unit 14 pleura and lungs. quiz clinical case a 55 year old man reported to his family physician that...
TRANSCRIPT

Unit 14
Pleura and Lungs

Quiz

Clinical Case
A 55 year old man reported to his family physician that
he had a solid swelling in his scrotum. There was no
ulceration of the scrotal skin and a red glow could not be
seen using transillumination. The lump was diagnosed as an advanced carcinoma of
the testis.

Plate 242
Three divisions to the thorax:
2 Pleural Cavities and
a Mediastinum
The 2 Pleural Cavities
are closed and
separate spaces
M
PP
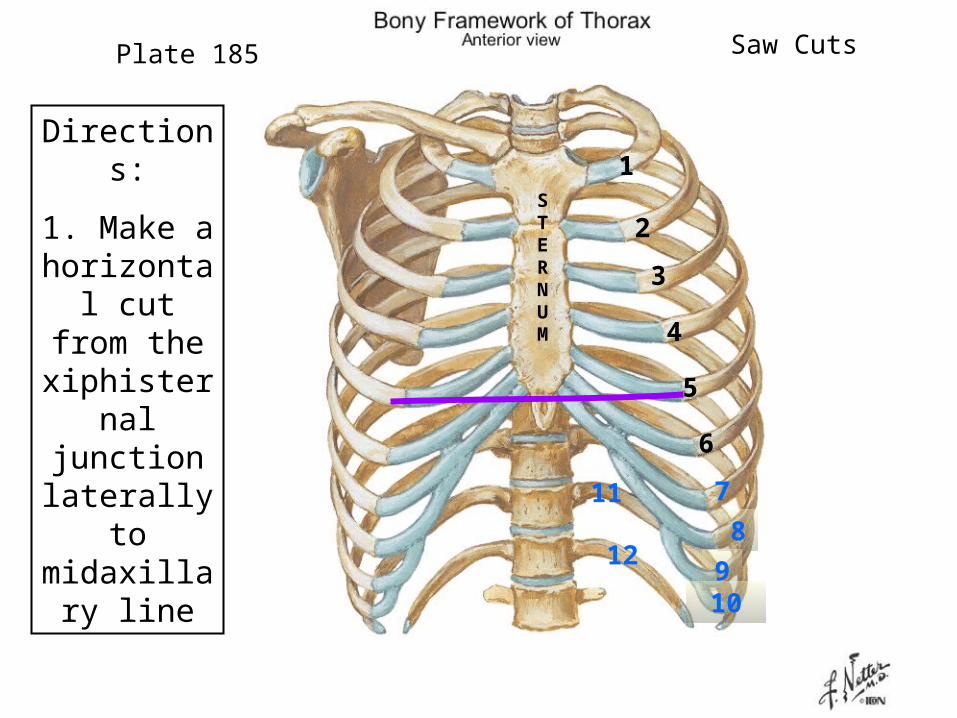
Directions:
1. Make a horizontal cut from
the xiphisternal junction laterally to midaxillar
y line
Plate 185
1
2
3
4
5
6
7
8
910
11
12
STERNUM
Saw Cuts

2. Cut through the ribs in a
superior direction to rib 2 – midaxillary line
4. Pry the rib cage upward
and separate
any pleura
3. Saw through the sternal angle and use a scalpel to
cut through muscles in the
intercostal spaces
Plate 185
1
2
3
4
5
6
7
8
910
11
12
STERNUM
Saw Cuts

Remember, the Internal
Thoracic artery
terminates as the
Musculophrenic and Superior
Epigastric arteries
Superior Epigastric
Musculophrenic
Internal Thoracic Artery
Anterior Intercostal
Arteries
Sternum
Identify the Internal Thoracic
artery and any
Parasternal lymph nodes
Plate 191 Internal Thoracic Cage
Subclavian Artery

If the parietal pleura was freed intact from the thoracic wall,
incise it parasternally and reflect it laterally to expose the lungs in their respective pleural
cavities.The visceral pleura is a covering on the surface of the lungs. The parietal pleura lines the pleural cavity. The space between the two membranes is the pleural
cavity. The visceral and parietal pleura are continuous with one another at the root
(hilum) of the lung.

