachycardia/fibrillation
Verbalizes cardiovacular changes associated with aging: irregular apical pulse, murmurs, ECG abnormalities, hypertension, orthostatic/postural hypotension
Performs Interventions Verifies vital signs prior to administering cardiovacular medications
Reviews parameters for medication administration (PCAR/MAR, patient condition)
Administers and evaluates patient's response to medications including but not limited to: diuretics, digoxin, antihypertensives, dysrhythmics and anti-thrombotics.
Applies and maintains anti-embolism stockings/ sequential compression devices. Identifies time off is limited to 1 hour every 12 hours. Reviews chest x-ray report and verifies MD awareness of results if abnormal Reviews labs/ diagnostics: troponin, CK, CKMB, cardiovascular drug levels, Hgb, Hct, basic metabolic panel, lipid panel, ECG, echocardiogram, stress test and/ or nuclear medicine scans
Positions patient for comfort and optimal circulation
Documents patient's tolerance in performing ADL's Assesses for patient smoking cessation needs; offers cessation program information Assesses appropriate diet, medication, life style choices. Completes and documents acute MI and Heart Failure Core Measures
Page 17

UP-PGH CBO
Educates, teaches and completes discharge information specific to cardiovascular disease. Provides education booklet re: heart disease. Informs MD of rhythm abnormalities, abnormal labs, hemodynamic changes; and telemetry changes
Connects epicardial/transvenous wires to pacemaker and presses emergency button as indicated. Applies transcutaneous pads and connects to pacemaker module, turns device on, sets rate to 60 and MA at 20
Documents assessment, problems & interventions Documents patient's tolerance of performing ADL's
Documents rhythm when obtaining a set of vital signs
GASTROINTESTINAL SYSTEM Performs Assessment Inspects, auscultates, and palpates the abdomen Assesses oral cavity Assesses nutritional status; labs, intake, calorie count, weight, swallowing impairment, food preferences
Evaluates nutritional and fluid intake. Collaborates with nutrition services when indicated.
Assesses all GI drains/ tubes; patency, output, color, consistency & amount of drainage
Assesses enteral feeding devices and site Identifies abnormalities: oral mucosa, infections of the mucosa, altered bowel sounds, muscle wasting, abdominal pain, jaundice, changes in bowel habits, constipation , diarrhea, stenorrhea, nausea, vomiting, hemoptysis, hematemesis, evidence of dysphasia or aspiration
Assesses presence of ostomy: output, stoma viability, skin condition
Verifies and documents daily bowel movement Evaluates geriatric age related changes: Increased gastric emptying time, decreased salivary flow, decreased absorption, decreased gastric acid secretion, reduced gastrointestinal motility resulting in alteration in drug metabolism and bowel habits.
Evaluates fluid & electrolyte status related to nausea,
Page 18

UP-PGH CBOvomiting, & diarrhea and implements treatment regimenEvaluates lab results: albumin, pre-albumin, total lymphocyte count
Verifies initial placement of small bore feeding tube by x-ray report. Marks and documents tube length at nare.
Ongoing assessment for nasal feeding tubes: verifies that marking is at nare, tube is not coiled at back of throat.
Assesses for watery eyes, coughing and changes in vocal quality which indicates incorrect tube placement
Performs Interventions Inserts and maintains nasogastric tube for suctioning and/or small bore feeding tubes for nutrition
Maintains patency of feeding tubes. Flushes with NS q 4-6 hr, & before and after medications
Uses aseptic technique when handling enteral feeding: washes hands, dons non sterile gloves when setting up tube feeding, administering meds, checking residual.Uses med administration port when giving meds or checking residual.
Administers medications via a gastric or nasogastric tube
Confirms placement of nasogastric tube by auscultation of injected air and aspiration of stomach contents (if able).
Administers medications to alleviate constipation and/ or diarrhea
Collaborates with MD and institutes a bowel management program
Performs administration of enema, suppositories
Prepares patients for GI diagnostic testing
Collaborates with MD for stress ulcer prevention
Trends and evaluates weight changes Documents amount of food ingested by number of items eaten (1-5)
Documents intake and output
Page 19

