university of groningen different aspects of hyperthermic
TRANSCRIPT

University of Groningen
Different aspects of hyperthermic isolated limb perfusionGinkel, Robert Johannes van
IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite fromit. Please check the document version below.
Document VersionPublisher's PDF, also known as Version of record
Publication date:2002
Link to publication in University of Groningen/UMCG research database
Citation for published version (APA):Ginkel, R. J. V. (2002). Different aspects of hyperthermic isolated limb perfusion. s.n.
CopyrightOther than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of theauthor(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons).
The publication may also be distributed here under the terms of Article 25fa of the Dutch Copyright Act, indicated by the “Taverne” license.More information can be found on the University of Groningen website: https://www.rug.nl/library/open-access/self-archiving-pure/taverne-amendment.
Take-down policyIf you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediatelyand investigate your claim.
Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons thenumber of authors shown on this cover page is limited to 10 maximum.
Download date: 19-12-2021

DIFFERENT ASPECTS OF HYPERTHERMIC
ISOLATED LIMB PERFUSION

This research was financially supported by the Dutch Cancer Society (Nederlandse
Kankerbestrijding KWF) grant GUKC 90-06.
ISBN: 90-367-1716-7
Page lay out: P. van der Sijde, Groningen, The Netherlands
Printed by: Ponsen en Looijen BV, Wageningen, The Netherlands

RIJKSUNIVERSITEIT GRONINGEN
DIFFERENT ASPECTS OF HYPERTHERMIC ISOLATED LIMB
PERFUSION
Proefschrift
ter verkrijging van het doctoraat in de
Medische Wetenschappen
aan de Rijksuniversiteit Groningen
op gezag van de
Rector Magnificus, dr. F. Zwarts,
in het openbaar te verdedigen op
woensdag 20 november 2002
om 16.00 uur
door
Robert Johannes van Ginkel
geboren op 12 mei 1964
te Amsterdam
.

Promotores Prof. dr. H.J. Hoekstra
Prof. dr. H. Schraffordt Koops
Prof. dr. W. Vaalburg
Beoordelingscommissie Prof. dr. B.B.R. Kroon
Prof. dr. M.F. von Meyenfeldt
Prof. dr. W.M. Molenaar

Voor opa Hans
Paranimfen Drs. D.J. Klees
Drs. R.P. Winkel


Contents
Chapter 1 General introduction and aim of the thesis 9
Chapter 2 Hyperthermic isolated limb perfusion with cisplatin in the localtreatment of spontaneous canine osteosarcoma:Assessment of short term effectsJournal of Surgical Oncology 1995; 59: 169-176. 29
Chapter 3 Hyperthermic isolated limb perfusion with TNF and cisplatinin the treatment of osteosarcoma of the extremities:A feasibility study in healthy dogsSarcoma 1999; 3: 89-94. 45
Chapter 4 Hyperthermic isolated limb perfusion with cisplatin in fourpatients with sarcomas of soft tissue and boneEuropean Journal of Surgical Oncology 1996; 22: 528-531 57
Chapter 5 Isolated limb perfusion of an irradiated foot with TNF,interferon and melphalanArchives of Surgery 1996; 131: 672-674. 67
Chapter 6 FDG-PET to evaluate response to hyperthermic isolated limbperfusion for locally advanced soft-tissue sarcomaJournal of Nuclear Medicine 1996; 37: 984-990. 77
Chapter 7 [1-11C]-Tyrosine PET to evaluate response to hyperthermicisolated limb perfusion for locally advanced soft-tissuesarcoma & skin cancerJournal of Nuclear Medicine 1999; 40: 262-267. 93
Chapter 8 Value of Continuous Leakage Monitoring with RadioactiveIodine-131 Labeled Human Serum Albumin DuringHyperthermic Isolated Limb Perfusion with TNFand MelphalanAnnals of Surgical Oncology 2002; 9: 355-363. 107
Chapter 9 Summary and conclusionsSamenvatting en conclusies 125
Dankwoord 140
Curriculum vitae 142
Publications 143


9
General introduction and aim of the thesis

10
Chapter 1
Before Tumor Necrosis Factor
The first report of the beneficial effect of intravenously administered nitrogen-mustard
on tumor growth appeared just after the second world war.1 Soon afterwards reports
were published on the advantageous effect of intra-arterially administered nitrogen-
mustard on malignant tumors.2-4 Using technology to support extracorporeal
circulation developed for cardiac surgery in the 1950s, the surgical oncologists Creech,
Krementz, Ryan and Winblad of the Tulane University in New Orleans developed
the technique of isolated limb perfusion (ILP).5 In this procedure the blood circulation
of a tumor bearing limb is isolated from the circulation of the rest of the body by
clamping the major artery and vein and tightening a tourniquet around the root of the
limb. The major artery and vein are subsequently connected to a heart-lung machine
and the cytotoxic drug is administered through this isolated circuit. Key point in ILP
is that the dose of chemotherapeutics used, can be 15-20 fold the maximum systemic
tolerated dose, since vital organs are isolated from the perfusion circuit.6-8
The original patient population treated with ILP was a subgroup of melanoma patients
who had extensive local recurrence in the arm or leg. The initial drug used for ILP to
treat extremity melanoma was melphalan (L-phenylalanine mustard). Melphalan is
an alkylating agent of the bischloroethylamine type comprising nitrogen mustard
and phenylalanine. Phenylanaline is a metabolite of melanin and therefore melphalan
specifically targets melanocytes and melanoma cells. Its cytotoxicity appears to be
related to the extent of its interstrand cross-linking with DNA. Like other bifunctional
alkylating agents, it is effective against both resting and rapidly dividing tumor cells.
In 1959 Creech, Krementz and Ryan described their initial results of patients treated
with regional perfusion. The first patient was a 76 year old male with multiple
melanoma satellites on his upper leg. After regional perfusion with melphalan the
satellites disappeared completely and the patient died at the age of 92 with no local
recurrence. The case history of this patient was frequently illustrated at lectures and
a poster with pictures of this patient decorated the entrance of the surgical ward of
the Tulane University for many years. Cavaliere and co-workers investigated the
addition of hyperthermia in the treatment of cancer and, as this appeared to augment
the anti-tumor effects of melphalan, in doing so they laid the basis for hyperthermic
isolated limp perfusion (HILP).9 At temperatures of 41.5 degrees C and higher a
direct anti-tumor effect was observed however, this was accompanied with
unacceptable local toxicity.10 To avert this increased local toxicity it was established
that mild hyperthermia with temperatures of 39 to 40 degrees C was best used.
Wieberdink introduced the optimal dose calculations of melphalan based on limb
volume instead of patient weight, since the latter may lead to under- or overtreatment
of an individual dependent on body habitus.11 An essential component of HILP is

11
Introduction
monitoring the perfusion leakage to the systemic circulation and being able to make
adjustments during treatment to reduce this leakage. Different methods to measure
leakage are used. Stehlin and associates were the first to describe a method of
continuous external leakage monitoring with radioactive Iodine-131 labeled human
serum albumin (RISA).12 This is still the method most frequently used nowadays. It
places a gamma counter over the precordium with RISA in the perfusion circuit,
which allows continuous readings and estimations of the leak of the perfusion solution
into the systemic circulation.13
From 1969 until recently, ILP with hyperthermia and melphalan was the gold standard
for regional treatment of in-transit melanoma. The response rates to this therapeutic
HILP are considerably higher to any other systemic therapy for this type of tumor.
Objective response rates have been reported as high as 70% to 100%, with complete
response rates between 54% and 65%. The median duration of responses is
approximately 9 months, and some patients experience a long-term disease control
with this regional therapy.14,15
Many publications on HILP for melanoma combine adjuvant perfusions with
therapeutic perfusions, often with different treatment schedules, making the
interpretation of available data very difficult. A publication on the 35-year experience
with HILP of the Tulane Hospital serves as a good example for this problem. Over
1100 cases were reported with a median follow-up longer than 10 years. However,
an evidence based conclusion about the benefit of the procedure could not be made.16
A prospective randomized German study published in the 1980s reported a significant
improvement in survival after adjuvant HILP.17 However, the numbers of patients
treated were small, and the outcome in the control group was much worse than
expected compared to historical controls, which meant that this trial could not be
used in arguing for adjuvant HILP.18 The value of HILP as an adjuvant treatment
modality in patients with high risk stage I disease (more than 1.5 mm Breslow
thickness), was recently evaluated in a prospective randomized trial by the European
Organization for Research on Treatment of Cancer (EORTC).19 This study showed
no overall survival benefit for patients treated with HILP with melphalan followed
by local excision compared to patients that had undergone local excision only.
However, a slight benefit in disease free survival was seen in the perfusion group.
With the publication of this study as a negative trial, no adjuvant HILP should be
performed after resection of primary melanoma. Another patient population that may
benefit from a adjuvant HILP are those who have developed in-transit metastases
that have been excisionally biopsied. These patients are at a much greater risk for
additional recurrences in the limb than patients with high-risk primary cutaneous
melanoma who have not had a regional recurrence. A small prospective study from

12
Chapter 1
Sweden found a significant improvement in tumor free survival in the perfusion
group, however no overall survival benefit was demonstrated.20 In conclusion, adjuvant
HILP with melphalan should not be used for high-risk primary melanoma and should
only be used as an adjuvant in the setting of a clinical trial with patients with in-
transit metastases.
Other chemotherapeutic agents used in HILP for melanoma have shown much lower
subjective response rates often with a higher toxicity. Cisplatin as one of the most
successful alternatives with a 50% to 60% response rate showed a high frequency of
peripheral neuropathy.21-23 The most successful systemic treatment agent for melanoma
is DTIC but used in regional perfusion this agent leads to a complete response rate of
11% and a partial response of only 26%.24
Although HILP was most frequently used in the treatment of extremity melanoma,
the procedure was also applied to soft tissue sarcomas (STS) of the extremity.
Krementz described their initial results in 113 patients. Fifty-four patients treated
with HILP without surgical excision of the tumor showed an early response rate of
83%, however only four patients had a complete regression of the tumor.25 Several
studies were published on the treatment of STS with HILP and melphalan, these
studies also have the problem of being heterogeneous as to the type of STS, disease
stage and therapy performed, making comparison difficult. The local recurrence rates
range from 0% to 25% with a 5-year survival rate of 56% to 69%.26-31 Other perfusion
agents have been investigated in the treatment of STS with HILP. Klaase et al.
described the use of doxorubicin as the sole perfusion agent but this was ineffective.
The complete remissions observed in four patients occurred after perfusion with
doxorubicin combined with melphalan. Local toxicity was high, and tissue necrosis
necessitated amputation in three cases.32 However in a study of Rossi et al, tumor
necrosis was more than 50% in 17 patients (74%) and limb-sparing surgery was
feasible in 20 patients (91%). They concluded that HILP with doxorubicin is an
active and well-tolerated procedure within a multidisciplinary approach of the
treatment of limb sarcomas.33 Pommier and Di Filippo investigated cisplatin as a
perfusion agent in the treatment of STS. 34,35 Seventeen patients whose sarcomas
were measured prior to HILP, none of the patients showed a complete response,
three had a partial response (18%), five had a minimal response (29%), seven had no
change (41%), and two had progression (12%).34 In conclusion, results with HILP
for STS were not impressive and alternative strategies for limb preservation by intra-
venous and intra-arterial adriamycin with preoperative or postoperative radiation
therapy followed by compartmental excisions, were able to provide adequate local
control for most extremity STS.36-39

13
Introduction
Introducing Tumor Necrosis Factor
William Coley, a surgeon who lived and worked in New York City during the second
half of the 19th century, was the first to investigate the phenomenon of tumor necrosis,
occurring in patients suffering from severe infections. By administering preparations
of gram-positive and gram-negative bacteria or their products to patients with
inoperable neoplastic diseases, Coley hoped to bring about an involution of the tumor.
The side effects of Coley’s regimen were unacceptable, however, and his treatment
ultimately fell into disrepute.40,41 Shear and co-workers, seeking to isolate an active
therapeutic fraction from Coley’s toxins, purified what they called the “bacterial
polysaccharide” from Serratia marcescens organisms.42-44 This molecule, now known
as lipopolysaccharide (LPS), was shown to induce hemorrhagic necrosis of
transplantable tumors in mice.45 A major conceptual advance occurred with the work
of O’Malley, et al., who reported that an endogenous factor appeared in the serum of
animals treated with LPS, which could induce hemorrhagic necrosis of tumors grown
in animals that had not been exposed to LPS. This information, though published in
a prominent journal, was largely overlooked for over 20 years.46 The transferability
of tumor-necrotizing activity from one animal to another was then identified by Old
and co-workers, who showed that a factor produced in mice pretreated with Bacillus
Calmette-Guérin (BCG) and subsequently challenged with LPS was capable of
causing hemorrhagic necrosis of the meth A sarcoma, grown in the skin of a recipient
animal.47 The factor was dubbed “tumor necrosis factor” (TNF). A large number of
studies reveal that TNF is produced principally by macrophages.48-51 A long period of
time elapsed between the identification of TNF and its isolation in pure form. TNF
from a human source was first isolated by Aggarwal and colleagues at Genentec.52
The molecular cloning of the TNF DNA was accomplished almost simultaneously
by a number of workers at separate biotechnology firms and the cloning of the human
TNF locus followed soon afterwards.53-56
A lot of articles published both in scientific literature and in popular press claimed,
that this molecule would prove to be a revolutionary tool in the battle against cancer.
However, phase I and II clinical trials of systemic TNF were very disappointing. An
overall response rate of 1-2% was seen in almost 1000 patients treated with systemic
TNF.57-60 The dose-limiting toxicity of TNF was typical hypotension, clearly
delineating the central role of this cytokine as a mediator of the pathophysiology of
septic shock.61-64 This dose-limiting toxicity in patients kept the peak intravascular
level achievable in humans 100-fold lower than the level needed for an anti-tumor
effect in a mouse model.65,66
Because it seemed impossible to achieve effective systemic concentrations of TNF
in patients, and because it appeared to act very rapidly with a short, single treatment

14
Chapter 1
in animal models, TNF was ideally suited for use in HILP. Ferdy Lejeune and Danielle
Lienard, surgical oncologists working in Brussels at the time, were the first to link
high-dose TNF and HILP to treat 19 patients with cutaneous melanoma and 4 patients
with STS in the early 1990s.67 In this setting, the equivalent intravascular levels that
led to responses in mice (1-3 µg/ml) could be achieved in the perfusion circuit.68 In a
pilot study of 3 patients with TNF as the sole perfusion agent, one complete response
of 7 months, one partial response of 21 days, and one minor response lasting for
1 month were observed. Posner described these 3 patients and another 3, treated with
HILP and TNF as the sole perfusion agent. One patient had a complete response,
2 patients had a partial response of less than 1 month’s duration and no response was
seen in 3 patients. HILP with TNF as the sole perfusion agent showed inadequate
activity. Three of these 6 patients had been reperfused with TNF and melphalan
resulting in 2 complete responses and 1 partial response.69 In vitro and vivo studies
had already shown an enhanced cytotoxic activity of TNF when chemotherapeutic
drugs, especially alkylating agents were added.70,71 The treatment regimen conceived
by Lejeune was a combination of preoperative subcutaneous interferon-gamma (IFN)
and perfusion with low-dose IFN, high-dose TNF and melphalan for a 90-minute
treatment period. The IFN was added to the regimen because it synergized with TNF
in pre-clinical studies.72,73 In all 23 cases, an early and spectacular softening of the
tumors was seen within the first 3 days after treatment, consistent with the TNF
effect seen in the murine models. Sixteen of 19 patients with melanoma (84%) and 3
out of 4 patients with a STS (75%) showed a complete response. Three melanoma
(16%) and 1 STS (25%) showed a partial response.67,74
Based on the initial study, two prospective randomized trials were initiated. In Europe,
Lejeune and colleagues started a prospective randomized phase II study of patients
with advanced melanoma of the limbs with in-transit metastasis. They compared 32
patients who received melphalan plus TNF and IFN to 32 patients who received
melphalan plus TNF only. The overall response rate and the complete response rate
were higher for the patients treated with IFN compared to the ones treated with
melphalan TNF only, 100% vs. 91% and 78% vs. 69% respectively, but the differences
were not significant.75 In the United States a trial comparing melphalan alone to the
identical dose of melphalan combined with TNF and IFN was initiated by Fraker in
patients with in-transit melanoma of the extremity with no known disease outside
the extremity. At an interim analysis of this study the complete response rate for
melphalan, TNF and IFN perfusion arm was 80% and 61% for the melphalan alone
perfusion arm. In a subgroup of patients with a high tumor burden of the extremity,
the melphalan, TNF and IFN perfusion arm had a much more dramatic effect (67%
complete responses) than what could be achieved by melphalan alone (17% complete

15
Introduction
responses). Patients with low tumor burden or small tumors showed equivalent results
with both of these two perfusion regimens, 87% complete responses with TNF versus
81% with melphalan only.76 The complete response rate seen with melphalan alone
in this study is somewhat better than that reported by other investigators and in order
to draw conclusions about the value of TNF as an adjunct to HILP in melanoma
patients, more patients need to be included.
When the benefit of TNF with melphalan in HILP for bulky melanoma was observed,
the same regimen was applied to STS.67 The results were much more positive in this
combination compared to melphalan alone, and several series have been published
demonstrating limb preservation in patients deemed to have unresectable tumors
with amputation as the only surgical option.77-79 The overall approach with large
extremity sarcomas that have no local resection options because of their relationship
to neurovascular and bony structures, is to conduct HILP with TNF and melphalan.
This treatment results in significant tumor shrinkage in 6 to 12 weeks. A second
procedure is performed after this period to resect the remaining tumor that is often
reduced in size. Patients with multifocal sarcoma do not undergo the secondary
resection, similar to those patients suffering from in-transit melanoma. The European
trial of 186 patients showed complete responses in 18% and partial responses in 57%
of the cases measuring tumor size.77 HILP with TNF and melphalan was also feasible
in patients with locally advanced extremity STS with disseminated disease as local
control improved the quality of life.80 These studies on bulky extremity sarcomas
demonstrated that TNF acts by attacking the tumor vasculature with rapid elimination
of tumor blood flow within days after treatment.81 Other more unusual tumors of the
extremity such as Merkel cell carcinoma, which often spreads by in-transit metastases
within the limb, as well as eccrine adenocarcinoma and basal and squamous cell skin
carcinoma have been reported to respond to HILP with melphalan plus TNF.82 Again,
because this treatment acts via an apparent antiangiogenic mechanism, it may be
applicable against all solid malignancies, with the tumor endothelium as the target
tissue, which is similar across several histologies.
Toxicity of HILP
Toxicity of HILP can be categorized as a side effect from systemic exposure to the
drugs and as a side effect due to the regional effects of high-dose exposure. The
systemic exposure depends not only on the adequacy of the isolation during HILP,
but is also caused by systemic exposure to the perfused drug during reperfusion.
Although the limb is flushed after perfusion, residual active agents still remain in the
limb either within the intravascular space or in the interstitial fluid, which results in
a systemic peak of drug concentration following the re-establishment of normal
16
Chapter 1
vascular flow to the extremity. Systemic leakage of melphalan has been described
and consisted of nausea and vomiting (22%), bone marrow depression in 4% and
miscellaneous systemic side-effects, including fever and minimal scalp hair loss,
occurring in 19 patients (5%).83 With the introduction of high-dose TNF at levels 10
times the maximum tolerated systemic intravenous bolus, isolation was all the more
important, but it introduced also another path to systemic toxicity namely the induction
of secondary host mediators during HILP that are subsequently released into the
systemic circulation after the perfusion. For standard chemotherapeutics, there is
little or no induction of host mediators.84 The systemic effects of TNF HILP reflect
the reported toxicity present in phase 1 systemic TNF trials. The most serious
complication is hypotension. In the first report by Lienard, 23% (7/31) of the patients
treated experienced hypotension, and 10% (3/31) showed severe hypotension.74 All
patients in this initial trial received dopamine (3 mg/kg/min) at the time of TNF
injection into the perfusate as a prophylaxis against hypotension. The most significant
toxicity of TNF limb perfusions can be summarized as a so called Systemic
Inflammatory Response Syndrome (SIRS). This was observed in all patients and
was accompanied by fever, rise in cardiac output, fall in systemic vascular resistance
and the need for fluid resuscitation and inotropes. Perfusion with melphalan as the
sole perfusion agent did not trigger these effects. Detailed analysis showed positive
correlations between maximum TNF concentrations and systemic vascular resistance
and cardiac index.85 The National Cancer Institute perfusion group demonstrated the
relation between the vascular response and the need for vasopressor support and
systemic TNF levels in patients with TNF leakage as well.86 Lejeune also demonstrated
severe toxicity in patients with leaks of >5%.67,68 Vrouwenraets et al. reported an
absence of severe systemic toxicity of TNF in patients without systemic leakage.87
Stam et al. observed only a mild postoperative toxicity in the event of significant
leakage during perfusion.88 This was easily managed on the ICU with fluid substitution
and, in some cases, with vasopressors. All these systemical side effects of TNF HILP
were minimal, transient, and could easily be managed with appropriate resuscitative
techniques.89,90
The normal tissues in the limb that are perfused such as skin, muscle, peripheral
nerves, blood vessels, bone, cartilage, and synovium comprising the skeletal system,
are also exposed to the same concentrations of anti-neoplastic agents active against
the tumor. Wieberdink developed a grading system to score these regional toxicities.11
The toxicities seen with melphalan are skin erythema, some with areas of blistering
and subcutaneous edema, in virtually all patients.91,92 The skin changes as well as this
edema universally returns to normal after several months. The most important
toxicities are the effects on muscle and peripheral nerves. Myopathy can occur with

17
Introduction
mild muscle discomfort and in the worst case may cause a compartment syndrome
with potential muscle necrosis and subsequent limb loss. This is the main reason
why a prophylactic fasciotomy is performed after HILP at the University Hospital in
Groningen.93 Long term analysis of limb function after fasciotomy showed no impaired
function of the perfused limb compared to the contralateral none perfused limb. 94This
was in contrast with other reports claiming approximately 5% to 10% of the patients
have significant long-term discomfort in their extremity after HILP, a difference that
can be possibly explained by the prophylactic fasciotomy. Initial reports from Lienard
et al. indicate that TNF and IFN add little to the regional toxicity of limb perfusions
compared to melphalan alone. Skin erythema and desquamation, edema, joint stiffness,
and peripheral neuropathy appear to occur in the same number of patients as after
melphalan alone perfusions.
Positron Emission Tomography
Positron Emission Tomography (PET) is a non invasive, diagnostic imaging technique
for measuring the metabolic activity of cells in the human body with the aid of short-
lived positron emitting radiopharmaceuticals. Traditional diagnostic techniques, such
as x-rays, CT scans or MRI, produce images of the body’s anatomy or structure.
The first step in a PET-study is to label a selected compound with a positron emitting
radionuclide. Starting from non-radioactive atoms, a cyclotron is used to produce
radionuclides. In a cyclotron, particles such as protons or deuterons (hydrogen and
deuterium atoms without their orbital electrons) are brought to high energies by
traversing several hundred orbits within the cyclotron. When the protons or deuterons
orbits near the maximum radius of the cyclotron, they are removed through
electrostatic or magnetic deflection and are impinged upon small volume hollow
metallic cylinders filled with a nonradioactive gas or liquid. Nuclear reactions take
place within the cylinder (target) between the high energy particle (proton or deuteron)
and the contents of the target. With different target materials, different radioactive
products can be obtained. These are then separated from the target material and can
be used in the synthesis of more complex radiopharmaceuticals. The most frequently
applied radionuclides in PET are carbon-11 (11C, half-life 20 minutes), nitrogen-13
(13N half-life 10 minutes), oxygen-15 (15O half-life 2 minutes) and fluorine-18 (18F
half-life 110 minutes).
The production of the radiopharmaceutical is performed with the use of automated
synthesis systems. These are located within lead-walled (5-6 cm thick) cabinets so
called “hot cells”. The precise composition of the radiopharmaceutical is assured by
testing the products with e.g. high pressure liquid chromatography before
administrating them to the patient. Sterility and pyrogen testing are performed on

18
Chapter 1
every dose afterwards.
The radionuclides now incorporated within the radiopharmaceutical, have a surplus
of positive nuclear particles. Because this is an unstable situation, these radionuclides
either capture an electron or emit a positron (which is a particle with the same weight
as an electron, but with a positive charge) to achieve stability, depending on the
energy of the nucleus. After a positron is emitted, it is rapidly slowed down by
interactions within the surrounding tissue until all its kinetic energy (velocity) is
lost. At this point, the positron combines momentarily with an electron. The
combination of particles (positron and electron) then totally annihilates or disintegrates
and results in two diametrically (1800 apart) photons of exactly 511 keV energy. The
pairs of photons are emitted equally from the body in all directions. In general, several
million events (photon pairs) are accumulated for each PET image.
The next step in PET is to detect the emitted photons with the PET camera. The PET
camera used for this study at the University of Groningen contains 8192 crystals
oriented into 16 rings arranged in two rings of 64 detector blocks each 512 detectors
per ring. The 16 rings are used to collect 16 planes (slices) of data and an additional
15 cross-planes (slices) are obtained by collecting photon interactions between
adjacent direct planes for a total of 31 planes. The scanner has a 10.4 cm axial field
of view. Patients are positioned comfortably on a table which moves through the
opening of the scanner. Some patients require only one field of view (10 cm) to
visualize a particular area of the body while others are moved through the scanner
using 9-10 bed positions (90-100 cm) to complete whole body imaging. PET cameras
make use of the fact that the two annihilation quanta have opposite directions. Emitted
photons can be absorbed by the detectors in the camera. Each detector has connections
with many opposite detectors. A signal is said to be caused by annihilation if the
capture of a photon by two opposite detectors coincides within 20 nsec. Simultaneous
detection of two of these photons by detectors on opposite sides of an object places
the site of the annihilation or on about a line connecting the centers of the two detectors.
At this point mapping the distribution of annihilations in the field of view by a
computer is possible and an image can be reconstructed. If the annihilation originates
outside the volume between the two detectors, only one of the photons can be detected,
and since the detection of a single photon does not satisfy the coincidence condition,
the event is rejected. The image achieved is generally presented as a gray scale image
of a cross-section of the patient, with the intensity of each picture element proportional
to the isotope concentration at that point in the patient.
Fluorine-18 labeled 2-fluoro-2-deoxy-D-glucose (FDG) is one of the most widely
used radiopharmaceuticals used in PET and has proven to be of value in the
visualization of various types of tumors.95,96 The use of FDG is based on Warburg´s

19
Introduction
observation of increased glycolysis in cancer cells. The citric acid cycle, which is
more efficient in adenosine triphosphate generation, is suppressed.97 As a result, cancer
cells accumulate the glucose analog FDG which is trapped intracellularly as FDG
phosphate. The FDG consumption, and since FDG acts in the same way as glucose,
the glucose consumption can be determined with the use of a three-compartment
model: plasma-FDG, tissue-FDG and tissue-FDG-6-phosphate, as described by
Sokoloff.98 The tissue components can be measured by the PET camera and the plasma
components can be measured by counting the activity in blood samples. With the
compartment model, the glucose consumption can be calculated in µmol per 100
grams of tissue per minute.
The majority of the PET studies with amino acid tracers have been performed with
L-[methyl-11C]-methionine (MET). 99-101 MET reflects amino acid uptake rather than
protein synthesis and because it is involved in other metabolic pathways such as
transmethylation and polyamine synthesis, this may lead to accumulation of a variety
of nonprotein metabolites in tumor tissue.102-104 This complicated metabolism of
methionine has made it impossible to create a precise metabolic model. Carboxyl-
labeled amino acids, such as L-[1-11C]-tyrosine (TYR), L-[1-11C]-methionine and L-
[1-11C]-leucine, appear to be more appropriate compounds to determine protein
synthesis in tumors.103,105 The main metabolite of these amino acids is 11CO2, which
is rapidly cleared from tissue and exhaled and does not contribute to the PET-measured11C radioactivity in tumor tissue. Using a method developed at the PET Center
Groningen, the protein synthesis rate can be determined using 11C labeled L-amino
acids with a four-compartment model: plasma-amino-acid, tissue-nonprotein-amino-
acid, metabolites and protein-incorporated-amino-acid.106
The aim of this thesis
Hyperthermic isolated limb perfusion is a major surgical procedure and over the
years new developments have been initiated and examined. Traditionally the
University Hospital Groningen plays an important role in the history of regional
perfusion and therefore this thesis describes different aspects of regional perfusion
during the last decade.
1. What are the short term effects of HILP with cisplatin in the local
treatment of spontaneous osteosarcoma in dogs?
2. Is HILP with TNF and cisplatin feasible in the canine model?
3. What are the results of HILP with cisplatin in patients with sarcomas of
soft tissue and bone?

20
Chapter 1
4. What is the relation between the tumor vascularization and the vascular
changes after irradiation therapy?
5. How does HILP influence the glucose metabolism and protein metabolism
as studied by PET, and is it possible to predict the outcome of therapy?
6. Is it worthwhile to monitor continuous leakage with RISA during HILP
with TNF and melphalan?

21
Introduction
References
1 Gilman A, Philips F.S. The biological actions and therapeutic applications of the β-
chlorethyl amines and sulfides. Science 1946; 103: 409-415.
2 Bierman H.R., Kelly K.H., Byron R.L., Dod K.S., Shimkin M.B. Studies on the
blood supply of tumors in men. Intra-arterial Nitrogen Mustard therapy of cutaneous
lesions. J Nat Cancer Inst 1951; 11: 891-897.
3 Klopp CT. Regional intra-arterial nitrogen mustard as an adjunct to radiation therapy.
Am J Roentgenol 1953; 70: 1005-1014.
4 Klopp CT, Alford RC, Bateman J, Berry GN, Winschip T. Fractionated intra-arterial
cancer chemotherapy with methyl bis amine hydrochloride: A preliminary report.
Ann Surg 1950; 132: 811-832.
5 Creech O, Krementz ET, Ryan RF, Winblad JN. Chemotherapy of cancer: regional
perfusion utilizing an extra-corporeal circuit. Ann Surg 1958; 148: 616-632.
6 Hafstrom L, Hugander A, Jonsson PE, Westling H, Ehrsson H. Blood leakage and
melphalan leakage from the perfusion circuit during regional hyperthermic perfusion
for malignant melanoma. Cancer Treat Rep 1984; 68: 867-872.
7 Briele HA, Djuric M, Jung DT, et al. Pharmacokinetics of melphalan in clinical
isolation perfusion of the extremities. Cancer Res 1985; 45: 1885-1889.
8 Benckhuijsen C, Kroon BB, Van Geel AN, Wieberdink J. Regional perfusion
treatment with melphalan for melanoma in a limb: an evaluation of drug kinetics.
Eur J Surg Oncol 1988; 14: 157-163.
9 Cavaliere R, Ciocatto EC, Giovanella BC, et al. Selective heat sensitivity of cancer
cells. Biochemical and clinical studies. Cancer 1967; 20: 1351-1381.
10 Stehlin JS, Jr. Hyperthermic perfusion with chemotherapy for cancers of the
extremities. Surg Gynecol Obstet 1969; 129: 305-308.
11 Wieberdink J, Benckhuysen C, Braat RP, Van Slooten EA, Olthuis GAA. Dosimetry
in isolation perfusion of the limb by assessment of perfused tissue volume and grading
of toxic tissue reactions. Eur J Cancer Clin Oncol 1982; 18: 905-910.
12 Stehlin JS, Clark RL, Dewey WC. Continuous monitoring of leakage during regional
perfusion. Arch Surg 1961; 83: 943-950.
13 Barker WC, Andrich MP, Alexander HR, Fraker DL. Continuous intraoperative
external monitoring of perfusate leak using iodine-131 human serum albumin during
isolated perfusion of the liver and limbs. Eur J Nucl Med 1995; 22: 1242-1248.
14 Klaase JM, Kroon BB, Van Geel AN, et al. Prognostic factors for tumor response
and limb recurrence-free interval in patients with advanced melanoma of the limbs
treated with regional isolated perfusion with melphalan. Surgery 1994; 115: 39-45.
15 Thompson JF, Hunt JA, Shannon KF, Kam PC. Frequency and duration of remission
after isolated limb perfusion for melanoma. Arch Surg 1997; 132: 903-907.
16 Krementz ET, Carter RD, Sutherland CM, et al. Regional chemotherapy for
melanoma. A 35-year experience. Ann Surg 1994; 220: 520-534.
17 Ghussen F, Krüger I, Groth W, Stützer H. The role of regional hyperthermic cytostatic
perfusion in the treatment of extremity melanoma. Cancer 1988; 61: 654-659.
18 Schraffordt Koops H, Kroon BB, Oldhoff J, Hoekstra HJ. Controversies concerning
adjuvant regional isolated perfusion for stage I melanoma of the extremities. World
J Surg 1992; 16: 241-245.

22
Chapter 1
19 Schraffordt Koops H, Vaglini M, Suciu S, et al. Prophylactic isolated limb perfusion
for localized, high-risk limb melanoma: results of a multicenter randomized phase
III trial. European Organization for Research and Treatment of Cancer Malignant
Melanoma Cooperative Group Protocol 18832, the World Health Organization
Melanoma Program Trial 15, and the North American Perfusion Group Southwest
Oncology Group-8593. J Clin Oncol 1998; 16: 2906-2912.
20 Hafstrom L, Rudenstam CM, Blomquist E, et al. Regional hyperthermic perfusion
with melphalan after surgery for recurrent malignant melanoma of the extremities.
Swedish Melanoma Study Group. J Clin Oncol 1991; 9: 2091-2094.
21 Hoekstra HJ, Schraffordt Koops H, De Vries EGE, Van Weerden TW, Oldhoff J.
Toxicity of hyperthermic isolated limb perfusion with cisplatin for recurrent
melanoma of the lower extremity after previous perfusion treatment. Cancer 1993;
72: 1224-1229.
22 van Ginkel RJ, Schraffordt Koops H, de Vries EG, et al. Hyperthermic isolated limb
perfusion with cisplatin in four patients with sarcomas of soft tissue and bone. Eur
J Surg Oncol 1996; 22: 528-531.
23 Thompson JF, Gianoutsos MP. Isolated limb perfusion for melanoma: effectiveness
and toxicity of cisplatin compared with that of melphalan and other drugs. World J
Surg 1992; 16: 227-233.
24 Vaglini M, Belli F, Marolda R, et al. Hyperthermic antiblastic perfusion with DTIC
in stage IIIA-IIIAB melanoma of the extremities. Eur J Surg Oncol 1987; 13: 127-
129.
25 Krementz ET, Carter RD, Sutherland CM, Hutton I. Chemotherapy of sarcomas of
the limbs by regional perfusion. Ann Surg 1977; 185: 555-564.
26 McBride CM. Sarcomas of the limbs. Results of adjuvant chemotherapy using
isolation perfusion. Arch Surg 1974; 109: 304-308.
27 Stehlin JS, de Ipolyi PD, Giovanella BC, Gutierrez AE, Anderson RF. Soft tissue
sarcomas of the extremity. Multidisciplinary therapy employing hyperthermic
perfusion. Am J Surg 1975; 130: 643-646.
28 Cavaliere R, Di Filippo F, Moricca G, et al. Hyperthermia and chemotherapy by
regional perfusion for tumors of the extremities. Prog Clin Biol Res 1982; 107: 775-
792.
29 Lehti PM, Moseley HS, Janoff K, Stevens K, Fletcher WS. Improved survival for
soft tissue sarcoma of the extremities by regional hyperthermic perfusion, local
excision and radiation therapy. Surg Gynecol Obstet 1986; 162: 149-152.
30 Krementz ET. Lucy Wortham James lecture. Regional perfusion. Current
sophistication, what next? Cancer 1986; 57: 416-432.
31 Hoekstra HJ, Schraffordt Koops H, Molenaar WM, Oldhoff J. Results of isolated
regional perfusion in the treatment of malignant soft tissue tumors of the extremities.
Cancer 1987; 60: 1703-1707.
32 Klaase JM, Kroon BBR, Benckhuijsen C, et al. Results of regional isolation perfusion
with cytostatics in patients with soft tissue tumors of the extremities. Cancer 1989;
64: 616-621.
33 Rossi CR, Vecchiato A, Foletto M, et al. Phase II study on neoadjuvant hyperthermic-
antiblastic perfusion with doxorubicin in patients with intermediate or high grade
limb sarcomas. Cancer 1994; 73: 2140-2146.

