ueda2012 -incretin based therapy of type 2 diabetes mellitus_d.adel
TRANSCRIPT
Incretin Based Therapy of Type 2 Diabetes Mellitus
BY
Prof. ADEL A EL-SAYED MDChairman Elect
Middle East and North Africa (MENA) Region
International Diabetes Federation (IDF)
Professor of Internal Medicine
Sohag Faculty of Medicine
Sohag-EGYPT
Pathophysiology of Type 2 Diabetes
• Insulin resistance.
• Beta cell dysfunction.
Pathophysiology of Type 2 Diabetes
Insulin Resistance
• Insulin Resistance starts very early in the course of the disease.
• insulin resistance alone will not produce diabetes. If beta-cell function is normal, one can compensate for insulin resistance by increasing insulin secretion.
Pathophysiology of Type 2 Diabetes
Beta cell defect• all type 2 patients have at least a relative defect in both
beta-cell function and mass. • Function: in the (UKPDS), newly diagnosed people with
diabetes had, on average, only about 50% of normal beta-cell function.[Diabetes. 1995;44:1249-1258 , Diab Res Clin Pract. 1998;40(suppl):S21-S25. ]
• Mass: Autopsy studies comparing the volume of beta
cells in nondiabetic individuals with that of people with diabetes found a 41% decrease in beta-cell mass among people with type 2 diabetes
Pathophysiology of Type 2 Diabetes
Beta cell defect
IV glucose infusion to a nondiabetic individual results in a biphasic insulin response:
- Immediate first-phase insulin response in the first few minutes.
- Second-phase response, more prolonged.
Pathophysiology of Type 2 Diabetes
Beta cell defect
• This first-phase insulin response is absent in type 2 diabetic patients contributing to the excessive and prolonged glucose rise after a meal in those with diabetes Diabetologia. 2004;47(suppl 1):A279.
• Infusing insulin can only partially improve this condition.
Pathophysiology of Type 2 Diabetes
Other Factors
• Historically, hyperglycemia in diabetes has been viewed as a failure of insulin-mediated glucose disposal into muscle and adipose tissue.
• This looks to be an over simplification of a more complicated issue.
Pathophysiology of Type 2 Diabetes
Other Factors
• Two other factors:
- Glucagon.
- Gastric emptying.
Pathophysiology of Type 2 Diabetes
The Glucagon Factor
• In response to a carbohydrate-containing meal, individuals without diabetes not only increase insulin secretion but also simultaneously decrease pancreatic alpha-cell glucagon secretion.
• The decrease in glucagon is associated with a decrease in hepatic glucose production, and along with the insulin response, results in a very modest increase in postprandial glucose.
N Engl J Med. 1971;285:443-449.
Pathophysiology of Type 2 Diabetes
The Glucagon Factor
• In contrast, the glucagon secretion in type 2 diabetics is not decreased, and may even be paradoxically increased.
• These insulin and glucagon abnormalities produce an excessive postprandial glucose excursion.
• more than 40 years ago, Roger Unger presciently stated, "One wonders if the development of a pharmacologic means of suppressing glucagon to appropriate levels would increase the effectiveness of available treatments for diabetes.
N Engl J Med. 1971;285:443-449.
Pathophysiology of Type 2 Diabetes
The Gastric Emptying Factor
• Many factors can affect the rate of gastric emptying.
• studies suggest that all other factors being equal, most people with type 1 and type 2 diabetes have accelerated gastric emptying compared to those without diabetes.
Gastroenterology. 1990;98:A378.
One last observation
• In healthy individuals, an oral glucose load is associated with a greater insulin response than administration of an isoglycemic IV glucose infusion designed to mimic the plasma glucose excursion achieved by the oral glucose load.
• Incretin hormones were discovered during
researchers trials to find out interpretation to this phenomenon which has been called the incretin effect.
J Clin Endocrinol Metab. 1986;63:492-498.
What are incretins?
• Hormones produced by the gastrointestinal tract in response to incoming nutrients, and have important actions that contribute to glucose homeostasis.
• Two hormones:
- Gastric inhibitory polypeptide (GIP) . - Glucagon-like peptide-1 (GLP-1).
What are incretins?
Gastric Inhibitory Polypeptide (GIP)
• Type 2 diabetes patients have a resistance to GIP, making it a less attractive therapeutic target.
What are incretins? Glucagon-like peptide-1 (GLP-1)
• a 30-amino acid peptide secreted in response to the oral ingestion of nutrients by L cells, primarily in the ileum and colon.
• There are GLP-1 receptors in islet cells and in the central nervous system, among other places.
• GLP-1 is metabolized by the enzyme dipeptidyl peptidase-IV (DPP-IV) .
Actions of GLP-1
• It enhances glucose-dependent insulin secretion.
• Inhibits glucagon secretion and therefore hepatic glucose production.
• Slows gastric emptying. • Increases satiety resulting in less food
intake. • Stimulates insulin gene transcription and
insulin synthesis.
Actions of GLP-1
• In animal studies: it increases beta-cell mass by decreasing apoptosis and increasing both beta-cell replication and neogenesis from pancreatic ductal cells.
Diabetes Care. 2003;26:2929-2940.
Actions of GLP-1
• Important, as glucose levels approach the normal range, the GLP-1 effects on insulin stimulation and glucagon inhibition declined (glucose dependence - reduction of hypoglycemia - therapeutic advantage) Diabetologia. 1993;36:741-744.

Actions of GLP-1 The Problem
• Unfortunately, GLP-1 is rapidly broken down by the DPP-IV enzyme (very short half-life in plasma - requires continuous IV infusion).
What to do?
• Incretin mimetics are glucagon-like peptide-1 (GLP-1) agonists (Exenatide).
• Dipeptidyl peptidase-IV (DPP-IV) antagonists inhibit the breakdown of GLP-1 (Sitagliptin).
THANK YOU
Exenatide
• The first incretin-related therapy available for patients with type 2 diabetes.
• Naturally occurring peptide from the saliva of the Gila Monster.
• Has an approximate 50% amino acid homology with GLP-1.
• Binds to GLP-1 receptors and behaves as GLP-1.
• Resistant to DPP-IV inactivation.

Exenatide Problems
• It is measurably present in plasma for up to 10 hours. Suitable for twice a day administration by subcutaneous injection.
Regul Pept. 2004;117:77-88.
Am J Health Syst Pharm. 2005;62:173-181.
Exenatide Problems
• Nausea (sometimes accompanied with vomiting) has uniformly been observed across the clinical trials, although most episodes were mild-to-moderate in intensity and generally intermittent.
• Usually more frequent at the initiation of treatment and decreased over the course of several weeks.
Dipeptidyl Peptidase-IV Antagonists Sitagliptin
• The concept is to allow the endogenous GLP-1 to remain in circulation for a longer period.
• DPP-IV inhibitors are oral, rather than injectable. • Weight neutral. • associated with a low incidence of hypoglycemia
or gastrointestinal side effects. Diabetes Care. 2004;27:2874-2880.
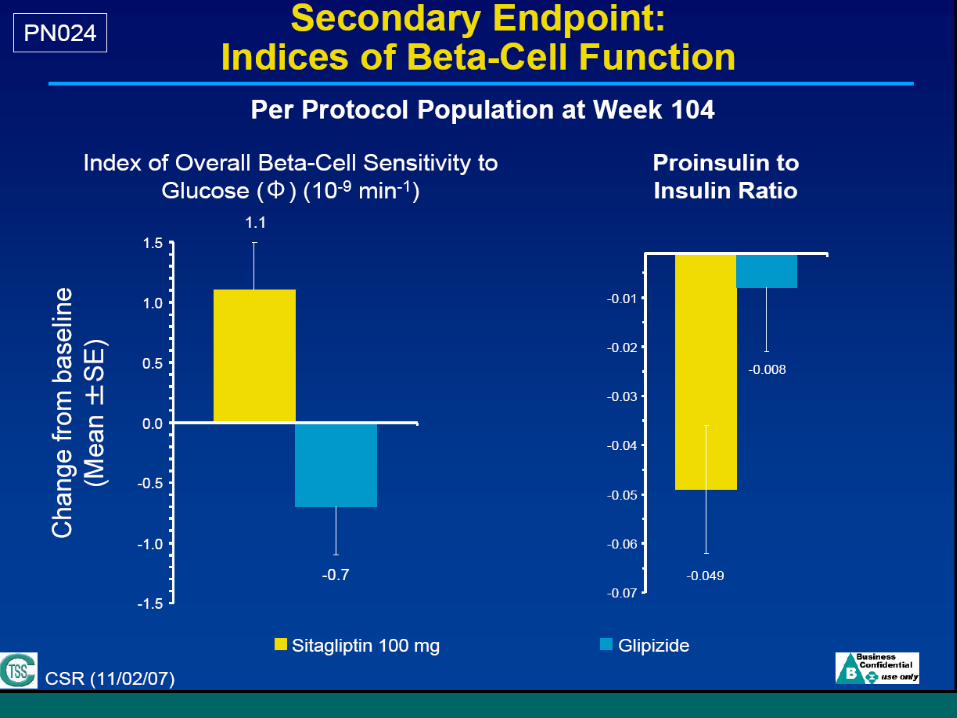
• Long-term studies suggest a durable effect on glycemia and improvement in of beta-cell function. (www.glucagon.com).
