university of groningen lifestyle interventions in
TRANSCRIPT
University of Groningen
Lifestyle interventions in patients with a severe mental illnessLooijmans, Anne
IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite fromit. Please check the document version below.
Document VersionPublisher's PDF, also known as Version of record
Publication date:2018
Link to publication in University of Groningen/UMCG research database
Citation for published version (APA):Looijmans, A. (2018). Lifestyle interventions in patients with a severe mental illness: Addressing self-management and living environment to improve health. Rijksuniversiteit Groningen.
CopyrightOther than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of theauthor(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons).
The publication may also be distributed here under the terms of Article 25fa of the Dutch Copyright Act, indicated by the “Taverne” license.More information can be found on the University of Groningen website: https://www.rug.nl/library/open-access/self-archiving-pure/taverne-amendment.
Take-down policyIf you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediatelyand investigate your claim.
Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons thenumber of authors shown on this cover page is limited to 10 maximum.
Download date: 17-12-2021
Changing the obesogenic environment to improve cardiometabolic health in residential patients with a severe mental illness: cluster randomized controlled trial
Anne Looijmans, Annemarie P.M. Stiekema, Richard Bruggeman, Lisette van der Meer, Ronald P. Stolk, Robert A. Schoevers, Frederike Jörg* & Eva Corpeleijn** Equal contribution as senior authors
The British Journal of Psychiatry, 2017; 211(4)
Chapter 3

42
Chapter 3
ABSTRACT
Background:Forpatientswithseverementalillness(SMI)inresidentialfacilities,adoptingahealthylifestyleishamperedbytheobesitypromoting(obesogenic)environment.
Aims: To determine the effectiveness of a 12-month lifestyle intervention addressingtheobesogenicenvironmentwithrespecttodietandphysicalactivitytoimprovewaistcircumferenceandcardiometabolicriskfactorsversuscare-as-usual(DutchTrialRegistry:NTR2720).
Method: In a multi-site cluster-randomized controlled pragmatic trial, 29 care teamswererandomizedinto15intervention(365patients)and14controlteams(371patients).Interventionstaffweretrainedtoimprovetheobesogenicenvironment.
Results: Waistcircumferencedecreased1.51cm(95%CI=-2.99;-0.04) in interventionversuscontrolgroupafter3monthsandmetabolicsyndromeZ-scoredecreased0.22s.d.(95%CI = -0.38; -0.06). After 12months, the decrease inwaist circumferencewas nolongerstatisticallysignificantlydifferent(-1.28cm;95%CI=-2.79;0.23,p=0.097).
Conclusions:TargetingtheobesogenicenvironmentofresidentialpatientswithSMIhasthepotentialtofacilitatereductionofabdominaladiposityandcardiometabolicrisk,butmaintaininginitialreductionsoverthelongertermremainschallenging.

3
43
ELIPS – somatic outcom
es
INTRODUCTION
Patientswithaseverementalillness(SMI),mostlyschizophrenia,otherpsychoticdisorders,majordepressionorbipolardisorder,havealmost twice thenormal riskofprematuredeathfromcardiovasculardisease1,aremorelikelytosufferfromthemetabolicsyndrome(MS)2,andhaveanup to30years shortened lifeexpectancycompared to thegeneralpopulation3.Theincreasedmortalityriskisassociatedwithsideeffectsofantipsychoticmedicationaswellasunhealthybutmodifiablelifestylebehaviors4. LifestyleinterventionsinSMIpatientshavepreviouslybeenshowntoreducebodyweight5 andwaist circumference, and to improve cardiometabolic risk factors such asserum triglyceride levels, fasting glucose and insulin concentrations6,7. These studiesincludedmostlyoutpatients8,9orfirstepisodepatientswith schizophrenia10,11,whereasstudies in SMI patients admitted to sheltered or clinical care facilities are scarce. Inaddition,sustainabilityofeffectsisquestionable. Mostlifestyleinterventionsaredesignedtostimulateindividualstochangetheirdietandphysicalactivitybehaviorandinvolvecounseling,goalsettingandweightmonitoring.The challenge of these programs is that they highly depend on individual patients’interests,motivationandcapacities,whicharereducedinSMIpatientsduetonegativesymptomsandcognitivedeficits12.Inresidentialfacilities,thesettingisimportantaswellsincefacilitiesareoftencharacterizedbyan‘obesogenic’environmentduetoabundantprovisionofunhealthyfoodproductsandalackofdailyactivities13,14.Theapproachtofocusontheobesogenicenvironment,‘makingthehealthychoicetheeasychoice’byeducatingstaffhowtochangedailypracticewithregardtohealthynutritionandphysicalactivitiesinthefacility,mayleadtosustainablechangesforallresidentialSMIpatients.TwostudiesaddressedtheobesogenicenvironmentofSMIresidentialpatientsbymodifyingthefooddelivery15oradjustingtheofferedfoodcombinedwithnutritionalcounselingandexercisesessions16,andreportedpromisingimprovementsinpatients’somatichealth.However,thesestudieslackedacontrolgroup15orhadasmallsamplesize16.AnotherapproachthatmayworkwellfortheSMIpopulationisthe‘smallchangeapproach’.Thisapproachaimsformodestlifestylechangesleadingtomodest,butsustainableweightlossinthelong-term17. We developed the Effectiveness of Lifestyle Interventions in PSychiatry (ELIPS)trial18.Inthistrial,wedesignedalifestyleinterventiontoimprovecardiometabolichealthof SMIpatients living in residential facilitiesby stimulatingahealthy lifestylevia smallbut sustainable changes in theobesogenicenvironment. TheELIPS trial is apragmaticrandomizedcontrolledtrial(RCT),designedtooffertailored,scalableandimplementableinterventions19.Thismeansthatalready in thetrialphase, the interventionwasaimedat and implemented by regular staff members in daily care. We expected stable orimproved cardiometabolic health in the intervention group compared to deterioratedcardiometabolic health in the control group. In addition, we explored whether theinterventioneffectdependsongender,ageandtypeoffacility.