23
Introduction
34 Pommier RF, Moseley HS, Cohen J, et al. Pharmacokinetics, toxicity, and short-
term results of cisplatin hyperthermic isolated limb perfusion for soft-tissue sarcoma
and melanoma of the extremities. Am J Surg 1988; 155: 667-671.
35 Di Filippo F, Calabro AM, Cavallari A, et al. The role of hyperthermic perfusion as
a first step in the treatment of soft tissue sarcoma of the extremities. World J Surg
1988; 12: 332-339.
36 Suit HD, Mankin HJ, Wood WC, Proppe KH. Preoperative, intraoperative, and
postoperative radiation in the treatment of primary soft tissue sarcoma. Cancer 1985;
55: 2659-2667.
37 Eilber FR, Giuliano AE, Huth JF, Morton DL. A randomized prospective trial using
postoperative adjuvant chemotherapy (adriamycin) in high-grade extremity soft-
tissue sarcoma. Am J Clin Oncol 1988; 11: 39-45.
38 Hoekstra HJ, Schraffordt Koops H, Molenaar WM, et al. A combination of
intraarterial chemotherapy, preoperative and postoperative radiotherapy, and surgery
as limb-saving treatment of primarily unresectable high-grade soft tissue sarcomas
of the extremities. Cancer 1989; 63: 59-62.
39 Williard WC, Hajdu SI, Casper ES, Brennan MF. Comparison of amputation with
limb-sparing operations for adult soft tissue sarcoma of the extremity. Ann Surg
1992; 215 : 269-275.
40 Coley WB. The treatment of malignant tumors by repeated inoculations of erysipelas;
with a report of ten original cases. Am J Med Sci 1893; 105: 487-511.
41 Coley WB. Late results of the treatment of inoperable sarcoma by mixed toxins of
erysipelas and bacillus prodigiosus. Am J Med Sci 1906; 131: 375-430.
42 Shear MJ, Turner FC, Perrault A, Shovelton J. Chemical treatment of tumors. V.
Isolation of the hemorrhage-producing fraction from Serratia marcescens (Bacillus
prodigiosus) culture filtrate. J Nat Cancer Inst 1943; 4: 81-97.
43 Shear MJ, Perrault A, Adams JR, Jr. Chemical treatment of tumors. VI. Methods
employed in determining the potency of hemorrhage-producing bacterial
preparations. J Nat Cancer Inst 1943; 4: 99-105.
44 Hartwell JL, Shear MJ, Adams JR, Jr. Chemical treatment of tumors. VII. Nature of
the hemorrhage-producing fraction from Serratia marcescens (Bacillus prodigiosus)
culture filtrate. J Nat Cancer Inst 1943; 4: 107-122.
45 Shear MJ. Chemical treatment of tumors. IX. Reactions of mice with primary
subcutaneous tumors to injection of a hemorrhage-producing fraction bacterial
polysaccharide. J Nat Cancer Inst 1944; 4: 461-476.
46 O’Malley WE, Shear MJ, Achinstein B. Action of bacterial polysaccharide on tumors.
II. Damage of sarcoma 37 by serum of mice treated with Serratia marcescens
polysaccharide, and induced tolerance. J Nat Cancer Inst 1962; 29: 1169-1175.
47 Carswell EA, Old LJ, Kassel RL. An endotoxin induced serum factor that causes
necrosis of tumors. Proc Natl Acad Sci USA 1975; 72: 3666-3670.
48 Mannel DN, Falk W, Meltzer MS. Inhibition of nonspecific tumoricidal activity by
activated macrophages with antiserum against a soluble cytotoxic factor. Infect Immun
1981; 33: 156-164.
49 Matthews N. Tumour-necrosis factor from the rabbit. V. Synthesis in vitro by
mononuclear phagocytes from various tissues of normal and BCG- injected rabbits.
Br J Cancer 1981; 44: 418-424.

24
Chapter 1
50 Zacharchuk CM, Drysdale BE, Mayer MM, Shin HS. Macrophage-mediated
cytotoxicity: role of a soluble macrophage cytotoxic factor similar to lymphotoxin
and tumor necrosis factor. Proc Natl Acad Sci U S A 1983; 80: 6341-6345.
51 Bloksma N, Hofhuis FM, Willers JM. Role of mononuclear phagocyte function in
endotoxin-induced tumor necrosis. Eur J Cancer Clin Oncol 1984; 20: 397-403.
52 Aggarwal BB, Kohr WJ, Hass PE, et al. Human tumor necrosis factor. Production,
purification, and characterization. J Biol Chem 1985; 260: 2345-2354.
53 Pennica D, Nedwin GE, Hayflick JS, et al. Human tumor necrosis factor: precursor
structure, expression and homology to lymphotoxin. Nature 1984; 312: 724-729.
54 Wang AM, Creasey AA, Ladner MB, et al. Molecular cloning of the complementary
DNA for human tumor necrosis factor. Science 1985; 228: 149-154.
55 Shirai T, Yamaguchi H, Ito H, Todd CW, Wallace RB. Cloning and expression in
Escherichia coli of the gene for human tumor necrosis factor. Nature 1985; 313:
803-806.
56 Nedwin GE, Naylor SL, Sakaguchi AY, et al. Human lymphotoxin and tumor necrosis
factor genes: structure, homology and chromosomal localization. Nucleic Acids Res
1985; 13: 6361-6373.
57 Kemeny N, Childs B, Larchian W, Rosado K, Kelsen D. A phase II trial of
recombinant tumor necrosis factor in patients with advanced colorectal carcinoma.
Cancer 1990; 66: 659-663.
58 Schaadt M, Pfreundschuh M, Lorscheidt G, et al. Phase II study of recombinant
human tumor necrosis factor in colorectal carcinoma. J Biol Response Mod 1990; 9:
247-250.
59 Whitehead RP, Fleming T, MacDonald JS, et al. A phase II trial of recombinant
tumor necrosis factor in patients with metastatic colorectal adenocarcinoma: a
Southwest Oncology Group study. J Biol Response Mod 1990; 9: 588-591.
60 Feldman ER, Creagan ET, Schaid DJ, Ahmann DL. Phase II trial of recombinant
tumor necrosis factor in disseminated malignant melanoma. Am J Clin Oncol 1992;
15: 256-259.
61 Feinberg B, Kurzrock R, Talpaz M, et al. A phase I trial of intravenously-administered
recombinant tumor necrosis factor-alpha in cancer patients. J Clin Oncol 1988; 6:
1328-1334.
62 Spriggs DR, Sherman ML, Michie H, et al. Recombinant human tumor necrosis
factor administered as a 24- hour intravenous infusion. A phase I and pharmacologic
study. J Natl Cancer Inst 1988; 80: 1039-1044.
63 Jakubowski AA, Casper ES, Gabrilove JL, et al. Phase I trial of intramuscularly
administered tumor necrosis factor in patients with advanced cancer. J Clin Oncol
1989; 7: 298-303.
64 Tracey KJ, Lowry SF, Fahey TJ3, et al. Cachectin/tumor necrosis factor induces
lethal shock and stress hormone responses in the dog. Surg Gynecol Obstet 1987;
164: 415-422.
65 Chapman PB, Lester TJ, Casper ES, et al. Clinical pharmacology of recombinant
human tumor necrosis factor in patients with advanced cancer. J Clin Oncol 1987;
5: 1942-1951.
66 Creaven PJ, Plager JE, Dupere S, et al. Phase I clinical trial of recombinant human
tumor necrosis factor. Cancer Chemother Pharmacol 1987; 20: 137-144.

25
Introduction
67 Lienard D, Ewalenko P, Delmotte JJ, Renard N, Lejeune FJ. High-dose recombinant
tumor necrosis factor alpha in combination with interferon gamma and melphalan
in isolation perfusion of the limbs for melanoma and sarcoma. J Clin Oncol 1992;
10: 52-60.
68 Gerain J, Lienard D, Ewalenko P, Lejeune FJ. High serum levels of TNF-alpha after
its administration for isolation perfusion of the limb. Cytokine 1992; 4: 585-591.
69 Posner MC, Lienard D, Lejeune FJ, Rosenfelder D, Kirkwood J. Hyperthermic
Isolated Limb Perfusion With Tumor Necrosis Factor Alone for Melanoma. Cancer
J Sci Am 1995; 1: 274-274.
70 Mutch DG, Powell CB, Kao MS, Collins JL. In vitro analysis of the anticancer
potential of tumor necrosis factor in combination with cisplatin. Gynecol Oncol
1989; 34: 328-333.
71 Regenass U, Muller M, Curschellas E, Matter A. Anti-tumor effects of tumor necrosis
factor in combination with chemotherapeutic agents. Int J Cancer 1987; 39: 266-
273.
72 Aggarwal BB, Eessalu TE, Hass PE. Characterization of receptors for human tumor
necrosis factor and their regulation by gamma-interferon. Nature 1985; 318: 665-
667.
73 Ruggiero V, Tavernier J, Fiers W, Baglioni C. Induction of the synthesis of tumor
necrosis factor receptors by interferon-gamma. J Immunol 1986; 136: 2445-2450.
74 Lienard D, Lejeune FJ, Ewalenko P. In transit metastases of malignant melanoma
treated by high dose rTNF alpha in combination with interferon-gamma and
melphalan in isolation perfusion. World J Surg 1992; 16: 234-240.
75 Lienard D, Eggermont AM, Kroon BB, Schraffordt Koops H, Lejeune FJ. Isolated
limb perfusion in primary and recurrent melanoma: indications and results. Semin
Surg Oncol 1998; 14: 202-209.
76 Fraker DL, Alexander HR, Bartlett DL, Rosenberg SA. A prospective randomized
trial of therapeutic isolated limb perfusion (ILP) comparing melphalan (M) versus
melphalan, tumor necrosis factor (TNF) and interferon, an initial report.
Proc.Soc.Surg.Oncol. 1996; 6 (Abstract).
77 Eggermont AMM, Schraffordt Koops H, Lienard D, et al. Isolated limb perfusion
with high-dose tumor necrosis factor-alfa in combination with interferon-gamma
and melphalan for nonresectable extremity soft tissue sarcomas: a multicenter trial.
J Clin Oncol 1996; 14: 2653-2665.
78 Eggermont AM, Schraffordt Koops H, Klausner JM, et al. Isolated limb perfusion
with tumor necrosis factor and melphalan for limb salvage in 186 patients with
locally advanced soft tissue extremity sarcomas. The cumulative multicenter
European experience. Ann Surg 1996; 224: 756-64; discussion 764-5.
79 Gutman M, Inbar M, Lev Shlush D, et al. High dose tumor necrosis factor-alpha
and melphalan administered via isolated limb perfusion for advanced limb soft tissue
sarcoma results in a >90% response rate and limb preservation. Cancer 1997; 79:
1129-1137.
80 Olieman AF, van Ginkel RJ, Molenaar WM, Schraffordt Koops H, Hoekstra HJ.
Hyperthermic isolated limb perfusion with tumor necrosis factor- alpha and
melphalan as palliative limb-saving treatment in patients with locally advanced soft-
tissue sarcomas of the extremities with regional or distant metastases. Is it
worthwhile? Arch Orthop Trauma Surg 1998; 118: 70-74.

26
Chapter 1
81 Olieman AF, van Ginkel RJ, Hoekstra HJ, et al. Angiographic response of locally
advanced soft-tissue sarcoma following hyperthermic isolated limb perfusion with
tumor necrosis factor. Ann Surg Oncol 1997; 4: 64-69.
82 Olieman AF, Lienard D, Eggermont AM, et al. Hyperthermic isolated limb perfusion
with tumor necrosis factor alpha, interferon gamma, and melphalan for locally
advanced nonmelanoma skin tumors of the extremities: a multicenter study. Arch
Surg 1999; 134: 303-307.
83 Sonneveld EJ, Vrouenraets BC, Van Geel BN, et al. Systemic toxicity after isolated
limb perfusion with melphalan for melanoma. Eur J Surg Oncol 1996; 22: 521-527.
84 Zwaveling JH, Maring JK, Mulder AB, et al. Effects of hyperthermic isolated limb
perfusion with recombinant tumor necrosis factor alpha and melphalan on the human
fibrinolytic system. Cancer Res 1996; 56: 3948-3953.
85 Zwaveling JH, Maring JK, Clarke FL, et al. High plasma tumor necrosis factor
(TNF)-alpha concentrations and a sepsis-like syndrome in patients undergoing
hyperthermic isolated limb perfusion with recombinant TNF-alpha, interferon-
gamma, and melphalan. Crit Care Med 1996; 24: 765-770.
86 Thom AK, Alexander HR, Andrich MP, et al. Cytokine levels and systemic toxicity
in patients undergoing isolated limb perfusion with high-dose tumor necrosis factor,
interferon gamma, and melphalan. J Clin Oncol 1995; 13: 264-273.
87 Vrouenraets BC, Kroon BB, Ogilvie AC, et al. Absence of severe systemic toxicity
after leakage-controlled isolated limb perfusion with tumor necrosis factor-alpha
and melphalan. Ann Surg Oncol 1999; 6: 405-412.
88 Stam TC, Swaak AJ, de Vries MR, ten Hagen TL, Eggermont AM. Systemic toxicity
and cytokine/acute phase protein levels in patients after isolated limb perfusion with
tumor necrosis factor-alpha complicated by high leakage. Ann Surg Oncol 2000; 7:
268-275.
89 Eggimann P, Chiolero R, Chassot PG, et al. Systemic and hemodynamic effects of
recombinant tumor necrosis factor alpha in isolation perfusion of the limbs. Chest
1995; 107: 1074-1082.
90 Fawcett WJ, Hill S, Sheldon J, et al. Hemodynamic changes and circulating
recombinant tumor necrosis factor-alpha concentrations in a patient undergoing
isolated limb perfusion. Crit Care Med 1993; 21: 796-800.
91 Van Geel AN, van Wijk J, Wieberdink J. Functional morbidity after regional isolated
perfusion of the limb for melanoma. Cancer 1989; 63: 1092-1096.
92 Vrouenraets BC, Klaase JM, Nieweg OE, Kroon BB. Toxicity and morbidity of
isolated limb perfusion. Semin Surg Oncol 1998; 14: 224-231.
93 Schraffordt Koops H. Prevention of neural and muscular lesions during hyperthermic
regional perfusion. Surg Gynecol Obstet 1972; 135: 401-403.
94 Olieman AF, Schraffordt Koops H, Geertzen JH, et al. Functional morbidity of
hyperthermic isolated regional perfusion of the extremities. Ann Surg Oncol 1994;
1: 382-388.
95 Strauss LG, Conti PS. The applications of PET in clinical oncology. J Nucl Med
1991; 32: 623-648.
96 Kern KA, Brunetti A, Norton JA, et al. Metabolic imaging of human extremity
musculoskeletal tumors by PET. J Nucl Med 1988; 29: 181-186.
97 Warburg O. On the origin of cancer cells. Science 1956; 123: 309-314.

27
Introduction
98 Sokoloff L, Reivich M, Kennedy C, et al. The [14C]deoxyglucose method for the
measurement of local cerebral glucose utilization: theory, procedure, and normal
values in the conscious and anesthetized albino rat. Journal of Neurochemistry 1977;
28: 897-916.
99 Schober O, Meyer GJ, Duden C, et al. [Amino acid uptake in brain tumors using
positron emission tomography as an indicator for evaluating metabolic activity and
malignancy]. ROFO Fortschr Geb Rontgenstr Nuklearmed 1987; 147: 503-509.
100 Derlon JM, Bourdet C, Bustany P, et al. [11C]L-methionine uptake in gliomas.
Neurosurgery 1989; 25: 720-728.
101 Lilja A, Lundqvist H, Olsson Y, et al. Positron emission tomography and computed
tomography in differential diagnosis between recurrent or residual glioma and
treatment-induced brain lesions. Acta Radiol 1989; 30: 121-128.
102 Daemen BJ, Elsinga PH, Ishiwata K, Paans AM, Vaalburg W. A comparative PET
study using different 11C-labelled amino acids in Walker 256 carcinosarcoma-bearing
rats. Int J Rad Appl Instrum [B] 1991; 18: 197-204.
103 Ishiwata K, Vaalburg W, Elsinga PH, Paans AM, Woldring MG. Comparison of L-
[1-11C]methionine and L-methyl-[11C]methionine for measuring in vivo protein
synthesis rates with PET. J Nucl Med 1988; 29: 1419-1427.
104 Ishiwata K, Kubota K, Murakami M, Kubota R, Senda M. A comparative study on
protein incorporation of L-[methyl- 3H]methionine, L-[1-14C]leucine and L-2-
[18F]fluorotyrosine in tumor bearing mice. Nucl Med Biol 1993; 20: 895-899.
105 Bolster JM, Vaalburg W, Paans AM, et al. Carbon-11 labelled tyrosine to study
tumor metabolism by positron emission tomography (PET). Eur J Nucl Med 1986;
12: 321-324.
106 Willemsen ATM, van Waarde A, Paans AM, et al. In vivo protein synthesis rate
determination in primary or recurrent brain tumors using L-[1-11C]-tyrosine and
PET. J Nucl Med 1995; 36: 411-419.

28

29
Robert J. van Ginkel1
Harald J. Hoekstra1
Freek J. Meutstege2
Jan W. Oosterhuis3
Donald R.A. Uges4
Heimen Schraffordt Koops1
Departments of Surgical Oncology1 and Pharmacy4, University Hospital Groningen,
Department of Veterinary Medicine2, State University Utrecht, and
Dr. Daniel den Hoed Cancer Center3, Rotterdam, The Netherlands.
Journal of Surgical Oncology 1995; 59: 169-176.
Hyperthermic isolated limb perfusion with cisplatin
in the local treatment of spontaneous canine
osteosarcoma: Assessment of short-term effects

30
Chapter 2
Abstract
To increase the effect of cisplatin on locoregional osteosarcoma, the short term effect
of hyperthermic isolated limb perfusion (HILP) with cisplatin (30 mg/L extremity
volume) was studied in 28 dogs with spontaneous osteogenic sarcoma using clinical,
radiological, and histological parameters. Thirty days postoperative mortality was
14.3 %. Total platinum levels at the start of perfusion were 28.2 ± 14.3 mg/L. A
significant improvement (p<0.001) in the clinical score was observed in the overall
group at 6 and 12 weeks after perfusion. The radiological parameter showed a
stationary X-ray 2 weeks after perfusion and an improved X-ray 6 weeks after
perfusion. Overall histological scores showed a moderate effect according to the
Huvos classification. No additional therapeutic effect, according to the three
parameters, could be demonstrated by increasing the perfusate temperature by 1°C.
HILP with cisplatin is feasible in the local treatment of spontaneous osteosarcoma
in dogs with acceptable locoregional toxicity. However the histological results were
modest, with none of the dogs showing a complete response 6 weeks after perfusion.
Therefore, the search for the ideal perfusion agent with substantial contribution to
the limb-sparing treatment in human osteosarcoma, continues.
Introduction
Osteosarcoma is the most frequent primary malignant bone tumor in humans. Until
the early 1970s, the most common approach to the management of localized
osteosarcoma was surgical resection, amputation or radiation. In most large series of
patients treated in this manner, long term survival was only 20%.1,2 During the past
few decades, the use and further development of systemic neoadjuvant chemotherapy,
e.g., including high-dose methotrexate (HD-MTX) and cisplatin, appears to have a
definite influence on the disease free and overall survival for patients with
osteosarcoma.3-5 The effect of the systemic neoadjuvant chemotherapy on the primary
bone tumor, the improved surgical resection technique, and the development of
prosthetic replacement techniques also improved the limb salvage rate for
osteosarcomas, especially for the lower extremity. Salvage rates varying from 40 %
to almost 80 % are reported.6
However, the potential local tumor effect of the systemic neoadjuvant chemotherapy
is not always favorable, although a good response of the local tumor to systemic
chemotherapy demonstrated prognostic value.7 Increasing the systemic chemotherapy
dose to achieve a higher local tumor response is limited due to the nephrotoxicity
and ototoxicity of cisplatin. To avoid systemic toxicity but to raise the effect on the
local tumor and thereby facilitate limb preserving procedures, a local treatment of
the primary tumor could be the solution.

31
Cisplatin perfusion for canine osteosarcoma
With hyperthermic isolated limb perfusion (HILP) as a local treatment modality, it is
possible to obtain very high local drug concentrations in a limb with minimal systemic
toxicity.8 The value of cisplatin in HILP has also been demonstrated in humans for
melanoma and various soft tissue sarcomas.9-11 Fletcher and associates showed that
250 mg/m2 was the maximum tolerable dose of cisplatin for lower-extremity
perfusions, with improved local control rates for sarcomas and melanoma of the
extremities without regional nodal metastases.12 Before introducing HILP with
cisplatin in the clinical treatment of osteosarcoma of the limb, the short term effect
of this treatment modality on the primary tumor was investigated by clinical,
radiological, and histological parameters in dogs with spontaneous osteogenic sarcoma
of the limb. Biological behavior of osteosarcoma is similar both in human and in
dogs; a locally aggressive bone tumor predominantly occurring in the long bones
with early hematogenous metastases to the lungs.13,14 The differences between canine
and human osteosarcoma are that in humans a younger age group (adolescence) is
most commonly affected, and the tumor is less common.With the high frequency of
occurrence in dogs, allows canine osteosarcoma is a useful model for evaluation of
new treatment regimens in humans as rapid case accrual and rapid time to reach
measurable end points are possible. The canine osteosarcoma therefore appears to be
a valid model for studying the potential treatment of HILP with cisplatin in the local
treatment of osteosarcomas of the extremity in humans.
Materials and methods
Dogs
Twenty-eight dogs with an average weight of 45 ± 10.0 kg and a mean age of 7 ± 2.5
years with spontaneous, histologically proven, previously untreated, primary
osteosarcoma of the extremity, without radiographic evidence of distant metastases,
underwent HILP with cisplatin. Preoperatively, all dogs were thoroughly clinically
evaluated at the Department of Veterinary Medicine and underwent a complete blood
count (CDC), serum chemistry profile, and X-rays of the primary tumor and thorax.
The perfusion procedure was performed at the Central Animal Facility of the State
University Groningen, while follow-up was performed at the Department of Veterinary
Medicine Utrecht. The study was approved by the Animal Welfare Committee of the
Faculty of Medicine of the State University Groningen.
Anesthetics
All dogs were premedicated with atropine sulfate (0.5 mg, i.m.) and piritramide (15-
17.5 mg, i.m.)(Dipidolor, Janssen Pharmaceutica, Tilburg, The Netherlands). The
dogs were anesthetized with thiopenthal (30 mg/kg BW, i.v.)(Pentothal, Abbott,

32
Chapter 2
Amstelveen, The Netherlands) and after muscle relaxation with pancuroniumbromide
(0.08mg/kg BW, i.v.)(Pavulon, Organon, Oss, The Netherlands), the dogs were
ventilated by means of a Siemens Servo Ventilator 900B, with a mixture of
nitrousoxide and oxygen. The oxygen concentration in the gas mixture, continuously
measured by means of an oxygen analyzer (Taylor Servomex OA 272), and minute
volume (4-6 L/min), were adjusted to maintain an end-expiratory CO2 concentration
of 4-5% (Siemens CO2-analyser 930). The dogs were placed in the supine position
on a heated mattress to maintain their normal body temperature of 38 °C.15 During
the operations, all dogs were given about 500 ml of Isodex through the cephalic vein.
Operation and perfusion techniques
The iliac or axillary vessels of the affected limb were exposed under sterile conditions
and collateral vessels were clipped. Cannulas were inserted into the artery (Bardic,
16F-18F) and vein (Portex, 6-8 mm). Both cannulas were connected to an
extracorporeal circuit consisting of an occlusive roller pump, a cardiotomy reservoir
and a bubble oxygenator with heat-exchanger. A canvas tourniquet was placed around
the base of the extremity to complete isolation of the limb from the systemic
circulation. The perfusate consisted of 350 ml of 5% dextran 40 in glucose 5% (Isodex,
Pharmacia AB, Uppsala, Sweden), 250 ml red blood cells (typed canine blood donors),
250 ml plasma, 30 ml sodium bicarbonate 8.4%, and 0.5 ml 5000 IU/ml heparin
(Thromboliquine, Organon BV, Oss, the Netherlands). A mixture of oxygen, air, and
carbon dioxide through the oxygenator was adjusted to maintain the blood gas values
within the physiological range and, when necessary, bicarbonate was added to adjust
the pH.
All perfusions were performed under hyperthermic conditions. To study the effects
of additional heat to the perfusate, two groups of dogs were randomized. In group I
(14 dogs), HILP of the extremity was performed at 39-40°C limb temperature; and
for group II (14 dogs), HILP was performed at 40-41 °C limb temperature. The arterial
line temperature was kept at 40-41 °C in group I and at 41-42 °C in group II. In
addition a 1000 Watt infrared lamp was placed at a distance of 90 cm to heat the
extremity. Thermistor probes (Electrolaboriet, Copenhagen, Denmark) were inserted
into the subcutaneous tissue and into a muscle of the proximal limb just above the
knee for continuous monitoring of the temperatures during perfusion. The perfusion
time was 1 hour and the perfusion was followed by washout of the extremity with
500 ml of Isodex. Tourniquet, cannulas and clips were then removed and the incisions
in the vessels were repaired. Protamine hydrochloride (Hoffman La Roche, Mijdrecht,
The Netherlands) was administered to neutralize heparin, in a ratio of 1:1 to the
initial dose of heparin. All dogs were observed for one night and allowed to go home

33
Cisplatin perfusion for canine osteosarcoma
with the owner the next day. No anti-inflammatory medications or analgesics were
administered during follow up.
The dosage of cisplatin (Platinol 0.5 mg/ml�, Bristol Myers SAE, Barcelona, Spain)
used in the perfusion had been established in a previous study which showed massive
edema with necrosis and fibrosis with cellular infiltrates in skeletal muscle throughout
the perfused extremity in dogs that received 45 mg cisplatin per liter extremity
volume.16 These local side effects were not seen after a 30% dose reduction to 30
mg/L extremity volume, as used in the present study. The volume of the extremity
was determined by submersion in water to the tourniquet border and measurement of
displaced water volume. Extremity volumes varied from 1.7 ± 0.27 L. Cisplatin was
added to the circulated perfusate in 10 minutes. During perfusion, serum platinum
levels were determined in the regional and systemic circulation at 0, 10, 20, 30, 40,
50, and 60 minutes by flameless atomic absorption spectrophotometry (FAAS).
Local effect parameters
Short-term effects on the tumor were determined using three parameters: clinical,
radiological, and histological. The clinical score was determined by a veterinarian
on the basis of gait analysis: walking on three legs (score I), severe limp (score II),
slight limp (score III), walking normally (score IV). This score was determined 1
week before and at 2, 6 and 12 weeks after perfusion. The radiological score was
determined by a veterinarian radiologist on conventional X-rays in two directions of
the extremity according to methods described earlier.17,18 Preperfusion X-rays were
compared with 2 and 6 week postperfusion X-rays: progression (score I), stationary
(score II), regression (score III), the latter defined as a decrease in tumor volume,
increased ossification of intraosseous tumor osteoid, periosteal new bone and soft
tissue margin more densely ossified and well-defined resulting in a more benign
appearance. Biopsies from the tumor were taken before, and 2 and 6 weeks after
perfusion at random in three directions with a 3.5 mm diameter Coombs bone biopsy
system.19 The histological score was determined by a pathologist on the material
obtained from the biopsies, according to the criteria of Huvos et al.20 no reaction
(score I), moderate effect (score II), good effect (score III), total necrosis (score IV).
The radiological as well as the histological scores describe the response to treatment;
therefore, it was not possible to score these parameters 1 week before treatment, as it
was with the clinical score. All dogs were followed for local and systemic side effects
by the cisplatin perfusion.

34
Chapter 2
Statistical Considerations
Mean clinical, radiological and histological scores of the total group were analyzed
with the Pittman test. Differences between group I and II were analyzed with the
Yates & Cockran test. The survival curve was calculated according to the Kaplan
Meier method.21 P-values <0.05 were considered significant.
Results
Although the dogs underwent a thorough clinical work-up before treatment, the
investigators were confronted with a 30 days postoperative mortality of 14.3%
(4 dogs). The first dog, 10 years of age, died at the end of the perfusion from cardiac
failure. The other two dogs, both 6 years of age, died postoperatively due to pulmonary
and cardiac failure. Postmortem examination of those two dogs was not obtained
from their owners. A fourth dog died 1 week after the perfusion from a large myocardial
infarction. Postmortem examination of this animal showed a completely necrotic
tumor.
No systemic or normal tissue side effects of the perfusion were encountered. The
local reaction of the limb to the perfusion consisted of an initial slight edema that
reached a maximum on the third postoperative day and disappeared completely within
the first week. Total platinum levels in the perfusate ranged from 28.2 ± 14.3 mg/L at
the start of perfusion to 12.1 ± 5.3 mg/L at the end of a 1-hour perfusion in the total
group. There was no significant difference in platinum levels during perfusion between
group I and II. Systemic platinum levels never rose above 0.7 mg/L in both groups
(Fig. 1).
Fig. 1 Concentration of total platinum
(tPt) measured in the perfusate during
cisplatin perfusion. Values are the
mean of all dogs; error bars are ± SEM.
Time 0 is the time of administration of
30 mg cisplatin per liter extremity vol-
ume.

35
Cisplatin perfusion for canine osteosarcoma
Ta
ble
1D
istribu
tion
of clin
ical param
eters at 1 w
eek b
efore, an
d at 2
, 6 an
d 1
2 w
eeks after p
erfusio
n
Clin
ical
Gro
up
I an
d II
Gro
up
IG
rou
p II
Tim
e-1
we
ek
2 w
eeks
6 w
eeks
12 w
eek
-1 w
eek
2 w
eeks
6 w
eeks
12 w
eeks
-1 w
eek
2 w
ee
ks
6 w
ee
ks
12 w
eeks
Nu
mb
er o
f do
gs
N=
28
N=
24
N=
24
N=
17
N=
14
N=
11
N=
11
N=
9N
=14
N=
13
N=
13
N=
8
I Th
ree
leg
s 6
(21%
) 5
(21%
) 3
(13%
)2 (1
2%
)3 (2
1%
)_
1 (9
%)
_3
(21%
)5 (3
8%
)2 (1
5%
)2
(25%
)
II Se
ve
re lim
p1
5 (5
4%
) 6
(25%
) 3
(13%
)2 (1
2%
)8 (5
8%
)5 (4
5%
)_
_7 (5
0%
)1 (8
%)
3 (2
4%
)2 (2
5%
)
III Slig
ht lim
p 6
(21%
)11
(46%
) 8
(33%
)4 (2
4%
)3 (2
1%
)6 (5
5%
)6 (5
5%
)3 (3
3%
)3
(21%
)5 (3
8%
)2 (1
5%
)1
(13%
)
IV W
alk
s n
orm
ally
1 (4
%)
2 (8
%)
10 (4
1%
)9 (5
2%
)_
_4 (3
5%
)6 (6
7%
)1 (8
%)
2 (1
6%
)6 (4
6%
)3
(47%
)

36
Chapter 2
The clinical scores in the total group before and after treatment could be compared.
Before perfusion: 6 dogs (21%) walked on three legs; 15 dogs (54%) walked with a
severe limp; 6 dogs (21%) walked with a slight limp; and 2 dogs (4%) walked
normally. Two weeks after perfusion: 5 dogs (21%) walked on three legs; 6 dogs
(25%) walked with a severe limp; 11 dogs (46%) walked with a slight limp; and 2
dogs (8%) walked normally (Table 1).At 6 and 12 weeks after HILP therapy, the
improvement of walking with a severe limp towards a normal walking pattern
continued.
Radiological scores for the total group 2 weeks after perfusion: progression in 3
dogs (12%); stationary in 13 dogs (52%); and an improved X-ray was found in 9
dogs (36%). Radiological scores 6 weeks after perfusion: progression in 6 dogs (25%);
stationary in 3 dogs (12%) and an improved X-ray was found in 15 dogs (63%)
(Table 2). These scores illustrate a change from a stationary X-ray, 2 weeks after
perfusion toward an improved X-ray 6 weeks after perfusion.
The histological effect of cisplatin on the tumor was classified according to Huvos et
al.20 Biopsy scores for the total group two weeks after perfusion showed: no reaction,
Huvos I in 5 dogs (20%); moderate effect, Huvos II in 8 dogs (32%); good effect,
Huvos III in 7 dogs (28%); total necrosis, Huvos IV in 5 dogs (20%). Six weeks after
perfusion, biopsy scores were as follows: no reaction, Huvos I in 3 dogs (14%);
moderate effect, Huvos II in 12 dogs (57%); good effect, Huvos III in 6 dogs (29%);
total necrosis, Huvos IV in none of the dogs (Table 3). At 2 and at 6 weeks after
perfusion, the overall histological score is one of moderate effect according to Huvos
et al.20
After summation of the individual scores, there was a significant improvement
(p<0.001) in the clinical score in the total group 6 and 12 weeks after perfusion;
respectively; 2.04 before perfusion to 3.04 6 weeks and 3.18 at 12 weeks after
perfusion (Table 4). Radiological and histological scores only classify the response
to treatment; therefore, mean radiological and histological scores before and after
perfusion could not be compared. However, a comparison of the radiological and
histological scores between 2-6 weeks could be made. There was no significant
improvement or deterioration in radiological and histological mean scores between
2-6 weeks in the total group. Analysis of the distribution and the mean scores of all
three parameters demonstrate that additional hyperthermia of 1°C (group I versus
group II) did not improve the results of the measured parameters. Retrospective
analysis of survival time showed a median survival for all dogs of 115 days (Fig. 2).
Three dogs underwent a resection or amputation of the affected limb and survived
12, 24 and 43 months, respectively, after perfusion without evidence of disease.

37
Cisplatin perfusion for canine osteosarcoma
Table 2 Distribution of radiological parameters at 2 and 6 weeks after perfusion
Radiological Group I and II Group I Group II
Time 2 weeks 6 weeks 2 weeks 6 weeks 2 weeks 6 weeks
Number of dogs N=25 N=24 N=12 * N=11 N=13 N=13
I progression 3 (12%) 6 (25%) 2 (18%) 3 (23%) 4 (31%)
II stationary 13 (52%) 3 (12%) 10 (83%) 1 (9%) 3 (23%) 2 (15%)
III improved 9 (36%) 15 (63%) 2 (17%) 8 (73%) 7 (54%) 7 (54%)
*The radiological score of the dog that died 1 week after perfusion from a myocardial infarction included
Table 3 Distribution of histological parameters at 2 and 6 weeks after perfusion
Histology Group I and II Group I Group II
Time 2 weeks 6 weeks 2 weeks 6 weeks 2 weeks 6 weeks
Number of dogs N=25 * N=21 N=12 * N=11 N=13 N=10
I no reaction 5 (20%) 3 (14%) 1 (8%) 1 (10%) 4 (30%) 2 (20%)
II moderate 8 (32%) 12 (57%) 2 (17%) 5 (45%) 6 (46%) 7 (70%)
III good 7 (28%) 6 (29%) 7 (58%) 5 (45%) 1 (10%)
IV necrosis 5 (20%) 2 (17%) 3 (24%)
*The histological score of the dog that died 1 week after perfusion from a myocardial infarction included
Table 4 Mean clinical, radiological and histological scores
Mean scores Clinical Radiological Histological
Time -1 wks 2 wks 6 wks 12 wks 2 wks 6 wks 2 wks 6 wks
Mean group I 1.93 2.55 3.18 3.67 * 2.17 2.55 2.83 2.36
Mean group II 2.14 2.31 2.92 2.63 2.31 2.23 2.15 1.90
Mean group I + II 2.04 2.42 3.04 ** 3.18 ** 2.24 2.38 2.48 2.14
*p < 0.05 group I versus group II; ** p < 0.001 compared with the pre-perfusion score

38
Chapter 2
Discussion
In the treatment of osteogenic sarcoma a distinction can be made between systemic
therapy and locoregional treatment. Systemic therapy is primarily concerned with
eradicating possible micrometastatic disease and its use was a major breakthrough in
the clinical treatment of osteosarcomas in the 1970s. About 60 % of patients with
resectable primary tumors and no metastases at diagnosis will be cured.
The primary objective in locoregional treatment is to prevent local recurrence and
allow limb salvage procedures in an attempt to preserve limb function. New surgical
techniques and the development of endoprosthetic materials, coupled with the systemic
neo adjuvant chemotherapy, have offered less radical surgery for 40 % - 80 % of
patients with osteosarcoma in the 1980s.6 Procedures that increase tumor necrosis of
the primary tumor, and with that reduction of viable tumor cells and tumor volume,
could contribute to limb preservation strategies. At first changes in systemic
chemotherapy regimens were investigated to achieve this goal. In 1978, cisplatin
exhibited activity in the treatment of osteogenic sarcoma.22,23 Since its first use,
cisplatin has been one of the most effective chemotherapeutic agents and has been
incorporated in most systemic treatment regimens for osteosarcoma. The potential
local tumor effect of systemically administered cisplatin, however, is limited due to
the nephrotoxicity and ototoxicity of cisplatin. Techniques that administer cisplatin
locally have been introduced to surmount these systemic side effect restrictions.
Powers et al. demonstrated the superiority of the intra-arterial administration of
cisplatin to the intravenous route in canine osteosarcoma.24 Jaffe et al. reported a 50
% response rate from intra-arterial infusion with cisplatin in osteosarcoma and
recommended it for use in inoperable tumors, to render them suitable for limb
salvage.25 On the other hand, Wile et al. demonstrated the superiority regional perfusion
with cisplatin to the intra-arterial or intravenous route in an experimental
pharmacokinetic study.26
Fig. 2 Survival of all dogs after
treatment with cisplatin hyperther-
mic isolated limb perfusion. Ex-
cluded are 3 dogs treated with
cisplatin perfusion, followed by
resection of the osteosarcoma

39
Cisplatin perfusion for canine osteosarcoma
In a study of cisplatin pharmacokinetics during HILP in humans with recurrent
melanoma, cisplatin levels were 10-20 times higher than those found in systemic
treatment and about 5 times higher than those found in intra-arterial infusion.27 During
these perfusions, high total platinum concentrations in the limb were reached that
would be unacceptably toxic for systemic use. A substantial drug extraction occurred
with minimal leakage to the systemic circulation.
The aim of the present study was to investigate the short-term effect of HILP with
cisplatin in dogs with spontaneous osteosarcoma. All three parameters used to evaluate
the short-term effect showed a trend toward improvement. However, only the clinical
score reached statistical significance for the total group with 1.93 before perfusion,
2.42 (n.s.), 3.04 (p<0.001), and 3.18 (p<0.001) at 2, 6 and 12 weeks, respectively,
after perfusion. The mean radiological score was 2.24 and 2.38 at 2 and 6 weeks
after perfusion, i.e. 15 out of 24 (63%) dogs had an improved radiological picture 6
weeks after perfusion, compared with the picture before perfusion. The histological
results showed a moderate effect at 2 weeks (mean score 2.48) with a slightly lower
mean score at 6 weeks (2.14). This could be an indication that viable tumor cells are
growing out between 2 and 6 weeks after an initial favorable response to perfusion,
meaning that a limb salvage procedure should be planned 2 weeks after perfusion.
Surprisingly none of the dogs showed a complete histological response of the tumor
6 weeks after perfusion. Three dogs with total necrosis 2 weeks after perfusion, showed
viable tumor cells 6 weeks after perfusion. Sampling error could account for these
observations. Although high total platinum levels in the perfusate were reached, the
histological outcome were modest and comparable with those observed in the systemic
treatment of osteogenic sarcoma.
Although several authors report an enhanced toxicity of cisplatin combined with
hyperthermia,28,29 due to phenomena of enhanced blood flow, enhanced cellular drug
uptake, tissue extraction, DNA cross-linking and decreased DNA repair30-34 , no
additional therapeutic effect, according to the three parameters, could be demonstrated
by increasing the limb temperature by 1°C (group II). The mean clinical, radiological
and histological scores for both groups were comparable at 2 and 6 weeks. At 12
weeks however the second group deteriorated in clinical score significantly with
regard to the first group (p < 0.05). Elevated normal tissue damage, occurring at
higher perfusion temperatures could be a reasonable explanation for this observed
difference in clinical performance of the dogs.
Median survival time in our series for all dogs was 115 days, similar to survival
times in dogs that had amputation alone without any adjuvant chemotherapy.35 This
may not be a surprising, as it is estimated that 90 % of the dogs with osteosarcoma
already have micrometastatic disease predominantly in the lungs.36 An improvement

40
Chapter 2
of survival is only to be expected when the locoregional treatment is combined with
effective systemical therapy to eradicate micrometastatic disease. Mc Ewen et al.
improved the overall median survival time from 77 to 222 days (p<0.002) using
adjuvant treatment with liposome-encapsulated muramyl tripeptidephophatidyle-
thanolamine (liposome/MTP-PE) after amputation for osteosarcoma in dogs.36
Combining HILP for local treatment together with adjuvant liposome/MTP-PE as
the systemic component, may improve local control and increase disease free survival
in canine osteosarcoma.
The present study shows that a single HILP with cisplatin in dogs having extremity
osteosarcoma is feasible with acceptable locoregional toxicity, improved functional
outcome at 6 and 12 weeks and a steadily improving radiological picture. However,
the histological results were modest with none of the dogs showing a complete
response 6 weeks after perfusion. Results of recent publications and of our own
experience with a new perfusion modality, which combines tumor necrosis factor
(TNF), Interferon (IFN), and melphalan in patients with recurrent melanoma or soft
tissue sarcoma, are very promising.37,38 Since the endothelial cells are supposed to
play a key role in the working mechanism of TNF, osteosarcomas with a high extent
of tumor vessels, are of particular interest. Therefore the combination of TNF and
Interferon with cisplatin could theoretically induce more tumor necrosis in
osteosarcoma than could perfusion with cisplatin alone. A similar study designed to
investigate the additional effect of TNF with cisplatin in the treatment of canine
osteogenic sarcoma, is being initiated. If results are as good as they are in the treatment
of recurrent melanoma and soft tissue sarcoma a step forward could be made in the
locoregional treatment of osteosarcoma.
Conclusions
HILP with cisplatin is feasible in the local treatment of spontaneous osteosarcoma in
dogs with acceptable locoregional toxicity, improved functional outcome at 6 and 12
weeks, and a steadily improving radiologic picture. However the histological results
were modest with none of the dogs showing a complete response 6 weeks after
perfusion and no additional therapeutic effect, according to the three parameters,
could be demonstrated by increasing the perfusate temperature by 1°C. Therefore,
the search for the ideal perfusion agent with substantial contribution to the limb
sparing treatment in human osteosarcoma continues.