UP-PGH CBOEnsures oral care for patient's with stomatitis, herpes simplex of mouth is provided, NPO or ADL dependent
Maintains apiration precautions: HOB elevated 30 degrees, suction at bedside, proper placement of cervical collar , high semi-fowler's for 30 mnutes after eating
Acute Care Guidelines of Care
Collaborates with pharmacy to identify medications that cause or relieve nausea or anorexia
Monitors NPO status and collaborates with MD and nutrition to ensure adequate nutritional intake
GENITO-URINARY SYSTEM Performs Assessment Reviews patient history for renal insuficiency, renal failure, renal transplant
Inspects perineal area and assesses mucous membranes
Reviews patient's record to determine clinical conditions that may effect fluid status; e.g. ESRD, renal insuficiency, CHF, dehydration
Performs bladder volume assessment using the bladder scanner
Monitors intake and output Assesses urinary devices for patency, amount, color & clarity of drainage
Assesses for bladder spasms/discomfort and implements treatment
Obtains and labels lab specimens as ordered or indicated for patient's condition
Assesses perineum Performs Interventions Collaborates with MD to ensure optimal fluid management
Secures urological tubing with securement device Obtains & labels specimen from catheter Demonstrates irrigation of urological catheters; e.g. manual, IBI, CBI (use of sterile irrigant and equipment)
Evaluates urinary output (color, quantity, clarity, odor, etc).
Page 20

UP-PGH CBOEvaluates for changes in urinary patterns (frequency, urgency, pain, burning )
Obtains and labels 24 hour urine collection sample Verbalizes that NO blood pressure readings, lab draws or IV starts are done in extremities with hemodialysis access or anticipated hemodialysis access
Identifies adverse effects of hemodialysis: bleeding, hypotension and hyperglycemia
Administers pain, insulin, anticonvulsant medications irrespective of hemodialysis; consults with MD to hold all other medication categories
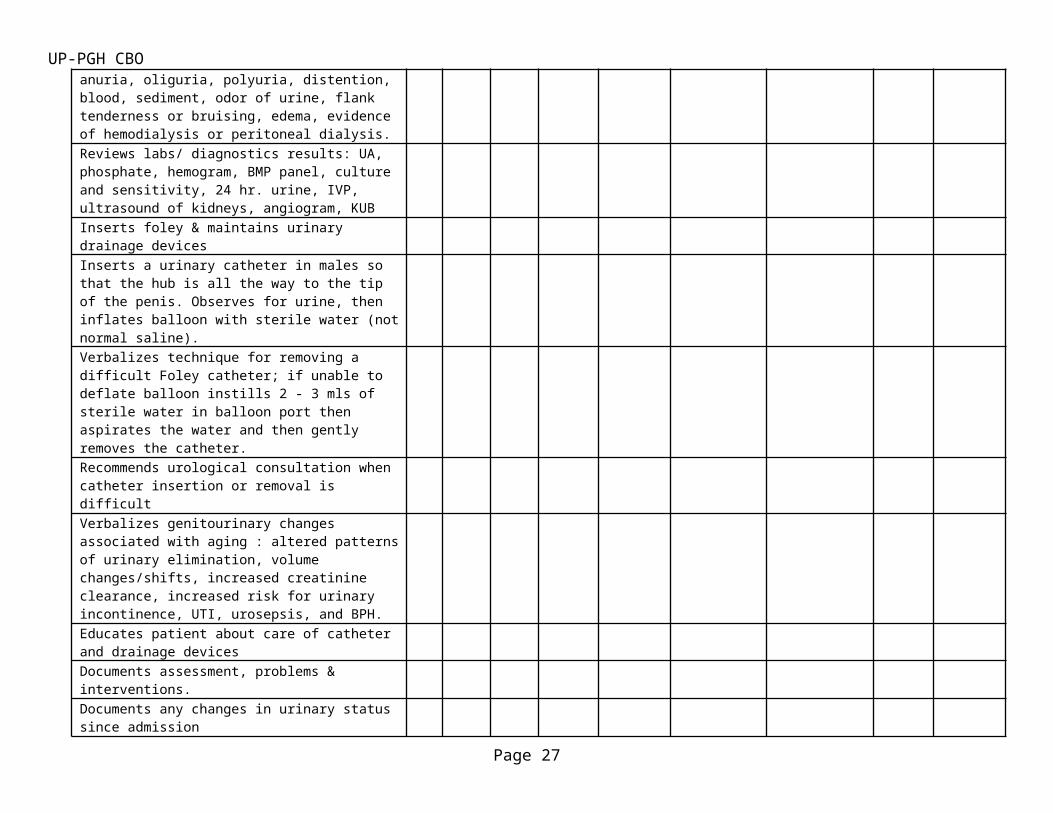
Verbalizes abnormal findings: pain, dysuria, increased urinary frequency, anuria, oliguria, polyuria, distention, blood, sediment, odor of urine, flank tenderness or bruising, edema, evidence of hemodialysis or peritoneal dialysis.
Reviews labs/ diagnostics results: UA, phosphate, hemogram, BMP panel, culture and sensitivity, 24 hr. urine, IVP, ultrasound of kidneys, angiogram, KUB
Inserts foley & maintains urinary drainage devices Inserts a urinary catheter in males so that the hub is all the way to the tip of the penis. Observes for urine, then inflates balloon with sterile water (not normal saline).
Verbalizes technique for removing a difficult Foley catheter; if unable to deflate balloon instills 2 - 3 mls of sterile water in balloon port then aspirates the water and then gently removes the catheter.
Recommends urological consultation when catheter insertion or removal is difficult
Verbalizes genitourinary changes associated with aging : altered patterns of urinary elimination, volume changes/shifts, increased creatinine clearance, increased risk for urinary incontinence, UTI, urosepsis, and BPH.
Educates patient about care of catheter and drainage devices
Documents assessment, problems & interventions. Documents any changes in urinary status since admission
Page 21