Lung bud expands into primitive
pleural cavity-5th week; this is the first of 3 body
cavities
Identify the parts of the
parietal pleura
MEDIASTINUM
Pleura and Cavity
Serous fluid
Pleura
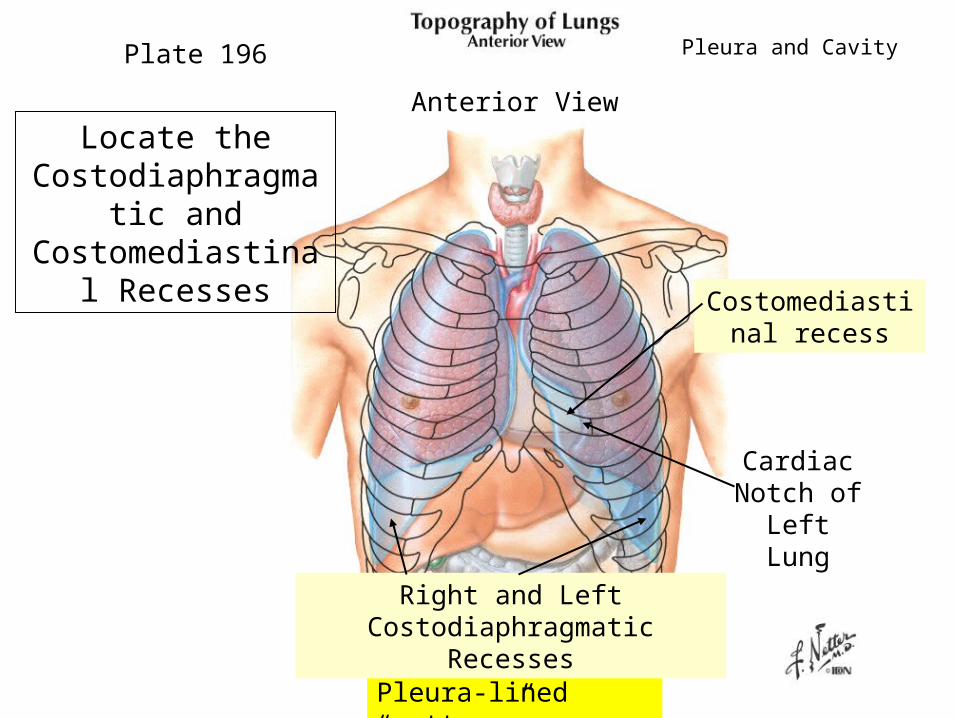
Locate the Costodiaphragmat
ic and Costomediastinal
Recesses
Pleura-lined “gutters”
Plate 196
Right and Left Costodiaphragmatic Recesses
Costomediastinal recess
Cardiac Notch of Left Lung
Pleura and Cavity
Anterior View

Plate 197 Pleura and Cavity
Left Costodiaphragmatic Recess
Right Costodiaphragmatic Recess
Posterior View

Plate 196
Cardiac Notch of Left Lung
Lingula
Apex
Base Base
IdentifyCardiac Notch
LingulaApex Base

Retract the lungs laterally to expose the Mediastinal
pleura covering the Fibrous Pericardium
Plate 193
Mediastinal Part of Parietal
Pleura
Fibrous Pericardium of
Heart Sac
Lungs

