tumours of the head and neck. introduction head and neck cancer is remarkable for its ability to...
TRANSCRIPT

Tumours of the head and neck
Tumours of the head and neck

IntroductionIntroduction
• Head and neck cancer is remarkable for its ability to cause extensive local tissue destruction and regional node involvement in the absence of distant metastasis

IntroductionIntroduction
• Tumours are usually confined to the primary sites
• Regional nodes & haematogenous metastasis are very rare and late in the disease process
• Loco-regional treatment by either surgery, radiotherapy or combination of the two is frequently curative

IntroductionIntroduction
• Many of the oral lesions may have had an initial lesion that were potentially curable.
• The cure could be predicted if the lesion is diagnosed early and the appropriate therapy is given before the disease reaches advance stages to become incurable

IntroductionIntroduction
• Cancer of the oral cavity in Saudi Arabia is not an uncommon disease
• It account for more than 25% of all malignancies, in the Southern region, it might reach up to 35%
• In males, it is third in frequency following lung and prostate cancer
• In females, it is second following
breast cancer

IntroductionIntroduction
• The spectrum of malignant tumours to affect the oral cavity vary widely and includes:• Surface epithelium
• Squamous cell carcinoma over 90%
• Glandular epithelium• Adenocarcinomas in females• Mucoepidermoid carcinomas in males
• Mesenchymal tissues• Lymphomas, Sarcomas are very rare

IntroductionIntroduction
Surface Epithelium1- Squamous cell Carcinoma
• Undifferentiated carcinoma• Differentiated carcinoma• Adenoid squamous
carcinoma• Verrucous carcinoma
2- Basal cell carcinoma
3- Malignant Melanoma
IntroductionIntroduction
Glandular epithelium
1- Adenocarcinoma
2- Mucoepidermoid carcinoma
3- Adenoid cystic carcinoma
4- Acinic cell carcinoma
5- Undifferentiated carcinoma

IntroductionIntroduction
Mesenchymal tissues
1. Sarcoma • Fibrosarcoma • Rhadomyosarcoma• Osteogenic sarcoma• Chondrosarcoma• Neurogenic sarcoma• Angiosarcoma• Synovial cell sarcoma
2. Hodgkin’s & non-Hodgkin’s lymphomas
3. Plasmacytoma & multiple myeloma
4. LeukaemiaMetastatic carcinoma, sarcoma

IntroductionIntroduction
• Prognostic Indicators:• Sex: Poor prognosis in females• General condition & health status of patient• T stage• Number of histologically positive nodes • Surgical margin status• Type of therapy and blood transfusion

IntroductionIntroduction
• Aetiology:• Smoking• Alcohol consumption
• They have synergistic role• Burning tar gives off a variety of active substances
e.g. benzopyrene, methyl cholanthrine, which will be broken by arylhydrocarbon hydroxylase into epoxide, carcinogen, that bind to the DNA
• Snuff dipping and Shama user

Introduction AetiologyIntroduction Aetiology
• Chronic irritation from sharp jagged teeth• Chemicals:
• Asbestos, Nickel-Chromate, in nasal and paranasal sinuses tumours
• Wood dust in Adenocarcinoma of the nose
• Dietary factors:• Vitamin A deficiency• Vitamin B deficiency, Patereson-Kelly syndrome
• Radiation exposure• Viruses:
• Human Papilloma Virus HPV• Epstein-Barr Virus EBV• Human Immunodeficiency Virus HIV• Hepatitis virus

IntroductionIntroduction
• Acquired capability of cancer cell:• Limitless replicative potential• Evading apoptosis• Self-sufficiency in growth signal• Insensitive to antigrowth signals• Sustained angiogenesis• Tissue invasion and metastasis

AssessmentAssessment
• Clinical Examination:• Tumours, when first seen,
are almost always confined to the head and neck with no distant metastasis
• Head and neck tumours are rarely irremovable, all structures can be removed with the tumour in continuity and repaired later
• The majority of cases are potentially treatable

AssessmentAssessment
• Whether to treat or not depend on:• the age• the health status of the
patient • advance stage• local disease

AssessmentAssessment
• Full assessment will lead to one of the following conclusions:• Patient is potentially
curable• Primary tumour is
curable but patient develop another illness
• Patient is incurable but should be treated
• Patient is incurable and should not be treated

