understanding the complement cascade and its role in cold … · cold agglutinin disease is an...
TRANSCRIPT
1M-CAgD-US-3006 February 2018
Understanding the Complement Cascade and Its Role inCold Agglutinin Disease
2M-CAgD-US-3006M-CAgD-US-3006 February 2018
Instructions
This information is provided as an educational resource for healthcare providers. It is not intended to be a substitute for review of the underlying reference materials and scientific literature. Healthcare providers should make all treatment decisions based on their medical judgement and the clinical profile of the individual patient. The following document cannot be copied, modified, used or distributed without the express written consent of Bioverativ.

3M-CAgD-US-3006
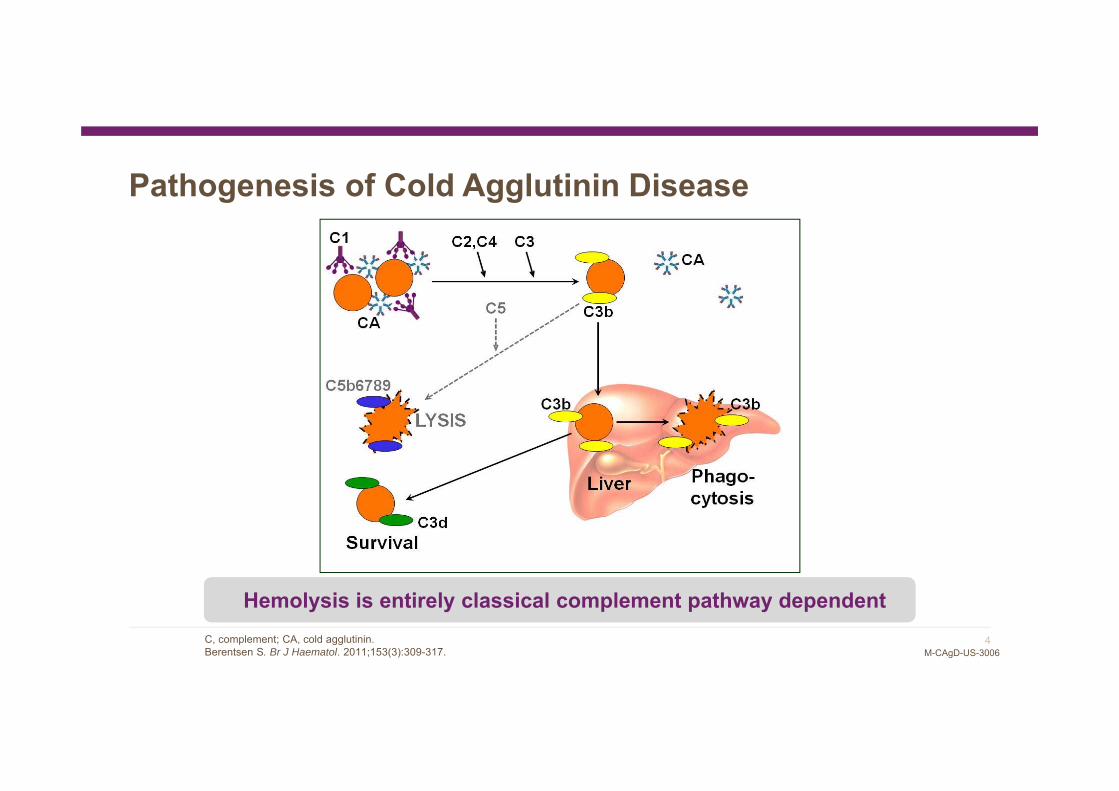
Pathogenesis of Cold Agglutinin Disease
LPD, lymphoproliferative disorder.Randen U, et al. Haematologica. 2014;99(3):497-504.
• Cold agglutinin–
associated
lymphoproliferative bone
marrow disorder
• A distinct type of LPD
• Cold agglutinin–
associated
lymphoproliferative bone
marrow disorder
• A distinct type of LPD
4M-CAgD-US-3006
Pathogenesis of Cold Agglutinin Disease
Hemolysis is entirely classical complement pathway dependentHemolysis is entirely classical complement pathway dependentC, complement; CA, cold agglutinin.Berentsen S. Br J Haematol. 2011;153(3):309-317.