44
Chapter 3
METHODS
TheELIPSstudyprotocolwaspublished18andwillbeshortlyexplainedbelow.TheMedicalEthical Committee for Research inMental Health Care (Metigg) concluded that studyprotocolanduseofanonymizeddatafromRoutineOutcomeMonitoring(ROM;below)was inaccordancewiththeDeclarationofHelsinkiand(inter)national regulations,andthat the study did not fall under the scope of theMedical Research InvolvingHumanSubjectsAct,therebywaivinginformedconsent.ThetrialwasregisteredintheDutchTrialRegistry(NTR2720,www.trialregister.nl).
Participants and recruitmentSMIpatientsfromallshelteredandlong-termclinicalcareteams(n=29teams,20-65patientsperteam)oftwomentalhealthorganizationsintheNetherlandswereincludedinthestudyfromSeptember2010untilDecember2011iftheyparticipatedintheannualROM(below)(Figure 1). Long-term clinical care facilities deliver direct, all-day intensive professionalcare.Shelteredfacilitiesprovidesupportedliving,acombinationofhousingandservicesinthecommunity.Exclusioncriteriawereagebelow18,pregnancy,Korsakovsyndromeorinabilitytoparticipateintests.Intotal240patientsperarmwereneededtodetectaclinicalrelevantchangeof-5%inwaistcircumference(alpha=0.05,power0.90),takingintoaccountanestimated10%dropoutbasedonthefactthatmeasurementswerepartofroutineoutcomemonitoringscreeningsperformedinawell-establishedinfrastructure.
InterventionThe ELIPS intervention was directed at nursing teams and addressed the obesogenicenvironment of patients; see ELIPS study protocol18 for examples from practice. Theintervention consistedof a preparation, implementationandmonitoringphase. In theone-month preparation phase, lifestyle coaches introduced themselves to staff andpatients, screened the environment and teams’ daily routines, and listed patients’and teams’ preferences and sites’ logistic possibilities. Lifestyle coaches created ateam-tailored lifestyle plan based on listed preferences and possibilities and four pre-establishedELIPSlifestylegoals:(a)tostimulatephysicalactivity;(b)toincreasesupply/availabilityofhealthyfoodproducts;(c)toorganizeatleastoneactivityperweekfocusedonahealthydietand(d)toimprovetheobesogenicenvironmentonorganizationallevel.Inthe3-monthsimplementationphase,lifestylecoachesimplementedtheplannedELIPSlifestyleactivitiesasdescribed intheteam-tailored lifestyleplan.Lifestylecoachesfirstdemonstrated activities to staff, then carriedout the activities togetherwith staffandfinally supervised staff while they carried out the activities. Lifestyle coaches trainedteamstocreateahealthyenvironmentandstimulatehealthybehaviorsinpatients.Attheendoftheimplementationphase,teamssetgoalstoachieveinthe9-monthsmonitoringphase.Inthemonitoringphase,alifestylecoachvisitedallinterventionteamstwiceand

3
45
ELIPS – somatic outcom
es
discussedwiththeteamandteamleaderwhethergoalswereachieved,whichbarriersinachievingthegoalswereencounteredanddiscussedoptionstotacklethesebarriers.Also,theresearchersorganizedonebenchmarkmeetingforallinterventionteamleaderswheredifficultiesinachievingteamgoalswerediscussedandtips,tricksandsuccessfulexampleswereshared.LifestylecoachesweretrainedfortwodaysontheELIPSlifestyleprogram,motivational interviewingtechniquesandonthepatientpopulation.Lifestylecoacheswerefulfillingthefinaloffouryearsofeducationtobecomeprofessionallifestylecoaches. Because lifestyle coaches were still in training, each team had two lifestylecoachesat itsdisposal,whowereappointedby the research team.Perweek, lifestylecoachesspentonaverage8hoursonactivitieswithpatients(6contacthoursandabout2hourpreparationtime)and8hoursontrainingofstaffandorganizationalaspects,likedevelopinginformationmaterials,meetingswithstaff,andprojectmanagement.
30 Teams agreed to
participate 1 Team excluded: exclusively served
patients suffering from Korsakov’s syndrome29 Teams clustered in
13 clusters of 2 or 5 teams
Intervention arm: 15 teams; 400 patients
Control arm: 14 teams; 414 patients
Baseline measures: 400 patients;
vcd for 329 patients
Start intervention: 3-month
implementation phaseCare as usual
3-month follow-up:vcd for 318 patients
3-month follow-up:vcd for 320 patients
Care as usual9-months monitoring phase
12-month follow-up:vcd for 341 patients
12-month follow-up:vcd for 339 patients
1-month preparation phase
Included in analysis: 344 patients with at
least one somaticmeasure
Included in analysis: 320 patients with at
least one somaticmeasure
Included in analysis: 284 patients with at
least one somaticmeasure
Included in analysis: 298 patients with at
least one somaticmeasure
Included in analysis: 326 patients with at
least one somaticmeasure
Included in analysis: 322 patients with at
least one somaticmeasure
In final analysis forprimary outcome:
316 patients
In final analysis forprimary outcome:
320 patients
Randomization per cluster
Baseline measures: 414 patients;
vcd for 352 patients
Legend:vcd = valid care data
Figure 1. FlowchartofpatientsintheELIPStrial.Atotalof736patientshaveatleastonephysicalmeasureatbaselineor12-monthsfollow-upandwereincludedintheanalysis(notretraceableinflowchart).

46
Chapter 3
Patientsinthecontrolconditionreceivedcareasusual.Lifestyleinitiativesincontrolteamsweredocumented.Randomizationwasperformedatteamlevelusingarandomizedblockdesignwith12clustersoftwocomparableteamsandoneclusteroffivecomparableteamsbasedonmentalhealthcareorganization,typeoffacility,caseloadsizeandlocation(urbanorrural).Teamswererandomizedfifty-fiftyintointerventionorcontrolarmwithcomputerizedrandomnumbergeneratorbyanon-participatingresearchnurse.
Measurements and outcomesPrimary outcome was waist circumference (WC) at three and twelve months afterbaseline. Secondary outcomes were Body Mass Index (BMI; kg/m2) and metabolicsyndromeZ-score.Informationonage,gender,diagnosisandmedicationusewasderivedfrompatientrecords.PhysicalhealthdatawerecollectedbytrainednursesinannualROMscreenings,partoftheongoingPHAMOUS(PharmacotherapyOutcomeandMonitoringSurvey) cohort20. AnnualROMscreeningsare standardcare inbothorganizationsandwererescheduledone/twoweeksbeforestartoftheintervention(baselinemeasure)andthreeandtwelvemonthsthereafter(follow-upmeasurements).Patientsreceivedasmallfeefortheadditional3-monthsROMscreening(€5.00/$5.38).ROMnurseswereblindedtointerventionallocation.WCwasmeasuredtwiceinstandingpositionattheendofanexpirationusingaflexiblenon-stretchingtapehalfwaybetweeniliaccrestandlowestrib.Weightwasmeasuredbycalibratedscales(Seca,model813,Hamburg,Germany)inlightclothingwithoutshoesorjackets.Heightwasmeasuredwithoutshoes.Systolicanddiastolicbloodpressure(BP)weremeasuredusinganautomatedbloodpressuremonitor(BOSOmedicuscontrol,Jungingen,Germany)insittingpositionafterfiveminutesrest.Patientsvisiteda(hospital) laboratorytocollectafastingbloodsampleforlevelsof lipids(totalcholesterol,LDL-cholesterol,HDL-cholesterolandtriglycerides)andglucosemetabolism(glucose,HbA1c). Ifnot fasting, thiswas routinely indicatedon the formby thenurse. The metabolic syndrome was defined as the presence of three or more of thefollowingcriteria21:(a)waistcircumference≥88/102cm(female/male);(b)systolicBP≥130and/ordiastolicBP≥85mmHgorreceivingantihypertensivemedication;(c)HDL-C<1.03/1.3mmol/L(female/male;divideby0.0259toconverttomg/dL)orreceivinglipid-loweringmedication;(d)triglycerides≥1.7mmol/L(divideby0.0113toconverttomg/dL)orreceiving lipid-loweringmedication;and(e)fastingglucose≥6.1mmol/L(divideby0.0555 to convert tomg/dL)22, receivingantihyperglycemicmedicationor reportingadiagnosisfordiabetes.Whenfastingglucoselevelswerenotavailable(baseline:46%,n=342; 3-months: 53%, n=392; 12-months: 46%, n=342), patients were considered tofulfilltheglucoseriskcriterioniftheyreportedtohavediabetes(9.6%,n=71)orifHbA1c≥6.0%23.TheindividualcomponentswerestandardizedintoZ-scores(withHDL-cholesterolZ-scoremultipliedby-1)24,25andthesumdividedbyfivewasusedasacontinuousvariablefor the degree ofmetabolic syndrome (MS Z-score). BPwas standardized usingmeanarterialpressure(MAP).
3
47
ELIPS – somatic outcom
es
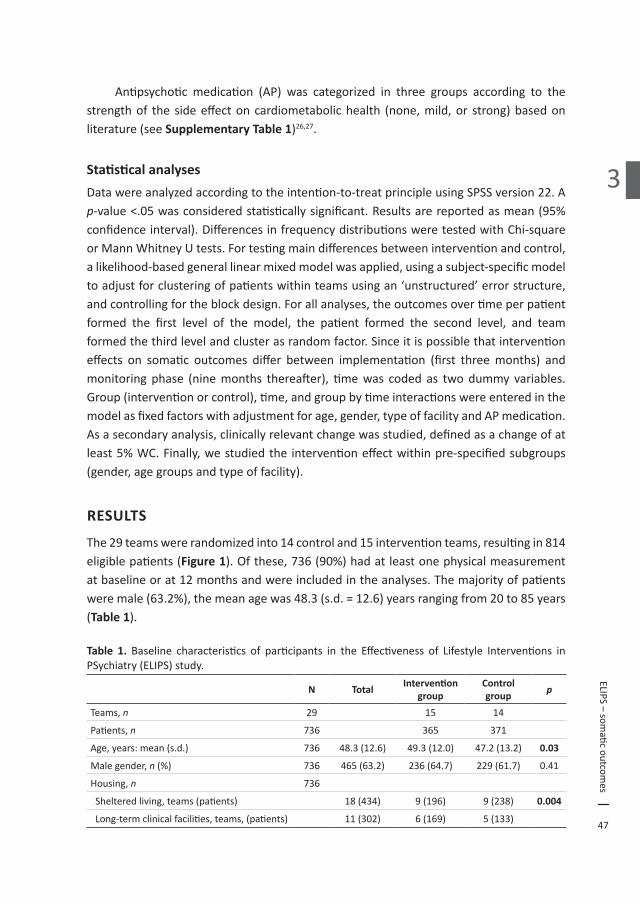
Antipsychotic medication (AP) was categorized in three groups according to thestrengthof the sideeffectoncardiometabolichealth (none,mild,or strong)basedonliterature(seeSupplementary Table 1)26,27.
Statistical analysesDatawereanalyzedaccordingtotheintention-to-treatprincipleusingSPSSversion22.Ap-value<.05wasconsideredstatisticallysignificant.Resultsarereportedasmean(95%confidenceinterval).DifferencesinfrequencydistributionsweretestedwithChi-squareorMannWhitneyUtests.Fortestingmaindifferencesbetweeninterventionandcontrol,alikelihood-basedgenerallinearmixedmodelwasapplied,usingasubject-specificmodeltoadjustforclusteringofpatientswithinteamsusingan‘unstructured’errorstructure,andcontrollingfortheblockdesign.Forallanalyses,theoutcomesovertimeperpatientformed the first level of the model, the patient formed the second level, and teamformedthethirdlevelandclusterasrandomfactor.Sinceitispossiblethatinterventioneffects on somatic outcomes differ between implementation (first threemonths) andmonitoring phase (ninemonths thereafter), timewas coded as twodummy variables.Group(interventionorcontrol),time,andgroupbytimeinteractionswereenteredinthemodelasfixedfactorswithadjustmentforage,gender,typeoffacilityandAPmedication.Asasecondaryanalysis,clinicallyrelevantchangewasstudied,definedasachangeofatleast5%WC.Finally,westudiedthe interventioneffectwithinpre-specifiedsubgroups(gender,agegroupsandtypeoffacility).
RESULTS
The29teamswererandomizedinto14controland15interventionteams,resultingin814eligiblepatients(Figure 1).Ofthese,736(90%)hadatleastonephysicalmeasurementatbaselineorat12monthsandwereincludedintheanalyses.Themajorityofpatientsweremale(63.2%),themeanagewas48.3(s.d.=12.6)yearsrangingfrom20to85years(Table 1).
Table 1. Baseline characteristics of participants in the Effectiveness of Lifestyle Interventions inPSychiatry(ELIPS)study.
N Total Intervention group
Control group p
Teams,n 29 15 14
Patients,n 736 365 371
Age,years:mean(s.d.) 736 48.3(12.6) 49.3(12.0) 47.2(13.2) 0.03
Malegender,n(%) 736 465(63.2) 236(64.7) 229(61.7) 0.41
Housing,n 736
Shelteredliving,teams(patients) 18(434) 9(196) 9(238) 0.004
Long-termclinicalfacilities,teams,(patients) 11(302) 6(169) 5(133)