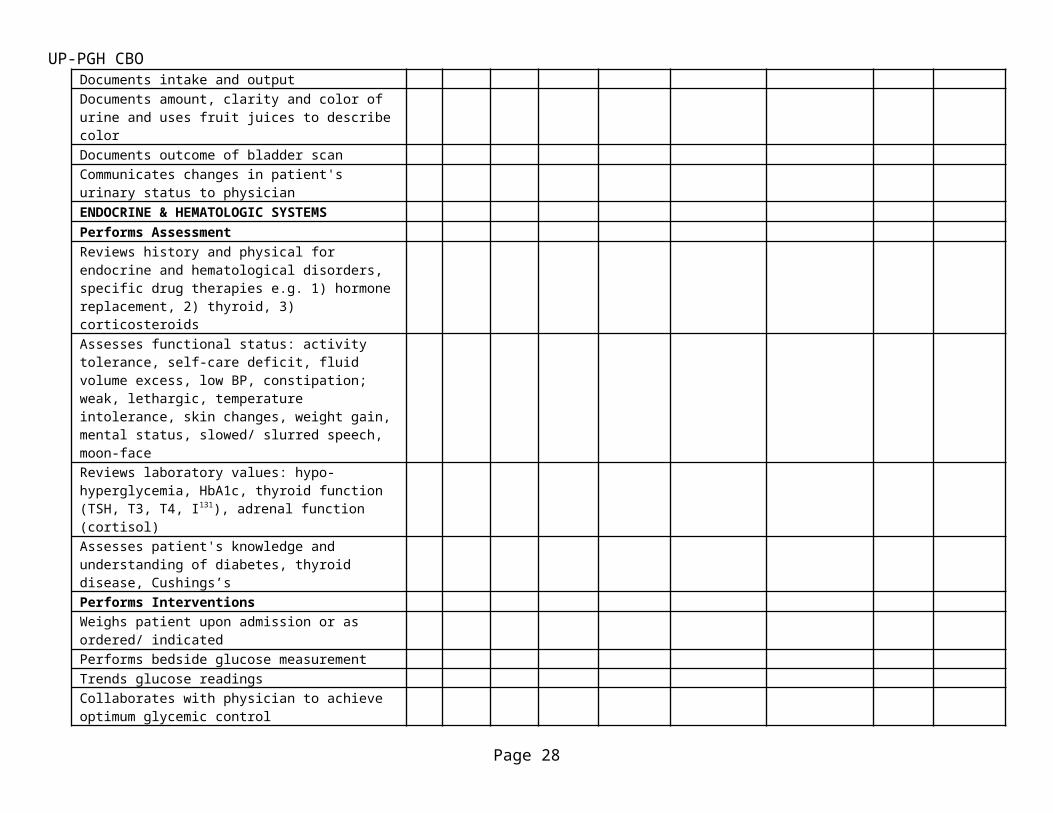
UP-PGH CBODocuments intake and output Documents amount, clarity and color of urine and uses fruit juices to describe color
Documents outcome of bladder scan Communicates changes in patient's urinary status to physician
ENDOCRINE & HEMATOLOGIC SYSTEMS Performs Assessment Reviews history and physical for endocrine and hematological disorders, specific drug therapies e.g. 1) hormone replacement, 2) thyroid, 3) corticosteroids
Assesses functional status: activity tolerance, self-care deficit, fluid volume excess, low BP, constipation; weak, lethargic, temperature intolerance, skin changes, weight gain, mental status, slowed/ slurred speech, moon-face
Reviews laboratory values: hypo-hyperglycemia, HbA1c, thyroid function (TSH, T3, T4, I131), adrenal function (cortisol)
Assesses patient's knowledge and understanding of diabetes, thyroid disease, Cushings’s
Performs Interventions Weighs patient upon admission or as ordered/ indicatedPerforms bedside glucose measurement Trends glucose readings Collaborates with physician to achieve optimum glycemic control
Evaluates patient for signs and symptoms of hypo-hyperglycemia
Initiates dietitian consultation Assesses need for laboratory testing, collaborates with MD on use of hematopoietic growth factors
Initiates hypoglycemia protocol when indicated. Verbalizes location of hypoglycemia protocol.
Educates patient with focus on knowledge deficits identified in the diabetes assessment form.
Documents assessment, problems & interventions
Page 22