5M-CAgD-US-3006
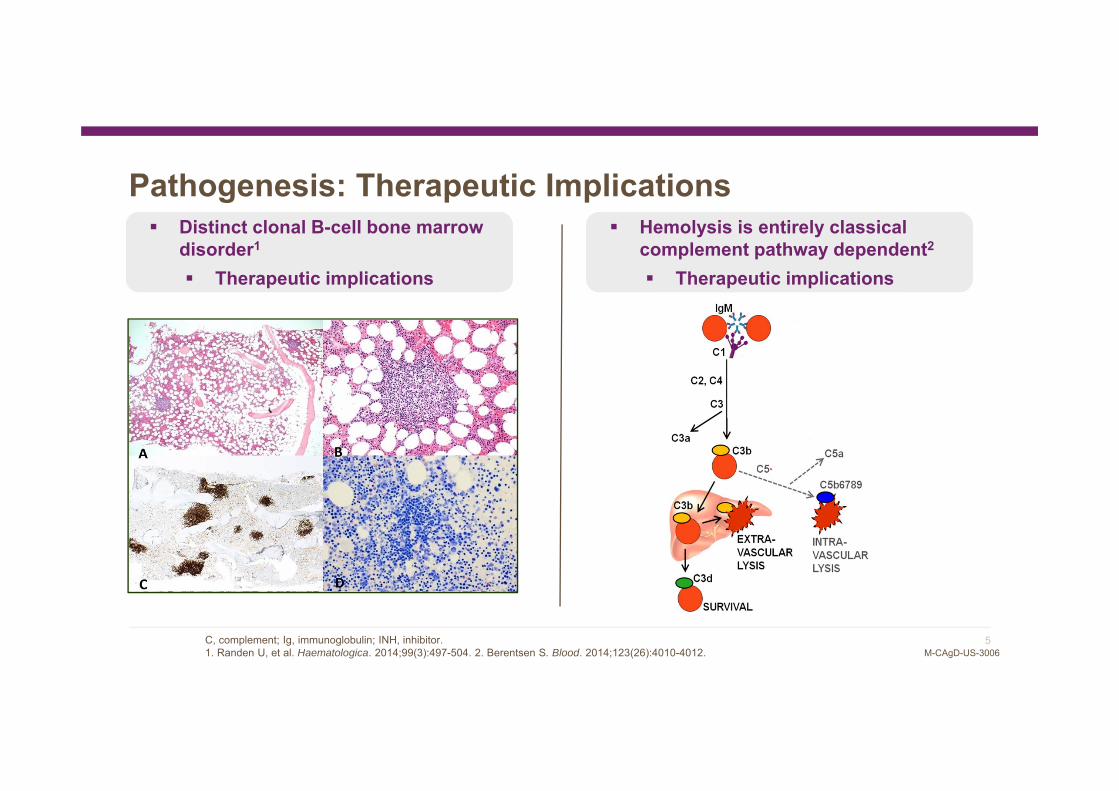
Pathogenesis: Therapeutic Implications Hemolysis is entirely classical
complement pathway dependent2
Therapeutic implications
Distinct clonal B-cell bone marrow disorder1
Therapeutic implications
C, complement; Ig, immunoglobulin; INH, inhibitor.1. Randen U, et al. Haematologica. 2014;99(3):497-504. 2. Berentsen S. Blood. 2014;123(26):4010-4012.
BIVV009BIVV009 is under
development and is not approved for the treatment of
cold agglutinin disease

6M-CAgD-US-3006
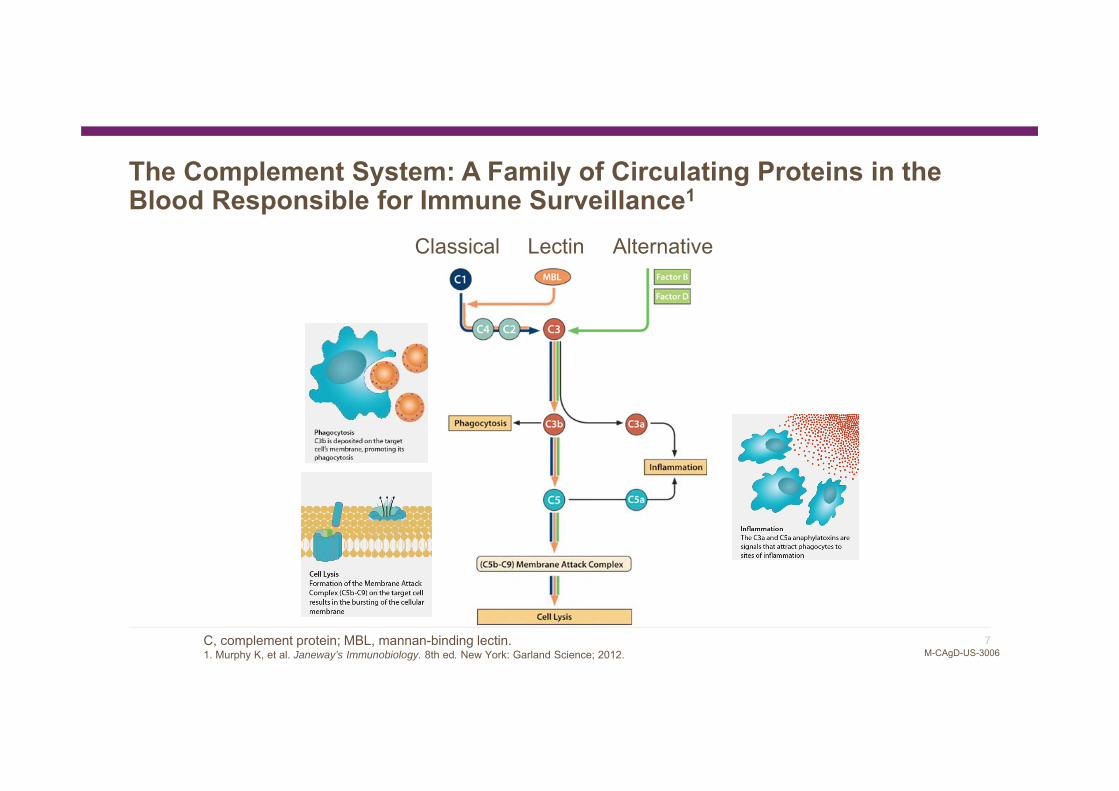
The Complement System: A Family of Circulating Proteins in the Blood Responsible for Immune Surveillance1
Classical Lectin Alternative
C, complement protein; MBL, mannan-binding lectin.1. Murphy K, et al. Janeway’s Immunobiology. 8th ed. New York: Garland Science; 2012.