Sitagliptin
• Sitagliptin, is the first agent in this class to have received FDA approval.
• Incidence of adverse reactions with sitagliptin in clinical trials was similar to placebo.
• Sitagliptin is indicated as monotherapy and in combination with metformin or thiazolidinediones.
• The usual recommended dose is 100 mg once daily.
Sitagliptin
• Efficacy
• Body weight
• ß-cell function
• Hypoglycemia
• CV risk and CV events
• Guidelines
• Summary
SitagliptinEfficacy: HbA1c reduction
• Nauck et al.2007
Non-inferiority of sitagliptin to glipizide (on top of metformin)
31
Screening
Single-blindplacebo
Double-blind treatment period:Sulfonylurea or sitagliptin 100 mg/day
Metformin monotherapy
Week 2:Eligible if HbA1c
≥6.5% to ≤10%
If on an OHA, D/CContinue/start
metformin
Day 1Randomization Week 52
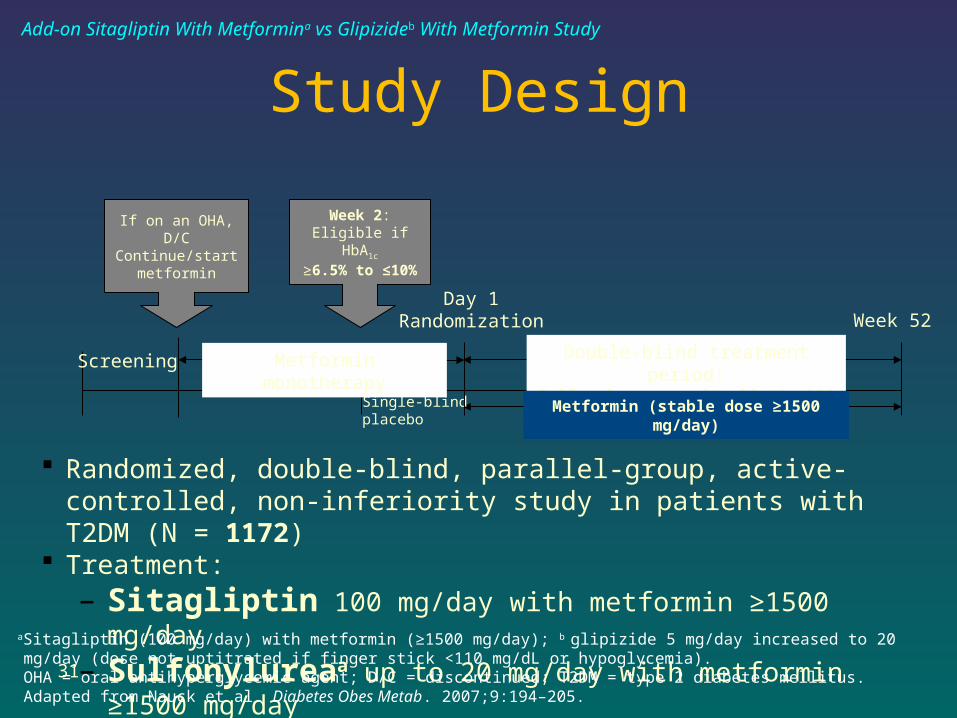
Randomized, double-blind, parallel-group, active-controlled, non-inferiority study in patients with T2DM (N = 1172)
Treatment:– Sitagliptin 100 mg/day with metformin ≥1500 mg/day– Sulfonylureaa up to 20 mg/day with metformin ≥1500 mg/day
aSitagliptin (100 mg/day) with metformin (≥1500 mg/day); b glipizide 5 mg/day increased to 20 mg/day (dose not uptitrated if finger stick <110 mg/dL or hypoglycemia).OHA = oral antihyperglycemic agent; D/C = discontinued; T2DM = type 2 diabetes mellitus.Adapted from Nauck et al. Diabetes Obes Metab. 2007;9:194–205.
Study Design
Metformin (stable dose ≥1500 mg/day)
Add-on Sitagliptin With Metformina vs Glipizideb With Metformin Study
32
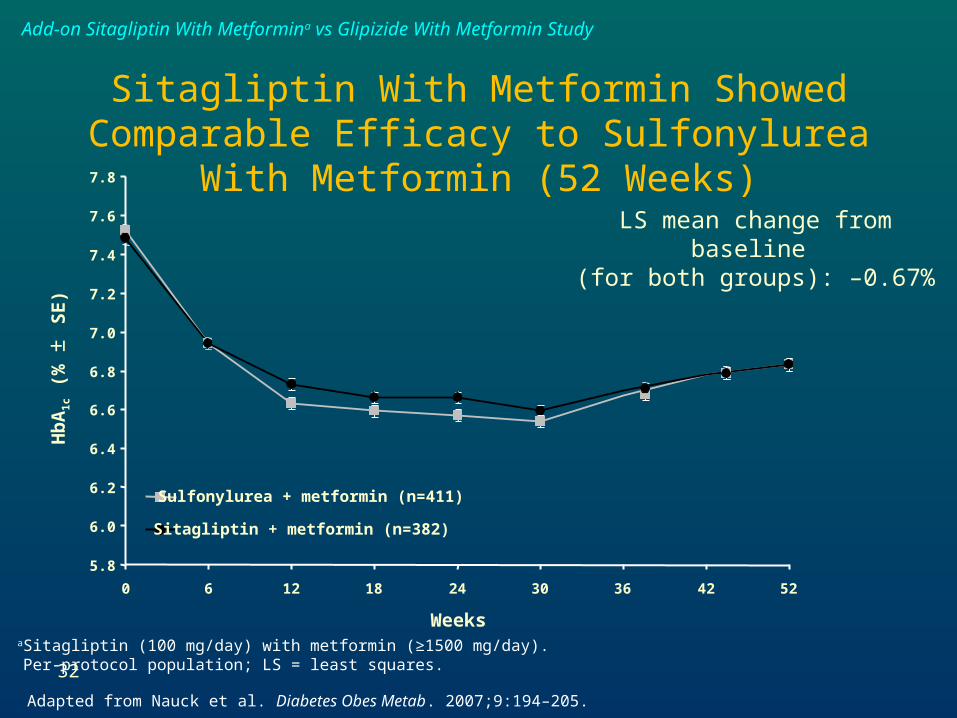
Sulfonylurea + metformin (n=411)
Sitagliptin + metformin (n=382)
Hb
A1
c (
% ±
SE
)
LS mean change from baseline (for both groups): –0.67%
Weeks
5.8
6.0
6.2
6.4
6.6
6.8
7.0
7.2
7.4
7.6
7.8
0 6 12 18 24 30 36 42 52
aSitagliptin (100 mg/day) with metformin (≥1500 mg/day).Per-protocol population; LS = least squares.
Adapted from Nauck et al. Diabetes Obes Metab. 2007;9:194–205.
Sitagliptin With Metformin Showed Comparable Efficacy to Sulfonylurea With Metformin (52
Weeks)
Add-on Sitagliptin With Metformina vs Glipizide With Metformin Study
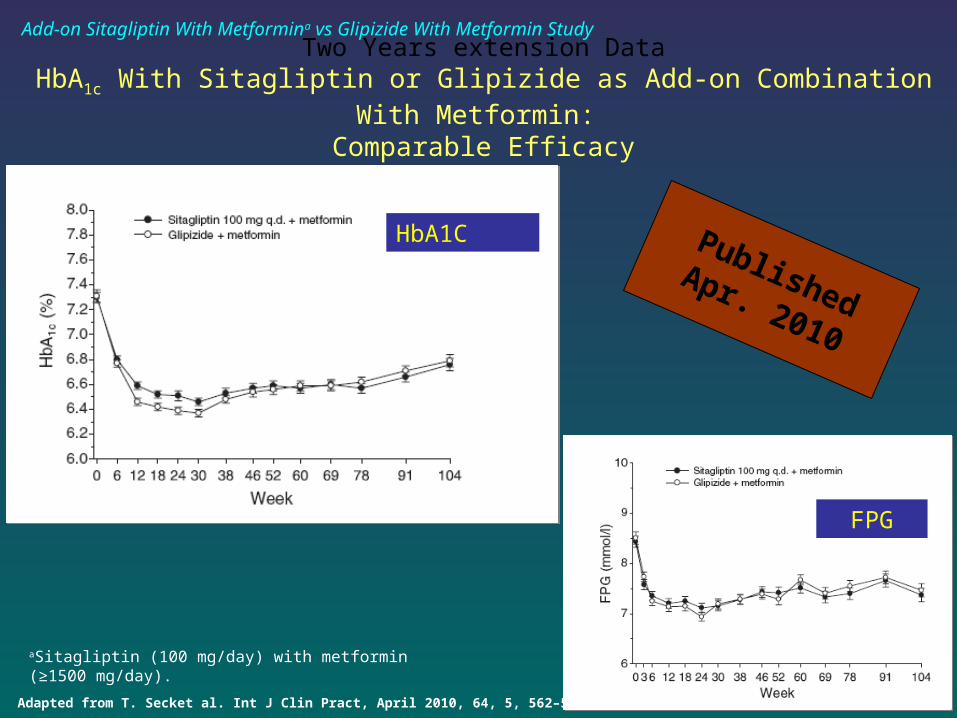
Adapted from T. Secket al. Int J Clin Pract, April 2010, 64, 5, 562–576.
