unified osteopathic field theory - academy of...
TRANSCRIPT
Biomechanics of the Unified Osteopathic Field Theory
Clarence L. Nicodemus, D.O., Ph.D. (with inspiration and contribution by Ken Lossing, D.O.)
AAO Convocation Louisville, KY
March 22-23, 2012

Examine the components:
“Osteopathic Field”
“Unified”
“Biomechanics”
Biomechanics of the Unified Osteopathic Field
March 22-23, 2012 C. L. Nicodemus, DO, PhD
2

It all starts with Dr. Still. He was:
An original
Unique
Creative
A Visionary
Correct
“_____________________________________”
March 22-23, 2012 C. L. Nicodemus, DO, PhD
3
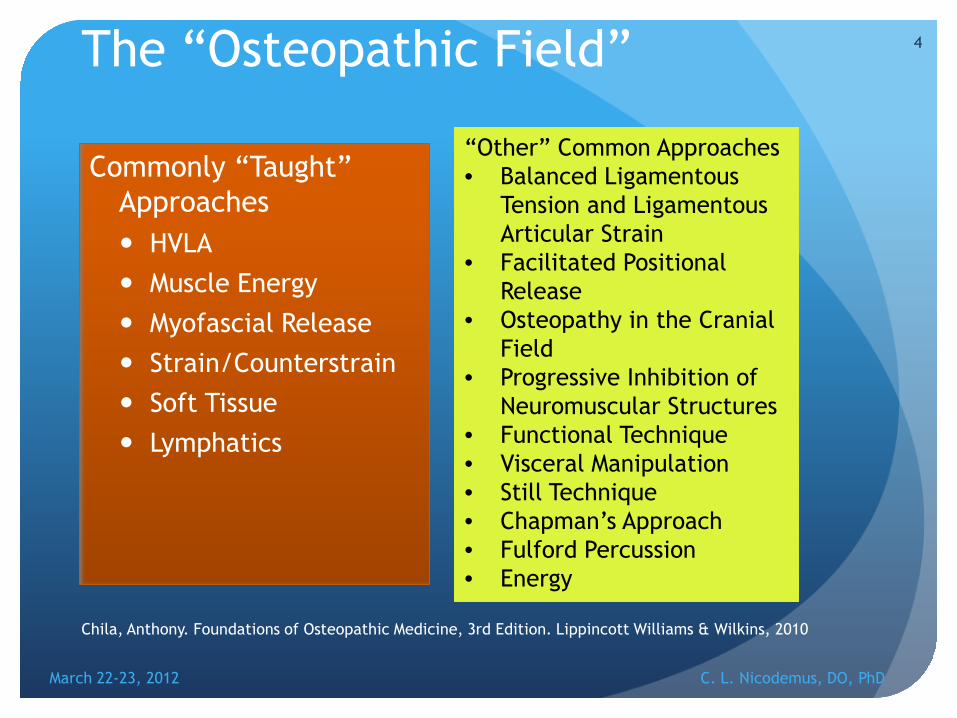
The “Osteopathic Field” Commonly “Taught”
Approaches HVLA Muscle Energy Myofascial Release Strain/Counterstrain Soft Tissue Lymphatics
4
“Other” Common Approaches • Balanced Ligamentous
Tension and Ligamentous Articular Strain
• Facilitated Positional Release
• Osteopathy in the Cranial Field
• Progressive Inhibition of Neuromuscular Structures
• Functional Technique • Visceral Manipulation • Still Technique • Chapman’s Approach • Fulford Percussion • Energy
March 22-23, 2012 C. L. Nicodemus, DO, PhD
Chila, Anthony. Foundations of Osteopathic Medicine, 3rd Edition. Lippincott Williams & Wilkins, 2010

Unified Field Theory
Einstein's attempt to unify the General Theory of Relativity with electromagnetism
5
March 22-23, 2012 C. L. Nicodemus, DO, PhD
Wrong Field Theory

Unified Osteopathic Field Theory
All theories of manual medicine are based on manipulating the same basic human tissues.
Further, all human tissues exhibit the same fundamental biomechanical property, namely, viscoelasticity.
6
March 22-23, 2012 C. L. Nicodemus, DO, PhD

Many different aspects/models
Fascial Model- Distensability, tested with motion testing and fascial pull.
Fluid model- circulation, tested with doppler ultrasound, perfusion studies, or palpation.
Neurological Model- electrochemical information, tested with palpation and motion testing, EMG.
Biomechanical Model- Inherent and induced-Tested with palpation, ROM, sensing
Energetic Model- temperature changes, electricity, etc….
7
March 22-23, 2012 C. L. Nicodemus, DO, PhD

What is common among these approaches?
March 22-23, 2012 C. L. Nicodemus, DO, PhD
8
Commonly “Taught” Approaches HVLA Muscle Energy Myofascial Release Strain/Counterstrain Soft Tissue Lymphatics
“Other” Common Approaches • Balanced Ligamentous
Tension and Ligamentous Articular Strain
• Facilitated Positional Release
• Osteopathy in the Cranial Field
• Progressive Inhibition of Neuromuscular Structures
• Functional Technique • Visceral Manipulation • Still Technique • Chapman’s Approach • Fulford Percussion • Energy

Hands and Tissues (and more)
It is called Manipulative Medicine because hands manipulate tissues
We also engage our mind, energy, intuition, spirit
It is very difficult to measure the latter
So we focus on the former
March 22-23, 2012 C. L. Nicodemus, DO, PhD
9