AssessmentAssessment
• History:• Age:
• Patient are generally over 45 years.• Tumours affecting younger age group are usually
sinister, defective immunological make-up• Most tumours are of epithelial origin and they
require years of abuse by smoking and tobacco • Tumours in younger patients, who do not smoke,
is usually very sinister• Tumours developing in an immuno-compromised
patients do not respond to any treatment modality

AssessmentAssessment
• Complaint:• Vary widely and is often
unreliable• Painless lump which persisted
for a varying period of time • Persistent ulceration• Difficulty of wearing denture• Later Symptoms:
• Pain locally or referred to the jaw or ear
• Difficulty with chewing food and swallowing
• Altered speech and respiratory difficulty
• Asymptomatic and noticed during routine dental examination

AssessmentAssessment
• The patient general condition:• Assessed with full investigation and classified for
performance status1. Grade 0 Fully active without restriction2. Grade 1 Ambulatory but restricted in physically
strenuous activity3. Grade 2 Ambulatory but unable to carry out any
work activity4. Grade 3 Confined to bed but capable of limited
self care5. Grade 4 Confined to bed and unable to carry out
any self care
Karnofsky Status

AssessmentAssessment
• Examination:• Think in term of T Staging, delineate its border
by inspection and palpation• Record and draw the lesion from different
angles using normal anatomical landmarks• The status of teeth should be assessed as
causative and if radiotherapy is to considered

AssessmentAssessment
• Staging of cancer:• Subdividing the malignant lesion into groups
with similar behaviour• Act as a guide to appropriate treatment • Act as a guide to prognosis• Permits more reliable comparison of results
• Primary site:• Histological type, size and extend of the primary
• Node metastasis• Haematogenous metastasis

StagingStaging
• Primary Tumour:• Indicated by the letter T and the suffix 1,2, 3 or 4
represent more advancing disease• T1 – tumour 2 cm or less
• T2 – tumour more than 2 but less than 4 cm
• T3 – tumour more than 4 cm
• T4 – Tumour more than 4 cm with deep invasion of underlying tissues
• T0 – No evidence of primary tumour• Tis – Carcinoma in Situ• TX – Extend of primary tumour cannot be assessed

StagingStaging
• Lymph node:• Is used to describe progressive lymph node
involvement• N1 – Single epsilateral nodes 3 cm or less in diameter
• N2 – Single epsilateral nodes more than 3 cm but less than 6 cm, or multiple clinically positive epsilateral less than 6 cm
• N2a – Single• N2b – Multiple
• N3 – Clinically positive epsilateral more than 6 cm, Bilateral or contralateral
• N3a – Epsilateral more than 6 cm• N3b – Bilateral, each side staged separately• N3c – Contralateral only

StagingStaging
• Distant metastasis:
• M0 – No metastases present
• M1 – Metastases clinically demonstrable
• MX – Metastases cannot be assessed

StagingStaging
• TNM Staging:• Stage I: T1, N0, M0
• Stage II: T2, N0, M0
• Stage III: T3, N0, M0
T1, 2 or 3, N1, M0
• Stage IV: T4, N0 or 1, M0
T1 – 4, N2 or 3, M0
T1 – 4, N1 – 3, M1
AJCC 1983
StagingStaging
• Stage I • compromise negative nodes and operable primary
• Stage II • operable primary with operable nodes
• Stage III• inoperable due advanced primary or advanced nodal
involvement• Stage IV
• Distant metastases preclude any surgical intervention

Surgical anatomySurgical anatomy
• The Lip:• Covered with non-keratinized
stratified squamous epithelium which is transparent, appear red, and contain no hair, sebaceous gland or pigments
• On the vermilion border it closely cover the orbicularis oris muscle but on the lingual side mucous gland is present within the muscle and mucosa
• The epithelium is 2 mm away from the muscle, ulcerative lesions will be fixed early in the disease

Surgical anatomy The LipSurgical anatomy The Lip
• Lymphatic drainage:• Mucosal and cutaneous systems.• Lower lip:
• One medial trunk which drain the inner third of the lip into the submental group
• Two lateral trunk which drain the outer two-third into the submandibular lymph nodes
• Anastomosis account for bilateral metastases
• Upper lip:• Drain into the periauricular, parotid, submandibular and
submental lymph nodes