41
Cisplatin perfusion for canine osteosarcoma
References
1 Mc Kenna RJ, Schwinn CD, Soong KY, Higinbotham NL. Sarcomata of the
osteogenic series: An analysis of 552 cases. J Bone Joint Surg 1966; 48A: 1-26.
2 Friedman MA, Carter SK. The therapy of osteogenic sarcoma: Current status and
thoughts for the future. J Surg Oncol 1972; 4: 482-510.
3 Rosen G, Tan C, Sanmaneechai A, et al. The rationale for multiple drug chemotherapy
in the treatment of osteogenic sarcoma. Cancer 1975; 35: 936-945.
4 Eilber F, Giuliano A, Eckardt J, et al. Adjuvant chemotherapy for osteosarcoma: A
randomized prospective trial. J Clin Oncol 1987; 5: 21-26.
5 Link MP, Goorin AM, Miser AW, et al. The effect of adjuvant chemotherapy on
relapse free survival in patient with osteosarcoma of an extremity. N Eng J Med
1986; 314: 1600-1606.
6 Meyer WH, Malawer MM. Osteosarcoma. Clinical features and evolving surgical
and chemotherapeutic strategies. Pediatr Clin North Am 1991; 38: 317-348.
7 Winkler K, Beron G, Delling G, et al. Neoadjuvant chemotherapy of osteosarcoma:
results of a randomized trial (COSS-82) with salvage chemotherapy based on
histological tumor response. J Clin Oncol 1988; 6: 329-337.
8 Hoekstra HJ, Naujocks T, Schraffordt Koops H, et al. Continuous leakage monitoring
during hyperthermic isolated regional perfusion of the lower limb: techniques and
results. Reg Cancer Treat 1992; 4: 301-304.
9 Klein ES, Ben-Ari GY. Isolation perfusion with cisplatin for malignant melanoma
of the limbs. Cancer 1987; 59: 1068-1071.
10 Roseman JM, Tench D, Bryant LR. The safe use of cisplatin in hyperthermic isolated
limb perfusion systems. Cancer 1985; 56: 742-744.
11 Hoekstra HJ, Schraffordt Koops H, De Vries EGE, Van Weerden TW, Oldhoff J.
Toxicity of hyperthermic isolated limb perfusion with cisplatin for recurrent
melanoma of the lower extremity after previous perfusion treatment. Cancer 1993;
72: 1224-1229.
13 Brodey RS. The use of naturally occurring cancer in domestic animals for research
into human cancer: General considerations and a review of canine skeletal
osteosarcoma. Yale J Biol Med 1979; 52: 345-361.
14 Wolke RE, Nielsen SE. Site incidence of canine osteosarcoma. J Small Anim Pract
1966; 7: 489-492.
15 Thrall DE, Page RL, Dewhirst MW, et al. Temperature measurements in normal
and tumor tissue in dogs undergoinig whole body hyperthermia. Cancer Res 1986;
46: 6229-6235.
16 De Vries J, Hartel RM, Schraffordt Koops H, Oosterhuis JW. Dosage of cisplatin in
hyperthermic isolated regional perfusion. Surg Res Commun 1987; 2: 107-112.
17 Den Heeten GJ, Thijn CJ, Kamps WA, et al. The effect of chemotherapy on
osteosarcoma of the extremities as apparent from conventional roentgenograms.
Pediatr Radiol 1986; 16: 407-411.
18 Smith J, Heelan RT, Huvos AG, et al. Radiographic changes in primary osteogenic
sarcoma following intensive chemotherapy. Radiology 1982; 143: 355-360.
19 Coombs R, Halliday K. Biopsy techniques. In: Coombs R, Friedlaender G, eds.
Bone tumor management. Cornwall, Great Britain: Robert Hartnoll Ltd. 1987; 1
edn. 81-87.

42
Chapter 2
20 Huvos AG, Rosen G, Marcove RC. Primary osteogenic sarcoma. Pathologic aspects
in 20 patients after treatment with chemotherapy, en bloc resection and prosthetic
replacement. Arch Pathol Lab Med 1977; 101: 14-18.
21 Kaplan EL, Meier P. Nonparametric estimates from incomplete observations. J Am
Stat Assoc 1958; 53: 457-481.
22 Baum E, Greenberg L, Gaynon P, Krivit W, Hammond D. Use of cisplatinum
diammine dichloride (CPDD) in osteogenic sarcoma (OS) in children.
Proc.Am.Assoc.Cancer Res.and ASCO 1978; 19: 385 (Abstract).
23 Ochs JJ, Freeman AI, Douglass HO, et al. Cis-dichloro-diammine platinum (II) in
advanced osteogenic sarcoma. Cancer Treat Rep 1978; 62: 239-245.
24 Powers BE, Withrow SJ, Thrall DE, et al. Percent tumor necrosis as predictor of
treatment response in canine osteosarcoma. Cancer 1991; 67: 126-134.
25 Jaffe N, Knapp J, Chuang VP, et al. Osteosarcoma: Intraarterial treatment of the
primary tumor with cis-diamminodichloro-platinum (CDP): angiographic, pathologic
and pharmacologic studies. Cancer 1983; 51: 402-407.
26 Wile AG, Kar R, Cohen RA, Jakowatz JG, Opfell RW. The pharmacokinetics of
cisplatin in experimental regional chemotherapy. Cancer 1987; 59: 695-700.
27 Guchelaar HJ, Hoekstra HJ, De Vries EGE, et al. Cisplatin and platinum
pharmacokinetics during hyperthermic isolated limb perfusion for human tumors of
the extremities. Br J Cancer 1992; 65: 898-902.
28 Alberts DS, Peng YM, Chen G. Therapeutic synergism of hyperthermia and cisplatin
in a mouse tumor model. J Nat Cancer Inst 1980; 65: 455-460.
29 Fisher G, Hahn GM. Enhancement of cisplatin(II)diamine-chloride cytotoxicity by
hyperthermia. Natl Cancer Inst Monogr 1982; 61: 255-257.
30 Herman TS. Temperature dependence of adriamycin, cis-diammine-
dichloroplatinum, bleomycin and 1,3-bis-(2-chloroethyl)-1- nitrosurea cytotoxicity
in vitro. Cancer Res 1983; 43: 517-520.
31 Herman TS, Teicher BA, Chan V, Collins LS, Abrams MJ. Effect of heat on the
cytotoxicity and interaction with DNA of a series of platinum complexes. J Rad
Oncol Biol Phys 1989; 16: 443-449.
32 Meyn RG, Corry PM, Fletcher SE, Demetriades M. Thermal enhancement of DNA
damage in mammalian cells treated with cis-diamminedichloro-platinum(II). Cancer
Res 1980; 40: 1130-1139.
33 Riviere JE, Page RL, Dewhirst MW, Tyczkowska K, Thrall DE. The effect of
hyperthermia on cisplatin pharmacokinetics in normal dogs. Int J Hyperth 1986; 2:
351-358.
34 Wallner KE, Degregorio MW, Li GC. Hyperthermic potentation of cis-
diamminedichloroplatinum(II) cytotoxicity in chinese hamster ovary cells resistent
to the drug. Cancer Res 1986; 46: 6242-6245.
35 Thompson JP, Fugent MJ. Evaluation of survival times after limb amputation, with
and without subsequent administration of cisplatin, for treatment of appendicular
osteosarcoma in dogs: 30 cases (1979-1990). J Am Vet Med Assoc 1992; 200: 531-
533.
36 Mac Ewen EG, Kurzman JD, Rosenthal RC, et al. Therapy for osteosarcoma in
dogs with intravenous injection of liposome-encapsulated muramyl tripeptide. J
Nat Cancer Inst 1989; 81: 935-938.

43
Cisplatin perfusion for canine osteosarcoma
37 Lienard D, Ewalenko P, Delmotte JJ, Renard N, Lejeune FJ. High-dose recombinant
tumor necrosis factor alpha in combination with interferon gamma and melphalan
in isolation perfusion of the limbs for melanoma and sarcoma. J Clin Oncol 1992;
10: 52-60.
38 Eggermont AMM, Lienard D, Schraffordt Koops H, Van Geel AN, Hoekstra HJ,
Lejeune FJ. Limb salvage by high dose tumor necrosis factor alpha (TNF) , gamma-
interferon (IFN) and melphalan isolated limb perfusion (ILP) in patients with
irresectable soft tissue sarcomas. Proc.Am.Soc.Clin.Oncol. 1992; 11: 1444 (Abstract).

44

45
Robert J. van Ginkel 1
Charles L.H. van Berlo 1
Peter C. Baas 1
Heimen Schraffordt Koops 1
Ries van Groningen á Stuling 1
Jan Elstrodt 2
Harald J. Hoekstra 1
Department of Surgical Oncology1 and Central Animal Laboratory2, University
Hospital Groningen, The Netherlands.
Sarcoma 1999; 3: 89-94.
Hyperthermic isolated limb perfusion with TNF and
cisplatin in the treatment of osteosarcoma of the
extremities: A feasibility study in healthy dogs

46
Chapter 3
Abstract
The feasibility of hyperthermic isolated limb perfusion (HILP) with tumor necrosis
factor-α (TNF) and cisplatin for the management of osteosarcoma was studied in the
canine model. During seven perfusions in six healthy mongrel dogs (weight 32±2 kg)
the technical aspects of HILP under mild hyperthermia (39-40o) were studied. In five
experiments HILP was performed with TNF alone (0.5 mg/L extremity volume), and
in two experiments TNF was combined with cisplatin (25 mg/L extremity volume).
During the perfusions physiological parameters were monitored and TNF and total
cisplatin concentrations were determined. Perfusion conditions (pH, PCO2, PO
2, flow
and pressure) remained within physiological ranges. Three dogs died within 24 hours
despite a sublethal systemical concentration of TNF that leaked from the perfusion
circuit. Three dogs were terminated; one dog after the second experiment in accor-
dance with Dutch ethical rules; one dog because it showed an invagination of the
small bowel resulting in an ileus; one dog because of necrosis of the perfused limb.
This feasibility study in healthy dogs demonstrated that HILP with TNF and cisplatin
was associated with a high mortality rate and therefore does not allow us to treat
dogs with spontaneous osteosarcoma with TNF and cisplatin HILP. Therefore, an
alternative model should be used in the search for the ideal combination of perfusion
agents for the limb sparing treatment in human osteosarcoma.
Introduction
Osteosarcoma is the most frequent primary malignant bone tumor in humans. Until
the 1970s the most common approach to the management of localized osteosarcoma
was surgical resection, amputation or radiation therapy.1 During the last decades a
definite role for neoadjuvant high dose methotrexate and cisplatin based
polychemotherapy was established.1-4 The potential local tumor effect of systemically
administered cisplatin, however, is limited due to the nephrotoxicity and ototoxicity
of cisplatin. Therefore an attempt was made to increase the local effect of cisplatin
without increasing systemic toxicity by using hyperthermic isolated regional limb
perfusion (HILP) with cisplatin in dogs with spontaneous osteosarcoma.5 These
studies showed an acceptable locoregional toxicity, improved functional outcome at
6 and 12 weeks, and a steadily improving radiological picture. However, the
histological results were modest, with none of the dogs showing a complete response
at 6 weeks after perfusion. The same experience was found in patients with sarcomas
of soft tissue and bone treated with cisplatin HILP.6 Results of recent publications
and of our own experience with a new perfusion modality, which combines tumor
necrosis factor-α (TNF) and melphalan in patients with recurrent melanoma or soft
tissue sarcoma, are very promising.7,8 However, in 6 of 8 evaluable patients with

47
Limb perfusion with TNF and cisplatin in healthy dogs
unresectable osteosarcoma of the lower limb treated with TNF and melphalan HILP,
histological evaluation revealed moderate results with ≥ 80% necrosis in 3 patients,
50%-60% necrosis in 2 patients and < 50% necrosis in one patient. After TNF and
melphalan HILP, limb sparing surgery was possible in 6 patients.9 As cisplatin is one
of the most active chemotherapeutics in the treatment of osteosarcoma, it seems
worthwhile to investigate the results of HILP with TNF and cisplatin. With the high
frequency of occurrence in dogs, canine osteosarcoma is a useful model for evaluation
of new treatment regimens in humans as rapid case accrual and rapid time to reach
measurable end points are possible.10 The canine osteosarcoma therefore appears to
be a valid model for studying the potential treatment of HILP with TNF and cisplatin
in the local treatment of osteosarcoma of the extremity in humans. To establish optimal
HILP conditions using TNF and cisplatin for local tumor control in dogs bearing
osteosarcoma, a feasibility study in healthy dogs was undertaken.
Materials and methods
Dogs
During 7 experiments in 6 healthy mongrel dogs with a mean average weight of 32 ±2 kg and a mean age of 6 ± 1 years different aspects of HILP with TNF and cisplatin
were studied. Preoperatively, all dogs were thoroughly clinically evaluated at the
Central Animal Facility of the University of Groningen. The study was approved by
the Animal Welfare Committee of the Faculty of Medicine of the Groningen
University.
Anesthetics
The dogs fastened for 12 hours and were anaesthetized with thiopental (30mg/kg
BW, i.v.)(Pentothal, Abbott, Amstelveen, The Netherlands) and after muscle relaxation
with pancuroniumbromide (0.08 mg/kg BW, i.v.) (Pavulon, Organon, Oss, The
Netherlands), the dogs were ventilated (Ohmeda Modulus 2) with a mixture of O2
and isoflurane. The oxygen concentration in the gas mixture was continuously
measured by means of an oxygen analyzer (Ohmeda Modulus 2) and minute volumes
( 4-6 L/min) were adjusted to maintain an end-expiratory CO2 concentration of 4-5%
(Siemens CO2 - analyzer 930). The dogs were placed in the supine position on a
heated mattress to maintain their normal body temperature of 38 0C.11 During the
operations all dogs were given about 2 L of glucose 5% through a cephalic or internal
jugular vein. Central arterial pressure was recorded as well as an ECG and diuresis.

48
Chapter 3
Operation and Perfusion Techniques
During anaesthesia the volume of the extremity was measured using Archimedes
rule (1.7-2 L). The iliac vessels were exposed under sterile conditions and collateral
vessels were clipped. Cannulas were inserted into the artery (Bardic, 14-18 F) and
vein ( Bardic, 14-18 F). Both cannulas were connected to an extracorporeal circuit
consisting of an occlusive roller pump, a cardiotomy reservoir and a bubble oxygenator
with heat-exchanger. A nylon tourniquet was placed around the base of the extremity
using, a pin in the bone and bandage around the middle to complete the isolation of
the limb from the systemic circulation. The perfusate consisted of 350 ml 5% dextran
40 in glucose 5% (Isodex, Pharmacia AB, Uppsala, Sweden), 250 ml red blood cells
(canine blood donors), 250 ml plasma, 30 ml sodiumbicarbonate 8.4% and 0.5 ml
5000 IU/ml heparin (Thromboliquine, Organon B.V., Oss, The Netherlands). The
mixture of oxygen, air and carbondioxide through the oxygenator was adjusted to
maintain the blood gas values within the physiological range and when necessary,
bicarbonate was added to adjust the pH value.
All perfusions were performed under mild hyperthermic conditions (39-400 C) and
optimal physiologic conditions.12,13 Thermistor probes (Electrolaboriet, Copenhagen,
Denmark) were inserted into the subcutaneous tissues and into a muscle of the thigh
just above the knee for continuous monitoring of the temperatures during perfusion.
In the first 5 experiments TNF was the sole perfusion agent, in the last 2 experiments
TNF was combined with cisplatin. The dosage of TNF (0.5 mg/L extremity volume)
(Boehringer, Ingelheim, Germany) was calculated not to exceed ten times acceptable
systemic levels (Systemic: 10 µg/kg bodyweight).14 The dosage of cisplatin (25 mg/
L extremity volume) (Platinol 0.5 mg/ml, Bristol Myers Squibb, Weesp, The
Netherlands) used in the perfusion had been established in a previous study and was
based on a maximum tolerable dose of 30 mg/ L extremity volume.15 Cisplatin was
added to the circulated perfusate in 10 minutes. During perfusion, serum TNF and
total cisplatin levels were determined in the regional and systemic circulation at 0, 5,
15, 30, 45, 60, 75 and 90 minutes by ELISA and flameless atomic absorption
spectophotometry (FAAS), respectively. The perfusion time was 1 hour, followed by
washout of the extremity with 3L of Isodex. Tourniquet, cannulas and clips were
then removed and the incisions in the vessels repaired. Protamine hydrochloride
(Hoffman La Roche, Mijdrecht, The Netherlands) was administered, to neutralize
heparin, in a ratio of 1:1 to the initial dose of heparin. All dogs were closely observed
during at least 24 hours. No anti-inflammatory or analgesic drugs were administered
during follow-up. All dogs were followed for local and systemic side effects of TNF
and cisplatin perfusion, as well as survival.

49
Limb perfusion with TNF and cisplatin in healthy dogs
Results
Table 1 shows the characteristics of the 7 experiments in 6 dogs. During the
experiments conditions for perfusions (pH, PCO2, PO
2) were kept within the
physiological ranges as in human perfusions. Figure 1 shows the flow, blood pressure,
perfusion pressures, weight gain or loss of the extra corporeal circuit and temperature
during 60 minutes of perfusion in the 7 experiments. In the first 5 experiments only
TNF was administered to the perfusion circuit. In the last two experiments cisplatin
was added. Figure 2 illustrates the TNF concentrations (mean ± SEM) in the perfused
limb as well as in the systemic circulation of the dog during perfusion and afterwards.
Peak TNF concentrations in the perfused limb were 650 ± 158 ng/ml and in the
systemic circulation of the dog 37 ± 15 ng/ml. The peak systemic concentrations in
the dog were in the same range as those of in TNF and melphalan HILP used in the
treatment of humans at our institute.16 Figure 3 shows the measured total cisplatin
values in the last two experiments. During the experiments we were not able to perform
any leakage monitoring by means of radionuclear detection techniques which are
used in the clinical perfusion setting. Therefore leakage was calculated afterwards
according to Stehlin with the amount of blood in the dogs estimated at 69 ml/kg
bodyweight.17 Calculated leakage values are summarized in Table 1.
Three dogs died within 24 hours: the first two during the TNF experiment, the third
after TNF and cisplatin perfusion. Postmortem examination of these animals did not
provide any macroscopic or microscopic evidence to explane the cause of death.
Three dogs were terminated; two due to treatment complications. One dog showed
an invagination of the small bowel resulting in an ileus and another was terminated 1
Table 1 Characteristics for the seven experiments in six dogs
Exp. Body Limb TNF Cisplatin Leakage Limb Follow-up
Nr. weight volume dose dose toxicity
(kg) (L) (mg) (mg) (%)
1 35 2.7 1.3 0 8.7 II Dead < 24 h
2 31.5 1.4 0.6 0 0.3 II Dead < 24 h
3 26.5 2.3 1.15 0 5.1 II Ileus, terminated < 1 wk
4 33.5 2.3 1.15 0 4.9 I Alive, experiment 1
5 31 1.9 1 0 6.1 n.a. Terminated, experiment 2
6 29.5 2.0 1 50 33.0 V Necrotic limb, terminated<1wk
7 28.5 1.8 0.8 50 10.8 II Dead < 24 h
Exp. Nr. = experiment number; n.a. = not applicable, dog 4 underwent 2 experiments; limb toxicity
according to Wieberdink 26; Grade I, no reaction, objectively and subjectively; Grade II, slight erythema,
edema or loss of sensation; Grade III, considerable erythema or edema with some blistering, slight
functional disturbances; Grade IV, extreme epidermolysis and/or obvious damage to the deep tissues
causing definite functional disturbances; Grade V, reaction that might necessitate amputation

50
Chapter 3
Fig. 1 Perfusion characteristics (flow, systemic blood pressure of the dog (BP); arterial
catheter pressure (P-art); venous catheter pressure (P-ven); extra corporeal circulation (ECC)
weight gain (+) or loss (-) and temperature of the perfused limb (oC)) in time during 60 min-
utes of perfusion in 7 experiments

51
Limb perfusion with TNF and cisplatin in healthy dogs
week after TNF and cisplatin perfusion because of necrosis of the perfused limb. The
third dog was terminated after the second experiment in accordance with the Dutch
ethical rules.
Discussion
In the treatment of osteogenic sarcoma a distinction can be made between systemic
therapy and locoregional treatment. High dose methotrexate based systemic
chemotherapy is primarily administered in order to eradicate possible micrometastatic
disease and its use was a major breakthrough in the clinical treatment of osteosarcomas
in the 1970s.1,2 Today about 60% of patients with resectable primary tumors and no
metastases at the time of the initial diagnosis will be cured.1 The primary objective in
locoregional treatment is to prevent local recurrence and allow limb salvage procedures
in an attempt to preserve limb function. New surgical techniques and the development
of endoprosthetic materials, coupled with the systemic neoadjuvant chemotherapy,
Fig. 2 TNF levels in ng/ml (mean
± SEM) as obtained by human TNF
ELISA in the perfused limb, as well
as in the systemic circulation of the
dog
Fig. 3 Total cisplatin levels (tPt) in
mg/L (mean ± SEM) as obtained
by flameless atomic absorption
spectrophotometry in the perfused
limb, as well as in the systemic cir-
culation of the dog

52
Chapter 3
have offered less radical surgery for 40-80% of patients with osteosarcoma since the
1980s.1,18 Procedures that increase tumor necrosis of the primary tumor, with reduction
of viable tumor cells and tumor volume, could contribute to limb preservation
strategies. Since its first use, cisplatin has been one of the most effective
chemotherapeutic agents and has been incorporated in most systemic treatment
regimens for osteosarcoma. A recent attempt to overcome its nephrotoxic and ototoxic
limitations by administering cisplatin in HILP in the treatment of spontaneous canine
osteosarcoma was histologically modest.5 Promising results of recent publications
and our own experience with a new combination perfusion modality (TNF and
melphalan) for recurrent melanoma or soft tissue sarcoma, but moderate histological
results in patients with osteosarcoma, prompted us to investigate the combination of
TNF and cisplatin in HILP for osteosarcoma.7-9 Since the endothelial cells are
supposed to play a key role in the working mechanism of TNF, osteosarcomas with
a high extent of tumor vessels, are of particular interest.
Before application of TNF and cisplatin HILP in humans and client owned
osteosarcoma bearing dogs, the present feasibility study was performed in normal
healthy dogs. Despite sufficient experience in HILP in dogs as well as in humans, an
unexpected high mortality rate was encountered. Although there was no mortality
related to the operation, 3 dogs died within 24 hours after perfusion (50%). This
direct postoperative mortality could not be explained by a surplus of systemical
leakage of TNF. In the experiment, thedog with the highest leakage and, as a
consequence the highest systemical TNF concentrations, survived immediately
postoperatively, and the dog with the lowest leakage (lowest systemical TNF
concentrations) died within 24 hours after perfusion. No correlation between leakage
and mortality rate could be established. Maximal leakage encountered in these
experiments was 33%, this corresponds with 330 µg TNF given systemically per
dog; since the average dog weighs 33 kg, the dose of TNF that reaches the systemical
circulation of the dog is sublethal (10 µg/kg).14 Although only sublethal doses of
TNF leaked to the systemical circulation, the clinical picture resembled responses
observed in lethal doses (>100µg/kg), characterized by progressive hypotension, shock
and death within 24 hours.19 Due to the lack of facilities, we were not able to support
the dogs with intensive postoperative care, as is the case after human TNF HILP. In
part this could explain the observed direct postoperative mortality and supports the
need for intensive treatment after TNF HILP in the dog.
Three dogs survived the first days after perfusion, however, one dog developed an
ileus and was terminated within 1 week after perfusion. One dog that underwent two
experiments survived the first without morbid effects, but was terminated after the
second experiment according to the Dutch ethical rules. Leg toxicity consisted in

53
Limb perfusion with TNF and cisplatin in healthy dogs
slight erythema and edema in all dogs except one in the cisplatin treated group. In
this dog, necrosis of the perfused limb was encountered, necessitating termination.
We have never observed necrosis of the perfused limb with the cisplatin dose used
(25 mg/L extremity volume) in experiments were cisplatin was the sole perfusion
agent.15 This observation may indicate that TNF might enhance the effect of cisplatin
to the local tissues of the perfused limb. The in vitro anticancer potential, and
overcoming cisplatin resistance with the combination of TNF and cisplatin in different
cell lines, has been established by others.20-22 Buell et al, demonstrated an increased
cellular cisplatin accumulation and DNA adduct formation as the possible cellular
basis for the augmented cisplatin cytotoxicity in the presence of TNF and
hyperthermia.23 Recently, Anda et al demonstrated that TNF selectively promoted
the in vitro permeability of the blood-brain barrier to CDDP without disrupting the
tight junctions.24 An improved penetration of cisplatin in the interstitial space due to
a higher permeability of the vascular wall, combined with an increased cellular
cisplatin accumulation and DNA adduct formation, could explain the observed
necrosis of the limb in this in vivo model with the cisplatin dose used, which was
previously non-toxic.
The observed mortality and morbidity that we encountered in this canine study was
in similar to the experience of Withrow and colleagues (unpublished observations).
The present results in normal elderly mongrel dogs indicate that treatment of dogs
with spontaneous osteosarcoma using TNF and cisplatin HILP is not appropriate.
Future research could focus on postoperative monitoring and care in dogs after TNF
HILP; perhaps a better alternative for testing the effect of TNF with cisplatin HILP,
is the use of the rat osteosarcoma model described by Manusama et al.,25 since rats
are much less susceptible to TNF than dogs.

54
Chapter 3
References
1 Ham SJ, Schraffordt Koops H, van der Graaf WT, et al. Historical, current and
future aspects of osteosarcoma treatment. Eur J Surg Oncol 1998; 24: 584-600.
2 Rosen G, Tan C, Sanmaneechai A, et al. The rationale for multiple drug chemotherapy
in the treatment of osteogenic sarcoma. Cancer 1975; 35: 936-945.
3 Link MP, Goorin AM, Miser AW, et al. The effect of adjuvant chemotherapy on
relapse free survival in patient with osteosarcoma of an extremity. N Eng J Med
1986; 314: 1600-1606.
4 Eilber F, Giuliano A, Eckardt J, et al. Adjuvant chemotherapy for osteosarcoma: A
randomized prospective trial. J Clin Oncol 1987; 5: 21-26.
5 van Ginkel RJ, Hoekstra HJ, Meutstege FJ, et al. Hyperthermic isolated regional
perfusion with cisplatin in the local treatment of spontaneous canine osteosarcoma:
assessment of short-term effects. J Surg Oncol 1995; 59: 169-176.
6 van Ginkel RJ, Schraffordt Koops H, de Vries EG, et al. Hyperthermic isolated limb
perfusion with cisplatin in four patients with sarcomas of soft tissue and bone. Eur
J Surg Oncol 1996; 22: 528-531.
7 Lienard D, Ewalenko P, Delmotte JJ, Renard N, Lejeune FJ. High-dose recombinant
tumor necrosis factor alpha in combination with interferon gamma and melphalan
in isolation perfusion of the limbs for melanoma and sarcoma. J Clin Oncol 1992;
10: 52-60.
8 Eggermont AMM, Schraffordt Koops H, Lienard D, et al. Isolated limb perfusion
with high-dose tumor necrosis factor-alfa in combination with interferon-gamma
and melphalan for nonresectable extremity soft tissue sarcomas: a multicenter trial.
J Clin Oncol 1996; 14: 2653-2665.
9 Bickels J, Manusama ER, Gutman M, et al. Isolated limb perfusion with tumor
necrosis factor alpha and melphalan for unresectable bone sarcomas of the lower
extremity. In: Manusama ER, ed. TNF-based isolated limb perfusion in the rat. The
Hague: Pasmans 1998; 1 edn. 105-117.
10 Withrow SJ, Powers BE, Straw RC, Wilkins RM. Comparative aspects of
osteosarcoma. Dog versus man. Clin Orthop 1991; 159-168.
11 Thrall DE, Page RL, Dewhirst MW, et al. Temperature measurements in normal
and tumor tissue in dogs undergoinig whole body hyperthermia. Cancer Res 1986;
46: 6229-6235.
12 Fontijne WP, Mook PH, Elstrodt JM, et al. Isolated hindlimb perfusion in dogs: the
effect of perfusion pressures on the oxygen supply (ptO2 histogram) to the skeletal
muscle. Surgery 1985; 97: 278-284.
13 Fontijne WP, De Vries J, Mook PH, et al. Improved tissue perfusion during pressure
regulated hyperthermic regional isolated perfusion in dogs. J Surg Oncol 1984; 26:
69-76.
14 Tracey KJ, Lowry SF, Fahey TJ3, et al. Cachectin/tumor necrosis factor induces
lethal shock and stress hormone responses in the dog. Surg Gynecol Obstet 1987;
164: 415-422.
15 De Vries J, Hartel RM, Schraffordt Koops H, Oosterhuis JW. Dosage of cisplatin in
hyperthermic isolated regional perfusion. Surg Res Commun 1987; 2: 107-112.

55
Limb perfusion with TNF and cisplatin in healthy dogs
16 Zwaveling JH, Maring JK, Clarke FL, et al. High plasma tumor necrosis factor
(TNF)-alpha concentrations and a sepsis-like syndrome in patients undergoing
hyperthermic isolated limb perfusion with recombinant TNF-alpha, interferon-
gamma, and melphalan. Crit Care Med 1996; 24: 765-770.
17 Stehlin JS, Clark RL, White EC, et al. The leakage factor in regional perfusion with
chemotherapeutic agents. A M A Arch Surg 1960; 80: 934-945.
18 Meyer WH, Malawer MM. Osteosarcoma. Clinical features and evolving surgical
and chemotherapeutic strategies. Pediatr Clin North Am 1991; 38: 317-348.
19 Eichenholz PW, Eichacker PQ, Hoffman WD, et al. Tumor necrosis factor challenges
in canines: patterns of cardiovascular dysfunction. Am J Physiol 1992; 263: H668-
75.
20 Mutch DG, Powell CB, Kao MS, Collins JL. In vitro analysis of the anticancer
potential of tumor necrosis factor in combination with cisplatin. Gynecol Oncol
1989; 34: 328-333.
21 Mizutani Y, Bonavida B. Overcoming cis-diamminedichloroplatinum (II) resistance
of human ovarian tumor cells by combination treatment with cis-
diamminedichloroplatinum (II) and tumor necrosis factor-alpha. Cancer 1993; 72:
809-818.
22 Sleijfer S, Le TK, de Jong S, et al. Combined cytotoxic effects of tumor necrosis
factor-alpha with various cytotoxic agents in tumor cell lines that are drug resistant
due to mutated p53. J Immunother 1999; 22: 48-53.
23 Buell JF, Reed E, Lee KB, et al. Synergistic effect and possible mechanisms of
tumor necrosis factor and cisplatin cytotoxicity under moderate hyperthermia against
gastric cancer cells. Ann Surg Oncol 1997; 4: 141-148.
24 Anda T, Yamashita H, Khalid H, et al. Effect of tumor necrosis factor-alpha on the
permeability of bovine brain microvessel endothelial cell monolayers. Neurol Res
1997; 19: 369-376.
25 Manusama ER, Stavast J, Durante NM, Marquet RL, Eggermont AMM. Isolated
limb perfusion with TNF alpha and melphalan in a rat osteosarcoma model: a new
anti-tumor approach. Eur J Surg Oncol 1996; 22: 152-157.
26 Wieberdink J, Benckhuysen C, Braat RP, Van Slooten EA, Olthuis GAA. Dosimetry
in isolation perfusion of the limb by assessment of perfused tissue volume and grading
of toxic tissue reactions. Eur J Cancer Clin Oncol 1982; 18: 905-910.