Biomechanics
“the application of mechanical laws to living structures.”
10
Saunders Comprehensive Veterinary Dictionary, 3 ed. © 2007 Elsevier, Inc.
March 22-23, 2012 C. L. Nicodemus, DO, PhD
Fundamental Biomechanics Review
11
March 22-23, 2012 C. L. Nicodemus, DO, PhD
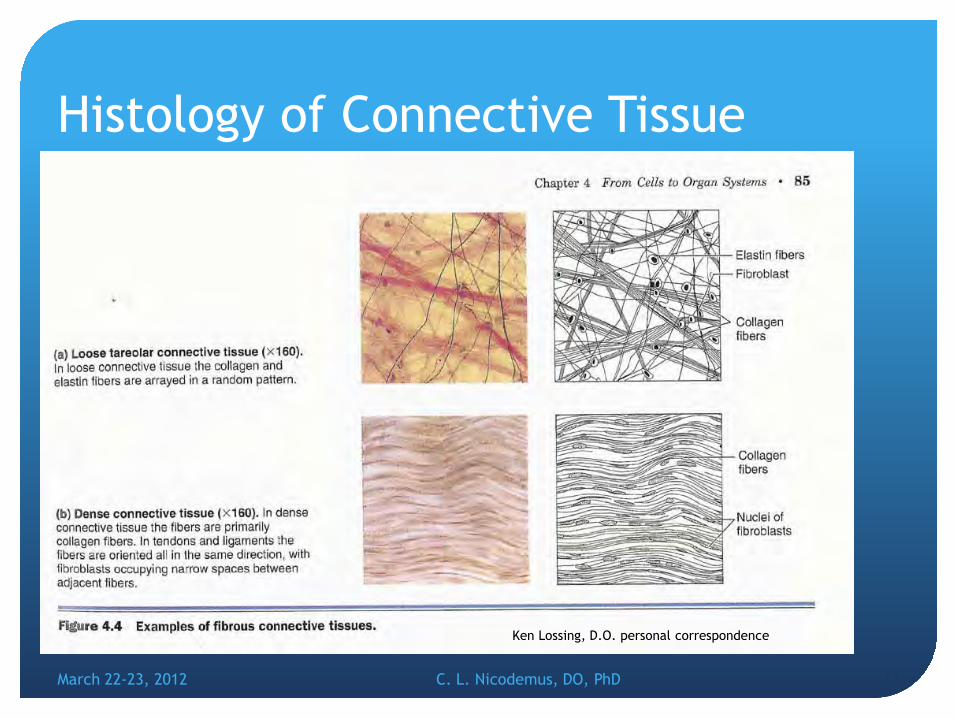
Histology of Connective Tissue
March 22-23, 2012 12 C. L. Nicodemus, DO, PhD
Ken Lossing, D.O. personal correspondence

Origin and Classes of Connective Tissue
March 22-23, 2012 C. L. Nicodemus, DO, PhD 13
http://classes.midlandstech.edu/carterp/Courses/bio210/chap04/
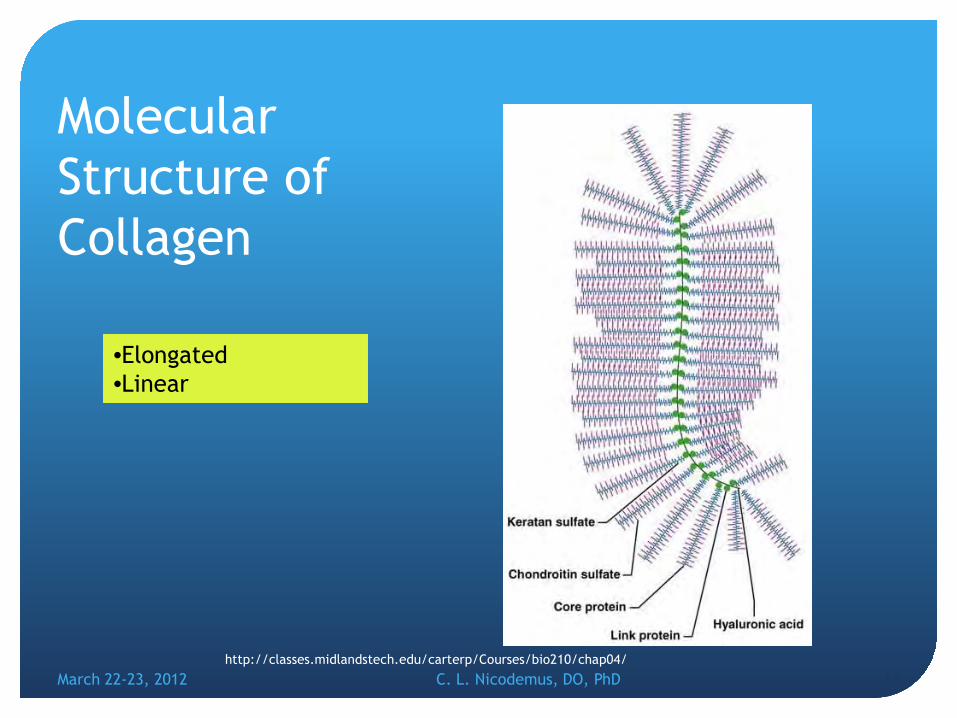
Molecular Structure of Collagen
March 22-23, 2012 C. L. Nicodemus, DO, PhD 14 http://classes.midlandstech.edu/carterp/Courses/bio210/chap04/
•Elongated •Linear

Other Components
March 22-23, 2012 C. L. Nicodemus, DO, PhD 15 http://classes.midlandstech.edu/carterp/Courses/bio210/chap04/
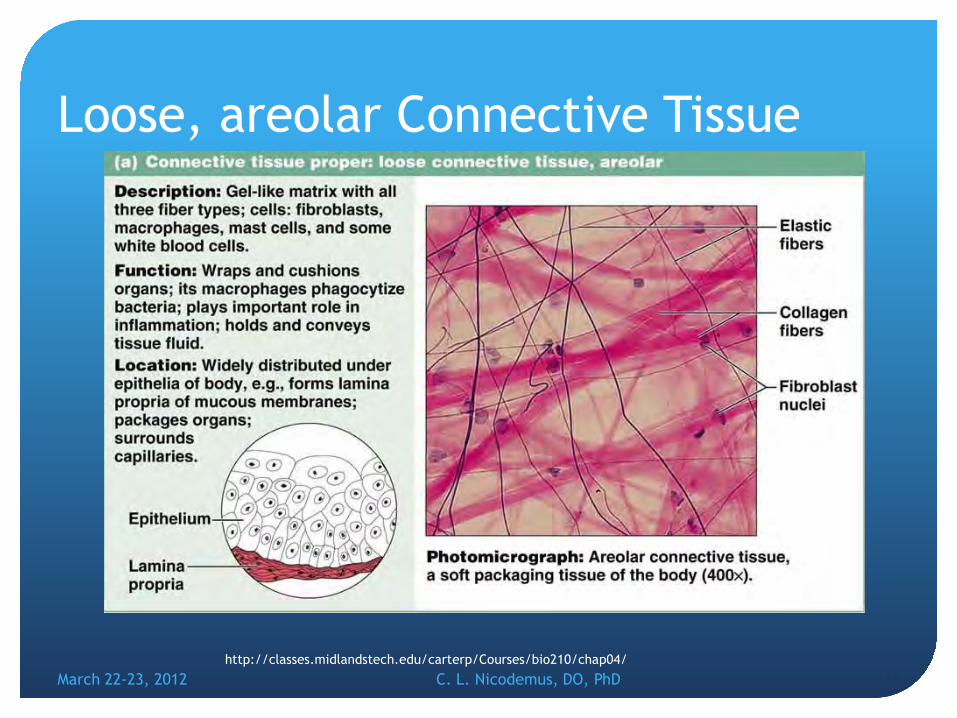
Loose, areolar Connective Tissue
March 22-23, 2012 C. L. Nicodemus, DO, PhD 16 http://classes.midlandstech.edu/carterp/Courses/bio210/chap04/