48
Chapter 3
Table 2. BaselineclinicalcharacteristicsofparticipantsintheEffectivenessofLifestyleInterventionsinPSychiatry(ELIPS)studya.
N Total Intervention group
Control group p
Body composition
Metabolicsyndrome,n(%) 387 226(58.4) 120(58.5) 106(58.2) 0.95
MetabolicsyndromeZ-score,mean(s.d.)b 387 0.45(1.02) 0.48(1.05) 0.42(0.98) 0.59
BodyMassIndex(BMI),kg/m2:mean(s.d.) 616 28.0(6.3) 27.8(6.3) 28.3(6.2) 0.27
BMIcategories,n(%): 0.34
Normal(BMI<25) 210(34.1) 108(36.6) 102(31.8)
Overweight(BMI25-29) 210(34.1) 100(33.9) 110(34.3)
ObeseI(BMI30-34) 117(19.0) 48(16.3) 69(21.5)
ObeseII(BMI35-39) 50(8.1) 27(9.2) 23(7.2)
ObeseIII(BMI≥40) 29(4.7) 12(4.1) 17(5.3)
Waistcircumference,cm:mean(s.d.)
Men 350 104.4(16.1) 105.6(15.4) 103.1(16.8) 0.14
Women 208 103.0(17.0) 104.0(18.7) 102.2(15.5) 0.45
Bloodpressure(BP),mmHG:mean(s.d.) 612
SystolicBP 129.8(18.8) 129.9(19.3) 129.8(18.3) 0.97
DiastolicBP 84.2(12.1) 84.6(12.8) 83.8(11.4) 0.43
UseofBP-loweringmedication,n(%) 646 137(21.2) 79(25.2) 58(17.5) 0.02
Lipids
Totalcholesterol,mmol/L:mean(s.d.) 477 5.19(1.13) 5.10(1.16) 5.29(1.08) 0.07
HDL-cholesterol,mmol/L:mean(s.d.)
Men 293 1.10(0.33) 1.08(0.32) 1.12(0.33) 0.38
Women 182 1.33(0.41) 1.38(0.39) 1.27(0.43) 0.06
LDL-cholesterol,mmol/L:mean(s.d.) 461 3.19(1.01) 3.07(1.02) 3.33(0.98) 0.005
Triglycerides,mmol/L:median(25-75th percentile) 475 1.67(1.12-2.42) 1.65(1.08-2.35) 1.69(1.14-2.50) 0.58
Useoflipidloweringmedication,n(%) 646 114(17.6) 64(20.4) 50(15.1) 0.08
Glucose metabolism
Fastingglucose, mmol/L:median(25-75thpercentile) 394 5.60(5.10-6.40) 5.60(5.20-6.30) 5.60(5.08-6.40) 0.34
HbA1c,%:median(25-75thpercentile) 301 5.60(5.25-6.00) 5.70(5.30-6.00) 5.50(5.10-5.90) 0.003
Useofglucose-loweringmedication,n(%) 646 104(16.1) 51(16.2) 53(16.0) 0.92
Psychiatric characteristics 736
Psychiatricdiagnosis,n(%)
Psychoticdisorder 534(72.6) 277(75.9) 257(69.3) 0.04
Mood disorder 76(10.3) 37(10.1) 39(10.5) 0.87
Personality disorder 238(32.3) 105(28.8) 133(35.8) 0.04
Psychiatriccomorbidity,n(%)c 179(24.3) 79(21.6) 100(27.0) 0.09
3
49
ELIPS – somatic outcom
es
Table 2. BaselineclinicalcharacteristicsofparticipantsintheEffectivenessofLifestyleInterventionsinPSychiatry(ELIPS)studya (continued).
N Total Intervention group
Control group p
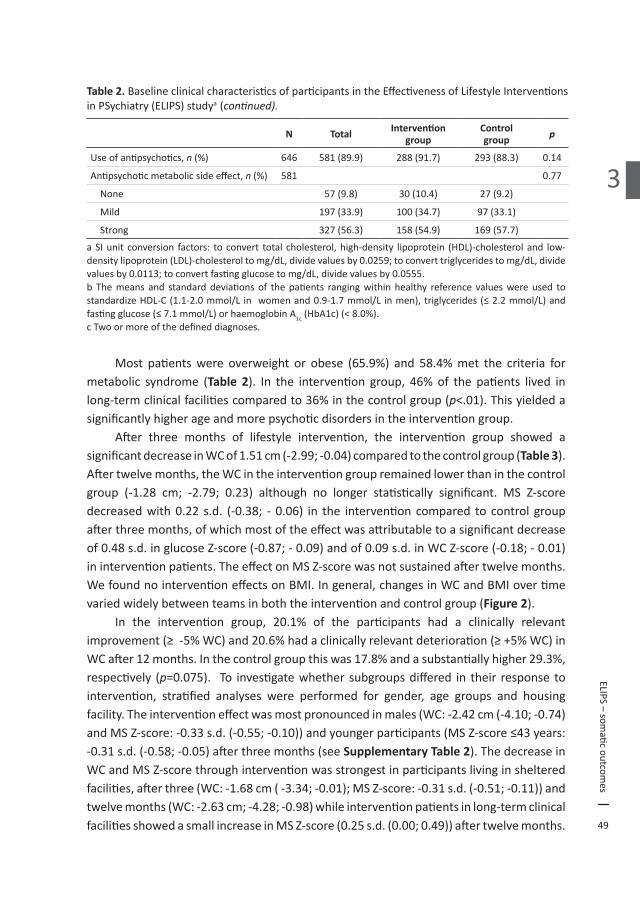
Useofantipsychotics,n(%) 646 581(89.9) 288(91.7) 293(88.3) 0.14
Antipsychoticmetabolicsideeffect,n(%) 581 0.77
None 57(9.8) 30(10.4) 27(9.2)
Mild 197(33.9) 100(34.7) 97(33.1)
Strong 327(56.3) 158(54.9) 169(57.7)
aSIunit conversion factors: to convert total cholesterol,high-density lipoprotein (HDL)-cholesteroland low-densitylipoprotein(LDL)-cholesteroltomg/dL,dividevaluesby0.0259;toconverttriglyceridestomg/dL,dividevaluesby0.0113;toconvertfastingglucosetomg/dL,dividevaluesby0.0555.b Themeans and standarddeviationsof thepatients rangingwithin healthy reference valueswereused tostandardizeHDL-C(1.1-2.0mmol/L in womenand0.9-1.7mmol/L inmen),triglycerides(≤2.2mmol/L)andfastingglucose(≤7.1mmol/L)orhaemoglobinA1c(HbA1c)(<8.0%).cTwoormoreofthedefineddiagnoses.
Most patientswere overweight or obese (65.9%) and 58.4%met the criteria formetabolic syndrome (Table 2). In the intervention group, 46%of the patients lived inlong-termclinicalfacilitiescomparedto36%inthecontrolgroup(p<.01).Thisyieldedasignificantlyhigherageandmorepsychoticdisordersintheinterventiongroup. After three months of lifestyle intervention, the intervention group showed asignificantdecreaseinWCof1.51cm(-2.99;-0.04)comparedtothecontrolgroup(Table 3). Aftertwelvemonths,theWCintheinterventiongroupremainedlowerthaninthecontrolgroup (-1.28 cm; -2.79; 0.23) although no longer statistically significant. MS Z-scoredecreasedwith0.22 s.d. (-0.38; - 0.06) in the interventioncompared to control groupafterthreemonths,ofwhichmostoftheeffectwasattributabletoasignificantdecreaseof0.48s.d.inglucoseZ-score(-0.87;-0.09)andof0.09s.d.inWCZ-score(-0.18;-0.01)ininterventionpatients.TheeffectonMSZ-scorewasnotsustainedaftertwelvemonths.WefoundnointerventioneffectsonBMI.Ingeneral,changesinWCandBMIovertimevariedwidelybetweenteamsinboththeinterventionandcontrolgroup(Figure 2). In the intervention group, 20.1% of the participants had a clinically relevantimprovement(≥-5%WC)and20.6%hadaclinicallyrelevantdeterioration(≥+5%WC)inWCafter12months.Inthecontrolgroupthiswas17.8%andasubstantiallyhigher29.3%,respectively (p=0.075). To investigatewhethersubgroupsdiffered in their response tointervention, stratified analyses were performed for gender, age groups and housingfacility.Theinterventioneffectwasmostpronouncedinmales(WC:-2.42cm(-4.10;-0.74)andMSZ-score:-0.33s.d.(-0.55;-0.10))andyoungerparticipants(MSZ-score≤43years:-0.31s.d.(-0.58;-0.05)afterthreemonths(seeSupplementary Table 2).ThedecreaseinWCandMSZ-scorethroughinterventionwasstrongestinparticipantslivinginshelteredfacilities,afterthree(WC:-1.68cm(-3.34;-0.01);MSZ-score:-0.31s.d.(-0.51;-0.11))andtwelvemonths(WC:-2.63cm;-4.28;-0.98)whileinterventionpatientsinlong-termclinicalfacilitiesshowedasmallincreaseinMSZ-score(0.25s.d.(0.00;0.49))aftertwelvemonths.