UP-PGH CBODocuments glucose readings, episodes of hypoglycemia and treatment and patient's response
Documents diabetes education Documents that the diabetes education booklet was provided and written information was given to the patient.
Documents the titles/names of written information given to patient in the plan of care
Documents pt/family understanding of diabetes education
Maintains appropriate temperature comfort measures (blankets, circulation)Tracks signs & symptoms of thyroid over-medication (tachycardia, nervousness, insomnia)MUSCULOSKELETAL SYSTEM Performs Assessment Reviews H & P, operative report, trauma reportPerforms pain assessmentInspects musculoskeletal system: spinal alignment, gait, extremities, strength Compares affected to unaffected side/extremity Identifies abnormalities: spinal curvatures, kyphosis, loss of height, asymmetry, dislocations, contractures, stiffness or fixation of joint, deformity, evidence of fracture or dislocation, tenderness, warmth, coolness, moistness, skin changes, bone or joint crepitus, numbness and tingling. Identifies abnormal findings: numbness, parasthesia, flaccidity, lack of muscle movement, weak, thready, or bounding pulses, compartment syndrome Assesses affected areas for variation in skin color, skin temperature, skin turgor, nodules, masses, swelling, hematoma Assesses body position, mobility & muscle strength Assesses pulses, capillary refill, movement and sensation of affected extremities Assesses orthopedic appliances for proper application, including but not limited to: traction, Halo, external fixator, continuous passive motion, cast, sling, splint
Page 23

UP-PGH CBOAssesses for complications related to ortho devices (e.g. skin breakdown, increase in pain, improper placement), loosening of screws, pins Evaluates range of motion. . Assesses patients admitted with orthopaedic devices: e.g. external fixators, halo, casts, braces, slings
Assesses neuromuscular and neurovascular status of affected area. Compares to unaffected side. Performed together by the off-going & on-coming RN.
Evaluates labs/diagnostics: CBC, calcium, phosphorus, sedimentation rate (ESR), rheumatoid factor (RF), C-reactive protein (CRP), x-rays, bone scans, MRI, Mylogram, CT scan, EMG, culture & sensitivity, SGOT, uric acid, PT, PTT, INR
Maintains total hip, knee, spine and fall precautions Assesses use of and/or need for assistive device Verbalizes musculoskeletal changes associated with aging: loss of muscle and bone, decreased muscle strength, frail bones, decreased coordination, gait changes, increased muscle fatigue, kyphosis
Identifies needs of patients with spinal cord injury, amputation, quadraplegia, hemiplegia, and/or paraplegia
Performs secondary post trauma assessment Assesses bowel/bladder patterns and identifies abnormalities
Assesses proper assembly of overhead frame and trapeze
Performs Interventions
Notifies MD of alteration in motor function or sensation of extremities
Applies & maintains orthopaedic devices: braces, kydex jacket, CPM, knee immobilizer, slings, prostheses and/ or orthotics, post operative shoes
Utilizes appropriate assistive devices Collaborates with OT, PT, Ortho Technician Utilizes joint arthroplastic clinical pathways Educates patient and family on signs and symptoms of common complications associated with musculoskeletal injury: surgical site and bone
Page 24