Loose, adipose Connective Tissue
March 22-23, 2012 C. L. Nicodemus, DO, PhD 17 http://classes.midlandstech.edu/carterp/Courses/bio210/chap04/

Loose, recticular Connective Tissue
March 22-23, 2012 C. L. Nicodemus, DO, PhD 18 http://classes.midlandstech.edu/carterp/Courses/bio210/chap04/

Dense, regular Connective Tissue
March 22-23, 2012 C. L. Nicodemus, DO, PhD 19 http://classes.midlandstech.edu/carterp/Courses/bio210/chap04/
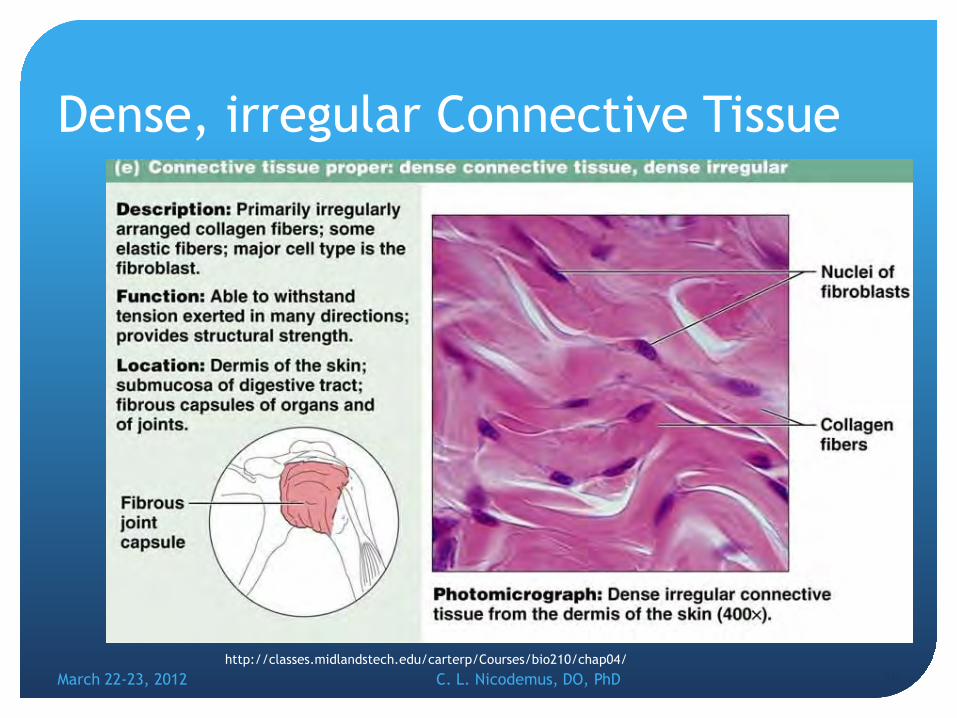
Dense, irregular Connective Tissue
March 22-23, 2012 C. L. Nicodemus, DO, PhD 20 http://classes.midlandstech.edu/carterp/Courses/bio210/chap04/

Types of Connective Tissue
21 March 22-23, 2012 C. L. Nicodemus, DO, PhD
Ken Lossing, D.O. personal correspondence

Fascia The fascia is a loose, areolar connective tissue
composed of:
collagen-( literally glue –making) 14 types , most common is type 1 (90%)
ground substance
fibrin
Elastin- maintains the tensile strength of connective tissue
The collagen fibers are connected to other collagen fibers through chemical bonds.
22 March 22-23, 2012 C. L. Nicodemus, DO, PhD