56

57
Robert J. van Ginkel1
Heimen Schraffordt Koops1
Elisabeth G.E. de Vries2
Willemina M. Molenaar3
Donald R.A. Uges4
Harald J. Hoekstra1
Departments of Surgical Oncology1, Medical Oncology2, Pathology3, and
Pharmacy4 University Hospital Groningen, Groningen, The Netherlands.
European Journal of Surgical Oncology 1996; 22: 528-531.
Hyperthermic isolated limb perfusion with cisplatin
in four patients with sarcomas of soft tissue and
bone

58
Chapter 4
Abstract
The value of hyperthermic isolated limb perfusion (HILP) with cisplatin in the
management of locally advanced soft tissue sarcomas or metastatic bone sarcoma
was studied. Four patients were treated with HILP under mild hyperthermia
(39-40 °C) with 20-30 mg cisplatin / L perfused limb volume. Toxicity in the perfused
limbs was moderate, and the erythema and edema that occurred resolved
spontaneously within 7-14 days as did the slight motor and sensory neuropathy over
a longer period of time. Clinically, a reduction of pain was observed in all patients.
Two weeks after perfusion, tumor biopsies were taken to evaluate tumor response.
Two patients showed a pathological complete response, one patient showed >90%
necrosis and one patient showed no response. Currently patients are treated with
tumor necrosis factor and melphalan as perfusion agents. The above mentioned results
make the combination of tumor necrosis factor with cisplatin in the isolated limb
perfusion setting an interesting option.
Introduction
Malignant bone and soft tissue sarcomas are a heterogeneous group of lesions, which
all arise from tissue of mesenchymal origin. With an incidence of 3 per 100000, and
given that somatic soft tissue and skeleton comprise more than 75 % of the average
body weight, these cancers are rare. Most sarcomas of soft tissue and bone originate
in the extremities and are often quite large at the time of diagnosis. Limb saving
treatment of extremity sarcomas of soft tissue and bone is a multidisciplinary matter
and has avoided ablative surgical procedures in the majority of patients.1,2 Apart
from locoregional treatments, systemic adjuvant chemotherapy is now well established
for the treatment of osteosarcoma3, whereas in soft tissue sarcomas it is still a subject
of investigation.4 The main goal of the systemic treatment is the eradication of possible
micrometastatic disease with a possible favourable response on the primary tumor.
With hyperthermic isolated limb perfusion (HILP) it is possible to obtain a higher
local chemotherapy concentration in the perfused extremity than with systemically
administered chemotherapy.5 Cisplatin, discovered in 1965 by Rosenberg et al.6 is
one of the most active chemotherapeutic agents and it has been postulated that a high
dose of cisplatin could create significant necrosis of the primary tumor. Before
introducing cisplatin perfusions in the clinical treatment for sarcomas of soft tissue
and bone, a dose escalating and feasibility study in spontaneous canine osteogenic
sarcoma showed a maximum tolerable dose of 30 mg cisplatin / L extremity volume,
with improvements in clinical and X-ray parameters after treatment.7,8 The aim of
the present study was to investigate the feasibility and efficacy of HILP with cisplatin
in the locoregional tumor control of locally advanced soft tissue sarcomas or metastatic

59
Cisplatin perfusion in patients with sarcomas
bone sarcomas.
Patients and methods
Patients eligible for the study were suffering from histologically proven locally
advanced extremity sarcomas of soft tissue or bone. The primary tumor was locally
not resectable locally except when an amputation of the affected limb was performed.
Patients were treated with the intent of preserving the affected extremity.
Before perfusion the renal function of all patients was normal. Patients were
prehydrated with 2.5 L normal saline 12 hours preoperatively, and hydration was
maintained during the first 5 postoperative days, in order to protect against
nephrotoxicity. The perfusion technique employed is based on the technique developed
by Creech and Krementz9 and was performed during 60 min under mild hyperthermia
(39-40oC) and physiologically optimal conditions.10 Cisplatin (Platinol 0.5 mg/ml,
Bristol Myers SAE, Barcelona, Spain) was added to the perfusate over 10 min. In
this study the cisplatin dose, administered as part of a phase I-II dose finding study,
varied from 20-30 mg / L perfused limb volume.11 Leakage of cisplatin from the
perfused limb to the systemic circulation was checked by an isotope scanner placed
over the heart using 131I-albumin in the perfusate.12
All patients were followed up clinically by physical examination, chest X-rays and
routine blood chemistry for treatment related morbidity. In patients with a sarcoma
of bone, response to perfusion was scored on conventional X-rays in two directions.
Preperfusion X-rays were compared with 6 weeks postperfusion X-rays. Regression
of the tumor was defined as a decrease in tumor volume, increased ossification of
intra-osseous tumor osteoid, periosteal new bone, and soft tissue margins more densely
ossified, resulting in a more benign appearance of the tumor. One week after perfusion
an electromyogram was performed to investigate nerve toxicity of the cisplatin
perfusion. The local perfusion toxicity was graded according to the criteria described
by Wieberdink et al.11
Two weeks after perfusion, biopsies of the tumor were taken in three directions with
a 3.5 mm diameter Coombs bone biopsy system13 to evaluate the response of the
tumor to the perfusion treatment. The biopsies were histologically scored: little or no
effect of chemotherapy noted (score I), a partial response to chemotherapy with 50%
- 90% tumor necrosis noted and attributable to chemotherapy (score II), > 90% tumor
necrosis (score III), no viable tumor cells noted in any of the histological sections
(score IV).
Before and during perfusion, 10 ml perfusate samples were collected at 10 min
intervals to determine total platinum (tPt) and ultrafiltrated platinum (fPt) levels as
previously published.14 The study was approved by the local Medical Ethical

60
Chapter 4
Committee of the Groningen University Hospital and all patients gave informed
consent.
Results
Four patients entered the study. Three patients presented with metastasized lower
extremity sarcoma of bone, in two patients the primary tumor concerned an
osteosarcoma and in one patient a malignant fibrous histiocytoma. Both osteosarcoma
patients had multiple lung metastases and the patient with the malignant fibrous
histiocytoma of bone had multiple skeletal metastases at time of diagnosis. The fourth
patient presented with a localised recurrent malignant fibrous histiocytoma of the
soft tissues. She had first been treated with local excision followed by radiotherapy
(Table 1). All primary tumors were localised in the lower extremity.
Characteristics of the perfusion and cisplatin dose used in each patient are summarized
in Table 2. No technical perfusion related problems were encountered. After perfusion,
the total serum proteins and albumin levels decreased in all patients. The mean total
serum proteins decreased from 73.7±0.5 to 46.7±4.8 g/L on the first postoperative
day, and mean serum albumin from 45.3±1.9 to 29.3±4.6 g/L (p<0.05 paired Student’s
t-test). Serum albumin was corrected postoperatively with intravenous albumin
administration.
The acute treatment related toxicity consisted of a local edema and erythema (Grade
II toxicity) in three patients, and one patient had a considerable edema and erythema
of the skin with some blistering (Grade III toxicity). The erythema and edema resolved
spontaneously within 7-14 days as did the slight motor and sensory neuropathy over
a longer period of time. All patients experienced pain relief after perfusion. The X-
rays of the first osteosarcoma patient showed regression of the tumor and more than
90% necrosis was found in the tumor biopsies 2 weeks after perfusion. In the second
osteosarcoma patient, a 5% leakage of albumin to the systemical circulation occurred.
After the treatment, the leaked cisplatin brought about a measurable reduction of the
pulmonary metastases before systemic treatment with cisplatin was started and caused
temporarily renal function disturbances. Notably, the primary tumor did not respond
to the perfusion in terms of the pathological evaluation. The X-rays could not be
properly scored in this patient due to bone formation after a pathological fracture.
Both osteosarcoma patients received systemic chemotherapy after cisplatin perfusion
because of metastatic disease at time of diagnosis. The patient with a malignant
fibrous histiocytoma of bone showed progression of the tumor on X-ray, however,
tumor biopsies showed a complete response. In none of these three patients was the
affected limb amputated, and all three patients died from distant metastatic disease
after 6, 12 and 7 months. After an initial complete response clinically and

61
Cisplatin perfusion in patients with sarcomas
pathologically, a recurrence was found in the patient with a malignant fibrous
histiocytoma of the soft tissues. Subsequently a lower leg amputation was performed
and this patient was alive without evidence of disease 36+ months after amputation.
Discussion
HILP was first used to treat patients with melanoma, and the drug employed was the
alkylating agent melphalan.9 Although the overall remission in melanoma patients is
80%, 60% of patients fail to achieve a complete response. Drugs which might be
more effective or less toxic than melphalan in the treatment of melanoma by HILP
have therefore been sought. The first report by Aigner et al15, indicated that cisplatin
might be an useful alternative to melphalan in the treatment of melanoma. Cisplatin
is a non-cell-cycle dependent drug, which forms DNA-crosslinks and inhibits DNA
synthesis.16 Klein and Ben-Ari17 experienced no serious toxicity after HILP with
cisplatin. In the present study toxicity was moderate. In a previous experience of
HILP with cisplatin however, we found an unacceptable treatment related neuropathy.18
With cisplatin dosages in the same range as in the present study, the only difference
from this study was that six of seven patients with recurrent extremity melanoma
were treated with one or more melphalan perfusions with or without dactinomycin
prior to the cisplatin perfusion.
The pharmacokinetic data from the patients in this study showed extremely high
perfusate levels of Pt, up to 30 times higher than systemic levels which remained
acceptably low.14 Given that effective intra-arterial and systemic levels of Pt are in
the range of 5.5 mg/L, HILP produced 2 to 10 times higher levels. The pharmacokinetic
data further indicated that HILP with cisplatin produced high levels of Pt in the
tumor and surrounding muscle and fat14, which may harbour malignant cells that
later result in local recurrences.
Both malignant fibrous histiocytomas responded with total necrosis in the biopsy
material. Recently we showed that malignant fibrous histiocytoma of bone is a very
Table 1 Patients characteristics
No. Age Sex Primary tumor Metastatic disease
1 21 M Osteosarcoma Lungs
2 10 F Osteosarcoma Lungs
3 70 M Malignant fibrous histiocytoma of bone Bone
4 58 F Recurrent malignant fibrous histiocytoma No
of soft tissues

62
Chapter 4
Ta
ble
2P
erfu
sio
n c
har
acte
rist
ics,
cis
pla
tin
do
sag
e, t
ox
icit
y a
nd
fo
llo
w-u
p
No
Perf
usio
nL
imb
Cis
pla
tin
To
tal
Flo
wL
eakag
eL
ocal
EM
GP
ath
olo
gic
al
X-r
ay o
f tu
mo
rF
ollo
w u
p
typ
eV
olu
me
do
se
cis
pla
tin
(ml/m
in)
(%)
To
xic
ity
sco
re 2
weeks
6 w
eeks a
fter
(mo
nth
s)
(mg
/L v
ol.)
do
se
gra
de
aft
er
HIL
PH
ILP
(mg
)
1Ilia
cal
13.0
20
260
750
4.2
IIS
light
moto
rIII
Regre
ssio
nD
OD
6
ne
uro
pa
thy
2Ilia
cal
5.0
25
125
520
5.0
IIN
orm
al
IN
ot evalu
able
DO
D 1
2
due to fra
ctu
re
3Ilia
cal
11.0
25
275
450
1.4
III
Norm
al
IVP
rogre
ssio
nD
OD
7
4P
oplit
eal
3.3
30
100
800
1.5
IIS
light
sensory
IVN
ot
perf
orm
ed
NE
D 3
6
ne
uro
pa
thy
DO
D =
dea
d o
f dis
ease
; N
ED
= n
o e
vid
ence
of
dis
ease
; E
MG
= e
lect
rom
yogra
m
Loca
l per
fusi
on t
oxic
ity a
ccord
ing t
o W
ieber
din
k11:
Gra
de
I, n
o r
eact
ion, obje
ctiv
ely a
nd s
ubje
ctiv
ely;
Gra
de
II, sl
ight
eryth
ema,
oed
ema
or
loss
of
sensa
tion;
Gra
de
III,
consi
der
able
ery
them
a or
oed
ema
wit
h s
om
e bli
ster
ing, sl
ight
funct
ional
dis
turb
ance
s; G
rade
IV, ex
trem
e ep
ider
moly
sis
and/o
r obvio
us
dam
age
to
the
dee
p t
issu
es c
ausi
ng d
efin
ite
funct
ional
dis
turb
ance
s; G
rade
V,
reac
tion t
hat
mig
ht
nec
essi
tate
am
puta
tion

63
Cisplatin perfusion in patients with sarcomas
chemosensitive tumor.19 The malignant fibrous histiocytoma of soft tissue in the
present study however, recurred after 1 month. Fletcher et al. also reported a high
local recurrence rate of 66% (2 of 3 patients) in cisplatin perfusions for recurrent
malignant fibrous histiocytoma, indicating the difficulty of controlling local
recurrences of malignant fibrous histiocytoma with cisplatin perfusion.20
One osteosarcoma patient in the present study reacted with >90% necrosis of the
tumor, and in one patient the tumor showed no response after perfusion. These
moderate histological results in osteosarcomas are in accordance with our histological
data in canine experiments.8 The reason for this wide variation in response may be
exists in the sensitivity of the osteosarcoma cells, or that the pH changes in the tumor
occur during HILP, resulting in a less active form of cisplatin.16,21 Vaglini et al.22
found more favourable results with 95-100% necrosis of the tumor in eight of 11
evaluable osteosarcoma patients, 60-70% necrosis in two patients and 40% necrosis
in one patient after HILP with cisplatin combined with intra-arterial infusion of
cisplatin and systemic high-dose methotrexate.22. HILP with cisplatin was well
tolerated. The only significant complication was an extensive edema of the extremity
that spontaneously resolved in 2-3 weeks. Clinically, they observed a significant
reduction of pain, macroscopic reduction of tumor diameter, functional improvement
and rearrangement of the bone on the X-ray.
In the present study, no limb-salvage procedures were performed because of rapid
progression of systemic disease. In one osteosarcoma patient with a 5 % albumin
leakage, the accordingly leaked Pt brought about a measurable reduction of the
pulmonary metastasis, although the primary tumor did not respond. Di Filippo
demonstrated a systemical peak of Pt 3 hours after HILP due to the release of bound
Pt. Although this was encouraging, since a prolonged presence of Pt in the perfused
limb may contribute to lower recurrence rates, this indicated the need for adequate
and prolonged hyperhydration therapy after HILP with cisplatin, in order to prevend
nephro- and ototoxicity.
Following the treatment of the four patients described in this study, the Groningen
University Hospital now participates in a trial with a new perfusion modality, which
combines melphalan with biological response modifiers such as tumor necrosis factor
and interferon.23,24 As the endothelial cells are the main target cells of tumor necrosis
factor in these new perfusion schedules, treatment with this modality of sarcomas of
soft tissue and bone with a high extent of tumor vessels are of particular interest. A
trial which combines tumor necrosis factor with cisplatin as perfusion agents in the
treatment of sarcomas of soft tissue and bone could be clinically important.

64
Chapter 4
References
1. Suit HD. Local control and patient survival. Int J Radiat Oncol Biol Phys 1992; 23:
653-60.
2. Sadoski C, Suit HD, Rosenberg A, et al. Preoperative radiation, surgical margins,
and local control of extremity sarcomas of soft tissues. J Surg Oncol 1993; 52: 223-
30.
3. Eilber F, Giuliano A, Eckardt J, et al. Adjuvant chemotherapy for osteosarcoma: A
randomized prospective trial. J Clin Oncol 1987; 5: 21-6.
4. Casper ES, Gaynor JJ, Harrison LB, et al. Preoperative and postoperative adjuvant
combination chemotherapy for adults with high grade soft tissue sarcoma. Cancer
1994; 73: 1644-51.
5. Hoekstra HJ, Schraffordt Koops H, Molenaar WM, et al. Results of isolated regional
perfusion in the treatment of malignant soft tissue tumors of the extremities. Cancer
1987; 60: 1703-7.
6. Rosenberg B, Van Camp L, Krigas T. Inhibition of cell division in escherichia coli
by electrolysis products from platinum electrode. Nature 1965; 205: 157-64.
7. De Vries J, Hartel RM, Schraffordt Koops H, et al. Dosage of cisplatin in
hyperthermic isolated regional perfusion. Surg Res Commun 1987; 2: 107-12.
8. van Ginkel RJ, Hoekstra HJ, Meutstege FJ, et al. Hyperthermic isolated regional
perfusion with cisplatin in the local treatment of spontaneous canine osteosarcoma:
assessment of short-term effects. J Surg Oncol 1995; 59: 169-76.
9. Creech O, Krementz ET, Ryan RF, et al. Chemotherapy of cancer: regional perfusion
utilizing an extra-corporeal circuit. Ann Surg 1958; 148: 616-32.
10. Fontijne WP, Mook PH, Schraffordt Koops H, et al. Improved tissue perfusion during
pressure regulated regional perfusion: a clinical study. Cancer 1985; 55: 1455-61.
11. Wieberdink J, Benckhuysen C, Braat RP, et al. Dosimetry in isolation perfusion of
the limb by assessment of perfused tissue volume and grading of toxic tissue reactions.
Eur J Cancer Clin Oncol 1982; 18: 905-10.
12. Hoekstra HJ, Naujocks T, Schraffordt Koops H, et al. Continuous leakage monitoring
during hyperthermic isolated regional perfusion of the lower limb: techniques and
results. Reg Cancer Treat 1992; 4: 301-4.
13. Coombs R, Halliday K: Biopsy techniques. Coombs R, Friedlaender G (eds). In:
Bone tumor management (1st edn). Cornwall, Great Britain: Robert Hartnoll Ltd.
1987: 81-7.
14. Guchelaar HJ, Hoekstra HJ, De Vries EGE, et al. Cisplatin and platinum
pharmacokinetics during hyperthermic isolated limb perfusion for human tumors of
the extremities. Br J Cancer 1992; 65: 898-902.
15. Aigner K, Schwemmle K. Technic of isolated perfusion of the extremities. Experience
with 171 cases. Langenbecks Arch Chir 1983; 359: 113-22.
16. Rosenberg B. Fundamental studies with cisplatin. Cancer 1985; 55: 2303-l6.
17. Klein ES, Ben-Ari GY. Isolation perfusion with cisplatin for malignant melanoma
of the limbs. Cancer 1987; 59: 1068-71.
18. Hoekstra HJ, Schraffordt Koops H, De Vries EGE, et al. Toxicity of hyperthermic
isolated limb perfusion with cisplatin for recurrent melanoma of the lower extremity
after previous perfusion treatment. Cancer 1993; 72: 1224-9.

65
Cisplatin perfusion in patients with sarcomas
19. Ham SJ, Hoekstra HJ, van der Graaf WTA, et al. The value of high-dose methotrexate
based (HD-MTX) neoadjuvant chemotherapy in malignant fibrous histiocytoma
(MFH) of bone. J Clin Oncol 1996;
20. Fletcher WS, Pommier RF, Woltering EA, et al. Pharmacokinetics and results of
dose escalation in cis-platin hyperthermic isolation limb perfusion. Ann Surg Oncol
1994; 1: 236-43.
21. van der Zee J, Broekmeyer-Reurink MP, van den Berg AP, et al. Temperature
distribution and pH changes during hyperthermic regional isolation perfusion. Eur
J Cancer Clin Oncol 1989; 25: 1157-63.
22. Vaglini M, Belli F, Santinami M. Isolation perfusion of the lower limb with platinum.
World J Surg 1988; 12: 307-9.
23. Lienard D, Ewalenko P, Delmotte JJ, et al. High-dose recombinant tumor necrosis
factor alpha in combination with interferon gamma and melphalan in isolation
perfusion of the limbs for melanoma and sarcoma. J Clin Oncol 1992; 10: 52-60.
24. Eggermont AMM, Lienard D, Schraffordt Koops H, et al. Limb salvage by high
dose tumor necrosis factor alpha (TNF) , gamma-interferon (IFN) and melphalan
isolated limb perfusion (ILP) in patients with irresectable soft tissue sarcomas. Proc
Am Soc Clin Oncol 1992; 11: 1444

66

67
Robert J. van Ginkel1
Harald J. Hoekstra1
Alex M.M. Eggermont2
Elisabeth Pras3
Heimen Schraffordt Koops1
Departments of Surgical Oncology1, Radiotherapy3, University Hospital
Groningen, Groningen, The Netherlands and Dr. Daniel den Hoed Cancer Center2,
Rotterdam, The Netherlands.
Archives of Surgery 1996; 131: 672-674.
Isolated limb perfusion of an irradiated foot with
TNF, interferon and melphalan

68
Chapter 5
Abstract
Hyperthermic isolated limb perfusion (HILP) with tumor necrosis factor alpha (TNF),
interferon gamma (IFN) and melphalan is a highly effective limbsaving treatment in
patients with irresectable soft tissue sarcoma or satellitosis and in-transit metastases
of melanoma. A 57-yr old woman presented with the second recurrence of a high
grade malignant fibrous histiocytoma of the right foot following previous local
resection plus curative adjuvant radiotherapy. The first recurrence of the lesion was
treated by HILP with cisplatin; the second recurrence was treated by HILP with
TNF, IFN and melphalan. The tumor and the area that had been irradiated showed a
bluish color a few hours after tumor necrosis factor perfusion. Nine days after TNF
perfusion a lower leg amputation had to be performed because of severe necrosis of
the foot.
Introduction
Recently Lienard and colleagues described the magnificent effect of hyperthermic
isolated limb perfusion (HILP) with recombinant tumor necrosis factor alfa (TNF),
recombinant interferon gamma (IFN) and melphalan in 23 patients with locally
advanced melanomas and soft tissue sarcomas of the extremities.1 The effect on the
tumors was striking: 19 (83%) complete responses and four (17%) partial responses
after a single perfusion with the triple-drug regimen. Local toxicity in the perfused
limb was minimal, 88% grade II and 12% grade III classified according to
Wieberdink.2 These figures are comparable with local tissue toxicity in patients treated
with melphalan as the single perfusion agent. The preliminary results of this study
suggested that high-dose TNF can be administrated safely by regional perfusion.
HILP of the limb with this triple drug regimen was started in 1991 at Groningen
University Hospital in the Netherlands, one of several institutions participating in a
multicenter study. The effect of this new combined modality therapy of isolated limb
perfusion and delayed surgery in a patient with a previous history of irradiation of
the foot is described.
Case report
In 1988 a 57-yr old woman presented with a 5 x 6 cm high grade malignant fibrous
histiocytoma on the lateral side of the right foot without distant metastases. She
refused a curative amputation of the lower leg. Therefore a marginal resection was
performed, followed by 60 Gy external beam radiotherapy, 40 Gy (2 Gy per day) on
the whole foot, and a 20 Gy boost on the tumor (Fig. 1). Two years after initial
treatment the tumor recurred locally without evidence of distant metastases. Again
she refused a lower leg amputation. In an attempted to render the tumor resectable,

69
Radiotherapy prior to HILP with TNF
HILP through the popliteal vessels with 100 mg cisplatin (30mg cisplatin per liter
limb volume) was performed. Histologic biopsy specimens of the tumor obtained 1
and 2 weeks after cisplatin perfusion showed no viable tumor cells, and a complete
remission was observed clinically.
In January 1991 the second local recurrence without distant metastases was observed,
again with persistent refusal by the patient for a curative amputation. During six
months the patient withdrew from follow-up but presented in June 1991 with a local
ulcerating tumor measuring 10 x 12 cm, still without metastatic disease (Fig. 2).
Because of the patients persistent refusal to undergo an amputation, a HILP with
TNF, IFN and melphalan was suggested and informed consent was obtained. One
and 2 days before HILP, a dose of 0,2 mg of IFN (Boehringer Ingelheim, Ingelheim,
Germany) was administered subcutaneously. A 90-minute mild hyperthermic (39°C
to 40°C), popliteal perfusion was performed with 0,2 mg of IFN, 4 mg of TNF
Fig. 1 Clinical appearance of the
patients right foot demonstrating the
radiation field and dosages of the ini-
tial treatment
Fig. 2 Clinical appearance of the
patients right foot demonstrating
the second recurrence

70
Chapter 5
(Boehringer Ingelheim), and 45 mg of melphalan (10 mg/L of limb volume)(Burroughs
Welcome, London, England). Leakage to the systemic circulation measured with131I labeled albumin as a tracer was 2.8 %.3 ECG, urine output, blood pressure,
venous and pulmonary pressures were recorded during and after perfusion until the
second postoperative day. A continuous infusion of dopamine at 2.8 mg/kg/min for
18 hours was given. Postoperatively the patient experienced fever and chills but no
hematological, hepatic or renal toxicity was observed.
A few hours after TNF perfusion, the entire right foot appeared bluish up to a definite
line at the ankle; the rest of the leg had a normal circulation. Two days after perfusion,
the tumor was black and necrotic in concordance with the 60-Gy total dose
Fig. 3 The right foot and ankle re-
gion 2 days after hyperthermic iso-
lated limb perfusion with TNF, IFN
and melphalan. The tumor is black
necrotic and the rest of the foot is
blue, sharply delineated at the edge
of the radiation field.
Fig 4 Left, A necrotic tumor tissue specimen after tumor necrosis factor perfusion (hema-
toxylin-eosin, x64) Right, The border area between nonirradiated normal skin (right) and
irradiated skin (left). The irradiated site demonstrates infiltration of both the dermis and the
epidermis with granulocytes and marked stasis with thrombosis of the microcirculation. In
the nonirradiated area, normal vascular structures are seen (hematoxylin-eosin, x64).

71
Radiotherapy prior to HILP with TNF
radiotherapy field, while the rest of the foot (40-Gy field) was blue and showed
some dry shrinkage of the skin (Fig. 3). Because of the severe necrosis, amputation
of the right foot below the knee had to be performed 9 days after TNF perfusion.
Histological findings were consistent with complete necrosis of the tumor (Fig. 4,
left). The amputation wound healed without complications, and the patient is alive
without evidence of disease 3 years after TNF perfusion and subsequent amputation.
Discussion
In 1975, Carswell et al. showed that tumor-necrotizing activity in the sera of animals
given injections of endotoxin was due to a host factor named tumor necrosis factor
(TNF).4 The mechanisms of the anti tumor activity of TNF however, are still not
elucidated and basis of further research. The results of intralesional or intravenous
administration of recombinant human TNF in mice with solid Meth A sarcoma of the
skin were recently described by van de Wiel and Bloksma.5 Treatment with TNF
caused red discoloration and necrosis of the central portion of the tumor within 24
hours. However, incubation of Meth A cells in the presence of TNF in vitro did not
affect their capacity to incorporate tritiated thymidine, indicating resistance of the
Meth A cells to TNF in vitro and supporting the thought that other mechanisms are
responsible for the observed discoloration and necrosis of the tumor in vivo.
Microscopic investigations of the tumors showed hyperemia, congestion, endothelial
damage and hemorrhage in the central part of the tumor, while just outside the tumor
edema and an infiltrate of polymorphonuclear cells was seen. Locally injected normal
skins with TNF showed moderate vascular effects without necrosis. This and other
investigations demonstrated that the vascular endothelial cells in particular are the
main target cells of this TNF induced antitumor effect.6,7 When incubated with TNF,
cultured endothelial monolayers show two phenomena. Stolpen et al. demonstrated
that TNF causes morphological changes of the endothelial cells, they become
elongated, overlap, rearrange their actin filaments and lose their stainable fibronectin
matrix.8 Suppression of anticoagulant mechanisms and the production of the
procoagulant cofactor tissue factor, is the second phenomenon9. These TNF-induced
changes are more prominent in areas with growing and/or migrating endothelial cells,
a situation that occurs within the tumor bed and explaining why the tumor vasculature
is more susceptible for TNF compared with normal vessels.10 A higher expression of
TNF receptors on the endothelial cell surface of dividing and growing endothelial
cells seem to be the cause of this high sensitivity for TNF.10,11 In summary; TNF
exposure emerges an altered endothelial cell phenotype, anticoagulant mechanisms
are suppressed and tissue factor is produced, leading to fibrin accumulation at the
endothelial cell surface 12 and thrombus formation in the tumor vessel, causing

72
Chapter 5
circulatory stasis and ischemia inside the tumor followed by necrosis of the tumor.
Besides this early vascular phenomenon, a latter in time occurring immune effect
with polymorphonuclear cell binding to the activated endothelium,7,13,14 and a direct
cytotoxic effect of TNF demonstrated in vitro against a variety of cell lines 15,16 are
two other mechanisms that could contribute in the anti-tumor effect of TNF.
In our case, not only the vascularization of the tumor was affected by TNF exposure
but also the microvascularization of the area that had been irradiated 3 years earlier.
Microscopical examination of the border area between irradiated and nonirradiated
areas revealed infiltration of both dermis and the epidermis with granulocytes, and
marked stasis with trombosis of the micro circulation of the irradiated area, causing
necrosis. These phenomena were absent from the perfused nonirradiated area (Fig.
4,right).
Late effects of normal tissues after radiotherapy are well known. Hopewell
demonstrated that arteries of the hamsters cheek pouch showed localized constrictions
after irradiation.17 These constrictions were caused by clones of dividing endothelial
cells and might be the predominant factor influencing the degeneration of the capillary
bed after radiotherapy.18 Evidence of this occlusive effect of vessels by proliferating
endothelial cells after radiation have also been reported by other investigators.19 Since
dividing and migrating endothelial cells are more sensitive to TNF than quiescent
endothelial cells, it is likely that not only the dividing and migrating endothelial cells
of the tumor bed but also the endothelial cells in the irradiated area of the foot in this
patient were activated by TNF, causing stasis and thrombosis of the microcirculation
in both areas. Recently Milas and coworkers also demonstrated a synergistic effect
between radiotherapy and TNF.20,21
One and a half year before TNF perfusion, this patient received HILP with cisplatin.
No literature is available describing the acute or long term effect of cisplatin on the
endothelial cells, however treatment with antineoplastic agents is associated with
vascular toxicity.22 With regard to cisplatin Vogelzang et al. described the relation
between hypomagnesemia and an increased risk of Raynaud´s phenomenon after
cisplatin, vinblastine and bleomycin treatment.23 Jackson et al. described a thrombotic
microangiopathic syndrome characterized by renal insufficiency, microangiopathic
hemolytic anemia and thrombocytopenia in patients treated with an identical
regimen.24 Histological examination of renal biopsy specimens showed marked
luminal narrowing of small arteries as a result of thrombus formation and subintimal
thickening. Whether cisplatin is the sole agent responsible for this vascular effect
remains unclear especially since it is known that bleomycin in this combination
chemotherapy has a prominent effect on endothelial cells.25 Analysis of cisplatin
perfusions data, performed at our clinic showed severe neurotoxicity, yet no signs of

73
Radiotherapy prior to HILP with TNF
vascular disturbances were found (i.e. Raynaud´s phenomenon).26 A synergistic effect
between cisplatin and radiotherapy is known when cisplatin is administered shortly
before or after radiotherapy,27 in this patient the interval between radiotherapy and
cisplatin perfusion lasted to long to make synergism likely.
Other radiation-related or radiation-independent factors may also be contributory,
i.e., the radiation dosage, time interval between radiation and TNF perfusion, and
the irradiated anatomical site. To distinguish the contribution of each of these different
factors experimental investigations should be performed. Awaiting the results of such
experiments, we would like to alert surgeons and radiation oncologists to the possible
complications that may occur after TNF perfusion, when the perfused limb has already
been irradiated.

74
Chapter 5
References
1 Lienard D, Ewalenko P, Delmotte JJ, Renard N, Lejeune FJ. High-dose recombinant
tumor necrosis factor alpha in combination with interferon gamma and melphalan
in isolation perfusion of the limbs for melanoma and sarcoma. J Clin Oncol 1992;
10: 52-60.
2 Wieberdink J, Benckhuysen C, Braat RP, Van Slooten EA, Olthuis GAA. Dosimetry
in isolation perfusion of the limb by assessment of perfused tissue volume and grading
of toxic tissue reactions. Eur J Cancer Clin Oncol 1982; 18: 905-910.
3 Hoekstra HJ, Naujocks T, Schraffordt Koops H, et al. Continuous leakage monitoring
during hyperthermic isolated regional perfusion of the lower limb: techniques and
results. Reg Cancer Treat 1992; 4: 301-304.
4 Carswell EA, Old LJ, Kassel RL. An endotoxin induced serum factor that causes
necrosis of tumors. Proc Natl Acad Sci USA 1975; 72: 3666-3670.
5 Van de Wiel PA, Bloksma N, Kuper CF, Hofhuis FM, Willers JM. Macroscopic and
microscopic early effects of tumor necrosis factor on murine Meth A sarcoma, and
relation to curative activity. J Pathol 1989; 157: 65-73.
6 Van de Wiel PA, Pieters RH, van der Pijl A, Bloksma N. Synergic action between
tumor necrosis factor and endotoxins or poly(A.U) on cultured bovine endothelial
cells. Cancer Immunol Immunother 1989; 29: 23-28.
7 Palladino MAJR, Shalaby MR, Kramer SM, et al. Characterization of the antitumor
activities of human tumor necrosis factor-? and the comparison with other cytokines:
induction of tumor-specific immunity. J Immunol 1987; 138 : 4023-4032.
8 Stolpen AH, Guinan EC, Fiers W, Pober JS. Recombinant tumor necrosis factor and
immune interferon act singly and in combination to reorganize human vascular
endothelial cell monolayers. Am J Pathol 1986; 123: 16-24.
9 Nawroth PP, Stern DM. Modulation of endothelial cell hemostatic properties by
tumor necrosis factor. J Exp Med 1986; 163: 740-745.
10 Gerlach H, Lieberman H, Bach R, et al. Enhanced responsiveness of endothelium
in the growing/motile state to tumor necrosis factor/cachectin [published erratum
appears in J Exp Med 1989 Nov 1;170(5):1793]. J Exp Med 1989; 170: 913-931.
11 Espevik TP, Brockhaus M, Loetscher H, Nonstad U, Shalaby R. Characterization of
binding and biological effects of monoclonal antibodies against a human tumor
necrosis factor receptor. J Exp Med 1990; 171: 415-426.
12 Nawroth P, Handley D, Matsueda G, et al. Tumor necrosis factor/cachectin-induced
intravascular fibrin formation in meth A fibrosarcomas. J Exp Med 1988; 168: 637-
647.
13 Gamble JR, Harlan JM, Klebanoff SJ, Vadas MA. Stimulation of the adherence of
neutrophils to umbilical vein endothelium by human recombinant tumor necrosis
factor. Proc Natl Acad Sci U S A 1985; 82: 8667-8671.
14 Renard N, Lienard D, Lespagnard L, et al. Early endothelium activation and
polymorphonuclear cell invasion precede specific necrosis of human melanoma and
sarcoma treated by intravascular high-dose tumor necrosis factor alpha (TNF). Int J
Cancer 1994; 57: 656-663.
15 Helson L, Green S, Carswell E, Old LJ. Effect of tumor necrosis factor on cultured
human melanoma cells. Nature 1975; 258: 731-732.

75
Radiotherapy prior to HILP with TNF
16 Sugarman BJ, Aggarwal BB, Hass PE, Figari IS, Palladino MA. Recombinant human
tumor necrosis factor-alpha: effects on proliferation of normal and transformed cells
in vitro. Science 1985; 230: 943-945.
17 Hopewell JW. Early and late changes in the functional vascularity of the hamster
cheek pouch after local x-irradiation. Radiat Res 1975; 63: 157-164.
18 Hopewell JW. Letter: The late vascular effects of radiation. Br J Radiol 1974; 47:
157-158.
19 Fajardo LF, Stewart JR. Capillary injury preceding radiation-induced myocardial
fibrosis. Radiology 1971; 101: 429-433.
20 Nishiguchi I, Willingham V, Milas L. Tumor necrosis factor as an adjunct to
fractionated radiotherapy in the treatment of murine tumors. Int J Radiat Oncol Biol
Phys 1990; 18: 555-558.
21 Sersa G, Willingham V, Milas L. Anti-tumor effects of tumor necrosis factor alone
or combined with radiotherapy. Int J Cancer 1988; 42: 129-134.
22 Doll DC, Ringenberg QS, Yarbro JW. Vascular toxicity associated with antineoplastic
agents. J Clin Oncol 1986; 4: 1405-1417.
23 Vogelzang NJ, Torkelson JL, Kennedy BJ. Hypomagnesemia, renal dysfunction,
and Raynaud’s phenomenon in patients treated with cisplatin, vinblastine, and
bleomycin. Cancer 1985; 56: 2765-2770.
24 Jackson AM, Rose BD, Graff LG, et al. Thrombotic microangiopathy and renal
failure associated with antineoplastic chemotherapy. Ann Intern Med 1984; 101:
41-44.
25 Nicolson GL, Custead SE. Effects of chemotherapeutic drugs on platelet and
metastatic tumor cell-endothelial cell interactions as a model for assessing vascular
endothelial integrity. Cancer Res 1985; 45: 331-336.
26 Hoekstra HJ, Schraffordt Koops H, De Vries EGE, Van Weerden TW, Oldhoff J.
Toxicity of hyperthermic isolated limb perfusion with cisplatin for recurrent
melanoma of the lower extremity after previous perfusion treatment. Cancer 1993;
72: 1224-1229.
27 Vokes EE. Interactions of chemotherapy and radiation. Semin Oncol 1993; 20: 70-
79.