7M-CAgD-US-3006
The Complement System: A Family of Circulating Proteins in the Blood Responsible for Immune Surveillance1
Classical Lectin Alternative
C, complement protein; MBL, mannan-binding lectin.1. Murphy K, et al. Janeway’s Immunobiology. 8th ed. New York: Garland Science; 2012.
8M-CAgD-US-3006
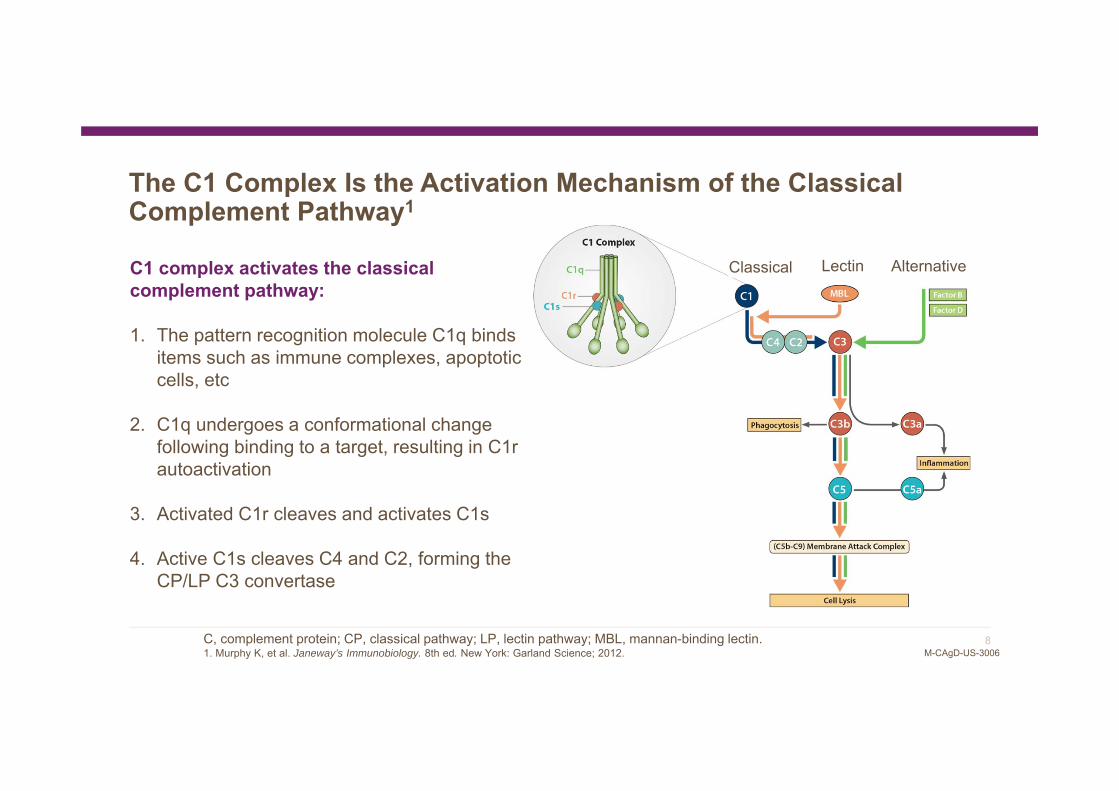
The C1 Complex Is the Activation Mechanism of the Classical Complement Pathway1
C1 complex activates the classical complement pathway:
1. The pattern recognition molecule C1q binds items such as immune complexes, apoptotic cells, etc
2. C1q undergoes a conformational change following binding to a target, resulting in C1r autoactivation
3. Activated C1r cleaves and activates C1s
4. Active C1s cleaves C4 and C2, forming the CP/LP C3 convertase
C, complement protein; CP, classical pathway; LP, lectin pathway; MBL, mannan-binding lectin.1. Murphy K, et al. Janeway’s Immunobiology. 8th ed. New York: Garland Science; 2012.
Classical Lectin Alternative

9M-CAgD-US-3006
The Classical Pathway Activates Upon Binding to Antibodies: A Bridge Between the Innate and Adaptive Immune Systems
C, complement protein; IgG, immunoglobulin G.1. Murphy K, et al. Janeway’s Immunobiology. 8th ed. New York: Garland Science; 2012.