Effects of loading
23
March 22-23, 2012 C. L. Nicodemus, DO, PhD
Chila, Anthony. Foundations of Osteopathic Medicine, 3rd Edition. Lippincott Williams & Wilkins, 2010
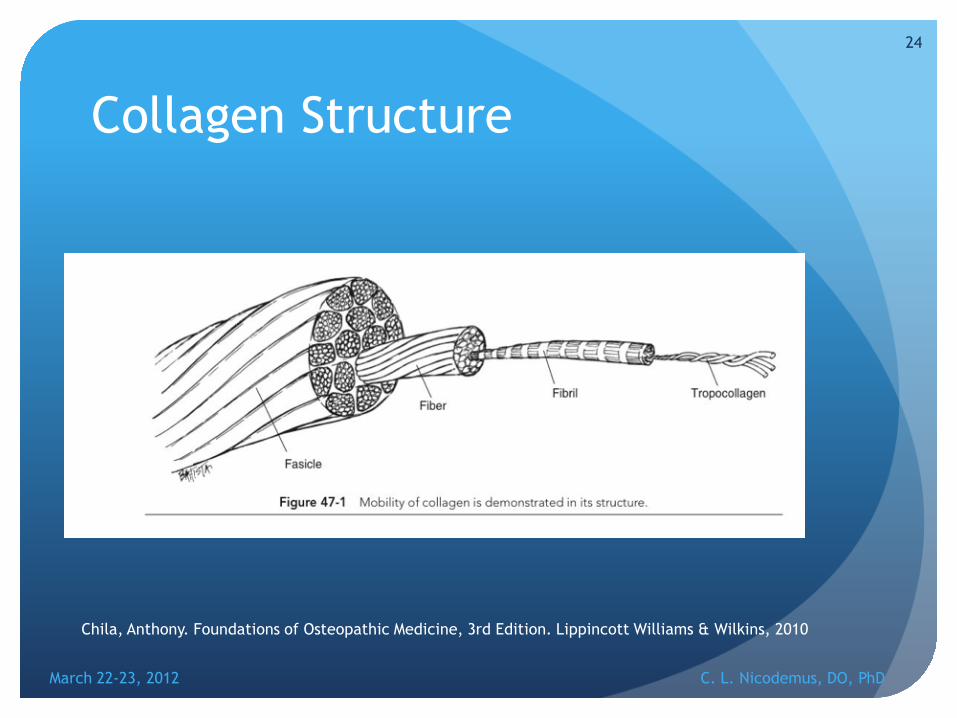
Collagen Structure
24
March 22-23, 2012 C. L. Nicodemus, DO, PhD
Chila, Anthony. Foundations of Osteopathic Medicine, 3rd Edition. Lippincott Williams & Wilkins, 2010
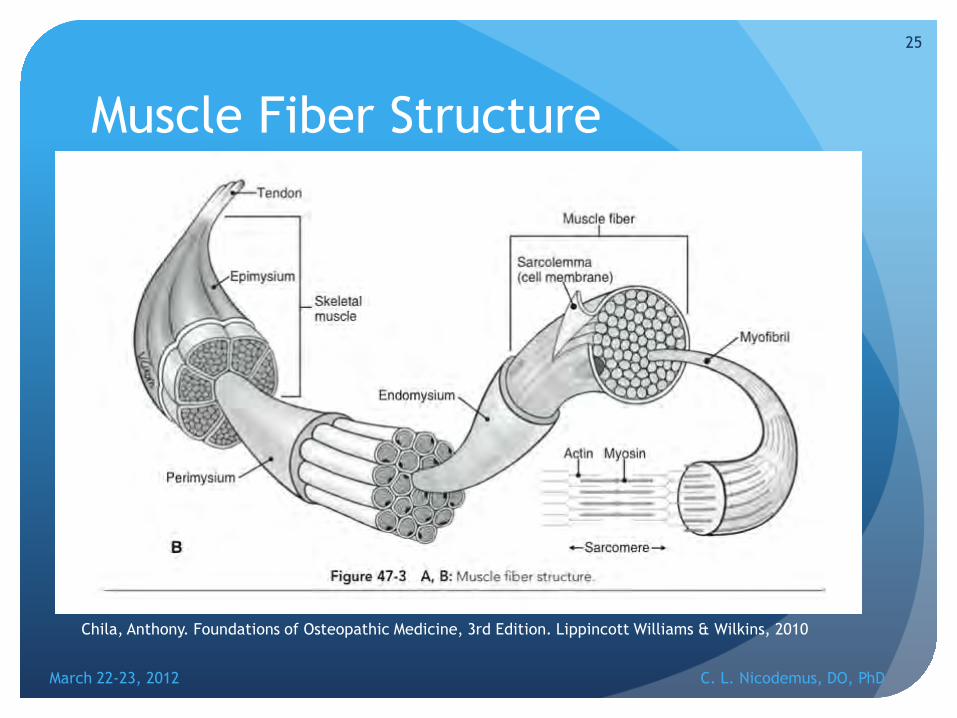
Muscle Fiber Structure
25
March 22-23, 2012 C. L. Nicodemus, DO, PhD
Chila, Anthony. Foundations of Osteopathic Medicine, 3rd Edition. Lippincott Williams & Wilkins, 2010

Terminology
26
terminology [tur-muh-nol-uh-jee]
March 22-23, 2012 C. L. Nicodemus, DO, PhD

Strain and Stress
Strain: is a measure of the degree or intensity of deformation. Elongation per unit gage length. Units of strain – mm/mm, in/in STRAIN = ΔL/L
Stress: force per unit area, may be shear stress, tensile stress, or compressive stress. Units of stress- N/m2 (pascal), dyn/cm2, lbs/in2. STRESS=F/A
Shear stress is a “cross fiber” action. Units of stress- N/m2 (pascal), dyn/cm2, lbs/in2. SHEAR STRESS = F’/A
27
March 22-23, 2012 C. L. Nicodemus, DO, PhD

Elastic Deformation
IDEAL or PURELY elastic
Stress > PE > KE
E= elastic modulus = Δ stress/Δ strain
28
Stre
ss
Strain
Strain
E
1
loading unloading
March 22-23, 2012 C. L. Nicodemus, DO, PhD
Think rubber band
Ken Lossing, DO
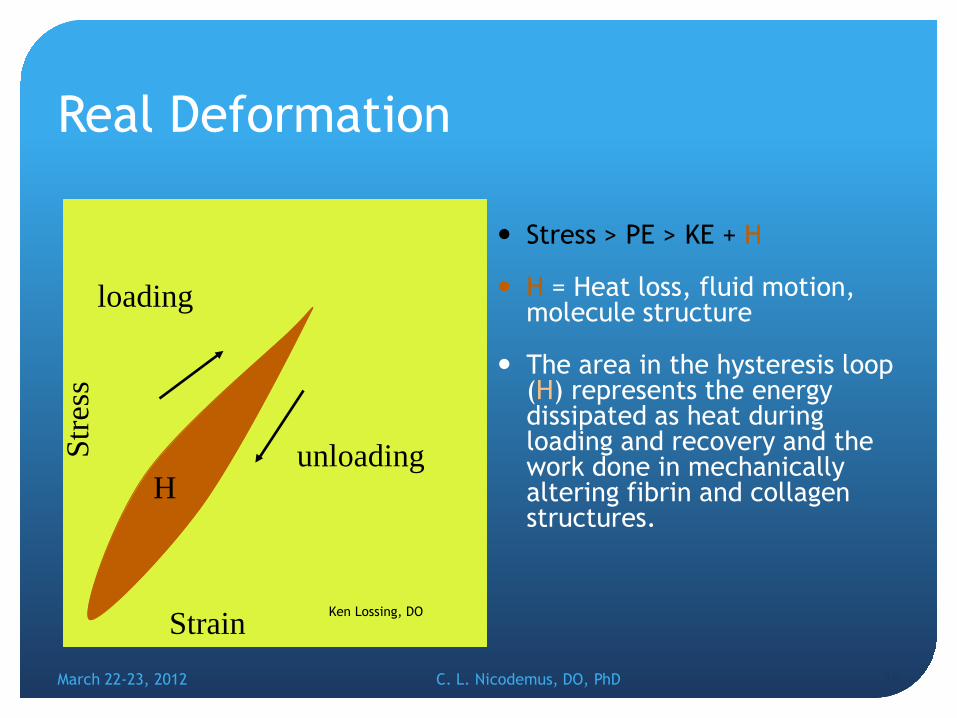
Real Deformation
Stress > PE > KE + H
H = Heat loss, fluid motion, molecule structure
The area in the hysteresis loop (H) represents the energy dissipated as heat during loading and recovery and the work done in mechanically altering fibrin and collagen structures.
29
Stre
ss
Strain
loading
unloading H
March 22-23, 2012 C. L. Nicodemus, DO, PhD
Ken Lossing, DO

Actual Data for a Tendon (rat)
30
Repetitive cycles change the response
10 cycles = stable
March 22-23, 2012 C. L. Nicodemus, DO, PhD
http://www.engin.umich.edu/class/bme456/

Creep and Hysteresis
31
? Hysteresis??
March 22-23, 2012 C. L. Nicodemus, DO, PhD

Creep I
32
March 22-23, 2012 C. L. Nicodemus, DO, PhD
http://www.engin.umich.edu/class/bme456/

Creep II
33
March 22-23, 2012 C. L. Nicodemus, DO, PhD
http://www.engin.umich.edu/class/bme456/
Viscoelasticity
having viscous as well as elastic properties
a combination of viscous and elastic properties in a material, with the relative contribution of each being
, , , and . [and
]
34
March 22-23, 2012 C. L. Nicodemus, DO, PhD

Actual Data for a Tendon (rat)
35
Repetitive cycles change the response
10 cycles = stable
March 22-23, 2012 C. L. Nicodemus, DO, PhD
http://www.engin.umich.edu/class/bme456/
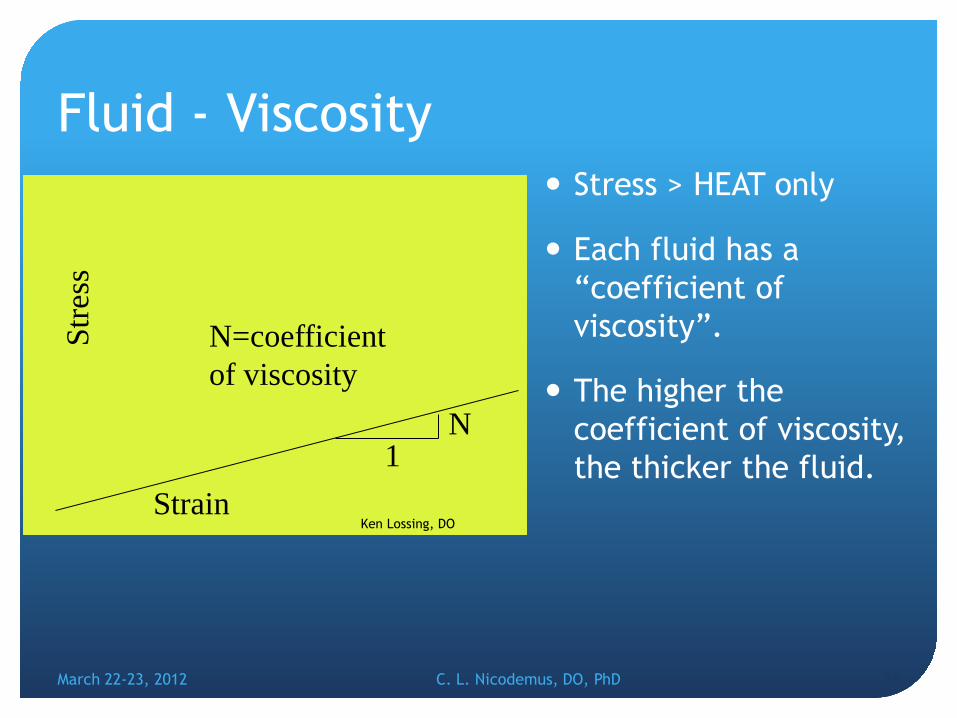
Fluid - Viscosity Stress > HEAT only
Each fluid has a “coefficient of viscosity”.
The higher the coefficient of viscosity, the thicker the fluid.
36
Stre
ss
Strain
N=coefficient of viscosity
1 N
March 22-23, 2012 C. L. Nicodemus, DO, PhD
Ken Lossing, DO

Viscosity
March 22-23, 2012 C. L. Nicodemus, DO, PhD
37
Catsup
Peanut Butter
OR

Viscoelastic change Resulting stress is not
only a function of strain, and temperature, but also the strain rate, in other words the speed at which a load ( strain) is applied will affect the amount of stress in the tissue. This is called “time dependant material behavior”.
Rhythm of the tissue!
38
Strain
Stre
ss
Increasing stiffness
March 22-23, 2012 C. L. Nicodemus, DO, PhD
Ken Lossing, DO
Strain Rate
Temperature

March 22-23, 2012 C. L. Nicodemus, DO, PhD
39

Creep and Hysteresis
When a load (stress) is applied to a viscoelastic material, molecular bonding is re-arranged and thus the material elongates or “creeps”.
As the re-arrangement occurs, a back-stress develops. When the back stress matches the applied stress, creep stops.
When the load is released, the back stress returns, the original length returns (with losses of energy due to the heat of mechanical re-arrangement). This is hysteresis.
Visco = creep; Back stress return = elastic
40
March 22-23, 2012 C. L. Nicodemus, DO, PhD