76

77
Robert J. van Ginkel1
Harald J. Hoekstra1
Jan Pruim2
Omgo E. Nieweg1,3
Willemina M. Molenaar4
Anne M.J. Paans2
Anton T.M. Willemsen2
Wim Vaalburg2
Heimen Schraffordt Koops1
Department of Surgical Oncology1, PET Center2 and Department of Pathology4,
University Hospital Groningen, The Netherlands and Department of Surgery3, The
Netherlands Cancer Institute, Amsterdam, The Netherlands.
Journal of Nuclear Medicine 1996; 37: 984-990.
FDG-PET to evaluate response to hyperthermic
isolated limb perfusion for locally advanced soft-
tissue sarcoma

78
Chapter 6
Abstract
We investigated FDG-PET in patients undergoing hyperthermic isolated limb
perfusion (HILP) with TNF, IFN and melphalan for locally advanced soft-tissue
sarcoma of the extremities. Twenty patients (11 women, 9 men; aged 18-80 yrs, mean
age 49 yrs) were studied. FDG-PET studies were performed before, 2 and 8 weeks
after HILP. After the final PET study, the tumor was resected and pathologically
graded. Patients with a pathologically complete response (pCR) showed no viable
tumor after treatment. Those with a pathologically partial response (pPR) showed
various amounts of viable tumor in the resected tumor specimens. Seven patients
showed a pCR (35%) and 12 patients showed a pPR (60%). In one patient,
pathological examination was not performed (5%). The pre-perfusion glucose
consumption in the pCR group was significantly higher than in the pPR group
(p<0.05). Visual analysis of the PET images after perfusion showed a rim of increased
FDG uptake around a core of absent FDG uptake in 12 patients. The rim signal
contained a fibrous pseudocapsule with inflammatory tissue in the pCR group, but
viable tumor tissue was seen in the pPR group. The glucose consumption in the pCR
group at 2 and 8 weeks after perfusion had decreased significantly (p<0.05) compared
with the glucose consumption in the pPR group. Based on the pretreatment glucose
consumption in soft-tissue sarcomas, one could predict the probability of a patient
achieving a complete pathologically response after TNF HILP. FDG-PET indicated
the pathologic tumor response to HILP, although the lack of specificity of FDG, in
terms of differentiation between an inflammatory response and viable tumor tissue,
hampered the discrimination between pCR and pPR.
Introduction
Malignant soft-tissue sarcomas are a heterogeneous group of lesions that all arise
from tissue of mesenchymal origin and are characterized by aggressive local growth
and hematogenic metastases. They account for 1% of all malignant tumors and have
an incidence rate of 2 per 100.000. About 60% of these tumors occur in the extremities
and are often quite large at diagnosis.1 Limb-saving treatment of extremity soft-tissue
sarcomas is a multidisciplinary matter, with surgery and radiotherapy as the usual
treatment protocol.2,3 This combination therapy has avoided ablative surgical
procedures in the majority of patients.
The majority of locally advanced extremity soft-tissue sarcomas are treated by
amputation. Intra-arterial chemotherapy with adriamycin, combined with preoperative
radiotherapy, surgery and postoperative radiotherapy is effective in the treatment of
locally advanced soft-tissue sarcoma, but significant morbidity does occur.4 Recently
Eilber et al. reported a complete response rate of 49% and a limb-saving rate of 98%

79
FDG-PET to evaluate response to TNF perfusion
with neo-adjuvant chemotherapy and radiation for high-grade extremity soft-tissue
sarcoma with low treatment morbidity.5 Hyperthermic isolated limb perfusion (HILP)
also proved to be of value in the treatment for locally advanced extremity soft-tissue
sarcoma.6-8 With HILP, chemotherapeutic tissue concentrations may be up to 20 times
higher than can be attained with systemic administration.9 The introduction of
recombinant tumor necrosis factor-alpha (TNF), interferon-gamma (IFN) and
melphalan in regional perfusion represents a promising new development.10 With
this perfusion regimen, a complete response rate of 55% and a partial response rate
of 40% can be reached in the treatment of locally advanced soft-tissue sarcoma of
the extremities with a limb-saving rate of 90%.11 Since 1991, this perfusion strategy
has been used at our institution for these types of soft-tissue sarcomas.
PET enables visualization and quantification of metabolic processes in vivo. Fluorine-
18-2-fluoro-2-deoxy-D-glucose (FDG) has proven to be of value in the visualization
of various types of tumors.12,13 The use of FDG is based on Warburg´s observation of
increased glycolysis in cancer cells. The citric acid cycle, which is more efficient in
adenosine tri-phosphate generation, is suppressed.14 As a result, cancer cells
accumulate the glucose analog FDG which is trapped intracellularly as FDG
phosphate. FDG-PET can visualize soft-tissue sarcomas, indicate the malignancy
grade and detect locally recurrent disease.15-17 Various clinical reports suggest the
feasibility of FDG-PET to assess tumor response to radiotherapy and chemotherapy.18-20 This particular application of PET as a noninvasive technique to evaluate the
outcome of such often aggravating and expensive therapy may have a significant
effect on patient management. Ineffective treatment could be adjusted or discontinued
in an early stage and effective treatment could be continued with confidence.
The perfusion protocol provides us with histology before and after regional
chemotherapy. The tumor responses to this regional drug treatment are variable. This
clinical setting creates an opportunity to investigate the value of a noninvasive
diagnostic technique in the determination of tumor response to chemotherapy. The
aim of the present study was to investigate FDG-PET in patients undergoing HILP
for locally advanced soft-tissue sarcoma and to correlate PET findings with histology
before and after treatment.
Materials and methods
Patients
Twenty (11 women, 9 men, aged 18-80 yrs, mean age 49 yrs) patients with biopsy-
proven soft-tissue sarcomas were entered in the study. Informed consent was obtained
from each patient. The diagnosis of the tumors was determined in a standard fashion
and graded according to Coindre.21,22 Thirteen patients presented with a newly

80
Chapter 6
diagnosed soft-tissue sarcoma (65%) and seven patients with a local recurrence (35%),
that had been previously treated with surgery alone. Nineteen tumors were located in
the lower limb (95%), and one patient (5%) had a sarcoma located in the right elbow.
All tumors were considered primarily irresectable because of size, their multicentricity
in the limb or fixation to the neurovascular bundle or bone. Median tumor size was
8.5 cm (range 2-30 cm). To render the tumors resectable for limb salvage, patients
were treated with HILP.
Treatment protocol
HILP is based on the technique developed by Creech and Krementz.23 Briefly, after
ligation of all collateral vessels and heparinization of the patient with 3.3 mg heparin/
kg bodyweight (Thromboliquine, Organon BV, Oss, the Netherlands), the axillary,
iliac, femoral or popliteal vessels were cannulated and connected to an extracorporeal
circuit. The perfused limb was wrapped in a thermal blanket to reduce heat loss and
a tourniquet was applied at the root of the extremity to minimize leakage of the
perfusate into the systemic circulation. Perfusion was performed during 90 min under
mild hyperthermia (39-40oC) and physiologically optimal conditions.24 At the start
of perfusion, 3 mg (upper extremity) or 4 mg (lower extremity) TNF (Boehringer,
Ingelheim, Germany) were injected as a bolus into the arterial line. Melphalan
(Burroughs Wellcome, London, England) was administered 30 min later, 10 mg/L
extremity volume (leg) or 13 mg/L extremity volume (arm).25 Since all perfusions
were performed in a Phase II clinical trial, the initial 13 patients in the PET study
also received a dose of 0.2 mg INF (Boehringer, Ingelheim, Germany) subcutaneously
1 and 2 days before perfusion, followed by 0.2 mg INF injected into the arterial line
at the start of perfusion. The final seven patients in the PET study did not receive the
INF. This alteration in treatment schedule was due to the decision of the trial
commission to investigate the additional effect of INF in the perfusion regiment
while the PET study was still in progress.
All perfusions were performed with a bubble oxygenator roller pump and heat
exchanger. The perfusate was oxygenated by a mixture of O2 and CO
2 and consisted
of 350 ml 5% dextran 40 in glucose 5% (Isodex, Pharmacia AB, Uppsala, Sweden),
500 ml blood (250 ml red blood cells, 250 ml plasma), 30 ml 8.4% NaHCO3, 0.5 ml
5000 IU/ml heparin. After 90 min of perfusion, the limb was flushed with 2 liters
dextran 40 in glucose 5% (Isodex, Pharmacia AB, Uppsala, Sweden) and 500 ml
blood (250 ml red blood cells, 250 ml plasma), catheters were removed, the circulation
restored and the heparin antagonized with protamine chloride (Hoffman La Roche,
Mijdrecht, the Netherlands). A lateral fasciotomy of the anterior compartment of the
lower leg or arm was performed to prevent a compartment syndrome.26 Approximately

81
FDG-PET to evaluate response to TNF perfusion
8 weeks after perfusion (median 61 days, range 43-106 days) the residual tumor
masses were excised and pathologically examined.
Pathological examination
The tumor was measured in three dimensions and the percentage of necrosis estimated.
Representative tumor sections were taken, encompassing macroscopically different
tumor areas, including necrosis. Generally, one section per centimeter largest diameter
with a minimum of three was taken. Based on an integration of gross and microscopic
findings, a final estimate of the percentages of viable and necrotic or regressive tumor
was made. If possible, macroscopic examination and tissue sampling were performed
based on the latest PET images. The results were classified as either pathologically
complete response (pCR) or pathologically partial response (pPR), when remaining
viable tumor was observed.
PET imaging
Patients were scheduled for three PET studies: shortly before perfusion (median 14
days, range 1-30 days), two weeks after perfusion (median 13 days, range 7-27 days)
and shortly before resection of residual tumor tissue (median 55 days, range 42-77
days after perfusion). FDG was routinely produced by a robotic system following
the procedure as described by Hamacher27 with a radiochemical purity of more than
98%. PET sessions were performed using a Siemens ECAT 951/31 PET-camera
(Siemens/CTI, Knoxville, USA).
All patients fasted for at least 6 hours before the investigation. Serum glucose levels
were measured before each PET session and were found to be normal. A 20-gauge
needle was inserted into the radial artery under local anesthesia. In the contralateral
arm, an intravenous canula was inserted in the cephalic vein for the injection of the
FDG. The patients were positioned supine in the camera, with the tumor in the field
of view based on physical examination.
After attenuation scanning using 68Ge/68Ga source, 370 MBq (10mCi) FDG were
administered intravenously over 1 min. Dynamic images were acquired from the
time of injection after a dynamic protocol (five 1-min, five 2-min, five 3-min, two 5-
min, two 10-min, for a total duration of 60 min). Simultaneously, 2-ml blood samples
were taken from the arterial canula (time points 0.5, 1, 1.5, 2, 2.5, 3, 3.5, 4, 4.5, 5, 10,
15, 25, 35, 45 and 55 min post-injection). The blood samples were centrifuged and
plasma activity was assessed using a well counter that was cross-calibrated with the
positron camera. Whole-body images were obtained after dynamic scanning. Total
time for the imaging procedure was approximately 2.5 hours.

82
Chapter 6
Data analysis
Images were displayed in coronal, sagittal and transaxial projections on a computer
display applying standard ECAT software (Siemens/CTI, Knoxville, USA) and
interpreted independently by two experienced physicians. Before perfusion, the tumor
location was first defined in all relevant tomographic planes of the study. Each tumor
was outlined automatically with a threshold technique that defines its contours at a
manually chosen percentage of the maximum number of counts per pixel. The level
of the threshold was chosen with the purpose to match the size of the region of
interest with the tumor size as outlined by MRI or CT. For each patient, a fixed
percentage (median 40, range 30-60) was used in all planes. All pixels above the
threshold were used for the calculation. An average time-activity curve as well as the
total volume of the lesion was obtained. Combining the averaged time-activity data
with the plasma input data, the average metabolic rate of glucose consumption
(MRglc) in µmol/100g tumor tissue /min was calculated using Patlak analysis,
assuming a lumped constant of 0.42.28,29 After perfusion, this threshold technique
could not be used since large areas of the tumors became inactive. The MRglc after
perfusion was therefore calculated by placing multiple regions of interest (ROI) over
the original tumor in all relevant planes of the study. Consequently, the necrotic parts
of the tumor that originated after perfusion were incorporated in this calculation.
The MRglc in the active parts of the tumor after perfusion was calculated separately
with the ROI technique. The change in MRglc after perfusion was related to the pre-
perfusional value and expressed as a percentage of basal value.
Visual evaluation of the PET studies was performed by quantifying the degree of
viable (active areas on the PET studies) and necrotic tumor (inactive areas) as a
percentage before and after perfusion.
Statistical analysis
Statistical procedures included a two-factor experiment with repeated measures on
one factor to compare glucose consumption between measures and groups. Analyses
were performed on datasets corrected for missing data according to Winer.30 Posthoc
comparison was made with Student t-tests. A p-value < 0.05 was considered
significant. SPSS/PC+
statistical software was used.
Results
The tumor characteristics, PET results and pathological response for each patient are
summarized in Tables 1 and 2. Pathological examination of the residual tumor mass
showed no viable tumor in seven patients (pCR 35%). In twelve patients, variable
amounts of viable tumor were found (pPR 60%). The pPR group also included one

83
FDG-PET to evaluate response to TNF perfusion
A B C
Ta
ble
1T
um
or ch
aracteristics for each
patien
t.
Pat.
His
tolo
gy
Gra
de
Nu
mb
er L
arg
est
Pe
rfusio
n a
gen
ts
Nr.
of
dia
mete
r
lesio
ns
(MR
I)
1R
ha
bdom
yosarc
om
aP
rimary
31
10 c
mT
NF, IF
N, M
elp
ha
lan
2D
ediffe
rentia
ted m
yxoid
liposarc
om
aP
rimary
31
20 c
mT
NF, IF
N, M
elp
ha
lan
3M
yxo
id lip
osarc
om
aR
ecurre
nt
12
15 c
mT
NF, IF
N, M
elp
hala
n
4P
erip
hera
l neuro
ecto
derm
al tu
mor
Prim
ary
33
8 c
mT
NF, M
elp
hala
n
5M
alig
nant fib
rous h
istio
cyto
ma
Prim
ary
31
5 c
mT
NF, M
elp
hala
n
6M
alig
nant fib
rous h
istio
cyto
ma
Recurre
nt
31
4 c
mT
NF, M
elp
hala
n
7S
yn
ovia
lsa
rco
ma
Prim
ary
31
8 c
mT
NF, M
elp
hala
n
8M
yxo
id c
hondro
sarc
om
aP
rimary
21
8 c
mT
NF, IF
N, M
elp
hala
n
9M
alig
nant fib
rous h
istio
cyto
ma
Prim
ary
21
19 c
mT
NF, IF
N, M
elp
ha
lan
10
Ma
lignant fib
rous h
istio
cyto
ma
Recurre
nt
124 *
2 c
mT
NF, IF
N, M
elp
hala
n
11M
alig
nant s
chw
annom
aR
ecurre
nt
37
5 c
mT
NF, M
elp
hala
n
12
Fib
rosarc
om
aP
rimary
31
23 c
mT
NF, IF
N, M
elp
hala
n
13
Syn
ovio
sa
rco
ma
Prim
ary
31
9 c
mT
NF, IF
N, M
elp
hala
n
14
Myxoid
liposarc
om
aR
ecurre
nt
12
8 c
mT
NF, IF
N, M
elp
hala
n
15
Dediffe
rentia
ted lip
osarc
om
aP
rimary
21
17 c
mT
NF, IF
N, M
elp
ha
lan
16
Le
iom
yo
sa
rco
ma
Recurre
nt
31
12 c
mT
NF, IF
N, M
elp
hala
n
17
An
gio
sarc
om
aP
rimary
31
30 c
mT
NF, M
elp
ha
lan
18
Malig
nant s
chw
annom
aR
ecurre
nt
21
8 c
mT
NF, IF
N, M
elp
hala
n
19
We
ll diffe
rentia
ted lip
osarc
om
aP
rimary
11
29 c
mT
NF, IF
N, M
elp
ha
lan
20
Ma
lignant fib
rous h
istio
cyto
ma
Prim
ary
34
5 c
mT
NF, M
elp
hala
n
* M
ultip
le small lesio
ns o
f the lo
wer leg
(0.5
- 2 cm
); TN
F =
tum
or n
ecrosis facto
r; IFN
= in
terferon

84
Chapter 6
Ta
ble
2P
ET
res
ult
s an
d p
atholo
gic
al r
esponse
for
each
pat
ient
V
isu
al evalu
ati
on
of
the
Meta
bo
lic r
ate
of
glu
co
se (µ m
ol/
10
0g
/min
)
P
ath
olo
gic
al
ev
alu
ati
on
P
ET
stu
die
s
Pat.
B
efo
re H
ILP
A
fter
HIL
P B
efo
re H
ILP
2
weeks a
fter
HIL
P 8
weeks a
fter
HIL
P R
esp
on
se %
via
ble
M
acro
/ m
icro
sco
pic
C
orr
esp
on
den
ce
no
.
% o
f tu
mo
r
%
of
tum
or
Tu
mo
rTu
mo
rR
imC
ore
Tu
mo
rR
imC
ore
tum
or
vie
w o
f P
ET
wit
h h
isto
log
y
acti
ve *
acti
ve *
11
00
< 1
03
6.7
3.7
8.4
0.6
n.q
.n
.q.
n.q
.p
CR
0rim
: p
se
ud
oca
psu
le+
core
: necro
sis
21
00
< 1
04
1.8
n.p
.n
.p.
n.p
.2
.76
.30
.4p
CR
0rim
: p
se
ud
oca
psu
le+
core
: necro
sis
3 8
080
3.6
n.q
.n.q
.n.q
.5.6
Absent
Absent
pC
R0
regre
ssiv
e tum
ort
issue
-
41
00
< 1
03
3.2
6.2
7.9
1.8
5.4
7.2
1.5
pC
R0
rim
: p
se
ud
oca
psu
le+
core
: necro
sis
51
00
< 1
03
6.3
5.0
6.5
1.4
4.3
6.1
0.9
pC
R0
rim
: p
se
ud
oca
psu
le+
core
: necro
sis
61
00
< 1
01
3.3
12
.8A
bse
nt
Ab
se
nt
0.9
Ab
se
nt
Ab
se
nt
pC
R0
reg
ressiv
e t
um
ort
issu
e+
71
00
< 1
01
8.0
4.5
5.9
1.7
7.2
7.4
1.6
pC
R0
rim
: p
se
ud
oca
psu
le+
core
: necro
sis
8 5
05
06
.44
.66
.31
.23
.95
.20
.9p
PR
< 1
0rim
: a
rea
s o
f via
ble
tu
mo
r-
core
: necro
sis
91
00
< 1
01
3.0
4.4
9.1
0.5
4.8
7.4
0.3
pP
R<
10
rim
: a
rea
s o
f via
ble
tu
mo
r
core
: necro
sis
10
100
< 1
04.8
7.0
Absent
Absent
n.p
.n.p
.n.p
.pP
R<
10
are
as o
f via
ble
tum
or
+
11100
< 1
08.0
n.q
.n.q
.n.q
.5.9
Absent
Absent
pP
R<
10
are
as o
f via
ble
tu
mor
+
12
100
< 1
0n.q
.n.p
.n.p
.n.p
.5.8
9.0
1.5
pP
R<
10
rim
: are
as o
f via
ble
tum
or
+
core
: necro
sis
13
100
< 1
012.5
5.0
8.1
1.2
3.6
6.9
1.0
pP
R<
20
rim
: are
as o
f via
ble
tum
or
+
core
: necro
sis
14
50
50
5.0
n.p
.n.p
.n.p
.4.2
Absent
Absent
pP
R50
are
as o
f via
ble
tum
or
+
15
50
50
12.5
9.0
Abse
nt
Absent
10.0
Absent
Absent
pP
R50
are
as o
f via
ble
tu
mor
+
16
50
50
22.5
5.7
10.1
1.0
n.p
.n.p
.n.p
.pP
R50
rim
: are
as o
f via
ble
tum
or
+
core
: necro
sis
17
30
30
3.3
2.9
13.4
1.2
7.1
26.1
1.4
pP
R50
rim
: are
as o
f via
ble
tum
or
+
core
: necro
sis
18
80
40
25.7
n.p
.n.p
.n.p
.11.3
17.3
2.4
pP
R50
rim
: are
as o
f via
ble
tum
or
+
core
: necro
sis
19
100
100
4.3
5.8
Abse
nt
Absent
4.3
Absent
Absent
pP
R100
via
ble
tum
or
+
20
80
< 2
024.2
4.4
8.4
3.0
n.p
.n.p
.n.p
.n.p
.n.p
.n.p
.n.p
.
* =
per
centa
ge
of
tum
or
volu
me
acti
ve
on P
ET
stu
dy;
pC
R =
pat
holo
gic
ally
com
ple
te r
esponse
; pP
R =
pat
holo
gic
ally
par
tial
res
ponse
; n.p
. =
not
per
form
ed;
n.q
. =
no
qu
anti
fica
tio
n

85
FDG-PET to evaluate response to TNF perfusion
Fig 1 Transversal image of a malignant fibrous histiocytoma of the lower leg in Patient 5.
Before perfusion (A) the tumor is clearly depicted as a homogeneous mass with a glucose
uptake of 36.3 µmol/100g tissue/min. Two (B) and 8 weeks after perfusion (C), the glucose
uptake in the tumor decreased to 5.0 and 4.3, respectively. The center of the tumor became
inactive surrounded by an active rim. Pathological examination revealed complete response.
The rim signal corresponded with a fibrotic vascular pseudocapsule with inflammatory tissue
surrounding a core of necrosis.
patient with no change in the percentage of viable tumor after treatment (clinically
this patient showed no response as well). In one patient (5%) the residual tumor was
not excised because of progressive distant disease. This patient died three months
after perfusion and data from this patient are excluded from the remainder of the
analyses.
Forty-nine of the scheduled 60 PET studies were completed (82%). Seven PET studies
were not performed due to patient-related problems. Technical problems prevented
quantification of PET data in four studies. Before perfusion, all tumors were easily
visualized on the baseline FDG-PET images. Twelve patients showed a homogeneous
active tumor on the preperfusion PET study, whereas eight patients also showed
inactive parts in the tumors before perfusion. Visual analysis of the PET images at 2
and 8 weeks after perfusion showed a rim of increased FDG uptake around a core of
absent FDG uptake in 12 patients (5 of 7 pCR, 7 of 12 pPR). The active rim
corresponded in the pCR patients with a fibrotic vascular pseudocapsule with reactive
inflammatory tissue, surrounding a core of absent FDG uptake representing necrosis
(Fig. 1). In patients with pPR, the active rim was found to contain both viable tumor
and an inflammatory response. Thus, the rim signal could correspond with either
viable tumor or a pseudocapsule with an inflammatory reaction. In seven patients
the tumor was visualized after perfusion as a homogeneous mass without the rim-
core configuration (2 of 7 pCR, 5 of 12 pPR). After perfusion, the amount of active
parts in the tumor declined significantly in 11 patients, corresponding with no or less
A B C

86
Chapter 6
than 20 % viable tumor tissue in the pathological specimens in each of these patients.
In two patients (Patients 3, 8) who also showed a good pathological response, the
PET study did not confirm this result. On histological examination, regressive tumor
tissue with an inflammatory reaction was found in Patient 3 and areas of viable tumor
accompanied by inflammatory tissue were found in Patient 8. The PET studies
correctly indicated moderate pathological outcome in six patients. Overall, 17 of 19
responses were correctly indicated by FDG-PET (89%), but the discrimination
between no and small amounts of viable tumor could not be made.
Pre-perfusion glucose consumption in the patients who ultimately had pCR was
significantly higher (p<0.05) than the pPR group (Fig. 2). At 2 and 8 weeks
postperfusion the MRglc in the pCR group had decreased significantly (p<0.05) in
contrast to the MRglc in the pPR group (Fig. 2). The most substantial decrease in
MRglc occurred within 2 weeks after perfusion. Figure 3 shows the percentage of
basal value of the tumor after perfusion. Patients in the pCR group showed a trend
towards a more reduced percentage of basal values than the pPR patients.
Three different histopathological groups could be distinguished after perfusion:
necrotic tissue, represented by the core MRglc of the pCR and pPR group, viable
tumor in combination with an inflammatory response, represented by the rim MRglc
of the pPR group and inflammatory with pseudocapsular tissue, represented by the
rim MRglc of the pCR group. The average MRglc in necrotic tissue was significantly
lower (p<0.05) than the values in tumor and inflammatory tissue, which were in the
same range (Fig. 4).
Fig. 2 MRglc of the tumor with
S.D. before, 2 and 8 weeks after
perfusion. Before perfusion, the
MRglc in the pCR group was sig-
nificantly higher than in the pPR
group (p<0.05). Two and 8 weeks
after perfusion, the MRglc in the
pCR group decreased significantly
(p < 0.05) in contrast to the pPR
group. HILP = hyperthermic iso-
lated limb perfusion.

87
FDG-PET to evaluate response to TNF perfusion
Fig. 3 Percentage of basal value of the
tumor for each patient, 2 and 8 weeks
after perfusion. pCR = pathologically
complete response; pPR = pathologi-
cally partial response; HILP = hyper-
thermic isolated limb perfusion
Fig. 4 MRglc in necrotic, tumor and in-
flammatory tissue. MRglc in necrotic
tissue was significantly lower (p<0.05)
than that in tumor and inflammatory tis-
sue. The latter two could not be discrimi-
nated based on MRglc
Discussion
PET has made it possible to study biochemical changes of cancer tissue and to study
the effect of treatment on metabolism in vivo. The present study demonstrates
substantial decrements in the glucose metabolism of soft-tissue sarcomas with a
pathologically complete response after perfusion with TNF. These changes were
already evident within 2 weeks. In patients with a pPR, this decrease was less
pronounced. An active rim with an inactive core was seen in 13 out of 20 patients
after perfusion. Pathological examination showed that areas of absent intratumoral
FDG uptake were consistent with necrotic tissue. The rim signal represented either
viable tumor or a fibrous pseudocapsule with inflammatory tissue. Unfortunately,
FDG-PET could not discriminate a complete response from a partial response due to
the overlap in glucose metabolism between viable tumor and inflammatory tissue.
An explanation for the observed rim-core pattern can be found in the working
mechanism of TNF. Briefly; TNF exposure invokes an altered endothelial cell
phenotype, anticoagulant mechanisms are suppressed and tissue factor is produced,
which leads to fibrin accumulation at the endothelial cell surface and thrombus

88
Chapter 6
formation in the tumor vessels, causing circulatory stasis and ischemia inside the
tumor followed by necrosis of the tumor cells adjacent to the occluded vessels.31
Necrotic tissue is unable to accumulate FDG and represents the core on the PET
image. The central necrosis elicits an inflammatory response with the formation of a
fibrous pseudocapsule. This is reflected by the rim on the PET image in the pCR
group. On the other hand, peripheral tumor cells may obtain enough nutrients from
the surrounding environment to survive. This is reflected by the rim signal in patients
with pPR. Jones et al. also found an active rim with FDG-PET after neo-adjuvant
chemotherapy of soft-tissue sarcomas. In their patients, the rim signal did not signify
viable tumor but only a fibrous pseudocapsule.32 FDG accumulation in active
inflammatory lesions is in concordance with the observation of Tahara et al. who
found an increased glucose uptake in abdominal abscesses.33 Kubota et al. also found
a high accumulation in macrophages and granulation tissue in a microautoradiographic
study.34 They state that one should consider not only the tumor cells as FDG uptake
source, but also the non-neoplastic cellular elements, that may accompany tumor
growth or necrosis. These phenomena will occur particularly in tumors subjected to
treatment. The fact that both viable tumor and inflammatory tissue accumulate FDG
is one of the major limitations of FDG as the radiopharmaceutical for cancer treatment
evaluation.
One pCR patient showed an elevated MRglc 8 weeks after perfusion, in another pCR
patient, the MRglc did not decrease 2 weeks after perfusion. These observations
could be explained by the inflammatory cell invasion in the tumor. Beside the early
vascular phenomenon, a subsequent immune effect with polymorphonuclear cell
binding to the activated endothelium is another mechanism contributing to the anti-
tumor effect of TNF.35-37 This homing of inflammatory cells in the tumor may be
responsible for a high MRglc after perfusion in these two patients. This is in
concordance with the observation that FDG uptake was diffusely increased in the
remainder of the perfused leg. This phenomenon is thought to be caused by the diffuse
inflammatory reaction that follows perfusion.
Quantitative analysis demonstrated that the pre-perfusion MRglc in the pCR group
was significantly higher than in the pPR group. Thus, high MRglc appears to predict
a good response to TNF perfusion. Since glucose uptake in soft-tissue sarcoma
correlates well with the malignancy grade of the tumor, high grade tumors could be
more susceptible to TNF perfusion.16,17 In 17 of 19 (89%) patients the visual evaluation
of the PET studies corresponded well with the pathological response. In two patients
with a good pathological response, the PET study did not confirm this. In both patients
areas of inflammatory tissue were found on histological examination corresponding
with active areas on the PET scan and therefore resulted in an overestimation of

89
FDG-PET to evaluate response to TNF perfusion
active tumor on the PET scans. Although visual evaluation gave a good indication of
the pathological outcome, the use of FDG-PET in routine clinical monitoring of
response of soft-tissue sarcomas to isolated limb perfusion is hampered by this overlap
between malignant tumor and inflammatory tissue.
Several other investigators have studied whether FDG-PET can be used to monitor
treatment for cancer. FDG uptake was found to decrease as early as 5 days after the
start of systemic therapy for breast cancer. 20,38 A change in FDG uptake was found to
better predict the ultimate outcome than change in tumor size. Decrease in FDG
uptake was more prominent in patients who responded favorably to radiotherapy or
chemotherapy for head and neck cancer compared to non-responding patients.18,39
Similar findings have been reported in other types of tumors and using a variety of
therapeutic schedules.19,40-43 These studies have in common that post-treatment PET
data were correlated with findings of physical examination, radiographic studies or,
at best, fine needle aspiration of the tumor mass, following generally accepted
guidelines.44 In none of these studies have the PET findings been verified by rigorous
microscopic examination of the whole tumor as the gold standard as we have done in
the present study. Our approach appears worthwhile, since change in tumor volume
and viability are not very well correlated. A palpable mass that remains after treatment
may consist of necrosis and fibrosis without viable tumor. On the other hand, viable
tumor may still remain when a palpable tumor that is visible on radiographic images
disappears after treatment. If one wants to investigate whether PET signifies an
improvement over radiographic techniques in the evaluation of treatment, it seems
less appropriate to use those same radiographic techniques as the reference standard.
Our results should be interpreted with caution. Our patient population was limited in
that it was a heterogeneous group of soft-tissue sarcomas and only large tumors were
included (median 8.5 cm). Additional data are needed on FDG-PET in more patients
with other tumor types treated with other drugs. Other PET tracers, such as labeled
aminoacids and 11C-thymidine, may be more suitable to distinguish between tumor
and inflammatory response.
Conclusion
The present study demonstrated that FDG-PET indicates the pathologic tumor
response to chemotherapy in an investigational setting used with isolated limb
perfusion for locally advanced soft-tissue sarcomas. The discrimination between viable
tumor and inflammatory tissue after perfusion treatment, however was hampered by
the limited specificity of FDG. A search for more specific tracers to monitor pathologic
tumor response is needed.

90
Chapter 6
References
1 Mazanet R, Antman KH. Sarcomas of soft tissue and bone. Cancer 1991; 68: 463-
473.
2 Suit HD. Local control and patient survival. Int J Radiat Oncol Biol Phys 1992; 23:
653-660.
3 Sadoski C, Suit HD, Rosenberg A, Mankin H, Efird J. Preoperative radiation, surgical
margins, and local control of extremity sarcomas of soft tissues. J Surg Oncol 1993;
52: 223-230.
4 Hoekstra HJ, Schraffordt Koops H, Molenaar WM, et al. A combination of intraarterial
chemotherapy, preoperative and postoperative radiotherapy, and surgery as limb-
saving treatment of primarily unresectable high-grade soft tissue sarcomas of the
extremities. Cancer 1989; 63: 59-62.
5 Eilber F, Eckardt J, Rosen G, Forscher C, Selch M. Improved complete response
rate with neoadjuvant chemotherapy and radiation for high grade extremity soft tissue
sarcoma. Proc.Am.Soc.Clin.Oncol. 1994; 13: 473 (Abstract).
6 Hoekstra HJ, Schraffordt Koops H, Molenaar WM, Oldhoff J. Results of isolated
regional perfusion in the treatment of malignant soft tissue tumors of the extremities.
Cancer 1987; 60: 1703-1707.
7 Lehti PM, Moseley HS, Janoff K, Stevens K, Fletcher WS. Improved survival for
soft tissue sarcoma of the extremities by regional hyperthermic perfusion, local
excision and radiation therapy. Surg Gynecol Obstet 1986; 162: 149-152.
8 Meyer M, Muchmore JH, Krementz ET. Pre- and perioperative perfusion
chemotherapy for soft tissue sarcoma of the limbs. Cancer Treat Res 1991; 56: 105-
126.
9 Guchelaar HJ, Hoekstra HJ, De Vries EGE, et al. Cisplatin and platinum
pharmacokinetics during hyperthermic isolated limb perfusion for human tumors of
the extremities. Br J Cancer 1992; 65: 898-902.
10 Lienard D, Ewalenko P, Delmotte JJ, Renard N, Lejeune FJ. High-dose recombinant
tumor necrosis factor alpha in combination with interferon gamma and melphalan in
isolation perfusion of the limbs for melanoma and sarcoma. J Clin Oncol 1992; 10:
52-60.
11 Eggermont AMM, Lienard D, Schraffordt Koops H, Rosenkaimer F, Lejeune FJ.
Treatment of irresectable soft tissue sarcomas of the limbs by isolation perfusion
with high dose TNFalfa in combination with interferon-gamma and melphalan. In:
Fiers W, Buurman WA, eds. Tumor Necrosis Factor: Molecular and cellular biology
and clinical relevance. Basel: Karger 1993; 1 edn. 239-243.
12 Strauss LG, Conti PS. The applications of PET in clinical oncology. J Nucl Med
1991; 32: 623-648.
13 Kern KA, Brunetti A, Norton JA, et al. Metabolic imaging of human extremity
musculoskeletal tumors by PET. J Nucl Med 1988; 29: 181-186.
14 Warburg O. On the origin of cancer cells. Science 1956; 123: 309-314.
15 Griffeth LK, Dehdashti F, McGuire AH, et al. PET evaluation of soft-tissue masses
with fluorine-18 fluoro-2- deoxy-D-glucose. Radiology 1992; 182: 185-194.
16 Adler LP, Blair HF, Makley JT, et al. Noninvasive grading of musculoskeletal tumors
using PET. J Nucl Med 1991; 32: 1508-1512.

91
FDG-PET to evaluate response to TNF perfusion
17 Nieweg OE, Pruim J, van Ginkel RJ, et al. Fluorine-18-fluorodeoxyglucose PET
imaging of soft-tissue sarcoma. J Nucl Med 1996; 37: 257-261.
18 Minn H, Paul R, Ahonen A. Evaluation of treatment response to radiotherapy in
head and neck cancer with fluorine-18-fluorodeoxyglucose. J Nucl Med 1988; 29:
1521-1525.
19 Ichiya Y, Kuwabara Y, Otsuka M, et al. Assessment of response to cancer therapy
using fluorine-18- fluorodeoxyglucose and positron emission tomography. J Nucl
Med 1991; 32: 1655-1660.
20 Wahl RL, Zasadny K, Helvie M, et al. Metabolic monitoring of breast cancer
chemohormonotherapy using positron emission tomography: initial evaluation. J
Clin Oncol 1993; 11: 2101-2111.
21 Enzinger FM and Weiss SW. Soft tissue tumors. St Louis, Missouri, U.S.A.: Mosby,
1988: 2 edn.
22 Coindre JM, Trojani M, Contesso G, et al. Reproducibility of a histopathologic
grading system for adult soft tissue sarcoma. Cancer 1986; 58: 306-309.
23 Creech O, Krementz ET, Ryan RF, Winblad JN. Chemotherapy of cancer: regional
perfusion utilizing an extra-corporeal circuit. Ann Surg 1958; 148: 616-632.
24 Fontijne WP, Mook PH, Schraffordt Koops H, Oldhoff J, Wildevuur CR. Improved
tissue perfusion during pressure regulated regional perfusion: a clinical study. Cancer
1985; 55: 1455-1461.
25 Wieberdink J, Benckhuysen C, Braat RP, Van Slooten EA, Olthuis GAA. Dosimetry
in isolation perfusion of the limb by assessment of perfused tissue volume and grading
of toxic tissue reactions. Eur J Cancer Clin Oncol 1982; 18: 905-910.
26 Schraffordt Koops H. Prevention of neural and muscular lesions during hyperthermic
regional perfusion. Surg Gynecol Obstet 1972; 135: 401-403.
27 Hamacher K, Coenen HH, Stöcklin G. Efficient stereospecific synthesis of no-carrier-
added 18F-fluoro-2-deoxy-D-glucose using aminopolyether supported nucleophilic
substitution. J Nucl Med 1986; 27: 235-238.
28 Patlak CS, Blasberg RG, Fenstermacher JD. Graphical evaluation of blood-to-brain
transfer constants from multiple-time uptake data. J Cereb Blood Flow Metab 1983;
3: 1-7.
29 Patlak CS, Blasberg RG. Graphical evaluation of blood-to-brain transfer constants
from multiple-time uptake data. Generalizations. J Cereb Blood Flow Metab 1985;
5: 584-590.
30 Winer BJ. Statistical principles in experimental design. New York: McGraw Hill,
1971: 2 edn.
31 Nawroth P, Handley D, Matsueda G, et al. Tumor necrosis factor/cachectin-induced
intravascular fibrin formation in meth A fibrosarcomas. J Exp Med 1988; 168: 637-
647.
32 Jones DN, Brizel DM, Charles HC, et al. Monitoring of response to neoadjuvant
therapy of soft tissue and musculoskeletal sarcomas using F18-FDG-PET.
J.Nucl.Med. 1994; 38P (Abstract).
33 Tahara T, Ichiya Y, Kuwabara Y, et al. High [18F]-fluorodeoxyglucose uptake in
abdominal abscesses: a PET study. J Comput Assist Tomogr 1989; 13: 829-831.
34 Kubota R, Yamada S, Kubota K, et al. Intratumoral distribution of fluorine-18-
fluorodeoxyglucose in vivo: high accumulation in macrophages and granulation
tissues studied by microautoradiography. J Nucl Med 1992; 33: 1972-1980.

92
35 Palladino MAJR, Shalaby MR, Kramer SM, et al. Characterization of the antitumor
activities of human tumor necrosis factor-? and the comparison with other cytokines:
induction of tumor-specific immunity. J Immunol 1987; 138 : 4023-4032.
36 Gamble JR, Harlan JM, Klebanoff SJ, Vadas MA. Stimulation of the adherence of
neutrophils to umbilical vein endothelium by human recombinant tumor necrosis
factor. Proc Natl Acad Sci U S A 1985; 82: 8667-8671.
37 Renard N, Lienard D, Lespagnard L, et al. Early endothelium activation and
polymorphonuclear cell invasion precede specific necrosis of human melanoma and
sarcoma treated by intravascular high-dose tumor necrosis factor alpha (TNF). Int J
Cancer 1994; 57: 656-663.
38 Nieweg OE, Wong WH, Singletary SE, Hortobagyi GN, Kim EE. Positron emission
tomography of glucose metabolism in breast cancer. Potential for tumor detection,
staging, and evaluation of chemotherapy. Ann N Y Acad Sci 1993; 698: 423-428.
39 Haberkorn U, Strauss LG, Dimitrakopoulou A, et al. Fluorodeoxyglucose imaging
of advanced head and neck cancer after chemotherapy. J Nucl Med 1993; 34: 12-17.
40 Haberkorn U, Strauss LG, Dimitrakopoulou A, et al. PET studies of
fluorodeoxyglucose metabolism in patients with recurrent colorectal tumors receiving
radiotherapy. J Nucl Med 1991; 32: 1485-1490.
41 Strauss LG, Dimitrakopoulou A, Haberkorn U, Ostertag H, Helus F, Lorenz WJ.
PET studies with FDG in patients with metastatic melanoma prior and after therapy.
Eur.J.Nucl.Med. 1991; 18: 685 (Abstract).
42 Abe Y, Matsuzawa T, Fujiwara T, et al. Clinical assessment of therapeutic effects on
cancer using 18F-2- fluoro-2-deoxy-D-glucose and positron emission tomography:
preliminary study of lung cancer. Int J Radiat Oncol Biol Phys 1990; 19: 1005-
1010.
43 Bares R, Horstmann K, Altehoefer C, et al. FDG-PET to assess local effects of
radiation or chemotherapy in patients with malignant lymphoma. J.Nucl.Med. 1991;
32: 918 (Abstract).
44 Miller AB, Hoogstraten B, Staquet M, Winkler A. Reporting results of cancer
treatment. Cancer 1981; 47: 207-214.