10M-CAgD-US-3006
Cold Agglutinin Disease
Overview:• Autoimmune hemolytic anemia1
• Prevalence1,2: ~1/60,000–1/100,000; incidence3,4: ~1/300,000–1/1,000,000 • ~5000 patients in the United States• Patients are often elderly2 and present with anemia, fatigue, hemoglobinuria, and
acrocyanosis4
Etiology: • Primary (idiopathic)1
• Secondary: caused by an underlying condition (eg, infection, malignancy)• Majority of patients have detectable clonal B cells responsible for the production
of an autoantibody that binds to RBC <37°C (cold)5
Clinical symptoms: • Frequent need for transfusions1
• Chronic anemia with related symptoms (decreased quality of life)4
• Agglutination-associated symptoms4
• Thromboembolic complications4 CA activation in the classical pathway6
C, complement protein; CA, cold agglutinin; RBC, red blood cell.1. Berentsen S, et al. Haematologica. 2006;91(4):460–466. 2. Gertz MA. Hematol Am Soc Hematol Educ Program.2006;19–23. 3. Sokol RJ, et al. Br Med J. 1981;282:2023–2027. 4. Mullins M, et al. Blood Adv. 2017;1(13):839–848. 5. Bass GF, et al. Autoimmunity Rev. 2014;13(4-5):560–564. 6. Shi J, et al. Blood. 2014;26(123):4015–4022.
11M-CAgD-US-3006
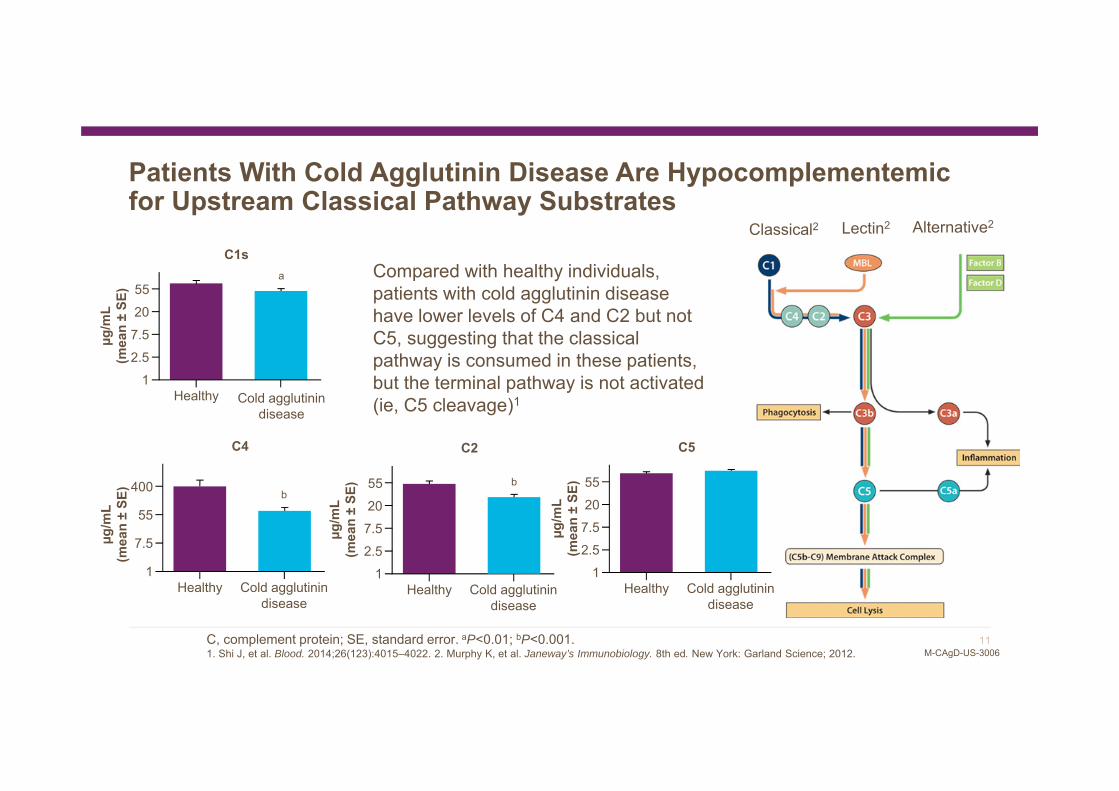
Compared with healthy individuals, patients with cold agglutinin disease have lower levels of C4 and C2 but not C5, suggesting that the classical pathway is consumed in these patients, but the terminal pathway is not activated (ie, C5 cleavage)1
Patients With Cold Agglutinin Disease Are Hypocomplementemic for Upstream Classical Pathway Substrates
55
2.51
C5
Healthy Cold agglutinin disease
µg/m
L(m
ean
±SE
)
7.520
µg/m
L(m
ean
±SE
)
C2
Healthy Cold agglutinin disease
55207.5
12.5
b400
55
7.5
1
C4
Healthy Cold agglutinin disease
µg/m
L(m
ean
±SE
) b
a55207.5
12.5
C1s
Healthy Cold agglutinin disease
µg/m
L(m
ean
±SE
)
C, complement protein; SE, standard error. aP<0.01; bP<0.001.1. Shi J, et al. Blood. 2014;26(123):4015–4022. 2. Murphy K, et al. Janeway’s Immunobiology. 8th ed. New York: Garland Science; 2012.