Viscoelasticity
having viscous as well as elastic properties
The property of a substance of exhibiting both elastic and viscous behavior, the application of stress causing temporary deformation if the stress is quickly removed but permanent deformation if it is maintained
a combination of viscous and elastic properties in a material, with the relative contribution of each being dependent on time, temperature, stress, and strain rate. [and electrical field]
41
March 22-23, 2012 C. L. Nicodemus, DO, PhD
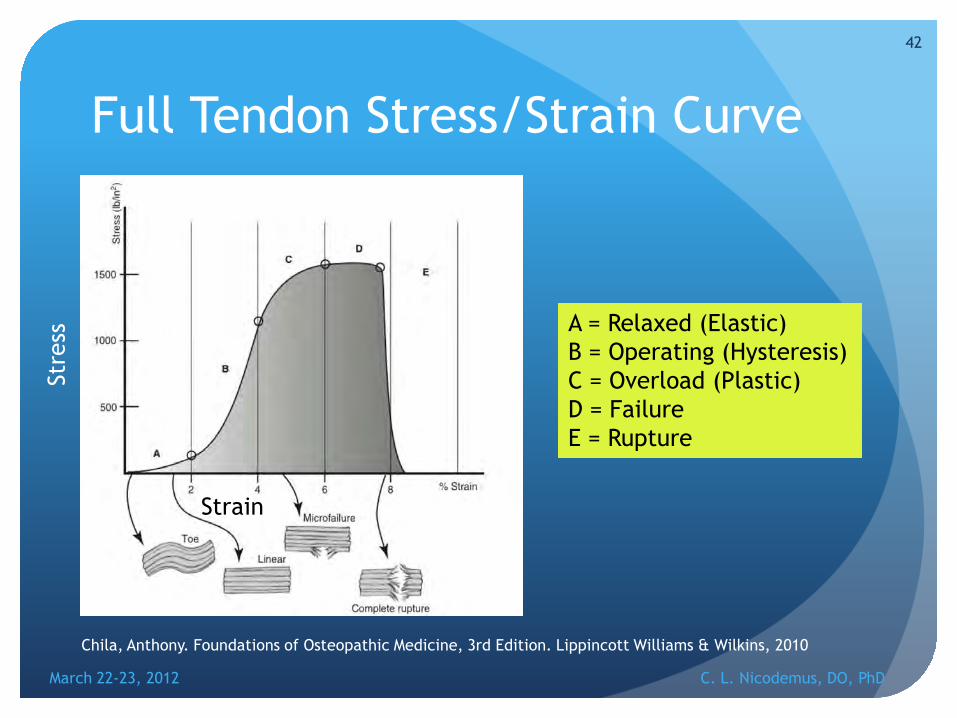
Full Tendon Stress/Strain Curve
42
A = Relaxed (Elastic) B = Operating (Hysteresis) C = Overload (Plastic) D = Failure E = Rupture
March 22-23, 2012 C. L. Nicodemus, DO, PhD
Chila, Anthony. Foundations of Osteopathic Medicine, 3rd Edition. Lippincott Williams & Wilkins, 2010
Stre
ss
Strain

Elastic Deformation A strain applied to a tissue will
result in a stress in the tissue
P=Proportionality limit-linear until then, and loading is matched with unloading
E=elastic limit
Y= yield strength, considerable elongation occurs without corresponding increase of stress
PD= Plastic deformation area
U=ultimate strength
R=rupture
43
Strain
Stre
ss
P E
Y
U
R
Strain
unloading
PD
March 22-23, 2012 C. L. Nicodemus, DO, PhD
Ken Lossing, DO
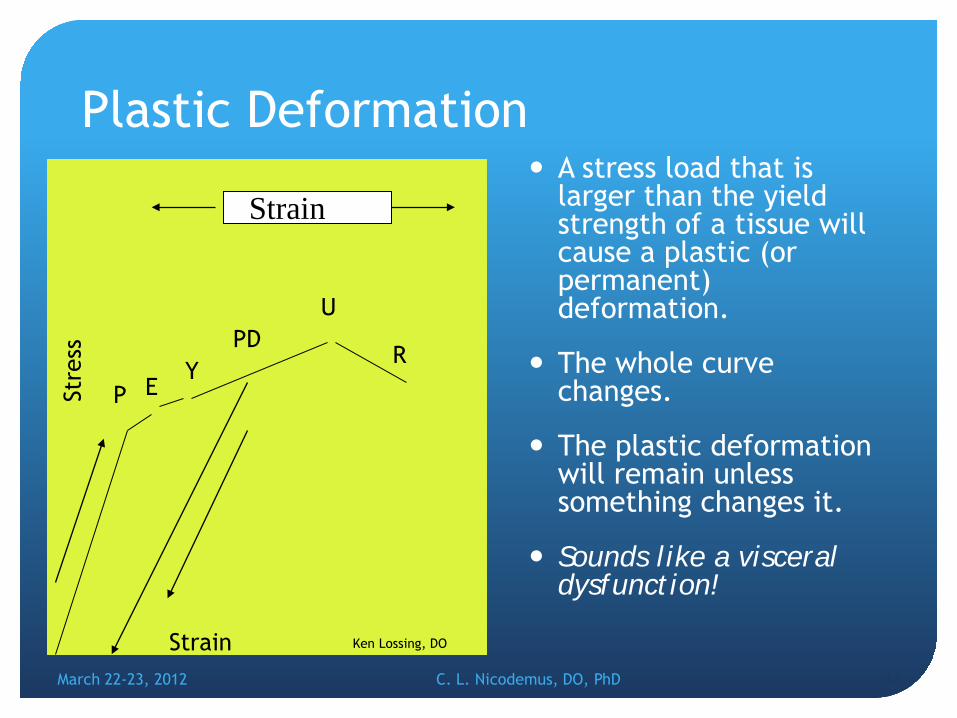
Plastic Deformation A stress load that is
larger than the yield strength of a tissue will cause a plastic (or permanent) deformation.
The whole curve changes.
The plastic deformation will remain unless something changes it.
Sounds like a visceral dysfunction!
44
Strain
Stre
ss
P E Y
U
R
Strain
March 22-23, 2012 C. L. Nicodemus, DO, PhD
Ken Lossing, DO
PD
Summary
March 22-23, 2012 C. L. Nicodemus, DO, PhD
45
Pizoelectricity
Chila, Anthony. Foundations of Osteopathic Medicine, 3rd Edition. Lippincott Williams & Wilkins, 2010
Force Effects in Connective Tissues •Elastic Deformation •Plastic Deformation •Viscosity •Stress •Strain •Creep •Hysteresis •Temperature •Density

Pizoelectric properties of Collagen Transducer (Stress > Current > vibration)
Biphasic signal (- load, + release)
Stress related signal (Current α Stress)
Stimulates osteocytes (- charge)
Stimulates and directs the migration of electrically sensitive cells (chemotaxis)
Activates cells (electro-sensitive cells)
46
Chila, Anthony. Foundations of Osteopathic Medicine, 3rd Edition. Lippincott Williams & Wilkins, 2010
March 22-23, 2012 C. L. Nicodemus, DO, PhD

