understanding mortality developments history and future and an international view henk van...
TRANSCRIPT
Understanding Mortality Developments
History and future and an international view
Henk van Broekhoven

Starter
• Mortality and trend modelling is not just a mathematical and econometric exercise.
• History is a bad predictor of the future.– Expert judgement need to be added, particularly
from a medical/demographic view– What happened in the past should first of all be
understood
2

Content
1. Understanding the history2. Explaining the history3. Trends, how to model?4. New trend model5. International results6. Other risks7. Pandemics
3

UNDERSTANDING THE HISTORY
4

We should understand the history
1850 1856 1862 1868 1874 1880 1886 1892 1898 1904 1910 1916 1922 1928 1934 1940 1946 1952 1958 1964 1970 1976 1982 1988 1994 2000 200630
40
50
60
70
80
90
Life expectancy at age zero, Netherlands
Male Female
5

We should understand the history
1850 1856 1862 1868 1874 1880 1886 1892 1898 1904 1910 1916 1922 1928 1934 1940 1946 1952 1958 1964 1970 1976 1982 1988 1994 2000 200630
40
50
60
70
80
90
Life expectancy at age zero, Netherlands
Male Female
6
Spanish Flu in 1918
Hunger winter
end of WW2
(1)(2)
female smoking reduced the increase of life expectancy after 1990

E(0) Norway
7
18501856186218681874188018861892189819041910191619221928193419401946195219581964197019761982198819942000200630
40
50
60
70
80
90
Life expectancy age 0 Norway
MaleFemale

Norway vs Netherlands
8
1850 1856 1862 1868 1874 1880 1886 1892 1898 1904 1910 1916 1922 1928 1934 1940 1946 1952 1958 1964 1970 1976 1982 1988 1994 2000 200630
40
50
60
70
80
90
Comparison NL and Norway in life expectancy
Norway Male NL Male Norway Female NL Female
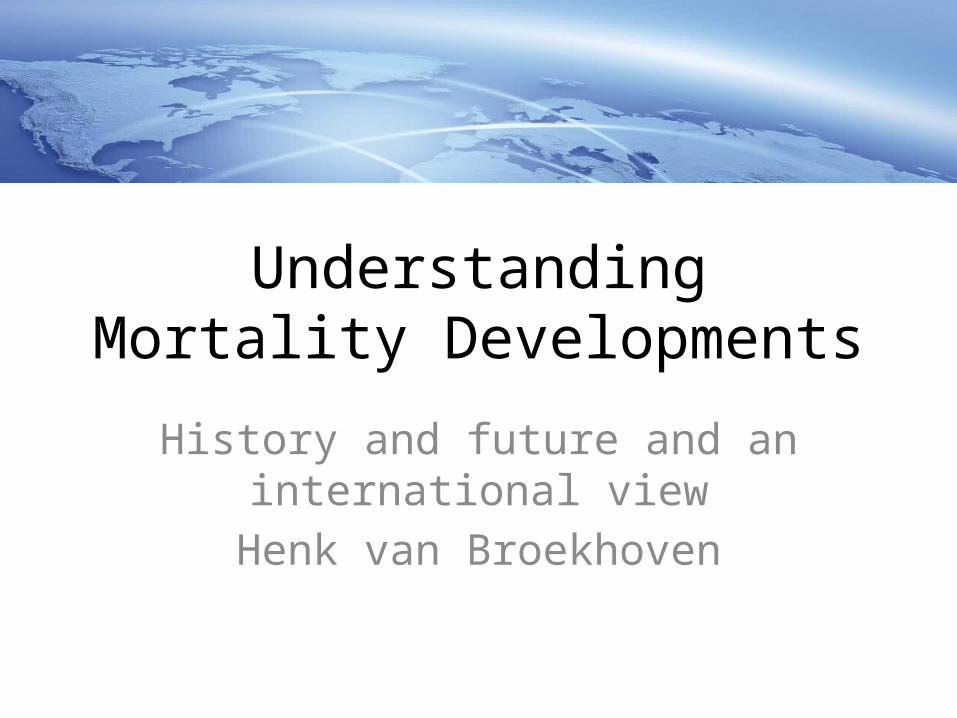
Comparison mortality by age
9
0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45 48 51 54 57 60 63 66 69 72 75 78 81 84 87 90 93 96 990.00001
0.0001
0.001
0.01
0.1
1
q(x) Male in 2009
NWNL
Comparison mortality by age
10
0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45 48 51 54 57 60 63 66 69 72 75 78 81 84 87 90 93 96 991
10
q(x) Female in 2009
NWNL