Two Years extension DataHbA1c With Sitagliptin or Glipizide as Add-on Combination With Metformin:
Comparable Efficacy
Published Apr. 2010
HbA1C
FPG
Add-on Sitagliptin With Metformina vs Glipizide With Metformin Study
aSitagliptin (100 mg/day) with metformin (≥1500 mg/day).
34
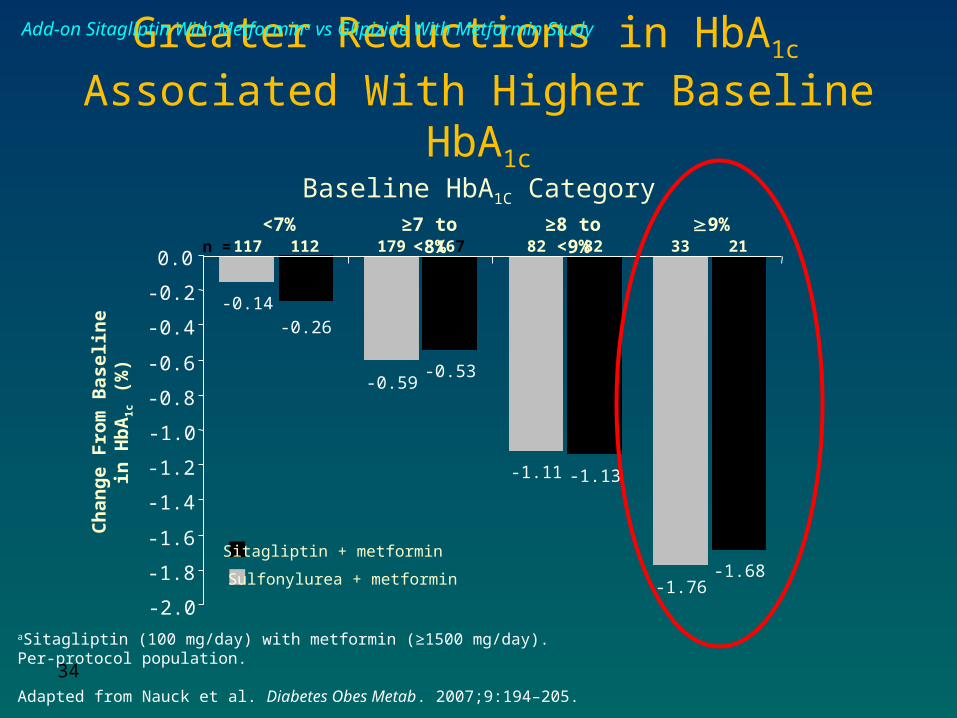
Baseline HbA1C Category
Ch
ang
e F
rom
Bas
elin
e in
H
bA
1c (
%)
n=117
117 112 179 167 82 82 33 21<7% ≥7 to <8% ≥8 to <9% 9%
-0.14
-0.59
-1.11
-1.76
-0.26
-0.53
-1.13
-1.68
-2.0
-1.8
-1.6
-1.4
-1.2
-1.0
-0.8
-0.6
-0.4
-0.2
0.0
Sitagliptin + metformin
Sulfonylurea + metformin
n =
Greater Reductions in HbA1c Associated With Higher Baseline HbA1c
aSitagliptin (100 mg/day) with metformin (≥1500 mg/day).Per-protocol population.
Adapted from Nauck et al. Diabetes Obes Metab. 2007;9:194–205.
Add-on Sitagliptin With Metformina vs Glipizide With Metformin Study
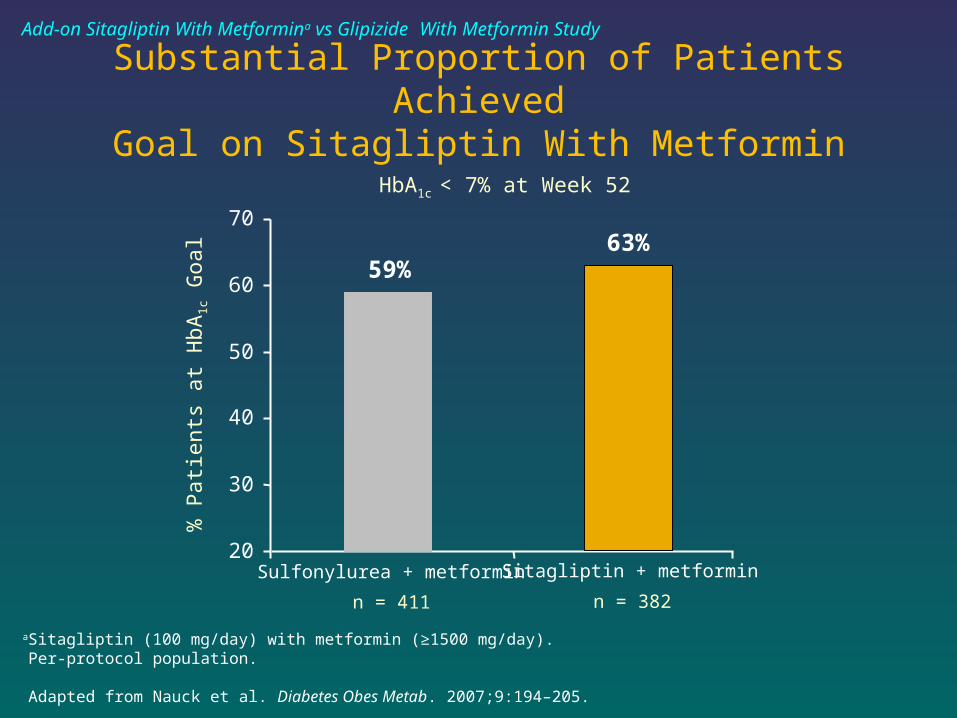
Substantial Proportion of Patients AchievedGoal on Sitagliptin With Metformin
n = 411
% P
atie
nts
at H
bA1c
Goa
lHbA1c < 7% at Week 52
20
30
40
50
60
70
n = 382
63%
Sitagliptin + metformin
59%
Sulfonylurea + metformin
aSitagliptin (100 mg/day) with metformin (≥1500 mg/day).Per-protocol population.
Adapted from Nauck et al. Diabetes Obes Metab. 2007;9:194–205.