Acupuncture is a pizoelectric fascial phenomenon.
March 22-23, 2012 C. L. Nicodemus, DO, PhD
47
Now look at applications
Visceral
Mechanical
March 22-23, 2012 C. L. Nicodemus, DO, PhD
48

Visceral (Broad) Ligament
March 22-23, 2012 C. L. Nicodemus, DO, PhD
49
Sacral Ligament
VS
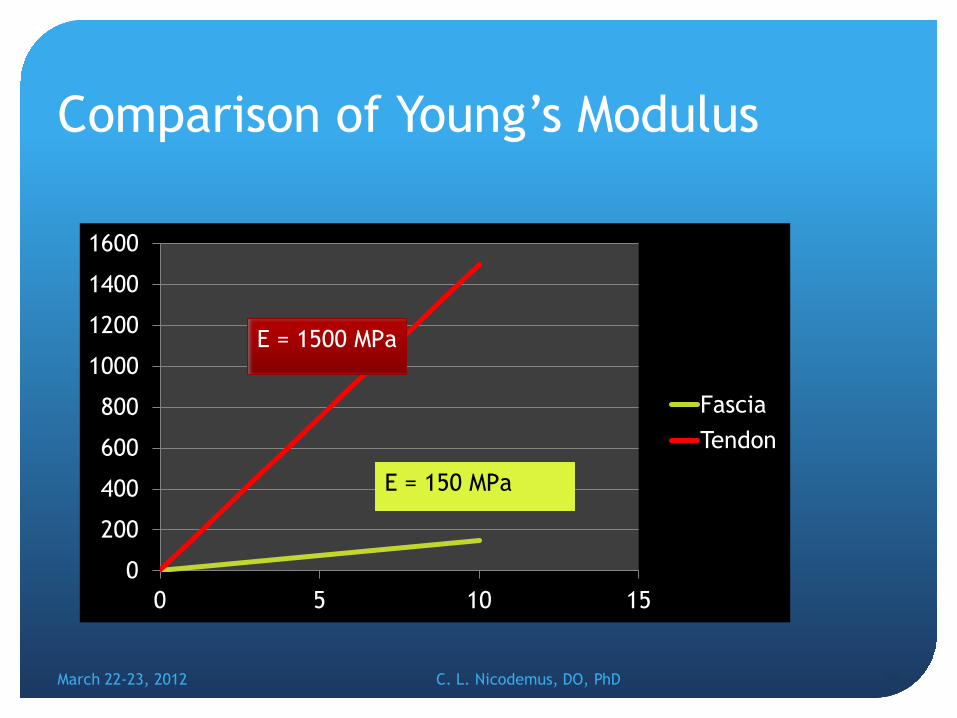
Comparison of Young’s Modulus
March 22-23, 2012 C. L. Nicodemus, DO, PhD 50
0
200
400
600
800
1000
1200
1400
1600
0 5 10 15
Fascia Tendon
E = 150 MPa
E = 1500 MPa

As Applied to Visceral Dysfunction
Constantly applied loads on visceral ligaments and fascia will have caused them to maximally elongate and to stiffen as a result of the molecular re-arrangement.
Releasing the cause of the chronic loading by re-balancing muscles, reducing joint restrictions, and balancing fascial strain patterns, internal stress of the tissues is reduced.
Reduction of the internal stress and stiffness causes release of constrained fluids held with in, such a lymph, venus and arteriol vessels.
Circulation returns, pain is reduced, and function returns.
Temperature changes occur; heat of inflammation is reduced, heat of circulation is increased, and heat of tissue molecular re-arrangement is increased.
51
March 22-23, 2012 C. L. Nicodemus, DO, PhD

Visceral Dysfunction
“Impaired or altered mobility or motility of the visceral system and related fascial, neurological, vascular, skeletal, and lymphatic elements”. American Osteopathic Association Glossary, 2011
This is reflected in abnormal motion tests, showing a change in the distensability of the attachments, or a change in their normal viscoelasticity.
52
March 22-23, 2012 C. L. Nicodemus, DO, PhD
SO,(to quote Dr. Lossing):
If there is a visceral dysfunction, the ligament has a certain amount of strain stored (potential) energy- “potency”, in a certain direction, and that tissue has a certain strain rate (speed) that it will respond to. This results in an altered viscoelasticity curve for that ligament. ( The viscosity is more, the elasticity is less).
When the internal strain is exactly matched, by application of force, direction, and speed, the tissue will change. Increasing the fluid exchange should accelerate the change. In the process there is a dissipation of heat, movement of fluid, and a restructuring of the elasticity curve.
53
March 22-23, 2012 C. L. Nicodemus, DO, PhD