EXPLAINING THE HISTORY
11

Explaining the history
• (1) The “Hump”– In the early 50ts for the ages 45-75 for male the mortality
rates went up. This was caused by:• Smoking of cigarettes• Traffic accidents• Heart failure
– All these impacts are the result of behaviour• Smoking• Eating habits in combination with less healthy exercise habits• More driving in cars
– This flat period of development make the insurers not aware of the potential longevity risk in their portfolio
12

Explaining the history
• (1) The “Hump” (cont.)– During the seventies all three causes changed• Less smoking for male • Traffic get safer (in 1969 yearly more than 3000 traffic
deaths in NL, nowadays around 600)• Medical developments regarding heart attacks in
combination with a healthier way of living (healthier food, more exercise)
– … and the mortality rates went down again
13

Explaining the history
• (2) Trend change in 2001– The increase of the life expectancy suddenly went
up to more than 0.3 years per year (before that between 0.15 and 0.2), both for male and female
– Happened in almost the whole Western World– Reasons• Continuation of less smoking (particularly male)• Angioplasty as a treatment in case of an heart attack.
This increased the survival chance dramatically
14

Mortality development
• The development of life expectancy depends on:– Medical development
• And is it available?
– Behaviour• Drinking, smoking, eating habits,...
– Environment• Drinking water, one of the most important reasons of the increase of the life expectancy
in the developed countries• Pollution
– Water, air
• Climate– And so climate change
– New diseases– Resistance against medicines (antibiotics)
15

We can split development in 3 parts:
1850 1856 1862 1868 1874 1880 1886 1892 1898 1904 1910 1916 1922 1928 1934 1940 1946 1952 1958 1964 1970 1976 1982 1988 1994 2000 200630
40
50
60
70
80
90
Life expectancy at age zero, Netherlands
Male Female
2
16
1
3

We can split development in 3 parts
• (1) – No development of e(0)– High volatility• People less protected against extreme weather, flu
epidemics• Tuberculosis
– High mortality for young children• In 1850: e(0) male: 38.3; e(5) male: 50.8!
– Comparable with the underdeveloped countries
17

We can split development in 3 parts
• (2)– After the industrial revolution– Steep increase of life expectancy• Medical developments• Cleaner drinking water
– Seen as THE most important reason for improvement
• Environment – Better protection: heating in houses, toilets etc.
• Comparable with emerging countries
18

We can split development in 3 parts
• (3)– Typical for developed countries– Developments like the quality of drinking water are
reaching the limits– Change in life expectancy depends more of:
• Behaviour• Medical developments
– Both can have positive or negative effects.– Particularly behaviour can cause more independency
in development between male and female.
19

TRENDS, HOW TO MODEL?
20

How to model?
• In (1) and (2) it is rather easy to predict the future using the history
• In (3) this is very complex. History can hardly be use as dataset to predict the future.– More shocks (like in 2001) can be expected – Also a decrease of life expectancies is possible in the
coming 50 years:• Climate change • Resistance of antibiotics.• Behaviour (obesities)• …
21

How to model?
• In practice we see also a movement from (2) to (3) – for example in Central European Countries.
22

How old can a human become?
• The oldest confirmed human became 122 years and 164 days
• Jeanne Calment• Born: 25 February 1875• Secret?
• On all her food olive oil• Port wine diet• 1 kg of chocolate a week
23

How old can a human become?
• It cannot be proven that the max age is increasing
• Medical experts mention that a real life span exist per person, depending on the genetic passport, but will be limited to around 125-130 years.
• Mortality rates seem to be almost constant above age 105 at a level 0.5-0.6.
24

Conclusion (from my side)
• Pure mathematical models to predict the future mortality are less accurate
• Expert judgment is always needed for several decisions moments– Particularly input from the medical world is
needed• There is also a risk that the life expectancies
are getting lower than expected
25

Some models
• Based on cause of death:– Very complex, impossible without medical input• And many expert judgement decisions
– Information used not always reliable (>80)– Correlation between causes of death
– Models limited to 10 years projection
26

Some models
• By structure:– Separate models for • Very young children (under age 5)• Accident hump (age 18-25)• Aging (exponential model)• Age independent part
– Lots of parameters needed. This makes it hard to estimate and control
27