Classical2 Lectin2 Alternative2
12M-CAgD-US-3006
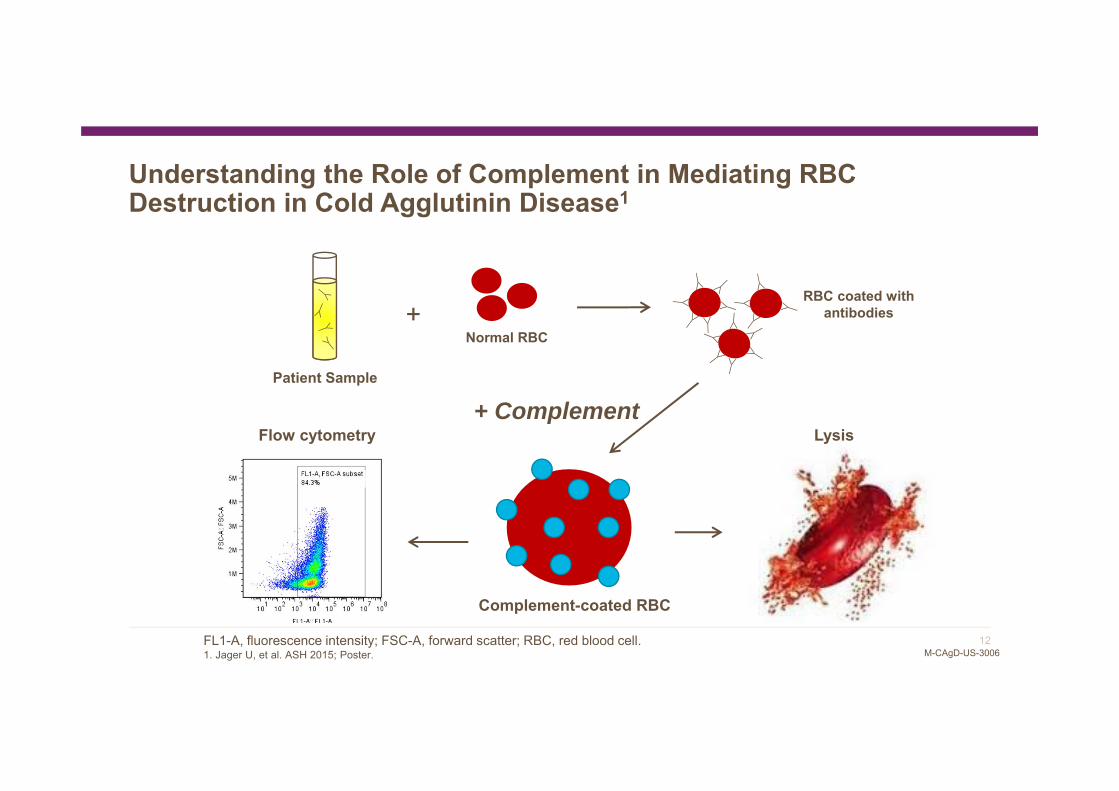
Understanding the Role of Complement in Mediating RBC Destruction in Cold Agglutinin Disease1
Patient Sample
Complement-coated RBC
Flow cytometry Lysis+ Complement
Normal RBC+
RBC coated with antibodies
FL1-A, fluorescence intensity; FSC-A, forward scatter; RBC, red blood cell.1. Jager U, et al. ASH 2015; Poster.