Multiple strains The body generally
accumulates many strains over a life time. The strain takes a certain amount of force to hold it there, exerting tension into the fascia. The one with the most force will have the biggest effect on the fascia.
Therefore, removing the biggest strain will have the largest effect on the body
54
50
20
30
10
March 22-23, 2012 C. L. Nicodemus, DO, PhD
Ken Lossing, DO
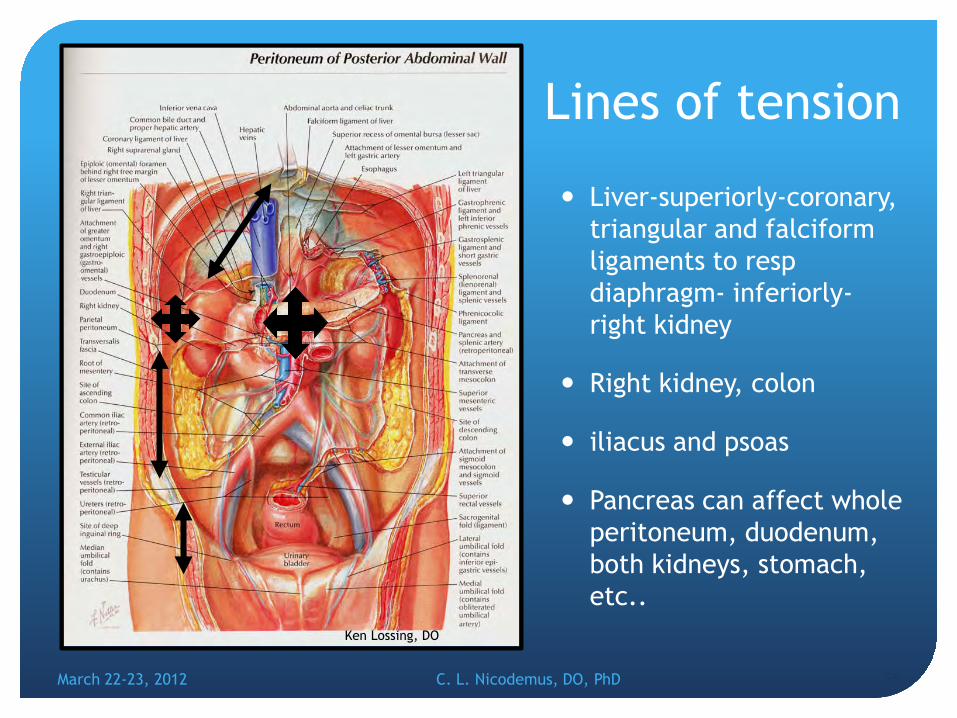
Lines of tension
Liver-superiorly-coronary, triangular and falciform ligaments to resp diaphragm- inferiorly- right kidney
Right kidney, colon
iliacus and psoas
Pancreas can affect whole peritoneum, duodenum, both kidneys, stomach, etc..
55 March 22-23, 2012 C. L. Nicodemus, DO, PhD
Ken Lossing, DO
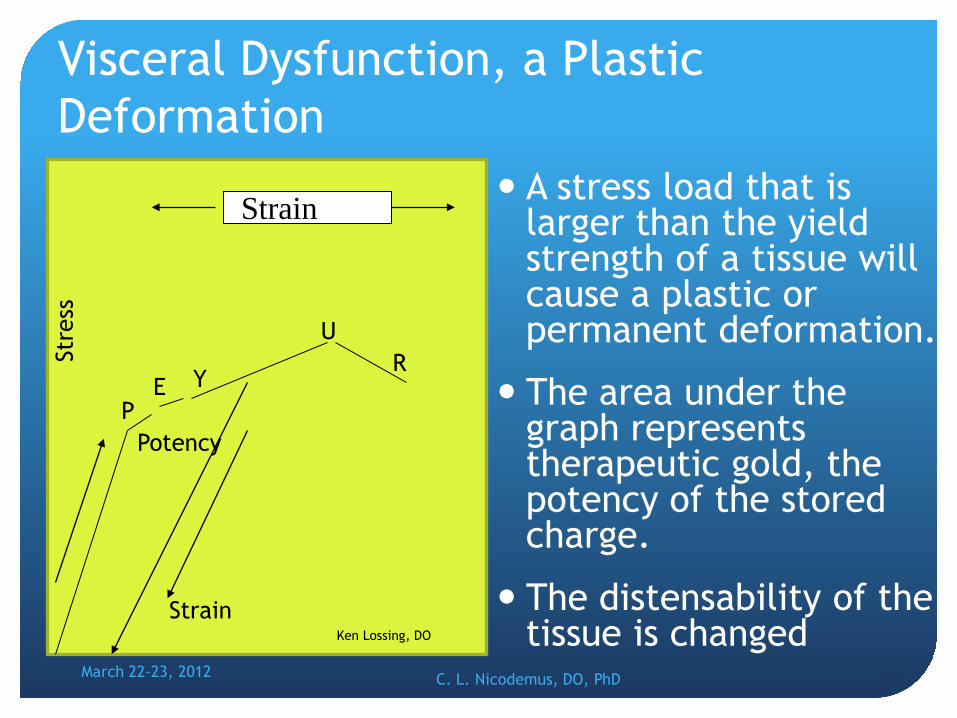
Visceral Dysfunction, a Plastic Deformation
A stress load that is larger than the yield strength of a tissue will cause a plastic or permanent deformation.
The area under the graph represents therapeutic gold, the potency of the stored charge.
The distensability of the tissue is changed
56
Strain
Stre
ss
P E Y
U R
Strain
Potency
March 22-23, 2012 C. L. Nicodemus, DO, PhD
Ken Lossing, DO

Ligaments and Fluid Shift With minimal additional
mechanical tension in ligaments, the first fluid vessels to be compressed (compromised) will be those of lowest pressure, the lymphatic vessels- relative edema, retention of metabolic byproducts.
With increased tension, comes venous congestion, increased retention of metabolic byproducts
and with more tension comes arterial compression- decreased nutrition, oxygen, and eventual death.
“obstructive lymphedema” - Robbins Pathologic Basis of Disease 57
Artery Vein
Lymph vessel
March 22-23, 2012 C. L. Nicodemus, DO, PhD
Ken Lossing, DO
Nerve
Neurovascular Bundle

Barriers
Physiologic Barrier: the limit of active motion.
Anatomic Barrier: The limit of motion imposed by anatomic structure: the limit of passive motion. Neutral: The point of balance of an articular surface from which all the motions physiologic to that articulation may take place
58 March 22-23, 2012 C. L. Nicodemus, DO, PhD
Ken Lossing, DO

Mechanical
End feel
Tightness
Bogginess
Hypertonic
Stiff
March 22-23, 2012 C. L. Nicodemus, DO, PhD
59
Motion testing Elastic Barrier:
The range between the physiologic barrier and anatomic barrier of motion in which passive ligamentous stretching occurs before tissue disruption.
If we move a ligament to its physiological barrier, it removes any slack in the ligament and starts to engage the elasticity of the ligament At this point, we are still below the elasticity limit of that tissue.
When we remove the straining force, the ligament returns to it’s original configuration- an elastic deformation.
60
March 22-23, 2012 C. L. Nicodemus, DO, PhD

This Applies to the whole body
Embryology, Histology , Gross anatomy, micro anatomy.
Ear, nose and throat
Visceral System
Lymphatic system
Nervous System
Endocrine system, immune system
Musculoskeletal System
61
March 22-23, 2012 C. L. Nicodemus, DO, PhD

Summary
Therefore, we need to expand our vision of osteopathy, to have the same vision as Dr Still.
All problems/symptoms that a patient experiences may have a functional component that is treatable.
Most of how we diagnose and treat is a function of its viscoelasticity….
No matter which dysfunction or treatment model we use.
March 22-23, 2012 C. L. Nicodemus, DO, PhD
62
A very unifying idea!

63
March 22-23, 2012 C. L. Nicodemus, DO, PhD
Niles, Superdog
Thank you! Any questions?