united way of east central iowa 990 fy 2013
DESCRIPTION
United Way of East Central Iowa 990 FY 2013TRANSCRIPT

Checkifself-employed
OMB No. 1545-0047
Department of the TreasuryInternal Revenue Service
Check ifapplicable:
AddresschangeNamechangeInitialreturn
Termin-atedAmendedreturn Gross receipts $
Applica-tionpending
232001 12-10-12
Beginning of Current Year
Paid
Preparer
Use Only
Under section 501(c), 527, or 4947(a)(1) of the Internal Revenue Code (except black lungbenefit trust or private foundation)
Open to Public Inspection
A For the 2012 calendar year, or tax year beginning and ending
B C D Employer identification number
E
G
H(a)
H(b)
H(c)
F Yes No
Yes No
I
J
K
Website: |
L M
1
2
3
4
5
6
7
3
4
5
6
7a
7b
a
b
Ac
tivi
tie
s &
Go
vern
an
ce
Prior Year Current Year
8
9
10
11
12
13
14
15
16
17
18
19
Re
ven
ue
a
b
Exp
en
se
s
End of Year
20
21
22
Sign
Here
Yes No
For Paperwork Reduction Act Notice, see the separate instructions.
|
(or P.O. box if mail is not delivered to street address) Room/suite
Are all affiliates included?
)501(c)(3) 501(c) ( (insert no.) 4947(a)(1) or 527
|Corporation Trust Association OtherForm of organization: Year of formation: State of legal domicile:
|
|
Net
Ass
ets
orFu
nd B
alan
ces
Under penalties of perjury, I declare that I have examined this return, including accompanying schedules and statements, and to the best of my knowledge and belief, it is
true, correct, and complete. Declaration of preparer (other than officer) is based on all information of which preparer has any knowledge.
Signature of officer Date
Type or print name and title
Date PTINPrint/Type preparer's name Preparer's signature
Firm's name Firm's EIN
Firm's address
Phone no.
Form
The organization may have to use a copy of this return to satisfy state reporting requirements.
Name of organization
Doing Business As
Number and street Telephone number
City, town, or post office, state, and ZIP code
Is this a group return
for affiliates?Name and address of principal officer:
If "No," attach a list. (see instructions)
Group exemption number |
Tax-exempt status:
Briefly describe the organization's mission or most significant activities:
Check this box if the organization discontinued its operations or disposed of more than 25% of its net assets.
Number of voting members of the governing body (Part VI, line 1a)
Number of independent voting members of the governing body (Part VI, line 1b)
Total number of individuals employed in calendar year 2012 (Part V, line 2a)
~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~
Total number of volunteers (estimate if necessary)
Total unrelated business revenue from Part VIII, column (C), line 12
Net unrelated business taxable income from Form 990-T, line 34
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~
����������������������
Contributions and grants (Part VIII, line 1h) ~~~~~~~~~~~~~~~~~~~~~
Program service revenue (Part VIII, line 2g) ~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~Investment income (Part VIII, column (A), lines 3, 4, and 7d)
Other revenue (Part VIII, column (A), lines 5, 6d, 8c, 9c, 10c, and 11e) ~~~~~~~~
Total revenue - add lines 8 through 11 (must equal Part VIII, column (A), line 12) ���
Grants and similar amounts paid (Part IX, column (A), lines 1-3)
Benefits paid to or for members (Part IX, column (A), line 4)
Salaries, other compensation, employee benefits (Part IX, column (A), lines 5-10)
~~~~~~~~~~~
~~~~~~~~~~~~~
~~~
Professional fundraising fees (Part IX, column (A), line 11e)
Total fundraising expenses (Part IX, column (D), line 25)
~~~~~~~~~~~~~~
Other expenses (Part IX, column (A), lines 11a-11d, 11f-24e)
Total expenses. Add lines 13-17 (must equal Part IX, column (A), line 25)
Revenue less expenses. Subtract line 18 from line 12
~~~~~~~~~~~~~
~~~~~~~
����������������
Total assets (Part X, line 16)
Total liabilities (Part X, line 26)
Net assets or fund balances. Subtract line 21 from line 20
~~~~~~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~~~
��������������
May the IRS discuss this return with the preparer shown above? (see instructions) ���������������������
LHA Form (2012)
Part I Summary
Signature BlockPart II
990
Return of Organization Exempt From Income Tax990 2012
§
==
999
JUL 1, 2012 JUN 30, 2013
UNITED WAY OF EAST CENTRAL IOWA, INC.42-0861239
317 7TH AVENUE SE 401 319-398-537211,591,128.
CEDAR RAPIDS, IA 52401-1604LOIS BUNTZ X
SAME AS C ABOVEX
WWW.UWECI.ORGX 1962 IA
UNITED WAY OF EAST CENTRAL IOWAWORKS TO ADVANCE THE COMMON GOOD BY FOCUSING ON THE BUILDING BLOCKS
313062
2500.0.
11,175,928. 10,724,807.122,423. 116,877.127,532. 106,814.123,378. 195,138.
11,549,261. 11,143,636.8,403,648. 8,505,487.
0. 0.1,680,911. 1,982,776.
0. 0.643,935.
892,005. 923,349.10,976,564. 11,411,612.
572,697. -267,976.
26,361,067. 25,791,627.7,881,908. 7,734,748.
18,479,159. 18,056,879.
LOIS BUNTZ, PRESIDENT/CEO
KAY HEGARTY P00091057MCGLADREY LLP 42-0714325221 THIRD AVENUE SE, STE 300CEDAR RAPIDS, IA 52401-1512 319-298-5333
X
SEE SCHEDULE O FOR ORGANIZATION MISSION STATEMENT CONTINUATION

Code: Expenses $ including grants of $ Revenue $
Code: Expenses $ including grants of $ Revenue $
Code: Expenses $ including grants of $ Revenue $
Expenses $ including grants of $ Revenue $
23200212-10-12
1
2
3
4
Yes No
Yes No
4a
4b
4c
4d
4e Total program service expenses
Form 990 (2012) Page
Check if Schedule O contains a response to any question in this Part III �����������������������������
Briefly describe the organization's mission:
Did the organization undertake any significant program services during the year which were not listed on
the prior Form 990 or 990-EZ?
If "Yes," describe these new services on Schedule O.
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Did the organization cease conducting, or make significant changes in how it conducts, any program services?
If "Yes," describe these changes on Schedule O.
~~~~~~
Describe the organization's program service accomplishments for each of its three largest program services, as measured by expenses.
Section 501(c)(3) and 501(c)(4) organizations are required to report the amount of grants and allocations to others, the total expenses, and
revenue, if any, for each program service reported.
( ) ( ) ( )
( ) ( ) ( )
( ) ( ) ( )
Other program services (Describe in Schedule O.)
( ) ( )
Form (2012)
2Statement of Program Service AccomplishmentsPart III
990
J
UNITED WAY OF EAST CENTRAL IOWA, INC. 42-0861239
X
UNITE THE CARING POWER OF COMMUNITIES TO INVEST IN EFFECTIVE SOLUTIONSTO IMPROVE PEOPLE'S LIVES.
X
X
3,236,081. 2,753,790.EDUCATION: HELPING CHILDREN AND YOUTH ACHIEVE THEIR POTENTIAL
COMMUNITY STRATEGIES:
YOUTH ACHIEVEMENT CORPS: A PARTNERSHIP WITH LOCAL SCHOOLS ANDNONPROFITS THAT LEVERAGES FEDERAL DOLLARS TO PLACE AMERICORPSVOLUNTEERS IN EARLY CHILDHOOD PROGRAMS, ELEMENTARY SCHOOLS, AND MIDDLESCHOOLS TO SUPPORT YOUTH FROM BIRTH THROUGH MIDDLE SCHOOL IN ACADEMICAND SOCIAL SKILLS.
READ EVERY DAY (RED) AHEAD: PROVIDES EDUCATIONAL MATERIALS, BOOKS, ANDPARENTING RESOURCES TO SERVE ECONOMICALLY DISADVANTAGED FAMILIES HELP
2,071,297. 1,762,600.INCOME: PROMOTING FINANCIAL STABILITY AND INDEPENDENCE
COMMUNITY STRATEGIES:
FAMILY FINANCIAL STABILITY: UNITED WAY IS HELPING LOW-INCOME FAMILIESINCREASE THEIR INCOME, BUILD SAVINGS AND GAIN AND SUSTAIN ASSETS.STRATEGIES THAT ASSIST FAMILIES IN ACHIEVING FINANCIAL STABILITY ANDINDEPENDENCE INCLUDE HOUSING AND FOOD ASSISTANCE, CASE MANAGEMENT,FINANCIAL EDUCATION, CREDIT REPAIR AND DEBT REDUCTION COUNSELING,EMPLOYMENT TRAINING AND SUPPORT, ACCESSING PUBLIC AND EMPLOYERBENEFITS, SAVINGS CAMPAIGNS AND EARNED INCOME TAX CREDIT.
2,819,715. 2,399,477.HEALTH: IMPROVING PEOPLE'S HEALTH AND ACCESS TO HEALTHCARE
COMMUNITY STRATEGIES:
WOMEN'S LEADERSHIP INITIATIVE: THE WOMEN'S LEADERSHIP INITIATIVEPARTNERS WITH THE COMMUNITY HEALTH FREE CLINIC, LINN COMMUNITY CARE ANDLINN COUNTY PUBLIC HEALTH TO PROVIDE NEEDED HEALTH CARE SERVICES TOLOW-INCOME, UNINSURED WOMEN. SERVICES INCLUDE PRESCRIPTION ASSISTANCE,EMERGENCY DENTAL CARE, EYE CARE/GLASSES, DIABETIC TESTING SUPPLIES ANDOTHER MEDICAL SUPPLIES, HEALTH SCREENINGS AND MEDICAL CO-PAYS.
IN ADDITION TO THIS INITIATIVE, UNITED WAY FUNDS PARTNER AGENCIES THAT
1,868,021. 1,589,620. 116,877.9,995,114.
SEE SCHEDULE O FOR CONTINUATION(S)

23200312-10-12
Yes No
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
1
2
3
4
5
6
7
8
9
10
Section 501(c)(3) organizations.
a
b
c
d
e
f
a
b
11a
11b
11c
11d
11e
11f
12a
12b
13
14a
14b
15
16
17
18
19
20a
20b
a
b
a
b
If "Yes," complete Schedule ASchedule B, Schedule of Contributors
If "Yes," complete Schedule C, Part I
If "Yes," complete Schedule C, Part II
If "Yes," complete Schedule C, Part III
If "Yes," complete Schedule D, Part I
If "Yes," complete Schedule D, Part IIIf "Yes," complete
Schedule D, Part III
If "Yes," complete Schedule D, Part IV
If "Yes," complete Schedule D, Part V
If "Yes," complete Schedule D,Part VI
If "Yes," complete Schedule D, Part VII
If "Yes," complete Schedule D, Part VIII
If "Yes," complete Schedule D, Part IXIf "Yes," complete Schedule D, Part X
If "Yes," complete Schedule D, Part XIf "Yes," complete
Schedule D, Parts XI and XII
If "Yes," and if the organization answered "No" to line 12a, then completing Schedule D, Parts XI and XII is optionalIf "Yes," complete Schedule E
If "Yes," complete Schedule F, Parts I and IV
If "Yes," complete Schedule F, Parts II and IV
If "Yes," complete Schedule F, Parts III and IV
If "Yes," complete Schedule G, Part I
If "Yes," complete Schedule G, Part IIIf "Yes,"
complete Schedule G, Part IIIIf "Yes," complete Schedule H
Form 990 (2012) Page
Is the organization described in section 501(c)(3) or 4947(a)(1) (other than a private foundation)?
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Is the organization required to complete ?
Did the organization engage in direct or indirect political campaign activities on behalf of or in opposition to candidates for
public office?
~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Did the organization engage in lobbying activities, or have a section 501(h) election in effect
during the tax year?
Is the organization a section 501(c)(4), 501(c)(5), or 501(c)(6) organization that receives membership dues, assessments, or
similar amounts as defined in Revenue Procedure 98-19?
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~
Did the organization maintain any donor advised funds or any similar funds or accounts for which donors have the right to
provide advice on the distribution or investment of amounts in such funds or accounts?
Did the organization receive or hold a conservation easement, including easements to preserve open space,
the environment, historic land areas, or historic structures?
Did the organization maintain collections of works of art, historical treasures, or other similar assets?
~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Did the organization report an amount in Part X, line 21, for escrow or custodial account liability; serve as a custodian for
amounts not listed in Part X; or provide credit counseling, debt management, credit repair, or debt negotiation services?
Did the organization, directly or through a related organization, hold assets in temporarily restricted endowments, permanent
endowments, or quasi-endowments?
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~
If the organization's answer to any of the following questions is "Yes," then complete Schedule D, Parts VI, VII, VIII, IX, or X
as applicable.
Did the organization report an amount for land, buildings, and equipment in Part X, line 10?
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Did the organization report an amount for investments - other securities in Part X, line 12 that is 5% or more of its total
assets reported in Part X, line 16?
Did the organization report an amount for investments - program related in Part X, line 13 that is 5% or more of its total
assets reported in Part X, line 16?
~~~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~
Did the organization report an amount for other assets in Part X, line 15 that is 5% or more of its total assets reported in
Part X, line 16?
Did the organization report an amount for other liabilities in Part X, line 25?
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~
Did the organization's separate or consolidated financial statements for the tax year include a footnote that addresses
the organization's liability for uncertain tax positions under FIN 48 (ASC 740)?
Did the organization obtain separate, independent audited financial statements for the tax year?
~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Was the organization included in consolidated, independent audited financial statements for the tax year?
~~~~~
Is the organization a school described in section 170(b)(1)(A)(ii)?
Did the organization maintain an office, employees, or agents outside of the United States?
~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~
Did the organization have aggregate revenues or expenses of more than $10,000 from grantmaking, fundraising, business,
investment, and program service activities outside the United States, or aggregate foreign investments valued at $100,000
or more? ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Did the organization report on Part IX, column (A), line 3, more than $5,000 of grants or assistance to any organization
or entity located outside the United States?
Did the organization report on Part IX, column (A), line 3, more than $5,000 of aggregate grants or assistance to individuals
located outside the United States?
~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~
Did the organization report a total of more than $15,000 of expenses for professional fundraising services on Part IX,
column (A), lines 6 and 11e? ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Did the organization report more than $15,000 total of fundraising event gross income and contributions on Part VIII, lines
1c and 8a? ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Did the organization report more than $15,000 of gross income from gaming activities on Part VIII, line 9a?
Did the organization operate one or more hospital facilities?
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~
If "Yes" to line 20a, did the organization attach a copy of its audited financial statements to this return? ����������
Form (2012)
3Part IV Checklist of Required Schedules
990
UNITED WAY OF EAST CENTRAL IOWA, INC. 42-0861239
XX
X
X
X
X
X
X
X
X
X
X
X
XX
X
X
XXX
X
X
X
X
X
XX

23200412-10-12
Yes No
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
21
22
23
24a
24b
24c
24d
25a
25b
26
27
28a
28b
28c
29
30
31
32
33
34
35a
35b
36
37
38
a
b
c
d
a
b
Section 501(c)(3) and 501(c)(4) organizations.
a
b
c
a
b
Section 501(c)(3) organizations.
Note.
(continued)
If "Yes," complete Schedule I, Parts I and II
If "Yes," complete Schedule I, Parts I and III
If "Yes," completeSchedule J
If "Yes," answer lines 24b through 24d and completeSchedule K. If "No", go to line 25
If "Yes," complete Schedule L, Part I
If "Yes," completeSchedule L, Part I
If "Yes," complete Schedule L, Part II
If "Yes," complete Schedule L, Part III
If "Yes," complete Schedule L, Part IVIf "Yes," complete Schedule L, Part IV
If "Yes," complete Schedule L, Part IVIf "Yes," complete Schedule M
If "Yes," complete Schedule M
If "Yes," complete Schedule N, Part IIf "Yes," complete
Schedule N, Part II
If "Yes," complete Schedule R, Part IIf "Yes," complete Schedule R, Part II, III, or IV, and
Part V, line 1
If "Yes," complete Schedule R, Part V, line 2
If "Yes," complete Schedule R, Part V, line 2
If "Yes," complete Schedule R, Part VI
Form 990 (2012) Page
Did the organization report more than $5,000 of grants and other assistance to any government or organization in the
United States on Part IX, column (A), line 1? ~~~~~~~~~~~~~~~~~~
Did the organization report more than $5,000 of grants and other assistance to individuals in the United States on Part IX,
column (A), line 2? ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Did the organization answer "Yes" to Part VII, Section A, line 3, 4, or 5 about compensation of the organization's current
and former officers, directors, trustees, key employees, and highest compensated employees?
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Did the organization have a tax-exempt bond issue with an outstanding principal amount of more than $100,000 as of the
last day of the year, that was issued after December 31, 2002?
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Did the organization invest any proceeds of tax-exempt bonds beyond a temporary period exception?
Did the organization maintain an escrow account other than a refunding escrow at any time during the year to defease
any tax-exempt bonds?
Did the organization act as an "on behalf of" issuer for bonds outstanding at any time during the year?
~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~
Did the organization engage in an excess benefit transaction with a
disqualified person during the year?
Is the organization aware that it engaged in an excess benefit transaction with a disqualified person in a prior year, and
that the transaction has not been reported on any of the organization's prior Forms 990 or 990-EZ?
~~~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Was a loan to or by a current or former officer, director, trustee, key employee, highest compensated employee, or disqualified
person outstanding as of the end of the organization's tax year?
Did the organization provide a grant or other assistance to an officer, director, trustee, key employee, substantial
contributor or employee thereof, a grant selection committee member, or to a 35% controlled entity or family member
of any of these persons?
~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Was the organization a party to a business transaction with one of the following parties (see Schedule L, Part IV
instructions for applicable filing thresholds, conditions, and exceptions):
A current or former officer, director, trustee, or key employee? ~~~~~~~~~~~
A family member of a current or former officer, director, trustee, or key employee?
An entity of which a current or former officer, director, trustee, or key employee (or a family member thereof) was an officer,
director, trustee, or direct or indirect owner?
~~
~~~~~~~~~~~~~~~~~~~~~
Did the organization receive more than $25,000 in non-cash contributions?
Did the organization receive contributions of art, historical treasures, or other similar assets, or qualified conservation
contributions?
~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Did the organization liquidate, terminate, or dissolve and cease operations?
Did the organization sell, exchange, dispose of, or transfer more than 25% of its net assets?
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Did the organization own 100% of an entity disregarded as separate from the organization under Regulations
sections 301.7701-2 and 301.7701-3?
Was the organization related to any tax-exempt or taxable entity?
~~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Did the organization have a controlled entity within the meaning of section 512(b)(13)?
If "Yes" to line 35a, did the organization receive any payment from or engage in any transaction with a controlled entity
within the meaning of section 512(b)(13)?
~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~
Did the organization make any transfers to an exempt non-charitable related organization?
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Did the organization conduct more than 5% of its activities through an entity that is not a related organization
and that is treated as a partnership for federal income tax purposes? ~~~~~~~~
Did the organization complete Schedule O and provide explanations in Schedule O for Part VI, lines 11b and 19?
All Form 990 filers are required to complete Schedule O �������������������������������
Form (2012)
4Part IV Checklist of Required Schedules
990
UNITED WAY OF EAST CENTRAL IOWA, INC. 42-0861239
X
X
X
X
X
X
X
X
XX
XX
X
X
X
X
XX
X
X
X
X

23200512-10-12
Sponsoring organizations maintaining donor advised funds and section 509(a)(3) supporting organizations.
Yes No
1
2
3
4
5
6
7
a
b
c
1a
1b
1c
a
b
2a
Note.
2b
3a
3b
4a
5a
5b
5c
6a
6b
7a
7b
7c
7e
7f
7g
7h
8
9a
9b
a
b
a
b
a
b
c
a
b
Organizations that may receive deductible contributions under section 170(c).
a
b
c
d
e
f
g
h
7d
8
9
10
11
12
13
14
Sponsoring organizations maintaining donor advised funds.
a
b
Section 501(c)(7) organizations.
a
b
10a
10b
Section 501(c)(12) organizations.
a
b
11a
11b
a
b
Section 4947(a)(1) non-exempt charitable trusts. 12a
12b
Section 501(c)(29) qualified nonprofit health insurance issuers.
Note.
a
b
c
a
b
13a
13b
13c
14a
14b
e-file
If "No," provide an explanation in Schedule O
If "No," provide an explanation in Schedule O
Did the organization receive a payment in excess of $75 made partly as a contribution and partly for goods and services provided to the payor?
Did the supporting
organization, or a donor advised fund maintained by a sponsoring organization, have excess business holdings at any time during the year?
Form (2012)
Form 990 (2012) Page
Check if Schedule O contains a response to any question in this Part V �����������������������������
Enter the number reported in Box 3 of Form 1096. Enter -0- if not applicable ~~~~~~~~~~~
Enter the number of Forms W-2G included in line 1a. Enter -0- if not applicable ~~~~~~~~~~
Did the organization comply with backup withholding rules for reportable payments to vendors and reportable gaming
(gambling) winnings to prize winners? �������������������������������������������
Enter the number of employees reported on Form W-3, Transmittal of Wage and Tax Statements,
filed for the calendar year ending with or within the year covered by this return ~~~~~~~~~~
If at least one is reported on line 2a, did the organization file all required federal employment tax returns?
If the sum of lines 1a and 2a is greater than 250, you may be required to (see instructions)
~~~~~~~~~~
Did the organization have unrelated business gross income of $1,000 or more during the year?
If "Yes," has it filed a Form 990-T for this year?
~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~
At any time during the calendar year, did the organization have an interest in, or a signature or other authority over, a
financial account in a foreign country (such as a bank account, securities account, or other financial account)?~~~~~~~
If "Yes," enter the name of the foreign country:
See instructions for filing requirements for Form TD F 90-22.1, Report of Foreign Bank and Financial Accounts.
Was the organization a party to a prohibited tax shelter transaction at any time during the tax year?
Did any taxable party notify the organization that it was or is a party to a prohibited tax shelter transaction?
~~~~~~~~~~~~
~~~~~~~~~
If "Yes," to line 5a or 5b, did the organization file Form 8886-T? ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Does the organization have annual gross receipts that are normally greater than $100,000, and did the organization solicit
any contributions that were not tax deductible as charitable contributions?
If "Yes," did the organization include with every solicitation an express statement that such contributions or gifts
were not tax deductible?
~~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
If "Yes," did the organization notify the donor of the value of the goods or services provided?
Did the organization sell, exchange, or otherwise dispose of tangible personal property for which it was required
to file Form 8282?
~~~~~~~~~~~~~~~
����������������������������������������������������
If "Yes," indicate the number of Forms 8282 filed during the year
Did the organization receive any funds, directly or indirectly, to pay premiums on a personal benefit contract?
~~~~~~~~~~~~~~~~
~~~~~~~
~~~~~~~~~Did the organization, during the year, pay premiums, directly or indirectly, on a personal benefit contract?
If the organization received a contribution of qualified intellectual property, did the organization file Form 8899 as required?
If the organization received a contribution of cars, boats, airplanes, or other vehicles, did the organization file a Form 1098-C?
~
Did the organization make any taxable distributions under section 4966?
Did the organization make a distribution to a donor, donor advisor, or related person?
~~~~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~
Enter:
Initiation fees and capital contributions included on Part VIII, line 12
Gross receipts, included on Form 990, Part VIII, line 12, for public use of club facilities
~~~~~~~~~~~~~~~
~~~~~~
Enter:
Gross income from members or shareholders
Gross income from other sources (Do not net amounts due or paid to other sources against
amounts due or received from them.)
~~~~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Is the organization filing Form 990 in lieu of Form 1041?
If "Yes," enter the amount of tax-exempt interest received or accrued during the year ������
Is the organization licensed to issue qualified health plans in more than one state?
See the instructions for additional information the organization must report on Schedule O.
~~~~~~~~~~~~~~~~~~~~~
Enter the amount of reserves the organization is required to maintain by the states in which the
organization is licensed to issue qualified health plans
Enter the amount of reserves on hand
~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Did the organization receive any payments for indoor tanning services during the tax year?
If "Yes," has it filed a Form 720 to report these payments?
~~~~~~~~~~~~~~~~
����������
5Part V Statements Regarding Other IRS Filings and Tax Compliance
990
J
UNITED WAY OF EAST CENTRAL IOWA, INC. 42-0861239
110
X
62X
X
X
XX
X
X
X
XX
X

23200612-10-12
Yes No
1a
1b
1
2
3
4
5
6
7
8
9
a
b
2
3
4
5
6
7a
7b
8a
8b
9
a
b
a
b
Yes No
10
11
a
b
10a
10b
11a
12a
12b
12c
13
14
15a
15b
16a
16b
a
b
12a
b
c
13
14
15
a
b
16a
b
17
18
19
20
For each "Yes" response to lines 2 through 7b below, and for a "No" responseto line 8a, 8b, or 10b below, describe the circumstances, processes, or changes in Schedule O. See instructions.
If "Yes," provide the names and addresses in Schedule O(This Section B requests information about policies not required by the Internal Revenue Code.)
If "No," go to line 13
If "Yes," describein Schedule O how this was done
(explain in Schedule O)
If there are material differences in voting rights among members of the governing body, or if the governing
body delegated broad authority to an executive committee or similar committee, explain in Schedule O.
Did the organization contemporaneously document the meetings held or written actions undertaken during the year by the following:
Were officers, directors, or trustees, and key employees required to disclose annually interests that could give rise to conflicts?
Form (2012)
Form 990 (2012) Page
Check if Schedule O contains a response to any question in this Part VI �����������������������������
Enter the number of voting members of the governing body at the end of the tax year
Enter the number of voting members included in line 1a, above, who are independent
~~~~~~
~~~~~~
Did any officer, director, trustee, or key employee have a family relationship or a business relationship with any other
officer, director, trustee, or key employee? ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Did the organization delegate control over management duties customarily performed by or under the direct supervision
of officers, directors, or trustees, or key employees to a management company or other person? ~~~~~~~~~~~~~~
Did the organization make any significant changes to its governing documents since the prior Form 990 was filed?
Did the organization become aware during the year of a significant diversion of the organization's assets?
Did the organization have members or stockholders?
~~~~~
~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Did the organization have members, stockholders, or other persons who had the power to elect or appoint one or
more members of the governing body?
Are any governance decisions of the organization reserved to (or subject to approval by) members, stockholders, or
persons other than the governing body?
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
The governing body?
Each committee with authority to act on behalf of the governing body?
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~~
Is there any officer, director, trustee, or key employee listed in Part VII, Section A, who cannot be reached at the
organization's mailing address? �����������������
Did the organization have local chapters, branches, or affiliates?
If "Yes," did the organization have written policies and procedures governing the activities of such chapters, affiliates,
and branches to ensure their operations are consistent with the organization's exempt purposes?
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~
Has the organization provided a complete copy of this Form 990 to all members of its governing body before filing the form?
Describe in Schedule O the process, if any, used by the organization to review this Form 990.
Did the organization have a written conflict of interest policy? ~~~~~~~~~~~~~~~~~~~~
~~~~~~
Did the organization regularly and consistently monitor and enforce compliance with the policy?
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Did the organization have a written whistleblower policy?
Did the organization have a written document retention and destruction policy?
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~
Did the process for determining compensation of the following persons include a review and approval by independent
persons, comparability data, and contemporaneous substantiation of the deliberation and decision?
The organization's CEO, Executive Director, or top management official
Other officers or key employees of the organization
If "Yes" to line 15a or 15b, describe the process in Schedule O (see instructions).
~~~~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Did the organization invest in, contribute assets to, or participate in a joint venture or similar arrangement with a
taxable entity during the year? ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
If "Yes," did the organization follow a written policy or procedure requiring the organization to evaluate its participation
in joint venture arrangements under applicable federal tax law, and take steps to safeguard the organization's
exempt status with respect to such arrangements? ������������������������������������
List the states with which a copy of this Form 990 is required to be filed
Section 6104 requires an organization to make its Forms 1023 (or 1024 if applicable), 990, and 990-T (Section 501(c)(3)s only) available
for public inspection. Indicate how you made these available. Check all that apply.
Own website Another's website Upon request Other
Describe in Schedule O whether (and if so, how), the organization made its governing documents, conflict of interest policy, and financial
statements available to the public during the tax year.
State the name, physical address, and telephone number of the person who possesses the books and records of the organization: |
6Part VI Governance, Management, and Disclosure
Section A. Governing Body and Management
Section B. Policies
Section C. Disclosure
990
J
UNITED WAY OF EAST CENTRAL IOWA, INC. 42-0861239
X
31
30
X
XXXX
X
X
XX
X
X
X
XX
XXX
XX
X
NONE
X X
LIYA FITZPATRICK - 319-398-5372317 7TH AVENUE SE #401, CEDAR RAPIDS, IA 52401