If you separate the Mediastinal pleura from the heart sac
you will find the Phrenic Nerve and
the Pericardiacophrenic vessels anterior to the ROOT of the
LUNG
Plate 211
Phrenic Nerve
Pericardiacophrenic Vessels
Lungs
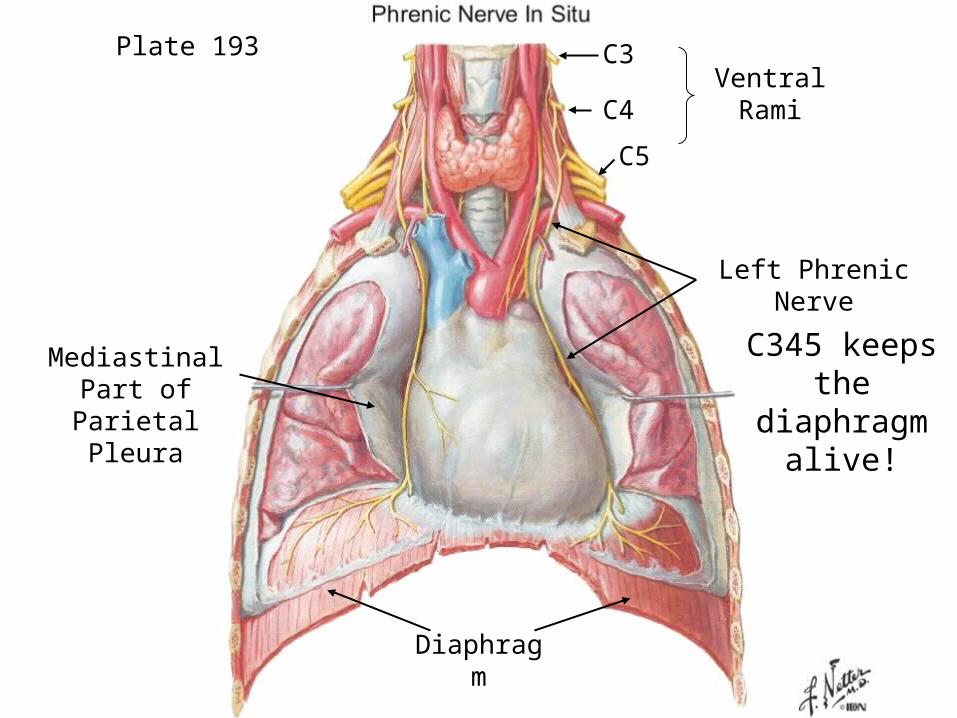
Left Phrenic Nerve
C3
C4
C5
Ventral Rami
Diaphragm
Mediastinal Part of Parietal
Pleura
C345 keeps the
diaphragm alive!
Plate 193

There may be
adhesions
Transect the root of the each lung
and remove the lungs from the pleural cavities

What is in the Root of the lung?
Identify:Pulmonary ArteryBronchi Pulmonary Veins Lymph NodesPulmonary Ligament
Plate 199B Lungs
Apex
Base
Lingula
Superior Lobe
Inferior Lobe
Superior Lobe
Oblique Fissure
Cut Pleur
a
Anterior
Pulmonary Ligament
Left Pulmonary ArteryLeft Main BronchusLeft Superior Pulmonary VeinsHilar Lymph NodesLeft Inferior Pulmonary Vein

Superior Lobe
Middle Lobe Inferior Lobe
Identify the same components on the right lung and on the corresponding
mediastinal surface
Plate 199A Lungs
Oblique Fissure
Horizontal Fissure
Rt. Lobar BronchiRt. Pulmonary ArteryRt. Superior Pulmonary VeinsHilar Lymph NodeRt. Inferior Pulmonary Vein
Anterior