50
Chapter 3
Table 3. Somaticoutcomesafter3and12monthsoflifestyleinterventioninin-patientswithseriousmentalillness:resultsofgenerallinearmixedmodelsanalyseswithadjustmentforage,gender,typeoffacilityandantipsychoticsideeffect.
Waist circumference (N=636)
Body mass index (N=654)
Metabolic syndrome Z-score (N=512)
β 95% CI p β 95% CI p β 95% CI p
Intervention effecta
3 monthsb -1.51 (-2.99;-0.04) 0.04 -0.13 (-0.49;0.23) 0.44 -0.22 (-0.38;-0.06) 0.008
12monthsb -1.28 (-2.79;0.23) 0.10 0.34 (-0.12;0.79) 0.14 -0.00 (-0.16;0.16) 0.99
Groupdifference(interventionvscontrol) 0.44 (-2.22;3.09) 0.75 -0.60 (-1.56;0.36) 0.22 -0.04 (-0.22;0.15) 0.70
Time effect only
3 months 1.11 (0.05;2.16) 0.04 0.10 (-0.15;0.36) 0.40 0.13 (0.01;0.26) 0.03
12months 0.75 (-0.31;1.80) 0.17 -0.04 (-0.36;0.29) 0.82 0.01 (-0.10;0.12) 0.89
Age 0.13 (0.02;0.24) 0.02 -0.02 (-0.06;0.02) 0.31 0.00 (-0.00;0.01) 0.51
Male gender 0.44 (-2.15;3.03) 0.74 -2.81 (-3.79;-1.83) .001 0.26 (0.08;0.44) 0.005
Shelteredfacility 0.76 (-4.67;6.18) 0.76 0.31 (-1.13;1.74) 0.67 -0.13 (-0.33;0.08) 0.20
Antipsychotic side effect on metabolism
Mild 1.09 (-2.04;4.22) 0.49 -0.34 (-1.20;0.52) 0.43 0.28 (-0.00;0.56) 0.06
Strong 2.73 (-0.38;5.83) 0.09 -0.05 (-0.91;0.81) 0.91 0.35 (0.07;0.63) 0.01aThecontrolgroupisthereferencegroup.bGroupxtime.
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
-20
-10
0
10
20 Waist change - intervention
Wai
st (c
m)
Team:N = 2 15 17 13 17 10 18 33 25 14 19 4 8 7 7
1 2 3 4 5 6 7 8 9 10 11 12 13 14
-20
-10
0
10
20 Waist change - control
Wai
st (c
m)
Team:N = 13 12 1 9 4 39 13 11 9 50 15 10 14 25
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15-6
-4
-2
0
2
4
6 BMI change - intervention
BM
I (kg
/m²)
Team:N = 2 15 22 14 22 11 19 38 25 16 21 6 10 9 11
1 2 3 4 5 6 7 8 9 10 11 12 13 14-6
-4
-2
0
2
4
6 BMI change - control
BM
I (kg
/m²)
Team:N = 13 13 2 11 8 42 14 14 9 58 15 12 15 27
Figure 2. Heterogeneity between teams inmean changes inwaist circumference andBMI aftertwelvemonths.Meanchangeinwaistcircumference(cm)andBMI(kg/m²)frombaselinetotwelvemonthsafterbaselineperteamwithNpatients.Errorbarsrepresentstandarderrorsofthemean.

3
51
ELIPS – somatic outcom
es
For comparabilitywith lifestyle intervention studies including SMIpatientswith aBMI ≥25kg/m28,weperformedsensitivityanalysesinthissubgroup.Findingsremainthesame:WCwasreducedwith1.79cm(-3.50;-0.08)atthreemonthsandatrendforreducedWCof1.59cm(-3.34;0.16)wasfoundattwelvemonths.MSZ-scoresdecreasedwith0.20s.d.(-0.40;-0.01)afterthreemonths.Again,nointerventioneffectsonBMIwerefound.
DISCUSSION
Main findingsThislarge,multi-site,randomizedcontrolledtrialshowedthatchangingtheobesogenicenvironment of SMI residential patients into a healthier environment significantlyreduced waist circumference and degree of metabolic syndrome after three monthsinterventioncomparedtocareasusual.Themagnitudeoftheseeffectsdecreasedwhen,afterthreemonths,stafftookoverthelifestyleactivities.Thisshowsthatimprovingtheobesogenicenvironmentcanevokebeneficialchangeswithouttargetingpatientsdirectly,butsustainabilityremainsachallenge. An innovative feature of the ELIPS intervention is the focus on the obesogenicenvironment as opposed to directly and solely targeting patients’ dietary and/orsedentarybehaviors13.Moreover,structuralchangesintheenvironmentwillaffecteverypatient,irrespectiveoftheirpersonalinterestinimprovingtheirlifestyles.Changingtheenvironmentusingasmallchangeapproachindeedresultedinasmallimprovement:1.5cminWCoverthreemonths.Ifthiscanbesustainedoveralongerperiodoftime,itwillhoweverleadtoclinicallyrelevantimprovementsinadiposityandtherebyreducingriskof cardiovasculardiseaseanddiabetes28,29. Earlier studies found that foreveryfive cmincreaseinWCtheriskofdeathincreasedwith13%forfemalesand17%formales30.
Comparison to previous studiesTwoearlierRCTsfocusedonresidentialpatients, targetingbothpatientsandstaffwitha 12-month lifestyle intervention with structural guidance of external coaches31,32.Forsbergandcolleaguesdidnotfind improvements inWCorglucose levels31.Thiswashowever a small study (n = 41). Hjorth and colleagues showed a reduction of 3.1 cminWC and stabilized fasting glucose levels versus increased glucose levels in controls,whichiscomparabletoourfindingofreductionsinWCandfastingglucoseZ-score.Theimprovement in glucose metabolism is consistent with studies showing that lifestyleinterventionsareeffectiveatpreventingtype2diabetesinthegeneralpopulation33.Thebeneficial effect on fasting glucose suggests that lifestyle improvements, possibly viaincreasedphysicalactivity,improveinsulinresistance34,35.Changesinphysicalactivitymayresultinchangesinbodycompositionwithreducedfatnessandincreasedmusclemass32,whichmayexplainthesignificanteffectsonWCbutnotBMI(Figure 2).Ameta-analysisoflifestyleinterventionsforSMIin-andoutpatientsconfirmedourresultsonWC(Cohen’s

52
Chapter 3
d =-0.37;95%CI=-0.60;-0.13)andfastingglucose(Cohen’sd =-0.24;95%CI=-0.32;-0.10)6. Studiesusing individualand/orgroupcounseling sessions, forexampleDaumitandcolleagues8andMcKibbinetal36,foundasignificantdecreaseof2.0to3.7cminWCaftersixmonthsofexercise,weightmanagementorpsycho-educationalsessions.Thus,alifestyleinterventioninSMIresidentialpatientsfocusingontheobesogenicenvironmentmayyieldcomparableresultsasinterventionstargetingpatientsdirectlywithindividualorgroupcounseling.
Possible factors influencing intervention implementation and sustainabilityChangesinwaistcircumferencevariedwidelybetweenteams(Figure 2).Thisismostlikelyrelatedtotheeasewithwhichteams implementedandsustainednew lifestylehabits.Structuralaspectsplayedarole,likeenvironmentalfeaturesofthefacility(e.g.physicalactivityopportunitiesinurbanvsruralsetting37),availablebudget(e.g.forhealthyfoodproducts) and availability of staff members (e.g. nurses being scheduled to organizeactivities).Furthermore, logisticchanges(e.g.alteringthetypeofbreadofferedduringlunch)werepossiblymoreeasilyimplementedthanculturalchanges(e.g.offeringwalk-and-talk therapy38insteadofsittinginthecounselingoffice).Perhapsofmoreinfluencewereattitudesofstaff:nursesdifferedintheirexperienceofconflictingpriorities(e.g.ahighworkload),conflictswithroledefinitions(e.g.nursesarenotdieticiansorphysicaltherapists)andconflictswithownhealthbehaviors (e.g.givingagoodexamplebynotorderingpizzaduringnightshifts)39,40. Thepragmaticcharacterof theELIPS trialallowedthe interventiontobe tailoredtotheresourcesofthefacility.Moreover,regularstaffimplementedtheinterventionineverydaypracticeafterthreemonthsoflifestylecoaching,givingaclearindicationofwhatisattainablein‘real-world’settings.Thedesignofthestudy,consistingofanimplementationand amonitoring (support) phase, demonstrated the difficulty of sustaining achievedimprovements.Despite involvementofregularstaffinorganizing lifestyleactivitiesandembeddinglifestyleactivitiesinteams’workingroutine,themagnitudeofeffectsachievedatthreemonthsdecreasedintheninemonthsthereafter,whenstaffmemberswerelessfrequentlyguidedbylifestylecoaches.Thisisinlinewithfindingsfromameta-analysisof lifestyle interventionsbyBradshawet.al.40andthestudyofDaumitandcolleagues8 whereinitialsignificanteffectsonWCwerenolongersignificantwhenthefrequencyofsessionsdecreasedandtrainedstaffmemberstookovermostoftheactivitiesoflifestylecoaches.So,improvementsinWCandglucoselevelsarewithinreach,butsustainabilitymightbeachievedonlywhenstaffmembersareguidedonaregularbasisbyalifestylecoachwhoseprimaryresponsibilityistopromotethepatients’lifestyle.Thefrequencyoftheseguidingcontactsneededtosustainormaximizeresultsinthelong-term,shouldbeexplored,butlikelyneedstoexceedtwovisitsinninemonths. TheELIPSinterventionseemedtobeespeciallybeneficialformalesandpatientslivinginshelteredfacilities.Perhapsthelifestyleactivities,possiblythephysicalactivities,were

3
53
ELIPS – somatic outcom
es
moreappealingtomalethanfemaleparticipants.Staffinlong-termclinicalcarefacilitiesmighthaveexperiencedmoreobstaclesinchangingroutines,anticipatingdysregulationofthemostseverelyillpatients.However,theseresultsneedtobeinterpretedwithcautionassubanalysesinevitablycontainedfewerpatientsthanneededaccordingtothepowercalculation,whichwasbasedonthecomparisonofinterventionandcontrolgrouponly.
Strengths and limitationsStrengthsandlimitationsofthestudyarerelatedtothepragmaticcharacteroftheRCT.Thecontrolconditionwaslesscontrolledthanitwouldhavebeeninanexplanatorytrial19.Despitebeinginthecontrolcondition,staffmembersorpatientsmayhavetakeninitiativeto work on a more healthy lifestyle, following the trend in society. The interventionconditionwouldhavedifferedlessbetweenfacilitiesifwehadnotusedateamtailoredlifestyleplan.Usinganimplementationapproachhoweverlargelyincreasestheexternalvalidityofthestudyresults.Ourinclusionstrategyfurtherincreasedtheexternalvaliditybyavoidingselectionbiasofparticipatingpatients19.
IMPLICATIONS
A small change approach focusing on the obesogenic environment of patients livingin shelteredor long-termcare facilitieshas thepotential toproduceclinically relevantreductions in adiposity and thereby reduce cardiometabolic risk. However, our smallresultsindicatethatchangingtheobesogenicenvironmentaloneisnotenough.Itshouldbeconsideredaprerequisiteforimprovingpatients’health13andbepartofanintegratedapproachofmultiple targets, including sensiblepharmaceutical strategies.Anext stepwouldbe todevelopascalable (nursing-)programformaintenanceofhealthychangesandinitiativesinthefacilities,thatiseffective,affordableandsustainableinthelongterm.

54
Chapter 3
REFERENCES1. Laursen TM,Wahlbeck K, Hällgren J, et al. Life expectancy and death by diseases of the
circulatorysysteminpatientswithbipolardisorderorschizophreniaintheNordiccountries.PLoS One.2013;8(6):1-7.
2. ZimmetP,AlbertiG,ShawJ.AnewIDFworldwidedefinitionofthemetabolicsyndrome:Therationaleandtheresults.Diabetes Voice.2005;50(3):31.
3. HertM,CorrellCU,Bobes J,etal.Physical illness inpatientswithseverementaldisorders.I. prevalence, impact of medications and disparities in health care. World Psychiatry.2011;10(1):52-77.
4. McEvoyJP,MeyerJM,GoffDC,etal.Prevalenceofthemetabolicsyndromeinpatientswithschizophrenia:Baselineresultsfromtheclinicalantipsychotictrialsofinterventioneffectiveness(CATIE)schizophreniatrialandcomparisonwithnationalestimatesfromNHANESIII.Schizophr Res.2005;80(1):19-32.
5. McGinty EE, Baller J, Azrin ST, Juliano-BultD,DaumitGL. Interventions to addressmedicalconditions and health-risk behaviors among persons with serious mental illness: Acomprehensivereview.Schizophr Bull.2016;42(1):96-124.
6. Bruins J, Jörg F, BruggemanR, SlooffC, Corpeleijn E, PijnenborgM. Theeffects of lifestyleinterventions on (long-term) weight management, cardiometabolic risk and depressivesymptomsinpeoplewithpsychoticdisorders:Ameta-analysis.PloS one.2014;9(12):e112276.
7. CabassaL,Ezell J, Lewis-FernándezR.Lifestyle interventions foradultswithseriousmentalillness:Asystematicliteraturereview.Psychiatric Services.2010;61(8):774-782.
8. DaumitGL,DickersonFB,WangN,etal.Abehavioralweight-lossinterventioninpersonswithseriousmentalillness.N Engl J Med.2013;368(17):1594-1602.
9. BrarJS,GanguliR,PandinaG,TurkozI,BerryS,MahmoudR.Effectsofbehavioraltherapyonweightlossinoverweightandobesepatientswithschizophreniaorschizoaffectivedisorder.J Clin Psychiatry.2005;66(2):205-212.
10. Alvarez-JiménezM,Gonzalez-BlanchC,Vazquez-BarqueroJL,etal.Attenuationofantipsychotic-inducedweightgainwithearlybehavioral interventionindrug-naivefirst-episodepsychosispatients:Arandomizedcontrolledtrial.J Clin Psychiatry.2006;67(8):1253-1260.
11. WuR,ZhaoJ,JinH,etal.Lifestyleinterventionandmetforminfortreatmentofantipsychotic-inducedweightgain:Arandomizedcontrolledtrial.JAMA.2008;299(2):185-193.
12. Hassapidou M, Papadimitriou K, Athanasiadou N, et al. Changes in body weight, bodycompositionandcardiovascularriskfactorsafterlong-termnutritionalinterventioninpatientswithseverementalillness:Anobservationalstudy.BMC Psychiatry.2011;11(1):1.
13. Swinburn B, Egger G, Raza F. Dissecting obesogenic environments: The development andapplication of a framework for identifying and prioritizing environmental interventions forobesity.Prev Med.1999;29(6):563-570.
14. FaulknerG, Cohn TA. Pharmacologic and nonpharmacologic strategies forweight gain andmetabolicdisturbanceinpatientstreatedwithantipsychoticmedications.Canadian Journal of Psychiatry.2006;51:502-511.
15. CohnT,GrantS,FaulknerGE.Schizophreniaandobesity:Addressingobesogenicenvironmentsinmentalhealthsettings.Schizophr Res.2010;121(1):277-278.
16. MelamedY, Stein-ReisnerO,GelkopfM, et al.Multi-modalweight control intervention forpeoplewithpersistentmentaldisorders.Psychiatr Rehabil J.2008;31(3):194-200.

3
55
ELIPS – somatic outcom
es
17. Sbrocco T, Nedegaard RC, Stone JM, Lewis EL. Behavioral choice treatment promotescontinuingweightloss:Preliminaryresultsofacognitive–behavioraldecision-basedtreatmentforobesity.J Consult Clin Psychol.1999;67(2):260.
18. Looijmans A, Jörg F, Schoevers RA, Bruggeman R, Stolk RP, Corpeleijn E. Changing theobesogenicenvironmentofseverementallyillresidentialpatients:ELIPS,aclusterrandomisedstudydesign.BMC Psychiatry.2014;14(1):293.
19. Treweek S, ZwarensteinM.Making trialsmatter: Pragmatic and explanatory trials and theproblemofapplicability.Trials.2009;10(37):9.
20. BruinsJ,PijnenborgMG,Bartels-VelthuisAA,etal.Cannabisuseinpeoplewithseverementalillness:Theassociationwithphysicalandmentalhealth-acohortstudy.Apharmacotherapymonitoringandoutcomesurveystudy.J Psychopharmacol.2016;30(4):354-362.
21. Grundy SM, Cleeman JI, Daniels SR, et al. Diagnosis and management of the metabolicsyndrome:Anamericanheartassociation/nationalheart,lung,andbloodinstitutescientificstatement.Circulation.2005;112(17):2735-2752.
22. ForouhiN,BalkauB,Borch-JohnsenK, et al. The threshold fordiagnosing impaired fastingglucose:ApositionstatementbytheEuropeandiabetesepidemiologygroup.Diabetologia.2006;49(5):822-827.
23. InternationalExpertCommittee.InternationalexpertcommitteereportontheroleoftheA1Cassayinthediagnosisofdiabetes.Diabetes Care.2009;32(7):1327-1334.
24. EisenmannJC.Ontheuseofacontinuousmetabolicsyndromescore inpediatricresearch.Cardiovascular diabetology.2008;7(1):1.
25. BakkerSJ,GansevoortRT,deZeeuwD.Metabolicsyndrome:A fatamorgana?Nephrol Dial Transplant.2007;22(1):15-20.
26. (Dutch) National Health Care Institute (Zorginstituut Nederland). Farmacotherapeutischkompas. http://www.farmacotherapeutischkompas.nl/inleidendeteksten/i/inl%20antipsycho tica.asp.AccessedJune23,2015.
27. UpToDate (Marder,S.&Stroup,T.S.).Selectedadverseeffectsofantipsychoticmedicationsfor schizophrenia. http://www.uptodate.com/contents/image?imageKey=PSYCH%2F82533 &topicKey=PSYCH%2F15766&source=see_link&utdPopup=true. Updated 2015. AccessedJune23,2015.
28. FarinHM,AbbasiF,ReavenGM.Comparisonofbodymassindexversuswaistcircumferencewiththemetabolicchangesthatincreasetheriskofcardiovasculardiseaseininsulin-resistantindividuals.Am J Cardiol.2006;98(8):1053-1056.
29. FoxKA,DespresJP,RichardAJ,BretteS,DeanfieldJE,IDEASteeringCommitteeandNationalCo-ordinators. Does abdominal obesity have a similar impact on cardiovascular diseaseanddiabetes?A studyof91,246ambulantpatients in27European countries.Eur Heart J.2009;30(24):3055-3063.
30. PischonT,BoeingH,HoffmannK,etal.GeneralandabdominaladiposityandriskofdeathinEurope.N Engl J Med.2008;359(20):2105-2120.
31. Forsberg KA, Björkman T, Sandman PO, SandlundM. Physical health-a cluster randomizedcontrolled lifestyle intervention amongpersonswith a psychiatric disability and their staff.Nordic Journal of Psychiatry.2008;62(6):486-495.
32. HjorthP,DavidsenAS,KilianR,etal. Improvingthephysicalhealthof long-termpsychiatricinpatients.Aust N Z J Psychiatry.2014;48(9):861-870.
33. Roumen C, Blaak EE, Corpeleijn E. Lifestyle intervention for prevention of diabetes:Determinantsofsuccessforfutureimplementation.Nutr Rev.2009;67(3):132-146.

56
Chapter 3
34. GoodyearP,LaurieJ,KahnM,BarbaraB.Exercise,glucosetransport,andinsulinsensitivity.Annu Rev Med.1998;49(1):235-261.
35. CorpeleijnE,SarisW,BlaakE.Metabolicflexibilityinthedevelopmentofinsulinresistanceandtype2diabetes:Effectsoflifestyle.Obesity reviews.2009;10(2):178-193.
36. McKibbinCL,PattersonTL,NormanG,etal.A lifestyle interventionforolderschizophreniapatientswithdiabetesmellitus:Arandomizedcontrolledtrial.Schizophr Res.2006;86(1):36-44.
37. KaczynskiAT,HendersonKA.Environmentalcorrelatesofphysicalactivity:Areviewofevidenceaboutparksandrecreation.Leisure Sciences.2007;29(4):315-354.
38. DoucettePA.Walkandtalk:Aninterventionforbehaviorallychallengedyouths.Adolescence.2004;39(154):373.
39. LeanM,LeaveyG,KillaspyH,etal.BarrierstothesustainabilityofaninterventiondesignedtoimprovepatientengagementwithinNHSmentalhealthrehabilitationunits:Aqualitativestudynestedwithinarandomisedcontrolledtrial.BMC Psychiatry.2015;15(1):209.
40. BradshawT,WeardenA,MarshallM,etal.Developingahealthylivinginterventionforpeoplewithearlypsychosisusingthemedicalresearchcouncil’sguidelinesoncomplexinterventions:Phase1oftheHELPER–InterACTprogramme.Int J Nurs Stud.2012;49(4):398-406.

3
57
ELIPS – somatic outcom
es
SUPPLEMENTARY MATERIALS
Supplementary Table 1. Categorizationofantipsychoticmedicationaccording to the strengthofthesideeffect(none,mildorstrong)oncardiometabolichealth. CategorizingisbasedontheDutchFarmacotherapeuticalCompass(FC),websiteUptoDate(UtD)andtheexpertopinion(EP)ofthreepsychiatrists.
Antipsychotic medication Source
No cardiometabolic influence
Aripiprazole FC
Haloperidol FC
Bromperidol EP
Flupenthixol FC
Pimozide FC
Sulpiride FC
Tiapride EP
Penfluridol EP
Fluphenazine UtD
Mild cardiometabolic influence
Risperidone FC
Quetiapine FC
Chlorprothixene EP
Levomepromazine EP
Paliperidone UtD
Periciazine EP
Pipamperon EP
Zuclopenthixol EP
Fluspirilene EP
Strong cardiometabolic influence
Clozapine FC
Olanzapine FC
Note: FC = (Dutch) National Health Care Institute (ZorginstituutNederland). Farmacotherapeutisch kompas.http://www.farmacotherapeutischkompas.nl/inleidendeteksten/i/inl%20antipsychotica.asp.Retrieved23 June2015; UtD = Selected adverse effects of antipsychotic medications for schizophrenia (www.uptodate.com).Retrieved3Augustus2015;EP=expertopinion.

58
Chapter 3
Supp
lem
enta
ry T
able
2. W
aistcirc
umferencean
dmetab
olicsy
ndromeZ-scoreaft
er3and
12mon
thsoflifestyleinterven
tioninSMIinp
atien
tsstrati
fied
forg
ende
r,type
offacilityand
agegroup
s.Resultsoflinea
rmixed
mod
elsa
nalysesw
ithadjustm
entforage,gen
der,type
offacilityand
anti
psycho
ticside
eff
ectifn
otstratifi
edfo
rthisfactor.
WA
IST
CIRC
UM
FERE
NCE
Gen
der
Type
of f
acili
ty
Men
(N=3
98)
Wom
en(N
=238
)Sh
elte
red
faci
lities
(N
=369
)Lo
ng-t
erm
clin
ical
car
e fa
ciliti
es
(N=2
67)
β95
% C
Ip
β95
% C
Ip
β95
% C
Ip
β95
% C
Ip
Interven
tioneff
ecta
3 m
onth
sb-2.42
(-4.10;-0
.74)
0.00
5-0.11
(-2.82;2.59)
0.94
-1.68
(-3.34;-0
.01)
0.05
-0.47
(-3.28;2.34)
0.74
12mon
thsb
-1.61
(-3.29;0.07)
0.06
-0.47
(-3.41;2.46)
0.75
-2.63
(-4.28;-0
.98)
0.00
21.14
(-1.78;4.06)
0.44
Grou
pdiffe
rence
(interven
tion
vscon
trol)
0.20
(-3.01;3.42)
0.90
1.96
(-2.63;6.54)
0.40
3.59
(0.41;6.78)
0.03
-4.36
(-8.91;0.18)
0.06
Timeeff
ecto
nly
3 m
onth
s1.17
(-0.04;2.39)
0.06
1.12
(-0.77;3.01)
0.24
1.74
(0.63;2.86)
0.00
2-0.07
(-2.23;2.10)
0.95
12mon
ths
0.56
(-0.64;1.75)
0.36
1.11
(-0.89;3.11)
0.27
1.45
(0.32;2.58)
0.01
-0.68
(-2.80;1.44)
0.53
Age
grou
ps
≤ 43
Yea
rs(N
=220
)44
–55
Year
s(N
=224
)≥
56 Y
ears
(N=1
92)
β95
% C
Ip
β95
% C
Ip
β95
% C
Ip
Interven
tioneff
ecta
at 3
mon
thsb
-1.53
(-3.93;0.88)
0.21
-2.38
(-5.00;0.24)
0.07
-0.38
(-3.13;2.37)
0.79
at1
2mon
thsb
-0.99
(-3.40;1.42)
0.42
-2.37
(-4.95;0.20)
0.07
-0.47
(-3.45;2.52)
0.76
Grou
pdiffe
rence
(interven
tion
vscon
trol)
1.35
(-3.10;5.81)
0.55
2.59
(-1.96;7.14)
0.26
-2.41
(-7.28;2.45)
0.33
Timeeff
ecto
nly
3 m
onth
s1.52
(-0.10;3.14)
0.07
1.36
(-0.59;3.31)
0.17
0.14
(-1.85;2.12)
0.89
12mon
ths
1.29
(-0.32;2.89)
0.12
1.39
(-0.48;3.25)
0.14
-0.72
(-2.82;1.37)
0.50

3
59
ELIPS – somatic outcom
es
Supp
lem
enta
ry T
able
2. W
aistcirc
umferencean
dmetab
olicsy
ndromeZ-scoreaft
er3and
12mon
thsoflifestyleinterven
tioninSMIinp
atien
tsstratifi
ed
forg
ende
r,type
offacilityand
agegroup
s.Resultsoflinea
rmixed
mod
elsa
nalysesw
ithadjustm
entforage,gen
der,type
offacilityand
anti
psycho
ticside
ifno
tstrati
fiedforthisfactor(
conti
nued
).
MET
ABO
LIC
SYN
DRO
ME
Z-SC
ORE
Gen
der
Type
of f
acili
ty
Men
(N=3
19)
Wom
en(N
=193
)Sh
elte
red
faci
lities
(N
=298
)Lo
ng-t
erm
clin
ical
car
e fa
ciliti
es
(N=2
14)
β95
% C
Ip
β95
% C
Ip
β95
% C
Ip
β95
% C
Ip
Interven
tioneff
ecta
3 m
onth
sb-0.33
(-0.55;-0
.10)
0.00
4-0.07
(-0.31;0.17)
0.58
-0.31
(-0.51;-0
.11)
0.00
2-0.14
(-0.42;0.14)
0.32
12mon
thsb
-0.10
(-0.31;0.11)
0.37
0.17
(-0.05;0.39)
0.14
-0.17
(-0.37;0.04)
0.11
0.25
(0.00;0.49)
<0.0
5
Grou
pdiffe
rence
(interven
tion
vscon
trol)
0.08
(-0.17;0.34)
0.53
-0.20
(-0.48;0.08)
0.16
0.24
(0.02;0.47)
0.04
-0.45
(-0.76;-0
.13)
0.00
5
Timeeff
ecto
nly
3 m
onth
s0.17
(-0.00;0.35)
0.06
0.08
(-0.10;0.25)
0.39
0.17
(0.03;0.32)
0.02
0.11
(-0.12;0.34)
0.34
12mon
ths
0.03
(-0.13;0.19)
0.73
-0.02
(-0.18;0.13)
0.78
0.16
(0.01;0.31)
0.04
-0.21
(-0.40;0.03)
0.03
Age
grou
ps
≤ 43
Yea
rs(N
=168
)44
–55
Year
s(N
=186
)≥
56 Y
ears
(N=1
58)
β95
% C
Ip
β95
% C
Ip
β95
% C
Ip
Interven
tioneff
ecta
3 m
onth
sb-0.31
(-0.58;-0
.05)
0.02
-0.06
(-0.31;0.19)
0.64
-0.26
(-0.59;0.07)
0.12
12mon
thsb
-0.16
(-0.43;0.12)
0.26
0.12
(-0.10;0.34)
0.29
0.07
(-0.25;0.40)
0.65
Grou
pdiffe
rence
(interven
tion
vscon
trol)
0.02
(-0.33;0.38)
0.91
-0.13
(-0.42;0.17)
0.40
-0.03
(-0.38;0.31)
0.84
Timeeff
ecto
nly
3 m
onth
s0.21
(0.02;0.39)
0.03
0.02
(-0.18;0.22)
0.84
0.13
(-0.12;0.39)
0.29
12mon
ths
0.18
(-0.01;0.38)
0.06
-0.05
(-0.22;0.12)
0.56
-0.14
(-0.38;0.11)
0.27
a The
con
trolgroup
isth
ereferencegrou
p.b G
roup
xtime.