UP-PGH CBOinfection, hemorrhage, VTE (PE, DVT), compartment syndrome, neurovascular compromise, fat emboli, dressing /cast constriction, immobilityReinforce safety measures related to ADL's secondary to changes in center of gravity
Evaluates sensory/motor effects of regional nerve block
Ensures antibiotics are administered in accordance with Surgical Infection Prevention Guidelines
Applies elevation and ice as indicated Maintains traction Collaborates with case manager & social worker to assist with discharge needs
Performs pin site care Provides VTE prophylaxis: pharmacologic, sequential compression devices, ankle pumps
Assesses and communicates lab results to MD Follows spine precautions (cervical collar per MD orders, full log role, order specialty bed, used slideboard)Documentation Documents assessment of abnormal findings, problems & interventions. Recognizes critical changes and contacts MD Documents appliances, devices, mobility status Documents skin integrity Documents neuromuscular and vascular status Documents and trends labs (Hgb and Hct, PT, PTT, INR) Documents reporting abnormalities to MD Documents nutritional intake and output Documents patient's adherence to mobility restrictions Documents non pharmacological interventions for comfort Documents patient’s moodSKIN AND WOUND Performs Assessment Assesses skin for intactness, integrity, moisture, dryness, edema Assesses need for specialty bed Inspects hair, nails, and skin for cleanliness
Page 25

UP-PGH CBODetermines pressure ulcer risk using Braden Scale on admission, every shift and changes in patient condition Assesses skin closures for sutures, staples, and other skin closures Assesses intactness and appropriateness of dressing and drainage q shift, prn and changes in patient condition Assesses and reassesses character of wounds with each dressing change. Not to exceed 7 days Assesses bony prominences Verbalizes skin changes associated with aging: decreased moisture, elasticity, friability, mobility, sensation. Inventories factors associated with skin breakdown; e.g. chronic illness, medications Identifies abnormalities: rash, itching, lesions, masses, wounds and surrounding tissue, pressure ulcers, break in skin integrity, stoma,drainage, hematoma, ecchymosis, infections, pain, tightness, non healing wounds, dehiscence, evisceration Performs Interventions Initiates skin care protocols Documents wounds including staging, length, width, depth, appearance, drainage, presence of slough or necrosis, type of dressing Photographs wounds upon admission, weekly, discharge and changes in wound condition Initiates consultation to Surgical wound team for unresolved skin issues Encourages and provides daily hygiene Collaborates with MD for podiatry referral Applies and maintains dressings as indicated Removes any dressing from another institution upon admission and evaluates wound 9 Participates in wound and skin surveys 9 Educates patient and family regarding wound, wound care and methods to relieve pressure and enhance adequate circulation Verbalizes indications and maintainence of wound vac Collaborates with Wound Ostomy Continence Doctor for stage 3 and stage 4 wounds (full thickness
Page 26
UP-PGH CBOwounds)Provides the following measures to prevent skin breakdown: turn q 2hrs, pads bony prominences, use of pillows, raises heels off bed, moisturizes dry skin, cleans incontinence as soon as possible Collaborates MD for application of pressure reducing/relieving devices for beds and chairs Encourages and promotes optimal nutritional intake. Considers nutrition consult
Sets up lifting devices: trapeze, overbed frames Implements use of lift team when applicable Obtains and labels wound culture Documents assessment, problems & interventions Documents wound status, changes in condition Documents use of special mattress Documents turning schedule
Documents dressing change: time, date, size, odor, drainage, treatment
Documents stoma color, moisture, position and drainage
Documents wound culture obtained Documents education to patient and family for optimal skin care and prevention of skin breakdown
PAIN/COMFORT Performs Assessment Assesses patient's pain using hospital approved scales on admission, at beginnning of every shift, with each set of routine vital signs and with any procedures or activity in which pain may be anticipated and/or every 4 hours
Assesses pain related to intensity, location, quality, pattern, onset/duration, intervention and effect of intervention
Reassesses patients comfort level if pain score is equal to or greater than 4, 1 hour after IM/IV medications, 2hr after oral medications until pain controlled and with each set of routine vital signs Reviews medical record for type of surgery or procedure, disease states associated with moderate to severe pain e.g. sickle cell crisis,
Page 27
UP-PGH CBOimmunosupression (HIV, diabetes, cancer), joint disease, shingles, as well as anesthetic or analgesic medications administeredAsks patient to determine acceptable level of pain/individual pain goal on initial screening and PRN Obtains patient's analgesic history including opioids, non-opioids, and adjuvant analgesics, e.g. anti-convulsants, anti-depressants Obtains patient's history of non-drug pain therapies Identifies abnormal findings associated with unrelieved pain: increased BP, HR, RR, behavioral changes, diaphoresis, grimacing, guarding, hypoventilation, abdominal rigidity, atelectasis, fatigue, sleep deprivation Validates patient's advocate/family report of pain Differentiates between patient's pain, anxiety, confusion, delirium and identifies when to use the RASS scale (+4 to 0 to -5)
Verbalizes pain issues related to aging: concept of pain, reporting pain, altered ADLs, depression
Assesses chronic pain management and effectiveness
Performs Interventions Administers pain/comfort medications based on patient's self-report/nonverbal behaviors and nurses assessment of patient's physiological status (e.g. BP, RR, O2 sat)
The Nursing Practice Act Section 2725 (B)(1)
Monitors patient's response to pain medications: relief or reduction in pain as well as adverse effects of medications (e.g. hypotension, hypoventilation, itching, N/V, constipation and altered mental status,
Collaborates with MD to ensure timing of pain management regime. Addresses need to change medication schedule if periods of uncontrolled pain exist
Implements non-pharmacological measures for treatment of pain/discomfort; e.g. elevation, ice, positioning, massage, distraction therapy
Advocates for adjunctive holistic therapies when requested by the pt/family
Page 28

UP-PGH CBOPerforms set up of pain management devices (parenteral or epidural) and attaches to patient
Teaches patient how to use pain management devices. Reminds family/friends to not activate pain management device
Trends patients response to and satisfaction with pain management
Monitors regional nerve block devices for patency, leakage, dislodgement, and effectiveness
Verbalizes /demonstrates how to deliver a bolus of medication through epidural and PCA catheters
Collaborates with primary MD for referral to Pain Management Service
Ensures all epidural tubing is labeled with epidural signs
Demonstrates use of non verbal pain scale to rate non verbal patient's pain
DOCUMENTATION Documents assessments, problems, and interventions on designated pain management record
Documents comprehensive pain management history on PADB (Patient Admission Database)
Documents pain rating and in the pain assessment/reassessment screen
Initiates pain as a problem in the plan of care Utilizes the elements of informed consentSAFETY PRECAUTIONS Verbalizes isolation precautions; AFB airborne, airborne, droplet, contact and neutropenic
Aspiration, bleeding, falls, infection, neutropenia, restraints, seizure precautions, disaster preparedness
Provides safe environment: side rails up, call bell within reach, bed in low position, room clear of clutter, sufficient lighting
Lists or knows where to find safety goals EMERGENCY RESPONSE Performs Assessment Describes and Initiates emergency code response Implements cardiopulmonary resuscitation, when
Page 29

UP-PGH CBOindicatedAssesses status of Advanced Directive content Assesses for DNR order Performs Interventions Documents Assessment, Problems and Interventions Patient Education Assesses learning needs and barriers Performs periodic reassessment of needs Identifies best method of learning for pt/family Performs Educational Interventions Reviews discharge instructions with patient and/or responsible adult
Educates patient/family of treatments or devices requiring home care upon discharge / e.g. injections, assistive devices, drains, dressings, irrigation catheters, etc.
Ensures return demonstration of teaching MCP 380 Provides printed discharge instructions to patient Ensures patient or responsible adult signs discharge instructions DOCUMENTATION Documents Assessment, Problems and Interventions Medication Management Performs Assessment Assesses patient for possible contraindications of medications prescribed
Checks resources for identified drug allergies Instills eye lubricants and drops MCP 380.1 Assesses need for & response to PRN meds MCP 305.1 Performs Interventions MCP 380.1 Verbalizes the 5 Rights of medication administration Follows hospital guidelines for administration of high-risk medications
Maintains medication areas neat and free of clutter/trash
Verbalizes multi dose vial policy and labels multi-dose vial with expiration date Obtains access to Pyxis. Removes medications from Pyxis Logs into Pyxis device and obtains medications, exits
Page 30

UP-PGH CBOafter use
Verbalizes definition of Adverse Drug Reaction Initiates and or edits the Medication Reconciliation form Collaborates with MD and/or pharmacist to ensure continuity of medication regimen Reviews Medication Reconciliation form on discharge for accuracy and educates patients on medication regime to continue upon discharge Assesses patient response to medication and intervenes if indicated Documents all medications administered Documents Assessment, Problems and Interventions Intravenous Therapy Performs Assessment Verbalizes changing field IV access site within 24 hours of admission to the hospital if patient a trauma victim Selects IV catheter size according to patient need Assesses for presence of central and peripheral venous access; identifies infiltration, occlusion and dislodgement of catheters Performs venipuncture according to policy Maintains & changes dressings per standards Maintains & utilizes saline locks according to standards Utilizes non free-flow devices with all infusion pumps. Demonstrates free-flow check. Utilizes/maintains pumps per manufacturer guideline States/demonstrates proper procedure for D/C IV BLOOD ADMINISTRATION Assessments Verifies MD order for transfusion of blood product, differentiates that an order for a type and cross match is not an order to transfuse Verbalizes indication for transfusion Verifies consent for blood transfusion is present in chart, if not notifies MD Verbalizes that each blood administration tubing is
Page 31

UP-PGH CBOgood for 4 hours or 2 units of blood products whichever occurs firstAssesses that IV access for patency and that needle gauge is 22 g or larger
Verbalizes that all blood products (except Clotting Factors 8, 9 and Rhogam) require a blood filter
Verifies with second licensed person the transfusion order. Verifies the blood bag matches the transfusion record. This includes 1.) donor and recipient ABO type, 2.) expiration date, and 3.) blood unit number
Verifies at the bedside the patient's name and ID on the patient's armband matches with the transfusion record.
Documents with 2 signatures on the transfusion record Verbalizes signs and symptoms of transfusion reaction Verbalizes actions to be taken in the event of a transfusion reaction
Verbalizes that IV pump may be used for blood administration. Performs Interventions Returns blood /blood product to Blood Bank if not used within 30 minutes of removal from Blood Bank
Completes Blood Product Pick -Up form, pick up blood product from Blood Bank Verifies baseline vital signs were obtained within 30 minutes before the start of transfusion
Obtains vital signs 15 minutes after start of infusion and observes pt. closely. May delegate remainder of vital signs every hour until transfusion completed
Completes infusion of blood within 4 hours of removal from blood bank
AUTO TRANSFUSIONS
Assessment
Verbalizes use of micro-aggregate filter in addition to filter in standard blood administration set
Completes infusion of salvaged (shed) blood within 8 hours of drain insertion
Page 32