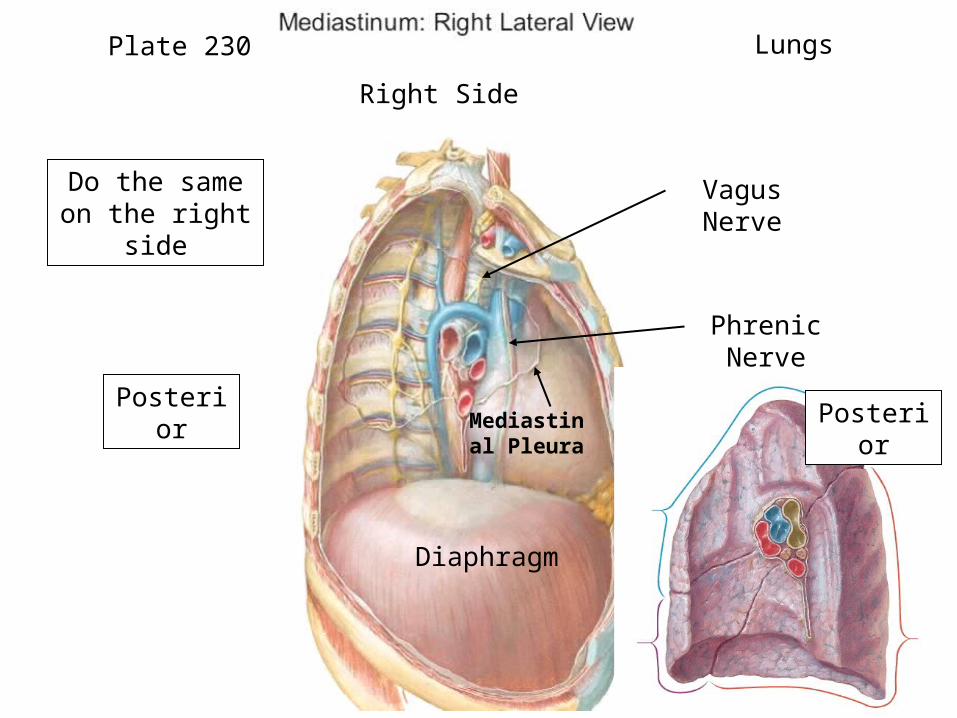
Identify the Vagus
Nerve as it passes
behind the root of the
lung
Note that the Phrenic
nerve passes in
front of the root of the
lung
Plate 231 Lungs
Vagus Nerve
Phrenic Nerve
DiaphragmPosterio
r
Left Side
Mediastinal Pleura
Phrenic Nerve
Vagus Nerve
Posterior
Diaphragm
Do the same on the right
side
Plate 230 Lungs
Right Side
Posterior
Mediastinal Pleura

Plate 198 Lungs
Three lobes: Superior, Middle, InferiorTwo fissures: Horizontal and Oblique
Two lobes: Superior, Inferior One fissure: Oblique
S
M
I
S
ILingul
a
Cardiac Notch
Horizontal Fissure
Oblique
Fissure
Base Base
Oblique Fissure
Right lung – shorter and wider due to liver
IdentifyApex
extends into the
neck

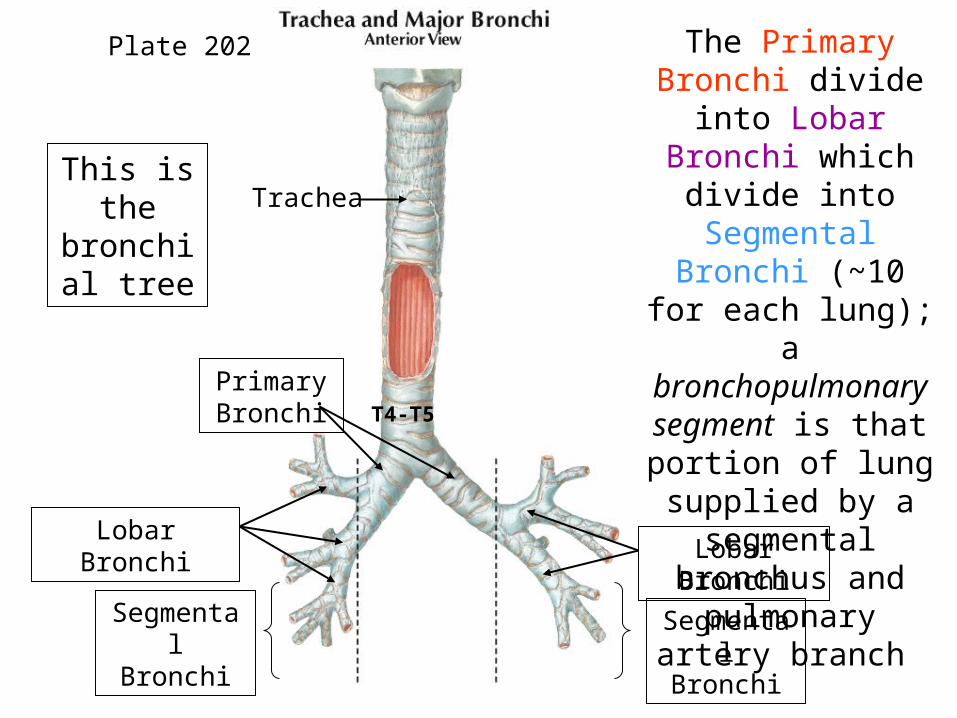
The Primary Bronchi divide into
Lobar Bronchi which divide into
Segmental Bronchi (~10 for
each lung); a bronchopulmonary segment is that
portion of lung supplied by a
segmental bronchus and
pulmonary artery branch
This is the
bronchial tree
Plate 202
Trachea
Primary Bronchi
Lobar BronchiLobar
BronchiSegmental Bronchi
Segmental Bronchi
T4-T5