93
Robert J. van Ginkel1
Annemieke C. Kole2
Omgo E. Nieweg1,3
Willemina M. Molenaar4
Jan Pruim2
Heimen Schraffordt Koops1
Wim Vaalburg2
Harald J. Hoekstra1
Department of Surgical Oncology1, PET Center2 and Department of Pathology4,
University Groningen Hospital, The Netherlands and Department of Surgery3, The
Netherlands Cancer Institute, Amsterdam, The Netherlands.
Journal of Nuclear Medicine 1999; 40: 262-267.
L-[1-11C]-Tyrosine PET to evaluate response to
hyperthermic isolated limb perfusion for locally
advanced soft-tissue sarcoma & skin cancer

94
Chapter 7
Abstract
PET with L-[1-11C]-tyrosine (TYR) was investigated in patients undergoing
hyperthermic isolated limb perfusion (HILP) with recombinant tumor necrosis factor
alpha (TNF) and melphalan for locally advanced soft-tissue sarcoma and skin cancer
of the lower limb. Seventeen patients (5 women, 12 men; age range 24-75 y; mean
age 52 y) were studied. TYR-PET studies were performed before HILP, and 2 and 8
weeks afterwards. The protein synthesis rates (PSR) in nanomoles per milliliter per
minute were calculated. After the final PET study, the tumor was resected and
pathologically examined. Patients with a pathologically complete response (pCR)
showed no viable tumor after treatment. Those with a pathologically partial response
(pPR) showed various amounts of viable tumor in the resected tumor specimens. Six
patients showed a pCR (35%) and 11 patients showed a pPR (65%). All tumors were
depicted as a hot spot on the PET study before HILP. The PSR in the pCR group at 2
and 8 weeks after perfusion had decreased significantly (p<0.05) compared to the
PSR before HILP. A significant difference was found in PSR between the pCR and
pPR group at 2 as well as at 8 week (p<0.05). Median PSR in nonviable tumor tissue
was 0.62 and ranged from 0.22 to 0.91. With a threshold PSR of 0.91, sensitivity and
specificity of TYR-PET were 82% and 100%, respectively. The predictive value of a
PSR > 0.91 for having viable tumor tissue after HILP was 100%, whereas the
predictive value of a PSR ≤0.91 for having nonviable tumor tissue after HILP was
75%. On pathological examination the 2 patients in the pPR group with a
PSR < 0.91 showed microscopic islets of tumor cells surrounded by extensive necrosis.
Based on the calculated PSR after HILP, TYR-PET gave a good indication of the
pathological outcome. Inflammatory tissue after treatment did not interfere with viable
tumor tissue on the images, suggesting that it may be worthwhile to pursue TYR-PET
in other therapy evaluation settings.
Introduction
Different metabolic processes such as glycolysis, protein synthesis, uptake of
disaccharides and transamination, are enhanced in tumors when compared to normal
tissues. PET enables visualization and quantification of metabolic processes in vivo.18Fluorine-labeled 2-fluoro-2-deoxy-D-glucose (FDG) is the most commonly used
radiopharmaceutical for PET and has proven to be of value to visualize various types
of solid tumors, to indicate the malignancy grade and to detect locally recurrent
disease.1-4 Various clinical reports suggest the feasibility of FDG-PET to assess tumor
response to radiotherapy and chemotherapy.5-7 A limitation of FDG-PET in therapy
evaluation is the inability to differentiate between viable tumor tissue and
inflammatory tissue.8-10 Therefore, there is a need for alternatives. Ishiwata et al.11
95
TYR-PET to evaluate response to TNF perfusion
have shown that the uptake of amino acids is high in tumor tissue due to an increased
protein synthesis rate (PSR). Amino acids play a minor role in the metabolism of
inflammatory cells, mainly neutrophils, compared to FDG. Most amino acid PET
studies have been performed with L-[methyl-11C]-methionine (MET).12-14 MET reflects
amino acid uptake rather than protein synthesis because it is involved in other
metabolic pathways such as transmethylation and polyamine synthesis.15,16 This
complicated metabolism of methionine has made it impossible to create a precise
metabolic model. Carboxyl-labeled amino acids, such as L-[1-11C]-tyrosine (TYR),
L-[1-11C]-methionine and L-[1-11C]-leucine, appear to be more appropriate compounds
to determine protein synthesis in tumors.16,17 The main metabolite of these amino
acids is 11CO2, which is rapidly cleared from tissue and exhaled and does not contribute
to the PET-measured 11C radioactivity in tumor tissue.
A model was developed to determine the PSR in tumor tissue using TYR.18 Initial
results in patients with brain tumors have been published recently.19 Kole et al. 20
reported a high uptake of TYR and, as a consequence, a high PSR in various types of
malignancies and low uptake in benign lesions. PET with TYR may be of value in
the assessment of the response of a malignant tumor to therapy, because a decrease
in tissue viability may result in a decrease in PSR.
Hyperthermic isolated limb perfusion (HILP) with recombinant tumor necrosis factor
alpha (TNF) and melphalan can usually prevent amputation in patients with locally
advanced soft-tissue sarcoma or extensive local regional melanoma.21,22 The aim of
this study was to investigate PET with TYR in patients undergoing HILP for locally
advanced soft-tissue sarcoma and skin cancer and to correlate PET findings with
histology before and after treatment.
Materials and methods
Patients
Seventeen patients (5 women, 12 men; aged 24-75 yrs; mean age 52 yrs) with biopsy-
proven soft-tissue sarcoma or melanoma participated in the study approved by the
Medical Ethical Committee of the institute. Informed consent was obtained from
each patient. Ten patients presented with a newly diagnosed soft-tissue sarcoma, 2
patients presented with a local recurrence of a soft-tissue sarcoma previously treated
with surgery alone, 4 patients presented with a melanoma and 1 patient presented
with a squamous cell carcinoma. All tumors were located in the lower limb. The
diagnosis of the tumors was determined in a standard fashion and soft-tissue sarcomas
were graded according to Coindre et al.23 All tumors were considered primarily
irresectable because of size, multicentricity in the limb, or fixation to the neurovascular
bundle or bone. Median tumor size was 10 cm (range 3-25 cm). Patients and tumor
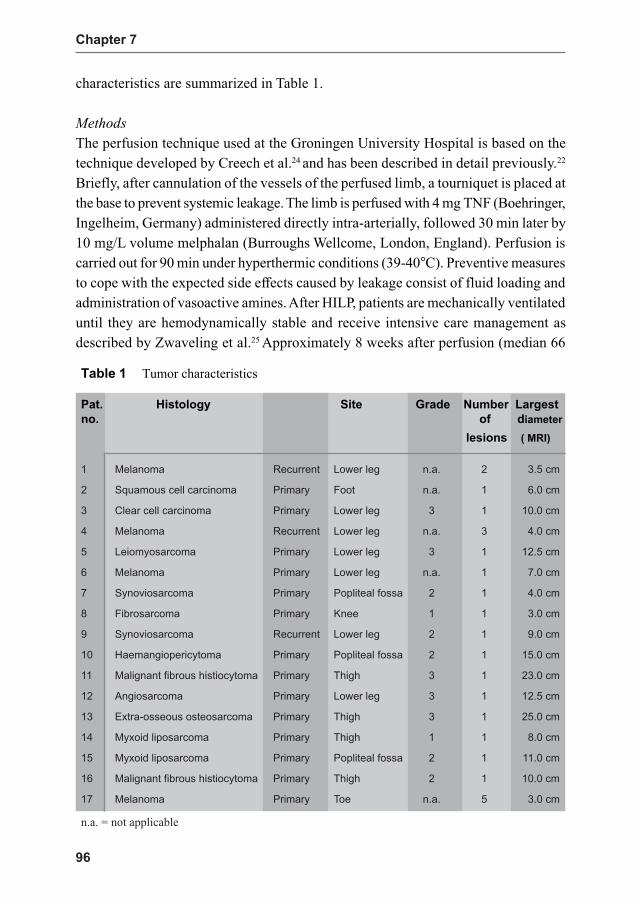
96
Chapter 7
characteristics are summarized in Table 1.
Methods
The perfusion technique used at the Groningen University Hospital is based on the
technique developed by Creech et al.24 and has been described in detail previously.22
Briefly, after cannulation of the vessels of the perfused limb, a tourniquet is placed at
the base to prevent systemic leakage. The limb is perfused with 4 mg TNF (Boehringer,
Ingelheim, Germany) administered directly intra-arterially, followed 30 min later by
10 mg/L volume melphalan (Burroughs Wellcome, London, England). Perfusion is
carried out for 90 min under hyperthermic conditions (39-40°C). Preventive measures
to cope with the expected side effects caused by leakage consist of fluid loading and
administration of vasoactive amines. After HILP, patients are mechanically ventilated
until they are hemodynamically stable and receive intensive care management as
described by Zwaveling et al.25 Approximately 8 weeks after perfusion (median 66
Table 1 Tumor characteristics
Pat. Histology Site Grade Number Largest
no. of diameter
lesions ( MRI)
1 Melanoma Recurrent Lower leg n.a. 2 3.5 cm
2 Squamous cell carcinoma Primary Foot n.a. 1 6.0 cm
3 Clear cell carcinoma Primary Lower leg 3 1 10.0 cm
4 Melanoma Recurrent Lower leg n.a. 3 4.0 cm
5 Leiomyosarcoma Primary Lower leg 3 1 12.5 cm
6 Melanoma Primary Lower leg n.a. 1 7.0 cm
7 Synoviosarcoma Primary Popliteal fossa 2 1 4.0 cm
8 Fibrosarcoma Primary Knee 1 1 3.0 cm
9 Synoviosarcoma Recurrent Lower leg 2 1 9.0 cm
10 Haemangiopericytoma Primary Popliteal fossa 2 1 15.0 cm
11 Malignant fibrous histiocytoma Primary Thigh 3 1 23.0 cm
12 Angiosarcoma Primary Lower leg 3 1 12.5 cm
13 Extra-osseous osteosarcoma Primary Thigh 3 1 25.0 cm
14 Myxoid liposarcoma Primary Thigh 1 1 8.0 cm
15 Myxoid liposarcoma Primary Popliteal fossa 2 1 11.0 cm
16 Malignant fibrous histiocytoma Primary Thigh 2 1 10.0 cm
17 Melanoma Primary Toe n.a. 5 3.0 cm
n.a. = not applicable

97
TYR-PET to evaluate response to TNF perfusion
days, range 27-125 days) the residual tumor masses were excised and pathologically
examined. The tumor remnants were measured in three dimensions and the percentage
of necrosis estimated. Representative tumor sections were taken, encompassing
macroscopically different tumor areas including necrosis. As a general rule, one section
per centimeter largest diameter with a minimum of three was taken. Based on an
integration of gross and microscopic findings, a final estimate of the percentages of
viable and necrotic or regressive tumor was made. If possible, macroscopic
examination and tissue sampling was performed based on the latest PET images.
The results were classified as either pathologically complete response (pCR) or
pathologically partial response (pPR), when remaining viable tumor was noted.
PET imaging
Patients were scheduled for three PET studies: shortly before perfusion (n = 17,
median 10 days, range 1 - 23 days), 2 weeks after perfusion (n = 14, median 16 days,
range 12 - 23 days) and shortly before resection of residual tumor tissue (n = 15,
median 55 days, range 47 - 68 days after perfusion). TYR was produced by a modified
microwave-induced Bücherer-Strecker synthesis26 , with a radiochemical purity of
more than 99%. PET sessions were performed using an ECAT 951/31 PET camera
(Siemens/CTI, Knoxville, USA).
All patients fasted for at least 8 hours before the investigation. Serum tyrosine levels
were measured before each PET session and were found to be normal (mean 0.053
mmol/L, range 0.028 - 0.1 mmol/L). A 20-gauge needle was inserted into the radial
artery under local anesthesia. In the contralateral arm, an intravenous canula was
inserted in the cephalic vein for the injection of TYR. The patients were positioned
supine in the camera, with the tumor in the field of view based on physical
examination.
After attenuation scanning using a 68Ge/68Ga source, we administered a mean dose of
322 MBq (range 126 - 381 MBq) TYR intravenously over 1 min. Dynamic images
were acquired from the time of injection following a dynamic protocol (ten 0.5 min,
three 5 min, three 10 min) for a total duration of 50 min. Simultaneously, 2-ml blood
samples were taken from the arterial canula (time points 0.25, 0.5, 0.75, 1.0, 1.25,
1.5, 1.75, 2.25, 2.45, 3.75, 4.75, 7.5, 12.5, 17.5, 25, 35, and 45 min postinjection).
The blood samples were centrifuged and plasma activity of TYR, the 11C-labeled
CO2 and protein levels were measured by high-performance liquid chromatography
(HPLC). The duration of the imaging procedure was approximately 2.5 h.

98
Chapter 7
Data analysis
Images were displayed in coronal, sagittal and transaxial projections on a computer
display using standard ECAT software and were interpreted independently by two
experienced physicians. To determine tumor PSR, one must first define the tumor in
all relevant tomographic planes of the study. Usually this is done by placing regions
of interest (ROIs) in each plane, matching the size of the tumor as outlined by MRI.
The tissue time-activity curves obtained from these ROIs can be averaged and the
average PSR can be calculated. Because this technique is rather laborious, an
alternative method was developed at our institute. By using the same activity threshold
as the one used to define the ROI, we selected all voxels in the study above this
threshold. For each analysis, a fixed percentage of 95% was used. The corresponding
activity was summed and the average time-activity curve and the total volume were
obtained. The advantage of this approach is that the analysis of the whole tumor is
performed quickly and simply and the results are identical to those of the ROI method.
Parts of the tumor that do not accumulate TYR are ignored by this method. By
combining this averaged time-activity data with the plasma input data (corrected for11CO
2 and 11C-proteins), we calculated the average PSR in nanomoles per milliliter
tumor tissue per minute using the modified Patlak analysis as described previously.18
The PSR in contralateral normal tissue was calculated using a ROI technique. A
tumor-to-nontumor ratio (T/N ratio) was calculated from the PSR in tumor tissue
and the PSR in contralateral normal tissue. The change in PSR after perfusion was
related to the preperfusional value and was expressed as a percentage of basal value.
Statistical analysis
The statistical procedures included a two-factor experiment with repeated measures
on one factor to compare PSR between measures and groups. Analyses were performed
on data sets corrected for missing data according to Winer.27 Post hoc comparison
was made with Student´s t-tests. A p value < 0.05 was considered significant. Analysis
was carried out by SPSS.
Results
PET results and pathological response for each patient are summarized in Table 2.
Pathological examination of the residual tumor mass showed no viable tumor in 6
patients (pCR 35%), 3 of whom had a melanoma. In 11 patients, variable amounts of
viable tumor were found at pathological examination (pPR 65%). Forty-six of the
scheduled 51 PET studies were completed (90%). Five PET studies were not
performed due to patient-related problems. All tumors were depicted as a hot spot on
the PET study before HILP with variable degrees of TYR accumulating parts (T/N

99
TYR-PET to evaluate response to TNF perfusion
Ta
ble
2P
ET
results an
d p
atholo
gical resp
onse
Pro
tein
sy
nth
es
is ra
te (n
mo
l/ml/m
in) P
ath
olo
gic
al e
va
lua
tion
Pa
t. Be
fore
HIL
P 2
we
ek
s a
fter H
ILP
8 w
ee
ks
afte
r HIL
P R
es
po
ns
e %
Via
ble
Ma
cro
/mic
ro-s
co
pic
vie
w
no
. Tu
mo
r Co
ntra
lat T
/N ra
tio T
um
or C
on
trala
t T/N
ratio
Tu
mo
r Co
ntra
lat T
/N ra
tio tu
mo
r
12.4
50.1
417.5
0.1
70.1
41
.20.2
20.4
10.5
pC
R0
Rim
with
infla
mm
ato
ry tis
sue
23.5
10.1
523.4
1.0
20.1
66
.40.9
10.2
04.6
pC
R0
Infla
mm
ato
ry tis
sue
32
.53
0.4
35
.9n
.p.
n.p
.n
.p.
0.5
00
.31
1.6
pC
R0
Infla
mm
ato
ry tis
su
e
42.0
60
.40
5.2
0.7
40.2
62
.9n
.p.
n.p
.n
.p.
pC
R0
Infla
mm
ato
ry tis
su
e
52.1
30.4
15.2
0.7
10.2
33
.10.8
50.2
04.3
pC
R0
Rim
with
infla
mm
ato
ry tis
sue
61.3
10.4
03
.30.6
20.2
72.3
0.3
50.2
11
.7pC
R0
Infla
mm
ato
ry tis
sue
72.0
60.2
48
.61.3
90.4
33.2
0.4
80.2
91
.7pP
R<
10
Mic
roscopic
isle
ts o
f via
ble
tum
or
81.7
60.2
57
.00.6
40.2
62.5
0.8
00.2
13
.8pP
R<
10
Mic
roscopic
isle
ts o
f via
ble
tum
or
90.9
20.3
32
.8n.p
.n.p
.n.p
.0.9
90.3
23.1
pP
R<
10
Mic
rosco
pic
isle
ts o
f via
ble
tum
or
10
2.0
00.2
38.7
2.3
00.3
07
.71.4
60.2
26.6
pP
R<
10
Are
as o
f via
ble
tum
or
11
2.3
00.2
68.9
1.2
60.1
87
.02.3
10.1
614.4
pP
R<
10
Are
as o
f via
ble
tum
or
12
5.2
70.2
521.1
2.7
90.1
815.5
n.p
.n
.p.
n.p
.pP
R<
10
Are
as o
f via
ble
tum
or
13
1.6
80
.17
9.9
n.p
.n
.p.
n.p
.3.9
10.4
88
.2pP
R<
20
Rim
with
via
ble
tum
or
14
0.7
30.2
43.4
1.6
10.4
73
.41.8
30.4
83.8
pP
R<
50
Are
as o
f via
ble
tum
or
15
0.6
40.2
42.7
1.3
50.3
34
.12.1
30.6
03.6
pP
R<
50
Are
as o
f via
ble
tum
or
16
2.9
00.4
66.3
1.4
70.4
33
.42.4
80.3
18.0
pP
R<
50
Are
as o
f via
ble
tum
or
17
1.6
10.2
46.7
1.2
40.0
913.8
0.9
40.0
811
.8pP
R<
50
Via
ble
tum
or
Contra
lat =
contra
late
ral n
orm
al tis
sue; p
CR
= p
ath
olo
gic
ally
com
ple
te re
sponse; p
PR
= p
ath
olo
gic
ally
partia
l response; n
.p. =
not p
erfo
rmed

100
Chapter 7
ratio > 1.00 in all patients). Preperfusion PSR in the patients who ultimately went on
to have a pCR was not significantly different from the PSR in the pPR group
(Fig.1). Analysis of the PET images at 2 and 8 weeks after perfusion showed a decrease
of TYR accumulating parts in all pCR patients.
Fig. 1 Protein synthesis rate (PSR) of
tumor with S.D. before, 2 and 8 weeks
after perfusion. Two and 8 weeks after
perfusion, PSR in pathologically com-
plete response (pCR) group decreased
significantly (p<0.05) in contrast with
PSR in pathologically partial response
(pPR) group. Significant difference
was found in PSR between the pCR and
pPR groups at 2 and 8 weeks (p<0.05).
HILP = hyperthermic isolated limb
perfusion
The PSR in the pCR group had decreased significantly at 2 and 8 weeks after perfusion
compared with preperfusional values (p<0.05) in contrast to the PSR in the pPR
group. A significant difference was found in PSR between the pCR and pPR group at
2 as well as at 8 weeks (p<0.05). The most substantial decrease in PSR occurred
within 2 weeks after perfusion. Figure 2 illustrates the succeeding PET studies in
patient 11. After an initial decrease in PSR at 2 wk, a renewed outgrow of the tumor
was observed at 8 weeks after perfusion. Necrosis within the tumor was visualized
as a cold spot. In this patient, TYR-PET indicated the need for an early resection of
the tumor as perfusion did not seem to have the desired result. Pathological
examination revealed areas of viable tumor that encompassed less than 10% of the
total tumor volume.
The median PSR in contralateral muscle tissue was 0.28 and ranged from 0.08 to
0.60. PSR in tumor tissue was higher than in the corresponding contralateral normal
tissue (p<0.05). Median PSR in nonviable tumor tissue was 0.62 and ranged from
0.22 to 0.91. With a threshold PSR of 0.91, the highest value obtained from nonviable
tumor tissue, the sensitivity and specificity of TYR-PET after HILP treatment were
82% and 100%, respectively. The predictive value of a PSR > 0.91 for having viable
tumor after HILP was 100%, whereas the predictive value of a PSR ≤ 0.91 for having
nonviable tumor tissue after HILP was 75% (Fig. 3). The two patients in the pPR
group with a PSR < 0.91, patients 8 and 9, showed microscopic islets of tumor cells
surrounded by extensive necrosis on pathological examination. With a threshold PSR
of 0.48, the lowest value obtained from viable tumor tissue, the sensitivity and

101
TYR-PET to evaluate response to TNF perfusion
specificity of TYR-PET after HILP treatment were 100% and 33%, respectively.
The predictive values for viable and nonviable tumor tissue after HILP were 73%
and 100%, respectively.
Figure 4 shows the percentage of basal value of the tumor after perfusion. All patients
in the pCR group showed a reduction of PSR whereas some pPR patients showed a
reduction and others an increase in PSR after perfusion. The reduction in the pCR
group was significant at 2 and 8 weeks after perfusion. However, based on a certain
percentage of reduction of basal value, no assumption could be made as to whether
or not the individual patient showed a pCR or a pPR.
Two different histopathological groups could be distinguished after perfusion:
nonviable tumor tissue, corresponding with inflammatory tissue, and viable tumor
tissue. Figure 5 shows the PSR in these two different histopathological groups
Fig 2. Transversel PET image of a patient with a malignant fibrous histiocytoma of the thigh
(patient 11). Before perfusion (A) the tumor is clearly depicted as a heterogeneous mass with
a PSR of 2.30 nmol/ml/min. After initial reduction in PSR (1.26) at 2 weeks after perfusion
(B), the malignant fibrous histiocytoma showed renewed growth (PSR 2.31) at 8 weeks after
perfusion (C). The gray scale equates a particular hue to a particular PSR in nmol/ml/min.
PA viable PA Nonviable Total
PET Viable 9 0 9
PET Nonviable 2 6 8
Total 11 6 17
Fig 3. Cross tabulation table with threshold PSR of 0.91. Sensitivity and specificity of TYR-
PET were 82% and 100%, respectively. Predictive value for viable tumor after HILP was
100%, whereas predictive value for nonviable tumor tissue after HILP was 75%. Two patients
in the pPR group with PSR<0.91, showed microscopic islets of tumor cells surrounded by
extensive necrosis on pathological examination. PA = pathology
A B C

102
Chapter 7
compared with the PSR in normal contralateral muscle. The average PSR in
inflammatory tissue was significantly lower than the PSR values in viable tumor
tissue (p<0.05).
Discussion
PET has made it possible to study biochemical changes of cancer tissue and to study
the effect of treatment on metabolism in vivo. This study demonstrates a significant
decline in the protein metabolism of locally advanced soft-tissue sarcomas and skin
cancer with a pathologically complete response after HILP with TNF and melphalan.
These changes were already evident within 2 weeks. In patients with a pPR, this
decrease was not significant. These findings are similar to the results of a previous
study performed in the same manner with FDG.9 With TYR-PET, however, there
was a significant difference at 2 and at 8 weeks in PSR between the pCR and pPR
groups, a finding that was not observed with FDG-PET. That previous finding may
have been caused by the fact that FDG is also accumulated by inflammatory tissue,
resulting in an overlap in glucose metabolism between viable tumor and inflammatory
tissue. In this study, TYR was also accumulated by inflammatory tissue that existed
Fig. 4 Percentage of basal value of tu-
mor for all patients 2 and 8 weeks after
perfusion. pCR = pathologically com-
plete response; pPR = pathologically
partial response; HILP = hyperthermic
isolated limb perfusion
Fig. 5 Protein synthesis rate (PSR) in
viable tumor, inflammatory and con-
tralateral normal tissue. PSR in viable
tumor tissue was significantly higher
than inflammatory tissue (p<0.05)

103
TYR-PET to evaluate response to TNF perfusion
after HILP but was accumulated significantly less than in viable tumor tissue. Because
TYR can better discriminate between viable tumor tissue and inflammatory tissue
than FDG, TYR is a more reliable technique to evaluate treatment response. The
major question for clinicians is the exact timing for the surgical resection after HILP
because the tumoricidal effect of HILP seems to be time related. If the threshold PSR
of 0.91 was exceeded 8 weeks after HILP, we could with certainty predict that viable
tumor was still present and surgical resection of the tumor remnants was indicated.
However, when resection was omitted with a PSR less than 0.91, there was a 25%
chance of leaving microscopic islets of tumor tissue. The resolution of the PET camera
may be the limiting factor in detecting these microscopic islets of viable tumor,
although it remains questionable if these small amounts of tumor tissue surrounded
by avascular necrosis can lead to a local recurrence. Instead of surgical resection,
these patients could possibly also be treated with external beam radiotherapy, and
monitored closely for development of a local recurrence. Leaving residual tumor
mass was safe when PSR was lower than 0.48 after HILP.
Before perfusion, there was no significant difference in PSR between the patients in
the pCR and pPR group. This was in contrast with the results of the FDG study
where we found a significant difference in glucose consumption before perfusion
between both groups.9 So TYR can not be used to predict the likelihood of a response
to HILP. For FDG we also found a correlation between tumor malignancy grade and
the level of glucose metabolism.3 This is not the case for the protein synthesis of the
different grades of soft-tissue sarcomas in this study but the number of patients is
small. This difference between FDG and TYR may be explained by the fact that
FDG is trapped inside the cell as a result of an increased level of glucose transporters
on the cell membrane.28 FDG accumulates as it reaches its end in its metabolic pathway
as FDG-6-phosphate; the more glucose transports there are on the cell membrane,
the more FDG is incorporated in the cell, corresponding with a high malignancy
grade. TYR, not hampered by an anorganic isotope, continues its metabolic pathway
and is not accumulated in the cell.
Combining the results of this study with the results of our previous FDG study, it is
tempting to state that FDG-PET should be performed before HILP to identify patients
who will most likely benefit from this treatment and TYR-PET should be performed
8 weeks after HILP to evaluate the outcome of the therapy. However, our results
should be interpreted with caution since this patient population is a small group of
heterogeneous soft-tissue sarcomas and skin cancers and only large tumors were
included. Additional data are needed on TYR-PET in more patients with other tumor
types treated with other chemotherapeutic agents and pathological examination as
the gold standard.

104
Chapter 7
Conclusion
This study demonstrates that TYR-PET indicates the pathologic tumor response to
chemotherapy in an investigational setting used with HILP with TNF and melphalan
for locally advanced tumors. Based on the calculated PSR after perfusion, a good
indication was found towards the pathological outcome. Inflammatory tissue after
treatment did not interfere with viable tumor on the images, suggesting that it may be
worthwhile to pursue TYR-PET in other therapy evaluation settings.
References
1 Conti PS, Lilien DL, Hawley K, et al. PET and [18F]-FDG in oncology: a clinical
update. Nucl Med Biol 1996; 23: 717-735.
2 Rigo P, Paulus P, Kaschten BJ, et al. Oncological applications of positron emission
tomography with fluorine-18 fluorodeoxyglucose. Eur J Nucl Med 1996; 23: 1641-
1674.
3 Nieweg OE, Pruim J, van Ginkel RJ, et al. Fluorine-18-fluorodeoxyglucose PET
imaging of soft-tissue sarcoma. J Nucl Med 1996; 37: 257-261.
4 Kole AC, Nieweg OE, van Ginkel RJ, et al. Detection of local recurrence of soft-
tissue sarcoma with positron emission tomography using [18F]fluorodeoxyglucose.
Ann Surg Oncol 1997; 4: 57-63.
5 Findlay M, Young H, Cunningham D, et al. Noninvasive monitoring of tumor
metabolism using fluorodeoxyglucose and positron emission tomography in colorectal
cancer liver metastases: correlation with tumor response to fluorouracil [see
comments]. J Clin Oncol 1996; 14: 700-708.
6 Jones DN, McCowage GB, Sostman HD, et al. Monitoring of neoadjuvant therapy
response of soft-tissue and musculoskeletal sarcoma using fluorine-18-FDG-PET.
Blood 1996; 37: 1438-1444.
7 Lindholm P, Leskinen Kallio S, Grenman R, et al. Evaluation of response to
radiotherapy in head and neck cancer by positron emission tomography and
[11C]methionine. Int J Radiat Oncol Biol Phys 1995; 32: 787-794.
8 Kubota R, Yamada S, Kubota K, et al. Intratumoral distribution of fluorine-18-
fluorodeoxyglucose in vivo: high accumulation in macrophages and granulation
tissues studied by microautoradiography. J Nucl Med 1992; 33: 1972-1980.
9 van Ginkel RJ, Hoekstra HJ, Pruim J, et al. FDG-PET to evaluate response to
hyperthermic isolated limb perfusion for locally advanced soft-tissue sarcoma. J
Nucl Med 1996; 37: 984-990.
10 Lewis PJ, Salama A. Uptake of fluorine-18-fluorodeoxyglucose in sarcoidosis. J
Nucl Med 1994; 35: 1647-1649.
11 Ishiwata K, Vaalburg W, Elsinga PH, Paans AM, Woldring MG. Metabolic studies
with L-[1-14C]tyrosine for the investigation of a kinetic model to measure protein
synthesis rates with PET. J Nucl Med 1988; 29: 524-529.
12 Schober O, Meyer GJ, Duden C, et al. [Amino acid uptake in brain tumors using
positron emission tomography as an indicator for evaluating metabolic activity and
malignancy]. ROFO Fortschr Geb Rontgenstr Nuklearmed 1987; 147: 503-509.

105
TYR-PET to evaluate response to TNF perfusion
13 Derlon JM, Bourdet C, Bustany P, et al. [11C]L-methionine uptake in gliomas.
Neurosurgery 1989; 25: 720-728.
14 Lilja A, Lundqvist H, Olsson Y, et al. Positron emission tomography and computed
tomography in differential diagnosis between recurrent or residual glioma and
treatment-induced brain lesions. Acta Radiol 1989; 30: 121-128.
15 Daemen BJ, Elsinga PH, Ishiwata K, Paans AM, Vaalburg W. A comparative PET
study using different 11C-labelled amino acids in Walker 256 carcinosarcoma-bearing
rats. Int J Rad Appl Instrum [B] 1991; 18: 197-204.
16 Ishiwata K, Vaalburg W, Elsinga PH, Paans AM, Woldring MG. Comparison of L-
[1-11C]methionine and L-methyl-[11C]methionine for measuring in vivo protein
synthesis rates with PET. J Nucl Med 1988; 29: 1419-1427.
17 Bolster JM, Vaalburg W, Paans AM, et al. Carbon-11 labelled tyrosine to study
tumor metabolism by positron emission tomography (PET). Eur J Nucl Med 1986;
12: 321-324.
18 Willemsen ATM, van Waarde A, Paans AM, et al. In vivo protein synthesis rate
determination in primary or recurrent brain tumors using L-[1-11C]-tyrosine and
PET. J Nucl Med 1995; 36: 411-419.
19 Pruim J, Willemsen AT, Molenaar WM, et al. Brain tumors: L-[1-C-11]tyrosine
PET for visualization and quantification of protein synthesis rate. Radiology 1995;
197: 221-226.
20 Kole AC, Pruim J, Nieweg OE, et al. PET with L-[1-carbon-11]-tyrosine to visualize
tumors and measure protein synthesis rates. J Nucl Med 1997; 38: 191-195.
21 Lienard D, Ewalenko P, Delmotte JJ, Renard N, Lejeune FJ. High-dose recombinant
tumor necrosis factor alpha in combination with interferon gamma and melphalan
in isolation perfusion of the limbs for melanoma and sarcoma. J Clin Oncol 1992;
10: 52-60.
22 Eggermont AMM, Schraffordt Koops H, Lienard D, et al. Isolated limb perfusion
with high-dose tumor necrosis factor-alfa in combination with interferon-gamma
and melphalan for nonresectable extremity soft tissue sarcomas: a multicenter trial.
J Clin Oncol 1996; 14: 2653-2665.
23 Coindre JM, Trojani M, Contesso G, et al. Reproducibility of a histopathologic
grading system for adult soft tissue sarcoma. Cancer 1986; 58: 306-309.
24 Creech O, Krementz ET, Ryan RF, Winblad JN. Chemotherapy of cancer: regional
perfusion utilizing an extra-corporeal circuit. Ann Surg 1958; 148: 616-632.
25 Zwaveling JH, Maring JK, Clarke FL, et al. High plasma tumor necrosis factor
(TNF)-alpha concentrations and a sepsis-like syndrome in patients undergoing
hyperthermic isolated limb perfusion with recombinant TNF-alpha, interferon-
gamma, and melphalan. Crit Care Med 1996; 24: 765-770.
26 Giron C, Luurtsema G, Vos MG, et al. Microwave-induced preparation of 11C-
amino-acids via NCA-Bücherer-Strecker synthesis. J Lab Compnd Radiopharm
1995; 37: 752-754.
27 Winer BJ. Statistical principles in experimental design. New York: McGraw Hill,
1971: 2 edn.
28 Brown RS, Wahl RL. Overexpression of Glut-1 glucose transporter in human breast
cancer. Cancer 1993; 72: 2979-2985.