13M-CAgD-US-3006
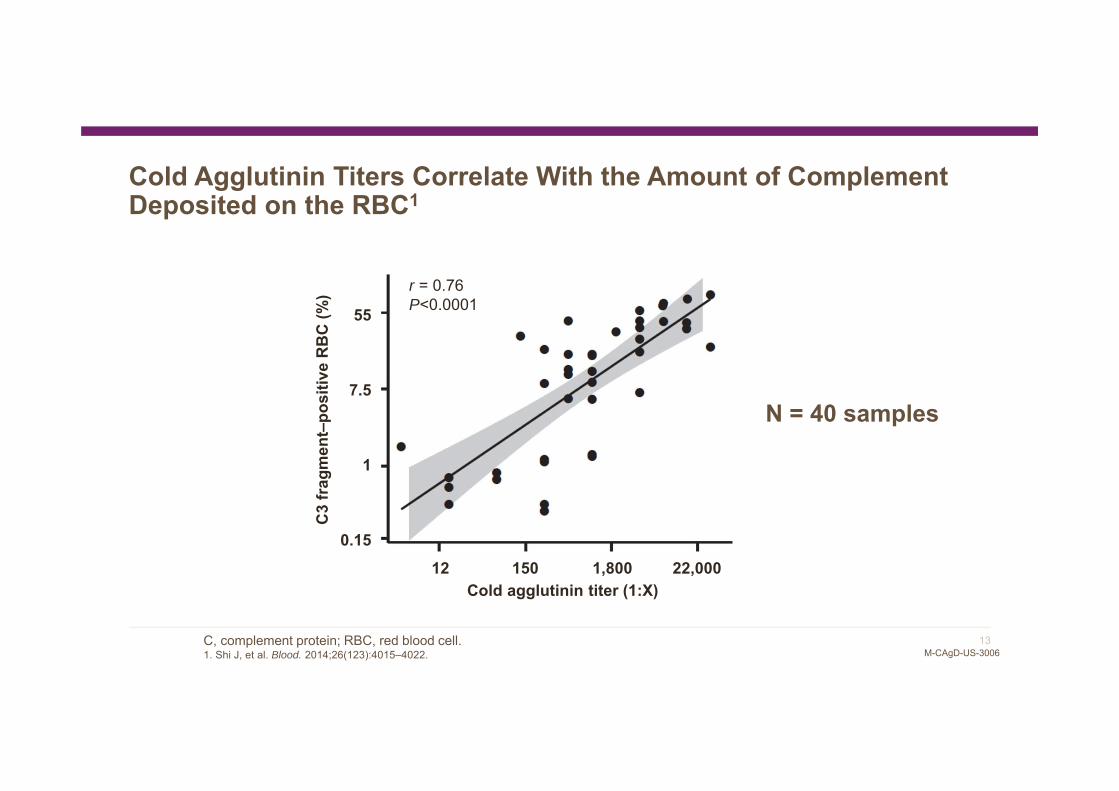
Cold Agglutinin Titers Correlate With the Amount of Complement Deposited on the RBC1
N = 40 samples
Cold agglutinin titer (1:X)12 150 1,800 22,000
55
7.5
1
0.15
C3
frag
men
t–po
sitiv
e R
BC
(%) r = 0.76
P<0.0001
C, complement protein; RBC, red blood cell.1. Shi J, et al. Blood. 2014;26(123):4015–4022.
14M-CAgD-US-3006
C3b Is an “Eat Me” Signal to Cells of the Immune System
MacrophageC3b-coated cells
C, complement protein.1. Wouters D, Zeerleder S. Haematologica. 2015;100(11):1388–1395.
PhagocytosisC3b is deposited on the target cell’s membrane, promoting its phagocytosis1

15M-CAgD-US-3006
An In Vitro Proxy for Extravascular Hemolysis
Normal RBC
+
RBC coated with complement
+ Complement
± inhibitor
+ Green dye
+Phagocytosis
RBC, red blood cell.
16M-CAgD-US-3006
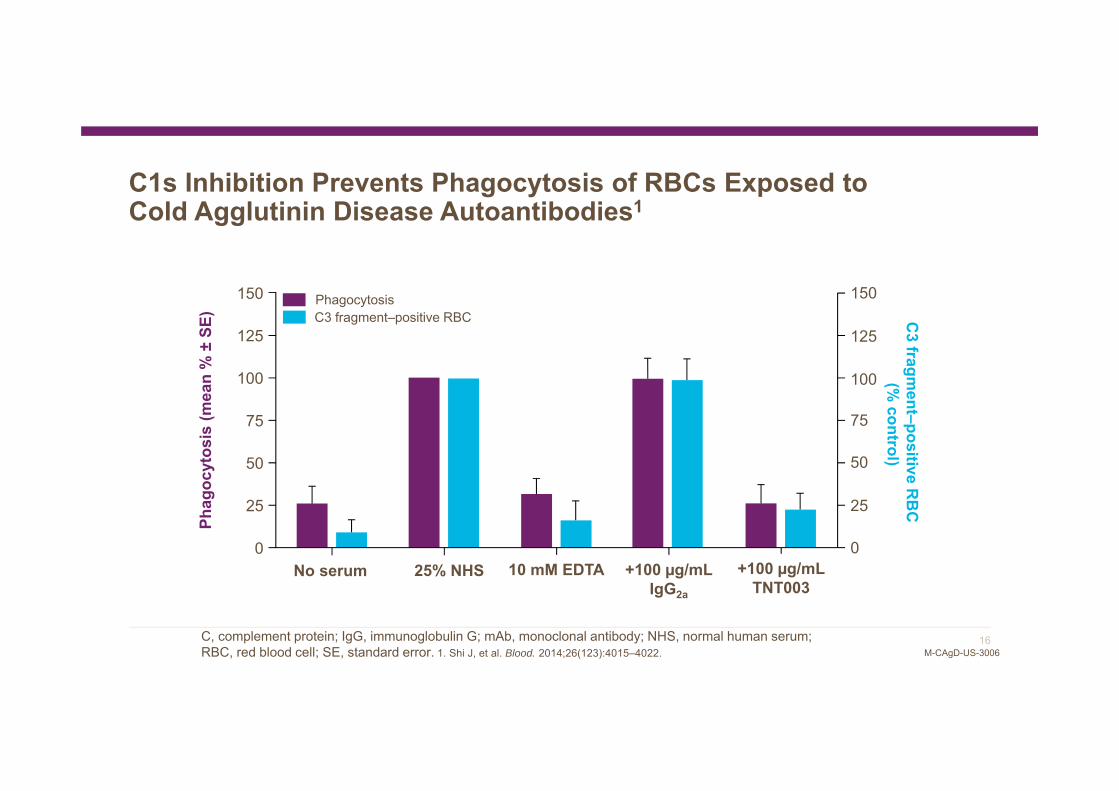