Some models
• Linear models like Lee Carter – Most likely too simple
• Short term – long term trend modelling– goal table approach– Good experience on the short term– Long term trend needs expert judgment
• Linear with adjustments for behaviour– CBS 2012: Average Western European mortality
adjusted for smoking behaviour 28

NEW STOCHASTIC TREND MODEL
29

New stochastic model
• Recently developed a new stochastic model for trend uncertainty
• This model is based on a multi-drift simulation, not the one-year volatility.
• Creates both one-year risk as multi-year risk measurements
30

New stochastic model
• Like in Lee Carter mortality development can be split in a drift plus a one year volatility.
• Other than in LC the volatility is not used to project future mortality, but the drift is analysed.
• To reduce the volatility a two-years average is taken– Volatility should be modelled as a separate sub-
risk (later more)31

New stochastic model
• The period we are analysing is first split into 16 years periods
• Each 16-year period is split into 2 8-year periods
• Each 8-year period is split into 2 4-year periods
• Each 4-year period is split into 2 2-year periods.
32

Example16 year drift
33

Example16 year drift
34

Example8 year drift
35

Example8 year drift
36
Then the same exercise for

How to use?
• Now we have many scenario’s • Before going into a simulation these scenario’s
are translated into the measurement we want: e.g. life expectancy or liabilities over a portfolio
• In this way dependencies are taken into account• The distributions are defined around the life
expectancies or liabilities– For the e(0) in this presentation I used Normal, with
some (negative) skewness
37

Results of the new model
38
195119551959196319671971197519791983198719911995199920032007201120152019202320272031203520392043204720512055205965
70
75
80
85
90
95
100
Male, history + futureDutch data
e(0)

First outcomes
20122014
20162018
20202022
20242026
20282030
20322034
20362038
20402042
20442046
20482050
20522054
20562058
206070
75
80
85
90
95
100
E(0) analyses met drift trend modelsimultie obv drifts 5000 simulatie scenarios
Based in Dutch data
95%BECBS95%90%99.50%Vaupel
39
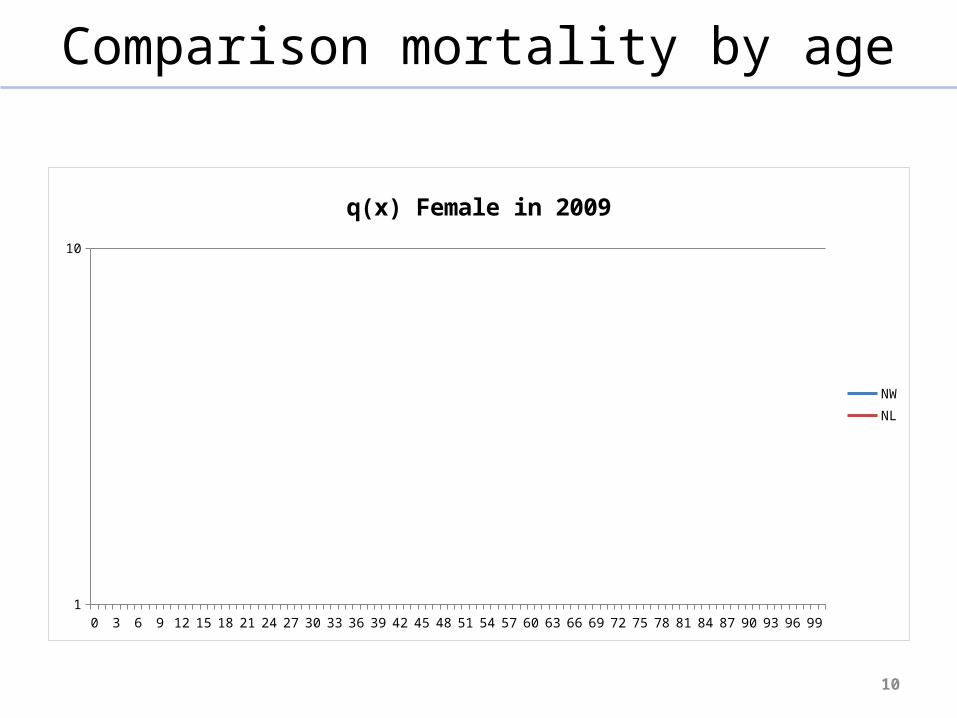
Some analysis for annuitiesexample for an immediate annuity
Age 75 65 55 45Life expectency 11,4 19,6 29,3 39,9
9,223 14,208 18,824 22,722
90% 5,14% 4,83% 4,21% 3,50%91% 5,38% 5,07% 4,42% 3,64%92% 5,62% 5,32% 4,63% 3,80%93% 5,91% 5,60% 4,85% 4,01%94% 6,30% 5,93% 5,10% 4,23%95% 6,68% 6,35% 5,44% 4,46%96% 7,15% 6,79% 5,77% 4,73%97% 7,81% 7,30% 6,26% 5,11%98% 8,47% 8,08% 6,95% 5,62%99% 9,53% 9,27% 7,97% 6,35%
90% 3,75% 2,45% 1,63% 1,07%95% 4,91% 3,20% 2,12% 1,39%
90% 4,52% 3,66%95% 8,29% 7,11%
10,46% 6,74% 4,44% 2,89%
99,50% 1,33% 1,51% 1,54% 1,44%Compare: result for one year trend uncertainty according to model
Multi year model Immediate annuity results:EC related to the BE
Best estimateConfidence level: Trend uncertainty calculated
Confidence level: Level uncertainty calculated
Confidence level: Level + Trend (diversified)
Standard model