106

107
Robert J. van Ginkel1
Piet C. Limburg2
D. Albertus Piers3
Heimen Schraffordt Koops1
Harald J. Hoekstra1
Department of Surgical Oncology1, Internal Medicine2 and Nuclear Medicine3,
University Hospital Groningen, The Netherlands.
Annals of Surgical Oncology 2002; 9: 355-363.
Value of continuous leakage monitoring with radio-
active Iodine-131 labeled human serum albumin
during hyperthermic isolated limb perfusion with
TNF and melphalan

108
Chapter 8
Abstract
The aim of this study was to analyze the value of continuous leakage monitoring with
radioactive Iodine-131 labeled human serum albumin (RISA) in patients treated with
hyperthermic isolated limb perfusion (HILP) with tumor necrosis factor alpha (TNF)
and melphalan. Forty-eight patients with melanoma (n = 14) or soft tissue sarcoma
(n = 34) of an extremity underwent 51 perfusions. Perfusion was performed at the
iliac level in 22 cases, at the popliteal level in 16 cases, at the femoral level in 7
cases and in 6 cases at the axillary level. Leakage rates, perfusion circuit and systemic
levels of TNF, interleukin-6, C-reactive protein (CRP) were determined, as were
systemic hematological and metabolic profiles and tumor response. The mean
isotopically measured leakage was 2.9 % (95% confidence interval 2.0 – 3.8%, range
0-15.5%). Systemic leakage was ≤2% in 28 perfusions (55%) and >2% in 23
perfusions (45%). The correlation between the maximal monitored leakage and
maximal systemic TNF levels was 0.7114 (p < 0.0001). The area under the curve
(AUC) for TNF in the perfusion circuit, indicating the exposure of the perfused limb
to TNF, was 18.7% lower in the >2% leakage group (p=0.0457). No significant
differences in tumor response were found between groups. AUC for systemic TNF,
indicating the exposure of the patient to TNF, was 18.1 times higher in the >2%
leakage group (p<0.0001) resulting in a significant decrease in leucocyte and platelet
count, hyperbilirubinemia, hypocholesterolemia and proteinemia. No beneficial effect
of the systemically leaked TNF and melphalan was seen on the occurrence of distant
metastasis during follow-up. There was a significant difference between perfusions
performed at the iliac and femoral levels compared with leakage values at the popliteal
level, p < 0.0001 and 0.0159 respectively. A good correlation between RISA leakage
measurement and TNF exposure during and after HILP with TNF and melphalan
was demonstrated. RISA leakage measurement serves as a good guide for the
effectiveness of isolation during perfusion. If leakage exceeds the 2% limit during
perfusion, less exposure of the tumor bearing limb to TNF, increased exposure of the
patient systemic circulation to TNF, and more systemic side effects can be expected.
Introduction
Creech and Krementz developed isolated limb perfusion with chemotherapy for the
treatment of extremity melanoma in humans in 1958.1 Stehlin et al modified the
technique in 1969 to include hyperthermia.2 Since then, hyperthermic isolated limb
perfusion (HILP) with different chemotherapeutic agents has been used by several
institutes worldwide for the treatment of advanced extremity melanoma and soft
tissue sarcoma. Recently, an international study comparing local excision and adjuvant

109
Leakage during isolated limb perfusion with TNF
HILP with melphalan with wide excision only revealed a trend for a longer disease-
free interval after HILP with melphalan but no benefit from HILP in terms of time to
distant metastasis or survival.3 With the conclusion that prophylactic HILP with
melphalan could not be recommended as an adjunct to standard surgery in high-risk
primary limb melanoma, the indication for HILP is currently restricted to advanced
melanoma and primarily irresectable soft tissue sarcoma. For these indications the
addition of tumor necrosis factor alpha (TNF) to melphalan seems promising.4,5
With the introduction of TNF, monitoring of leakage of the isolated circuit into the
systemic circulation has been mandatory since TNF levels in the perfusion circuit
are approximately 10 times the maximum tolerated systemic levels.6 If significant
leakage occurs during HILP, the resultant TNF induced systemic inflammatory
response syndrome (SIRS) could be fatal.7 Different methods for measurement of
leakage are used. In the early days, Stehlin et al determined the amount of radioactive
Iodine-131 labeled human serum albumin (RISA) through the use of blood samples
from the systemic circulation, and calculated the leakage factor (LF).8 Although
determination of blood samples takes time and is discontinuous, it is frequently used
by other groups.9,10 To overcome these disadvantages, Stehlin and associates were
the first to describe a method of continuous external leakage monitoring with RISA.11
Because of safety regulations, nuclear medicine techniques are not always allowed
in the operation zoom. Another method, the measurement of Evans blue concentration
in plasma by means of a spectral photometer, overcomes this problem.12 Two other
groups introduced the use of handheld gamma detectors for leakage measurements;
however, a great dependency was observed on the distance and angle from the source
with this system.13,14
Since 1991, patients with advanced melanoma or soft tissue sarcoma of the limbs,
have been treated at the Groningen University Hospital by HILP with TNF, melphalan
with or without interferon gamma (IFN) as perfusion agents, followed by delayed
surgical excision. The aim of this study was to analyze the value of continuous leakage
monitoring with RISA in patients treated with TNF perfusion with respect to systemic
levels of TNF, interleukin (IL)-6, C-reactive protein (CRP) as well as hematological
and metabolic profiles and tumor response.
Patients and methods
Forty-eight patients with melanoma (n = 14) or soft tissue sarcoma (n = 34) of the
extremity underwent 51 perfusions with a combination of TNF and melphalan, with
or without IFN. Twenty-one males and 27 females, with a median age of 54 years
(range 18-80 years) were treated. Perfusion was performed at the iliac level in 22
cases (43%), at the popliteal level in 16 cases (31%), at the femoral level in 7 cases

110
Chapter 8
(14%), and in 6 cases (12%) at the axillary level. All patients were treated after
informed consent was obtained according to institutional guidelines.
Perfusion Technique
The perfusion technique employed at the Groningen University Hospital is based on
the technique developed by Creech et al.1 and has been described in detail previously.15
Briefly, after ligation of all collateral vessels and heparinization of the patient with
3.3 mg heparin/kg bodyweight (Thromboliquine, Organon BV, Oss, the Netherlands),
the axillary, iliac (internal iliac artery is temporarily closed), femoral, or popliteal
vessels were cannulated and connected to an extracorporal circuit. The perfused limb
was wrapped in a thermal blanket to reduce heat loss. To prevent collateral circulation
in subcutaneous tissue and muscle, an occluding rubber bandage was twisted around
the root of the extremity and fixed around a pin inserted into the head of the humerus
(axillary perfusion) or iliac crest (iliac perfusion). An inflating tourniquet was used
in femoral or popliteal perfusions. Perfusion was performed during 90 min under
mild hyperthermia (39-40°C) and physiologically optimal conditions.16 At the start
of perfusion, 3 mg (upper extremity) or 4 mg (lower extremity) TNF (Boehringer,
Ingelheim, Germany) was injected as a bolus into the arterial line. Eighteen patients
also received a dose of 0.2 mg INF (Boehringer, Ingelheim, Germany) subcutaneously
1 and 2 days before perfusion, followed by 0.2 mg INF injected into the arterial line
at the start of perfusion. Melphalan (L-phenylalanine mustard, Glaxo-Wellcome,
London, England) was administered 30 min later, as 10 mg/L extremity volume (leg)
or 13 mg/L extremity volume (arm).17 The volume of the limb was determined before
surgery by immersion.
All perfusions were performed with a bubble oxygenator roller pump and heat
exchanger. The perfusate was oxygenated by a mixture of O2 and CO
2 and consisted
of 350 ml 5% dextran 40 in glucose 5% (Isodex, Pharmacia AB, Uppsala, Sweden),
500 ml blood (250 ml red blood cells, 250 ml plasma), 30 ml of 8.4% NaHCO3, 0.5
ml 5000 IU/ml heparin. The perfusions were flow regulated on the basis of the arterial
and venous pressure measured at one end of the double lumen catheter used. After 90
min of perfusion, the limb was flushed with 2 L dextran 40 in glucose 5% (Isodex)
and 500 ml blood (250 ml red blood cells, 250 ml plasma), catheters were removed,
the circulation restored and the heparin antagonized with protamine chloride (Hoffman
La Roche, Mijdrecht, the Netherlands). A lateral fasciotomy of the anterior
compartment of the lower leg or arm was performed to prevent a compartment
syndrome.18

111
Leakage during isolated limb perfusion with TNF
Leakage Measurement
Any leakage into the systemic circulation was continuously monitored with radioactive
tracers. A small calibration dose of RISA (0.5 MBq) and a dose of radioactive
Technetium-99m labeled human serum albumin (RTcSA; 10 MBq) were administered
into the systemic circulation, after surgical isolation of the extremity was
accomplished. The thyroid was saturated 1 day before the operation by oral
administration of iodine (15 drops of Lugol solution twice daily). A 10 times higher
dose of RISA (5 MBq) was injected into the perfusion circuit when perfusion was
stable. The 364-keV gamma rays emerging from the RISA and the 140-keV gamma
rays emerging from the RTcSA are measured with a NaI detector, which was placed
in a flat field lead lined collimator that was mounted on an articulating mobile stand.
This stand permits easy positioning of the detector, after it is covered with a sterile
bag, above the heart of the patient. Careful attention is paid to ensure that the field of
view of the detector did not cover parts of the HILP circuit. The detector signals
generated by the photomultiplier tube were directed to an amplifier and then to a
single-channel analyzer, allowing online data processing by a personal computer.
The count rate of the 0.5-MBq RISA determined a baseline count level, corrected for
room background. The 10-MBq RTcSA served to check the volume dilution caused
by to fluid infusions or displacement of the NaI detector during the registration period.
Leakage from the perfused limb to the systemic circulation resulted in an increase of
the baseline count level. This increase, corrected for the blood volume ratio and the
radioactivity ratio in both compartments, was a direct measure for the percentage of
leakage and was continuously registered during the whole procedure. Stehlin was
the first to describe the LF based on the following equation:
where cpmsystemic
is the systemic count rate observed during perfusion, cpmbaseline
is
the systemic count rate at the beginning of perfusion, Dsystemic
is the dose injected into
the patient’s systemic circulation, and Dperfusion
is the dose injected into the perfusion
circuit Vtotal
is the total blood volume (perfusion circuit + patient’s systemic
circulation), Vsystemic
is the blood volume of the patient’s systemic circulation.11
Blood sampling procedure and assays
A baseline blood sample from the patients systemic circulation was taken from an
indwelling radial artery cannula before the start of the operation, and at 5, 30, 60,
LF = (cpmsystemic - cpmbaseline)
< > Dsystemic
< > Vtotal
< > 100%
cpmbaseline Dperfusion Vsystemic

112
Chapter 8
and 89 min after the start of perfusion. Samples from the perfusion circuit were also
taken at the same time intervals. After restoration of the circulation in the perfused
limb, systemic samples were taken at 1, 5, 10, 30 and 60 min after removal of the
arterial clamps, hourly thereafter for at least 8 hours and finally the next morning.
Venous blood samples to study the hematological and metabolic profiles of urea
nitrogen, creatinine, bilirubin, alkaline phosphatase, aspartate aminotransferase,
alanine aminotransferase, gammaglutamyltranspeptidase, protein, cholesterol, lactic
dehydrogenase (LDH) with its iso-enzymes, creatine phosphokinase and myoglobin
were taken a day before perfusion, at the day of perfusion, and every day after
perfusion until day 7. A final blood sample was taken one month after perfusion.
Blood samples (3 ml) were collected in EDTA vacutainer tubes, and kept on melting
ice during transport to a centrifuge. Samples were centrifuged for 10 min at 3000
rpm at 0°C and the separated plasma kept at –80°C until analysis.
TNF levels were determined by specific immunoradiometric assay (Medgenix
Diagnostics, Soesterberg, the Netherlands). Samples were processed according to
the guidelines of the manufacturer. IL-6 and CRP levels were measured by in-house
sandwich ELISA’s as described previously19, by using commercial reagents for IL-6
(CLB, Amsterdam, the Netherlands; detection limit 10 ng/L) and for CRP (DAKO,
Glostrup, Denmark; normal level <2.3 mg/L).
Assessment of tumor response
Responses were assessed by standardized World Health Organization criteria.20
Complete response (CR) was defined as the disappearance of all measurable disease
in the limb for longer than 4 weeks, partial response (PR) as regression of the tumor
size by >50% for longer than 4 weeks, and no change (NC) as regression of <50% of
the tumor in the limb or progression of <25% for longer than 4 weeks. To analyze
whether or not a high systemic leakage was of influence in the occurrence of distant
metastasis subanalyses of this parameter in a group of patients with grade II and III
soft tissue sarcomas was performed.
Statistical analysis
Values are expressed as mean ± SEM. Comparison between mean values of different
groups was performed with the unpaired or in case of measuring the same variable in
the same patient at different time points, with the paired Student’s t-test. Areas under
the curve (AUC) were determined by the trapezoid rule. Survival curves were
calculated according to the Kaplan Meier method and log rank test.21 Values of
p ≤ .05 were considered to be statistically significant. Graph Pad Prismâ version 2.0
for Windows (GraphPad, San Diego, CA) statistical software was used.

113
Leakage during isolated limb perfusion with TNF
Results
Systemic leakage
For the 51 perfusions, the mean isotopically measured leakage was 2.9 % (95%
confidence interval, 2.0 – 3.8%, range 0-15.5%). After 60 minutes of perfusion in
the patient with the highest leakage (15.5%), it was noted that the rubber bandage
twisted around the root of the extremity was ruptured. Since this was the cause of the
high leakage and perfusion was not completed, the data from this patient are excluded
from the remainder of the analyses. Systemic leakage was ≤ 2% in 28 perfusions
(55%) and >2% in 23 perfusions (45%). In the latter group, 11 perfusions (22%) led
to systemic leakage of >5%. In addition, analysis of different parameters between
the group of patients with ≤ 2% leakage and the group of patients with >2% leakage,
was made. Figure 1 shows the measured leakage at different perfusion levels. There
was a significant difference between perfusions performed at the iliac and femoral
levels compared with leakage values at the popliteal level, (p < 0.0001 and 0.0159
respectively). There was no leakage encountered in patients with axillary perfusions.
Fig. 1 Scatter diagram of leakage at dif-
ferent perfusion levels, the uninterrupted
line represents mean values. A significant
difference was observed between perfu-
sions performed at the iliac and femoral
levels compared with leakage values at
the popliteal level, (p < 0.0001 and
0.0159 respectively)
Perfusion circuit levels
At 5 minutes, mean TNF levels in the perfusion circuit were 6798 ± 528 ng/ml
(Fig. 2). During perfusion, a significant drop in TNF levels in the perfusion circuit
occurred with a significant lower concentration of TNF in the perfused limb in patients
with >2% leakage at 30 (p = 0.0201), 60 (p = 0.0337) and 89 minutes (p = 0.002).
The calculated mean AUC, indicating the exposure of the perfused limb to TNF, was
18.7% less in the >2% leakage group (p=0.0457). IL-6 levels in the perfusate, as one
of the most important proinflammatory cytokines, progressively increased from 30
minutes until the end of the perfusion, reaching 4.2 ± 1.1 ng/ml in the ≤2% leakage

114
Chapter 8
Fig. 2 Tumor necresis factor (TNF)
levels in the perfusion circuit (mean ±SEM). A significant decrease in TNF
levels occurred with significant lower
concentration of TNF in the perfused
limb in patients with >2% leakage at
30 (p = 0.0201), 60 (p = 0.0337) and
89 minutes (p = 0.002). Mean area un-
der the curve, indicating the exposure
of the perfused limb to TNF, was 18.7%
less in the >2% leakage group
group and 11.7 ± 3.5 ng/ml in the >2% leakage group (p=0.0455). CRP levels in the
perfusion circuit remained at the detection level, and no significant differences were
observed between the leakage groups.
Systemic levels
Systemic TNF levels in patients with >2% leakage were already significantly higher
at 5 min after TNF injection compared with the group of patients with ≤2% leakage.
Peak systemic TNF values of 116.5 ± 28.9 ng/ml were reached in the >2% leakage
group at the end of perfusion, compared with 11.8 ± 3.4 ng/ml in the ≤2% leakage
group (p < 0.0001) (Fig. 3). The calculated mean systemic AUC, indicating the
exposure of the patient to TNF, was 18.1 times higher in the >2% leakage group
(p<0.0001). Ten minutes after release of the tourniquet we observed a significant
systemic peak level of TNF in the ≤2% group possibly caused by the TNF still present
in the perfused limb after the washout procedure (p=0.026). To calculate the correlation
between maximum systemic TNF levels and the maximum monitored leakage using
RISA measured during perfusion, Pearson’s correlation (two-tailed) was used. Figure
4 illustrates the observed correlation with r = 0.7114 and p < 0.0001. A strong
correlation was also found between the maximal observed leakage and maximum
IL-6 concentration measured in the postoperative period (r = 0.7737, P<0.0001).
IL-6 levels appeared in the systemic circulation 30 minutes after the start of the
perfusion and maximal levels were reached 2 hours after HILP (19.5 ± 5.8 ng/ml
≤2% leakage versus 77.7 ± 20.8 ng/ml >2% leakage; p=0.0089). The AUC of IL-6
was 4.7 times higher in the >2%leakage group compared with ≤2% leakage group
(p<0.0243).

115
Leakage during isolated limb perfusion with TNF
CRP started to increase 6 hours after HILP and reached its maximal value 2 days
after perfusion (185.8 ± 25.5 mg/L ≤2% leakage versus 226.7 ± 32.7 mg/L, >2%
leakage; not significant). The AUC of CRP between both groups however was not
significantly different.
Hematological and metabolic parameters
Leukocyte counts increased from 7.7 ± 0.3x109/L to 13.0 ± 0.6x109/L one day after
perfusion. Five, 6, and 7 days after perfusion a significant difference between the
two leakage groups was observed (Fig. 5). Platelet counts decreased from 303.6 ±13.4x109/L before perfusion to 124.3 ± 10.7x109/L 4 days after perfusion.
Fig. 3 Tumor necrosis factor (TNF) lev-
els in the systemic circulation of the pa-
tient (mean ± SEM). A significant dif-
ference was found between the >2%
leakage group and the ≤2% leakage
group is starting 5 min after TNF injec-
tion until the second postoperative day
(p<0.05). The mean systemic area un-
der the curve, indicating the exposure
of the patient to TNF, was 18-times
higher in the >2% leakage group
Fig. 4 Pearson’s correlation (two-
tailed) between maximal systemic TNF
levels measured during perfusion and
maximal monitored leakage using
RISA (r = 0.7114 and P<0.0001)

116
Chapter 8
The low platelet levels persisted longer in the >2% leakage group. Kidney function
was well preserved in all patients, although urea nitrogen and creatinine levels in the
>2% leakage group were significantly higher during the first 5 days after perfusion;
these levels however remained within normal limits. Liver function tests showed an
increase in bilirubin values from 10.5 ± 0.9 µmol/L to 44.8 ± 11.3 µmol/L, 4 days
after perfusion in the >2% leakage group, with significant differences compared with
the ≤2% leakage group (Fig. 6). Figure 6 illustrates the decrease in protein levels and
cholesterol levels after perfusion, with significant differences between both leakage
groups. Alkaline phosphatase increased from 86.1 ± 6.5 U/L to 159.4 ± 32.8 U/L,
aspartate aminotransferase increased from 22.8 ± 1.5 U/L to a maximum of 62.1 ±13.4 U/L on the fifth day after perfusion, alanine aminotransferase increased from
21.9 ± 2.6 U/L to a maximum of 80.3 ± 11.6 U/L on the sixth day after perfusion, and
gammaglutamyltransferase increased from 37.7 ± 8.7 U/L to a maximum of 120.1 ±18.6 U/L on the sixth day after perfusion. LDH increased from 224.8 ± 9.0 U/L to a
maximum of 417.3 ± 19.1 U/L on the second day after perfusion. LDH iso-enzymes
1 and 2 showed a decrease, whereas LDH iso-enzymes 4 and 5 increased one day
after perfusion. LDH iso-enzyme 3 remained at the same level. Creatine phospho-
kinase levels increased from 28.3 ± 2.4 U/L to a maximum of 496.4 ± 197.6 U/L on
Fig. 5 White blood cell count (WBC)
and platelets (PLT) levels from before
perfusion to 30 days after perfusion
(mean ± SEM). * indicates a significant
difference between both leakage groups
(p < 0.05)

117
Leakage during isolated limb perfusion with TNF
the second day after perfusion. Myoglobin levels increased from 30.2 ± 2.4 µg/L to
a maximum of 422.8 ± 99.7 µg/L one day after perfusion. None of these variables
showed a significant difference between both leakage groups.
Tumor Response
In the ≤2% leakage group, 14 patients showed a CR and the same number of patients
a PR. In the >2% leakage group, 11 patients showed a CR, 10 patients a PR and 2
patients had NC. No significant differences in response to TNF HILP were found
between the groups. No significant difference was observed in the occurrence of
distant metastasis or survival in the subanalyses of a group of patients with grade II
or III soft tissue sarcoma and >2% leakage (Fig. 7).
Fig. 6 Bilirubin, protein and cholesterol
levels from before perfusion to 30 days
after perfusion (mean ± SEM). * indicates
a significant difference between both leak-
age groups (p < 0.05)

118
Chapter 8
Discussion
The purpose of continuous leakage monitoring with RISA during HILP is to indicate
the amount of chemotherapeutic agent that is leaking from the perfusion circuit into
the patient’s systemic circulation. When leakage occurs, measures to reduce leakage
should be available. During perfusion there is a dynamic balance between two pressure
compartments: the patients systemic vasculature and the isolated circuit. The pressure
of the former compartment can be influenced by adjusting the systemic blood pressure,
whereas that of the latter can be affected by alterations in the extracorporeal flow
rate. Thus, to decrease leakage, the anesthesiologist can increase the patient’s blood
pressure or the surgeon can reduce the flow rate in the heart-lung machine. Different
methods for measurement of leakage have been used. The previously described method
with RISA is the most frequently used; however, a MEDLINE search to find any
articles calculating the correlation between systemic melphalan levels and leakage
in case of HILP with melphalan only, produced no results. The first report on TNF
levels after HILP with TNF, from Gérain et al. in 1992, demonstrated no significant
correlation between leakage and cytokine levels at any time, raising questions about
the value of the leakage measurement procedure.6
The aim of this study was to investigate whether or not the RISA leakage
measurements during HILP with TNF used in the Groningen University Hospital are
accurate in predicting systemic TNF levels. We observed a good correlation between
maximal systemic TNF levels and the maximum monitored leakage (r = 0.7114;
p < 0.0001). We were surprised to find that the correlation between maximal leakage
and maximal IL-6 concentration measured in the postoperative period was higher
than the correlation between maximal leakage and maximal TNF levels (r = 0.7737
versus r = 0.7114). IL-6 levels occurred in response to TNF, with a high correlation
between maximal levels of both cytokines (r = 8097). Stam et al. also found a strict
correlation between the degree of leakage estimated by isotope monitoring and the
Fig. 7 Absence of distant metastasis in
patients with grade II or III soft tissue sar-
coma. No significant difference was found
between the >2% leakage group and the
≤2% leakage group

119
Leakage during isolated limb perfusion with TNF
measured maximal systemic TNF levels in the same treatment setting (r = 0.7886,
p=0.0067; calculation based on their data).22 They also found a sharper relation
between systemic IL-6 curves and duration of exposure to high TNF levels in patients
with high leakage compared with a group of patients with no leakage. A significant
difference in leakage was found between the iliac/femoral perfusion levels and
popliteal perfusion level. This corresponds with the study of Klaase et al., who assessed
six variables for their influence on systemic leakage. The level of isolation and the
diameter of the venous cannula emerged as significant factors.23 In our study we
could not find a significant role for the diameter of the venous cannula (data not
shown). The importance of the perfusion level could be partly explained by the
different type of isolation technique used, namely, a rubber band tourniquet at the
iliacal level versus a inflatable pressure regulated band at the popliteal level.
In the analysis of our data, we distinguished two leakage groups, with a cutoff point
at 2%. Two percent represents approximately the measurement fault of the RISA
procedure. TNF levels in the perfusion circuit were about 7000 ng/ml, approximately
50-times higher than peak systemic levels. A significantly lower concentration of
TNF in the perfused limb in patients with >2% leakage was demonstrated resulting
in a decreased AUC, indicating an 18.7% lower exposure of the perfused limb to
TNF in the >2% leakage group. This decrease in TNF exposure, however, did not
result in a significant reduction of tumor response between the groups. This result
supports the initiation of TNF dose reduction studies. Thom et al. observed the same
decreased TNF perfusion circuit levels in patients with ≥1% leakage.24 The Rotterdam
perfusion group did not demonstrate a significant difference in perfusion circuit TNF
levels between a high and low-leakage group, possibly because of a limited number
of samples available.22
TNF levels in the systemic circulation of the patients were approximetely 100 ng/ml
in the >2% leakage group at the end of perfusion, compared with 10 ng/ml in the
≤2% leakage group. In patients with ≤2% leakage, systemic TNF exposure was 18.1
times less as calculated by the AUC. On the basis of the hypothesis that micro
metastatic disease is attacked by the leaked TNF and melphalan, a higher systemical
exposure of TNF could have its effect on the occurence of distant metastasis during
follow-up. However, subanalysis of the occurence of distant metastasis or survival
in a group of patients with grade II or III soft tissue sarcomas did not reveal this
phenomenon. IL-6, as one of the most important proinflammatory cytokines, appeared
in the systemic circulation 30 minutes after the start of the perfusion with maximum
levels reached 2 hours after HILP. CRP levels started to increase 6 hours after HILP
and reached its maximum 2 days after perfusion. A three wave pattern was seen; the
first wave caused by the systemically leaked TNF that generated a second wave of

120
Chapter 8
IL-6 some hours after perfusion, followed by a third wave of CRP that lasts for
several days.
TNF leakage was associated with a decrease in leucocyte and platelet count, with
significantly lower values in the >2% leakage group. Representing cytolytic liver
toxicity, a significantly hyperbilirubinemia, hypocholesterolemia and proteinemia
was observed in the >2% leakage group. A increase in the activity of the fraction of
LDH iso-enzymes 4 and 5 after perfusion was partly related to hepatotoxicity and
partly to muscle damage. No significant difference between both leakage groups
was found for creatine phosphokinase levels or myoglobin levels although both
parameters showed a significant rise after HILP. The same results were obtained by
Sorkin et al. who diminished TNF leakage after flow rate reduction during TNF
HILP.25 Analysis of our own flow data in relation to systemic leakage revealed a
weak negative correlation of r = -0.2910 with p = 0.0448 with a mean flow of 455 ±172 ml/min in our perfusions.
Like others, we also found a significant systemic TNF peak in patients with low
leakage after restoration of the circulation of the perfused limb.22,26 Despite a washout
procedure with 2 L of Isodex, TNF in the limb reaches the systemic circulation. A
corresponding rise in RISA was also observed.27 Therefore, today a more extensive
washout with 6 L and massage of the perfused limb is recommended in TNF perfusions
to reduce TNF release.
In a previous study we described the clinical features of HILP with TNF characterized
by a short- lived sepsis-like syndrome.28 This best called SIRS, was seen in all patients
and accompanied by fever, increase in cardiac output, a decrease in systemic vascular
resistance, and the need for fluid resuscitation and inotropes. Perfusion with melphalan
as the sole perfusion agent did not trigger these effects. Detailed analysis showed
positive correlations between maximum TNF concentrations and systemic vascular
resistance and cardiac index. The National Cancer Institute perfusion group
demonstrated the relation between the vascular response with the need for vasopressor
support and systemic TNF levels in patients with TNF leakage as well.24 Lejeune
also demonstrated severe toxicity in patients with leaks of >5%.4,6 Vrouwenraets et
al. reported an absence of severe systemic toxicity of TNF in patients without systemic
leakage.26 Stam et al. observed only a mild postoperative toxicity in the event of
significant leakage during perfusion.22 This was easily managed on the intensive
care unit with fluid substitution and, in some cases, vasopressors. On the basis of
their data, they rightly plead for renewed study of the potential use of TNF
systemically. Currently, SIRS is only seldom seen since the majority of the institutions
performing HILP with TNF and melphalan are experienced and are using a more
extensive washout procedure. One could ask oneself if leakage measurements during

121
Leakage during isolated limb perfusion with TNF
HILP are still worthwhile when side effects of TNF leakage are so easily dealt with.
In this study we demonstrated a good correlation between RISA leakage measurement
and TNF exposure during and after HILP with TNF and melphalan. RISA leakage
measurement serves as a good guide for the effectiveness of isolation during perfusion.
If leakage exceeds the 2% limit during perfusion, less exposure of the tumor bearing
limb to TNF, an increased exposure of the patient’s systemic circulation to TNF, and
more systemic side effects can be expected. Because leakage >2% did not influence
the tumor response, further dose-reduction studies of TNF in the HILP setting are
warranted.

122
Chapter 8
References
1 Creech O, Krementz ET, Ryan RF, Winblad JN. Chemotherapy of cancer: regional
perfusion utilizing an extra-corporeal circuit. Ann Surg 1958; 148: 616-632.
2 Stehlin JS. Hyperthermic perfusion with chemotherapy for cancers of the extremities.
Surg Gynecol Obstet 1969; 129: 305-308.
3 Schraffordt Koops H, Vaglini M, Suciu S, Kroon BB, Thompson JF, Gohl J, et al.
Prophylactic isolated limb perfusion for localized, high-risk limb melanoma: results
of a multicenter randomized phase III trial. European Organization for Research
and Treatment of Cancer Malignant Melanoma Cooperative Group Protocol 18832,
the World Health Organization Melanoma Program Trial 15, and the North American
Perfusion Group Southwest Oncology Group-8593. J Clin Oncol 1998; 16: 2906-
2912.
4 Lienard D, Ewalenko P, Delmotte JJ, Renard N, Lejeune FJ. High-dose recombinant
tumor necrosis factor alpha in combination with interferon gamma and melphalan
in isolation perfusion of the limbs for melanoma and sarcoma. J Clin Oncol 1992;
10: 52-60.
5 Eggermont AMM, Schraffordt Koops H, Lienard D, Kroon BBR, Van Geel AN,
Hoekstra HJ, et al. Isolated limb perfusion with high-dose tumor necrosis factor-
alfa in combination with interferon-gamma and melphalan for nonresectable
extremity soft tissue sarcomas: a multicenter trial. J Clin Oncol 1996; 14: 2653-
2665.
6 Gerain J, Lienard D, Ewalenko P, Lejeune FJ. High serum levels of TNF-alpha after
its administration for isolation perfusion of the limb. Cytokine 1992; 4: 585-591.
7 Eggimann P, Chiolero R, Chassot PG, Lienard D, Gerain J, Lejeune FJ. Systemic
and hemodynamic effects of recombinant tumor necrosis factor alpha in isolation
perfusion of the limbs. Chest 1995; 107: 1074-1082.
8 Stehlin JS, Clark RL, White EC, Healey JE, Dewey WC, Beerstecher S. The leakage
factor in regional perfusion with chemotherapeutic agents. A M A Arch Surg 1960;
80: 934-945.
9 Alexander C, Omlor G, Berberich R, Gross G, Feifel G. Rapid measurement of
blood leakage during regional chemotherapy. Eur J Nucl Med 1993; 20: 187-191.
10 Hafstrom L, Hugander A, Jonsson PE, Westling H, Ehrsson H. Blood leakage and
melphalan leakage from the perfusion circuit during regional hyperthermic perfusion
for malignant melanoma. Cancer Treat Rep 1984; 68: 867-872.
11 Stehlin JS, Clark RL, Dewey WC. Continuous monitoring of leakage during regional
perfusion. Arch Surg 1961; 83: 943-950.
12 Ghussen F, Nagel K, Sturz I, Isselhard W. A modified dye dilution method to estimate
leakage during regional isolated perfusion of the extremity. Res Exp Med (Berl)
1982; 180: 179-187.
13 Sardi A, Minton JP, Mojzisik C, Nieroda CA, Ferrara PJ, Hinkle GH, et al. The use
of a hand-held gamma detector improves the safety of isolated limb perfusion. J
Surg Oncol 1989; 41: 172-176.
14 Sandrock D, Horst F, Gatzemeier W, Ghorbani M, Rauschecker HF, Munz DL, et
al. Leakage measurement during selective limb perfusion using a gamma probe.
Eur J Nucl Med 1996; 23: 534-538.

123
Leakage during isolated limb perfusion with TNF
15 Schraffordt Koops H, Oldhoff J, Oosterhuis JW, Beekhuis H. Isolated regional
perfusion in malignant melanoma of the extremities. World J Surg 1987; 11: 527-
533.
16 Fontijne WP, Mook PH, Schraffordt Koops H, Oldhoff J, Wildevuur CR. Improved
tissue perfusion during pressure regulated regional perfusion: a clinical study. Cancer
1985; 55: 1455-1461.
17 Wieberdink J, Benckhuysen C, Braat RP, Van Slooten EA, Olthuis GAA. Dosimetry
in isolation perfusion of the limb by assessment of perfused tissue volume and grading
of toxic tissue reactions. Eur J Cancer Clin Oncol 1982; 18: 905-910.
18 Schraffordt Koops H. Prevention of neural and muscular lesions during hyperthermic
regional perfusion. Surg Gynecol Obstet 1972; 135: 401-403.
19 Maring JK, Klompmaker IJ, Zwaveling JH, van Der M, Limburg PC, Slooff MJ.
Endotoxins and cytokines during liver transplantation: changes in plasma levels
and effects on clinical outcome. Liver Transpl 2000; 6: 480-488.
20 World Health Organization. Handbook for Reporting Results of Cancer Treatment.
WHO Offset Publication no 48 Geneva, Switzerland, 1979 World Health
Organization.
21 Kaplan EL, Meier P. Nonparametric estimates from incomplete observations. J Am
Stat Assoc 1958; 53: 457-481.
22 Stam TC, Swaak AJ, de Vries MR, ten Hagen TL, Eggermont AM. Systemic toxicity
and cytokine/acute phase protein levels in patients after isolated limb perfusion with
tumor necrosis factor-alpha complicated by high leakage. Ann Surg Oncol 2000; 7:
268-275.
23 Klaase JM, Kroon BB, Van Geel AN, Eggermont AMM, Franklin HR. Systemic
leakage during isolated limb perfusion for melanoma. Br J Surg 1993; 80: 1124-
1126.
24 Thom AK, Alexander HR, Andrich MP, Barker WC, Rosenberg SA, Fraker DL.
Cytokine levels and systemic toxicity in patients undergoing isolated limb perfusion
with high-dose tumor necrosis factor, interferon gamma, and melphalan. J Clin Oncol
1995; 13: 264-273.
25 Sorkin P, Abu Abid S, Lev D, Gutman M, Aderka D, Halpern P, et al. Systemic
leakage and side effects of tumor necrosis factor alpha administered via isolated
limb perfusion can be manipulated by flow rate adjustment. Arch Surg 1995; 130:
1079-1084.
26 Vrouenraets BC, Kroon BB, Ogilvie AC, Van Geel AN, Nieweg OE, Swaak AJ, et
al. Absence of severe systemic toxicity after leakage-controlled isolated limb
perfusion with tumor necrosis factor-alpha and melphalan. Ann Surg Oncol 1999; 6:
405-412.
27 Barker WC, Andrich MP, Alexander HR, Fraker DL. Continuous intraoperative
external monitoring of perfusate leak using iodine-131 human serum albumin during
isolated perfusion of the liver and limbs. Eur J Nucl Med 1995; 22: 1242-1248.
28 Zwaveling JH, Maring JK, Clarke FL, van Ginkel RJ, Limburg PC, Hoekstra HJ, et
al. High plasma tumor necrosis factor (TNF)-alpha concentrations and a sepsis-like
syndrome in patients undergoing hyperthermic isolated limb perfusion with
recombinant TNF-alpha, interferon- gamma, and melphalan. Crit Care Med 1996;
24: 765-770.

124

125
Summary and conclusions
Samenvatting en conclusies

126
Chapter 9
Summary
Chapter 1
Using technology to support extracorporeal circulation developed for cardiac surgery
in the 1950s, the surgical oncologists Creech, Krementz, Ryan and Winblad of the
Tulane University in New Orleans developed the technique of isolated limb perfusion
(ILP). In this procedure the blood circulation of a tumor bearing limb is isolated
from the circulation of the rest of the body by clamping the major artery and vein and
tightening a tourniquet around the root of the limb. The artery and vein are
subsequently connected to a heart-lung machine and a cytotoxic drug is administered
through this isolated circuit. Key point in ILP is that the dose of chemotherapeutics
used, can be 15-20 fold the maximum systemic tolerated dose since vital organs are
isolated from the perfusion circuit. Cavaliere and co-workers investigated the addition
of hyperthermia in the treatment of cancer and, as this appeared to augment the anti-
tumor effects of melphalan, in doing so they laid the basis for hyperthermic isolated
limp perfusion (HILP). The original patient population treated with HILP was a
subgroup of melanoma patients with extensive local recurrence in the arm or leg.
Later on also patients with soft tissue sarcomas of the extremities were treated.
Throughout the years different chemotherapeutic agents were used in HILP, all with
variable results.
William Coley, a surgeon who lived and worked in New York City during the second
half of the 19th century, was the first to investigate the phenomenon of tumor necrosis,
occurring in patients suffering from severe infections. By administering preparations
of gram-positive and gram-negative bacteria or their products to patients with
inoperable neoplastic diseases, Coley hoped to bring about an involution of the tumor.
The side effects of Coley’s regimen were unacceptable, however, and his treatment
ultimately fell into disrepute. The phenomenon that bacteria were capable of producing
a tumor necrotisizing factor stimulated other investigators. In 1975 Old and co-workers
identified a factor produced in mice pretreated with Bacillus Calmette-Guérin (BCG)
and subsequently challenged with lipopolysaccharide (LPS). This factor was able to
cause hemorrhagic necrosis of the meth A sarcoma, grown in the skin of a recipient
animal. The factor was dubbed “tumor necrosis factor” (TNF). A lot of articles
published both in scientific literature and in popular press claimed, that this molecule
would prove to be a revolutionary tool in the battle against cancer. However, phase I
and II clinical trials of systemic TNF were marked by a disappointing overall response
rate of 1-2% and a dose-limiting toxicity of hypotension. This dose-limiting toxicity
in patients kept the peak intravascular level achievable in humans 100-fold lower
than the level needed to have an anti-tumor effect in a mouse model. Because it

127
Summary and conclusions
seemed impossible to achieve effective systemic concentrations of TNF in patients,
TNF was ideally suited for use in HILP where levels up to 10 to 20 times the
systemically tolerated dose could be achieved. Ferdy Lejeune and Danielle Lienard,
surgical oncologists working in Brussels at the time, were the first to observe the
dramatic effect of tumor necrosis in humans using HILP with a combination of TNF,
interferon (IFN) and melphalan.
The second part of the introduction describes the technique of positron emission
tomography (PET). This is a non invasive, diagnostic imaging technique for measuring
the metabolic activity of cells in the human body with the aid of short-lived positron
emitting radiopharmaceuticals. Not only is it possible to visualize the metabolic
processes of a tumor but it is also possible to quantify the metabolic processes. PET
was used to evaluate tumor metabolism and with that tumor response before and
after HILP with TNF, IFN and melphalan.
Chapter 2
Osteosarcoma is the most frequent occurring primary malignant bone tumor in human.
During the past few decades, the use and further development of systemic neo adjuvant
chemotherapy, e.g., including high-dose methotrexate (HD-MTX) and cisplatin,
appears to have a definite influence on the disease free and overall survival for patients
with osteosarcoma. However, the potential local tumor effect of this systemically
administered chemotherapy is not always favorable. To increase the effect of cisplatin
on locoregional osteosarcoma, the short term effect of HILP with cisplatin (30 mg/L
extremity volume) was studied in 28 dogs with spontaneous osteogenic sarcoma
using clinical, radiological, and histological parameters. Thirty days postoperatively
mortality was 14.3 %. Total platinum levels at the start of perfusion were
28.2 ± 14.3 mg/L. A significant improvement (p<0.001) in the clinical score was
observed in the overall group at 6 and 12 weeks after perfusion. The radiological
parameter showed a stationary X-ray 2 weeks after perfusion and an improved X-ray
6 weeks after perfusion. Overall histological scores showed a moderate effect
according to the Huvos classification. No additional therapeutic effect, according to
the three parameters, could be demonstrated by increasing the perfusate temperature
by 1°C. HILP with cisplatin is feasible in the local treatment of spontaneous
osteosarcoma in dogs with acceptable locoregional toxicity. However, the histological
results were modest, with none of the dogs showing a complete response 6 weeks
after perfusion. Therefore the search for the ideal perfusion agent with substantial
contribution to the limb sparing treatment in human osteosarcoma, continues.