Bronchopulmonary Segments
Plate 201
Bronchopulmonary segments are surgically separable: important in removal of tumors or
abscesses
Lungs
10 8-10
A bronchopulmonary segment contains a segmental bronchus, a branch of the pulmonary artery, and a branch of the bronchial
artery which run together in the central part of the segment.Lymphatics and veins
drain along the borders Arteries run with Airways

If a person inhales a foreign
object, it lodges in the right
bronchus. Why?
1. Shorter in length
2. Wider in diameter3. More vertical25 45
Plate 202 Lungs
Right
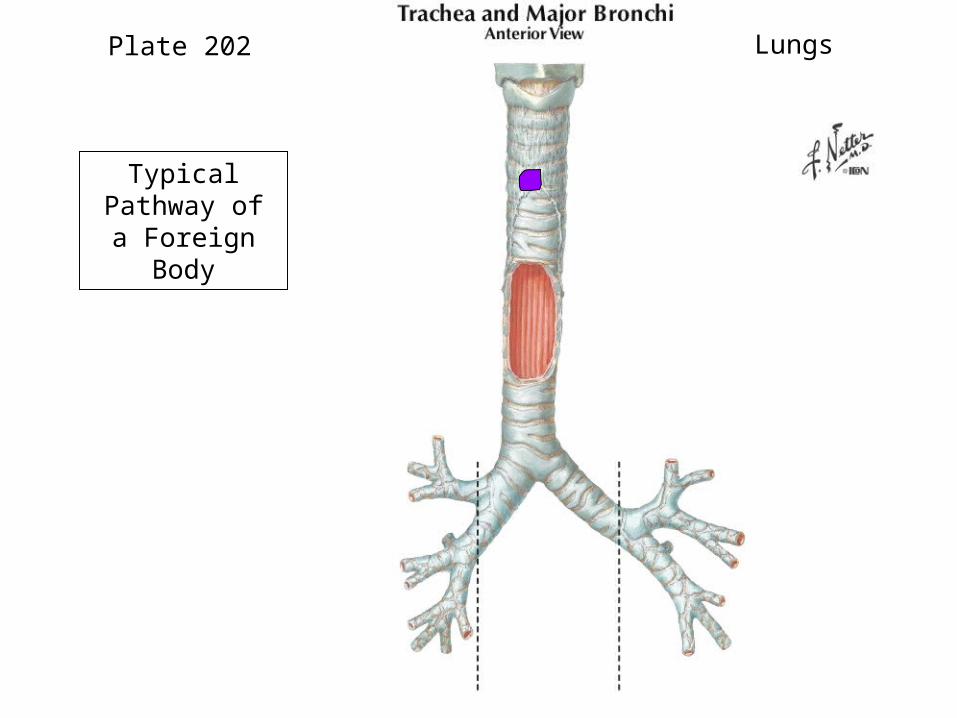
Plate 202 Lungs
Typical Pathway of a Foreign Body

Atelectasis of the right lung – total homogeneous opacity of
right side.
Atelectasis of the right middle and lower lobes of the lung – the intermediate
bronchus leads to dilated and occluded branches in the shrunken middle and
lower lobes. The rest of the right side is occupied by branches of upper lobe.
AP of right lungLateral of right lung
U