Surgical anatomy The LipSurgical anatomy The Lip
• Age and sex:• The sixth decade and Male :
female ratio is 80:1• 93% affect the lower lip with
squamous cell carcinoma, exophytic type
• 5% in the upper lip and commonly basal cell carcinoma, commoner in females• Solar exposure, more radiation on
the lower lip• Commoner in fair complexion• Smoker mainly pipe• In the upper lip, SCC metastasizes
earlier than lower lip

Surgical anatomy Surgical anatomy
• The buccal mucosa:• Covered with non-
keratinizing stratified squamous epithelium with multiple minor salivary glands
• It is tight over the buccinator muscle and fixed to the upper and lower sulci
• Lymphatic drainage:• The submandibular
lymph nodes to the lower deep cervical chain

Surgical anatomySurgical anatomy
• The tongue:• Specialized keratinized
epithelium with collection of minor salivary gland and muscle fibres
• The interlacing muscle fibres form an easy pathway for cancer spread and the constant movement of the tongue disseminates the disease widely
• Excision should be wide with 2 cm safe margin

Surgical anatomy The tongueSurgical anatomy The tongue
• A disease of the middle age and elderly with equal sex incidence
• 85% occurs in the lateral border of the anterior 2/3 while tip, dorsum and ventral surface are rarely involved
• The lesion may be infiltrative (small on the outside but palpation shows deep invasion) or exophytic and usually of the well-differentiated type

Surgical anatomy The tongueSurgical anatomy The tongue
• Lymph drainage:• Tip of the tongue:
• To the submental lymph nodes – to the lower deep cervical chains
• The anterior 2/3:• the lower deep cervical chains – jugulo-
omohyoid nodes• Suprahyoid block dissection of no value
• The posterior 1/3:• drain to the upper deep cervical chains
• The tip and middle part of the tongue have rich bilateral capillary network but less in the lateral margins
• The U-shaped floor of the mouth drain to the submandibular lymph nodes
• Bilateral drainage from the anterior part of the U

Surgical anatomySurgical anatomy
• The floor of the mouth:• Anterior medial part:
• Commoner than the lateral part• Spread medially into the ventral
surface of the tongue and laterally
• Deep spread to the base of the tongue and the hyoglossus and genioglossus muscles
• Shows bilateral lymphatic spread to the submandibular and the submental nodes

Surgical anatomy The floor of the mouthSurgical anatomy The floor of the mouth
• Lateral part:• Spread medially to the side of the tongue • Lateral spread to the alveolar ridge where presence
or absence of the teeth govern the outcome:• Teeth act as a barrier against buccal spread• In edentulous patient, the alveolar process has resorbed
and cortex is incomplete, tumour reaches the cancellous spaces and the canal and spread through the nerve.
• Deeper spread, mylohyoid muscle act as a barrier anteriorly, posteriorly the floor is close to the skin, appear as a palpable lump in the submandibular area

Surgical anatomySurgical anatomy
• The mandible:• Carcinoma of the lower
alveolus affects the antero-lateral part and spread to the floor of the mouth
• Tongue and floor of the mouth tumours reach the lower alveolus by marginal spread in the mucosa and submucosa overlying the sublingual, submandibular glands and the mylohyoid muscle.

Surgical anatomy The mandibleSurgical anatomy The mandible
• They act as barrier against deep infiltration
• Alveolar bone above the mylohyoid line is initially affected
• Edentulous jaws, mylohyoid line is on the occlusal ridge and the loss of the cortical bone barrier will allow tumour to spread downward into the medullary cavity

