ultrasound november 17
TRANSCRIPT

Dr Arun Gupta Director imaging
Dr Rakhee guptaDr Vinayak Mittal
Dr NiharikaMahajan
Dr Samkit k Sagma Dr Varun Dr Ritesh Mahajan
• ENDOMETRIUM ( NORMAL / FLUID DISTENDED / INDENTED BY FIBROIDS)
• FEMALE HYDROCELE ( CYST IN CANAL OF NUCK)
• PATENT PROCESSUS VAGINALIS • GRADE FOUR CLEFT LIP / PALATE• ELASTOGRAM IN TORSION TESTIS
ADVANCED USG LOUNGE

ENDOMETRIAL CAVITY
A (fairly) normal uterine cavity and endometrial lining are necessary in order to conceive and maintain a pregnancy. There are several conditions related to the cavity or the lining that can cause problems. 3 D RENDERED IMAGES CAN HELP IN FAIR VISUALIZATION OF CONTOUR AND CONTENTS OF CAVITY .


SUBMUCOSALFIBROID
SUBSEROSAL FIBROID SPARING THE CAVITY

FETAL HEAD
DORSUM OFFETAL TORSO
FLUID IN ENDOMETRIAL CAVITY
Fluid in the endometrial cavitycan result from a number of causesif excessive and associated with distension.
PathologyThere are essentially three types of fluid:hydrometra: simple fluidhaematometra haemorrhagic content / clotpyometra: pus
Premenopausalnormal (i.e. physiological)cervical stenosisimperforate hymen
PostmenopausalOften a concern and some advocate the presence of echogenic fluid or an accompanying abnormal endometrial thickness as an indication for endometrial sampling• cervical stenosis• endometrial carcinoma• endometrial hyperplasia• endometrial polyp• cervical polyp• use of oestrogen replacement therapy
Normal endometrial contour and thickness and relatively homogenous Fluid with no mid level echoes s/o BENIGN ETIOLOGY.

Spermatic cord hydrocele(SCH) refers to loculated fluid collection along the spermatic cord. It separated from and located above the testicle and the epididymis.It results from aberrant closure of the processus vaginalis.There are two recognised sub types
ENCYSTED HYDROCELE -fluid collection does not communicate with the peritoneum above or the tunica vaginalis below.
FUNICULAR HYDROCELE -fluid collection communicates with the peritoneum at the internal inguinal ring but does not communicate with the tunica vaginalis
PATENT PROCESSUS VAGINALIS

PATENT PROCESSUS VAGINALIS
No communication with tunica vaginalis .There is communication with peritoneum
HENCE FUNICULAR HYDROCELE ( SUBTYPE OF SPERMATIC CORD HYDROCELE) IS CONSIDERED

Hydrocele of the canal of Nuck is a rare condition in female children caused by a failure of complete obliteration of the canal of Nuck . The canal of Nuck is an abnormal patent pouch of peritoneum extending anterior to the round ligament of the uterus into the labia majora .Incomplete obliteration of this canal (patent processusvaginalis) can result in either an inguinal hernia or a hydrocoele .
FEMALE HYDROCELE CYST OF CANAL OF NUCK
( swelling in inguino-labial Region)
IMPORTANT THINGS :No communication with the peritoneum should be visible in case of a hydrocoele .There should be no change with the Valsalva maneuver .
Ultrasound is particularly useful because of its “real-time” nature and ability to precisely depict superficial structures .Ultrasound is an excellent technique to help exclude the presence of bowel in the swelling as seen in an inguinal hernia
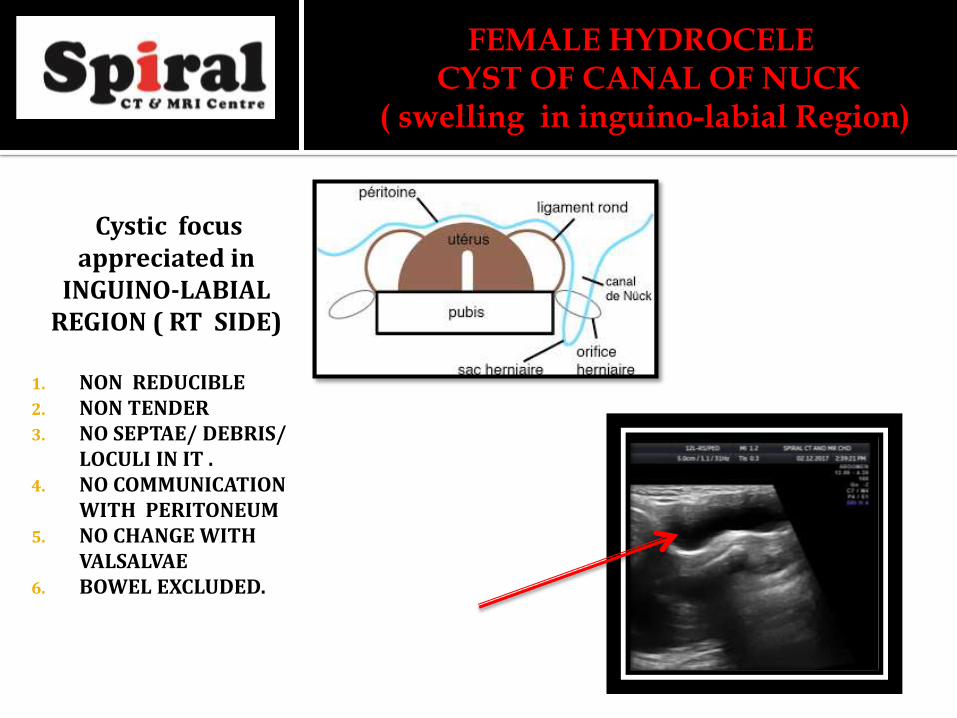
Cystic focus appreciated in
INGUINO-LABIAL REGION ( RT SIDE)
1. NON REDUCIBLE2. NON TENDER3. NO SEPTAE/ DEBRIS/
LOCULI IN IT .4. NO COMMUNICATION
WITH PERITONEUM5. NO CHANGE WITH
VALSALVAE6. BOWEL EXCLUDED.
FEMALE HYDROCELE CYST OF CANAL OF NUCK
( swelling in inguino-labial Region)