Bronchoscopic view of the
carina and left and right
primary bronchi
Distortions in the position of the carina may
indicate metastasis of bronchogenic
carcinoma into the
tracheobronchial lymph nodes
Carina
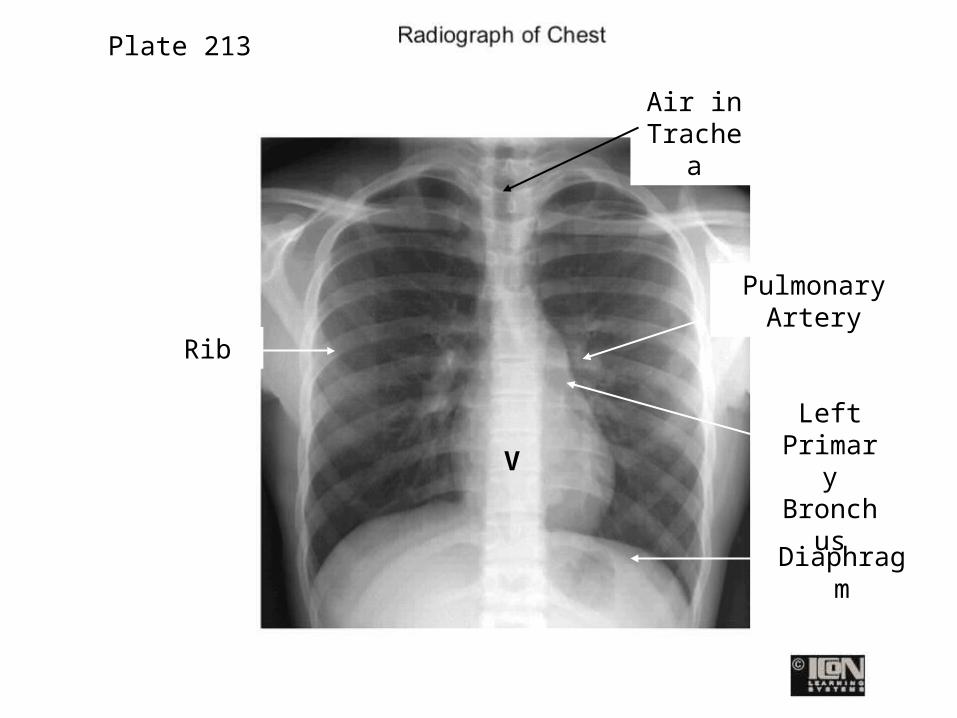
Air in Trachea
Pulmonary Artery
Diaphragm
Rib
V
Plate 213
Left Primary Bronch
us

In order for inspiration to occur, the lungs must expand. This increases lung
volume and decreases the pressure in the lungs to 758 mm Hg or below
atmospheric pressure (760 mm Hg). The lungs expand because the diaphragm increases the vertical diameter of the thorax and the external intercostals
elevate the ribs. Air will flow into the lungs because of this pressure difference.
Expiration is a passive process and occurs when the pressure in the lungs is
greater than the pressure in the atmosphere. Elastic recoil of the chest
wall and lungs occurs.Intrapleural pressure (in the pleural space) is
4 mm Hg below atmospheric pressure. This acts like a “suction” and keeps the alveoli
inflated.