C1s Inhibition Prevents Phagocytosis of RBCs Exposed to Cold Agglutinin Disease Autoantibodies1
No serum +100 µg/mL TNT003
+100 µg/mL IgG2a
25% NHS 10 mM EDTA
Phag
ocyt
osis
(mea
n %
±SE
) C3 fragm
ent–positive RB
C(%
control)
C3 fragment–positive RBCPhagocytosis 150
100
50
0
125
75
25
150
100
50
25
0
125
75
C, complement protein; IgG, immunoglobulin G; mAb, monoclonal antibody; NHS, normal human serum; RBC, red blood cell; SE, standard error. 1. Shi J, et al. Blood. 2014;26(123):4015–4022.
17M-CAgD-US-3006
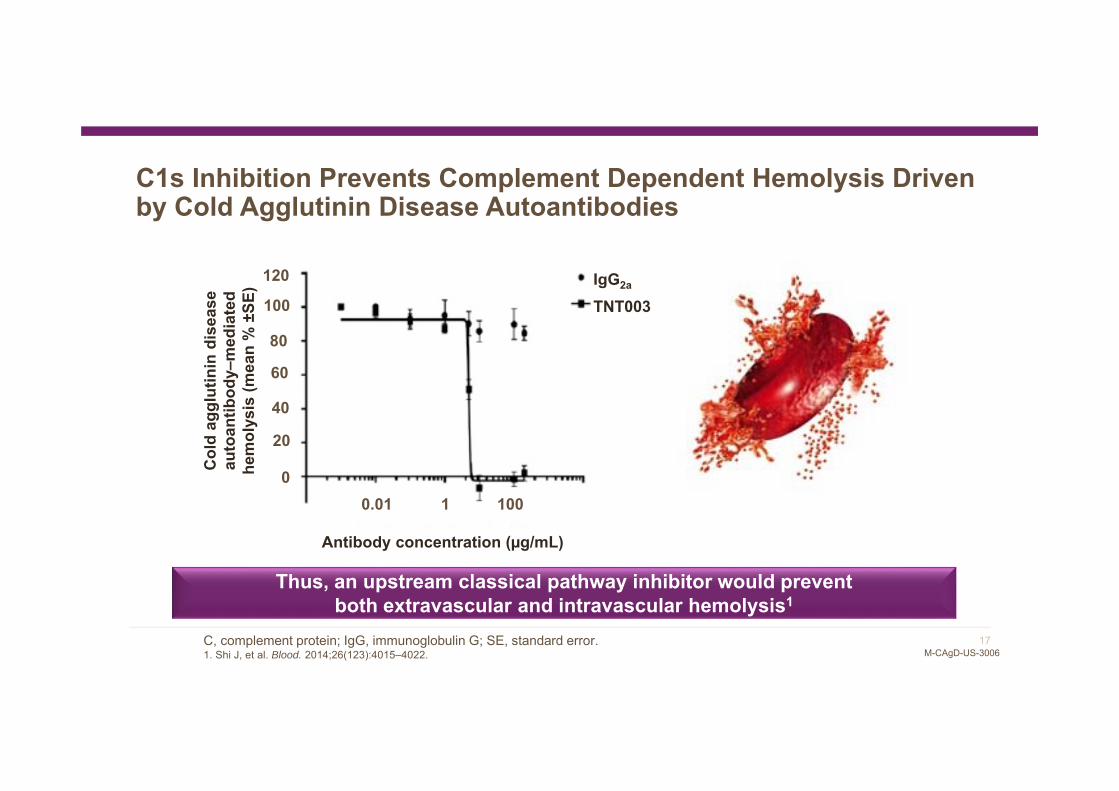
C1s Inhibition Prevents Complement Dependent Hemolysis Driven by Cold Agglutinin Disease Autoantibodies
Thus, an upstream classical pathway inhibitor would prevent both extravascular and intravascular hemolysis1
Antibody concentration (µg/mL)
C, complement protein; IgG, immunoglobulin G; SE, standard error.1. Shi J, et al. Blood. 2014;26(123):4015–4022.