Surgical anatomy The mandibleSurgical anatomy The mandible
• The inferior alveolar nerve provide a pathway for perineural spread in a predominately proximal direction with little involvement of the bone
• Nerve looks clinical normal till late • Spread is not continuous, multiple pathological
samples is required
• Lymphatic spread to the submandibular lymph nodes
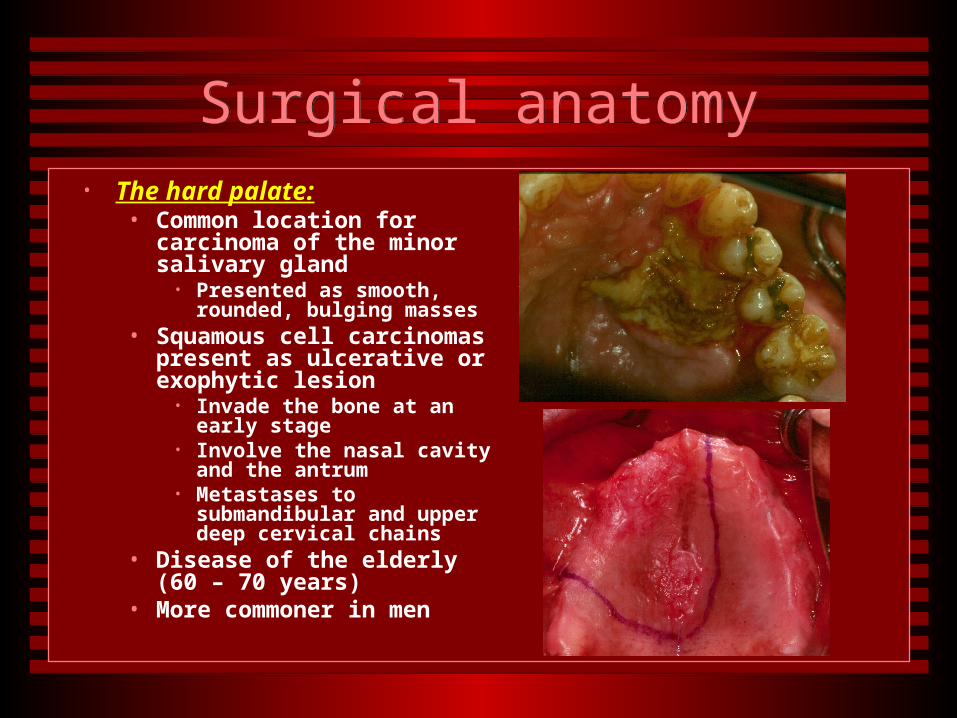
Surgical anatomySurgical anatomy• The hard palate:
• Common location for carcinoma of the minor salivary gland
• Presented as smooth, rounded, bulging masses
• Squamous cell carcinomas present as ulcerative or exophytic lesion
• Invade the bone at an early stage
• Involve the nasal cavity and the antrum
• Metastases to submandibular and upper deep cervical chains
• Disease of the elderly (60 – 70 years)
• More commoner in men

Surgical anatomySurgical anatomy
• The maxillary sinus:• The sinus is related to the
orbit, nose, alveolar process, infratemporal fossa and nasopharynx.
• It has an outlet to the nose, ethmoid sinuses and the root of the teeth
• The posterior ethmoidal air cell is separated from the optic nerve by a bar of bone but it is missing in 10% of cases and only encased in a sheath of dura, extension into the brain.

Surgical anatomy The maxillary sinusSurgical anatomy The maxillary sinus
• The inferior orbital fissure provide a route for entry of tumours into the orbit, the periostium offer an excellent resistant barrier to spread into the orbit
• The roots of the upper premolars and molars and the alveolus are in intimate contact to the floor
• The infratemporal fossa is the space behind the maxillary antrum and it connects to the para-pharyngyeal space, and the sphenoid bone superiorly with foramen spinosium and ovale with their emerging nerves

Surgical anatomy The maxillary sinusSurgical anatomy The maxillary sinus
• Lymphatic drainage:• Not fully understood• Drain posteriorly to the retropharyngeal nodes • Directly to the jugulo-digastric nodes• If it cross to the nose or the cheek it will drain to
submandibular lymph nodes
• Aetiology:• Wood dust, nickel, shoe factory and mustard
gas• Snuff is a contributing factor

Surgical anatomy The maxillary sinusSurgical anatomy The maxillary sinus
• Classification• T1 - confined to the mucosa of the infrastructure• T2 - confined to the mucosa of the suprastructure
without bone destruction - confined to infrastructure
mucosa with bone destruction of medial and inferior wall only
• T3 - More extensive tumour invading the cheek, the orbit, anterior ethmoid and pterygoid muscle
• T4 – Invading the cribriform plate, posterior ethmoid and sphenoid sinuses, nasopharynx, pterygoid plat and the base of the skull

Surgical anatomy The maxillary sinusSurgical anatomy The maxillary sinus
• Malignant tumours:• Squamous cell carcinoma:
• 50% of all malignant lesions of the sinus• Bone destruction and invasion of nose, ethmoid, orbit, anterior wall
and cheek, and palate or alveolar ridge and buccal sulcus
• Adenocarcinoma:• Uncommon, occurs in people working in wood industry• Histologically two types, high or low grade• Invade bone and present the same way like SCC
• Adenoid cystic carcinoma:• