university of groningen optimizing therapy in patients
TRANSCRIPT

University of Groningen
Optimizing therapy in patients with atrial fibrillation and heart failureMulder, Bart Antonius
IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite fromit. Please check the document version below.
Document VersionPublisher's PDF, also known as Version of record
Publication date:2015
Link to publication in University of Groningen/UMCG research database
Citation for published version (APA):Mulder, B. A. (2015). Optimizing therapy in patients with atrial fibrillation and heart failure. University ofGroningen.
CopyrightOther than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of theauthor(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons).
The publication may also be distributed here under the terms of Article 25fa of the Dutch Copyright Act, indicated by the “Taverne” license.More information can be found on the University of Groningen website: https://www.rug.nl/library/open-access/self-archiving-pure/taverne-amendment.
Take-down policyIf you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediatelyand investigate your claim.
Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons thenumber of authors shown on this cover page is limited to 10 maximum.
Download date: 22-02-2022

Atrial Fibrillation in CRT
109
Abstract AimsTo study the outcome of patients with atrial fibrillation (AF) treated with cardiac resynchronization therapy (CRT) in a tertiary referral center as data on CRT in these patients are sparse.
MethodsResponse was defined as left ventricular end-systolic volume reduction ≥ 15% at 6-months follow-up. Rate control was strictly instituted in order to obtain 100% biventricular pacing (assessed with exercise testing). In case of failure, atrio-ventricular nodal (AVN) ablation was performed.
ResultsOf 491 patients, 200 (41%) had a history of AF at baseline, 50 (10%) developed new-onset AF during follow-up. The other 241 (49%) patients never had AF during follow-up. Patients with AF were older and left atrial volume was larger (50 versus 38ml/m2). Twenty-seven patients (12 with AF at baseline) died before response assessment, 15 (56%) due to progression of heart failure. AVN ablation was eventually performed in a total of 28 (11%) AF patients. Echocardiographic CRT response rate was comparable in AF versus sinus rhythm patients (53% versus 56%, p=0.5). After a mean follow-up of 1.9±1.0 years cardiovascular mortality or heart failure hospitalization was comparable between patients with AF and sinus rhythm. Early new-onset AF (< 6 months after CRT implantation) was associated with worse prognosis (p=0.006).
ConclusionResponse and cardiovascular morbidity and mortality were comparable in patients with AF and with continuous sinus rhythm. New-onset AF occurring early after CRT implantation, however, was associated with impaired prognosis.
Chapter 7Cardiac resynchronization therapy in patients with and without atrial fibrillation.
Submitted
Bart A. MulderMariëlle KloostermanMichiel RienstraRogier P.M. MullerDirk J. Van VeldhuisenIsabelle C. Van GelderAlexander H. Maass

110
Atrial Fibrillation in CRT
111
CHAPTER 7
at the outpatient clinic for regular follow-up and for CRT interrogation at baseline and 6-monthly thereafter. All patients underwent echocardiographic atrioventricular delay optimization at 2-6 weeks post-implantation (AHM). The percentage biventricular pacing was assessed by monitoring device counters, and all patients performed a treadmill cardiopulmonary exercise tests to ensure biventricular pacing during exercise i.e., during higher heart rates. AF was monitored during follow-up and when encountered our protocol emphasizes aggressive rhythm or rate control strategy. Rhythm control includes institution of amiodarone and multiple electrical cardioversions if required. When rhythm control was no longer an option, AF was accepted and rate control therapy was instituted aiming for pharmacological strict rate control assessed with exercise testing to confirm continuous biventricular pacing. AVN ablation was only performed when pharmacological rate control therapy did not allow continuous biventricular pacing.
Figure 1. Flow chart.
IntroductionHeart failure and atrial fibrillation (AF) are common cardiovascular conditions and frequently occur together.(1) The prevalence of AF in heart failure varies from 10-15% in New York Heart Association (NYHA) II to 50% in NYHA IV.(2) Cardiac resynchronization therapy (CRT) is an established non-pharmacological therapy in patients with symptomatic heart failure and intraventricular conduction delay, despite optimal medication. It improves symptoms and quality of life and reduces hospitalizations for heart failure and risk of death.(3,4) A prerequisite for optimal benefit of CRT is continuous biventricular pacing. AF may lead to high and irregular ventricular rates, and as a consequence the percentage of biventricular pacing may decrease.(5-10) This has been the main reason for excluding AF in large randomized controlled trials. (3,4) There have been several retrospective cohort studies and substudies of large trials that demonstrate beneficial effects of CRT in patients with either a history of AF or permanent AF, but often atrioventricular node (AVN) ablation was required to ensure continuous biventricular pacing.(3,6,9,11-16) Development of new-onset of AF or recurrences of AF in heart failure patients treated with CRT is also common and is associated with impaired response and cardiovascular outcome.(17-19) We sought to investigate the clinical and prognostic impact of an history of AF, new-onset AF, and AF burden in heart failure patients treated with a CRT.
MethodsPatient population and study protocol Consecutive patients who received a CRT device in the University Medical Center Groningen from January 2001 to December 2012 were identified in this single-center retrospective observational study (Figure 1). Eligibility criteria for CRT implantation were based on the standard guidelines.(3) The presence of sinus rhythm was not a pre-requisite for CRT implantation. Our standard CRT protocol has been described before.(7,17,20) At baseline and 6-month follow-up patient history, physical examination, treadmill cardiopulmonary exercise testing, 12-lead electrocardiogram, and transthoracic echocardiography were performed. All patients were seen according to standard follow-up protocol

112
Atrial Fibrillation in CRT
113
CHAPTER 7
Statistical analysisBaseline descriptive statistics are presented as mean±standard deviation or median (range) for continuous variables and counts with percentages for categorical variables. Differences between patient characteristics were evaluated by the Student-t-test, Mann-Whitney-U test, Chi-square test, and Fisher’s exact test depending on normality and type of the data. To compare data within patient groups, paired Student’s t test was used for normally distributed data and Wilcoxon signed rank test for not normally distributed data. Differences among groups with respect to several outcome measures were evaluated with a chi-squared test for linear trend. The first occurrence of the outcome was assessed by Kaplan-Meier curves. Logistic regression was used to assess the association between co-variates and response. A stepwise approach based on z-score was used to include variates into the final model. All tests of significance were two-tailed, with p-values of <0.05 assumed to indicate significance.
ResultsBaseline characteristicsA total of 491 patients were included in this analysis, 200 (41%) had a history of AF at baseline, 50 (10%) developed new-onset AF during follow-up, and 241 (49%) never had AF (Figure 1, Table 1). Those with ever AF were older. Ischemic heart disease was equally common. Peak VO2 was lower in those with ever AF compared to patients with continuous sinus rhythm. NT-proBNP levels were higher in patients with ever AF (2019 versus 1154 pg/ml, p<0.001). There were no differences between patients with early or late new-onset AF (data not shown). In the first six months AF burden was for most patients either low (<10% AF burden, 42% of AF patients) or high (> 90% AF burden, 41% of AF patients, Figure 2).
Echocardiographic responseTwenty-seven patients (12 patients with AF at baseline) died before response assessment, 17 (63.4%) due to progression of HF, and 10 due to non-cardiovascular causes. Of the remaining 464 patients response was assessed (Table 2). In patients with AF and continuous sinus rhythm, left ventricular end systolic volume and left ventricular end diastolic volume reduced at six
Echocardiographic evaluationTransthoracic echocardiography was performed at baseline and after six months of follow-up. Images were obtained from the parasternal (long- and short-axis) and apical (two- and four chamber) views. Atrial dimensions, ventricular dimensions, septal thickness, and posterior wall thickness were assessed by standard measurements. Left ventricular end-diastolic (LVEDV) and end-systolic volumes (LVESV) were measured with the modified biplane Simpson method using the apical two- and four-chamber views performed by one independent investigator unaware (BAM) of the clinical response of the patient. Left ventricular ejection fraction (LVEF) was calculated from LVEDV and LVESV.
Definitions AF or atrial tachyarrhythmias were defined as any episode lasting at least 30 seconds with an atrial rate > 180 beats per minute as verified by electrocardiogram, Holter recording, or device interrogation. Documented AF before implantation was considered as history of AF. New-onset AF or atrial tachyarrhythmias were defined as atrial tachyarrhythmias occurring during follow-up in patients without a history of AF. AF burden was defined as the time being in AF during follow-up as assessed by device counters. CRT response was defined as a reduction in left ventricular end-systolic volume of 15% or more at six months of follow up. Early new-onset AF was defined as AF occurring within first six months after CRT implantation, late new-onset AF occurred after the first six months. Biventricular pacing was based on device counters. Cardiovascular mortality or heart failure hospitalization during long-term follow-up (beyond six months) was a secondary outcome of the study. Appropriate and inappropriate ICD shocks were also a secondary endpoint. Appropriate shocks were defined as shocks delivered by the ICD to terminate ventricular tachycardia or ventricular fibrillation documented by stored ICD electrograms. Inappropriate ICD shocks were defined as shocks that were not delivered for ventricular arrhythmias (eg, during AF with a high ventricular response) or because of oversensing as a result of lead problems (eg, lead fractures and lead dislocation or T wave oversensing). All shocks were evaluated by experienced electrophysiologists (ICVG and AHM) for appropriateness.

114
Atrial Fibrillation in CRT
115
CHAPTER 7
Table 1. Baseline characteristics of patients with AF (History of or new-onset AF) or sinus rhythm.
Ever AF(n=250)
Continuous Sinus
rhythm(n=241)
P-value
Age – yr – Mean±SD 66.6±10.3 64.4±11.3 0.028Male sex – no. (%) 188 (75.2) 168 (69.7) 0.173Type of atrial fibrillation – no. (%)
Paroxysmal 48 (19.2)Persistent 85 (34.0)Permanent 67 (26.8)New-onset AF 50 (20.0)
Baseline history AF duration – yrs – Median (IQR) 4.6 (1.1-10.1)Atrioventricular node ablation – no. (%) 28 (11.2)Previous myocardial infarction – no. (%) 94 (37.6) 93 (38.6) 0.821Coronary artery disease – no. (%) 118 (47.2) 125 (51.9) 0.301Ischaemic heart disease – no. (%) 119 (47.6) 127 (52.7) 0.259Cardiac surgery (CABG /valve-surgery) – no. (%) 85 (34.0) 56 (23.2) 0.008Hypertension – no. (%) 105 (42.0) 117 (48.5) 0.145Diabetes mellitus – no. (%) 50 (20.0) 50 (20.7) 0.837NYHA class for heart failure – no. (%) 0.106
II 76 (30.4) 87 (36.1)III 158 (63.2) 147 (61.0)IV 16 (6.4) 7 (2.9)
Blood pressure – mmHg – Mean±SDSystolic blood pressure 119±20 116±19 0.098Diastolic blood pressure 72±12 71±11 0.196
Body mass index, kg/m2 ‡ 26.9±4.0 27.1±5.2 0.636Peak VO2, mL/min/kg 14.3±4.9 15.7±4.7 0.008Electrocardiogram
Heart rate, b.p.m. – Mean±SD 76±15 74±15 0.086QRS duration – ms – Mean±SD 159±28 161±22 0.351Left bundle branch block – no. (%) 149 (59.6) 200 (83.0) <0.001Non-Left bundle branch block – no. (%) 41 (16.4) 23 (9.5)Ventricular paced – no. (%) 60 (24.0) 18 (7.5)
Medication – no. (%)Beta-blocker (including sotalol) 209 (83.6) 214 (88.8) 0.096ACEi 189 (75.6) 181 (75.1) 0.898ARB 49 (19.6) 48 (19.9) 0.930Diuretic 218 (87.2) 200 (83.0) 0.190Digoxin 56 (22.4) 21 (8.7) <0.001Amiodaron 54 (21.6) 21 (8.7) <0.001Statin 138 (55.2) 126 (52.3) 0.517Nitrate 34 (13.6) 38 (15.8) 0.497Oral anticoagulation 214 (85.6) 147 (61.0) <0.001Aspirin 54 (21.6) 79 (32.8) 0.005
Echocardiographic parametersLeft atrial size, parasternal – Mean±SD – mm 50±9 45±7 <0.001Left atrial size, length – Mean±SD – mm 69±10 62±9 <0.001Left atrial size, width – Mean±SD – mm 52±8 47±8 <0.001Left atrial volume index – Mean±SD – mL/m2 50±23 (207) 38±13 (212) <0.001Right atrial size, length – Mean±SD – mm 62±10 54±8 <0.001Right atrial size, width – Mean±SD – mm 49±8 43±7 <0.001Septal thickness – Mean±SD – mm 9±2 9±2 0.843Posterior wall thickness – Mean±SD – mm 9±2 9±1 0.555LV end-diastolic volume – Mean±SD – mL 224±93 235±100 0.202LV end-systolic volume – Mean±SD – mL 171±77 179±84 0.256Left ventricular ejection fraction – Mean±SD – % 25±9 24±9 0.157Mitral valve regurgitation, no. (%) 81 (32.4) 54 (22.4) 0.013Tricuspid valve regurgitation, no. (%) 36 (14.4) 15 (6.2) 0.003TAPSE – mm 16.9±4.6 20.4±4.6 <0.001
Laboratory valuesCreatinine – µmol/l - Median (IQR) 119 (88-137) 108 (81-122) 0.001NT-proBNP – pg/ml - Median (IQR) 2019
(900-3607)1154
(461-2640)<0.001
* Plus–minus values are means±SD. SD = Standard deviation; ACEi = angiotensin converting enzyme inhibitor; ARB = Angiotensin receptor blockers; IQR = interquartile range; LV=left ventricuarl; NYHA= New York Heart Association; NT-proBNP = N-terminal prohormone of brain natriuretic peptide, TAPSE = Tricuspid annular plane systolic excursion.‡The body-mass index is the weight in kilograms divided by the square of the height in meters.
months, and left ventricular ejection fraction improved. Response with >15% decrease in LVESV at six months was comparable for patients with AF versus patients with continuous sinus rhythm, p=0.5. In patients with new-onset AF comparable percentages of response were attained. Figure 3 shows the percentages of response amongst several categories of AF and percentage of AVN ablation in each group. Mean biventricular pacing in the first six months between the history of AF, new-onset AF and continuous sinus rhythm were 90±16, 93±15 and 96±11, respectively (P<0.001)
Determinants of echocardiographic responseA larger left ventricular end systolic volume at baseline was associated with a higher response rate whereas a larger left atrial size at baseline and ischemic cardiomyopathy were associated with a lower response rate (Table 4). Neither ever AF, new-onset AF nor AF burden were associated with response.
Outcome After mean follow-up of 1.9±1.0 years, cardiovascular mortality (35 [14.0%] versus 25 [10.4]) and heart failure hospitalizations (18 [7.2%] versus 24 [10.0%]) were comparable between patients with AF and those with continuous sinus rhythm (table 3). New-onset AF in general was not associated with
Figure 2. AF burden during the first six months in 215 patients with AF during follow up.
116
Atrial Fibrillation in CRT
117
CHAPTER 7
Sinus RhythmHistory of AFNew-onset AF
Sinus RhythmLate new-onset AF
Early new-onset AF
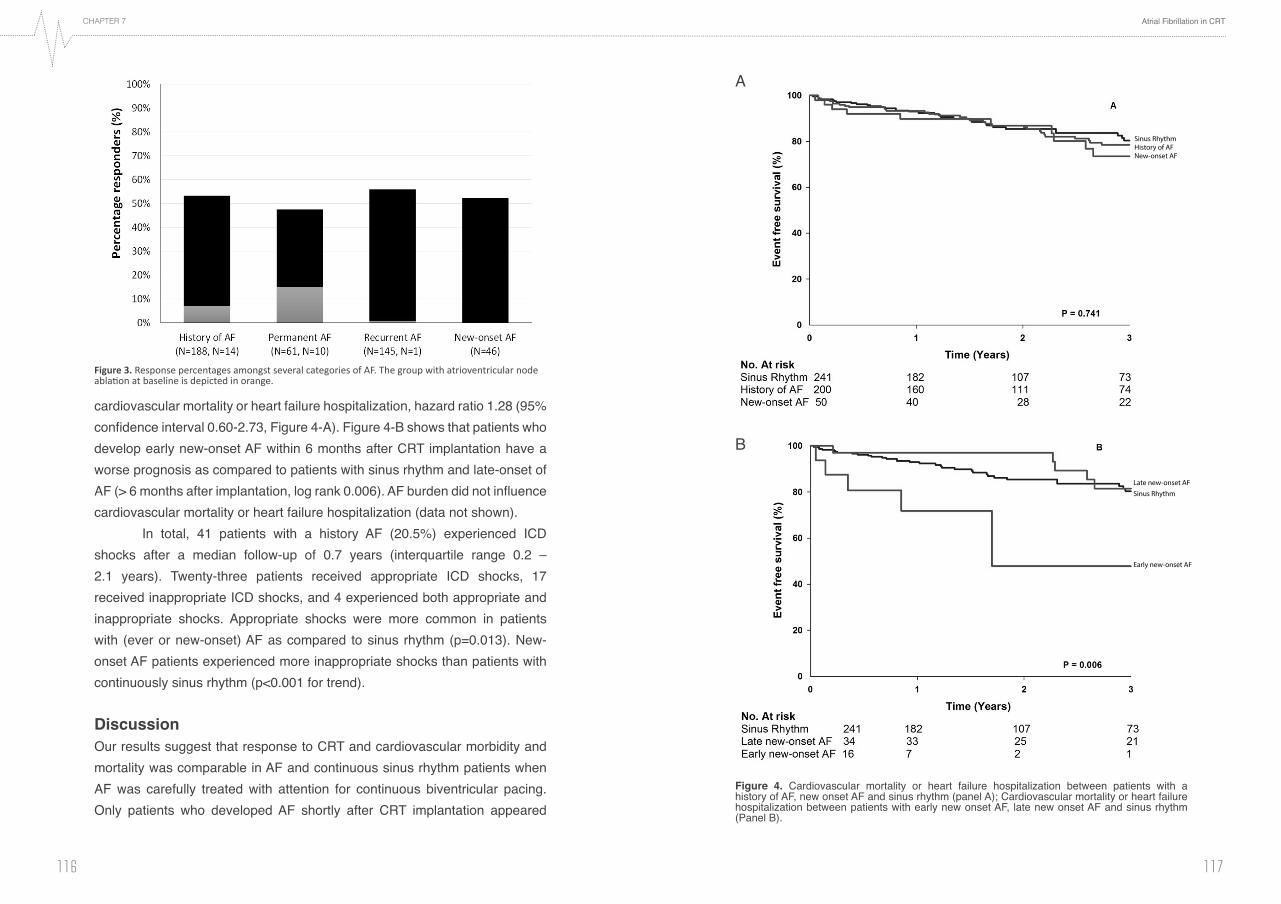
Figure 4. Cardiovascular mortality or heart failure hospitalization between patients with a history of AF, new onset AF and sinus rhythm (panel A); Cardiovascular mortality or heart failure hospitalization between patients with early new onset AF, late new onset AF and sinus rhythm (Panel B).
A
B
cardiovascular mortality or heart failure hospitalization, hazard ratio 1.28 (95% confidence interval 0.60-2.73, Figure 4-A). Figure 4-B shows that patients who develop early new-onset AF within 6 months after CRT implantation have a worse prognosis as compared to patients with sinus rhythm and late-onset of AF (> 6 months after implantation, log rank 0.006). AF burden did not influence cardiovascular mortality or heart failure hospitalization (data not shown). In total, 41 patients with a history AF (20.5%) experienced ICD shocks after a median follow-up of 0.7 years (interquartile range 0.2 – 2.1 years). Twenty-three patients received appropriate ICD shocks, 17 received inappropriate ICD shocks, and 4 experienced both appropriate and inappropriate shocks. Appropriate shocks were more common in patients with (ever or new-onset) AF as compared to sinus rhythm (p=0.013). New-onset AF patients experienced more inappropriate shocks than patients with continuously sinus rhythm (p<0.001 for trend).
Discussion Our results suggest that response to CRT and cardiovascular morbidity and mortality was comparable in AF and continuous sinus rhythm patients when AF was carefully treated with attention for continuous biventricular pacing. Only patients who developed AF shortly after CRT implantation appeared
Figure 3. Response percentages amongst several categories of AF. The group with atrioventricular node ablation at baseline is depicted in orange.

118
Atrial Fibrillation in CRT
119
CHAPTER 7
patients with permanent AF who are otherwise CRT candidates appear to gain minimal benefit from the addition of CRT compared to a standard implantable cardioverter defibrillator therapy.(16) Although no effect on mortality was observed, there was a trend toward less heart failure hospitalizations in the group randomized to CRT.(16) An earlier study in patients with permanent AF compared CRT with right ventricular pacing only.(23) In 37 patients CRT improved exercise tolerance compared to right ventricular pacing.(23) Patients in whom AVN node ablation was performed who were then randomized to either CRT or right ventricular pacing only, showed that CRT was superior in reducing morbidity.(24) The Multicenter Automatic Defibrillator Implantation Trial with Cardiac Resynchronization therapy (MADIT-CRT) substudy, recently showed, however, that the clinical benefit was not attenuated by a history of atrial tachyarrhythmias.(9) The present study supports the use of CRT in patients with AF, with similar response rates compared to current literature when careful attention is paid to continuous biventricular pacing including biventricular pacing assessment with an exercise test.(11,25,26) This was achieved with AVN ablation being only performed when pharmacological rate control therapy did not allow continuous biventricular pacing. Not only response for patients with AF, also long-term all-cause mortality or heart failure hospitalization was comparable.
New-onset atrial fibrillationNew-onset AF is associated with poor outcome.(17-19,27) Development of new-onset or recurrences of AF is common and is associated with impaired response, cardiovascular outcome and appropriate shocks.(7,17,18,28) The present study showed that new-onset AF itself was not associated with
Table 3. Cardiovascular outcomes and ICD shocks. History of AF (n=200)
Continuous Sinus rhythm
(n=241)New-onset AF (n=50)
P-value for
trendMortality – no. (%)
Cardiovascular mortality 25 (12.5) 25 (10.4) 10 (20.0) 0.466All-cause mortality 44 (22.0) 44 (18.3) 16 (32.0) 0.311
Heart failure hospitalization – no. (%) 15 (7.5) 24 (10.0) 3 (6.0) 0.349Shocks – no. (%)
Appropriate 23 (11.5) 15 (6.2) 9 (18.0) 0.053Inappropriate 17 (8.5) 2 (0.8) 4 (8.0) <0.001
AF = Atrial fibrillation; SR = Sinus rhythm.
to have a worse prognosis. Interestingly, inappropriate shocks seldom occur in patients with continuous sinus rhythm.
Atrial fibrillation in cardiac resynchronization therapy trialsAF is the most common arrhythmia in patients with heart failure and increases with severity of heart failure.(1,2) Despite its high prevalence, AF has always been considered an exclusion criterion in large CRT trials.(3,4) The reason for that has always been that AF limits biventricular pacing by loss of atrioventricular synchrony, which may lead to fusion or pseudo-fusion beats and suboptimal biventricular pacing. Whereas landmark trials showed benefit in outcome in terms of cardiovascular morbidity and mortality for patients with sinus rhythm(3,4), only one post-hoc analysis from a randomized trial showed results for patients with permanent AF.(16) The Cardiac Resynchronization in Heart Failure (CARE-HF) showed that CRT improved outcome regardless of whether new-onset AF developed.(16,21) There have been several retrospective cohort studies that demonstrate beneficial effects of CRT in patients with permanent AF, but often AVN ablation was required to ensure continuous biventricular pacing.(3,6,11-15) Whether the latter is applicable to all patients is uncertain as patients with dilated cardiomyopathy appear to benefit the most.(22) The Resynchronization for Ambulatory Heart Failure Trial (RAFT) concluded that in
Table 2. Echocardiographic measurem
ents and response at baseline and 6 months.
History of A
F (n=200)
New
-onset AF
(n=50)C
ontinuous Sinus rhythm
(n=241)P-value for
differences at six m
onths between
groupsB
aseline 6 m
onthsB
aseline6 m
onths B
aseline 6 m
onths LV end diastolic volum
e - Mean±SD
–mL
220±89199±85**
231±112216±88
235±100204±94**
0.507LV end systolic volum
e - Mean±SD
– mL
169±78138±70**
168±73147±73*
179±84143±83**
0.724LV ejection fraction – M
ean±SD – %
25±9
30±11**25±8
31±13*23±9
32±13**0.631
Responder no./total no. (%
)100/188 (53.2%
)24/46 (52.2%
)129/230 (56.1%
)0.548
TAPSE – mm
16.7±4.7
17.7±4.918.7±4.2
19.3±4.020.4±4.6
19.6±4.5*0.001
** P<0.001 for change at six months as com
pared to baseline (within rhythm
group). * p<0.05 for change at six months as com
pared to baseline (within rhythm
group. AF = atrial fibrillation; SR
= sinus rhythm; LV= Left ventricular; SD
= standard deviation; TAPSE = Tricuspid annular plane systolic excursion.

120
Atrial Fibrillation in CRT
121
CHAPTER 7
of AF were included. Furthermore data on AF were carefully collected and documented throughout the study and patients who had new-onset AF were not analyzed as sinus rhythm allowing observing a true sinus rhythm population. Whether or not patients who had early new-onset AF suffered from AF episodes before implantation is unknown. The present study was a retrospective analysis and was therefore not powered to assess outcome (in terms of response or cardiovascular mortality or heart failure hospitalization) in patients with AF comparing to those with sinus rhythm.
ConclusionsResponse and outcome was comparable in patients treated with CRT with either AF or continuous sinus rhythm. Patients with early new-onset AF after implantation appeared to have a worse prognosis. Careful ECG monitoring to adequately treat AF may be beneficial for these patients.
less response or long-term heart failure hospitalization or cardiovascular mortality, in contrast to earlier reports.(17,18,29,30) We showed, however, that the development of new-onset AF occurring shortly after CRT implantation is associated with unfavorable outcome. New-onset AF or recurrent episodes of AF have been shown to negatively impact prognosis not only in terms of heart failure hospitalization or cardiovascular mortality but also in functional status.(8,17,18,28,30,31) Whether or not our new onset AF patients did have AF before implantation remains unknown. However, it seems reasonable to monitor AF carefully during the first few months after implantation to ensure adequate therapy for AF (32,33) and biventricular pacing.(20) Perhaps home monitoring could be a way to ensure early detection and appropriate treatment of AF, also in severe heart failure. Currently, this is investigated in the Clinical effect of heart failure management via home monitoring with a focus on AF (EffecT, NCT00811382).(34) In addition, risk assessment of patients at risk for AF may contribute to improved outcome of CRT therapy.(35)
Strengths and LimitationsStrength of the present analysis is our CRT protocol allowing collecting of patient data treated according to our routine clinical protocol. Follow-up was substantial and a large percentage of patients with a history
Table 4. Determ
inants of echocardiographic response (defined as >15% reduction in left ventricular end systolic volum
e). U
nivariate Analyses
Multivariate A
nalysesO
R (95%
CI)
P valueO
R (95%
CI)
P valueIschem
ic cardiomyopathy
0.68 (0.47-0.99)0.043
0.64 (0.41-0.99)0.045
QR
S duration (per 10msec increase)
1.09 (1.00-1.18)0.047
Beta-blocker1.81 (1.08-3.03)
0.025Left atrial size, length (per 5m
m increase)
0.88 (0.80-0.97)0.010
0.86 (0.77-0.95)0.003
Right atrial size, length (per 5m
m increase)
0.90 (0.82-0.99)0.039
Left ventricular end diastolic volume (per 25m
l increase)1.07 (1.02-1.12)
0.009Left ventricular end systolic volum
e (per 25ml) increase
1.00 (1.00-1.01)<0.001
1.01 (1.00-1.01)<0.001
History of AF
0.91 (0.63-1.33)0.634
New
-onset AF0.90 (0.49-1.66)
0.736AF burden in first six m
onths0.99 (0.99-1.00)
0.600Biventricular pacing in first six m
onths1.01 (0.99-1.03)
0.129O
R = odds ratio; C
I = confidence interval. Multivariate analysis is adjusted for sex and age.

122
Atrial Fibrillation in CRT
123
CHAPTER 7
10. Boriani G, Gasparini M, Landolina M, Lunati M, Proclemer A, Lonardi G, Iacopino S, Rahue W, Biffi M, DiStefano P, Grammatico A, Santini M, ClinicalService cardiac centres. Incidence and clinical relevance of uncontrolled ventricular rate during atrial fibrillation in heart failure patients treated with cardiac resy. Eur J Heart Fail 2011;13:868-876.
11. Wilton SB, Leung AA, Ghali WA, Faris P, Exner DV. Outcomes of cardiac resynchronization therapy in patients with versus those without atrial fibrillation: a systematic review and meta-analysis. Heart Rhythm 2011;8:1088-1094.
12. Gasparini M, Auricchio A, Regoli F, Fantoni C, Kawabata M, Galimberti P, Pini D, Ceriotti C, Gronda E, Klersy C, Fratini S, Klein HH. Four-year efficacy of cardiac resynchronization therapy on exercise tolerance and disease progression: the importance of performing atrioventricular junction ablation in patients with atrial fibrillation. J Am Coll Cardiol 2006;48:734-743.
13. Gasparini M, Auricchio A, Metra M, Regoli F, Fantoni C, Lamp B, Curnis A, Vogt J, Klersy C, Multicentre Longitudinal Observational Study (MILOS) Group. Long-term survival in patients undergoing cardiac resynchronization therapy: the importance of performing atrio-ventricular junction ablation in patients with permanent atrial fibrillation. Eur Heart J 2008;29:1644-1652.
14. European Heart Rhythm Association, European Association for Cardio-Thoracic Surgery, Camm AJ, Kirchhof P, Lip GY, Schotten U, Savelieva I, Ernst S, Van Gelder IC, Al-Attar N, Hindricks G, Prendergast B, Heidbuchel H, Alfieri O, Angelini A, Atar D, Colonna P, De Caterina R, De Sutter J, Goette A, Gorenek B, Heldal M, Hohloser SH, Kolh P, Le Heuzey JY, Ponikowski P, Rutten FH, ESC Committee for Practice Guidelines, Vahanian A, Auricchio A, Bax J, Ceconi C, Dean V, Filippatos G, Funck-Brentano C, Hobbs R, Kearney P, McDonagh T, Popescu BA, Reiner Z, Sechtem U, Sirnes PA, Tendera M, Vardas PE, Widimsky P, Document Reviewers, Vardas PE, Agladze V, Aliot E, Balabanski T, Blomstrom-Lundqvist C, Capucci A, Crijns H, Dahlof B, Folliguet T, Glikson M, Goethals M, Gulba DC, Ho SY, Klautz RJ, Kose S, McMurray J, Perrone Filardi P, Raatikainen P, Salvador MJ, Schalij MJ, Shpektor A, Sousa J, Stepinska J, Uuetoa H, Zamorano JL, Zupan I. Guidelines for the management of atrial fibrillation: the Task Force for the Management of Atrial Fibrillation of the European Society of Cardiology (ESC). Europace 2010;12:1360-1420.
15. Molhoek SG, Bax JJ, Bleeker GB, Boersma E, van Erven L, Steendijk P, van der Wall EE, Schalij MJ. Comparison of response to cardiac resynchronization therapy in patients with sinus rhythm versus chronic atrial fibrillation. Am J Cardiol 2004;94:1506-1509.
16. Healey JS, Hohnloser SH, Exner DV, Birnie DH, Parkash R, Connolly SJ, Krahn AD, Simpson CS, Thibault B, Basta M, Philippon F, Dorian P, Nair GM, Sivakumaran S, Yetisir E, Wells GA, Tang AS, RAFT Investigators. Cardiac resynchronization therapy in patients with permanent atrial fibrillation: results from the Resynchronization for Ambulatory Heart Failure Trial (RAFT). Circ Heart Fail 2012;5:566-570.
17. Buck S, Rienstra M, Maass AH, Nieuwland W, Van Veldhuisen DJ, Van Gelder IC. Cardiac resynchronization therapy in patients with heart failure and atrial fibrillation: importance of new-onset atrial fibrillation and total atrial conduction time. Europace 2008;10:558-565.
18. Borleffs CJ, Ypenburg C, van Bommel RJ, Delgado V, van Erven L, Schalij MJ, Bax JJ. Clinical importance of new-onset atrial fibrillation after cardiac resynchronization therapy. Heart Rhythm 2009;6:305-310.
19. Smit MD, Moes ML, Maass AH, Achekar ID, Van Geel PP, Hillege HL, van Veldhuisen DJ, Van Gelder IC. The importance of whether atrial fibrillation or heart
References
1. Neuberger HR, Mewis C, van Veldhuisen DJ, Schotten U, van Gelder IC, Allessie MA, Bohm M. Management of atrial fibrillation in patients with heart failure. Eur Heart J 2007;28:2568-2577.
2. Anter E, Jessup M, Callans DJ. Atrial fibrillation and heart failure: treatment considerations for a dual epidemic. Circulation 2009;119:2516-2525.
3. McMurray JJ, Adamopoulos S, Anker SD, Auricchio A, Bohm M, Dickstein K, Falk V, Filippatos G, Fonseca C, Gomez-Sanchez MA, Jaarsma T, Kober L, Lip GY, Maggioni AP, Parkhomenko A, Pieske BM, Popescu BA, Ronnevik PK, Rutten FH, Schwitter J, Seferovic P, Stepinska J, Trindade PT, Voors AA, Zannad F, Zeiher A, Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology, Bax JJ, Baumgartner H, Ceconi C, Dean V, Deaton C, Fagard R, Funck-Brentano C, Hasdai D, Hoes A, Kirchhof P, Knuuti J, Kolh P, McDonagh T, Moulin C, Popescu BA, Reiner Z, Sechtem U, Sirnes PA, Tendera M, Torbicki A, Vahanian A, Windecker S, McDonagh T, Sechtem U, Bonet LA, Avraamides P, Ben Lamin HA, Brignole M, Coca A, Cowburn P, Dargie H, Elliott P, Flachskampf FA, Guida GF, Hardman S, Iung B, Merkely B, Mueller C, Nanas JN, Nielsen OW, Orn S, Parissis JT, Ponikowski P, ESC Committee for Practice Guidelines. ESC guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail 2012;14:803-869.
4. Jessup M, Abraham WT, Casey DE, Feldman AM, Francis GS, Ganiats TG, Konstam MA, Mancini DM, Rahko PS, Silver MA, Stevenson LW, Yancy CW. 2009 focused update: ACCF/AHA Guidelines for the Diagnosis and Management of Heart Failure in Adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines: developed in collaboration with the International Society for Heart and Lung Transplantation. Circulation 2009;119:1977-2016.
5. Cheng A, Landman SR, Stadler RW. Reasons for loss of cardiac resynchronization therapy pacing: insights from 32 844 patients. Circ Arrhythm Electrophysiol 2012;5:884-888.
6. Hayes DL, Boehmer JP, Day JD, Gilliam FR,3rd, Heidenreich PA, Seth M, Jones PW, Saxon LA. Cardiac resynchronization therapy and the relationship of percent biventricular pacing to symptoms and survival. Heart Rhythm 2011;8:1469-1475.
7. Smit MD, Maass AH, Hillege HL, Wiesfeld AC, Van Veldhuisen DJ, Van Gelder IC. Prognostic importance of natriuretic peptides and atrial fibrillation in patients receiving cardiac resynchronization therapy. Eur J Heart Fail 2011;13:543-550.
8. Santini M, Gasparini M, Landolina M, Lunati M, Proclemer A, Padeletti L, Catanzariti D, Molon G, Botto GL, La Rocca L, Grammatico A, Boriani G, cardiological centers participating in ClinicalService Project. Device-detected atrial tachyarrhythmias predict adverse outcome in real-world patients with implantable biventricular defibrillators. J Am Coll Cardiol 2011;57:167-172.
9. Ruwald AC, Pietrasik G, Goldenberg I, Kutyifa V, Daubert JP, Ruwald MH, Jons C, McNitt S, Wang P, Zareba W, Moss AJ. The Effect of Intermittent Atrial Tachyarrhythmia on Heart Failure or Death in Cardiac Resynchronization Therapy With Defibrillator Versus Implantable Cardioverter-Defibrillator Patients: A MADIT-CRT Substudy (Multicenter Automatic Defibrillator Implantation Trial With Cardiac Resynchronization Therapy). J Am Coll Cardiol 2014;63:1190-1197.

124
Atrial Fibrillation in CRT
125
CHAPTER 7
pacemakers in heart failure patients. J Cardiovasc Electrophysiol 2008;19:693-701.
32. Healey JS, Connolly SJ, Gold MR, Israel CW, Van Gelder IC, Capucci A, Lau CP, Fain E, Yang S, Bailleul C, Morillo CA, Carlson M, Themeles E, Kaufman ES, Hohnloser SH, ASSERT Investigators. Subclinical atrial fibrillation and the risk of stroke. N Engl J Med 2012;366:120-129.
33. Sanna T, Diener HC, Passman RS, Di Lazzaro V, Bernstein RA, Morillo CA, Rymer MM, Thijs V, Rogers T, Beckers F, Lindborg K, Brachmann J, CRYSTAL AF Investigators. Cryptogenic stroke and underlying atrial fibrillation. N Engl J Med 2014;370:2478-2486.
34. Ricci RP. Disease management: atrial fibrillation and home monitoring. Europace 2013;15 Suppl 1:i35-i39.
35. Kirchhof P, Breithardt G, Aliot E, Al Khatib S, Apostolakis S, Auricchio A, Bailleul C, Bax J, Benninger G, Blomstrom-Lundqvist C, Boersma L, Boriani G, Brandes A, Brown H, Brueckmann M, Calkins H, Casadei B, Clemens A, Crijns H, Derwand R, Dobrev D, Ezekowitz M, Fetsch T, Gerth A, Gillis A, Gulizia M, Hack G, Haegeli L, Hatem S, Georg Hausler K, Heidbuchel H, Hernandez-Brichis J, Jais P, Kappenberger L, Kautzner J, Kim S, Kuck KH, Lane D, Leute A, Lewalter T, Meyer R, Mont L, Moses G, Mueller M, Munzel F, Nabauer M, Nielsen JC, Oeff M, Oto A, Pieske B, Pisters R, Potpara T, Rasmussen L, Ravens U, Reiffel J, Richard-Lordereau I, Schafer H, Schotten U, Stegink W, Stein K, Steinbeck G, Szumowski L, Tavazzi L, Themistoclakis S, Thomitzek K, Van Gelder IC, von Stritzky B, Vincent A, Werring D, Willems S, Lip GY, Camm AJ. Personalized management of atrial fibrillation: Proceedings from the fourth Atrial Fibrillation competence NETwork/European Heart Rhythm Association consensus conference. Europace 2013;15:1540-1556.
failure develops first. Eur J Heart Fail 2012;14:1030-1040. 20. Maass AH, Buck S, Nieuwland W, Brugemann J, van Veldhuisen DJ, Van Gelder IC.
Importance of heart rate during exercise for response to cardiac resynchronization therapy. J Cardiovasc Electrophysiol 2009;20:773-780.
21. Tang AS, Wells GA, Talajic M, Arnold MO, Sheldon R, Connolly S, Hohnloser SH, Nichol G, Birnie DH, Sapp JL, Yee R, Healey JS, Rouleau JL, Resynchronization-Defibrillation for Ambulatory Heart Failure Trial Investigators. Cardiac-resynchronization therapy for mild-to-moderate heart failure. N Engl J Med 2010;363:2385-2395.
22. Sohinki D, Ho J, Srinivasan N, Collins LJ, Obel OA. Outcomes after atrioventricular node ablation and biventricular pacing in patients with refractory atrial fibrillation and heart failure: a comparison between non-ischaemic and ischaemic cardiomyopathy. Europace 2014;16:880-886.
23. Leclercq C, Walker S, Linde C, Clementy J, Marshall AJ, Ritter P, Djiane P, Mabo P, Levy T, Gadler F, Bailleul C, Daubert JC. Comparative effects of permanent biventricular and right-univentricular pacing in heart failure patients with chronic atrial fibrillation. Eur Heart J 2002;23:1780-1787.
24. Brignole M, Botto G, Mont L, Iacopino S, De Marchi G, Oddone D, Luzi M, Tolosana JM, Navazio A, Menozzi C. Cardiac resynchronization therapy in patients undergoing atrioventricular junction ablation for permanent atrial fibrillation: a randomized trial. Eur Heart J 2011;32:2420-2429.
25. Tolosana JM, Arnau AM, Madrid AH, Macias A, Lozano IF, Osca J, Quesada A, Toquero J, Frances RM, Bolao IG, Berruezo A, Sitges M, Alcala MG, Brugada J, Mont L, SPARE II investigators (Spanish Atrial Resynchronization Study II). Cardiac resynchronization therapy in patients with permanent atrial fibrillation. Is it mandatory to ablate the atrioventricular junction to obtain a good response? Eur J Heart Fail 2012;14:635-641.
26. Upadhyay GA, Choudhry NK, Auricchio A, Ruskin J, Singh JP. Cardiac resynchronization in patients with atrial fibrillation: a meta-analysis of prospective cohort studies. J Am Coll Cardiol 2008;52:1239-1246.
27. Rivero-Ayerza M, Scholte Op Reimer W, Lenzen M, Theuns DA, Jordaens L, Komajda M, Follath F, Swedberg K, Cleland JG. New-onset atrial fibrillation is an independent predictor of in-hospital mortality in hospitalized heart failure patients: results of the EuroHeart Failure Survey. Eur Heart J 2008;29:1618-1624.
28. Rienstra M, Smit MD, Nieuwland W, Tan ES, Wiesfeld AC, Anthonio RL, Van den Berg MP, Van Veldhuisen DJ, Van Gelder IC. Persistent atrial fibrillation is associated with appropriate shocks and heart failure in patients with left ventricular dysfunction treated with an implantable cardioverter defibrillator. Am Heart J 2007;153:120-126.
29. Fung JW, Yip GW, Zhang Q, Fang F, Chan JY, Li CM, Wu LW, Chan GC, Chan HC, Yu CM. Improvement of left atrial function is associated with lower incidence of atrial fibrillation and mortality after cardiac resynchronization therapy. Heart Rhythm 2008;5:780-786.
30. Hoppe UC, Casares JM, Eiskjaer H, Hagemann A, Cleland JG, Freemantle N, Erdmann E. Effect of cardiac resynchronization on the incidence of atrial fibrillation in patients with severe heart failure. Circulation 2006;114:18-25.
31. Puglisi A, Gasparini M, Lunati M, Sassara M, Padeletti L, Landolina M, Botto GL, Vincenti A, Bianchi S, Denaro A, Grammatico A, Boriani G, InSync III Italian Registry Investigators. Persistent atrial fibrillation worsens heart rate variability, activity and heart rate, as shown by a continuous monitoring by implantable biventricular