128
Chapter 9
Chapter 3
With the introduction of HILP with TNF, IFN and melphalan the question was raised
as to whether the combination of TNF with cisplatin in HILP could improve the
histological results after perfusion in dogs with spontaneous osteosarcoma. Before
starting with perfusion in dogs with osteosarcoma the feasibility of TNF perfusion
with and without cisplatin in healthy dogs was studied. During seven perfusions in
six mongrel dogs (weight 32±2 kg) the technical aspects of HILP under mild
hyperthermia (39-40o) were studied. In five experiments HILP was performed with
TNF alone (0.5 mg/L extremity volume), and in two experiments TNF was combined
with cisplatin (25 mg/L extremity volume). During the perfusions physiological
parameters were monitored and TNF and total cisplatin concentrations were
determined. Perfusion conditions (pH, PCO2, PO
2, flow and pressure) remained within
physiological ranges. Three dogs died within 24 hours despite a sublethal systemical
concentration of TNF that leaked from the perfusion circuit. Three dogs were
terminated; one dog after the second experiment in accordance with the Dutch ethical
rules; one dog because it showed an invagination of the small bowel resulting in an
ileus; one dog because of necrosis of the perfused limb. This feasibility study in
healthy dogs demonstrated that HILP with TNF and cisplatin was associated with a
high mortality rate and therefore does not allow us to treat dogs with spontaneous
osteosarcoma with TNF and cisplatin HILP.
Chapter 4
In order to study the value of HILP with cisplatin in the management of locally
advanced soft tissue sarcomas or metastatic bone sarcoma in humans, four patients
were treated in this manner under mild hyperthermia. Toxicity in the perfused limbs
was moderate, and the erythema and edema that occurred resolved spontaneously
within 7-14 days as did the slight motor and sensory neuropathy over a longer period
of time. Clinically, a reduction of pain was observed in all patients. Two weeks after
perfusion, tumor biopsies were taken to evaluate the response. Two patients showed
a pathological complete response, one patient showed >90% necrosis and one patient
showed no response. The histological results of this study were modest and with the
introduction of TNF in combination with melphalan as perfusion agents, no further
research with cisplatin as a perfusion agent was done.
Chapter 5
The first patient treated at the University Hospital Groningen with the perfusion
regimen of Lejeune, TNF with IFN and melphalan, had been treated with local
resection and adjuvant external beam radiotherapy 3 years earlier. Radiotherapy

129
Summary and conclusions
consisted of 40 Gy given 2 Gy per day in 4 weeks on the whole foot and a 20 Gy as
a boost on the tumor bed. The first recurrence of the lesion was treated by HILP with
cisplatin. After a second recurrence of the malignant fibrous histiocytoma and the
patient refusing curative amputation, was treated with HILP with 4 mg TNF, 0.2 mg
IFN and 45 mg melphalan. Already some hours after TNF perfusion, not only the
tumor on the foot showed a bluish color, but also the area that had been irradiated
three years ago. Nine days after TNF perfusion a lower leg amputation had to be
performed because of severe necrosis of the foot. Histology showed complete necrosis
of the tumor and marked thrombosis of the smaller vessels of the foot. TNF did not
only have a damaging influence on the endothelial cells of the tumor, but also on the
endothelial cells that developed after high dose irradiation therapy. An explanation
of the observed dramatic effect was described and the case served to alert other
surgeons in the field of TNF perfusions in treating patients with a history of irradiation
therapy.
Chapter 6
In order to study the glucose metabolism of soft tissue sarcomas before and after
HILP with TNF, IFN and melphalan, a FDG-PET study was performed in 20 patients
before to, 2 and 8 weeks after HILP. After the final PET study, the tumor was resected
and pathologically graded. Patients with a pathologically complete response (pCR)
showed no viable tumor after treatment. Those with a pathologically partial response
(pPR) showed various amounts of viable tumor in the resected tumor specimens.
Seven patients showed a pCR (35%) and 12 patients showed a pPR (60%). In one
patient, pathological examination was not performed (5%). The pre-perfusion glucose
consumption in the pCR group was significantly higher than in the pPR group
(p<0.05). Visual analysis of the PET images after perfusion showed a rim of increased
FDG uptake around a core of absent FDG uptake in 12 patients. The rim signal
contained a fibrous pseudocapsule with inflammatory tissue in the pCR group, but
viable tumor tissue was seen in the pPR group. The glucose consumption in the pCR
group at 2 and 8 weeks after perfusion had decreased significantly (p<0.05) compared
with the glucose consumption in the pPR group. Based on the pretreatment glucose
consumption in soft-tissue sarcomas one could predict the probability of a patient
achieving a complete pathologically response after TNF HILP. FDG-PET indicated
the pathologic tumor response to HILP, although the lack of specificity of FDG, in
terms of differentiation between an inflammatory response and viable tumor tissue,
hampered the discrimination between pCR and pPR.

130
Chapter 9
Chapter 7
After we had studied the glucose metabolism of tumors before and after HILP and
were confronted with the inability of FDG to discriminate between viable tumor
tissue and inflammatory tissue we decided to study the protein metabolism of tumors.
L-[1-11C]-tyrosine (TYR) was used as a tracer to study the protein metabolism before
and after HILP. Seventeen patients (5 women, 12 men; age range 24-75 y; mean age
52 y) were studied. TYR-PET studies were performed before HILP, and 2 and 8
weeks afterwards. The protein synthesis rates (PSRs) in nanomoles per milliliter per
minute were calculated. After the final PET study, the tumor was resected and
pathologically examined. Patients with a pathologically complete response (pCR)
showed no viable tumor after treatment. Those with a pathologically partial response
(pPR) showed various amounts of viable tumor in the resected tumor specimens. Six
patients showed a pCR (35%) and 11 patients showed a pPR (65%). All tumors were
depicted as a hot spot on the PET study before HILP. The PSR in the pCR group at 2
and 8 weeks after perfusion had decreased significantly (p<0.05) compared to the
PSR before HILP. A significant difference was found in PSR between the pCR and
pPR group at 2 as well as at 8 weeks (p<0.05). Median PSR in nonviable tumor
tissue was 0.62 and ranged from 0.22 to 0.91. With a threshold PSR of 0.91, sensitivity
and specificity of TYR-PET were 82% and 100%, respectively. The predictive value
of a PSR > 0.91 for having viable tumor tissue after HILP was 100%, whereas the
predictive value of a PSR ≤ 0.91 for having nonviable tumor tissue after HILP was
75%. On pathological examination the 2 patients in the pPR group with a PSR < 0.91
showed microscopic islets of tumor cells surrounded by extensive necrosis.
Inflammatory tissue after treatment did not interfere with viable tumor tissue on the
images. Combining the results of the FDG and TYR-PET studies, we concluded that
FDG-PET predicted the probability of a patient achieving a pathological complete
response after perfusion and TYR-PET gave a good indication of the pathological
outcome.
Chapter 8
With the introduction of TNF, the monitoring of leakage of the isolated circuit into
the systemic circulation is mandatory since TNF levels in the perfusion circuit are
approximately 10 times the maximum tolerated systemic levels. If significant leakage
occurs during HILP the resultant TNF induced systemic inflammatory response
syndrome (SIRS) could be fatal. The aim of this study was to analyze the value of
continuous leakage monitoring with radioactive Iodine-131 labeled human serum
albumin (RISA) in patients treated with HILP with TNF and melphalan. Forty-eight
patients with melanoma (n = 14) or soft tissue sarcoma (n = 34) of an extremity

131
Summary and conclusions
underwent 51 perfusions. Perfusion was performed at the iliac level in 22 cases, at
the popliteal level in 16 cases, at the femoral level in 7 cases and in 6 cases at the
axillary level. Leakage rates, perfusion circuit and systemic levels of TNF, interleukin-
6, C-reactive protein (CRP) were determined, as were systemic hematological and
metabolic profiles and tumor response. The mean isotopically measured leakage was
2.9 % (95% confidence interval 2.0 – 3.8%, range 0-15.5%). Systemic leakage was
≤2% in 28 perfusions (55%) and >2% in 23 perfusions (45%). The correlation between
the maximal monitored leakage and the maximal systemic TNF levels was 0.7114
(p < 0.0001). The area under the curve (AUC) for TNF in the perfusion circuit,
indicating the exposure of the perfused limb to TNF, was 18.7% lower in the >2%
leakage group (p=0.0457). No significant differences in tumor response were found
between groups. AUC for systemic TNF, indicating the exposure of the patient to
TNF, was 18.1 times higher in the >2% leakage group (p<0.0001) resulting in a
significant decrease in leukocyte and platelet count, hyperbilirubinemia,
hypocholesterolemia and proteinemia. No beneficial effect of the systemically leaked
TNF and melphalan was seen on the occurrence of distant metastasis during follow-
up. There was a significant difference between perfusions performed at the iliac and
femoral levels compared with leakage values at the popliteal level, p < 0.0001 and
0.0159 respectively. A good correlation between RISA leakage measurement and
TNF exposure during and after HILP with TNF and melphalan was demonstrated.
RISA leakage measurement serves as a good guide for the effectiveness of isolation
during perfusion. If leakage exceeds the 2% limit during perfusion, less exposure of
the tumor bearing limb to TNF, increased exposure of the patient systemic circulation
to TNF, and more systemic side effects can be expected.
Conclusions
1. HILP with cisplatin in dogs with spontaneous osteosarcoma can be done safely
with improvement of clinical and radiological parameters although histological
results were modest.
2. Since we encountered an unacceptable mortality and morbidity rate in HILP
with TNF and cisplatin in healthy dogs, an experiment in dogs with spontaneous
osteosarcoma was not initiated.
3. HILP with cisplatin in patients with sarcomas of soft tissue and bone resulted in
a reduction of pain after treatment. However, the histological outcome was
moderate.
4. HILP with TNF, IFN and melphalan does not only have an effect on the
vasculature of a tumor, but can also elicit an activation of the vasculature
originated after irradiation therapy.

132
Chapter 9
5. By studying the glucose metabolism of a tumor before HILP with TNF and
melphalan with the aid of FDG-PET, an assumption can be made about the
reaction of the tumor to TNF HILP.
6. In order to evaluate the result of HILP with TNF and melphalan one should
perform a TYR-PET study to measure the protein metabolism of the tumor after
HILP.
7. In order to determine leakage of TNF from the isolated circuit of the extremity
to the systemical circulation of the patient, continuous recording with radioactive
Iodine-131 labeled human serum albumin is an appropriate procedure.

133
Summary and conclusions
Samenvatting
Hoofdstuk 1
De Amerikaanse artsen Creech, Krementz, Ryan en Winbald pasten in de jaren vijftig
voor het eerst de techniek van geïsoleerde ledemaat perfusie (ILP) toe. Dankzij de
uitvinding van de hartlong machine, enige jaren tevoren ontwikkeld ten behoeve van
de hartchirurgie, konden zij de bloedsomloop van een arm of been tijdens een operatie
isoleren van de circulatie van de rest van het lichaam. Eenmaal aangesloten op een
hartlong machine was het mogelijk om aan dit geïsoleerde circuit een zeer hoge
dosis celdodende chemotherapeutica toe te voegen. Tumoren aan armen en benen
konden zo worden behandeld zonder dat vitale organen in de rest van het lichaam
van de patiënt werden blootgesteld aan chemotherapeutica.
Cavaliere en zijn medewerkers bestudeerden in de jaren zeventig het additionele
tumordodende effect van warmte, en legden daarmee de basis voor hypertherme
geïsoleerde ledemaat perfusie (HILP). Aanvankelijk vooral toegepast bij patiënten
met een melanoom (een kwaadaardige huidtumor) werd HILP later ook ingezet bij
de behandeling van tumoren van de weke delen (spieren, bindweefsel en bot). Door
de jaren heen zijn verschillende chemotherapeutica gebruikt met wisselend succes.
William Coley, een New Yorkse chirurg die aan het eind van de negentiende eeuw
leefde, ontdekte dat een extract van bacteriën, ingespoten in tumoren, in enkele
gevallen een regressie van de tumor opleverde. Soms was het middel echter erger
dan de kwaal en overleden patienten aan deze behandeling. Overtuigd van de gedachte
dat bacteriën een factor tegen tumoren konden produceren diende Old en zijn
medewerkers in 1975 endotoxine (een bestanddeel van de celwand van sommige
bacteriën) aan muizen toe. Het bloed van deze met endotoxine behandelde muizen
bleek bij andere muizen een ineenschrompelen van de tumor te veroorzaken. De met
endotoxine behandelde muizen moesten dus een factor in het bloed gemaakt hebben
die tumoren bij de tweede groep muizen deed verdwijnen. Deze tumordodende factor
kreeg de illustere naam ‘tumor necrosis factor’, kortweg TNF. Aanvankelijk waren
de verwachtingen over de kanker genezende werking van TNF hooggespannen. Toen
TNF echter na DNA recombinant technieken voor klinische trials beschikbaar kwam,
bleek het al in een zeer lage dosering ernstige bijwerkingen te hebben. Patiënten
toonden het beeld van een ernstige infectie met symptomen van lage bloeddruk,
koorts, verminderde hartwerking en een onvoldoende doorbloeding van de organen.
Een effect op de tumoren van deze patiënten werd nauwelijks waargenomen. TNF
leek dus niet alleen een tumordodend effect te hebben, maar eveneens een centrale
rol te spelen bij ontstekingsreacties. Aangezien ILP een 10 tot 20 keer zo hoge dosering

134
Chapter 9
van chemotherapie mogelijk maakt in een geïsoleerde extremiteit, kwamen twee
Belgische chirurgen, Lejeune en Lienard, op het idee om TNF in de ILP setting te
gebruiken. Met TNF alleen bereikten zij onvoldoende effect, maar in combinatie
met melphalan waren de resultaten opzienbarend. Voor het eerst werd het effect van
tumornecrose, zoals dat eerder bij muizen werd gezien, ook waargenomen bij mensen.
Het tweede deel van de introductie geeft een overzicht van het werkingsmechanisme
van de techniek ‘positron emissie tomografie’ (PET). Met behulp van positron
uitzendende ‘tracers’ kan het metabolisme van tumoren niet alleen zichtbaar worden
gemaakt, maar ook in maat en getal worden uitgedrukt. Deze nieuwe techniek werd
gebruikt om de veranderingen in het tumormetabolisme te bestuderen voor en na
behandeling met HILP.
Hoofdstuk 2
Het osteosarcoom is de meest voorkomende bottumor bij de mens en komt met name
bij jonge mensen voor. Begin jaren zeventig werd een grote stap voorwaarts gezet in
de behandeling van deze tumoren door de introductie van systemische neoadjuvant
chemotherapie met hoge doseringen methotrexaat en cisplatinum. Evenwel, met deze
systemische chemotherapie leken vooral (micro)metastasen in de longen behandeld
te worden die bepalend waren voor de prognose; het lokale effect op de primaire
tumor was niet altijd optimaal. De vraag was of dit lokale effect verhoogd kon worden
door patiënten met een osteosarcoom van arm of been eerst te behandelen met HILP
en cisplatinum als chemotherapeuticum waarvoor het osteosarcoom gevoelig is.
Voorafgaand aan een klinische toepassing werd eerst een studie bij honden verricht.
Achtentwintig honden met een osteosarcoom werden behandeld met een cisplatinum
HILP. Het effect van de behandeling werd geëvalueerd aan de hand van klinische,
radiologische en histologische parameters. Zes weken na behandeling toonde het
looppatroon en de radiologische parameters een significante verbetering. Het
histologisch effect van de behandeling was bescheiden volgens de classificatie van
Huvos. Vier honden overleden binnen 30 dagen na behandeling. Door de temperatuur
van de perfusie met 1 °C te verhogen naar 42 °C werd geen significante verbetering
gezien ten opzichte van de groep honden die met een lagere temperatuur waren
behandeld.
Geconcludeerd kon worden dat HILP bij honden met een osteosarcoom goed
uitvoerbaar was met verbetering van de klinische en radiologische parameters. Het
histologisch effect was echter onvoldoende en het zoeken naar het ideale perfusie
chemotherapeuticum voor behandeling van het osteosarcoom moest daarom worden
voortgezet.

135
Summary and conclusions
Hoofdstuk 3
Met de introductie van ‘tumor necrosis factor’ gebruikt bij HILP, ontstond de vraag
of het histologisch effect van cisplatinum bij honden met een osteosarcoom wellicht
verbeterd kon worden als TNF werd toegevoegd. Alvorens honden met een
osteosarcoom te behandelen werd eerst bij gezonde honden gekeken naar het effect
van een perfusie met TNF alleen en de combinatie met TNF en cisplatinum.
Bij 6 honden werden 7 perfusies verricht met milde hyperthermie. Gedurende 5
perfusies werd alleen TNF gebruikt en in twee gevallen werd hier cisplatinum aan
toegevoegd. Perfusie condities zoals pH, pCO2, pO
2, de stroom van het perfusaat en
de druk bleven binnen fysiologische grenzen. Drie honden overleden binnen 24 uur
na de perfusie ondanks een gemeten subletale systemische dosis van TNF. Drie honden
moesten worden afgemaakt. Eén hond omdat deze nog een tweede perfusie aan een
andere poot onderging; conform de Nederlandse ethische regelgeving mag na een
tweede experiment een dier niet meer uit een narcose ontwaken. Eén hond kreeg na
behandeling een ileus berustend op een invaginatie van de darm. De derde hond
ontwikkelde een totale necrose van de met TNF en cisplatinum geperfundeerde poot.
Gezien de onacceptabele mortaliteit en morbiditeit bij deze experimenten werd het
niet zinvol geacht om een experiment te starten waarbij honden met een osteosarcoom
op deze manier behandeld zouden worden.
Hoofdstuk 4
Om het effect van HILP met cisplatinum bij patiënten met een weke delen sarcoom
of een osteosarcoom te beoordelen werden vier patiënten op deze wijze behandeld
onder milde hyperthermie. De toxiciteit na perfusie was gering, erytheem en oedeem
verdwenen tussen de 7de tot 14de dag postoperatief evenals de lichte motorische en
sensorische neuropathie. Klinisch stond met name een vermindering van de pijn op
de voorgrond. Twee weken na behandeling werden histologische biopten van de tumor
genomen. Bij twee patiënten werden in deze biopten geen vitale tumorcellen
gevonden, bij één patiënt was er sprake van meer dan 90% necrose in de biopten en
bij één patiënt werd geen histologisch effect van de perfusie gezien. De resultaten
van deze studie waren veel belovend, maar verder onderzoek naar de
toepassingsmogelijkheden van cisplatinum als perfusie chemotherapeuticum werd
niet meer uitgevoerd, omdat het gebruik van TNF in combinatie met melphalan toen
in zwang kwam.
Hoofdstuk 5
De eerste patiënt die in Groningen met het perfusie-regime van Lejeune behandeld
werd (TNF in combinatie met IFN en melphalan) was drie jaar eerder behandeld met

136
Chapter 9
lokale excisie gevolgd door bestraling met 40 Gy gegeven in 2 Gy per dag gedurende
4 weken. Twee jaar later werd een eerste recidief van de tumor behandeld met een
cisplatinum perfusie. Na een complete regressie recidiveerde de tumor opnieuw en
omdat perfusie met TNF, IFN en melphalan het enige alternatief was voor amputatie
werd de patiënte op deze manier behandeld. Kort na perfusie trad er een blauwe
verkleuring op van de tumor maar ook van het gebied dat 3 jaar eerder bestraald was.
Negen dagen na perfusie was alsnog een amputatie van de voet noodzakelijk wegens
de ernstige necrose die was opgetreden. Histologisch onderzoek toonde necrose van
de tumor aan maar ook trombusvorming in de capillairen in het bestraalde gebied.
TNF bleek niet alleen een effect te hebben op het endotheel van de tumorvaten, maar
ook op het endotheel van bloedvaten ontstaan na bestraling. Een mogelijk
werkingsmechanisme werd beschreven en de casus diende als waarschuwing voor
andere chirurgen die zich met TNF HILP bezig hielden om voorzichtig te zijn bij
patiënten die reeds eerder waren bestraald.
Hoofdstuk 6
Om het glucose metabolisme van weke delen sarcomen te bestuderen voor en na
behandeling met TNF HILP, werd bij twintig patiënten voor perfusie, twee weken na
perfusie en acht weken na perfusie een positron emissie tomografie (PET) studie
verricht met 18Fluorine-gelabeled 2-fluoro-2-deoxy-D-glucose (FDG). Na de laatste
FDG-PET studie werd het restant van de tumor geëxcideerd en pathologisch
onderzocht. Deze pathologische bevindingen werden met de gegevens van de PET-
studie vergeleken. Bij een pathologisch complete response (pCR), werden er geen
vitale tumorcellen in het resectie preparaat gevonden. Indien er nog wel vitale
tumorcellen werden gevonden werd een pathologisch partiele response (pPR)
geclassificeerd. Zeven patiënten hadden een complete respons (35%), 12 patiënten
een partiële respons (60%) en bij één patiënt (5%) werd geen pathologisch onderzoek
verricht. Bij tumoren die een complete respons toonden na de perfusie was het
glucosemetabolisme voor de perfusie significant verhoogd. Visuele analyse van de
PET-studies na perfusie lieten een rand van verhoogd glucosemetabolisme zien om
een kern van verminderd glucosemetabolisme bij 12 patiënten. Bij patiënten met een
complete respons bevatte deze rand een pseudo-kapsel met ontstekingscellen, echter
bij patiënten met een partiele respons werd nog vitaal tumorweefsel in de rand
gevonden. De kern bestond uit necrotisch vervallen tumorweefsel. Het
glucosemetabolisme van de patiënten met een complete respons daalde significant
na de perfusie, terwijl deze daling bij patiënten met een partiele respons minder
uitgesproken was.
Aan de hand van het glucosemetabolisme voor perfusie viel te voorspellen of een

137
Summary and conclusions
patiënt gunstig zou reageren op een behandeling met een perfusie van TNF en
melphalan. Tevens gaf FDG-PET na de behandeling een indicatie over het bereikte
effect, maar het was niet goed mogelijk om te differentiëren tussen een complete of
een partiele respons, gezien de overlap in glucosemetabolisme van tumor- en
ontstekingsweefsel.
Hoofdstuk 7
Nu duidelijk was dat zich bij het bestuderen van het glucosemetabolisme met behulp
van PET een differentiatieprobleem van ontstekingsweefsel en tumorweefsel voor
deed, werd een nieuwe weg ingeslagen. Besloten werd om het eiwitmetabolisme van
tumoren voor en na behandeling met een TNF/melphalan perfusie te bestuderen. Als
tracer voor het eiwitmetabolisme werd L-[1-11C]-tyrosine (TYR) gebruikt. Zeventien
patiënten werden in deze studie bestudeerd. Ook nu werd een TYR-PET studie voor,
twee weken na en acht weken na perfusie verricht en werden de resultaten vergeleken
met die van pathologisch onderzoek van het gereseceerde tumorweefsel. Zes patiënten
(35%) hadden bij pathologisch onderzoek geen vitaal tumorweefsel meer en toonden
een complete respons. Elf patiënten (65%) hadden nog vitaal tumorweefsel in het
gereseceerde preparaat en toonden daarmee een partiele respons. Voor behandeling
waren alle tumoren goed zichtbaar met TYR-PET. Patiënten die na perfusie een
complete respons toonden hadden een significante daling van het eiwitmetabolisme,
dit in tegenstelling tot patiënten met een partiële respons. Bij een eiwitmetabolisme-
grenswaarde van 0,91 of hoger was er na perfusie nog altijd sprake van vitaal
tumorweefsel bij pathologisch onderzoek. Indien het eiwitmetabolisme lager was
dan 0,91 bleek er bij twee patiënten bij pathologisch onderzoek nog sprake te zijn
van vitaal tumorweefsel. Dit vitaal ogende tumorweefsel werd echter omgeven door
necrotisch tumorweefsel. Aan de hand van het berekende eiwitmetabolisme na perfusie
was het dus mogelijk om het effect van de behandeling te beoordelen.
Ontstekingsweefsel intervereerde niet met vitaal tumorweefsel voor wat betreft het
eiwitmetabolisme. Deze studie, in combinatie met die beschreven in hoofdstuk 6,
levert op dat met FDG-PET accuraat te voorspellen is of een tumor goed op de
perfusiebehandeling zal reageren; bovendien is het met TYR-PET mogelijk om het
resultaat van die behandeling te evalueren op de aanwezigheid van vitaal
tumorweefsel.
Hoofdstuk 8
Aangezien er tijdens perfusie met hoge dosis chemotherapeutica wordt gewerkt in
het geïsoleerde circuit is het van belang om elke vorm van lekkage naar de rest van
het lichaam te voorkomen. Mocht lekkage toch optreden, dan is het van belang om te

138
Chapter 9
meten in welke mate. Met name sinds de introductie van TNF, dat al in een zeer lage
dosering sterke toxische gevolgen kan hebben, is dit aspect belangrijk geworden.
Van oudsher wordt lekkage tijdens perfusie met radioactief Jodium-131 gelabeled
serum albumine (RISA) gemeten. Hierbij wordt een lage dosis RISA aan de
systemische circulatie van de patiënt toegediend en een tien keer hogere dosering
aan het geïsoleerde perfusie circuit. Bij lekkage van het perfusie circuit naar de
systemische circulatie zal er een toename van de radioactiviteit in het lichaam van de
patiënt optreden. Dit wordt met behulp van een teller geplaatst boven het hart van de
patiënt gemeten. In dit hoofdstuk werd gekeken naar de correlatie tussen deze
radioactief gemeten lekkage en de systemisch gemeten waarden van TNF.
Achtenveertig patiënten ondergingen 51 perfusies met TNF en melphalan. In 22
gevallen betrof het een perfusie op iliacaal niveau, in 16 gevallen op popliteaal niveau,
in zeven gevallen op femoraal niveau en zes patiënten ondergingen een perfusie van
de arm. Lekkage waarden, systemische en perfusie circuitspiegels van TNF, IL-6 en
CRP werden bepaald alsmede systemische hematologische en metabolische spiegels.
Tevens werd er gekeken of er een verband was tussen lekkage en tumorresponse.
Gemiddeld was de lekkage 2,9% (spreiding 0-15,5%). Bij 28 perfusies was de lekkage
≤2% en bij 23 perfusies >2%. De correlatiecoëfficiënt tussen de maximaal gemeten
lekkage gedurende de perfusie en de maximale TNF-spiegel in de systemische
circulatie van de patiënt was 0.7114 (P<0.0001). De oppervlakte onder de
concentratiecurve van TNF gemeten in het perfusiecircuit, als indicator voor de
blootstelling van de tumor aan de hoeveelheid TNF, was 18,7% lager in de groep van
patiënten met >2% lekkage (P=0.0457). Er werd geen significant verschil gezien in
tumorrespons tussen beide lekkage groepen ondanks het feit dat de blootstelling van
de tumor aan TNF in de lage lekkage groep hoger was. Vergelijkenderwijs werd de
systemische circulatie van de patiënt in de groep met >2% lekkage aan een 18,1
maal hogere TNF dosering blootgesteld hetgeen resulteerde in een significante daling
van het leukocyten- en trombocytengetal. Ook werd vaker een hyperbilirubinaemie,
een hypocholestoroleamie en een proteïnemie vastgesteld. Een gunstig effect van de
verhoogde concentratie van TNF in de >2% lekkage groep op het in de follow-up
optreden van afstandsmetastasen werd niet gezien. Perfusies op iliacaal en femoraal
niveau hadden een significant hoger lekkage-percentage in vergelijking met perfusies
op popliteaal niveau. Gezien de goede correlatie tussen lekkage en gemeten
systemische TNF waarden kon worden gesteld dat lekkage gemeten door middel van
RISA een goede richtlijn geeft gedurende de perfusie over de lekkage. Indien de
lekkage ≤2% is wordt de tumor in de geperfundeerde extremiteit aan een hogere
dosering TNF blootgesteld en de systemische circulatie van de patiënt aan een
significant lagere dosering.

139
Summary and conclusions
Conclusies
1. HILP met cisplatinum bij honden met een osteosarcoom is goed uitvoerbaar met
verbetering van de klinische en radiologische parameters na behandeling. Het
histologisch effect is echter onvoldoende.
2. Gezien de onacceptabele mortaliteit en morbiditeit bij HILP met TNF en
cisplatinum bij gezonde honden is het niet zinvol een experiment bij honden
met een osteosarcoom uit te voeren.
3. HILP met cisplatinum bij patiënten met een wekedelen sarcoom of een
osteosarcoom resulteert met name in een afname van pijn na behandeling. Ook
hier zijn de histologische resultaten echter bescheiden.
4. HILP met TNF, IFN en melphalan kan naast een effect op de neovascularisatie
van tumoren ook invloed hebben op endotheel ontstaan na radiotherapie.
5. Door het glucose metabolisme van een tumor voor HILP met TNF en melphalan
te bestuderen middels FDG-PET is het mogelijk om te voorspellen of een tumor
goed op de behandeling zal reageren.
6. Om het resultaat van HILP met TNF en melphalan te bestuderen is het bepalen
van het eiwitmetabolisme door middel van TYR-PET na perfusie de aangewezen
methode.
7. Om lekkage van TNF vanuit de geïsoleerde circulatie in de extremiteit naar de
rest van het lichaam te bepalen is continue meeting met radioactief Jodium-131
gelabeled serum albumine waardevol.

140
DANKWOORD
Ook dit proefschrift is kunnen ontstaan door de samenwerking van velen. Het is
moeilijk om volledig te zijn maar al diegene die een bijdrage geleverd hebben wil ik
hartelijk bedanken voor hun inzet en hulp. Hierbij gaan mijn gedachten uit naar de
verpleegkundigen van de verpleegafdeling chirurgische oncologie, de verpleeg-
kundigen van het operatie centrum, de verpleegkundigen van de chirurgische intensive
care, de registratie assistenten van de polikliniek chirurgie, de laboranten van de diverse
laboratoria, en de perfusionisten van het Academisch Ziekenhuis Groningen. De
medewerkers van het PET-centrum en de afdeling nucleaire geneeskunde van het
zelfde ziekenhuis, alsmede de medewerkers van het Centraal Dierenlaboratorium van
de Rijksuniversiteit Groningen.
In het bijzonder dank ik prof. dr. H.J. Hoekstra, prof. dr. Schraffordt Koops en prof.
dr. W. Vaalburg voor het in mij gestelde vertrouwen, hun steun en begeleiding.
Prof. Dr. H.J. Hoekstra, beste Harald, na mijn diensttijd bood jij mij als arts-
onderzoeker de gelegenheid en vrijheid om bij de chirurgische oncologie te komen
werken als arts onderzoeker. Enkele gingen mij vooraf en velen zouden mij volgen
en dat kan ook niet anders met jou enthousiasme en vindingrijkheid op
onderzoeksgebied. Op naar het volgende decennium.
Prof. Dr. H. Schraffordt Koops, als een van de pioniers in Nederland op het gebied
van de TNF perfusies legde u de basis voor een diversiteit aan onderzoeken. Het was
een leerzame ervaring een radar van het geheel te zijn.
Prof. Dr. W. Vaalburg, bedankt voor de prima sfeer op het PET-centrum met een
groep van enthousiaste medewerkers en een diversiteit aan specialismen die op het
PET-centrum onderzoek doen.
De leden van de beoordelingscommissie, bestaande uit prof. dr. B.B.R. Kroon, prof.
dr. M.F. von Meyenfeldt en prof. dr. W.M. Molenaar ben ik dank verschuldigd voor
de beoordeling van dit proefschrift.
Ik wil alle patiënten, honden en hun eigenaren bedanken voor hun onmisbare bijdrage
bij het tot stand komen van dit proefschrift.

141
Alle chirurgen en mijn collega assistenten in het Academisch Ziekenhuis Groningen
en het Medisch Centrum Leeuwarden wil ik bedanken voor de samenwerking en
hetgeen ik heb mogen leren tijdens mijn opleiding tot chirurg.
Drs. D. Klees en drs. R.P. Winkel, beste Dirk en Robert, bij de gedachte aan paranimfen
kwamen jullie als eerste in beeld. Hoe zou dat toch komen ?
Grote dank ben ik verschuldigd aan mijn ouders die mij alle kans hebben geboden
om mijzelf te ontplooien. Pa heeft de afronding van mijn promotie helaas niet meer
mee kunnen maken. In dierbare herinnering draag ik dit proefschrift aan hem op
wetende dat hij het weet.
Lieve Klaar, jij bent onmisbaar. Na tien jaar, drie kinderen, een opleiding en een
eigenzaak verder, blijft thuis het belangrijkste gelukkig ben jij er om alles in goede
banen te leiden.
Joris, Ties en Maxime, jullie gekwek klinkt als muziek in papa’s oren als ik boven
wat probeer te werken en voor een “koffie koppie” drinken blijf ik graag naar beneden
komen.

142
Curriculum Vitae
Robert Johannes van Ginkel was born on May 12th , 1964 in Amsterdam, the
Netherlands. After finishing high school (Rythoviuscollege, Eersel) in 1982, he went
to the Technical University Eindhoven to study Chemistry. After one year he went to
Medical School at the University of Groningen. After graduation in 1991 he served
in the Royal Dutch Army in the Hague, the Netherlands. From February 1993 until
December 1995 he joined a research program at the Department of Surgical Oncology,
University Hospital Groningen (Prof. dr. H. Schraffordt Koops). In January 1995
until September 1996 he worked as a transplant coordinator of the Northern and
Eastern part of the Netherlands. In September 1996 he started his training in Surgery
at the Surgical Department of the University Hospital Groningen (Prof. dr. R. van
Schilfgaarde) followed in September 1999 at the Surgical Department of the Medical
Center Leeuwarden, the Netherlands (Dr. D.C. Busman).

143
Publications
van Ginkel RJ, Kole AC, Nieweg OE, Molenaar WM, Pruim J, Koops HS, Vaalburg W,
Hoekstra HJ. L-[1-11C]-tyrosine PET to evaluate response to hyperthermic isolated limb
perfusion for locally advanced soft-tissue sarcoma and skin cancer. J Nucl Med 1999; 40:
262-267.
Olieman AF, Pras E, van Ginkel RJ, Molenaar WM, Schraffordt Koops H, Hoekstra HJ.
Feasibility and efficacy of external beam radiotherapy after hyperthermic isolated limb
perfusion with TNF-alpha and melphalan for limb-saving treatment in locally advanced
extremity soft- tissue sarcoma. Int J Radiat Oncol Biol Phys 1998; 40: 807-814.
Olieman AF, van Ginkel RJ, Molenaar WM, Schraffordt Koops H, Hoekstra HJ. Hyperthermic
isolated limb perfusion with tumour necrosis factor- alpha and melphalan as palliative limb-
saving treatment in patients with locally advanced soft-tissue sarcomas of the extremities
with regional or distant metastases. Is it worthwhile? Arch Orthop Trauma Surg 1998; 118:
70-74.
Olieman AF, van Ginkel RJ, Hoekstra HJ, Mooyaart EL, Molenaar WM, Koops HS.
Angiographic response of locally advanced soft-tissue sarcoma following hyperthermic
isolated limb perfusion with tumor necrosis factor. Ann Surg Oncol 1997; 4: 64-69.
Sleijfer S, van Ginkel RJ, van der Mark TW, Hoekstra HJ, Zwaveling JH, Schraffordt Koops
H, Mulder NH. Effects of hyperthermic isolated limb perfusion with tumor necrosis factor-
alpha and melphalan on pulmonary function assessments. J Immunother 1997; 20: 202-207.
Zwaveling JH, Hoekstra HJ, Maring JK, van Ginkel RJ, Schraffordt Koops H, Smit AJ,
Girbes AR. Renal function in cancer patients treated with hyperthermic isolated limb perfusion
with recombinant tumor necrosis factor- alpha and melphalan. Nephron 1997; 76: 146-152.
Kole AC, Pruim J, Nieweg OE, van Ginkel RJ, Hoekstra HJ, Schraffordt Koops H, Vaalburg
W. PET with L-[1-carbon-11]-tyrosine to visualize tumors and measure protein synthesis
rates. J Nucl Med 1997; 38: 191-195.
Kole AC, Nieweg OE, van Ginkel RJ, Pruim J, Hoekstra HJ, Paans AM, Vaalburg W, Koops
HS. Detection of local recurrence of soft-tissue sarcoma with positron emission tomography
using [18F]fluorodeoxyglucose. Ann Surg Oncol 1997; 4: 57-63.
van Ginkel RJ, Schraffordt Koops H, de Vries EG, Molenaar WM, Uges DR, Hoekstra HJ.
Hyperthermic isolated limb perfusion with cisplatin in four patients with sarcomas of soft
tissue and bone. Eur J Surg Oncol 1996; 22: 528-531.
van Ginkel RJ, Hoekstra HJ, Pruim J, Nieweg OE, Molenaar WM, Paans AM, Willemsen
AT, Vaalburg W, Koops HS. FDG-PET to evaluate response to hyperthermic isolated limb
perfusion for locally advanced soft-tissue sarcoma. J Nucl Med 1996; 37: 984-990.

144
Zwaveling JH, Maring JK, Clarke FL, van Ginkel RJ, Limburg PC, Hoekstra HJ, Koops HS,
Girbes AR. High plasma tumor necrosis factor (TNF)-alpha concentrations and a sepsis-like
syndrome in patients undergoing hyperthermic isolated limb perfusion with recombinant
TNF-alpha, interferon- gamma, and melphalan. Crit Care Med 1996; 24: 765-770.
Zwaveling JH, Maring JK, Mulder AB, Bom VJ, van Ginkel RJ, Schraffordt Koops H, Girbes
AR, Hoekstra HJ, van der Meer J. Effects of hyperthermic isolated limb perfusion with
recombinant tumor necrosis factor alpha and melphalan on the human fibrinolytic system.
Cancer Res 1996; 56: 3948-3953.
Nieweg OE, Pruim J, van Ginkel RJ, Hoekstra HJ, Paans AM, Molenaar WM, Koops HS,
Vaalburg W. Fluorine-18-fluorodeoxyglucose PET imaging of soft-tissue sarcoma. J Nucl
Med 1996; 37: 257-261.
van Ginkel RJ, Hoekstra HJ, Eggermont AMM, Pras E, Koops HS. Isolated limb perfusion
of an irradiated foot with tumor necrosis factor, interferon, and melphalan. Arch Surg 1996;
131: 672-674.
Zwaveling JH, Maring JK, Moshage H, van Ginkel RJ, Hoekstra HJ, Schraffordt Koops H,
Donse IF, Girbes AR. Role of nitric oxide in recombinant tumor necrosis factor-alpha- induced
circulatory shock: a study in patients treated for cancer with isolated limb perfusion. Crit
Care Med 1996; 24: 1806-1810.
Mulder AB, Zwaveling JH, Smid WM, Maring JK, van Ginkel RJ, Girbes AR, Schraffordt
Koops H, van der Meer J. Augmented procoagulant activity in cancer patients, treated with
recombinant interferon-gamma in addition to recombinant tumor necrosis factor-alpha and
melphalan. Thromb Haemost 1996; 76: 897-901.
van Ginkel RJ, Hoekstra HJ, Meutstege FJ, Oosterhuis JW, Uges DRA, Schraffordt Koops
H. Hyperthermic isolated regional perfusion with cisplatin in the local treatment of
spontaneous canine osteosarcoma: assessment of short-term effects. J Surg Oncol 1995; 59:
169-176.