Add-on Sitagliptin With Metformina vs Glipizide With Metformin Study
Weight gain
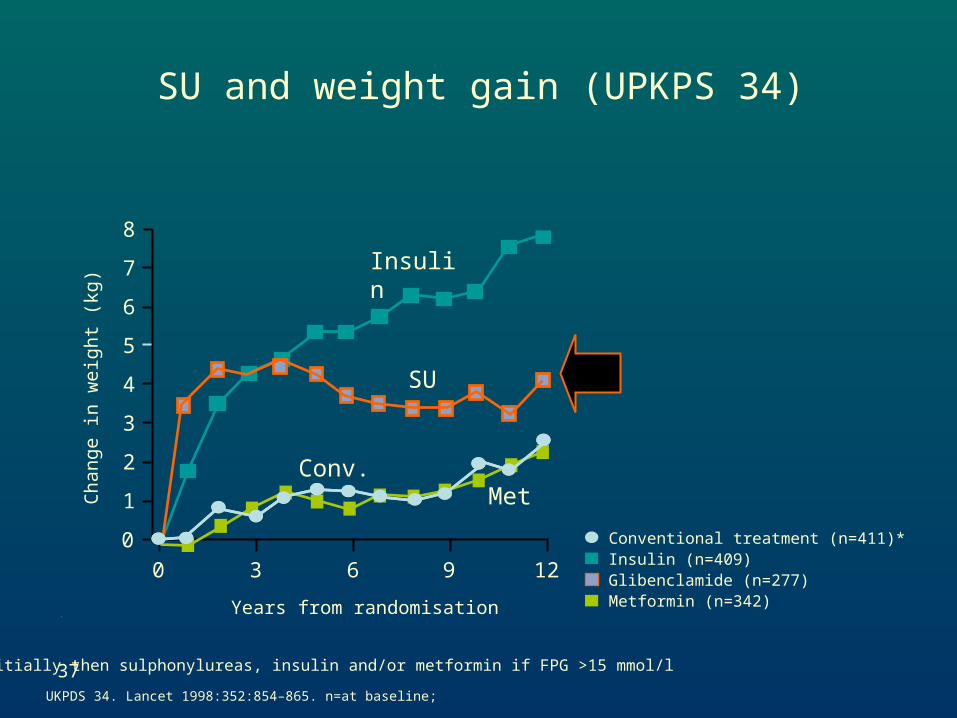
37UKPDS 34. Lancet 1998:352:854–865. n=at baseline;
Chang
e in w
eig
ht
(kg)
Years from randomisation
*diet initially then sulphonylureas, insulin and/or metformin if FPG >15 mmol/l
0
1
5
0 3 6 9 12
8
7
6
4
3
2
Insulin (n=409)Glibenclamide (n=277)Metformin (n=342)
Conventional treatment (n=411)*
Insulin
SU
Conv.Met
SU and weight gain (UPKPS 34)

Abdominal obesity is linked to a higher risk for myocardial infarction
Yusuf S. et al. Lancet 2004; 364:937-52
INTERHEART-Study:Case control study in 52 countries: 15152 cases vs 14820 controls
Abdominal obesity* leads to a significantly higher risk
for myocardial infarction:
OR (99%CI): 4.5 and 4.7 in W Eur and N Amer population
*waist/hip/ratio: upper tertile vs lowest tertile
39
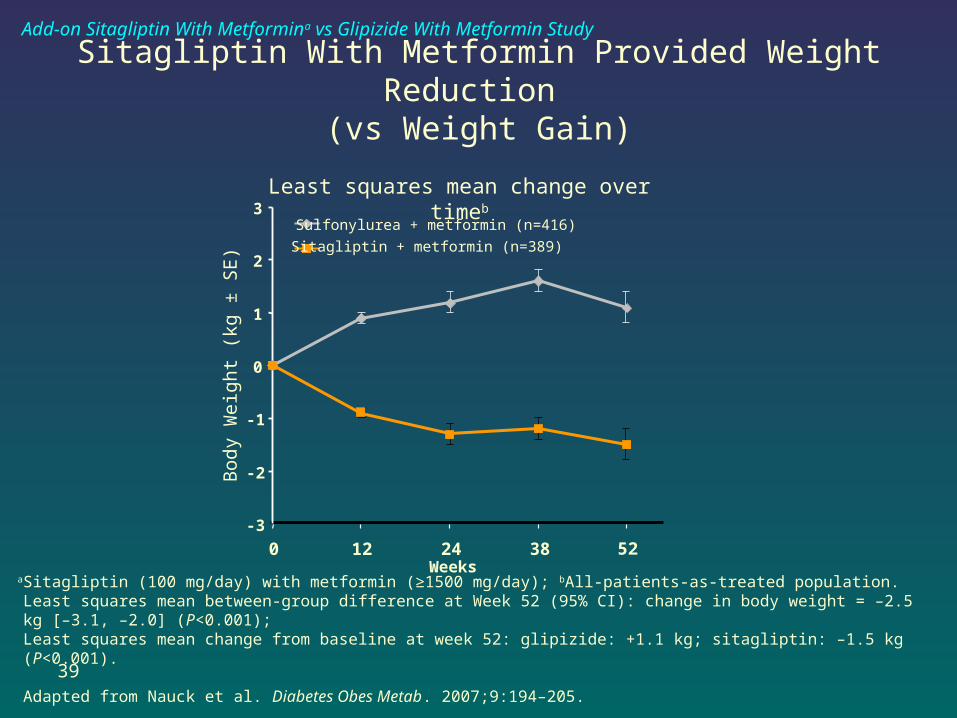
Sitagliptin With Metformin Provided Weight Reduction (vs Weight Gain)
aSitagliptin (100 mg/day) with metformin (≥1500 mg/day); bAll-patients-as-treated population.Least squares mean between-group difference at Week 52 (95% CI): change in body weight = –2.5 kg [–3.1, –2.0] (P<0.001);Least squares mean change from baseline at week 52: glipizide: +1.1 kg; sitagliptin: –1.5 kg (P<0.001).
Adapted from Nauck et al. Diabetes Obes Metab. 2007;9:194–205.
Bod
y W
eigh
t (k
g ±
SE
)Sulfonylurea + metformin (n=416)
Sitagliptin + metformin (n=389)
-3
-2
-1
0
1
2
3
Weeks
Least squares mean change over timeb
0 12 24 38 52
Add-on Sitagliptin With Metformina vs Glipizide With Metformin Study
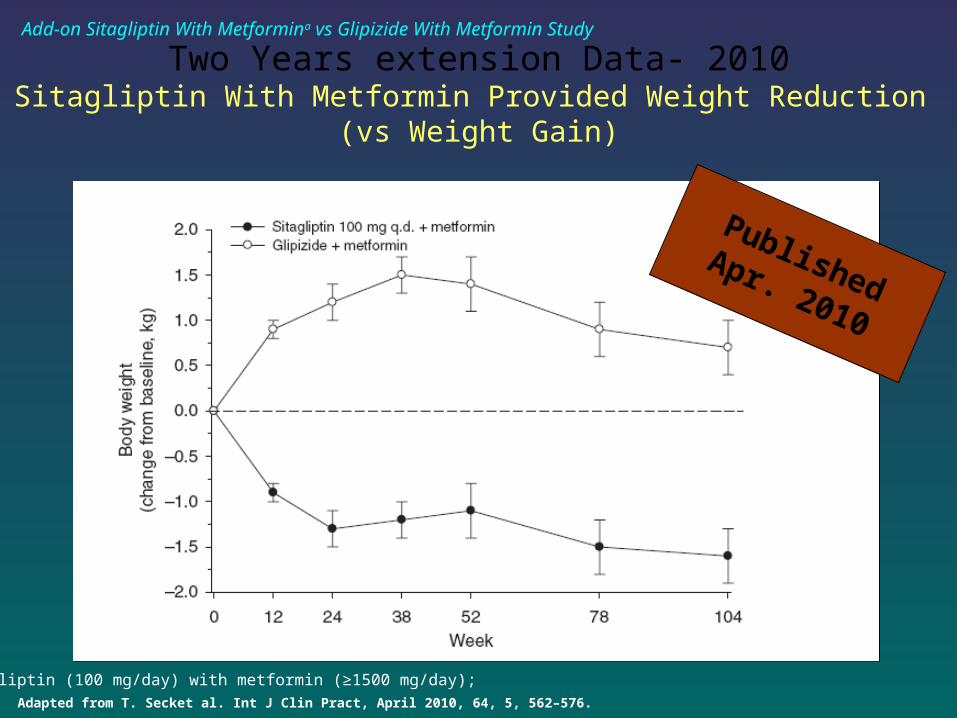
Two Years extension Data- 2010Sitagliptin With Metformin Provided Weight Reduction
(vs Weight Gain)
Published Apr. 2010
Adapted from T. Secket al. Int J Clin Pract, April 2010, 64, 5, 562–576.
Add-on Sitagliptin With Metformina vs Glipizide With Metformin Study
aSitagliptin (100 mg/day) with metformin (≥1500 mg/day);
Beta-cell function
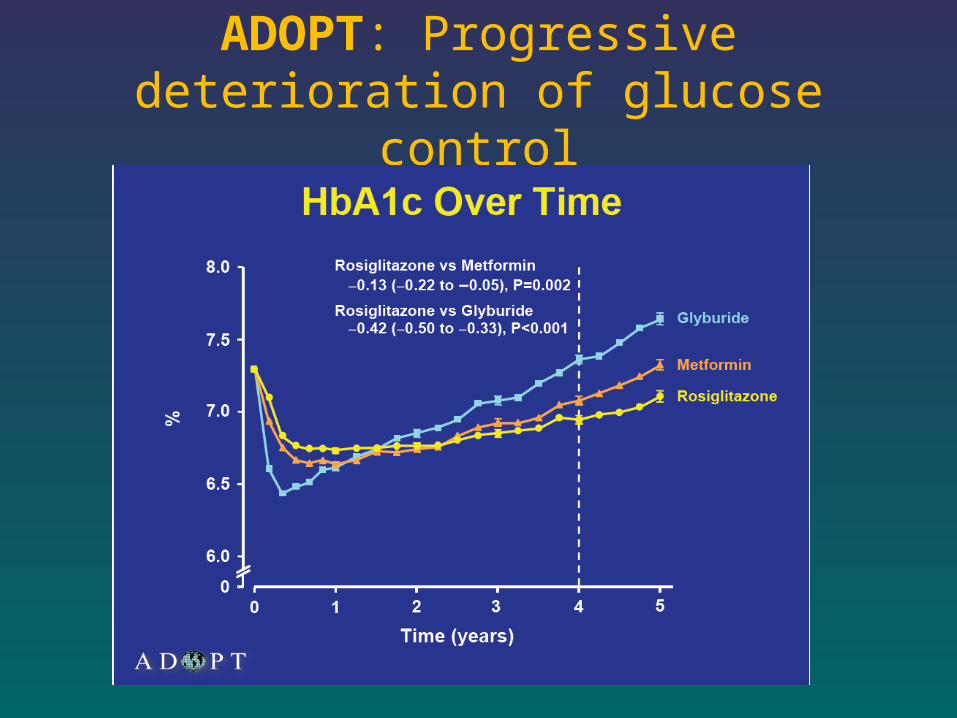
ADOPT: Progressive deterioration of glucose control
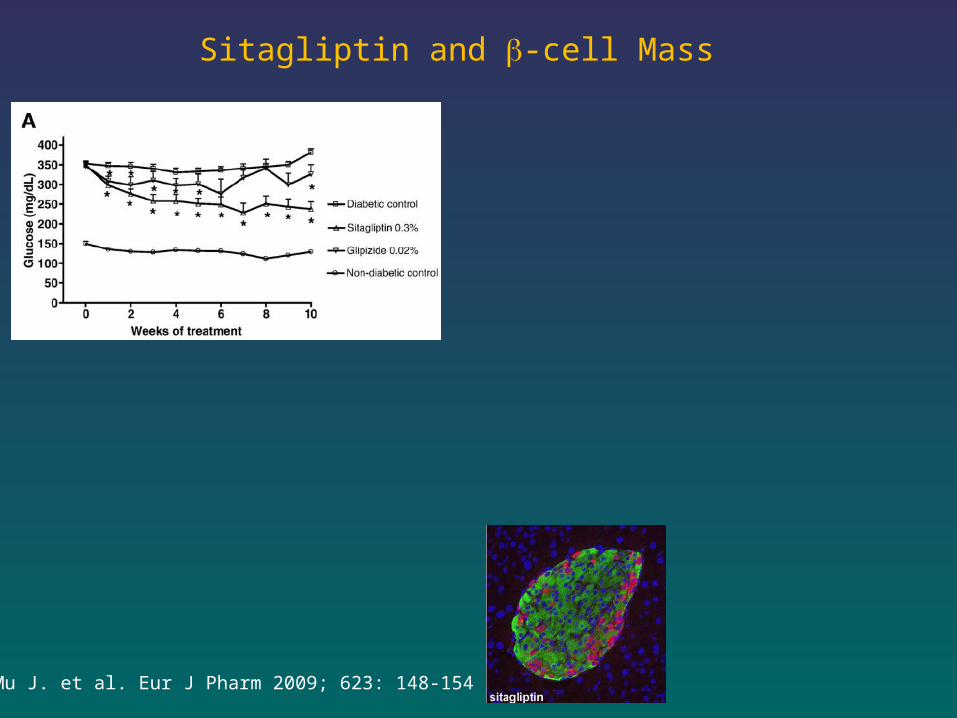
Sitagliptin and -cell Mass
Mu J. et al. Eur J Pharm 2009; 623: 148-154
44
Hypoglycemic events
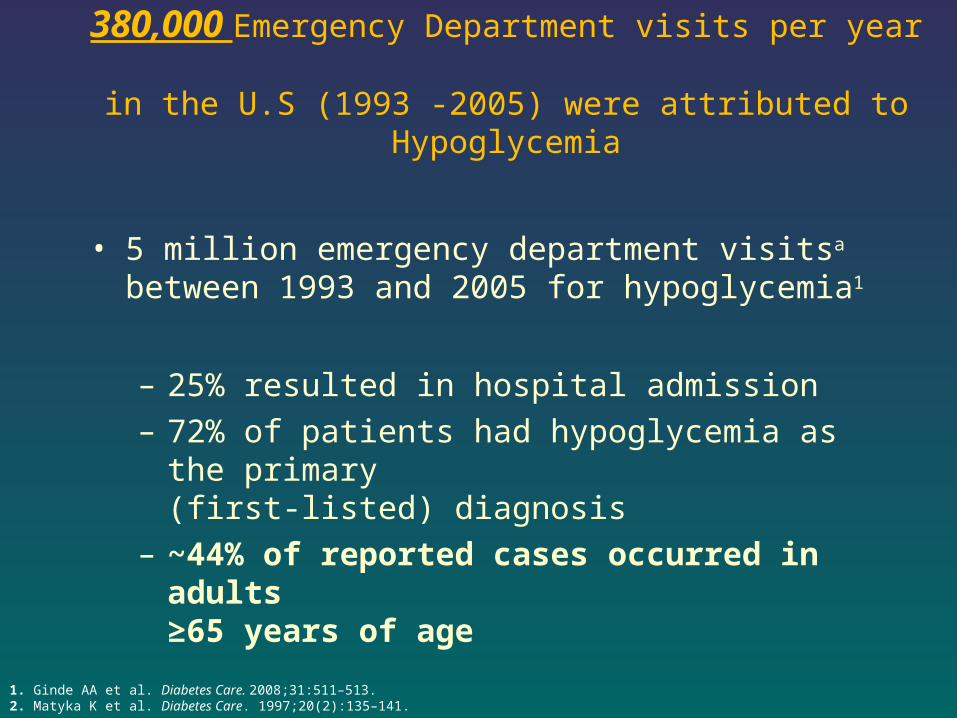
380,000 Emergency Department visits per year in the U.S (1993 -2005) were attributed to Hypoglycemia
• 5 million emergency department visitsa between 1993 and 2005 for hypoglycemia1
– 25% resulted in hospital admission– 72% of patients had hypoglycemia as the primary
(first-listed) diagnosis– ~44% of reported cases occurred in adults
≥65 years of age
1. Ginde AA et al. Diabetes Care. 2008;31:511–513.2. Matyka K et al. Diabetes Care. 1997;20(2):135–141.
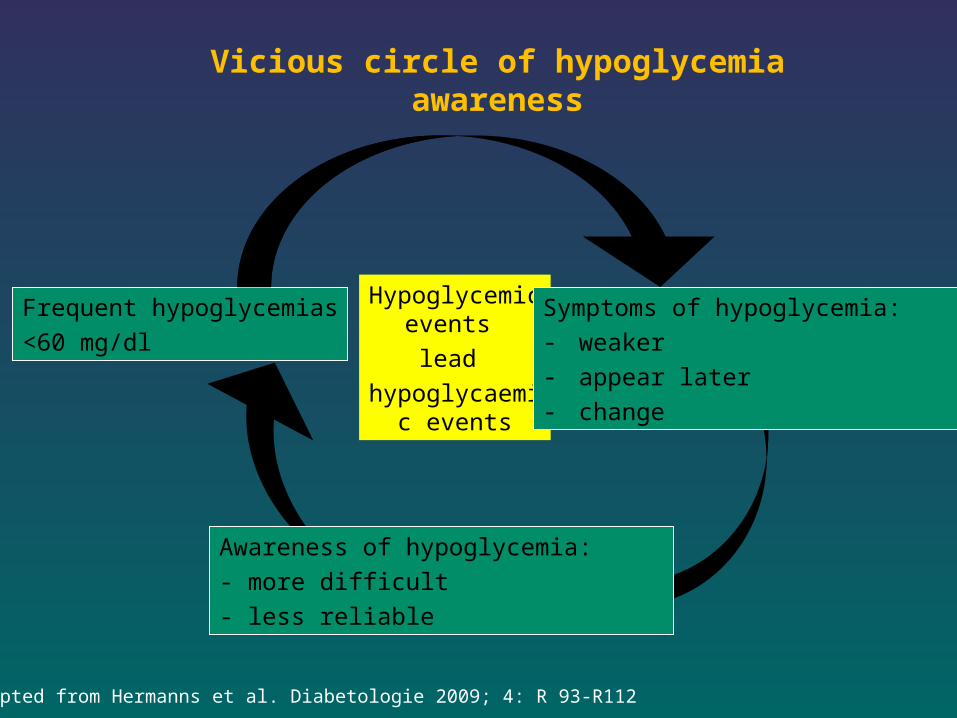
Vicious circle of hypoglycemia awareness
Hypoglycemic events
lead
hypoglycaemic events
Frequent hypoglycemias
<60 mg/dl
Adapted from Hermanns et al. Diabetologie 2009; 4: R 93-R112
Symptoms of hypoglycemia:
- weaker
- appear later
- change
Awareness of hypoglycemia:
- more difficult
- less reliable
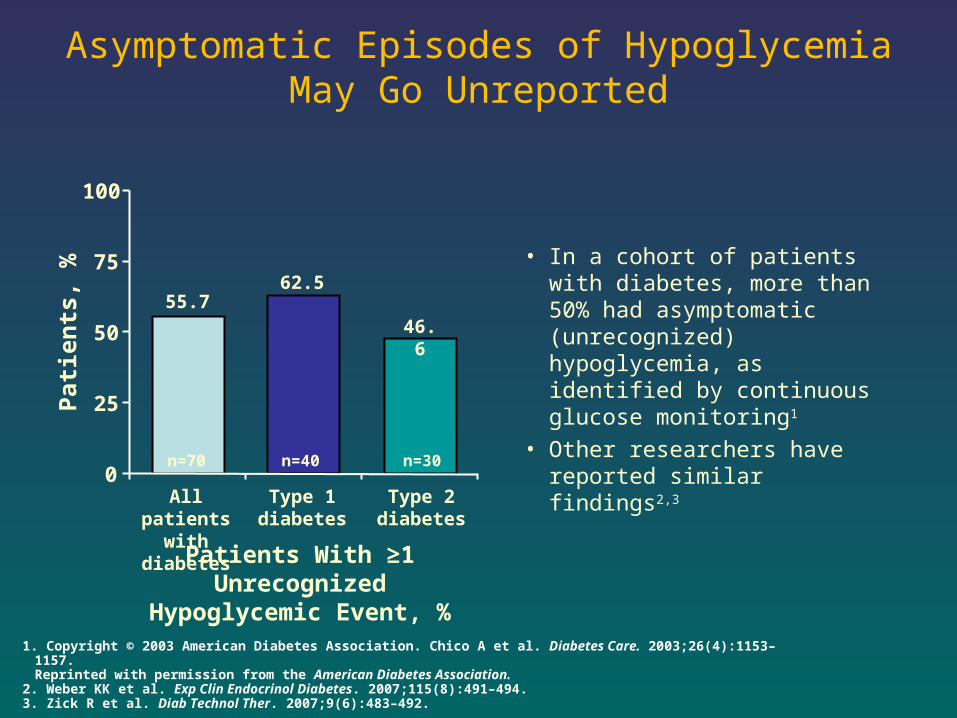
Asymptomatic Episodes of Hypoglycemia May Go Unreported
• In a cohort of patients with diabetes, more than 50% had asymptomatic (unrecognized) hypoglycemia, as identified by continuous glucose monitoring1
• Other researchers have reported similar findings2,3
1. Copyright © 2003 American Diabetes Association. Chico A et al. Diabetes Care. 2003;26(4):1153–1157. Reprinted with permission from the American Diabetes Association.
2. Weber KK et al. Exp Clin Endocrinol Diabetes. 2007;115(8):491–494. 3. Zick R et al. Diab Technol Ther. 2007;9(6):483–492.
0
25
50
75
100
All patients with diabetes
Type 1 diabetes
Patie
nts,
%
Type 2diabetes
55.762.5
46.6
Patients With ≥1 Unrecognized Hypoglycemic Event, %
n=70 n=40 n=30
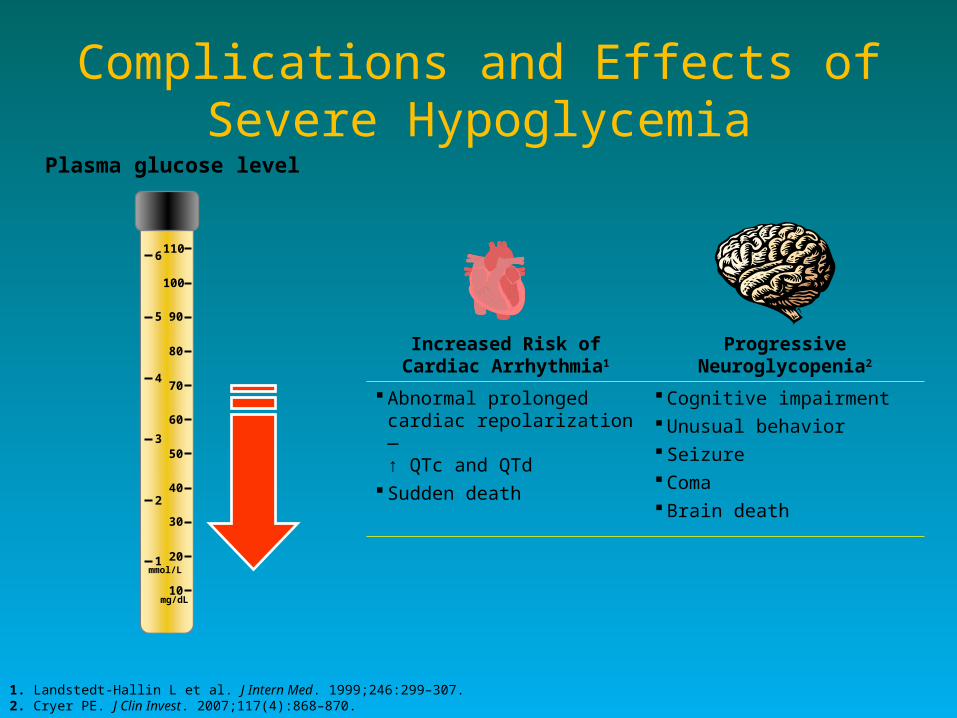
Complications and Effects of Severe Hypoglycemia
Plasma glucose level
10
20
30
40
50
60
70
80
90
100
110
1
2
3
4
5
6
mg/dL
mmol/L
1. Landstedt-Hallin L et al. J Intern Med. 1999;246:299–307.2. Cryer PE. J Clin Invest. 2007;117(4):868–870.
Increased Risk of Cardiac Arrhythmia1
Progressive Neuroglycopenia2
Abnormal prolonged cardiac repolarization—↑ QTc and QTd
Sudden death
Cognitive impairment Unusual behavior Seizure Coma Brain death
50
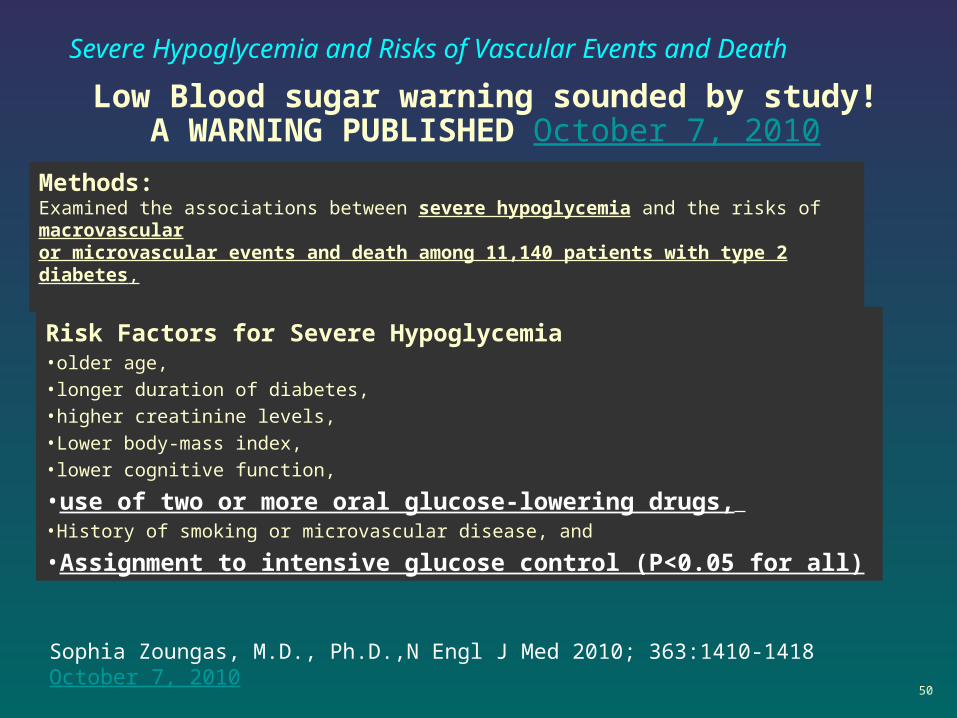
Low Blood sugar warning sounded by study!A WARNING PUBLISHED October 7, 2010
Severe Hypoglycemia and Risks of Vascular Events and Death
Methods:Examined the associations between severe hypoglycemia and the risks of macrovascularor microvascular events and death among 11,140 patients with type 2 diabetes,
Risk Factors for Severe Hypoglycemia•older age, •longer duration of diabetes, •higher creatinine levels, •Lower body-mass index, •lower cognitive function,
•use of two or more oral glucose-lowering drugs, •History of smoking or microvascular disease, and
•Assignment to intensive glucose control (P<0.05 for all)
Sophia Zoungas, M.D., Ph.D.,N Engl J Med 2010; 363:1410-1418October 7, 2010
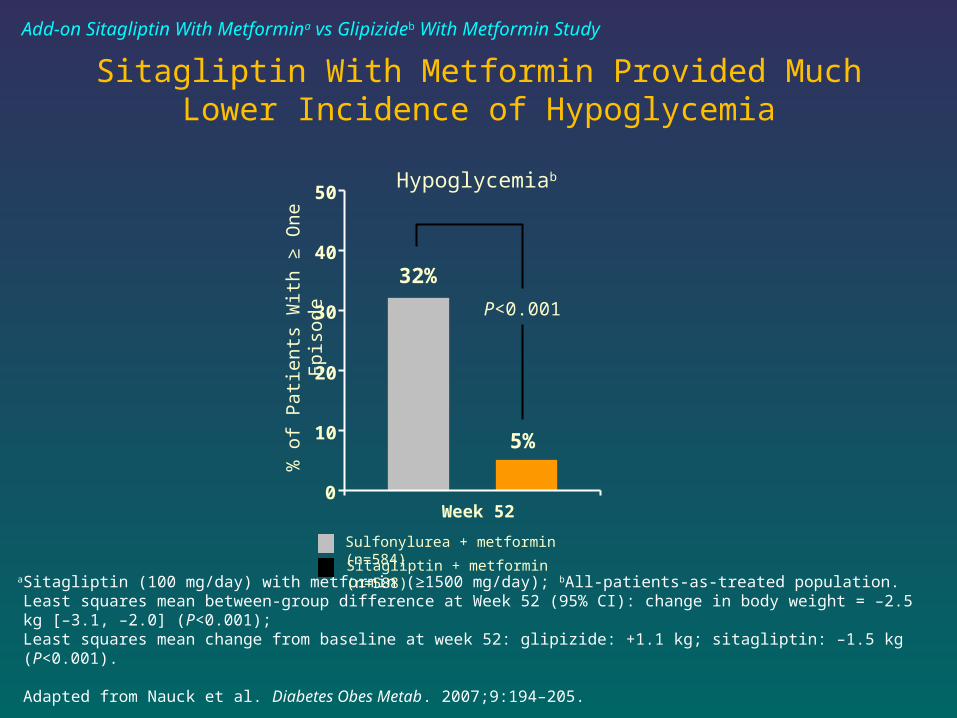
Sitagliptin With Metformin Provided Much Lower Incidence of Hypoglycemia
aSitagliptin (100 mg/day) with metformin (≥1500 mg/day); bAll-patients-as-treated population.Least squares mean between-group difference at Week 52 (95% CI): change in body weight = –2.5 kg [–3.1, –2.0] (P<0.001);Least squares mean change from baseline at week 52: glipizide: +1.1 kg; sitagliptin: –1.5 kg (P<0.001).
Adapted from Nauck et al. Diabetes Obes Metab. 2007;9:194–205.
Hypoglycemiab
P<0.001
32%
5%
0
10
20
30
40
50
Week 52
% o
f P
atie
nts
With
≥ O
ne
Epi
sode
Sulfonylurea + metformin (n=584)
Sitagliptin + metformin (n=588)
Add-on Sitagliptin With Metformina vs Glipizideb With Metformin Study
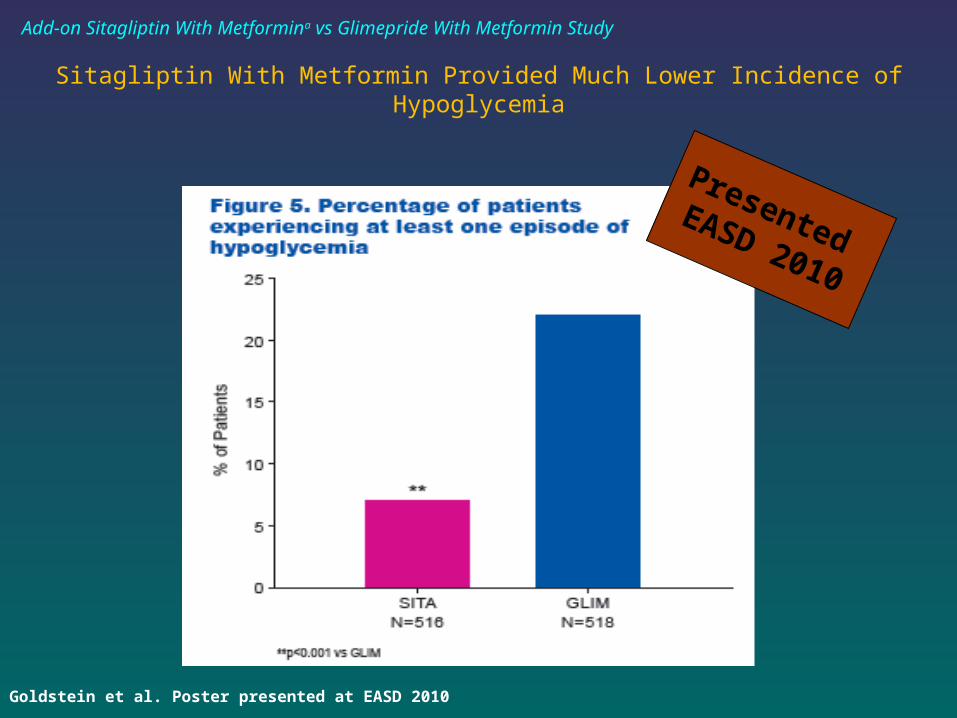
Presented EASD 2010
BJ. Goldstein et al. Poster presented at EASD 2010
Sitagliptin With Metformin Provided Much Lower Incidence of Hypoglycemia
Add-on Sitagliptin With Metformina vs Glimepride With Metformin Study
53
Guidelines
54
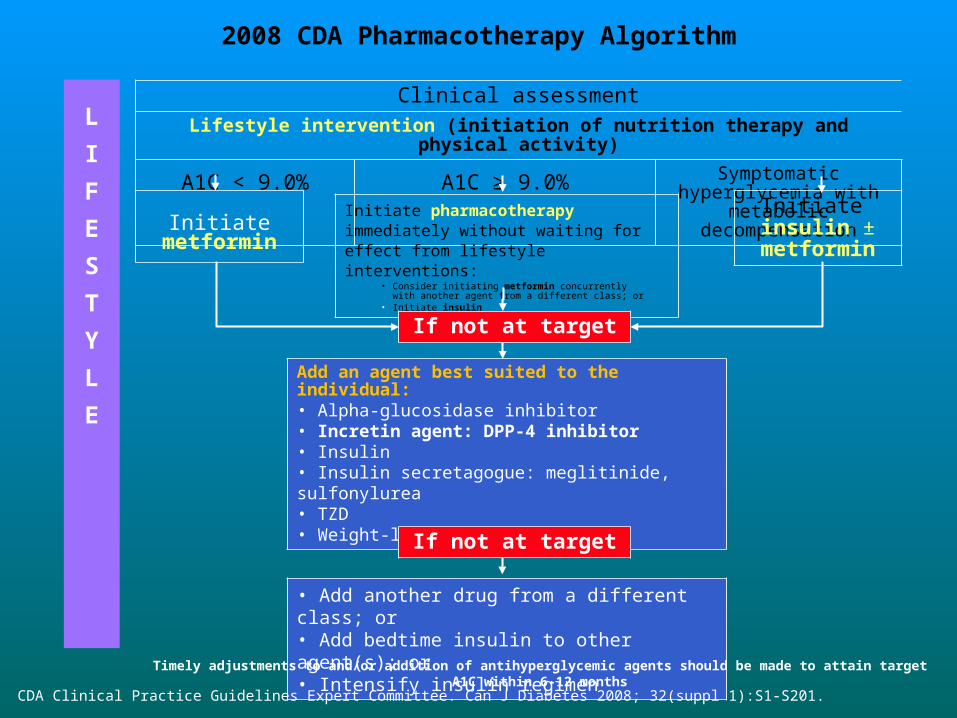
2008 CDA Pharmacotherapy Algorithm
Clinical assessmentLifestyle intervention (initiation of nutrition therapy and physical activity)
A1C < 9.0% A1C ≥ 9.0% Symptomatic hyperglycemia with metabolic decompensation
Initiate pharmacotherapy immediately without waiting for effect from lifestyle interventions:
• Consider initiating metformin concurrently with another agent from a different class; or
• Initiate insulin
Initiate metforminInitiate
insulin ± metformin
Add an agent best suited to the individual:• Alpha-glucosidase inhibitor• Incretin agent: DPP-4 inhibitor• Insulin• Insulin secretagogue: meglitinide, sulfonylurea• TZD• Weight-loss agent
• Add another drug from a different class; or• Add bedtime insulin to other agent(s); or • Intensify insulin regimen
If not at target
If not at target
L
I
F
E
S
T
Y
L
E
Timely adjustments to and/or addition of antihyperglycemic agents should be made to attain target A1C within 6-12 months
CDA Clinical Practice Guidelines Expert Committee. Can J Diabetes 2008; 32(suppl 1):S1-S201.