IgG2a
TNT003
120
100
80
60
40
20
00.01 1 100
Col
d ag
glut
inin
dis
ease
au
toan
tibod
y–m
edia
ted
hem
olys
is (m
ean
% ±
SE)
18M-CAgD-US-3006
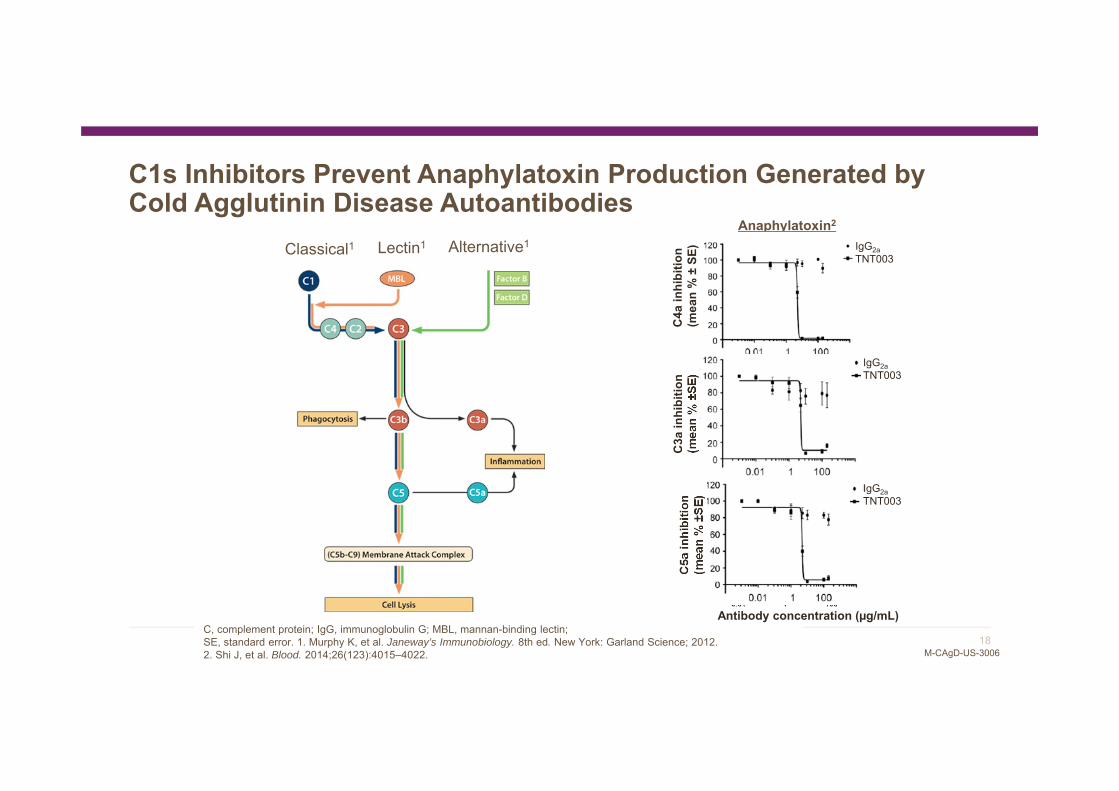
C1s Inhibitors Prevent Anaphylatoxin Production Generated by Cold Agglutinin Disease Autoantibodies
[Ab] g/mL
C5a
(% In
hibi
tion)
0.01 1 1000
50
100
0.01 1 1000
50
100
Anaphylatoxin2
C3a
inhi
bitio
n (m
ean
% ±
SE)
C5a
inhi
bitio
n (m
ean
% ±
SE)
C, complement protein; IgG, immunoglobulin G; MBL, mannan-binding lectin; SE, standard error. 1. Murphy K, et al. Janeway’s Immunobiology. 8th ed. New York: Garland Science; 2012. 2. Shi J, et al. Blood. 2014;26(123):4015–4022.
Classical1 Lectin1 Alternative1 IgG2aTNT003
IgG2aTNT003
IgG2aTNT003
C4a
inhi
bitio
n(m
ean
% ±
SE)
Antibody concentration (µg/mL)

19M-CAgD-US-3006
Summary
Cold agglutinin disease is an autoimmune hemolytic anemia1
Cold agglutinins bind to the RBC and activate the classical complement pathway, leading to opsonin (C3b) deposition on the RBC surface and, in some cases, direct cellular lysis2,3
Opsonin-coated RBCs travel to the liver where they are phagocytosed2,3
Classical pathway inhibitors that target upstream of C3 and prevent opsonin deposition rescue cells from being phagocytosed or lysed by complement, specifically demonstrating the role of the classical pathway in mediating cold agglutinin–driven complement activation4
Classical pathway inhibitors, therefore, could potentially be efficacious in the treatment of cold agglutinin disease4
C, complement protein; RBC, red blood cell.1. Berentsen S, et al. Haematologica. 2006;91(4):460–466. 2. Stone MJ. Blood. 2010;116(17):3119–3120. 3. Berentsen S. Clin Lymphoma Myeloma. 2009;9(1):110-112. 4. Shi J, et al. Blood. 2014;26(123):4015–4022.