An upper lip defect may be seen and is best appreciated on angled coronal scanning. A vertical hypo-echoic region through the fetal upper lip usually represents the defect in cleft lip. This finding may be corroborated by a similar defect of the soft tissues of the upper lip overlying the maxillain the axial plane.The palate can be examined in the transverse (axial) plane. 3D ultrasound may further assist in
diagnosis. It is good practice to comment on fetal swallowing in real time at the time, the scan in performed.
CLEFT LIP AND CLEFT PALATE
HYPOECHOIC DEFECT IN THE MAXILLARY REGION
BOTH MESENCHYMAL AND BONE DEFECT

The Nyberg 1995 antenatal ultrasound classification system is divided in 5 types
•Type I: isolated cleft lip alone•Type II: unilateral cleft lip and palate•Type III: bilateral cleft lip and palate
( seen as premaxillary echogenicmass ) •Type IV: midline/median cleft lip and palate•Type V: facial clefts associated with the amniotic band syndrome or the limb-body-wall complexAn isolated cleft palate is almost impossible to diagnose in-utero and is not part of this classification.
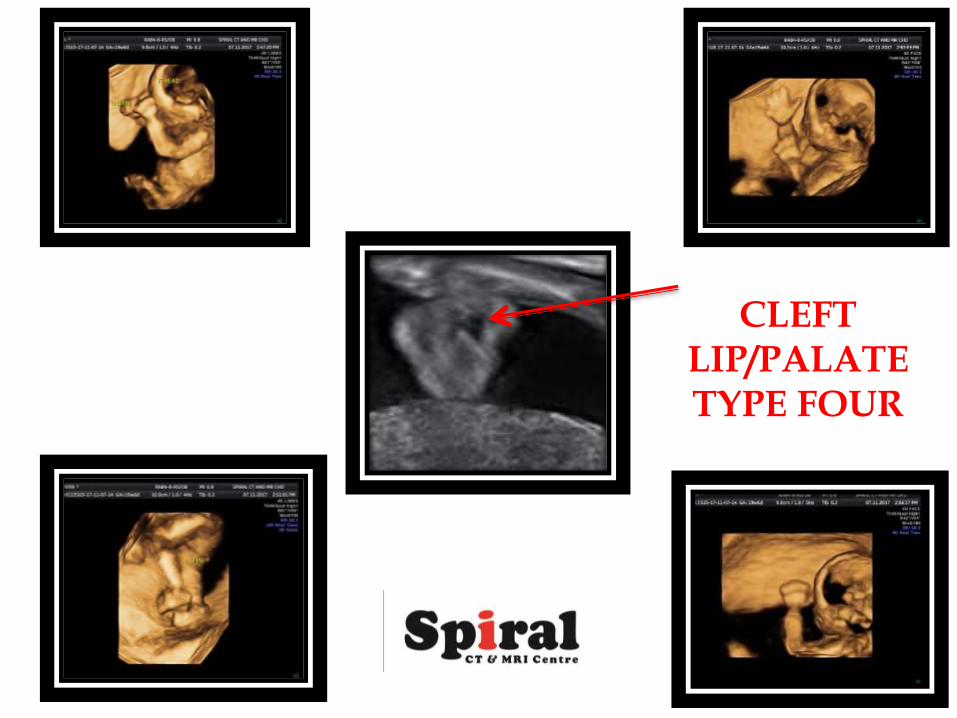
CLEFT LIP/PALATETYPE FOUR

The central part of testis has red color code corroborative with differentially soft
consistency ( post torsion follow up case )

DIAGNOSTICULTRASOUNDFOURTH EDITIONCarol M. Rumack, MD, FACRJ. William Charboneau, MD, FACRDeborah Levine, MD, FACR