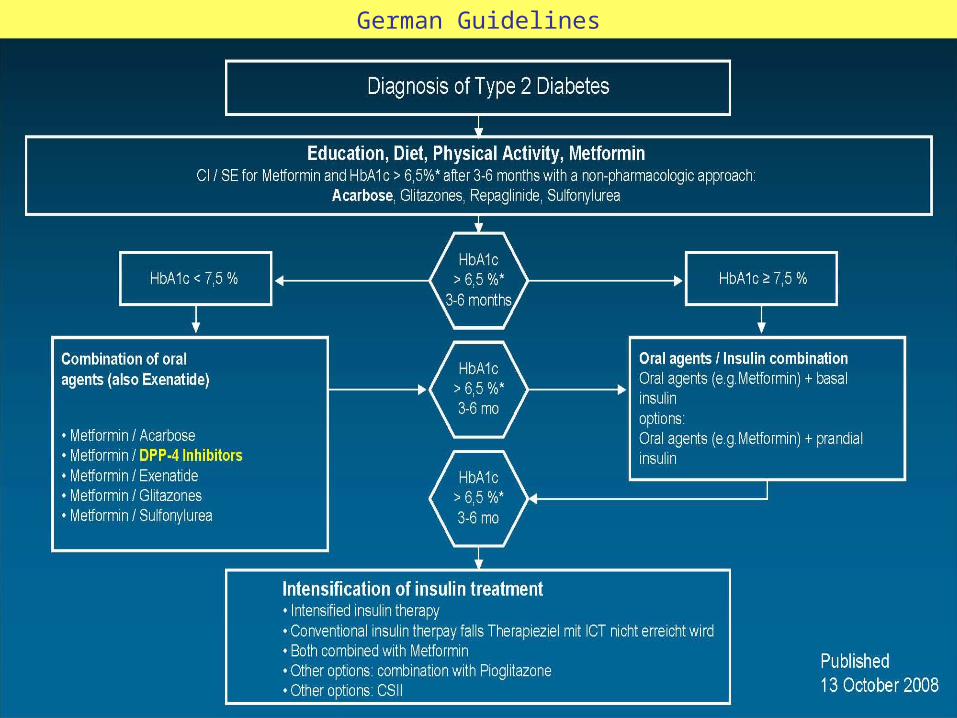
German Guidelines
57
58
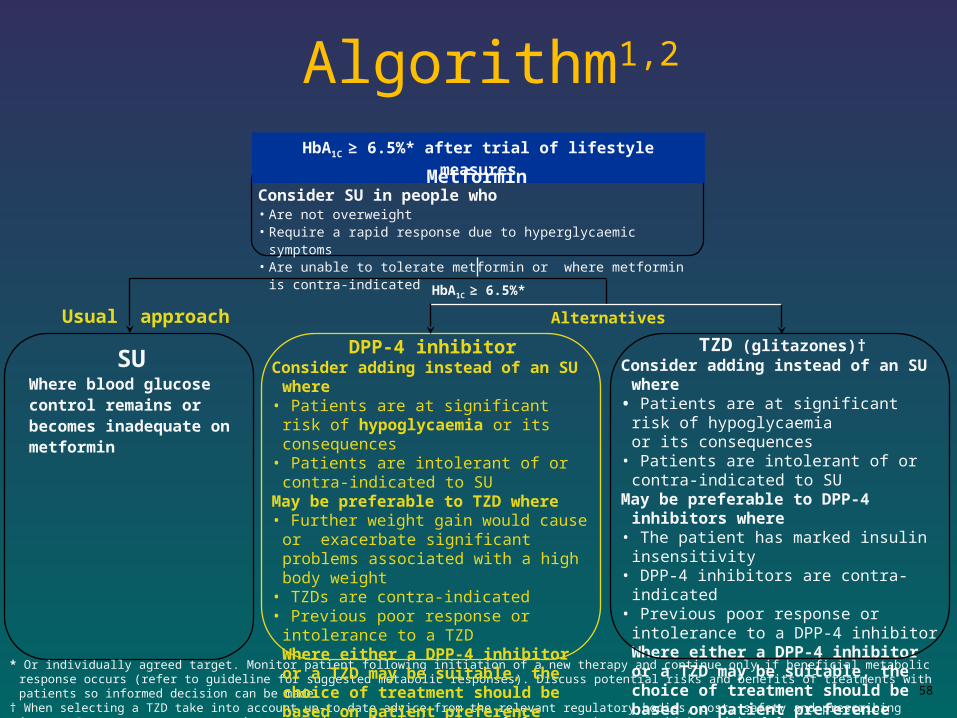
Algorithm1,2
HbA1C ≥ 6.5%* after trial of lifestyle measures
SUWhere blood glucose control remains or becomes inadequate on metformin
TZD (glitazones)†Consider adding instead of an SU where• Patients are at significant risk of
hypoglycaemia or its consequences
• Patients are intolerant of or contra-indicated to SU
May be preferable to DPP-4 inhibitors where
• The patient has marked insulin insensitivity• DPP-4 inhibitors are contra-indicated• Previous poor response or intolerance to a
DPP-4 inhibitorWhere either a DPP-4 inhibitor or a TZD may be suitable, the choice of treatment should be based on patient preference
* Or individually agreed target. Monitor patient following initiation of a new therapy and continue only if beneficial metabolic response occurs (refer to guideline for suggested metabolic responses). Discuss potential risks and benefits of treatments with patients so informed decision can be made.
† When selecting a TZD take into account up-to-date advice from the relevant regulatory bodies, cost, safety and prescribing issues. Do not commence or continue a TZD in people who have heart failure, or who are at higher risk of fracture.
HbA1C ≥ 6.5%*
Usual approach
DPP-4 inhibitorConsider adding instead of an SU where• Patients are at significant risk of
hypoglycaemia or its consequences• Patients are intolerant of or contra-indicated
to SUMay be preferable to TZD where• Further weight gain would cause or
exacerbate significant problems associated with a high body weight
• TZDs are contra-indicated• Previous poor response or intolerance to a
TZDWhere either a DPP-4 inhibitor or a TZD may be suitable, the choice of treatment should be based on patient preference
Alternatives
MetforminConsider SU in people who• Are not overweight• Require a rapid response due to hyperglycaemic symptoms• Are unable to tolerate metformin or where metformin is contra-indicated
59
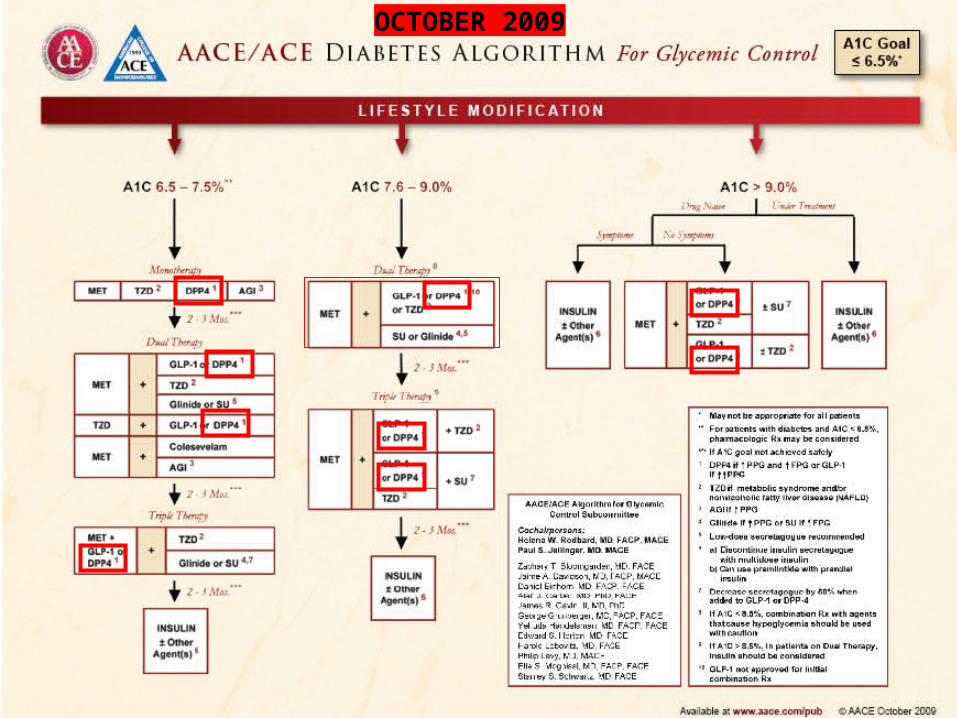
OCTOBER 2009
Summary
• DPP-IV inhibitors raise GLP-1 levels 2- to 3-fold.• Sitagliptin is the first of the DPP-IV inhibitors to
receive FDA approval. • Sitagliptin is effective in glycemic control and
HbA1c reduction.• The incidence of hypoglycemia with Sitagliptin is
very low. • Sitagliptin appears to be weight beneficial and
have an incidence of adverse reactions similar to placebo in clinical trials.
• It preserves and may improve beta cell funcion.• Recently it is recognized as safe and effective
therapy in most of the guidelines.
THANK YOU…..