INTERNATIONAL VIEW
41

International view
• Following the ideas countries that are in situation 3 should have comparable trend developments (save development level)
• Also following several studies the uncertainty should be comparable over the countries (I would like to add under the same circumstances) and can be used in case a lack of data exist in a country– Li Lee – CBS
42

Countries in (3)
43

Countries in (3)
44

Countries in (3)Model outcomes for male
45
2012 BE 2060 2060 incl. 95% unc.95% uncertaintyAUSTRIA 78.24 88.13 92.66 4.53BELGIUM 77.78 86.28 90.80 4.52DENMARK 77.82 87.17 92.34 5.17FRANCE 78.62 88.46 92.50 4.04ITALY 79.96 88.66 93.78 5.13NETHERLANDS 79.28 87.85 92.82 4.97NORWAY 79.36 87.77 92.77 5.00UK 78.99 89.39 93.19 3.80USA 76.84 85.91 89.95 4.04SWISS 80.57 89.27 92.80 3.53SWEDEN 79.97 87.24 90.53 3.29

Countries in (3)Model outcomes for male
46

Conclusions
• Indeed the uncertainty results of comparable countries are indeed close, but:– Larger countries have a somewhat lower
uncertainty (still some volatility left?)– Need to look at Sweden and Swiss
47
OTHER MORTALITY RISKS
48

Other risks
• Beside trend uncertainty mortality risk also contains:– Volatility– Level uncertainty– Calamity (extreme event)
49

Volatility
• Volatility because of “whole population issues” is based on a dependency in mortality because of for example– Appearance or non-appearance of Cold winters– Appearance or non-appearance of Hot summers– Seasonal flu epidemics– Severe accidents or natural disasters– Extreme events like a pandemic– … other ?

Volatility
• Also within the whole population mortality there will be a random effect, particularly because mortality rates are set by age/gender.– This part of the volatility is not part of the
mortality risk to be modelled• The random effect is measured in the insured
population involved.

Level uncertainty
• Level uncertainty should cover the statistical uncertainty in translating whole population mortality (or mortality based on some reference table) into mortality for the specific insured group.
52

EXTREME EVENTS, PANDEMICS
53

• For mortality extreme event modelling is generally based on a pandemic scenario.– E.g. in Solvency II the Spanish Flu is translated into
the modern times.• But…
How to model: extreme events

• But…• A pandemic risk is not a constant over time– Risk situation changes over time– This is measured in the WHO pandemic ratio– Solvency II• In general once in 40 years a pandemic• 1 in the 5 of them is worse enough to be a a “Solvency
II shock” • But this is measured in case WHO ratio is 1!
How to model: extreme events

• But the WHO 1 level was always higher than 1– In general 3.
• So what is the 1 in 200 scenario
• Perhaps better to talk about a scenario instead of 1 in 200.– Scenario can be the Spanish flu
How to model: extreme events
WHO, new proposal for phases
• Recently WHO proposed a new four-phase alert system replacing the old six-phase system:– Interpandemic
• The period between pandemics
– Alert• When a new subtype has been identified and increased vigilance and
risk management are warranted
– Pandemic• A period of global spread of a new subtype as indicated by global risk
assessment based on virologic, epidemiologic and clinical data
– Transition• Global risk drops, prompting stepdowns in global actions and response
activities
57

Conclusion
• Particularly for modelling extreme events we should look more at “conditional” modelling
58
59
Det er det ....
Takk