Indi
vidu
al tr
uste
e or
dire
ctor
Inst
itutio
nal t
rust
ee
Offi
cer
Key
empl
oyee
Hig
hest
com
pens
ated
empl
oyee
Form
er
(do not check more than onebox, unless person is both anofficer and a director/trustee)
232007 12-10-12
current
Section A. Officers, Directors, Trustees, Key Employees, and Highest Compensated Employees
1a
current
current
former
former directors or trustees
(A) (B) (C) (D) (E) (F)
Complete this table for all persons required to be listed. Report compensation for the calendar year ending with or within the organization's tax year.
List the organization's five highest compensated employees (other than an officer, director, trustee, or key employee) who received reportablecompensation (Box 5 of Form W-2 and/or Box 7 of Form 1099-MISC) of more than $100,000 from the organization and any related organizations
Form 990 (2012) Page
Check if Schedule O contains a response to any question in this Part VII�����������������������������
¥ List all of the organization's officers, directors, trustees (whether individuals or organizations), regardless of amount of compensation.Enter -0- in columns (D), (E), and (F) if no compensation was paid.
¥ List all of the organization's key employees, if any. See instructions for definition of "key employee."¥
.
¥ List all of the organization's officers, key employees, and highest compensated employees who received more than $100,000 ofreportable compensation from the organization and any related organizations.
¥ List all of the organization's that received, in the capacity as a former director or trustee of the organization,more than $10,000 of reportable compensation from the organization and any related organizations.
List persons in the following order: individual trustees or directors; institutional trustees; officers; key employees; highest compensated employees; and former such persons.
Check this box if neither the organization nor any related organization compensated any current officer, director, or trustee.
PositionName and Title Average hours per
week (list any
hours forrelated
organizationsbelowline)
Reportablecompensation
from the
organization(W-2/1099-MISC)
Reportablecompensationfrom related
organizations(W-2/1099-MISC)
Estimatedamount of
othercompensation
from theorganizationand related
organizations
Form (2012)
7Part VII Compensation of Officers, Directors, Trustees, Key Employees, Highest Compensated
Employees, and Independent Contractors
990
UNITED WAY OF EAST CENTRAL IOWA, INC. 42-0861239
(1) LOIS BUNTZ 50.00PRESIDENT/CEO X X 129,538. 0. 21,729.(2) GREG NEUMEYER 1.00BOARD CHAIR X X 0. 0. 0.(3) BRAD HART 1.00BOARD VICE CHAIR X X 0. 0. 0.(4) KATIE MULHOLLAND 1.00SECRETARY X X 0. 0. 0.(5) KYLE DECKER 1.00TREASURER X X 0. 0. 0.(6) JON BANCKS 1.00DIRECTOR X 0. 0. 0.(7) DAVE BENSON 1.00DIRECTOR X 0. 0. 0.(8) GREG BRECHT 1.00DIRECTOR X 0. 0. 0.(9) KARL CASSELL 1.00DIRECTOR X 0. 0. 0.(10) GARY CHADICK 1.00DIRECTOR X 0. 0. 0.(11) JACK EVANS 1.00DIRECTOR X 0. 0. 0.(12) MATT EVANS 1.00DIRECTOR X 0. 0. 0.(13) BARBARA GAY 1.00DIRECTOR X 0. 0. 0.(14) CATHY GULLICKSON 1.00DIRECTOR X 0. 0. 0.(15) JIM HADDAD 1.00DIRECTOR X 0. 0. 0.(16) STUART HAKER 1.00DIRECTOR X 0. 0. 0.(17) TIM KINTNER 1.00DIRECTOR X 0. 0. 0.

Form
er
Indi
vidu
al tr
uste
e or
dire
ctor
Inst
itutio
nal t
rust
ee
Offi
cer
Hig
hest
com
pens
ated
empl
oyee
Key
empl
oyee
(do not check more than onebox, unless person is both anofficer and a director/trustee)
23200812-10-12
Section A. Officers, Directors, Trustees, Key Employees, and Highest Compensated Employees
(B) (C)(A) (D) (E) (F)
1b
c
d
Sub-total
Total from continuation sheets to Part VII, Section A
Total (add lines 1b and 1c)
2
Yes No
3
4
5
former
3
4
5
Section B. Independent Contractors
1
(A) (B) (C)
2
(continued)
If "Yes," complete Schedule J for such individual
If "Yes," complete Schedule J for such individual
If "Yes," complete Schedule J for such person
Page Form 990 (2012)
PositionAverage hours per
week(list any
hours forrelated
organizationsbelowline)
Name and title Reportablecompensation
from the
organization(W-2/1099-MISC)
Reportablecompensationfrom related
organizations(W-2/1099-MISC)
Estimatedamount of
othercompensation
from theorganizationand related
organizations
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~ |
~~~~~~~~ |
���������������������� |
Total number of individuals (including but not limited to those listed above) who received more than $100,000 of reportable
compensation from the organization |
Did the organization list any officer, director, or trustee, key employee, or highest compensated employee on
line 1a? ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
For any individual listed on line 1a, is the sum of reportable compensation and other compensation from the organization
and related organizations greater than $150,000? ~~~~~~~~~~~~~
Did any person listed on line 1a receive or accrue compensation from any unrelated organization or individual for services
rendered to the organization? ������������������������
Complete this table for your five highest compensated independent contractors that received more than $100,000 of compensation from
the organization. Report compensation for the calendar year ending with or within the organization's tax year.
Name and business address Description of services Compensation
Total number of independent contractors (including but not limited to those listed above) who received more than
$100,000 of compensation from the organization |
Form (2012)
8Part VII
990
UNITED WAY OF EAST CENTRAL IOWA, INC. 42-0861239
(18) KEVIN KNUTSON 1.00DIRECTOR X 0. 0. 0.(19) DOUG KOPP 1.00DIRECTOR X 0. 0. 0.(20) DICK LORENZ 1.00DIRECTOR X 0. 0. 0.(21) BETH MALICKI 1.00DIRECTOR X 0. 0. 0.(22) RICK MOYLE 1.00DIRECTOR X 0. 0. 0.(23) RON OLSON 1.00DIRECTOR X 0. 0. 0.(24) MATT O'ROURKE 1.00DIRECTOR X 0. 0. 0.(25) MAUREEN OSAKO 1.00DIRECTOR X 0. 0. 0.(26) MARY ANN OSBORN 1.00DIRECTOR X 0. 0. 0.
129,538. 0. 21,729.68,875. 0. 5,980.
198,413. 0. 27,709.
1
X
X
X
NONE
0SEE PART VII, SECTION A CONTINUATION SHEETS

Indi
vidu
al tr
uste
e or
dire
ctor
Inst
itutio
nal t
rust
ee
Offi
cer
Key
empl
oyee
Hig
hest
com
pens
ated
em
ploy
ee
Form
er
23220107-25-12
Section A. Officers, Directors, Trustees, Key Employees, and Highest Compensated Employees
(A) (B) (C) (D) (E) (F)
(continued)Form 990
Name and title Average hours per
week(list any
hours forrelated
organizationsbelowline)
Position (check all that apply)
Reportablecompensation
from the
organization(W-2/1099-MISC)
Reportablecompensationfrom related
organizations(W-2/1099-MISC)
Estimatedamount of
othercompensation
from theorganizationand related
organizations
Total to Part VII, Section A, line 1c �������������������������
Part VII
UNITED WAY OF EAST CENTRAL IOWA, INC. 42-0861239
(27) STEVE OVEL 1.00DIRECTOR X 0. 0. 0.(28) DICK PILCHER 1.00DIRECTOR X 0. 0. 0.(29) DAVE POHLMAN 1.00DIRECTOR X 0. 0. 0.(30) CATHY TERUKINA 1.00DIRECTOR X 0. 0. 0.(31) MIKE TRACHTA 1.00DIRECTOR X 0. 0. 0.(32) MIKE WILKINS 1.00DIRECTOR X 0. 0. 0.(33) KRISTINE RILEY 50.00VP/CFO X 68,875. 0. 5,980.(34) TIM STILES 50.00VP/COO X 0. 0. 0.
68,875. 5,980.

Noncash contributions included in lines 1a-1f: $
23200912-10-12
Total revenue.
(A) (B) (C) (D)
1 a
b
c
d
e
f
g
h
1
1
1
1
1
1
a
b
c
d
e
f
Co
ntr
ibu
tio
ns, G
ifts
, G
ran
tsa
nd
Oth
er
Sim
ila
r A
mo
un
ts
Total.
a
b
c
d
e
f
g
2
Pro
gra
m S
erv
ice
Re
ven
ue
Total.
3
4
5
6 a
b
c
d
a
b
c
d
7
a
b
c
8
a
b
9 a
b
c
a
b
10 a
b
c
a
b
11 a
b
c
d
e Total.
Oth
er
Re
ven
ue
12
Revenue excludedfrom tax undersections 512,513, or 514
All other contributions, gifts, grants, and
similar amounts not included above
See instructions.
Form (2012)
Page Form 990 (2012)
Check if Schedule O contains a response to any question in this Part VIII ���������������������������
Total revenue Related orexempt function
revenue
Unrelatedbusinessrevenue
Federated campaigns
Membership dues
~~~~~~
~~~~~~~~
Fundraising events
Related organizations
~~~~~~~~
~~~~~~
Government grants (contributions)
~~
Add lines 1a-1f ����������������� |
Business Code
All other program service revenue ~~~~~
Add lines 2a-2f ����������������� |
Investment income (including dividends, interest, and
other similar amounts)
Income from investment of tax-exempt bond proceeds
~~~~~~~~~~~~~~~~~ |
|
Royalties ����������������������� |
(i) Real (ii) Personal
Gross rents
Less: rental expenses
Rental income or (loss)
Net rental income or (loss)
~~~~~~~
~~~
~~
�������������� |
Gross amount from sales of
assets other than inventory
(i) Securities (ii) Other
Less: cost or other basis
and sales expenses
Gain or (loss)
~~~
~~~~~~~
Net gain or (loss) ������������������� |
Gross income from fundraising events (not
including $ of
contributions reported on line 1c). See
Part IV, line 18 ~~~~~~~~~~~~~
Less: direct expenses~~~~~~~~~~
Net income or (loss) from fundraising events ����� |
Gross income from gaming activities. See
Part IV, line 19 ~~~~~~~~~~~~~
Less: direct expenses
Net income or (loss) from gaming activities
~~~~~~~~~
������ |
Gross sales of inventory, less returns
and allowances ~~~~~~~~~~~~~
Less: cost of goods sold
Net income or (loss) from sales of inventory
~~~~~~~~
������ |
Miscellaneous Revenue Business Code
All other revenue ~~~~~~~~~~~~~
Add lines 11a-11d ~~~~~~~~~~~~~~~ |
|�������������
9Part VIII Statement of Revenue
990
UNITED WAY OF EAST CENTRAL IOWA, INC. 42-0861239
62,249.
10,662,558.84,629.
10,724,807.
DONOR DESIGNATION FEES 900099 101,167. 101,167.SPECIAL EVENT REVENUE 900099 15,710. 15,710.
116,877.
81,324. 81,324.
472,982.
447,492.25,490.
25,490. 25,490.
SPONSORSHIPS 900099 166,300. 166,300.
900099 28,838. 28,838.195,138.
11,143,636. 116,877. 0. 301,952.

Check here if following SOP 98-2 (ASC 958-720)
232010 12-10-12
Total functional expenses.
Joint costs.
(A) (B) (C) (D)
1
2
3
4
5
6
7
8
9
10
11
a
b
c
d
e
f
g
12
13
14
15
16
17
18
19
20
21
22
23
24
a
b
c
d
e
25
26
Section 501(c)(3) and 501(c)(4) organizations must complete all columns. All other organizations must complete column (A).
Grants and other assistance to governments and
organizations in the United States. See Part IV, line 21
Compensation not included above, to disqualified
persons (as defined under section 4958(f)(1)) and
persons described in section 4958(c)(3)(B)
Pension plan accruals and contributions (include
section 401(k) and 403(b) employer contributions)
Professional fundraising services. See Part IV, line 17
(If line 11g amount exceeds 10% of line 25,
column (A) amount, list line 11g expenses on Sch O.)
Other expenses. Itemize expenses not covered above. (List miscellaneous expenses in line 24e. If line24e amount exceeds 10% of line 25, column (A)amount, list line 24e expenses on Schedule O.)
Add lines 1 through 24e
Complete this line only if the organization
reported in column (B) joint costs from a combined
educational campaign and fundraising solicitation.
Form 990 (2012) Page
Check if Schedule O contains a response to any question in this Part IX ��������������������������
Total expenses Program serviceexpenses
Management andgeneral expenses
Fundraisingexpenses
Grants and other assistance to individuals in
the United States. See Part IV, line 22 ~~~
Grants and other assistance to governments,
organizations, and individuals outside the
United States. See Part IV, lines 15 and 16 ~
Benefits paid to or for members ~~~~~~~
Compensation of current officers, directors,
trustees, and key employees ~~~~~~~~
~~~
Other salaries and wages ~~~~~~~~~~
Other employee benefits ~~~~~~~~~~
Payroll taxes ~~~~~~~~~~~~~~~~
Fees for services (non-employees):
Management
Legal
Accounting
Lobbying
~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~
Investment management fees
Other.
~~~~~~~~
Advertising and promotion
Office expenses
Information technology
Royalties
~~~~~~~~~
~~~~~~~~~~~~~~~
~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~
Occupancy ~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~Travel
Payments of travel or entertainment expenses
for any federal, state, or local public officials
Conferences, conventions, and meetings ~~
Interest
Payments to affiliates
~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~
Depreciation, depletion, and amortization
Insurance
~~
~~~~~~~~~~~~~~~~~
~~
All other expenses
|
Form (2012)
Do not include amounts reported on lines 6b,7b, 8b, 9b, and 10b of Part VIII.
10Part IX Statement of Functional Expenses
990
UNITED WAY OF EAST CENTRAL IOWA, INC. 42-0861239
8,505,487. 8,505,487.
214,570. 63,925. 45,004. 105,641.
1,408,228. 802,102. 344,890. 261,236.
82,520. 47,103. 20,436. 14,981.162,070. 85,140. 50,725. 26,205.115,388. 58,958. 29,935. 26,495.
4,586. 4,586.29,745. 29,745.1,800. 1,800.
2,105. 2,105.
46,071. 26,968. 17,712. 1,391.102,150. 28,248. 42,828. 31,074.25,733. 9,530. 7,597. 8,606.46,076. 27,127. 10,874. 8,075.
141,297. 58,490. 34,702. 48,105.36,021. 34,121. 1,551. 349.
59,099. 32,003. 12,157. 14,939.
104,801. 37,169. 32,105. 35,527.41,172. 16,550. 9,358. 15,264.
SPECIAL PROJECTS 175,271. 140,314. 4,792. 30,165.DONATED MATERIALS 84,629. 9,020. 66,267. 9,342.AWARDS 5,994. 2,513. 1,310. 2,171.ORGANIZATIONAL DUES 2,697. 1,225. 990. 482.
14,102. 7,321. 2,894. 3,887.11,411,612. 9,995,114. 772,563. 643,935.

23201112-10-12
(A) (B)
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
1
2
3
4
5
6
7
8
9
10c
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
a
b
10a
10b
Asse
ts
Total assets.
Lia
bilit
ies
Total liabilities.
Organizations that follow SFAS 117 (ASC 958), check here and
complete lines 27 through 29, and lines 33 and 34.
27
28
29
Organizations that do not follow SFAS 117 (ASC 958), check here
and complete lines 30 through 34.
30
31
32
33
34
Ne
t A
sse
ts o
r F
un
d B
ala
nc
es
Form 990 (2012) Page
Check if Schedule O contains a response to any question in this Part X ������������������������������
Beginning of year End of year
Cash - non-interest-bearing
Savings and temporary cash investments
Pledges and grants receivable, net
~~~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~
Accounts receivable, net ~~~~~~~~~~~~~~~~~~~~~~~~~~
Loans and other receivables from current and former officers, directors,
trustees, key employees, and highest compensated employees. Complete
Part II of Schedule L ~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Loans and other receivables from other disqualified persons (as defined under
section 4958(f)(1)), persons described in section 4958(c)(3)(B), and contributing
employers and sponsoring organizations of section 501(c)(9) voluntary
employees' beneficiary organizations (see instr). Complete Part II of Sch L ~~
Notes and loans receivable, net
Inventories for sale or use
Prepaid expenses and deferred charges
~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~
Land, buildings, and equipment: cost or other
basis. Complete Part VI of Schedule D
Less: accumulated depreciation
~~~
~~~~~~
Investments - publicly traded securities
Investments - other securities. See Part IV, line 11
Investments - program-related. See Part IV, line 11
Intangible assets
~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~
~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Other assets. See Part IV, line 11 ~~~~~~~~~~~~~~~~~~~~~~
Add lines 1 through 15 (must equal line 34) ����������
Accounts payable and accrued expenses
Grants payable
Deferred revenue
~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Tax-exempt bond liabilities
Escrow or custodial account liability. Complete Part IV of Schedule D
~~~~~~~~~~~~~~~~~~~~~~~~~
~~~~
Loans and other payables to current and former officers, directors, trustees,
key employees, highest compensated employees, and disqualified persons.
Complete Part II of Schedule L ~~~~~~~~~~~~~~~~~~~~~~~
Secured mortgages and notes payable to unrelated third parties ~~~~~~
Unsecured notes and loans payable to unrelated third parties ~~~~~~~~
Other liabilities (including federal income tax, payables to related third
parties, and other liabilities not included on lines 17-24). Complete Part X of
Schedule D ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Add lines 17 through 25 ������������������
|
Unrestricted net assets
Temporarily restricted net assets
Permanently restricted net assets
~~~~~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~
|
Capital stock or trust principal, or current funds
Paid-in or capital surplus, or land, building, or equipment fund
Retained earnings, endowment, accumulated income, or other funds
~~~~~~~~~~~~~~~
~~~~~~~~
~~~~
Total net assets or fund balances ~~~~~~~~~~~~~~~~~~~~~~
Total liabilities and net assets/fund balances ����������������
Form (2012)
11Balance SheetPart X
990
UNITED WAY OF EAST CENTRAL IOWA, INC. 42-0861239
200. 200.5,117,617. 4,569,113.4,146,374. 4,288,803.578,162. 596,739.
35,873. 33,672.
401,959.199,588. 236,500. 202,371.
1,229,564. 1,274,421.301,939. 335,435.
14,259,764. 14,039,476.
455,074. 451,397.26,361,067. 25,791,627.
197,535. 237,004.7,290,357. 7,106,335.
394,016. 391,409.7,881,908. 7,734,748.
X
7,239,323. 7,223,938.10,896,185. 10,489,290.
343,651. 343,651.
18,479,159. 18,056,879.26,361,067. 25,791,627.