Bucket Handle - Lateral
Pump Handle - AP Plus diaphragm movements
Movements of the thoracic cage which increase or decrease the
intrathoracic volume resulting in pressure changes causing inspiration or expiration.
Page 89
Moore
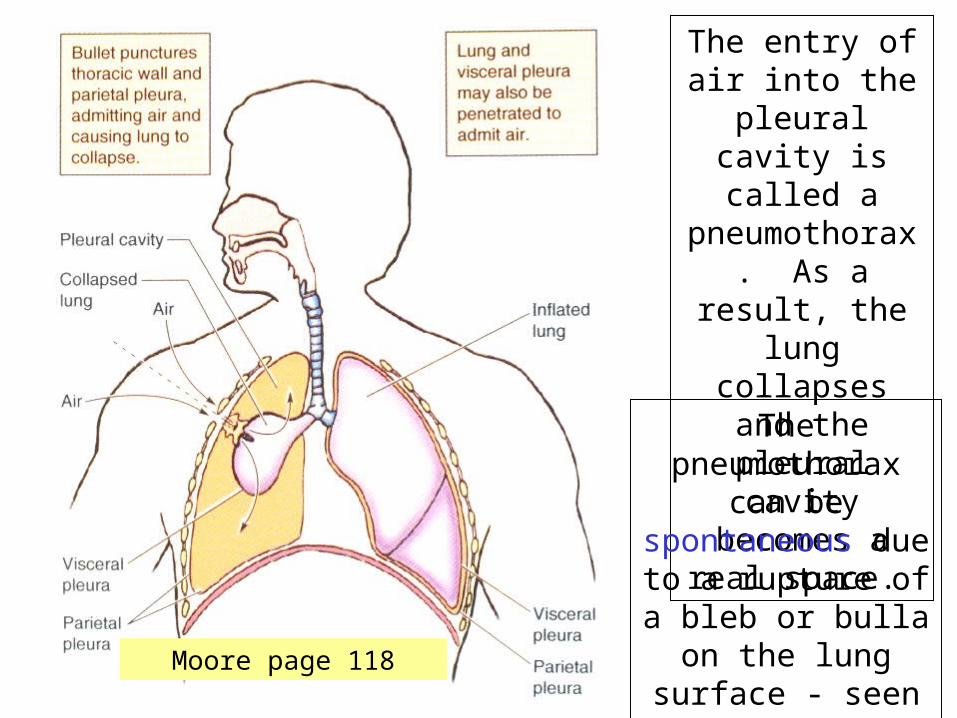
The entry of air into the
pleural cavity is called a
pneumothorax. As a result,
the lung collapses and
the pleural cavity
becomes a real space.
The pneumothorax
can be spontaneous due to a rupture of a bleb or bulla on
the lung surface - seen in men 20-
40 years
Moore page 118

Typically in a patient with no known lung disease, but can occur secondary to
diseases of the lung.

Simple Pneumothorax
Detail
Common presentation:
Tall, thin male teenager
Abrupt onset dyspneaChest pain
Hyperresonant percussion on affected
sideBreath sounds
diminished

This is another type of pneumothorax - an open pneumothorax; air flows easily in and out of the open wound. Mediastinal structures are pushed to the opposite side with inspiration but return with expiration.

In a tension pneumothorax, the wound is covered by skin, muscle or clothing. The air becomes trapped in the pleural space and Mediastinal structures are pushed to the opposite side. One lung is collapsed and the other lung is compressed. Trachea deviates away from the lesion. This is a lethal condition. Pressure must be relieved!
Clinical signs: distended neck veins, shifted trachea, decreased breath sounds in both lungs, hypotension,
agitation

Classic signs of a tension pneumothorax:
Deviation of trachea away from side of tension
Shift in mediastinum
Depression of hemi-diaphragm
Post-mortem chest X-ray of left tension pneumothorax
Cardiovascular function
compromised due to venous obstruction of
heart

Tension pneumothoraxidentified on CT scan

Moore, page 119

To remove blood or other fluids, a needle is inserted closer to the upper border of the rib below to avoid nerves. The 9th interspace in the midaxillary line
during expiration is a safe place - above the diaphragm.
Hydrothorax: due to a pleural effusion (escape of fluid into the pleura space)
Hemothorax: blood entering the pleural space – e.g., from a chest wound
Page 119 Moore
9
10
CLINICAL CASEA woman was stabbed in the right side
of her lower neck. The stab wound was approximately 2.5 cm superior to
the medial third of the clavicle. Shortly after the bleeding was controlled, the woman began breathing rapidly and
was given oxygen by the paramedics. Physical examination revealed a significant shift of mediastinal
structures and poor breath sounds were heard on the right side of the
chest.

Laboratory