UP-PGH CBOPerforms Interventions Verifies baseline vital signs were obtained within 30 minutes of start of transfusion
MCP 617.1
Obtains vital signs 15 minutes after start of infusion and observes pt. closely. May delegate remainder of vital signs every hour until transfusion completed or discontinued
Documents vital signs, amount of blood product infused and if a patient has had a transfusion reaction on the transfusion record
Spiritual Care/Psychosocial Care Performs Assessment Assesses spiritual perspective of health Assesses spiritual needs during treatment Performs Interventions Verbalizes indications for contacting Social Work and Pastoral Care Demonstrates ability to access Social Work and Pastoral Care Provides means to meet spiritual needs Considers spiritual needs when providing care Addresses spiritual needs in Plan of Care Advocates for patient's requests for chaplaincy/spiritual counsel Focus Areas Restraints and Seclusion Performs Assessment Initiates alternative measures to use of restraints: e.g. de-escalating behavior, moving bed closer to nurses station, family members at bedside, judicious use of medications, distraction techniques
Identifies patients at risk for needing restraint Differentiates between the need for medical vs. behavioral restraint Applies and maintains restraints, obtains MD order within 12 hours of applying restraint
Reassesses need for continuing restraints every 2 hours Properly applies restraints Monitors restrained patient at required time intervals Documents Assessment, Problems &
Page 33

UP-PGH CBOInterventionsChecks presence and timeliness of MD order and renewal order Completes restraint seclusion documentation form frequency? Appropriately enters patient data in Unit log book COMMUNICATION Communicates clearly and concisely Gives change of shift /hand off report that includes patient age, dx, problems, plan of care treatments, interventions, response to care and progress in attaining goals Prioritizes care using critical thinking, trending of vital signs, data, monitoring, timeline strategies and specified goals. Evaluates and communicates results. Demonstrates paging system including phone page, emergency page. Delegates tasks and assignments appropriately to members of the team to include: NA, INTERNS, RN, other clinical staff Makes shift change rounds with on-coming RN Verbalizes how and when to obtain intepreter services: must be used for consent, relaying of diagnoses and assessment Identifies needs of diverse populations, cultures and custodial patients
Recognizes and communicates an appropriate plan for dealing with an ethical dilemma; requests an ethics consultation Communicates risk management issues by communicating with charge nurse, nurse manager and completing of QVR (Quality Variance Report) Contacts security to assist with management of aggressive, combative, attempting to elope or sign out patients
Unit Management Performs tour of nursing units, nutrition services, discharge pharmacy, inpatient pharmacy, cafeteria, conference rooms, Interventional Radiology, Lab, and Radiology
Reviews location and contents of: mailboxes, Page 34

UP-PGH CBOresource manuals (unit, equipment and competency), intranet, MCPs, patient refreshments, patient education materialsUses hospital operator to determine physician on call or uses scheduling in web reference to locate on call physicians Locates and reviews work schedule Locates and documents on appropriate schedule forms the following: requesting specific schedule, vacation time, education leave, floating holidays Uses ATM system for payroll Locates fire alarms and verbalizes use Locates fire extinguisher and demonstrates use if trained Locates oxygen shut off valve and verbalizes how to shut off if instructed to do so Locates emergency exits and reviews emergency evacuation routes INTERVENTION Activates code system and demonstrates use of code alerts: ADAM = abducted or missing infant/child BLUE = medical emergency response ORANGE = internal hospital emergency PINK = maternal/child emergency RED = fire response TEN = bomb threat GREY = disruptive or violent behavior TRIAGE = mass casualty STROKE CODE=new onset stroke symptoms TAN = Bomb Threat GREY = Disruptive Behavior TRIAGE = Mass casualty
STROKE = New onset of stroke symptoms Accesses Web-Outlook once a shift and PRN Accesses web reference for clinical guidelines, micromedex, care notes, policies and procedures, physician schedules INTERVENTIONS
Verbalizes and demonstrates use and problem solving of the following equipment: beds, gurneys,
Page 35

UP-PGH CBOmonitors (set-up, alarm settings, pressure lines), IV pumps, PCA device, epidural/regional device, sequential compression devices, auto-transfusion devices Is there a checkoff for this??PROFESSIONAL NURSE Informs patient of rights and responsibilities Advocates for pt./family by 1.) Assisting them to define needs and establish goals 2.) Participates in decision making 3.) Provides care congruent with pt./family needs/goals 4.) Upholds pt./family rights 5.) Demonstrates cultural competency Maintains professional appearance Wears name badge while on duty with photo clearly visible Demonstrates an attitude of respect for patients, visitors and employees Signatures: include initials with full signature & title. example: JSD- Juan S. David, RN Orientee Preceptor 1 Preceptor 2
Page 36

Page 37