23201212-10-12
1
2
3
4
5
6
7
8
9
10
1
2
3
4
5
6
7
8
9
10
Yes No
1
2
3
a
b
c
2a
2b
2c
a
b
3a
3b
Form 990 (2012) Page
Check if Schedule O contains a response to any question in this Part XI �����������������������������
Total revenue (must equal Part VIII, column (A), line 12)
Total expenses (must equal Part IX, column (A), line 25)
Revenue less expenses. Subtract line 2 from line 1
Net assets or fund balances at beginning of year (must equal Part X, line 33, column (A))
~~~~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~
Net unrealized gains (losses) on investments
Donated services and use of facilities
Investment expenses
Prior period adjustments
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Other changes in net assets or fund balances (explain in Schedule O)
Net assets or fund balances at end of year. Combine lines 3 through 9 (must equal Part X, line 33,
column (B))
~~~~~~~~~~~~~~~~~~~
�����������������������������������������������
Check if Schedule O contains a response to any question in this Part XII�����������������������������
Accounting method used to prepare the Form 990: Cash Accrual Other
If the organization changed its method of accounting from a prior year or checked "Other," explain in Schedule O.
Were the organization's financial statements compiled or reviewed by an independent accountant? ~~~~~~~~~~~~
If "Yes," check a box below to indicate whether the financial statements for the year were compiled or reviewed on a
separate basis, consolidated basis, or both:
Separate basis Consolidated basis Both consolidated and separate basis
Were the organization's financial statements audited by an independent accountant? ~~~~~~~~~~~~~~~~~~~
If "Yes," check a box below to indicate whether the financial statements for the year were audited on a separate basis,
consolidated basis, or both:
Separate basis Consolidated basis Both consolidated and separate basis
If "Yes" to line 2a or 2b, does the organization have a committee that assumes responsibility for oversight of the audit,
review, or compilation of its financial statements and selection of an independent accountant?~~~~~~~~~~~~~~~
If the organization changed either its oversight process or selection process during the tax year, explain in Schedule O.
As a result of a federal award, was the organization required to undergo an audit or audits as set forth in the Single Audit
Act and OMB Circular A-133? ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
If "Yes," did the organization undergo the required audit or audits? If the organization did not undergo the required audit
or audits, explain why in Schedule O and describe any steps taken to undergo such audits ����������������
Form (2012)
12Part XI Reconciliation of Net Assets
Part XII Financial Statements and Reporting
990
UNITED WAY OF EAST CENTRAL IOWA, INC. 42-0861239
X
11,143,636.11,411,612.-267,976.
18,479,159.39,872.
-194,176.
18,056,879.
X
X
X
X
X
X

OMB No. 1545-0047
Department of the TreasuryInternal Revenue Service
23202112-04-12
(iii)
(see instructions)
(iv) (i)
(v)
(i)
(vi)
(i)
(i) (ii) (vii)
(Form 990 or 990-EZ)
Complete if the organization is a section 501(c)(3) organization or a section
4947(a)(1) nonexempt charitable trust.
| Attach to Form 990 or Form 990-EZ. | See separate instructions.
Open to PublicInspection
Name of the organization Employer identification number
1
2
3
4
5
6
7
8
9
10
11
section 170(b)(1)(A)(i).
section 170(b)(1)(A)(ii).
section 170(b)(1)(A)(iii).
section 170(b)(1)(A)(iii).
section 170(b)(1)(A)(iv).
section 170(b)(1)(A)(v).
section 170(b)(1)(A)(vi).
section 170(b)(1)(A)(vi).
section 509(a)(2).
section 509(a)(4).
section 509(a)(3).
a b c d
e
f
g
h
(i)
(ii)
(iii)
Yes No
11g(i)
11g(ii)
11g(iii)
Yes No Yes No Yes No
Total
For Paperwork Reduction Act Notice, see the Instructions for
Form 990 or 990-EZ.
Schedule A (Form 990 or 990-EZ) 2012
Type of organization (described on lines 1-9 above or IRC section
)
Is the organizationin col. listed in yourgoverning document?
Did you notify theorganization in col.
of your support?
Is theorganization in col.
organized in theU.S.?
Name of supportedorganization
EIN Amount of monetarysupport
(All organizations must complete this part.) See instructions.
The organization is not a private foundation because it is: (For lines 1 through 11, check only one box.)
A church, convention of churches, or association of churches described in
A school described in (Attach Schedule E.)
A hospital or a cooperative hospital service organization described in
A medical research organization operated in conjunction with a hospital described in Enter the hospital's name,
city, and state:
An organization operated for the benefit of a college or university owned or operated by a governmental unit described in
(Complete Part II.)
A federal, state, or local government or governmental unit described in
An organization that normally receives a substantial part of its support from a governmental unit or from the general public described in
(Complete Part II.)
A community trust described in (Complete Part II.)
An organization that normally receives: (1) more than 33 1/3% of its support from contributions, membership fees, and gross receipts from
activities related to its exempt functions - subject to certain exceptions, and (2) no more than 33 1/3% of its support from gross investment
income and unrelated business taxable income (less section 511 tax) from businesses acquired by the organization after June 30, 1975.
See (Complete Part III.)
An organization organized and operated exclusively to test for public safety. See
An organization organized and operated exclusively for the benefit of, to perform the functions of, or to carry out the purposes of one or
more publicly supported organizations described in section 509(a)(1) or section 509(a)(2). See Check the box that
describes the type of supporting organization and complete lines 11e through 11h.
Type I Type II Type III - Functionally integrated Type III - Non-functionally integrated
By checking this box, I certify that the organization is not controlled directly or indirectly by one or more disqualified persons other than
foundation managers and other than one or more publicly supported organizations described in section 509(a)(1) or section 509(a)(2).
If the organization received a written determination from the IRS that it is a Type I, Type II, or Type III
supporting organization, check this box
Since August 17, 2006, has the organization accepted any gift or contribution from any of the following persons?
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
A person who directly or indirectly controls, either alone or together with persons described in (ii) and (iii) below,
the governing body of the supported organization?
A family member of a person described in (i) above?
A 35% controlled entity of a person described in (i) or (ii) above?
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~
Provide the following information about the supported organization(s).
LHA
SCHEDULE A
Part I Reason for Public Charity Status
Public Charity Status and Public Support 2012
UNITED WAY OF EAST CENTRAL IOWA, INC. 42-0861239
X

Subtract line 5 from line 4.
23202212-04-12
Calendar year (or fiscal year beginning in)
Calendar year (or fiscal year beginning in) |
2
(a) (b) (c) (d) (e) (f)
1
2
3
4
5
Total.
6 Public support.
(a) (b) (c) (d) (e) (f)
7
8
9
10
11
12
13
Total support.
12
First five years.
stop here
14
15
14
15
16
17
18
a
b
a
b
33 1/3% support test - 2012.
stop here.
33 1/3% support test - 2011.
stop here.
10% -facts-and-circumstances test - 2012.
stop here.
10% -facts-and-circumstances test - 2011.
stop here.
Private foundation.
Schedule A (Form 990 or 990-EZ) 2012
|
Add lines 7 through 10
Schedule A (Form 990 or 990-EZ) 2012 Page
(Complete only if you checked the box on line 5, 7, or 8 of Part I or if the organization failed to qualify under Part III. If the organization
fails to qualify under the tests listed below, please complete Part III.)
2008 2009 2010 2011 2012 Total
Gifts, grants, contributions, and
membership fees received. (Do not
include any "unusual grants.") ~~
Tax revenues levied for the organ-
ization's benefit and either paid to
or expended on its behalf ~~~~
The value of services or facilities
furnished by a governmental unit to
the organization without charge ~
Add lines 1 through 3 ~~~
The portion of total contributions
by each person (other than a
governmental unit or publicly
supported organization) included
on line 1 that exceeds 2% of the
amount shown on line 11,
column (f) ~~~~~~~~~~~~
2008 2009 2010 2011 2012 Total
Amounts from line 4 ~~~~~~~
Gross income from interest,
dividends, payments received on
securities loans, rents, royalties
and income from similar sources ~
Net income from unrelated business
activities, whether or not the
business is regularly carried on ~
Other income. Do not include gain
or loss from the sale of capital
assets (Explain in Part IV.) ~~~~
Gross receipts from related activities, etc. (see instructions) ~~~~~~~~~~~~~~~~~~~~~~~
If the Form 990 is for the organization's first, second, third, fourth, or fifth tax year as a section 501(c)(3)
organization, check this box and ��������������������������������������������� |
~~~~~~~~~~~~Public support percentage for 2012 (line 6, column (f) divided by line 11, column (f))
Public support percentage from 2011 Schedule A, Part II, line 14
%
%~~~~~~~~~~~~~~~~~~~~~
If the organization did not check the box on line 13, and line 14 is 33 1/3% or more, check this box and
The organization qualifies as a publicly supported organization ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~ |
If the organization did not check a box on line 13 or 16a, and line 15 is 33 1/3% or more, check this box
and The organization qualifies as a publicly supported organization ~~~~~~~~~~~~~~~~~~~~~~~~~~~~ |
If the organization did not check a box on line 13, 16a, or 16b, and line 14 is 10% or more,
and if the organization meets the "facts-and-circumstances" test, check this box and Explain in Part IV how the organization
meets the "facts-and-circumstances" test. The organization qualifies as a publicly supported organization ~~~~~~~~~~~~~~~ |
If the organization did not check a box on line 13, 16a, 16b, or 17a, and line 15 is 10% or
more, and if the organization meets the "facts-and-circumstances" test, check this box and Explain in Part IV how the
organization meets the "facts-and-circumstances" test. The organization qualifies as a publicly supported organization ~~~~~~~~ |
If the organization did not check a box on line 13, 16a, 16b, 17a, or 17b, check this box and see instructions ��� |
Part II Support Schedule for Organizations Described in Sections 170(b)(1)(A)(iv) and 170(b)(1)(A)(vi)
Section A. Public Support
Section B. Total Support
Section C. Computation of Public Support Percentage
UNITED WAY OF EAST CENTRAL IOWA, INC. 42-0861239
11,787,491. 10,075,307. 11,200,033. 11,175,928. 10,724,807. 54,963,566.
11,787,491. 10,075,307. 11,200,033. 11,175,928. 10,724,807. 54,963,566.
10,758,971.44,204,595.
11,787,491. 10,075,307. 11,200,033. 11,175,928. 10,724,807. 54,963,566.
130,227. 88,319. 95,532. 108,139. 81,324. 503,541.
119,884. 102,565. 126,863. 123,378. 195,138. 667,828.56,134,935.454,640.
78.7582.25
X

(Subtract line 7c from line 6.)
Amounts included on lines 2 and 3 received
from other than disqualified persons that
exceed the greater of $5,000 or 1% of the
amount on line 13 for the year
(Add lines 9, 10c, 11, and 12.)
232023 12-04-12
Calendar year (or fiscal year beginning in) |
Calendar year (or fiscal year beginning in) |
Total support.
3
(a) (b) (c) (d) (e) (f)
1
2
3
4
5
6
7
Total.
a
b
c
8 Public support
(a) (b) (c) (d) (e) (f)
9
10a
b
c11
12
13
14 First five years.
stop here
15
16
15
16
17
18
19
20
2012
2011
17
18
a
b
33 1/3% support tests - 2012.
stop here.
33 1/3% support tests - 2011.
stop here.
Private foundation.
Schedule A (Form 990 or 990-EZ) 2012
Unrelated business taxable income
(less section 511 taxes) from businesses
acquired after June 30, 1975
Schedule A (Form 990 or 990-EZ) 2012 Page
(Complete only if you checked the box on line 9 of Part I or if the organization failed to qualify under Part II. If the organization fails to
qualify under the tests listed below, please complete Part II.)
2008 2009 2010 2011 2012 Total
Gifts, grants, contributions, and
membership fees received. (Do not
include any "unusual grants.") ~~
Gross receipts from admissions,merchandise sold or services per-formed, or facilities furnished inany activity that is related to theorganization's tax-exempt purpose
Gross receipts from activities that
are not an unrelated trade or bus-
iness under section 513 ~~~~~
Tax revenues levied for the organ-
ization's benefit and either paid to
or expended on its behalf ~~~~
The value of services or facilities
furnished by a governmental unit to
the organization without charge ~
~~~ Add lines 1 through 5
Amounts included on lines 1, 2, and
3 received from disqualified persons
~~~~~~
Add lines 7a and 7b ~~~~~~~
2008 2009 2010 2011 2012 Total
Amounts from line 6 ~~~~~~~Gross income from interest, dividends, payments received on securities loans, rents, royalties and income from similar sources ~
~~~~
Add lines 10a and 10b ~~~~~~Net income from unrelated businessactivities not included in line 10b, whether or not the business is regularly carried on ~~~~~~~Other income. Do not include gainor loss from the sale of capitalassets (Explain in Part IV.) ~~~~
If the Form 990 is for the organization's first, second, third, fourth, or fifth tax year as a section 501(c)(3) organization,
check this box and ���������������������������������������������������� |
Public support percentage for 2012 (line 8, column (f) divided by line 13, column (f))
Public support percentage from 2011 Schedule A, Part III, line 15
~~~~~~~~~~~~ %
%��������������������
Investment income percentage for (line 10c, column (f) divided by line 13, column (f))
Investment income percentage from Schedule A, Part III, line 17
~~~~~~~~ %
%~~~~~~~~~~~~~~~~~~
If the organization did not check the box on line 14, and line 15 is more than 33 1/3% , and line 17 is not
more than 33 1/3% , check this box and The organization qualifies as a publicly supported organization ~~~~~~~~~~ |
If the organization did not check a box on line 14 or line 19a, and line 16 is more than 33 1/3% , and
line 18 is not more than 33 1/3% , check this box and The organization qualifies as a publicly supported organization~~~~ |
If the organization did not check a box on line 14, 19a, or 19b, check this box and see instructions �������� |
Part III Support Schedule for Organizations Described in Section 509(a)(2)
Section A. Public Support
Section B. Total Support
Section C. Computation of Public Support Percentage
Section D. Computation of Investment Income Percentage

OMB No. 1545-0047
Department of the TreasuryInternal Revenue Service
22345112-21-12
Schedule B (Form 990, 990-EZ, or 990-PF) (2012)
(Form 990, 990-EZ,or 990-PF) | Attach to Form 990, Form 990-EZ, or Form 990-PF.
Name of the organization Employer identification number
Organization type
Filers of: Section:
not
General Rule Special Rule.
Note.
General Rule
Special Rules
(1) (2)
General Rule
Caution.
must
For Paperwork Reduction Act Notice, see the Instructions for Form 990, 990-EZ, or 990-PF.
exclusively
exclusively exclusively
(check one):
Form 990 or 990-EZ 501(c)( ) (enter number) organization
4947(a)(1) nonexempt charitable trust treated as a private foundation
527 political organization
Form 990-PF 501(c)(3) exempt private foundation
4947(a)(1) nonexempt charitable trust treated as a private foundation
501(c)(3) taxable private foundation
Check if your organization is covered by the or a
Only a section 501(c)(7), (8), or (10) organization can check boxes for both the General Rule and a Special Rule. See instructions.
For an organization filing Form 990, 990-EZ, or 990-PF that received, during the year, $5,000 or more (in money or property) from any one
contributor. Complete Parts I and II.
For a section 501(c)(3) organization filing Form 990 or 990-EZ that met the 33 1/3% support test of the regulations under sections
509(a)(1) and 170(b)(1)(A)(vi) and received from any one contributor, during the year, a contribution of the greater of $5,000 or 2%
of the amount on (i) Form 990, Part VIII, line 1h, or (ii) Form 990-EZ, line 1. Complete Parts I and II.
For a section 501(c)(7), (8), or (10) organization filing Form 990 or 990-EZ that received from any one contributor, during the year,
total contributions of more than $1,000 for use for religious, charitable, scientific, literary, or educational purposes, or
the prevention of cruelty to children or animals. Complete Parts I, II, and III.
For a section 501(c)(7), (8), or (10) organization filing Form 990 or 990-EZ that received from any one contributor, during the year,
contributions for use for religious, charitable, etc., purposes, but these contributions did not total to more than $1,000.
If this box is checked, enter here the total contributions that were received during the year for an religious, charitable, etc.,
purpose. Do not complete any of the parts unless the applies to this organization because it received nonexclusively
religious, charitable, etc., contributions of $5,000 or more during the year ~~~~~~~~~~~~~~~~~ | $
An organization that is not covered by the General Rule and/or the Special Rules does not file Schedule B (Form 990, 990-EZ, or 990-PF),
but it answer "No" on Part IV, line 2, of its Form 990; or check the box on line H of its Form 990-EZ or on Part I, line 2 of its Form 990-PF, to
certify that it does not meet the filing requirements of Schedule B (Form 990, 990-EZ, or 990-PF).
LHA
Schedule B Schedule of Contributors
2012
UNITED WAY OF EAST CENTRAL IOWA, INC. 42-0861239
X 3
X

223452 12-21-12
Name of organization Employer identification number
Schedule B (Form 990, 990-EZ, or 990-PF) (2012)
(a)
No.
(b)
Name, address, and ZIP + 4
(c)
Total contributions
(d)
Type of contribution
Person
Payroll
Noncash
(a)
No.
(b)
Name, address, and ZIP + 4
(c)
Total contributions
(d)
Type of contribution
Person
Payroll
Noncash
(a)
No.
(b)
Name, address, and ZIP + 4
(c)
Total contributions
(d)
Type of contribution
Person
Payroll
Noncash
(a)
No.
(b)
Name, address, and ZIP + 4
(c)
Total contributions
(d)
Type of contribution
Person
Payroll
Noncash
(a)
No.
(b)
Name, address, and ZIP + 4
(c)
Total contributions
(d)
Type of contribution
Person
Payroll
Noncash
(a)
No.
(b)
Name, address, and ZIP + 4
(c)
Total contributions
(d)
Type of contribution
Person
Payroll
Noncash
Schedule B (Form 990, 990-EZ, or 990-PF) (2012) Page
(see instructions). Use duplicate copies of Part I if additional space is needed.
$
(Complete Part II if thereis a noncash contribution.)
$
(Complete Part II if thereis a noncash contribution.)
$
(Complete Part II if thereis a noncash contribution.)
$
(Complete Part II if thereis a noncash contribution.)
$
(Complete Part II if thereis a noncash contribution.)
$
(Complete Part II if thereis a noncash contribution.)
2
Part I Contributors
UNITED WAY OF EAST CENTRAL IOWA, INC. 42-0861239
1 TRANSAMERICA XX
4333 EDGEWOOD ROAD NE 1,620,318.
CEDAR RAPIDS, IA 52499
2 CARGILL, INC XX
P.O. BOX 1467 293,749.
CEDAR RAPIDS, IA 52406-1467
3 ROCKWELL COLLINS XX
400 COLLINS RD NE 1,720,250.
CEDAR RAPIDS, IA 52498
4 ALLIANT ENERGY XX
PO BOX 351 291,203.
CEDAR RAPIDS, IA 52406-0351
5 ZACH JOHNSON FOUNDATION X
PO BOX 2336 357,385.
CEDAR RAPIDS, IA 52406
6 GENERAL MILLS, INC. XX
PO BOX 3007 501,824.
CEDAR RAPIDS, IA 52406-3007

223452 12-21-12
Name of organization Employer identification number
Schedule B (Form 990, 990-EZ, or 990-PF) (2012)
(a)
No.
(b)
Name, address, and ZIP + 4
(c)
Total contributions
(d)
Type of contribution
Person
Payroll
Noncash
(a)
No.
(b)
Name, address, and ZIP + 4
(c)
Total contributions
(d)
Type of contribution
Person
Payroll
Noncash
(a)
No.
(b)
Name, address, and ZIP + 4
(c)
Total contributions
(d)
Type of contribution
Person
Payroll
Noncash
(a)
No.
(b)
Name, address, and ZIP + 4
(c)
Total contributions
(d)
Type of contribution
Person
Payroll
Noncash
(a)
No.
(b)
Name, address, and ZIP + 4
(c)
Total contributions
(d)
Type of contribution
Person
Payroll
Noncash
(a)
No.
(b)
Name, address, and ZIP + 4
(c)
Total contributions
(d)
Type of contribution
Person
Payroll
Noncash
Schedule B (Form 990, 990-EZ, or 990-PF) (2012) Page
(see instructions). Use duplicate copies of Part I if additional space is needed.
$
(Complete Part II if thereis a noncash contribution.)
$
(Complete Part II if thereis a noncash contribution.)
$
(Complete Part II if thereis a noncash contribution.)
$
(Complete Part II if thereis a noncash contribution.)
$
(Complete Part II if thereis a noncash contribution.)
$
(Complete Part II if thereis a noncash contribution.)
2
Part I Contributors
UNITED WAY OF EAST CENTRAL IOWA, INC. 42-0861239
7 HALL-PERRINE FOUNDATION X
115 THIRD STREET SE, SUITE 803 550,000.
CEDAR RAPIDS, IA 52401-1222

223453 12-21-12
Name of organization Employer identification number
Schedule B (Form 990, 990-EZ, or 990-PF) (2012)
(a)
No.
from
Part I
(c)
FMV (or estimate)
(see instructions)
(b)
Description of noncash property given
(d)
Date received
(a)
No.
from
Part I
(c)
FMV (or estimate)
(see instructions)
(b)
Description of noncash property given
(d)
Date received
(a)
No.
from
Part I
(c)
FMV (or estimate)
(see instructions)
(b)
Description of noncash property given
(d)
Date received
(a)
No.
from
Part I
(c)
FMV (or estimate)
(see instructions)
(b)
Description of noncash property given
(d)
Date received
(a)
No.
from
Part I
(c)
FMV (or estimate)
(see instructions)
(b)
Description of noncash property given
(d)
Date received
(a)
No.
from
Part I
(c)
FMV (or estimate)
(see instructions)
(b)
Description of noncash property given
(d)
Date received
Schedule B (Form 990, 990-EZ, or 990-PF) (2012) Page
(see instructions). Use duplicate copies of Part II if additional space is needed.
$
$
$
$
$
$
3
Part II Noncash Property
UNITED WAY OF EAST CENTRAL IOWA, INC. 42-0861239

(Enter this information once.)
223454 12-21-12
Name of organization Employer identification number
religious, charitable, etc., individual contributions to section 501(c)(7), (8), or (10) organizations that total more than $1,000 for theyear. (a) (e) and
$1,000 or less
Schedule B (Form 990, 990-EZ, or 990-PF) (2012)
(a) No.fromPart I
(b) Purpose of gift (c) Use of gift (d) Description of how gift is held
(e) Transfer of gift
Transferee's name, address, and ZIP + 4 Relationship of transferor to transferee
(a) No.fromPart I
(b) Purpose of gift (c) Use of gift (d) Description of how gift is held
(e) Transfer of gift
Transferee's name, address, and ZIP + 4 Relationship of transferor to transferee
(a) No.fromPart I
(b) Purpose of gift (c) Use of gift (d) Description of how gift is held
(e) Transfer of gift
Transferee's name, address, and ZIP + 4 Relationship of transferor to transferee
(a) No.fromPart I
(b) Purpose of gift (c) Use of gift (d) Description of how gift is held
(e) Transfer of gift
Transferee's name, address, and ZIP + 4 Relationship of transferor to transferee
exclusively Complete columns through the following line entry. For organizations completing Part III, enter
the total of religious, charitable, etc., contributions of for the year.
Schedule B (Form 990, 990-EZ, or 990-PF) (2012) Page
| $
Use duplicate copies of Part III if additional space is needed.
Exclusively
4
Part III
UNITED WAY OF EAST CENTRAL IOWA, INC. 42-0861239
OMB No. 1545-0047
Department of the TreasuryInternal Revenue Service
23204101-07-13
(Form 990 or 990-EZ)For Organizations Exempt From Income Tax Under section 501(c) and section 527
Open to PublicInspection
Complete if the organization is described below. Attach to Form 990 or Form 990-EZ.
| See separate instructions.
If the organization answered "Yes," to Form 990, Part IV, line 3, or Form 990-EZ, Part V, line 46 (Political Campaign Activities), then
If the organization answered "Yes," to Form 990, Part IV, line 4, or Form 990-EZ, Part VI, line 47 (Lobbying Activities), then
If the organization answered "Yes," to Form 990, Part IV, line 5 (Proxy Tax), or Form 990-EZ, Part V, line 35c (Proxy Tax), then
Employer identification number
1
2
3
1
2
3
4
Yes No
a
b
Yes No
1
2
3
4
5
Form 1120-POL Yes No
(a) (b) (c) (d) (e)
For Paperwork Reduction Act Notice, see the Instructions for Form 990 or 990-EZ. Schedule C (Form 990 or 990-EZ) 2012
¥ Section 501(c)(3) organizations: Complete Parts I-A and B. Do not complete Part I-C.
¥ Section 501(c) (other than section 501(c)(3)) organizations: Complete Parts I-A and C below. Do not complete Part I-B.
¥ Section 527 organizations: Complete Part I-A only.
¥ Section 501(c)(3) organizations that have filed Form 5768 (election under section 501(h)): Complete Part II-A. Do not complete Part II-B.
¥ Section 501(c)(3) organizations that have NOT filed Form 5768 (election under section 501(h)): Complete Part II-B. Do not complete Part II-A.
¥ Section 501(c)(4), (5), or (6) organizations: Complete Part III.Name of organization
Provide a description of the organization's direct and indirect political campaign activities in Part IV.
Political expenditures
Volunteer hours
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~ $
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Enter the amount of any excise tax incurred by the organization under section 4955
Enter the amount of any excise tax incurred by organization managers under section 4955
If the organization incurred a section 4955 tax, did it file Form 4720 for this year?
~~~~~~~~~~~~~ $
~~~~~~~~~~ $
~~~~~~~~~~~~~~~~~~~
Was a correction made?
If "Yes," describe in Part IV.
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Enter the amount directly expended by the filing organization for section 527 exempt function activities
Enter the amount of the filing organization's funds contributed to other organizations for section 527
exempt function activities
~~~~ $
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~ $
Total exempt function expenditures. Add lines 1 and 2. Enter here and on Form 1120-POL,
line 17b
Did the filing organization file for this year?
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~ $
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Enter the names, addresses and employer identification number (EIN) of all section 527 political organizations to which the filing organization
made payments. For each organization listed, enter the amount paid from the filing organization's funds. Also enter the amount of political
contributions received that were promptly and directly delivered to a separate political organization, such as a separate segregated fund or a
political action committee (PAC). If additional space is needed, provide information in Part IV.
Name Address EIN Amount paid fromfiling organization's
funds. If none, enter -0-.
Amount of politicalcontributions received and
promptly and directlydelivered to a separatepolitical organization.
If none, enter -0-.
LHA
SCHEDULE C
Part I-A Complete if the organization is exempt under section 501(c) or is a section 527 organization.
Part I-B Complete if the organization is exempt under section 501(c)(3).
Part I-C Complete if the organization is exempt under section 501(c), except section 501(c)(3).
Political Campaign and Lobbying Activities2012
J J
J
JJ
J
J
J
UNITED WAY OF EAST CENTRAL IOWA, INC. 42-0861239

23204201-07-13
If the amount on line 1e, column (a) or (b) is:
2
A
B
Limits on Lobbying Expenditures(The term "expenditures" means amounts paid or incurred.)
(a) (b)
1a
b
c
d
e
f
The lobbying nontaxable amount is:
g
h
i
j
Yes No
4-Year Averaging Period Under Section 501(h)(Some organizations that made a section 501(h) election do not have to complete all of the five
columns below. See the instructions for lines 2a through 2f on page 4.)
Lobbying Expenditures During 4-Year Averaging Period
(a) (b) (c) (d) (e)
2a
b
c
d
e
f
Schedule C (Form 990 or 990-EZ) 2012
Schedule C (Form 990 or 990-EZ) 2012 Page
Check if the filing organization belongs to an affiliated group (and list in Part IV each affiliated group member's name, address, EIN,
expenses, and share of excess lobbying expenditures).
Check if the filing organization checked box A and "limited control" provisions apply.
Filingorganization's
totals
Affiliated grouptotals
Total lobbying expenditures to influence public opinion (grass roots lobbying)
Total lobbying expenditures to influence a legislative body (direct lobbying)
~~~~~~~~~~
~~~~~~~~~~~
Total lobbying expenditures (add lines 1a and 1b)
Other exempt purpose expenditures
~~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Total exempt purpose expenditures (add lines 1c and 1d)
Lobbying nontaxable amount. Enter the amount from the following table in both columns.
~~~~~~~~~~~~~~~~~~~~
Not over $500,000
Over $500,000 but not over $1,000,000
Over $1,000,000 but not over $1,500,000
Over $1,500,000 but not over $17,000,000
Over $17,000,000
20% of the amount on line 1e.
$100,000 plus 15% of the excess over $500,000.
$175,000 plus 10% of the excess over $1,000,000.
$225,000 plus 5% of the excess over $1,500,000.
$1,000,000.
Grassroots nontaxable amount (enter 25% of line 1f)
Subtract line 1g from line 1a. If zero or less, enter -0-
Subtract line 1f from line 1c. If zero or less, enter -0-
~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~
If there is an amount other than zero on either line 1h or line 1i, did the organization file Form 4720
reporting section 4911 tax for this year? ��������������������������������������
Calendar year (or fiscal year beginning in)
2009 2010 2011 2012 Total
Lobbying nontaxable amount
Lobbying ceiling amount
(150% of line 2a, column(e))
Total lobbying expenditures
Grassroots nontaxable amount
Grassroots ceiling amount
(150% of line 2d, column (e))
Grassroots lobbying expenditures
Part II-A Complete if the organization is exempt under section 501(c)(3) and filed Form 5768 (election under section 501(h)).
J
J
UNITED WAY OF EAST CENTRAL IOWA, INC. 42-0861239

23204301-07-13
3
(a) (b)
Yes No Amount
1
a
b
c
d
e
f
g
h
i
j
a
b
c
d
2
Yes No
1
2
3
1
2
3
1
2
3
4
5
(do not include amounts of political
expenses for which the section 527(f) tax was paid).
1
2a
2b
2c
3
4
5
a
b
c
Schedule C (Form 990 or 990-EZ) 2012
For each "Yes," response to lines 1a through 1i below, provide in Part IV a detailed descriptionof the lobbying activity.
Schedule C (Form 990 or 990-EZ) 2012 Page
During the year, did the filing organization attempt to influence foreign, national, state or
local legislation, including any attempt to influence public opinion on a legislative matter
or referendum, through the use of:
Volunteers?
Paid staff or management (include compensation in expenses reported on lines 1c through 1i)?
Media advertisements?
Mailings to members, legislators, or the public?
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
~
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~
Publications, or published or broadcast statements?
Grants to other organizations for lobbying purposes?
~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~
Direct contact with legislators, their staffs, government officials, or a legislative body?
Rallies, demonstrations, seminars, conventions, speeches, lectures, or any similar means?
Other activities?
~~~~~~
~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Total. Add lines 1c through 1i
Did the activities in line 1 cause the organization to be not described in section 501(c)(3)?
If "Yes," enter the amount of any tax incurred under section 4912
If "Yes," enter the amount of any tax incurred by organization managers under section 4912
If the filing organization incurred a section 4912 tax, did it file Form 4720 for this year?
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
~~~~
~~~~~~~~~~~~~~~~
~~~
������
Were substantially all (90% or more) dues received nondeductible by members?
Did the organization make only in-house lobbying expenditures of $2,000 or less?
Did the organization agree to carry over lobbying and political expenditures from the prior year?
~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~
���������
Dues, assessments and similar amounts from members
Section 162(e) nondeductible lobbying and political expenditures
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Current year
Carryover from last year
Total
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Aggregate amount reported in section 6033(e)(1)(A) notices of nondeductible section 162(e) dues
If notices were sent and the amount on line 2c exceeds the amount on line 3, what portion of the excess
does the organization agree to carryover to the reasonable estimate of nondeductible lobbying and political
expenditure next year?
~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Taxable amount of lobbying and political expenditures (see instructions) ���������������������
Complete this part to provide the descriptions required for Part I-A, line 1; Part I-B, line 4; Part I-C, line 5; Part II-A (affiliated group list); Part II-A, line 2;
and Part II-B, line 1. Also, complete this part for any additional information.
Part II-B Complete if the organization is exempt under section 501(c)(3) and has NOT filed Form 5768(election under section 501(h)).
Part III-A Complete if the organization is exempt under section 501(c)(4), section 501(c)(5), or section 501(c)(6).
Part III-B Complete if the organization is exempt under section 501(c)(4), section 501(c)(5), or section 501(c)(6) and if either (a) BOTH Part III-A, lines 1 and 2, are answered "No," OR (b) Part III-A, line 3, isanswered "Yes."
Part IV Supplemental Information
UNITED WAY OF EAST CENTRAL IOWA, INC. 42-0861239
XXXXXXXX
X 1,800.1,800.
X
PART II-B, LINE 1, LOBBYING ACTIVITIES:
CONTRACTED L&L MURPHY CONSULTING TO PROVIDE PUBLIC POLICY SUPPORT
SERVICES. IN ADDITION, THE ORGANZATION IS A MEMBER OF A NATIONAL
ASSOCIATION OF UNITED WAYS, UNITED WAY WORLDWIDE, AS WELL AS A LOCAL
ASSOCIATION OF UNITED WAYS, UNITED WAYS OF IOWA, TO WHICH IT PAYS
ANNUAL MEMBERSHIP DUES. A SMALL PORTION OF THE ANNUAL DUES PAID TO

23204401-07-13
4
Schedule C (Form 990 or 990-EZ) 2012
(continued)Schedule C (Form 990 or 990-EZ) 2012 Page
Part IV Supplemental Information
UNITED WAY OF EAST CENTRAL IOWA, INC. 42-0861239
UNITED WAY WORLDWIDE AND UNITED WAYS OF IOWA IS EXPENDED ON LOBBYING
ACTIVITIES. HOWEVER, SINCE THIS LOBBYING ACTIVITY IS NOT CARRIED ON
DIRECTLY BY THE FILING ORGANIZATION, THE LOBBYING PORTION OF
ASSOCIATION DUES IS NOT REFLECTED IN THE AMOUNT OF LOBBYING
EXPENDITURES IN PART II-B.
OMB No. 1545-0047
Department of the TreasuryInternal Revenue Service
23205112-10-12
Held at the End of the Tax Year
(Form 990) | Complete if the organization answered "Yes," to Form 990,
Part IV, line 6, 7, 8, 9, 10, 11a, 11b, 11c, 11d, 11e, 11f, 12a, or 12b.
| Attach to Form 990. | See separate instructions.Open to PublicInspection
Name of the organization Employer identification number
(a) (b)
1
2
3
4
5
6
Yes No
Yes No
1
2
3
4
5
6
7
8
9
a
b
c
d
2a
2b
2c
2d
Yes No
Yes No
1
2
a
b
(i)
(ii)
a
b
For Paperwork Reduction Act Notice, see the Instructions for Form 990. Schedule D (Form 990) 2012
Complete if the
organization answered "Yes" to Form 990, Part IV, line 6.
Donor advised funds Funds and other accounts
Total number at end of year
Aggregate contributions to (during year)
Aggregate grants from (during year)
Aggregate value at end of year
~~~~~~~~~~~~~~~
~~~~~~~~
~~~~~~~~~~
~~~~~~~~~~~~~
Did the organization inform all donors and donor advisors in writing that the assets held in donor advised funds
are the organization's property, subject to the organization's exclusive legal control?~~~~~~~~~~~~~~~~~~
Did the organization inform all grantees, donors, and donor advisors in writing that grant funds can be used only
for charitable purposes and not for the benefit of the donor or donor advisor, or for any other purpose conferring
impermissible private benefit? ��������������������������������������������
Complete if the organization answered "Yes" to Form 990, Part IV, line 7.
Purpose(s) of conservation easements held by the organization (check all that apply).
Preservation of land for public use (e.g., recreation or education)
Protection of natural habitat
Preservation of open space
Preservation of an historically important land area
Preservation of a certified historic structure
Complete lines 2a through 2d if the organization held a qualified conservation contribution in the form of a conservation easement on the last
day of the tax year.
Total number of conservation easements
Total acreage restricted by conservation easements
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~~
Number of conservation easements on a certified historic structure included in (a)
Number of conservation easements included in (c) acquired after 8/17/06, and not on a historic structure
listed in the National Register
~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Number of conservation easements modified, transferred, released, extinguished, or terminated by the organization during the tax
year |
Number of states where property subject to conservation easement is located |
Does the organization have a written policy regarding the periodic monitoring, inspection, handling of
violations, and enforcement of the conservation easements it holds? ~~~~~~~~~~~~~~~~~~~~~~~~~
Staff and volunteer hours devoted to monitoring, inspecting, and enforcing conservation easements during the year |
Amount of expenses incurred in monitoring, inspecting, and enforcing conservation easements during the year | $
Does each conservation easement reported on line 2(d) above satisfy the requirements of section 170(h)(4)(B)(i)
and section 170(h)(4)(B)(ii)? ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
In Part XIII, describe how the organization reports conservation easements in its revenue and expense statement, and balance sheet, and
include, if applicable, the text of the footnote to the organization's financial statements that describes the organization's accounting for
conservation easements.
Complete if the organization answered "Yes" to Form 990, Part IV, line 8.
If the organization elected, as permitted under SFAS 116 (ASC 958), not to report in its revenue statement and balance sheet works of art,
historical treasures, or other similar assets held for public exhibition, education, or research in furtherance of public service, provide, in Part XIII,
the text of the footnote to its financial statements that describes these items.
If the organization elected, as permitted under SFAS 116 (ASC 958), to report in its revenue statement and balance sheet works of art, historical
treasures, or other similar assets held for public exhibition, education, or research in furtherance of public service, provide the following amounts
relating to these items:
Revenues included in Form 990, Part VIII, line 1
Assets included in Form 990, Part X
~~~~~~~~~~~~~~~~~~~~~~~~~~~~ | $
$~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~ |
If the organization received or held works of art, historical treasures, or other similar assets for financial gain, provide
the following amounts required to be reported under SFAS 116 (ASC 958) relating to these items:
Revenues included in Form 990, Part VIII, line 1
Assets included in Form 990, Part X
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~ | $
$~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~ |
LHA
Part I Organizations Maintaining Donor Advised Funds or Other Similar Funds or Accounts.
Part II Conservation Easements.
Part III Organizations Maintaining Collections of Art, Historical Treasures, or Other Similar Assets.
SCHEDULE D Supplemental Financial Statements 2012
UNITED WAY OF EAST CENTRAL IOWA, INC. 42-0861239

23205212-10-12
3
4
5
a
b
c
d
e
Yes No
1
2
a
b
c
d
e
f
a
b
Yes No
1c
1d
1e
1f
Yes No
(a) (b) (c) (d) (e)
1
2
3
4
a
b
c
d
e
f
g
a
b
c
a
b
Yes No
(i)
(ii)
3a(i)
3a(ii)
3b
(a) (b) (c) (d)
1a
b
c
d
e
Total.
Schedule D (Form 990) 2012
(continued)
(Column (d) must equal Form 990, Part X, column (B), line 10(c).)
Two years back Three years back Four years back
Schedule D (Form 990) 2012 Page
Using the organization's acquisition, accession, and other records, check any of the following that are a significant use of its collection items
(check all that apply):
Public exhibition
Scholarly research
Preservation for future generations
Loan or exchange programs
Other
Provide a description of the organization's collections and explain how they further the organization's exempt purpose in Part XIII.
During the year, did the organization solicit or receive donations of art, historical treasures, or other similar assets
to be sold to raise funds rather than to be maintained as part of the organization's collection? ������������
Complete if the organization answered "Yes" to Form 990, Part IV, line 9, orreported an amount on Form 990, Part X, line 21.
Is the organization an agent, trustee, custodian or other intermediary for contributions or other assets not included
on Form 990, Part X?
If "Yes," explain the arrangement in Part XIII and complete the following table:
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Amount
Beginning balance
Additions during the year
Distributions during the year
Ending balance
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Did the organization include an amount on Form 990, Part X, line 21?
If "Yes," explain the arrangement in Part XIII. Check here if the explanation has been provided in Part XIII
~~~~~~~~~~~~~~~~~~~~~~~~~
�������������
Complete if the organization answered "Yes" to Form 990, Part IV, line 10.
Current year Prior year
Beginning of year balance
Contributions
Net investment earnings, gains, and losses
Grants or scholarships
~~~~~~~
~~~~~~~~~~~~~~
~~~~~~~~~
Other expenditures for facilities
and programs
Administrative expenses
End of year balance
~~~~~~~~~~~~~
~~~~~~~~
~~~~~~~~~~
Provide the estimated percentage of the current year end balance (line 1g, column (a)) held as:
Board designated or quasi-endowment
Permanent endowment
Temporarily restricted endowment
The percentages in lines 2a, 2b, and 2c should equal 100% .
| %
| %
| %
Are there endowment funds not in the possession of the organization that are held and administered for the organization
by:
unrelated organizations
related organizations
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
If "Yes" to 3a(ii), are the related organizations listed as required on Schedule R?
Describe in Part XIII the intended uses of the organization's endowment funds.
~~~~~~~~~~~~~~~~~~~~~~
See Form 990, Part X, line 10.
Description of property Cost or otherbasis (investment)
Cost or otherbasis (other)
Accumulateddepreciation
Book value
Land
Buildings
Leasehold improvements
~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~
~~~~~~~~~~
Equipment
Other
~~~~~~~~~~~~~~~~~
��������������������
Add lines 1a through 1e. |������������
2Part III Organizations Maintaining Collections of Art, Historical Treasures, or Other Similar Assets
Part IV Escrow and Custodial Arrangements.
Part V Endowment Funds.
Part VI Land, Buildings, and Equipment.
UNITED WAY OF EAST CENTRAL IOWA, INC. 42-0861239
1,531,503. 1,588,240. 1,241,401. 1,114,513. 1,413,926.50. 6,108. 176,666. 2,950. 400.
142,320. -598. 218,498. 177,288. -252,483.
59,806. 58,127. 44,359. 49,058. 44,046.4,211. 4,120. 3,966. 4,292. 3,284.
1,609,856. 1,531,503. 1,588,240. 1,241,401. 1,114,513.
36.5021.35
42.15
XX
401,959. 199,588. 202,371.
202,371.

(including name of security)
23205312-10-12
Total.
Total.
(a) (b) (c)
(a) (b) (c)
(a) (b)
Total.
(a) (b) 1.
Total.
2.
Schedule D (Form 990) 2012
(Column (b) must equal Form 990, Part X, col. (B) line 15.)
(Column (b) must equal Form 990, Part X, col. (B) line 25.)
Description of security or category
(Col. (b) must equal Form 990, Part X, col. (B) line 12.) |
(Col. (b) must equal Form 990, Part X, col. (B) line 13.) |
Schedule D (Form 990) 2012 Page
See Form 990, Part X, line 12.
Book value Method of valuation: Cost or end-of-year market value
(1)
(2)
(3)
Financial derivatives
Closely-held equity interests
Other
~~~~~~~~~~~~~~~
~~~~~~~~~~~
(A)
(B)
(C)
(D)
(E)
(F)
(G)
(H)
(I)
Description of investment typeSee Form 990, Part X, line 13.
Book value Method of valuation: Cost or end-of-year market value
(1)
(2)
(3)
(4)
(5)
(6)
(7)
(8)
(9)
(10)
See Form 990, Part X, line 15.
Description Book value
(1)
(2)
(3)
(4)
(5)
(6)
(7)
(8)
(9)
(10)
���������������������������� |
See Form 990, Part X, line 25.
Description of liability Book value
(1)
(2)
(3)
(4)
(5)
(6)
(7)
(8)
(9)
(10)
(11)
Federal income taxes
����� |
FIN 48 (ASC 740) Footnote. In Part XIII, provide the text of the footnote to the organization's financial statements that reports the organization's
liability for uncertain tax positions under FIN 48 (ASC 740). Check here if the text of the footnote has been provided in Part XIII ������
3Part VII Investments - Other Securities.
Part VIII Investments - Program Related.
Part IX Other Assets.
Part X Other Liabilities.
UNITED WAY OF EAST CENTRAL IOWA, INC. 42-0861239
INVESTMENT IN FCFH-IOWA,INC. 187,506. COSTINVESTMENT IN HUMANSERVICES CAMPUS OF EASTCENTRAL IOWA 13,851,970. COST
14,039,476.
PAYABLE TO FCFH-IOWA, INC. 305,000.AMOUNTS HELD ON BEHALF OF OTHERS 86,409.
391,409.
X

23205412-10-12
1
2
3
4
5
1
a
b
c
d
e
2a
2b
2c
2d
2a 2d 2e
32e 1
1
a
b
c
4a
4b
4a 4b
3 4c.
4c
5
1
2
3
4
5
1
a
b
c
d
e
2a
2b
2c
2d
2a 2d
2e 1
2e
3
1
a
b
c
4a
4b
4a 4b
3 4c.
4c
5
Schedule D (Form 990) 2012
(This must equal Form 990, Part I, line 12.)
(This must equal Form 990, Part I, line 18.)
Schedule D (Form 990) 2012 Page
Total revenue, gains, and other support per audited financial statements
Amounts included on line 1 but not on Form 990, Part VIII, line 12:
~~~~~~~~~~~~~~~~~~~
Net unrealized gains on investments
Donated services and use of facilities
Recoveries of prior year grants
Other (Describe in Part XIII.)
~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~~
Add lines through ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Subtract line from line ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Amounts included on Form 990, Part VIII, line 12, but not on line :
Investment expenses not included on Form 990, Part VIII, line 7b
Other (Describe in Part XIII.)
~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~~
Add lines and
Total revenue. Add lines and
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
�����������������
Total expenses and losses per audited financial statements
Amounts included on line 1 but not on Form 990, Part IX, line 25:
~~~~~~~~~~~~~~~~~~~~~~~~~~
Donated services and use of facilities
Prior year adjustments
Other losses
Other (Describe in Part XIII.)
~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~~
Add lines through
Subtract line from line
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Amounts included on Form 990, Part IX, line 25, but not on line :
Investment expenses not included on Form 990, Part VIII, line 7b
Other (Describe in Part XIII.)
~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~~
Add lines and
Total expenses. Add lines and
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
����������������
Complete this part to provide the descriptions required for Part II, lines 3, 5, and 9; Part III, lines 1a and 4; Part IV, lines 1b and 2b; Part V, line 4; Part
X, line 2; Part XI, lines 2d and 4b; and Part XII, lines 2d and 4b. Also complete this part to provide any additional information.
4Part XI Reconciliation of Revenue per Audited Financial Statements With Revenue per Return
Part XII Reconciliation of Expenses per Audited Financial Statements With Expenses per Return
Part XIII Supplemental Information
UNITED WAY OF EAST CENTRAL IOWA, INC. 42-0861239
10,422,759.
39,872.7,515.
486,002.533,389.
9,889,370.
2,105.1,252,161.
1,254,266.11,143,636.
10,845,039.
7,515.
680,178.687,693.
10,157,346.
2,105.1,252,161.
1,254,266.11,411,612.
PART V, LINE 4: THE ENDOWMENTS OF THE ORGANIZATION CONSIST OF VARIOUS
FUNDS ESTABLISHED TO SUPPORT THE GENERAL OPERATING NEEDS OF THE
ORGANIZATION. ITS ENDOWMENTS CONSIST OF BOTH DONOR-RESTRICTED ENDOWMENT
FUNDS AND FUNDS DESIGNATED BY THE BOARD OF DIRECTORS TO FUNCTION AS
ENDOWMENTS. PERMANENTLY RESTRICTED NET ASSETS CONSISTS OF $343,651 OF
ENDOWMENTS WHICH MUST BE INVESTED IN PERPETUITY, THE INCOME FROM WHICH IS
EXPENDABLE TO SUPPORT THE OPERATIONS OF THE ORGANIZATION.

23205512-10-12
5
Schedule D (Form 990) 2012
(continued)Schedule D (Form 990) 2012 Page Part XIII Supplemental Information
UNITED WAY OF EAST CENTRAL IOWA, INC. 42-0861239
PART X, LINE 2: THE ORGANIZATION IS EXEMPT FROM INCOME TAXES UNDER
PROVISIONS OF SECTION 501(C)(3) OF THE INTERNAL REVENUE CODE. AS SUCH, THE
ORGANIZATION IS TAXED ONLY ON ITS UNRELATED BUSINESS INCOME. MANAGEMENT
HAS DETERMINED THE ORGANIZATION DID NOT RECEIVE ANY UNRELATED BUSINESS
INCOME FOR THE YEARS ENDED JUNE 30, 2013 AND 2012. THE ORGANIZATION IS NOT
A PRIVATE FOUNDATION UNDER PROVISIONS OF SECTION 509(A) OF THE INTERNAL
REVENUE CODE.
WHEN TAX RETURNS ARE FILED, IT IS HIGHLY CERTAIN THAT SOME POSITIONS TAKEN
WOULD BE SUSTAINED UPON EXAMINATION BY THE TAXING AUTHORITIES, WHILE
OTHERS ARE SUBJECT TO UNCERTAINTY ABOUT THE MERITS OF THE POSITION TAKEN
OR THE AMOUNT OF THE POSITION THAT WOULD ULTIMATELY BE SUSTAINED. THE
BENEFIT OF A TAX POSITION IS RECOGNIZED IN THE FINANCIAL STATEMENTS IN THE
PERIOD DURING WHICH, BASED UPON ALL AVAILABLE EVIDENCE, MANAGEMENT
BELIEVES IT IS MORE LIKELY THAN NOT THAT THE POSITION WILL BE SUSTAINED
UPON EXAMINATION, INCLUDING THE RESOLUTION OF APPEALS OR LITIGATION
PROCESSES, IF ANY. THE ORGANIZATION HAD NO UNRECOGNIZED TAX BENEFITS AS OF
AND FOR THE YEARS ENDED JUNE 30, 2013 AND 2012. THE ORGANIZATION IS NO
LONGER SUBJECT TO EXAMINATIONS BY FEDERAL AUTHORITIES FOR YEARS ENDED
BEFORE JUNE 30, 2010 NOR HAVE WE BEEN NOTIFIED OF ANY IMPENDING
EXAMINATIONS AND NO EXAMINATIONS ARE CURRENTLY IN PROCESS.
PART XI, LINE 2D - OTHER ADJUSTMENTS:
CHANGE IN BENEFICIAL INTEREST IN COMMUNITY FOUNDATION: 26,112.
REVENUE OF SUBSIDIARY - FCFH-IOWA, INC. 424,165.
REVENUE OF SUBSIDIARY - HUMAN SERVICES CAMPUS OF EAST
CENTRAL IOWA 513,223.
ELIMINATIONS OF REVENUE FOR CONSOLIDATION -477,498.

23205512-10-12
5
Schedule D (Form 990) 2012
(continued)Schedule D (Form 990) 2012 Page Part XIII Supplemental Information
UNITED WAY OF EAST CENTRAL IOWA, INC. 42-0861239
TOTAL TO SCHEDULE D, PART XI, LINE 2D 486,002.
PART XI, LINE 4B - OTHER ADJUSTMENTS:
DONOR OPTION ALLOCATIONS NETTED AGAINST REVENUE FOR AUDIT 1,252,161.
PART XII, LINE 2D - OTHER ADJUSTMENTS:
EXPENSE OF SUBSIDIARY - FCFH-IOWA, INC. 416,902.
EXPENSE OF SUBSIDIARY - HUMAN SERVICES CAMPUS OF EAST
CENTRAL IOWA 740,774.
ELIMINATIONS OF EXPENSE FOR CONSOLIDATION -477,498.
TOTAL TO SCHEDULE D, PART XII, LINE 2D 680,178.
PART XII, LINE 4B - OTHER ADJUSTMENTS:
DONOR OPTION ALLOCATIONS NETTED AGAINST REVENUE FOR AUDIT 1,252,161.

OM
B N
o.
15
45
-00
47
Dep
art
men
t o
f th
e T
reasu
ry
Inte
rnal R
even
ue S
erv
ice
23
21
01
12
-18
-12
Gra
nts
an
d O
the
r A
ssis
tan
ce
to
Org
an
iza
tio
ns,
Go
vern
me
nts
, a
nd
In
div
idu
als
in
th
e U
nit
ed
Sta
tes
SC
HE
DU
LE
I(F
orm
99
0)
Co
mp
lete
if
the
org
an
iza
tio
n a
nsw
ere
d "
Ye
s"
to F
orm
99
0, P
art
IV
, lin
e 2
1 o
r 2
2.
| A
tta
ch
to
Fo
rm 9
90
.
Op
en
to
Pu
blic
Insp
ec
tio
n
Em
plo
yer
ide
nti
fic
ati
on
nu
mb
er
Ge
ne
ral In
form
ati
on
on
Gra
nts
an
d A
ssis
tan
ce
Pa
rt I
1 2
Ye
sN
o
Pa
rt I
IG
ran
ts a
nd
Oth
er
Assis
tan
ce
to
Go
vern
me
nts
an
d O
rga
niz
ati
on
s in
th
e U
nit
ed
Sta
tes.
(f)
1 (
a)
(b)
(c)
(d)
(e)
(g)
(h)
2 3
Fo
r P
ap
erw
ork
Re
du
cti
on
Ac
t N
oti
ce
, se
e t
he
In
str
uc
tio
ns f
or
Fo
rm 9
90
.S
ch
ed
ule
I (
Fo
rm 9
90
) (2
01
2)
Nam
e o
f th
e o
rgan
izatio
n
Do
es
the o
rgan
izatio
n m
ain
tain
reco
rds
to s
ub
stan
tiate
th
e a
mo
un
t o
f th
e g
ran
ts o
r ass
ista
nce, th
e g
ran
tees'
elig
ibili
ty f
or
the g
ran
ts o
r ass
ista
nce, an
d t
he s
ele
ctio
n
crite
ria u
sed
to
aw
ard
th
e g
ran
ts o
r ass
ista
nce?
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
Desc
rib
e in
Part
IV
th
e o
rgan
izatio
n's
pro
ced
ure
s fo
r m
on
ito
rin
g t
he u
se o
f g
ran
t fu
nd
s in
th
e U
nited
Sta
tes.
Co
mp
lete
if t
he o
rgan
izatio
n a
nsw
ere
d "
Yes"
to
Fo
rm 9
90
, P
art
IV
, lin
e 2
1, fo
r an
y
recip
ien
t th
at
receiv
ed
mo
re t
han
$5
,00
0. P
art
II can
be d
up
licate
d if
ad
ditio
nal s
pace is
need
ed
.M
eth
od
of
valu
atio
n (b
oo
k,F
MV
, ap
pra
isal,
oth
er)
Nam
e a
nd
ad
dre
ss o
f o
rgan
izatio
no
r g
ove
rnm
en
tE
INIR
C s
ectio
nif
ap
plic
ab
leA
mo
un
t o
fcash
gra
nt
Am
ou
nt
of
no
n-c
ash
ass
ista
nce
Desc
rip
tio
n o
fn
on
-cash
ass
ista
nce
Pu
rpo
se o
f g
ran
to
r ass
ista
nce
En
ter
tota
l nu
mb
er
of
sectio
n 5
01
(c)(3
) an
d g
ove
rnm
en
t o
rgan
izatio
ns
liste
d in
th
e li
ne 1
tab
le
En
ter
tota
l nu
mb
er
of
oth
er
org
an
izatio
ns
liste
d in
th
e li
ne 1
tab
le
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
|
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
|
LH
A
2012
UNITED WAY OF EAST CENTRAL IOWA, INC.
42-0861239
X
ABBE CEN
TER
FOR
COMMUN
ITY
MENT
ALHEALTH -
520
11T
H STRE
ET N
W -
CEDAR RA
PIDS
, IA
52405
42-1
0452
57501(C)(3)
74,000.
0.N/A
N/A
PROGRAM FUNDING:HEALTH
AGING SE
RVIC
ES,
INC.
317 7TH
AVE
SE,
STE 30
2BCEDAR RA
PIDS
, IA
52401
-160
423
-708
5316
501(C)(3)
489,539.
0.N/A
N/A
PROGRAM FUNDING:HEALTH
AGING SE
RVIC
ES,
INC.
317 7T
H AV
E SE
, ST
E 30
2BCEDAR RA
PIDS
, IA
52401
-160
423
-708
5316
501(C)(3)
9,713.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
ALZHEIME
R'S
ASSO
CIATIO
N317 7TH
AVE
SE S
TE 402
CEDAR RA
PIDS
, IA
52401
42-1
3333
84501(C)(3)
37,783.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
ALZHEIME
R'S
ASSO
CIATIO
N EA
STCENTRAL
IOWA
CHA
PTER -
317
7TH
AVE
SE STE 4
02 -
CED
AR RAP
IDS,
IA
52401
42-1
3333
84501(C)(3)
45,000.
0.N/A
N/A
PROGRAM FUNDING:HEALTH
AMERICAN
CAN
CER
SOCIET
Y C.
R.4080 FIR
ST A
VENU
E NE
CEDAR RA
PIDS
, IA
52402
42-0
6803
53501(C)(3)
15,337.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
98.
0.
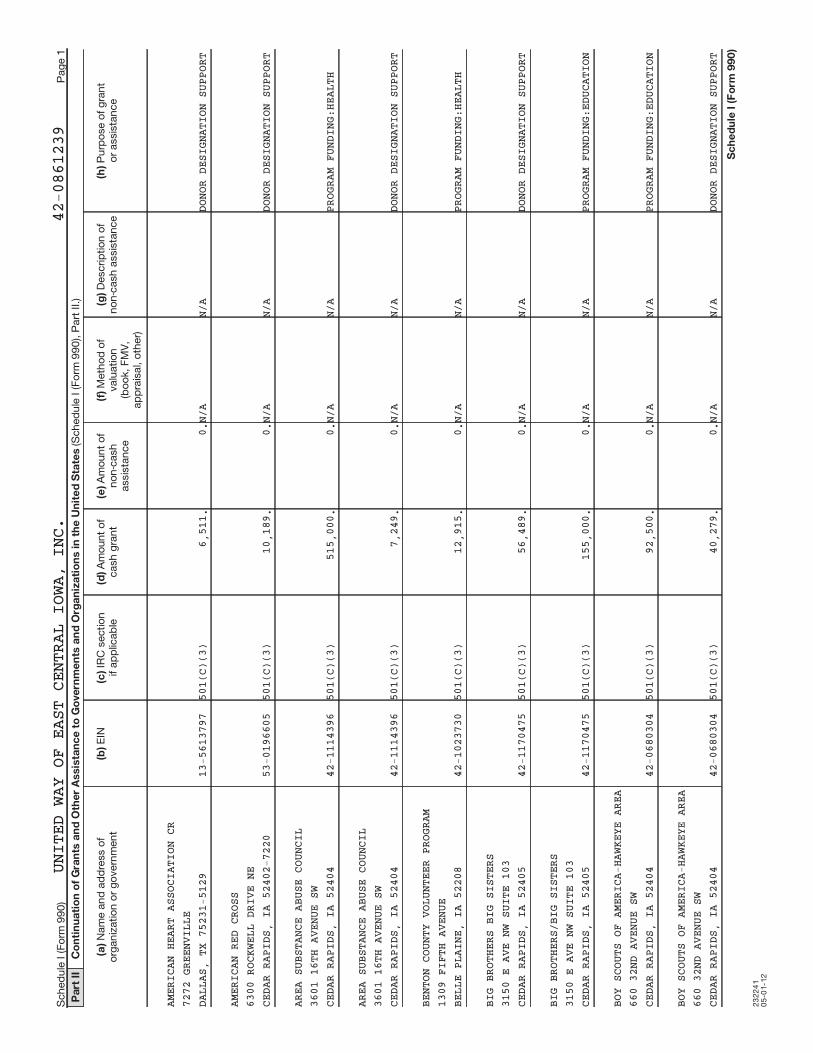
23
22
41
05
-01
-12
Pa
rt I
IC
on
tin
ua
tio
n o
f G
ran
ts a
nd
Oth
er
Assis
tan
ce
to
Go
vern
me
nts
an
d O
rga
niz
ati
on
s in
th
e U
nit
ed
Sta
tes
(a)
(b)
(c)
(d)
(e)
(f)
(g)
(h)
Sc
he
du
le I
(F
orm
99
0)
Sch
ed
ule
I (F
orm
99
0)
Pag
e 1
(Sch
ed
ule
I (F
orm
99
0), P
art
II.)
Nam
e a
nd
ad
dre
ss o
f o
rgan
izatio
n o
r g
ove
rnm
en
t E
IN IR
C s
ectio
nif
ap
plic
ab
le A
mo
un
t o
f cash
gra
nt
Am
ou
nt
of
no
n-c
ash
ass
ista
nce
Meth
od
of
valu
atio
n
(bo
ok,
FM
V,
ap
pra
isal,
oth
er)
Desc
rip
tio
n o
fn
on
-cash
ass
ista
nce
Pu
rpo
se o
f g
ran
to
r ass
ista
nce
UNITED WAY OF EAST CENTRAL IOWA, INC.
42-0861239
AMERICAN
HEA
RT A
SSOCIA
TION
CR
7272 GRE
ENVI
LLE
DALLAS,
TX 7
5231
-5129
13-5
6137
97501(C)(3)
6,511.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
AMERICAN
RED
CRO
SS6300 ROC
KWEL
L DR
IVE NE
CEDAR RA
PIDS
, IA
52402
-722
053
-019
6605
501(C)(3)
10,189.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
AREA SUB
STAN
CE A
BUSE C
OUNC
IL3601 16T
H AV
ENUE
SW
CEDAR RA
PIDS
, IA
52404
42-1
1143
96501(C)(3)
515,000.
0.N/A
N/A
PROGRAM FUNDING:HEALTH
AREA SUB
STAN
CE A
BUSE C
OUNC
IL3601 16T
H AV
ENUE
SW
CEDAR RA
PIDS
, IA
52404
42-1
1143
96501(C)(3)
7,249.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
BENTON C
OUNT
Y VO
LUNTEE
R PR
OGRA
M1309 FIF
TH A
VENU
EBELLE PL
AINE
, IA
52208
42-1
0237
30501(C)(3)
12,915.
0.N/A
N/A
PROGRAM FUNDING:HEALTH
BIG BROT
HERS
BIG
SISTE
RS3150 E A
VE N
W SU
ITE 10
3CEDAR RA
PIDS
, IA
52405
42-1
1704
75501(C)(3)
56,489.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
BIG BROT
HERS
/BIG
SISTE
RS3150 E A
VE N
W SU
ITE 10
3CEDAR RA
PIDS
, IA
52405
42-1
1704
75501(C)(3)
155,000.
0.N/A
N/A
PROGRAM FUNDING:EDUCATION
BOY SCOU
TS O
F AM
ERICA-
HAWK
EYE
AREA
660 32ND
AVE
NUE
SWCEDAR RA
PIDS
, IA
52404
42-0
6803
04501(C)(3)
92,500.
0.N/A
N/A
PROGRAM FUNDING:EDUCATION
BOY SCOU
TS O
F AM
ERICA-
HAWK
EYE
AREA
660 32ND
AVE
NUE
SWCEDAR RA
PIDS
, IA
52404
42-0
6803
04501(C)(3)
40,279.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
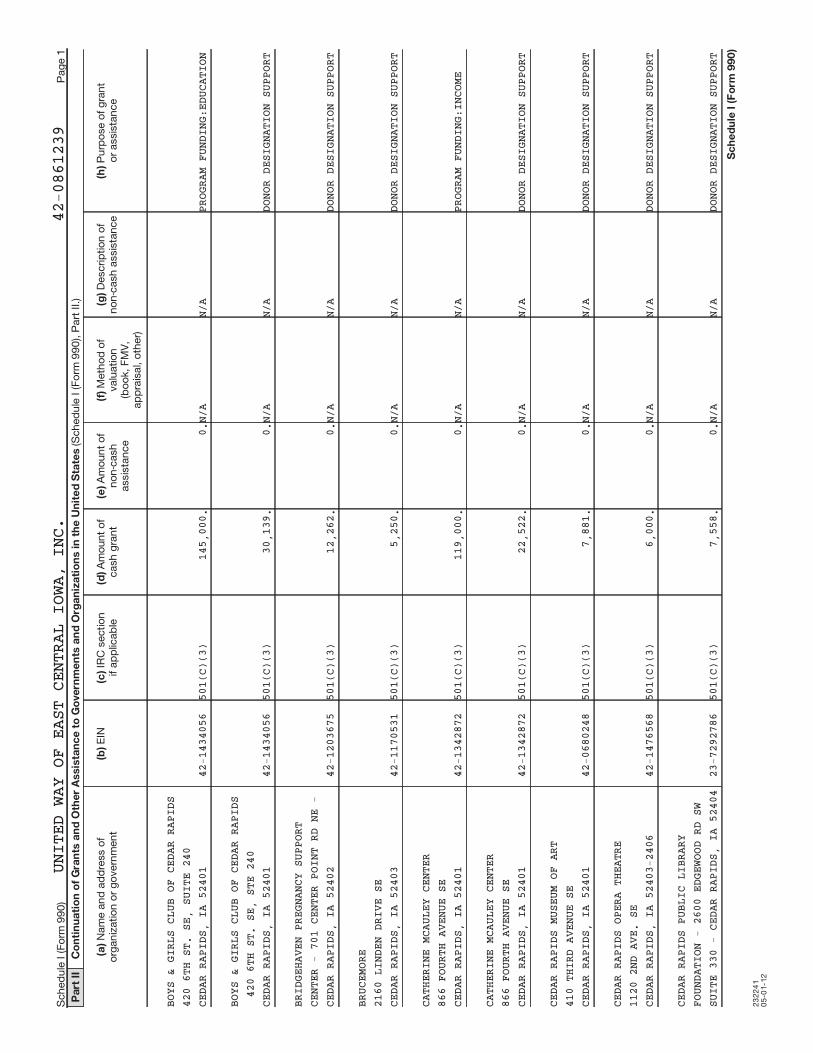
23
22
41
05
-01
-12
Pa
rt I
IC
on
tin
ua
tio
n o
f G
ran
ts a
nd
Oth
er
Assis
tan
ce
to
Go
vern
me
nts
an
d O
rga
niz
ati
on
s in
th
e U
nit
ed
Sta
tes
(a)
(b)
(c)
(d)
(e)
(f)
(g)
(h)
Sc
he
du
le I
(F
orm
99
0)
Sch
ed
ule
I (F
orm
99
0)
Pag
e 1
(Sch
ed
ule
I (F
orm
99
0), P
art
II.)
Nam
e a
nd
ad
dre
ss o
f o
rgan
izatio
n o
r g
ove
rnm
en
t E
IN IR
C s
ectio
nif
ap
plic
ab
le A
mo
un
t o
f cash
gra
nt
Am
ou
nt
of
no
n-c
ash
ass
ista
nce
Meth
od
of
valu
atio
n
(bo
ok,
FM
V,
ap
pra
isal,
oth
er)
Desc
rip
tio
n o
fn
on
-cash
ass
ista
nce
Pu
rpo
se o
f g
ran
to
r ass
ista
nce
UNITED WAY OF EAST CENTRAL IOWA, INC.
42-0861239
BOYS & G
IRLS
CLU
B OF C
EDAR
RAP
IDS
420 6TH
ST.
SE,
SUITE
240
CEDAR RA
PIDS
, IA
52401
42-1
4340
56501(C)(3)
145,000.
0.N/A
N/A
PROGRAM FUNDING:EDUCATION
BOYS & G
IRLS
CLU
B OF C
EDAR
RAP
IDS
420 6T
H ST
. SE
, ST
E 24
0CEDAR RA
PIDS
, IA
52401
42-1
4340
56501(C)(3)
30,139.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
BRIDGEHA
VEN
PREG
NANCY
SUPP
ORT
CENTER -
701
CEN
TER PO
INT
RD N
E -
CEDAR RA
PIDS
, IA
52402
42-1
2036
75501(C)(3)
12,262.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
BRUCEMOR
E2160 LIN
DEN
DRIV
E SE
CEDAR RA
PIDS
, IA
52403
42-1
1705
31501(C)(3)
5,250.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
CATHERIN
E MC
AULE
Y CENT
ER866 FOUR
TH A
VENU
E SE
CEDAR RA
PIDS
, IA
52401
42-1
3428
72501(C)(3)
119,000.
0.N/A
N/A
PROGRAM FUNDING:INCOME
CATHERIN
E MC
AULE
Y CENT
ER866 FOUR
TH A
VENU
E SE
CEDAR RA
PIDS
, IA
52401
42-1
3428
72501(C)(3)
22,522.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
CEDAR RA
PIDS
MUS
EUM OF
ART
410 THIR
D AV
ENUE
SE
CEDAR RA
PIDS
, IA
52401
42-0
6802
48501(C)(3)
7,881.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
CEDAR RA
PIDS
OPE
RA THE
ATRE
1120 2ND
AVE
. SE
CEDAR RA
PIDS
, IA
52403
-240
642
-147
6568
501(C)(3)
6,000.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
CEDAR RA
PIDS
PUB
LIC LI
BRAR
YFOUNDATI
ON -
260
0 EDGE
WOOD
RD
SWSUITE 33
0 -
CEDA
R RAPI
DS,
IA 5
2404
23-7
2927
86501(C)(3)
7,558.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
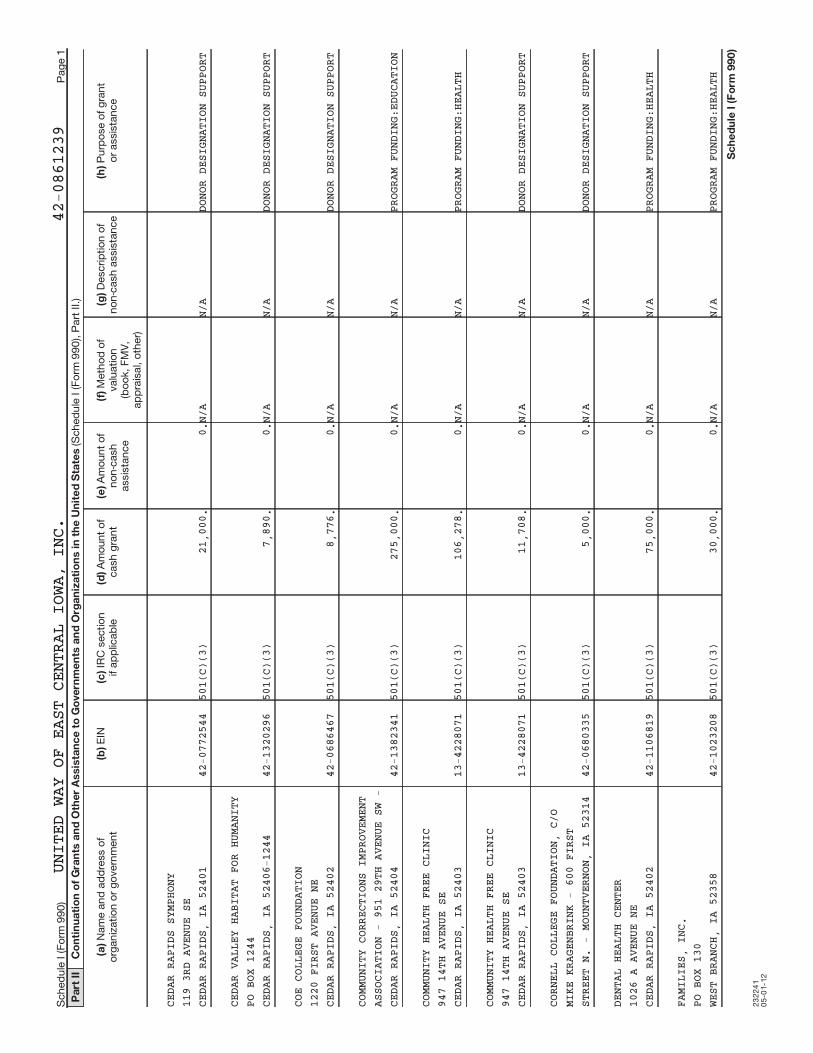
23
22
41
05
-01
-12
Pa
rt I
IC
on
tin
ua
tio
n o
f G
ran
ts a
nd
Oth
er
Assis
tan
ce
to
Go
vern
me
nts
an
d O
rga
niz
ati
on
s in
th
e U
nit
ed
Sta
tes
(a)
(b)
(c)
(d)
(e)
(f)
(g)
(h)
Sc
he
du
le I
(F
orm
99
0)
Sch
ed
ule
I (F
orm
99
0)
Pag
e 1
(Sch
ed
ule
I (F
orm
99
0), P
art
II.)
Nam
e a
nd
ad
dre
ss o
f o
rgan
izatio
n o
r g
ove
rnm
en
t E
IN IR
C s
ectio
nif
ap
plic
ab
le A
mo
un
t o
f cash
gra
nt
Am
ou
nt
of
no
n-c
ash
ass
ista
nce
Meth
od
of
valu
atio
n
(bo
ok,
FM
V,
ap
pra
isal,
oth
er)
Desc
rip
tio
n o
fn
on
-cash
ass
ista
nce
Pu
rpo
se o
f g
ran
to
r ass
ista
nce
UNITED WAY OF EAST CENTRAL IOWA, INC.
42-0861239
CEDAR RA
PIDS
SYM
PHONY
119 3RD
AVEN
UE S
ECEDAR RA
PIDS
, IA
52401
42-0
7725
44501(C)(3)
21,000.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
CEDAR VA
LLEY
HAB
ITAT F
OR H
UMAN
ITY
PO BOX 1
244
CEDAR RA
PIDS
, IA
52406
-124
442
-132
0296
501(C)(3)
7,890.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
COE COLL
EGE
FOUN
DATION
1220 FIR
ST A
VENU
E NE
CEDAR RA
PIDS
, IA
52402
42-0
6864
67501(C)(3)
8,776.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
COMMUNIT
Y CO
RREC
TIONS
IMPR
OVEM
ENT
ASSOCIAT
ION
- 95
1 29TH
AVE
NUE
SW -
CEDAR RA
PIDS
, IA
52404
42-1
3823
41501(C)(3)
275,000.
0.N/A
N/A
PROGRAM FUNDING:EDUCATION
COMMUNIT
Y HE
ALTH
FREE
CLIN
IC947 14TH
AVE
NUE
SECEDAR RA
PIDS
, IA
52403
13-4
2280
71501(C)(3)
106,278.
0.N/A
N/A
PROGRAM FUNDING:HEALTH
COMMUNIT
Y HE
ALTH
FREE
CLIN
IC947 14TH
AVE
NUE
SECEDAR RA
PIDS
, IA
52403
13-4
2280
71501(C)(3)
11,708.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
CORNELL
COLL
EGE
FOUNDA
TION
, C/
OMIKE KRA
GENB
RINK
- 600
FIR
STSTREET N
. -
MOUN
TVERNO
N, I
A 52
314
42-0
6803
35501(C)(3)
5,000.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
DENTAL H
EALT
H CE
NTER
1026 A A
VENU
E NE
CEDAR RA
PIDS
, IA
52402
42-1
1068
19501(C)(3)
75,000.
0.N/A
N/A
PROGRAM FUNDING:HEALTH
FAMILIES
, IN
C.PO BOX 1
30WEST BRA
NCH,
IA
52358
42-1
0232
08501(C)(3)
30,000.
0.N/A
N/A
PROGRAM FUNDING:HEALTH

23
22
41
05
-01
-12
Pa
rt I
IC
on
tin
ua
tio
n o
f G
ran
ts a
nd
Oth
er
Assis
tan
ce
to
Go
vern
me
nts
an
d O
rga
niz
ati
on
s in
th
e U
nit
ed
Sta
tes
(a)
(b)
(c)
(d)
(e)
(f)
(g)
(h)
Sc
he
du
le I
(F
orm
99
0)
Sch
ed
ule
I (F
orm
99
0)
Pag
e 1
(Sch
ed
ule
I (F
orm
99
0), P
art
II.)
Nam
e a
nd
ad
dre
ss o
f o
rgan
izatio
n o
r g
ove
rnm
en
t E
IN IR
C s
ectio
nif
ap
plic
ab
le A
mo
un
t o
f cash
gra
nt
Am
ou
nt
of
no
n-c
ash
ass
ista
nce
Meth
od
of
valu
atio
n
(bo
ok,
FM
V,
ap
pra
isal,
oth
er)
Desc
rip
tio
n o
fn
on
-cash
ass
ista
nce
Pu
rpo
se o
f g
ran
to
r ass
ista
nce
UNITED WAY OF EAST CENTRAL IOWA, INC.
42-0861239
FCFH-IOW
A, I
NC.
CASH: INITIATIVE FUND,
317 7TH
AVEN
UE S
E SUIT
E 40
1FAIR MARKET
ADMINISTRATIVE
NONCASH: TO ASSIST WITH
CEDAR RA
PIDS
, IA
52401
20-0
9369
54501(C)(3)
305,000.
16,960.VALUE
SERVICES
ADMINISTRATIVE COSTS
FIRST LU
THER
AN C
HURCH
1000 THI
RD A
VENU
E SE
CEDAR RA
PIDS
, IA
52403
39-1
8972
87501(C)(3)
7,391.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
FOUNDATI
ON 2
, IN
C.1714 JOH
NSON
AVE
NUE NW
CEDAR RA
PIDS
, IA
52405
42-1
0784
44501(C)(3)
570,762.
0.N/A
N/A
PROGRAM FUNDING:HEALTH
FOUR OAK
S FA
MILY
AND C
HILD
REN
SERVICES
- 5
400
KIRKWO
OD B
OULE
VARD
SW - CED
AR R
APID
S, IA
5240
442
-099
8726
501(C)(3)
9,835.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
GIRL SCO
UTS
OF E
ASTERN
IOW
A &
317 7T
H AV
ENUE
SE,
STE
201
CEDAR RA
PIDS
, IA
52401
-160
442
-100
8848
501(C)(3)
11,311.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
GIRL SCO
UTS
OF E
ASTERN
IOW
A &
WESTERN
ILLI
NOIS
- 317
7TH
AVE
NUE
SE, SUIT
E 20
1 -
CEDAR
RAPI
DS,
IA52401-16
0442
-100
8848
501(C)(3)
55,000.
0.N/A
N/A
PROGRAM FUNDING:EDUCATION
GOODWILL
IND
USTR
IES OF
THE
HEARTLAN
D -
1410
SOUTH
FIR
ST A
VE.
- IOWA C
ITY,
IA
52244
42-0
9235
63501(C)(3)
136,850.
0.N/A
N/A
PROGRAM FUNDING:INCOME
GOODWILL
OF
THE
HEARTL
AND
1410 SOU
TH F
IRST
AVE.
IOWACITY
, IA
522
4442
-092
3563
501(C)(3)
5,695.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
HAWKEYE
AREA
COM
MUNITY
ACT
ION
PROGRAM
- P.
O. B
OX 490
- H
IAWA
THA,
IA 52233
-049
042
-089
8405
501(C)(3)
574,000.
0.N/A
N/A
PROGRAM FUNDING:EDUCATION

23
22
41
05
-01
-12
Pa
rt I
IC
on
tin
ua
tio
n o
f G
ran
ts a
nd
Oth
er
Assis
tan
ce
to
Go
vern
me
nts
an
d O
rga
niz
ati
on
s in
th
e U
nit
ed
Sta
tes
(a)
(b)
(c)
(d)
(e)
(f)
(g)
(h)
Sc
he
du
le I
(F
orm
99
0)
Sch
ed
ule
I (F
orm
99
0)
Pag
e 1
(Sch
ed
ule
I (F
orm
99
0), P
art
II.)
Nam
e a
nd
ad
dre
ss o
f o
rgan
izatio
n o
r g
ove
rnm
en
t E
IN IR
C s
ectio
nif
ap
plic
ab
le A
mo
un
t o
f cash
gra
nt
Am
ou
nt
of
no
n-c
ash
ass
ista
nce
Meth
od
of
valu
atio
n
(bo
ok,
FM
V,
ap
pra
isal,
oth
er)
Desc
rip
tio
n o
fn
on
-cash
ass
ista
nce
Pu
rpo
se o
f g
ran
to
r ass
ista
nce
UNITED WAY OF EAST CENTRAL IOWA, INC.
42-0861239
HAWKEYE
AREA
COM
MUNITY
ACT
ION
PROGRAM
- P.
O. B
OX 490
- H
IAWA
THA,
IA 52233
-049
042
-089
8405
501(C)(3)
5,498.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
HEARTLAN
D VI
NEYA
RD CHR
ISTI
ANFELLOWSH
IP -
140
5 GREE
NHIL
L RO
AD -
CEDARFAL
LS,
IA 5
0613
42-1
3210
06501(C)(3)
16,450.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
HILLSIDE
WES
LEYA
N CHUR
CH2600 FIR
ST A
VENU
E NW
CEDAR RA
PIDS
, IA
52405
42-1
1119
74501(C)(3)
8,150.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
HORIZONS
, A
FAMI
LY SER
VICE
ALLIANCE
- P
O BO
X 667
- CE
DAR
RAPIDS,
IA 5
2406
42-1
1350
83501(C)(3)
746,883.
0.N/A
N/A
PROGRAM FUNDING:HEALTH
HORIZONS
, A
FAMI
LY SER
VICE
ALLIANCE
- P
O BO
X 667
- CE
DAR
RAPIDS,
IA 5
2406
42-1
1350
83501(C)(3)
16,386.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
HUMAN SE
RVIC
ES C
AMPUS
OF E
AST
CENTRAL
IOWA
- 3
17 7TH
AVE
NUE
SEFAIR MAR
KET
ADMINISTRATIVE
TO ASSIST WITH
SUITE 40
1 -
CEDA
R RAPI
DS,
IA 5
2401
27-0
4873
31501(C)(3)
0.37,419.VALUE
SERVICES
ADMINISTRATIVE COSTS
INDIAN C
REEK
NAT
URE CE
NTER
6665 OTI
S RO
AD S
ECEDAR RA
PIDS
, IA
52403
23-7
2601
97501(C)(3)
7,751.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
IOWA CIT
Y CO
MMUN
ITY CH
URCH
717 KIMB
ALL
AVE
IOWACITY
, IA
522
4531
-162
7188
501(C)(3)
5,400.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
IOWA LEG
AL A
ID317 7TH
AVEN
UE S
E, SUI
TE 4
04CEDAR RA
PIDS
, IA
52401
42-1
0792
27501(C)(3)
185,000.
0.N/A
N/A
PROGRAM FUNDING:INCOME

23
22
41
05
-01
-12
Pa
rt I
IC
on
tin
ua
tio
n o
f G
ran
ts a
nd
Oth
er
Assis
tan
ce
to
Go
vern
me
nts
an
d O
rga
niz
ati
on
s in
th
e U
nit
ed
Sta
tes
(a)
(b)
(c)
(d)
(e)
(f)
(g)
(h)
Sc
he
du
le I
(F
orm
99
0)
Sch
ed
ule
I (F
orm
99
0)
Pag
e 1
(Sch
ed
ule
I (F
orm
99
0), P
art
II.)
Nam
e a
nd
ad
dre
ss o
f o
rgan
izatio
n o
r g
ove
rnm
en
t E
IN IR
C s
ectio
nif
ap
plic
ab
le A
mo
un
t o
f cash
gra
nt
Am
ou
nt
of
no
n-c
ash
ass
ista
nce
Meth
od
of
valu
atio
n
(bo
ok,
FM
V,
ap
pra
isal,
oth
er)
Desc
rip
tio
n o
fn
on
-cash
ass
ista
nce
Pu
rpo
se o
f g
ran
to
r ass
ista
nce
UNITED WAY OF EAST CENTRAL IOWA, INC.
42-0861239
IOWA STA
TE U
NIVE
RSITY
EXTE
NSIO
N3279 7TH
AVE
NUE
MARION,
IA 5
2302
42-6
0214
46170(B)(1)(A)(V)
83,908.
0.N/A
N/A
PROGRAM FUNDING:EDUCATION
JANE BOY
D CO
MMUN
ITY HO
USE
943 14TH
AVE
NUE
SECEDAR RA
PIDS
, IA
52403
42-0
6803
59501(C)(3)
335,000.
0.N/A
N/A
PROGRAM FUNDING:EDUCATION
JANE BOY
D CO
MMUN
ITY HO
USE
943 14TH
AVE
NUE
SECEDAR RA
PIDS
, IA
52403
42-0
6803
59501(C)(3)
5,062.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
JUNIOR A
CHIE
VEME
NT OF
EAST
CEN
TRAL
IOWA - 3
24 T
HIRD
ST SE
#20
0 -
CEDAR RA
PIDS
, IA
52401
-184
142
-091
9209
501(C)(3)
11,638.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
JUVENILE
DIA
BETE
S RESE
ARCH
FOUNDATI
ON -
10
26 A A
VENU
E NE
,PO BOX 3
026
- CE
DAR RA
PIDS
, IA
52406
23-1
9077
29501(C)(3)
5,124.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
KIDS FIR
ST L
AW C
ENTER
420 6TH
STRE
ET S
E, SUI
TE 1
60CEDAR RA
PIDS
, IA
52401
20-2
1996
49501(C)(3)
63,000.
0.N/A
N/A
PROGRAM FUNDING:EDUCATION
KIDS FIR
ST L
AW C
ENTER
420 6T
H ST
REET
SE,
STE
160
CEDAR RA
PIDS
, IA
52401
20-2
1996
49501(C)(3)
11,048.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
KIRKWOOD
COM
MUNI
TY COL
LEGE
FOUNDATI
ON -
630
1 KIRK
WOOD
BLV
D SW
- CEDAR
RAPI
DS,
IA 524
0523
-707
6632
501(C)(3)
32,500.
0.N/A
N/A
PROGRAM FUNDING:INCOME
KIRKWOOD
COM
MUNI
TY COL
LEGE
FOUNDATI
ON -
PO
BOX 20
68 -
CED
ARRAPIDS,
IA 5
2406
23-7
0766
32501(C)(3)
32,500.
0.N/A
N/A
PROGRAM FUNDING:EDUCATION

23
22
41
05
-01
-12
Pa
rt I
IC
on
tin
ua
tio
n o
f G
ran
ts a
nd
Oth
er
Assis
tan
ce
to
Go
vern
me
nts
an
d O
rga
niz
ati
on
s in
th
e U
nit
ed
Sta
tes
(a)
(b)
(c)
(d)
(e)
(f)
(g)
(h)
Sc
he
du
le I
(F
orm
99
0)
Sch
ed
ule
I (F
orm
99
0)
Pag
e 1
(Sch
ed
ule
I (F
orm
99
0), P
art
II.)
Nam
e a
nd
ad
dre
ss o
f o
rgan
izatio
n o
r g
ove
rnm
en
t E
IN IR
C s
ectio
nif
ap
plic
ab
le A
mo
un
t o
f cash
gra
nt
Am
ou
nt
of
no
n-c
ash
ass
ista
nce
Meth
od
of
valu
atio
n
(bo
ok,
FM
V,
ap
pra
isal,
oth
er)
Desc
rip
tio
n o
fn
on
-cash
ass
ista
nce
Pu
rpo
se o
f g
ran
to
r ass
ista
nce
UNITED WAY OF EAST CENTRAL IOWA, INC.
42-0861239
KIRKWOOD
COM
MUNI
TY COL
LEGE
FOUNDATI
ON -
PO
BOX 20
68 -
CED
ARRAPIDS,
IA 5
2406
23-7
0766
32501(C)(3)
6,725.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
LINN COM
MUNI
TY C
ARE
1201 3RD
AVE
NUE
SECEDAR RA
PIDS
, IA
52403
20-2
4055
75501(C)(3)
6,500.
0.N/A
N/A
PROGRAM FUNDING:HEALTH
LINN MAR
SCH
OOL
FOUNDA
TION
2999 NOR
TH 1
0TH
STREET
MARION,
IA 5
2302
42-1
2671
25501(C)(3)
9,519.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
MECCA SE
RVIC
ES430 SOUT
HGAT
EIOWA CIT
Y, I
A 52
240
42-0
9460
31501(C)(3)
45,000.
0.N/A
N/A
PROGRAM FUNDING:HEALTH
MERCY ME
DICA
L CE
NTER F
OUND
ATIO
N701 10TH
STR
EET
SECEDAR RA
PIDS
, IA
52403
-125
151
-023
3180
501(C)(3)
10,970.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
MOUNT ME
RCY
UNIV
ERSITY
1330 ELM
HURS
T DR
IVE NE
CEDAR RA
PIDS
, IA
52402
42-0
6810
46501(C)(3)
8,000.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
NEIGHBOR
HOOD
TRA
NSPORT
ATIO
NSERVICE,
INC
-
PO BOX
81
- CE
DAR
RAPIDS,
IA 5
2406
-0081
26-1
3062
53501(C)(3)
127,250.
0.N/A
N/A
PROGRAM FUNDING:INCOME
RAPE VIC
TIM
ADVO
CACY P
ROGR
AM332 S. L
INN
ST,
SUITE
100
IOWA CIT
Y, I
A 52
240
42-6
0048
13501(C)(3)
32,000.
0.N/A
N/A
PROGRAM FUNDING:EDUCATION
RURAL EM
PLOY
MENT
ALTER
NATI
VES
P.O. BOX
24
CONROY,
IA 5
2220
-0024
42-1
1500
11501(C)(3)
35,000.
0.N/A
N/A
PROGRAM FUNDING:INCOME

23
22
41
05
-01
-12
Pa
rt I
IC
on
tin
ua
tio
n o
f G
ran
ts a
nd
Oth
er
Assis
tan
ce
to
Go
vern
me
nts
an
d O
rga
niz
ati
on
s in
th
e U
nit
ed
Sta
tes
(a)
(b)
(c)
(d)
(e)
(f)
(g)
(h)
Sc
he
du
le I
(F
orm
99
0)
Sch
ed
ule
I (F
orm
99
0)
Pag
e 1
(Sch
ed
ule
I (F
orm
99
0), P
art
II.)
Nam
e a
nd
ad
dre
ss o
f o
rgan
izatio
n o
r g
ove
rnm
en
t E
IN IR
C s
ectio
nif
ap
plic
ab
le A
mo
un
t o
f cash
gra
nt
Am
ou
nt
of
no
n-c
ash
ass
ista
nce
Meth
od
of
valu
atio
n
(bo
ok,
FM
V,
ap
pra
isal,
oth
er)
Desc
rip
tio
n o
fn
on
-cash
ass
ista
nce
Pu
rpo
se o
f g
ran
to
r ass
ista
nce
UNITED WAY OF EAST CENTRAL IOWA, INC.
42-0861239
SOUTHEAS
T LI
NN C
OMMUNI
TY C
ENTE
R108 SOUT
H WA
SHIN
GTON
LISBON,
IA 5
2253
43-1
4063
17501(C)(3)
15,450.
0.N/A
N/A
PROGRAM FUNDING:HEALTH
SOUTHEAS
T LI
NN C
OMMUNI
TY C
ENTE
R108 SOUT
H WA
SHIN
GTON
LISBON,
IA 5
2253
43-1
4063
17501(C)(3)
6,025.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
ST. ELIZ
ABET
H AN
N SETO
N CA
THLO
ICCHURCH -
135
0 LY
NDHURS
T DR
IVE
-HIAWATHA
, IA
522
3342
-133
8119
501(C)(3)
7,704.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
ST. JOSE
PH C
ATHO
LIC CH
URCH
-MARION -
179
0 14
TH ST
- MA
RION
, IA
52302
42-0
7825
34501(C)(3)
5,000.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
ST. LUKE
'S H
EALT
H CARE
FOU
NDAT
ION
855 A AV
ENUE
NE
#105
CEDAR RA
PIDS
, IA
52402
42-1
1068
19501(C)(3)
13,047.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
ST. MARY
'S C
ATHO
LIC CH
URCH
-SOLON, I
A -
174
9 RACI
NE A
VENU
E NE
- SOLON,
IA
5233
342
-080
5379
501(C)(3)
6,703.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
ST. MATT
HEWS
CAT
HOLIC
CHUR
CH2310 FIR
ST A
VENU
E NE
CEDAR RA
PIDS
, IA
52402
42-0
7303
42501(C)(3)
7,507.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
ST. PIUS
X C
ATHO
LIC CH
URCH
4949 COU
NCIL
STR
EET NE
CEDAR RA
PIDS
, IA
52402
42-0
8595
72501(C)(3)
8,390.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
STONEBRI
DGE
CHUR
CH1829 STO
NEY
POIN
T RD S
WCEDAR RA
PIDS
, IA
52404
42-1
1139
23501(C)(3)
14,130.
0.N/A
N/A
DONOR DESIGNATION SUPPORT

23
22
41
05
-01
-12
Pa
rt I
IC
on
tin
ua
tio
n o
f G
ran
ts a
nd
Oth
er
Assis
tan
ce
to
Go
vern
me
nts
an
d O
rga
niz
ati
on
s in
th
e U
nit
ed
Sta
tes
(a)
(b)
(c)
(d)
(e)
(f)
(g)
(h)
Sc
he
du
le I
(F
orm
99
0)
Sch
ed
ule
I (F
orm
99
0)
Pag
e 1
(Sch
ed
ule
I (F
orm
99
0), P
art
II.)
Nam
e a
nd
ad
dre
ss o
f o
rgan
izatio
n o
r g
ove
rnm
en
t E
IN IR
C s
ectio
nif
ap
plic
ab
le A
mo
un
t o
f cash
gra
nt
Am
ou
nt
of
no
n-c
ash
ass
ista
nce
Meth
od
of
valu
atio
n
(bo
ok,
FM
V,
ap
pra
isal,
oth
er)
Desc
rip
tio
n o
fn
on
-cash
ass
ista
nce
Pu
rpo
se o
f g
ran
to
r ass
ista
nce
UNITED WAY OF EAST CENTRAL IOWA, INC.
42-0861239
THE ARC
OF E
AST
CENTRA
L IO
WA680 2ND
ST S
E SU
ITE 20
0CEDAR RA
PIDS
, IA
52401
42-0
8053
77501(C)(3)
200,000.
0.N/A
N/A
PROGRAM FUNDING:INCOME
THE ARC
OF E
AST
CENTRA
L IO
WA680 2ND
ST S
E SU
ITE 20
0CEDAR RA
PIDS
, IA
52401
42-0
8053
77501(C)(3)
40,446.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
THE SAFE
PLA
CE F
OUNDAT
ION
527 SIXT
H AV
ENUE
SE
CEDAR RA
PIDS
, IA
52401
42-1
3484
41501(C)(3)
68,250.
0.N/A
N/A
PROGRAM FUNDING:INCOME
THE SALV
ATIO
N AR
MY1000 C A
VENU
E NW
CEDAR RA
PIDS
, IA
52405
36-2
1679
10501(C)(3)
158,000.
0.N/A
N/A
PROGRAM FUNDING:INCOME
THE SALV
ATIO
N AR
MY1000 C A
VENU
E NW
CEDAR RA
PIDS
, IA
52405
36-2
1679
10501(C)(3)
18,321.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
THEATRE
CEDA
R RA
PIDS
102 THIR
D ST
REET
SE
CEDAR RA
PIDS
, IA
52401
42-0
8909
13501(C)(3)
8,331.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
UNITED W
AY O
F JO
HNSON
COUN
TY,
INC.
1150 5
TH S
T, S
TE 2
90CORALVIL
LE,
IA 5
2241-2
933
42-6
0620
55501(C)(3)
18,033.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
UNITED W
AY O
F TR
ANSYLV
ANIA
COU
NTY
PO BOX 5
3BREVARD,
NC
2871
2-0053
23-7
1450
22501(C)(3)
6,200.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
VISITING
NUR
SE A
SSOCIA
TION
600 BOYS
ON R
OAD
NE, SU
ITE
2CEDAR RA
PIDS
, IA
52402
42-0
6804
91501(C)(3)
57,000.
0.N/A
N/A
PROGRAM FUNDING:HEALTH

23
22
41
05
-01
-12
Pa
rt I
IC
on
tin
ua
tio
n o
f G
ran
ts a
nd
Oth
er
Assis
tan
ce
to
Go
vern
me
nts
an
d O
rga
niz
ati
on
s in
th
e U
nit
ed
Sta
tes
(a)
(b)
(c)
(d)
(e)
(f)
(g)
(h)
Sc
he
du
le I
(F
orm
99
0)
Sch
ed
ule
I (F
orm
99
0)
Pag
e 1
(Sch
ed
ule
I (F
orm
99
0), P
art
II.)
Nam
e a
nd
ad
dre
ss o
f o
rgan
izatio
n o
r g
ove
rnm
en
t E
IN IR
C s
ectio
nif
ap
plic
ab
le A
mo
un
t o
f cash
gra
nt
Am
ou
nt
of
no
n-c
ash
ass
ista
nce
Meth
od
of
valu
atio
n
(bo
ok,
FM
V,
ap
pra
isal,
oth
er)
Desc
rip
tio
n o
fn
on
-cash
ass
ista
nce
Pu
rpo
se o
f g
ran
to
r ass
ista
nce
UNITED WAY OF EAST CENTRAL IOWA, INC.
42-0861239
VOLUNTEE
R SE
RVIC
ES OF
CEDA
R CO
UNTY
PO BOX 3
07TIPTON,
IA 5
2772
42-1
3416
50501(C)(3)
16,046.
0.N/A
N/A
PROGRAM FUNDING:HEALTH
WAYPOINT
SER
VICE
S318 5TH
ST S
ECEDAR RA
PIDS
, IA
52401
42-0
6803
07501(C)(3)
47,035.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
WAYPOINT
SER
VICE
S FOR
WOME
NCHILDREN
& F
AMIL
IES -
318
5TH
STSE - CED
AR R
APID
S, IA
5240
142
-068
0307
501(C)(3)
521,952.
0.N/A
N/A
PROGRAM FUNDING:INCOME
WILLIS D
ADY
EMER
GENCY
SHEL
TER
1247 FOU
RTH
AVEN
UE SE
CEDAR RA
PIDS
, IA
52403
42-1
3116
68501(C)(3)
115,000.
0.N/A
N/A
PROGRAM FUNDING:INCOME
WILLIS D
ADY
EMER
GENCY
SHEL
TER
1247 FOU
RTH
AVEN
UE SE
CEDAR RA
PIDS
, IA
52403
42-1
3116
68501(C)(3)
9,134.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
WITWER C
ENTE
R605 SECO
ND A
VE S
ECEDAR RA
PIDS
, IA
52401
42-1
1531
56501(C)(3)
100,000.
0.N/A
N/A
PROGRAM FUNDING:HEALTH
XAVIER F
OUND
ATIO
NPO BOX 1
0956
CEDAR RA
PIDS
, IA
52410
42-1
4792
38501(C)(3)
17,866.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
YMCA OF
THE
CEDA
R RAPI
DSMETROPOL
ITAN
- 2
07 SEV
ENTH
AVE
NUE
SE - CED
AR R
APID
S, IA
5240
142
-068
0306
501(C)(3)
12,267.
0.N/A
N/A
DONOR DESIGNATION SUPPORT
YMCA OF
THE
CEDA
R RAPI
DSMETROPOL
ITAN
ARE
A - 20
7 SE
VENT
HAVENUE S
E -
CEDA
R RAPI
DS,
IA 5
2401
42-0
6803
06501(C)(3)
145,000.
0.N/A
N/A
PROGRAM FUNDING:EDUCATION

23
22
41
05
-01
-12
Pa
rt I
IC
on
tin
ua
tio
n o
f G
ran
ts a
nd
Oth
er
Assis
tan
ce
to
Go
vern
me
nts
an
d O
rga
niz
ati
on
s in
th
e U
nit
ed
Sta
tes
(a)
(b)
(c)
(d)
(e)
(f)
(g)
(h)
Sc
he
du
le I
(F
orm
99
0)
Sch
ed
ule
I (F
orm
99
0)
Pag
e 1
(Sch
ed
ule
I (F
orm
99
0), P
art
II.)
Nam
e a
nd
ad
dre
ss o
f o
rgan
izatio
n o
r g
ove
rnm
en
t E
IN IR
C s
ectio
nif
ap
plic
ab
le A
mo
un
t o
f cash
gra
nt
Am
ou
nt
of
no
n-c
ash
ass
ista
nce
Meth
od
of
valu
atio
n
(bo
ok,
FM
V,
ap
pra
isal,
oth
er)
Desc
rip
tio
n o
fn
on
-cash
ass
ista
nce
Pu
rpo
se o
f g
ran
to
r ass
ista
nce
UNITED WAY OF EAST CENTRAL IOWA, INC.
42-0861239
YOUNG PA
RENT
S NE
TWORK
420 6TH
STRE
ET S
E SUIT
E 26
0CEDAR RA
PIDS
, IA
52401
42-1
3554
80501(C)(3)
297,000.
0.N/A
N/A
PROGRAM FUNDING:EDUCATION
YOUNG PA
RENT
S NE
TWORK
420 6TH
STRE
ET S
E SUIT
E 26
0CEDAR RA
PIDS
, IA
52401
42-1
3554
80501(C)(3)
21,399.
0.N/A
N/A
DONOR DESIGNATION SUPPORT

23
21
02
1
2-1
8-1
2
2P
art
III
Gra
nts
an
d O
the
r A
ssis
tan
ce
to
In
div
idu
als
in
th
e U
nit
ed
Sta
tes.
(e)
(a)
(b)
(c)
(d)
(f)
Pa
rt I
VS
up
ple
me
nta
l In
form
ati
on
.
Sc
he
du
le I
(F
orm
99
0)
(20
12
)
Sch
ed
ule
I (F
orm
99
0) (2
01
2)
Pag
e
Co
mp
lete
if t
he o
rgan
izatio
n a
nsw
ere
d "
Yes"
to
Fo
rm 9
90
, P
art
IV
, lin
e 2
2.
Part
III c
an
be d
up
licate
d if
ad
ditio
nal s
pace is
need
ed
.
Meth
od
of
valu
atio
n(b
oo
k, F
MV
, ap
pra
isal,
oth
er)
Typ
e o
f g
ran
t o
r ass
ista
nce
Nu
mb
er
of
recip
ien
tsA
mo
un
t o
fcash
gra
nt
Am
ou
nt
of
no
n-
cash
ass
ista
nce
Desc
rip
tio
n o
f n
on
-cash
ass
ista
nce
Co
mp
lete
th
is p
art
to
pro
vid
e t
he in
form
atio
n r
eq
uired
in P
art
I, lin
e 2
, P
art
III, co
lum
n (b
), a
nd
an
y o
ther
ad
ditio
nal i
nfo
rmatio
n.
UNITED WAY OF EAST CENTRAL IOWA, INC.
42-0861239
SCHEDULE I, PART I, LINE 2: PROGRAM FUNDING: PARTNER AGENCIES ARE REQUIRED
TO SUBMIT WRITTEN MID-YEAR AND END-OF-YEAR REPORTS WHERE THEY DESCRIBE
THEIR PROGRESS TOWARDS THE OUTCOME GOALS THEY COMMITTED TO UPON RECIEPT OF
FUNDING. AGENCIES REPORT NUMBER SERVED, ACTIVITIES AND OUTCOMES FOR THE
TARGET POPULATION (I.E., NUMBER WHO EXPERIENCED A MEASURED CHANGE IN
CONDITION DURING THE FUNDING PERIOD.) AGENCIES ALSO SUBMIT FINANCIAL
STATEMENTS AND IRS FORM 990 DOCUMENTS THAT ARE REVIEWED BY VOLUNTEER TEAMS
DURING EACH FUNDED PERIOD.

23229105-01-12
2
Schedule I (Form 990)
Schedule I (Form 990) Page
Part IV Supplemental Information
UNITED WAY OF EAST CENTRAL IOWA, INC. 42-0861239
DONOR DESIGNATIONS SUPPORT: 501(C)(3) TAX DETERMINATION LETTERS AND
ANTI-TERRORISM COMPLIANCE (PATRIOT ACT) FORMS ARE REQUIRED FOR ALL AGENCIES
BEFORE PAYOUT IS ISSUED. IRS WATCH LIST WEBSITES ARE REVIEWED TO VERIFY
AGENCY IS NOT INVOLVED IN OR SUPPORTIVE OF TERROIST ACTIVITY.
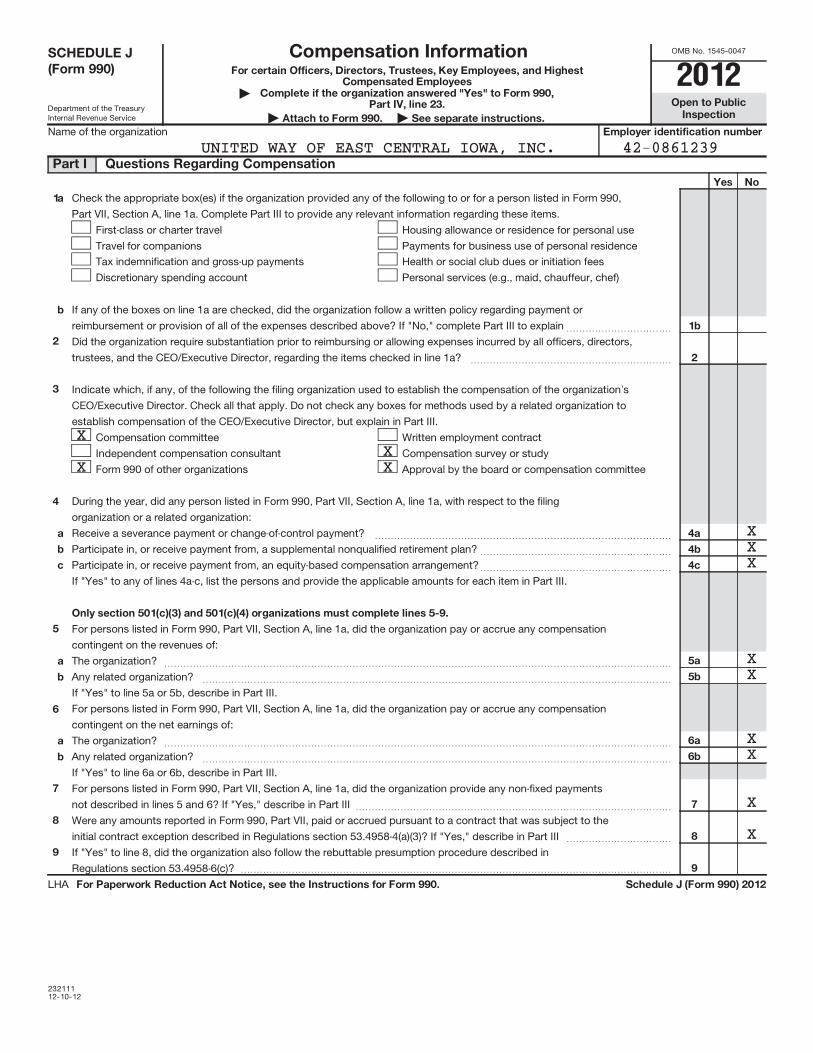
OMB No. 1545-0047
Department of the TreasuryInternal Revenue Service
23211112-10-12
For certain Officers, Directors, Trustees, Key Employees, and HighestCompensated Employees
Complete if the organization answered "Yes" to Form 990,Part IV, line 23. Open to Public
InspectionAttach to Form 990. See separate instructions.Employer identification number
Yes No
1a
b
1b
2
2
3
4
a
b
c
4a
4b
4c
Only section 501(c)(3) and 501(c)(4) organizations must complete lines 5-9.
5
5a
5b
6a
6b
7
8
9
a
b
6
a
b
7
8
9
For Paperwork Reduction Act Notice, see the Instructions for Form 990. Schedule J (Form 990) 2012
|
| |Name of the organization
Check the appropriate box(es) if the organization provided any of the following to or for a person listed in Form 990,
Part VII, Section A, line 1a. Complete Part III to provide any relevant information regarding these items.
First-class or charter travel
Travel for companions
Housing allowance or residence for personal use
Payments for business use of personal residence
Tax indemnification and gross-up payments
Discretionary spending account
Health or social club dues or initiation fees
Personal services (e.g., maid, chauffeur, chef)
If any of the boxes on line 1a are checked, did the organization follow a written policy regarding payment or
reimbursement or provision of all of the expenses described above? If "No," complete Part III to explain~~~~~~~~~~~
Did the organization require substantiation prior to reimbursing or allowing expenses incurred by all officers, directors,
trustees, and the CEO/Executive Director, regarding the items checked in line 1a? ~~~~~~~~~~~~~~~~~~~~~
Indicate which, if any, of the following the filing organization used to establish the compensation of the organization's
CEO/Executive Director. Check all that apply. Do not check any boxes for methods used by a related organization to
establish compensation of the CEO/Executive Director, but explain in Part III.
Compensation committee
Independent compensation consultant
Form 990 of other organizations
Written employment contract
Compensation survey or study
Approval by the board or compensation committee
During the year, did any person listed in Form 990, Part VII, Section A, line 1a, with respect to the filing
organization or a related organization:
Receive a severance payment or change-of-control payment?
Participate in, or receive payment from, a supplemental nonqualified retirement plan?
Participate in, or receive payment from, an equity-based compensation arrangement?
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~
If "Yes" to any of lines 4a-c, list the persons and provide the applicable amounts for each item in Part III.
For persons listed in Form 990, Part VII, Section A, line 1a, did the organization pay or accrue any compensation
contingent on the revenues of:
The organization?
Any related organization?
If "Yes" to line 5a or 5b, describe in Part III.
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
For persons listed in Form 990, Part VII, Section A, line 1a, did the organization pay or accrue any compensation
contingent on the net earnings of:
The organization?
Any related organization?
If "Yes" to line 6a or 6b, describe in Part III.
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
For persons listed in Form 990, Part VII, Section A, line 1a, did the organization provide any non-fixed payments
not described in lines 5 and 6? If "Yes," describe in Part III
Were any amounts reported in Form 990, Part VII, paid or accrued pursuant to a contract that was subject to the
initial contract exception described in Regulations section 53.4958-4(a)(3)? If "Yes," describe in Part III
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
~~~~~~~~~~~
If "Yes" to line 8, did the organization also follow the rebuttable presumption procedure described in
Regulations section 53.4958-6(c)? ���������������������������������������������
LHA
SCHEDULE J(Form 990)
Part I Questions Regarding Compensation
Compensation Information
2012
UNITED WAY OF EAST CENTRAL IOWA, INC. 42-0861239
XX
X X
XXX
XX
XX
X
X

23
21
12
12
-12
-12
2
Pa
rt I
IO
ffic
ers
, D
ire
cto
rs, T
ruste
es, K
ey
Em
plo
yee
s, a
nd
Hig
he
st
Co
mp
en
sa
ted
Em
plo
yee
s.
No
te.
(B)
(C)
(D
)
(E)
(F
)
(i)
(ii)
(i
ii)
(A)
(i)
(ii) (i)
(ii) (i)
(ii) (i)
(ii) (i)
(ii) (i)
(ii) (i)
(ii) (i)
(ii) (i)
(ii) (i)
(ii) (i)
(ii) (i)
(ii) (i)
(ii) (i)
(ii) (i)
(ii) (i)
(ii)
Sc
he
du
le J
(F
orm
99
0)
20
12
Sch
ed
ule
J (F
orm
99
0) 2
01
2P
ag
e
Use
du
plic
ate
co
pie
s if
ad
ditio
nal s
pace is
need
ed
.
Fo
r each
ind
ivid
ual w
ho
se c
om
pen
satio
n m
ust
be r
ep
ort
ed
in S
ch
ed
ule
J, re
po
rt c
om
pen
satio
n f
rom
th
e o
rgan
izatio
n o
n r
ow
(i)
an
d f
rom
rela
ted
org
an
izatio
ns,
desc
rib
ed
in t
he in
stru
ctio
ns,
on
ro
w (ii)
.D
o n
ot
list
an
y in
div
idu
als
th
at
are
no
t lis
ted
on
Fo
rm 9
90
, P
art
VII.
Th
e s
um
of
co
lum
ns
(B)(i)-
(iii)
for
each
list
ed
ind
ivid
ual m
ust
eq
ual t
he t
ota
l am
ou
nt
of
Fo
rm 9
90
, P
art
VII, S
ectio
n A
, lin
e 1
a, ap
plic
ab
le c
olu
mn
(D
) an
d (E
) am
ou
nts
fo
r th
at
ind
ivid
ual.
Bre
akd
ow
n o
f W
-2 a
nd
/or
10
99
-MIS
C c
om
pen
satio
nR
etire
men
t an
do
ther
defe
rred
co
mp
en
satio
n
No
nta
xab
leb
en
efit
sT
ota
l of
co
lum
ns
(B)(i)-
(D)
Co
mp
en
satio
nre
po
rted
as
defe
rred
in p
rio
r F
orm
99
0B
ase
co
mp
en
satio
nB
on
us
&in
cen
tive
co
mp
en
satio
n
Oth
er
rep
ort
ab
leco
mp
en
satio
n
Nam
e a
nd
Title
UNITED WAY OF EAST CENTRAL IOWA, INC.
42-0861239
(1) LOI
S BU
NTZ
129,538.
0.
0.
10,400.
11,329.
151,267.
0.
PRESIDEN
T/CE
O0.
0.
0.
0.
0.
0.
0.

OMB No. 1545-0047
Department of the TreasuryInternal Revenue Service
23214112-20-12
Complete if the organizations answered "Yes" on Form
990, Part IV, lines 29 or 30. Open to PublicInspectionAttach to Form 990.
Employer identification number
(a) (b) (c) (d)
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
29
Yes No
30
31
32
33
a
b
30a
31
32a
a
b
For Paperwork Reduction Act Notice, see the Instructions for Form 990. Schedule M (Form 990) (2012)
Name of the organization
Check ifapplicable
Number ofcontributions or
items contributed
Noncash contributionamounts reported on
Form 990, Part VIII, line 1g
Method of determiningnoncash contribution amounts
Art - Works of art
Art - Historical treasures
Art - Fractional interests
~~~~~~~~~~~~~
~~~~~~~~~
~~~~~~~~~~
Books and publications
Clothing and household goods
~~~~~~~~~~
~~~~~~
Cars and other vehicles
Boats and planes
Intellectual property
~~~~~~~~~~
~~~~~~~~~~~~~
~~~~~~~~~~~
Securities - Publicly traded
Securities - Closely held stock
~~~~~~~~
~~~~~~~
Securities - Partnership, LLC, or
trust interests
Securities - Miscellaneous
~~~~~~~~~~~~~~
~~~~~~~~
Qualified conservation contribution -
Historic structures
Qualified conservation contribution - Other
~~~~~~~~~~~~
~
Real estate - Residential
Real estate - Commercial
Real estate - Other
~~~~~~~~~
~~~~~~~~~
~~~~~~~~~~~~
Collectibles
Food inventory
Drugs and medical supplies
Taxidermy
~~~~~~~~~~~~~~~~
~~~~~~~~~~~~~~
~~~~~~~~
~~~~~~~~~~~~~~~~
Historical artifacts
Scientific specimens
Archeological artifacts
~~~~~~~~~~~~
~~~~~~~~~~~
~~~~~~~~~~
Other ( )
Other ( )
Other ( )
Other ( )
Number of Forms 8283 received by the organization during the tax year for contributions
for which the organization completed Form 8283, Part IV, Donee Acknowledgement ~~~~
During the year, did the organization receive by contribution any property reported in Part I, lines 1-28 that it must hold for
at least three years from the date of the initial contribution, and which is not required to be used for exempt purposes for
the entire holding period? ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
If "Yes," describe the arrangement in Part II.
Does the organization have a gift acceptance policy that requires the review of any non-standard contributions? ~~~~~~
Does the organization hire or use third parties or related organizations to solicit, process, or sell noncash
contributions? ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
If "Yes," describe in Part II.
If the organization did not report an amount in column (c) for a type of property for which column (a) is checked,
describe in Part II.
LHA
SCHEDULE M(Form 990)
Part I Types of Property
Noncash Contributions2012J
J
JJJJ
UNITED WAY OF EAST CENTRAL IOWA, INC. 42-0861239
X 3 2,168. FMV
ADVERTISING X 15 69,242. FMVPRIZE ITEMS X 5 13,099. FMVLINENS X 1 120. FMV
0
X
X
X

OMB No. 1545-0047
Department of the TreasuryInternal Revenue Service
23221101-04-13
(Form 990 or 990-EZ) Complete to provide information for responses to specific questions onForm 990 or 990-EZ or to provide any additional information.
| Attach to Form 990 or 990-EZ.Open to PublicInspection
Employer identification number
For Paperwork Reduction Act Notice, see the Instructions for Form 990 or 990-EZ. Schedule O (Form 990 or 990-EZ) (2012)
Name of the organization
LHA
SCHEDULE O Supplemental Information to Form 990 or 990-EZ 2012
UNITED WAY OF EAST CENTRAL IOWA, INC. 42-0861239
FORM 990, PART I, LINE 1, DESCRIPTION OF ORGANIZATION MISSION:
WE ALL NEED FOR A GOOD LIFE: EDUCATION, INCOME, AND HEALTH. UNITED
WAY'S GOAL IS TO CREATE POSITIVE, LASTING CHANGE THAT PREVENTS PROBLEMS
FROM HAPPENING IN THE FIRST PLACE. OUR EFFORTS EDUCATE RESIDENTS ABOUT
NEEDS IN THE COMMUNITY AND INSPIRE PEOPLE TO BE GENEROUS AND CARING.
UNITED WAY INVESTS DONOR DOLLARS IN QUALITY PROGRAMS SERVING THE AREA'S
LOW-INCOME RESIDENTS AND EDUCATIONALLY AT-RISK CHILDREN. ITS COMMUNITY
GOALS ARE:
1. INCREASE THE NUMBER OF LOW-INCOME CHILDREN READY FOR SCHOOL BY 50%.
2. INCREASE THE NUMBER OF LOW-INCOME YOUTH WITH 21ST CENTURY SKILLS BY
25%.
3. INCREASE THE NUMBER OF FINANCIALLY STABLE HOUSEHOLDS BY 15%.
4. INCREASE HEALTHY CHOICES BY 10%
5. INCREASE BY 25% THE NUMBER OF OLDER ADULTS WHO ARE ABLE TO MEET
THEIR DAILY LIVING NEEDS.
FORM 990, PART III, LINE 4A, PROGRAM SERVICE ACCOMPLISHMENTS:
THEIR YOUNG CHILDREN, AGES BIRTH TO FIVE, DEVELOP THE EARLY LANGUAGE
AND LITERACY SKILLS NEEDED TO BUILD KINDERGARTEN READINESS AND
LIFE-LONG LEARNING.
IN ADDITION TO THESE INITIATIVES, UNITED WAY FUNDS PARTNER AGENCIES
THAT PROVIDE CHILDCARE, PARENT EDUCATION AND QUALITY IMPROVEMENT
SERVICES FOCUSED ON FAMILIES WITH CHILDREN UNDER FIVE AND AGENCIES WHO
SUPPORT YOUTH ENGAGEMENT, SOCIAL-EMOTIONAL SKILLS, AND ACADEMIC GROWTH
TO OLDER YOUTH.
23221201-04-13
2
Employer identification number
Schedule O (Form 990 or 990-EZ) (2012)
Schedule O (Form 990 or 990-EZ) (2012) Page
Name of the organizationUNITED WAY OF EAST CENTRAL IOWA, INC. 42-0861239
FORM 990, PART III, LINE 4B, PROGRAM SERVICE ACCOMPLISHMENTS:
2-1-1 - CONNECTING RESIDENTS TO VOLUNTEER INCOME TAX ASSISTANCE: 2-1-1
CONTINUES TO BE A CRITICAL RESOURCE TO OUR COMMUNITY, CONNECTING
RESIDENTS TO NEEDED SERVICES. 2-1-1 CONTINUES TO CONNECT INDIVIDUALS TO
FREE TAX PREPARATION SITES. ABOVE THAT, 2-1-1 SCHEDULES TAX ASSISTANCE
APPOINTMENTS FOR AARP AND VITA, EFFICIENTLY CONNECTING LOW-INCOME
FAMILIES TO A SERVICE THAT BRINGS DOLLARS BACK TO OUR COMMUNITY.
- IN 2013, VOLUNTEER TAX PREPARERS ASSISTED WITH FILING OVER 3,425 TAX
RETURNS
- IN 2013, OVER 1.5 MILLION DOLLARS WAS CLAIMED IN EARNED INCOME TAX
CREDITS
KIRKWOOD PATHWAYS FOR ACADEMIC AND CAREER EDUCATION AND EMPLOYMENT
(KPACE) IS A COMMUNITY INITIATIVE THAT STARTED IN THE FALL OF 2011. THE
PURPOSE OF THE PROGRAM IS TO HELP LOW SKILL, LOW-INCOME INDIVIDUALS
DEVELOP WORKFORCE SKILLS NEEDED BY LOCAL INDUSTRY AND THAT OFFER A WAGE
SUFFICIENT TO MEET THE INDIVIDUAL'S/FAMILY'S BASIC EXPENSES. THE CAREER
PATHWAY PROGRAM OFFERS STUDENTS A CLEAR ROAD MAP FOR BUILDING SKILLS TO
PROGRESS IN THEIR FIELD OF INTEREST. LEARNERS CAN SEE THE SEQUENCE OF
STEPS THAT INCREASES SKILLS AND IMPROVES THE LEARNER'S CAREER AND WAGE
EARNING OPPORTUNITIES. ACADEMIC AND SOCIAL SUPPORT SERVICES ARE OFFERED
TO HELP STUDENTS SUCCEED.
FORM 990, PART III, LINE 4C, PROGRAM SERVICE ACCOMPLISHMENTS:
INCREASE FACTORS THAT CONTRIBUTE TO LONG-TERM HEALTH, REDUCE CRISIS AND
TRAUMA, IMPROVE MENTAL HEALTH, AND BUILD RESILIENCY AND INCREASE SOCIAL
23221201-04-13
2
Employer identification number
Schedule O (Form 990 or 990-EZ) (2012)
Schedule O (Form 990 or 990-EZ) (2012) Page
Name of the organizationUNITED WAY OF EAST CENTRAL IOWA, INC. 42-0861239
SUPPORTS THAT IMPROVE INDEPENDENCE AND THE ABILITY TO LIVE AND FUNCTION
WITHIN THE COMMUNITY.
FORM 990, PART III, LINE 4D, OTHER PROGRAM SERVICES:
VOLUNTEER MANAGEMENT: UNITED WAY EMPLOYS A FULL-TIME COMMUNITY
VOLUNTEER COORDINATOR WHO OVERSEES WORK DONE THROUGH THE EAST CENTRAL
IOWA VOLUNTEER CENTER. WE ALSO MANAGE THE VOLUNTEER NOW WEBSITE,
CONNECTING PEOPLE ONLINE TO VOLUNTEER OPPORTUNITIES AT NONPROFIT
ORGANIZATIONS IN THE AREA. UNITED WAY HOSTS THE ANNUAL "DAY OF
CARING" PROJECT WHICH BRINGS TOGETHER MORE THAN 1,200 VOLUNTEERS AND
NEARLY 100 SERVICE PROJECTS AT LOCAL NOT FOR PROFIT ORGANIZATIONS.
UNITED WAY 2-1-1: SINCE LAUNCHING IN EARLY 2004, OVER 420,545 PEOPLE IN
EASTERN IOWA HAVE CALLED 2-1-1 FOR SUPPORT. THE MAJORITY OF CALLS
REQUEST INFORMATION ABOUT UTILITY AND HOUSING ASSISTANCE, INFORMATION
AND REFERRAL, INCOME/SUPPORT ASSISTANCE, HEALTHCARE, INDIVIDUAL/FAMILY
SUPPORTS, AND FOOD. DURING THE 2008 FLOODS, UNITED WAY 2-1-1 BECAME A
VITAL RESOURCE FOR PERSONS IN NEED OF DISASTER ASSISTANCE AND RECOVERY
INFORMATION.
UNITED WAY OF EAST CENTRAL IOWA COORDINATES THE 2-1-1 SERVICE, WORKING
IN COLLABORATION WITH THE CEDAR VALLEY UNITED WAY, UNITED WAY OF
JOHNSON COUNTY, UNITED WAY OF WAPELLO COUNTY AND THE WAVERLY-SHELL ROCK
UNITED WAY. THIS BRINGS 2-1-1 SERVICES TO 30 EASTERN AND SOUTHEASTERN
IOWA COUNTIES.
UNITED WAY 2-1-1 PARTNERS WITH LINN, BENTON, BLACK HAWK, CEDAR,
JOHNSON, AND JONES COUNTIES EMERGENCY MANAGEMENT AGENCIES. THIS

23221201-04-13
2
Employer identification number
Schedule O (Form 990 or 990-EZ) (2012)
Schedule O (Form 990 or 990-EZ) (2012) Page
Name of the organizationUNITED WAY OF EAST CENTRAL IOWA, INC. 42-0861239
PARTNERSHIP ALLOWS 2-1-1 TO BE A RESOURCE TO COMMUNITIES IN THE EVENT
OF A DISASTER. INDIVIDUALS CAN CALL 2-1-1 TO RECEIVE ACCURATE AND
TIMELY INFORMATION DURING A DISASTER, SUCH AS A FLOOD, TORNADO OR AN
EMERGENCY AT THE DUANE ARNOLD ENERGY CENTER.
LABOR COMMUNITY SERVICES: UNITED WAY'S LABOR LIAISON EDUCATES LOCAL
UNION WORKERS ABOUT AVAILABLE AREA SERVICES AND ASSISTS THEM IN
ACCESSING THESE SERVICES.
KIDS ON COURSE - THE PURPOSE OF THIS PROGRAM IS TO PROMOTE AND PROVIDE
RICH CULTURAL EXPERIENCES AND ENRICHMENT OPPORTUNITIES TO STUDENTS AND
FAMILIES IN THE CEDAR RAPIDS COMMUNITY SCHOOL DISTRICT. THE PROGRAM
WILL ADVOCATE FOR STUDENTS BY NURTURING THEIR INTERESTS AND PROVIDING
OPPORTUNITIES TO FOSTER CONFIDENCE AND REALIZE ACADEMIC AND INDIVIDUAL
POTENTIAL.
RSVP - RETIRED SENIOR VOLUNTEER PROGRAM - RSVP OF LINN AND JONES
COUNTIES ENGAGES ADULTS, AGE 55 AND OLDER, IN VOLUNTEER SERVICES WHICH
MEET THE CRITICAL COMMUNITY NEEDS THAT IMPACT CITIZENS OF ALL AGES,
WHILE PROVIDING A HIGH QUALITY EXPERIENCE THAT WILL ENRICH THE LIVES OF
VOLUNTEERS. RSVP HAS APPROXIMATELY 500 MEMBERS WHO VOLUNTEER FOR NEARLY
80 PARTNER AGENCIES IN A WIDE VARIETY OF JOBS, CONTRIBUTING OVER 75,000
HOURS OF SERVICE ANNUALLY.
EXPENSES $ 1,868,021. INCL GRANTS OF $ 1,589,620. REVENUE $ 116,877.
FORM 990, PART VI, SECTION A, LINE 2: JACK EVANS, DIRECTOR AND MATT
EVANS, DIRECTOR HAVE A FAMILY RELATIONSHIP.
FORM 990, PART VI, SECTION B, LINE 11: THE SR. MANAGER/CONTROLLER WILL

23221201-04-13
2
Employer identification number
Schedule O (Form 990 or 990-EZ) (2012)
Schedule O (Form 990 or 990-EZ) (2012) Page
Name of the organizationUNITED WAY OF EAST CENTRAL IOWA, INC. 42-0861239
DIRECT THE COMPLETION OF THE FORM 990 AND WILL BE RESPONSIBLE FOR ENSURING
THAT THE RETURN IS FILED WITHIN THE IRS PRESCRIBED 135 DAYS FOLLOWING THE
CLOSE OF THE FISCAL YEAR, OR IF NEEDED, AN APPLICATION FOR EXTENSION OF
TIME IS FILED WITH THE IRS. MEMBERS OF THE UWECI BOARD OF DIRECTORS, WITH
ASSISTANCE FROM THE FINANCE & ADMINISTRATION AND AUDIT COMMITTEES, ARE
STEWARDS OF THE ORGANIZATION'S FINANCIAL RESOURCES AND ARE RESPONSIBLE FOR
ENSURING THAT THESE RESOURCES ARE USED TO FURTHER CHARITABLE PURPOSES. IN
ADDITION, BOARD AND COMMITTEE MEMBERS SHOULD MAINTAIN PROPER FINANCIAL
OVERSIGHT MAKING SURE THAT THE ORGANIZATION'S FUNDS ARE APPROPRIATELY
ACCOUNTED FOR BY RECEIVING AND REVIEWING UP TO DATE FINANCIAL INFORMATION
INCLUDING THE ANNUAL FORM 990. TO FACILITATE ADEQUATE FINANCIAL OVERSIGHT,
A DRAFT VERSION OF THE IRS FORM 990 WILL BE REVIEWED BY THE UWECI AUDIT
COMMITTEE. THE PREPARERS OF THE IRS FORM 990 WILL PROVIDE A BRIEF REVIEW
AND DISCUSSION OF THE FORM 990 POINTING OUT THE SIGNIFICANT AREAS AND HOW
THE NUMBERS RELATE TO THE AUDITED FINANCIAL STATEMENTS. AFTER AUDIT
COMMITTEE APPROVAL OF THE DRAFT AND SUBSEQUENT CHANGES, IF NECESSARY, A
FINAL COPY OF THE IRS FORM 990 WILL BE REVIEWED BY THE UWECI BOARD OF
DIRECTORS PRIOR TO SUBMISSION TO THE IRS. THE FORM 990 WILL BE DISTRIBUTED
ELECTRONICALLY TO ALL BOARD MEMBERS AND WILL BE PRESENTED TO THE BOARD OF
DIRECTORS ANNUALLY AT THE BOARD MEETING WHICH MOST CLOSELY CORRESPONDS WITH
THE COMPLETION OF THE IRS FORM 990.
FORM 990, PART VI, SECTION B, LINE 12C: THE CONFLICT OF INTEREST POLICY IS
REVIEWED BY THE UNITED WAY BOARD OF DIRECTORS EVERY THREE YEARS. UNITED WAY
OF AMERICA (UNITED WAY WORLD WIDE) REQUIRES A CONFLICT OF INTEREST POLICY
AS PART OF THE ANNUAL CERTIFICATION PROCESS. IN ADDITION THE IOWA
PRINCIPLES AND PRACTICES FOR CHARITABLE NONPROFIT EXCELLENCE RECOMMENDS
THIS POLICY FOR GOOD NONPROFIT PRACTICE. IT IS THE POLICY OF UNITED WAY OF
23221201-04-13
2
Employer identification number
Schedule O (Form 990 or 990-EZ) (2012)
Schedule O (Form 990 or 990-EZ) (2012) Page
Name of the organizationUNITED WAY OF EAST CENTRAL IOWA, INC. 42-0861239
EAST CENTRAL IOWA THAT CONFLICTS OF INTEREST SHOULD BE DISCLOSED AND
RESOLVED AT THE EARLIEST POSSIBLE TIME. EVERY UNITED WAY BOARD MEMBER,
FINANCE OR COMMUNITY BUILDING COMMITTEE MEMBER AND EMPLOYEE IS REQUIRED TO
SIGN A CONFLICT OF INTEREST POLICY ANNUALLY. THESE ARE COLLECTED AND FILED
BY THE EXECUTIVE ASSISTANT. EACH VOLUNTEER AND EMPLOYEE MUST DESIGNATE
CONFLICTS THAT RELATE TO PARTNER AGENCY RELATIONSHIPS, BUSINESS
AFFILIATIONS OR NEPOTISM. VOLUNTEERS THAT HAVE A CONFLICT OF INTEREST
REGARDING A UNITED WAY ALLOCATION OR VENDOR RELATIONSHIP CANNOT SERVE IN A
DECISION-MAKING CAPACITY. THESE INDIVIDUALS MUST RECUSE THEMSELVES FROM ANY
VOTING. THESE ACTIONS ARE DOCUMENTED IN THE MINUTES OF THE MEETINGS.
IF ANY VOLUNTEER OR EMPLOYEE HAS A CONCERN ABOUT A POTENTIAL OR ACTUAL
CONFLICT OF INTEREST AND HOW IT HAS BEEN RESOLVED, THE INDIVIDUAL IS
REQUESTED TO NOTIFY THE PRESIDENT/CEO. THE DISCUSSION AND RESOLUTION OF
THIS ISSUE WILL BE ADDRESSED BY THE EXECUTIVE COMMITTEE OF THE BOARD OF
DIRECTORS AND A RESPONSE WILL BE DOCUMENTED.
FORM 990, PART VI, SECTION B, LINE 15:
EXECUTIVE COMPENSATION REVIEW:
THE COMPENSATION OF THE CEO IS REVIEWED BY THE BOARD CHAIR, PAST BOARD
CHAIR, AND BOARD VICE CHAIR. INFORMATION FROM THE ANNUAL UNITED WAY OF
AMERICA ("UWA") COMPENSATION SURVEY ALONG WITH INFORMATION FROM THE FORM
990 OF OTHER ORGANIZATIONS IS UTILIZED TO FORM THE BASIS FOR THE CEO'S
COMPENSATION. THE COMPENSATION OF THE CEO IS A RECOMMENDATION FROM THE
BOARD CHAIR, PAST BOARD CHAIR AND BOARD VICE CHAIR AND MUST BE APPROVED BY
THE UWECI BOARD OF DIRECTORS.
OTHER OFFICER/KEY EMPLOYEE COMPENSATION REVIEW:

23221201-04-13
2
Employer identification number
Schedule O (Form 990 or 990-EZ) (2012)
Schedule O (Form 990 or 990-EZ) (2012) Page
Name of the organizationUNITED WAY OF EAST CENTRAL IOWA, INC. 42-0861239
THE COMPENSATION AND BENEFIT PROGRAMS ARE REVIEWED BY THE HUMAN RESOURCE
COMMITTEE OF THE BOARD OF DIRECTORS. SALARY SCHEDULES ARE REVIEWED ANNUALLY
WITH DATA FROM UWA AND LOCAL FIRMS.
FORM 990, PART VI, SECTION C, LINE 19: THE ORGANIZATION PUBLISHES ITS
ANNUAL AUDITED FINANCIAL STATEMENTS, MOST RECENTLY FILED FORM 990, AND IRS
DETERMINATION LETTER ON ITS EXTERNAL WEBSITE AT WWW.UWECI.ORG. ALL
GOVERNING DOCUMENTS, THE CONFLICT OF INTEREST POLICY, AND FINANCIAL
STATEMENTS CAN BE MADE AVAILABLE TO THE PUBLIC AT THEIR REQUEST.
FORM 990, PART XI, LINE 9, CHANGES IN NET ASSETS:
CHANGE IN BENEFICIAL INTEREST IN COMMUNITY FOUNDATION 26,112.
NET INCOME OF SUBSIDIARY - FCFH-IOWA, INC. 7,263.
NET INCOME OF SUBSIDIARY - HUMAN SERVICES CAMPUS OF EAST
CENTRAL IOWA -227,551.
TOTAL TO FORM 990, PART XI, LINE 9 -194,176.

OM
B N
o.
15
45
-00
47
Dep
art
men
t o
f th
e T
reasu
ryIn
tern
al R
even
ue S
erv
ice
Secti
on
51
2(b
)(13
)
co
ntr
olle
d
en
tity
?
23
21
61
12
-10
-12
SC
HE
DU
LE
R(F
orm
99
0)
Co
mp
lete
if
the
org
an
iza
tio
n a
nsw
ere
d "
Ye
s"
to F
orm
99
0, P
art
IV
, lin
e 3
3, 3
4, 3
5, 3
6, o
r 3
7.
Op
en
to
Pu
blic
Insp
ec
tio
nS
ee
se
pa
rate
in
str
uc
tio
ns.
Att
ac
h t
o F
orm
99
0.
Em
plo
yer
ide
nti
fic
ati
on
nu
mb
er
Pa
rt I
Ide
nti
fic
ati
on
of
Dis
reg
ard
ed
En
titi
es
(a)
(b)
(c)
(d)
(e)
(f)
Ide
nti
fic
ati
on
of
Re
late
d T
ax-E
xe
mp
t O
rga
niz
ati
on
s
Pa
rt I
I
(a)
(b)
(c)
(d)
(e)
(f)
(g)
Ye
sN
o
Fo
r P
ap
erw
ork
Re
du
cti
on
Ac
t N
oti
ce
, se
e t
he
In
str
uc
tio
ns f
or
Fo
rm 9
90
.S
ch
ed
ule
R (
Fo
rm 9
90
) 2
01
2
||
|
Nam
e o
f th
e o
rgan
izatio
n
(Co
mp
lete
if t
he o
rgan
izatio
n a
nsw
ere
d "
Yes"
to
Fo
rm 9
90
, P
art
IV
, lin
e 3
3.)
Nam
e, ad
dre
ss, an
d E
IN (if
ap
plic
ab
le)
of
dis
reg
ard
ed
en
tity
Prim
ary
activi
tyL
eg
al d
om
icile
(st
ate
or
fore
ign
co
un
try)
To
tal i
nco
me
En
d-o
f-ye
ar
ass
ets
Direct
co
ntr
olli
ng
en
tity
(Co
mp
lete
if t
he o
rgan
izatio
n a
nsw
ere
d "
Yes"
to
Fo
rm 9
90
, P
art
IV
, lin
e 3
4 b
ecau
se it
had
on
e o
r m
ore
rela
ted
tax-
exe
mp
to
rgan
izatio
ns
du
rin
g t
he t
ax
year.
)
Nam
e, ad
dre
ss, an
d E
INo
f re
late
d o
rgan
izatio
nP
rim
ary
activi
tyL
eg
al d
om
icile
(st
ate
or
fore
ign
co
un
try)
Exe
mp
t C
od
ese
ctio
nP
ub
lic c
harity
statu
s (if
sectio
n5
01
(c)(3
))
Direct
co
ntr
olli
ng
en
tity
LH
A
Re
late
d O
rga
niz
ati
on
s a
nd
Un
rela
ted
Pa
rtn
ers
hip
s2012
UNITED WAY OF EAST CENTRAL IOWA, INC.
42-0861239
HUMAN SE
RVIC
ES C
AMPU
S OF
EAS
T CE
NTRA
L IO
WA -
FACILITY TO HOUSE MULTIPLE
27-04873
31,
317
7TH
AVE
SE #
401,
CED
ARNO
N-PROFIT AGENCIES IN
UNITED WAY OF
RAPIDS,
IA
5240
1CE
NTRAL DOWNTOWN LOCATION
IOWA
501(C)(3
)LINE 11A, I
EAST CENTRAL IOWA
XFCFH-IOW
A, I
NC.
- 20-0
9369
54HEALTH AND HUMAN SERVICES
317 7TH
AVE
SE #
401
INFORMATION AND REFERRAL
UNITED WAY OF
CEDAR RA
PIDS
, IA
5240
1HE
LPLINE
IOWA
501(C)(3
)LINE 7
EAST CENTRAL IOWA
X

Leg
al
do
mic
ile(s
tate
or
fore
ign
co
un
try)
Gen
era
l o
rm
an
ag
ing
part
ner?
Dis
pro
po
rtio
n-
ate
allo
cati
on
s?
Secti
on
51
2(b
)(13
)co
ntr
olle
den
tity
?
Leg
al d
om
icile
(sta
te o
rfo
reig
nco
un
try)
23
21
62
1
2-1
0-1
2
2
Ide
nti
fic
ati
on
of
Re
late
d O
rga
niz
ati
on
s T
axa
ble
as a
Pa
rtn
ers
hip
P
art
III
(a)
(b)
(c)
(d)
(e)
(f)
(g)
(h)
(i)
(j)
(k)
Ye
sN
oY
es
No
Ide
nti
fic
ati
on
of
Re
late
d O
rga
niz
ati
on
s T
axa
ble
as a
Co
rpo
rati
on
or
Tru
st
Pa
rt I
V
(a)
(b)
(c)
(d)
(e)
(f)
(g)
(h)
(i)
Ye
sN
o
Sc
he
du
le R
(F
orm
99
0)
20
12
Pre
dom
inan
t inc
ome
(rel
ated
, unr
elat
ed,
excl
uded
from
tax
unde
rse
ctio
ns 5
12-5
14)
Sch
ed
ule
R (F
orm
99
0) 2
01
2P
ag
e
(Co
mp
lete
if t
he o
rgan
izatio
n a
nsw
ere
d "
Yes"
to
Fo
rm 9
90
, P
art
IV
, lin
e 3
4 b
ecau
se it
had
on
e o
r m
ore
rela
ted
org
an
izatio
ns
treate
d a
s a p
art
ners
hip
du
rin
g t
he t
ax
year.
)
Nam
e, ad
dre
ss, an
d E
INo
f re
late
d o
rgan
izatio
nP
rim
ary
activi
tyD
irect
co
ntr
olli
ng
en
tity
Sh
are
of
tota
lin
co
me
Sh
are
of
en
d-o
f-ye
ar
ass
ets
Co
de V
-UB
Iam
ou
nt
in b
ox
20
of
Sch
ed
ule
K-1
(F
orm
10
65
)
Perc
en
tag
eo
wn
ers
hip
(Co
mp
lete
if t
he o
rgan
izatio
n a
nsw
ere
d "
Yes"
to
Fo
rm 9
90
, P
art
IV
, lin
e 3
4 b
ecau
se it
had
on
e o
r m
ore
rela
ted
org
an
izatio
ns
treate
d a
s a c
orp
ora
tio
n o
r tr
ust
du
rin
g t
he t
ax
year.
)
Nam
e, ad
dre
ss, an
d E
INo
f re
late
d o
rgan
izatio
nP
rim
ary
activi
tyD
irect
co
ntr
olli
ng
en
tity
Typ
e o
f en
tity
(C c
orp
, S
co
rp,
or
tru
st)
Sh
are
of
tota
lin
co
me
Sh
are
of
en
d-o
f-ye
ar
ass
ets
Perc
en
tag
eo
wn
ers
hip
UNITED WAY OF EAST CENTRAL IOWA, INC.
42-0861239

23
21
63
1
2-1
0-1
2
3
Pa
rt V
Tra
nsa
cti
on
s W
ith
Re
late
d O
rga
niz
ati
on
s
No
te.
Ye
sN
o
1
a b c d e f g h i j k l m n o p q r s
(i)
(ii)
(i
ii)
(iv)
1
a
1b
1c
1d
1e 1f
1g
1h 1i
1j
1k 1l
1m 1n
1o
1p
1q 1r
1s
2
(a)
(b)
(c)
(d)
(1)
(2)
(3)
(4)
(5)
(6)
Sc
he
du
le R
(F
orm
99
0)
20
12
Sch
ed
ule
R (F
orm
99
0) 2
01
2P
ag
e
(Co
mp
lete
if t
he o
rgan
izatio
n a
nsw
ere
d "
Yes"
to
Fo
rm 9
90
, P
art
IV
, lin
e 3
4, 3
5b
, o
r 3
6.)
Co
mp
lete
lin
e 1
if a
ny
en
tity
is li
sted
in P
art
s II, III, o
r IV
of
this
sch
ed
ule
.
Du
rin
g t
he t
ax
year,
did
th
e o
rgan
izatio
n e
ng
ag
e in
an
y o
f th
e f
ollo
win
g t
ran
sactio
ns
with
on
e o
r m
ore
rela
ted
org
an
izatio
ns
liste
d in
Part
s II-IV
?
Receip
t o
f in
tere
st
an
nu
itie
s ro
yaltie
s o
r re
nt
fro
m a
co
ntr
olle
d e
ntity
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
Gift
, g
ran
t, o
r cap
ital c
on
trib
utio
n t
o r
ela
ted
org
an
izatio
n(s
)
Gift
, g
ran
t, o
r cap
ital c
on
trib
utio
n f
rom
rela
ted
org
an
izatio
n(s
)
Lo
an
s o
r lo
an
gu
ara
nte
es
to o
r fo
r re
late
d o
rgan
izatio
n(s
)
Lo
an
s o
r lo
an
gu
ara
nte
es
by
rela
ted
org
an
izatio
n(s
)
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~
Div
iden
ds
fro
m r
ela
ted
org
an
izatio
n(s
)~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
Sale
of
ass
ets
to
rela
ted
org
an
izatio
n(s
)
Pu
rch
ase
of
ass
ets
fro
m r
ela
ted
org
an
izatio
n(s
)
Exc
han
ge o
f ass
ets
with
rela
ted
org
an
izatio
n(s
)
Lease
of
facili
ties,
eq
uip
men
t, o
r o
ther
ass
ets
to
rela
ted
org
an
izatio
n(s
)
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~
Lease
of
facili
ties,
eq
uip
men
t, o
r o
ther
ass
ets
fro
m r
ela
ted
org
an
izatio
n(s
)
Perf
orm
an
ce o
f se
rvic
es
or
mem
bers
hip
or
fun
dra
isin
g s
olic
itatio
ns
for
rela
ted
org
an
izatio
n(s
)
Perf
orm
an
ce o
f se
rvic
es
or
mem
bers
hip
or
fun
dra
isin
g s
olic
itatio
ns
by
rela
ted
org
an
izatio
n(s
)
Sh
arin
g o
f fa
cili
ties,
eq
uip
men
t, m
aili
ng
list
s, o
r o
ther
ass
ets
with
rela
ted
org
an
izatio
n(s
)
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~
Sh
arin
g o
f p
aid
em
plo
yees
with
rela
ted
org
an
izatio
n(s
)~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
Reim
bu
rsem
en
t p
aid
to
rela
ted
org
an
izatio
n(s
) fo
r exp
en
ses
Reim
bu
rsem
en
t p
aid
by
rela
ted
org
an
izatio
n(s
) fo
r exp
en
ses
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~
Oth
er
tran
sfer
of
cash
or
pro
pert
y to
rela
ted
org
an
izatio
n(s
)
Oth
er
tran
sfer
of
cash
or
pro
pert
y fr
om
rela
ted
org
an
izatio
n(s
)~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~~
~
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
If t
he a
nsw
er
to a
ny
of
the a
bo
ve is
"Y
es,
" se
e t
he in
stru
ctio
ns
for
info
rmatio
n o
n w
ho
mu
st c
om
ple
te t
his
lin
e, in
clu
din
g c
ove
red
rela
tio
nsh
ips
an
d t
ran
sactio
n t
hre
sho
lds.
Nam
e o
f o
ther
org
an
izatio
nT
ran
sactio
nty
pe (a-s
)A
mo
un
t in
volv
ed
Meth
od
of
dete
rmin
ing
am
ou
nt
invo
lved
UNITED WAY OF EAST CENTRAL IOWA, INC.
42-0861239
XX
X X X X X X X X
X XX
X X
XX
X X
FCFH-IOWA, INC.
B305,000.CASH
HUMAN SERVICES CAMPUS OF EAST CENTRAL IOWA
K107,300.CASH
FCFH-IOWA, INC.
Q68,334.ACTUAL EXPENSES

Are
all
partn
ers
sec.
501(
c)(3
)or
gs.?
Dis
prop
or-
tiona
teal
loca
tions
?
Gen
era
l o
rm
an
ag
ing
part
ner?
23
21
64
12
-10
-12
Yes
No
Yes
No
YesN
4
Pa
rt V
IU
nre
late
d O
rga
niz
ati
on
s T
axa
ble
as a
Pa
rtn
ers
hip
(a)
(b)
(c)
(d)
(e)
(f)
(g)
(h)
(i)
(j)
(k)
o
Sc
he
du
le R
(F
orm
99
0)
20
12
Pre
dom
inan
t inc
ome
(rel
ated
, unr
elat
ed,
excl
uded
from
tax
unde
r se
ctio
n 51
2-51
4)
Cod
e V
-UB
Iam
ount
in b
ox 2
0of
Sch
edul
e K
-1(F
orm
106
5)
Sch
ed
ule
R (F
orm
99
0) 2
01
2P
ag
e
(Co
mp
lete
if t
he o
rgan
izatio
n a
nsw
ere
d "
Yes"
to
Fo
rm 9
90
, P
art
IV
, lin
e 3
7.)
Pro
vid
e t
he f
ollo
win
g in
form
atio
n f
or
each
en
tity
taxe
d a
s a p
art
ners
hip
th
rou
gh
wh
ich
th
e o
rgan
izatio
n c
on
du
cte
d m
ore
th
an
fiv
e p
erc
en
t o
f its
activi
ties
(measu
red
by
tota
l ass
ets
or
gro
ss r
eve
nu
e)
that
was
no
t a r
ela
ted
org
an
izatio
n. S
ee in
stru
ctio
ns
reg
ard
ing
exc
lusi
on
fo
r cert
ain
inve
stm
en
t p
art
ners
hip
s.
Nam
e, ad
dre
ss, an
d E
INo
f en
tity
Prim
ary
activi
tyL
eg
al d
om
icile
(sta
te o
r fo
reig
nco
un
try)
Sh
are
of
tota
lin
co
me
Sh
are
of
en
d-o
f-ye
ar
ass
ets
Perc
en
tag
eo
wn
ers
hip
UNITED WAY OF EAST CENTRAL IOWA, INC.
42-0861239

232165 12-10-12
5
Schedule R (Form 990) 2012
Schedule R (Form 990) 2012 Page
Complete this part to provide additional information for responses to questions on Schedule R (see instructions).
Part VII Supplemental Information
UNITED WAY OF EAST CENTRAL IOWA, INC. 42-0861239

OMB No. 1545-1878
Form
For calendar year 2012, or fiscal year beginning , 2012, and ending ,20
Department of the TreasuryInternal Revenue Service
22305111-05-12
Employer identification number
Enter five numbers, butdo not enter all zeros
ERO firm name
do not enter all zeros
| Do not send to the IRS. Keep for your records.
1a, 2a, 3a, 4a, 5a, 1b, 2b, 3b, 4b, 5b,Do not
1a
2a
3a
4a
5a
| b Total revenue, 1b
2b
3b
4b
5b
| b Total revenue,
| b Total tax
| b Tax based on investment income
| b Balance Due
(a) (b) (c)
Officer's PIN: check one box only
ERO's EFIN/PIN.
Pub. 4163,
For Paperwork Reduction Act Notice, see instructions.
e-file
Name of exempt organization
Name and title of officer
~~~
~~~~~~~~
Officer's signature | Date |
ERO's signature | Date |
Form (2012)
(Whole Dollars Only)
Check the box for the return for which you are using this Form 8879-EO and enter the applicable amount, if any, from the return. If you check the boxon line or below, and the amount on that line for the return being filed with this form was blank, then leave line orwhichever is applicable, blank (do not enter -0-). But, if you entered -0- on the return, then enter -0- on the applicable line below. complete morethan 1 line in Part I.
Form 990 check here
Form 990-EZ check here
Form 1120-POL check here
if any (Form 990, Part VIII, column (A), line 12)~~~~~~~
if any (Form 990-EZ, line 9) ~~~~~~~~~~~~~~
(Form 1120-POL, line 22) ~~~~~~~~~~~~~~~~
Form 990-PF check here
Form 8868 check here
(Form 990-PF, Part VI, line 5)
(Form 8868, Part I, line 3c or Part II, line 8c)
Under penalties of perjury, I declare that I am an officer of the above organization and that I have examined a copy of the organization's 2012electronic return and accompanying schedules and statements and to the best of my knowledge and belief, they are true, correct, and complete. Ifurther declare that the amount in Part I above is the amount shown on the copy of the organization's electronic return. I consent to allow myintermediate service provider, transmitter, or electronic return originator (ERO) to send the organization's return to the IRS and to receive from the IRS
an acknowledgement of receipt or reason for rejection of the transmission, the reason for any delay in processing the return or refund, and the date of any refund. If applicable, I authorize the U.S. Treasury and its designated Financial Agent to initiate an electronic funds withdrawal (directdebit) entry to the financial institution account indicated in the tax preparation software for payment of the organization's federal taxes owed on thisreturn, and the financial institution to debit the entry to this account. To revoke a payment, I must contact the U.S. Treasury Financial Agent at1-888-353-4537 no later than 2 business days prior to the payment (settlement) date. I also authorize the financial institutions involved in theprocessing of the electronic payment of taxes to receive confidential information necessary to answer inquiries and resolve issues related to thepayment. I have selected a personal identification number (PIN) as my signature for the organization's electronic return and, if applicable, theorganization's consent to electronic funds withdrawal.
I authorize to enter my PIN
as my signature on the organization's tax year 2012 electronically filed return. If I have indicated within this return that a copy of the returnis being filed with a state agency(ies) regulating charities as part of the IRS Fed/State program, I also authorize the aforementioned ERO toenter my PIN on the return's disclosure consent screen.
As an officer of the organization, I will enter my PIN as my signature on the organization's tax year 2012 electronically filed return. If I haveindicated within this return that a copy of the return is being filed with a state agency(ies) regulating charities as part of the IRS Fed/Stateprogram, I will enter my PIN on the return's disclosure consent screen.
Enter your six-digit electronic filing identification
number (EFIN) followed by your five-digit self-selected PIN.
I certify that the above numeric entry is my PIN, which is my signature on the 2012 electronically filed return for the organization indicated above. Iconfirm that I am submitting this return in accordance with the requirements of Modernized e-File (MeF) Information for Authorized IRS
Providers for Business Returns.
LHA
e-fileIRS Signature Authorizationfor an Exempt Organization
Part I Type of Return and Return Information
Part II Declaration and Signature Authorization of Officer
Part III Certification and Authentication
ERO Must Retain This Form - See InstructionsDo Not Submit This Form To the IRS Unless Requested To Do So
8879-EO
8879-EO
2012
JUL 1 JUN 30 13
UNITED WAY OF EAST CENTRAL IOWA, INC. 42-0861239
LOIS BUNTZPRESIDENT/CEO
X 11143636
X MCGLADREY LLP 61239
42396691057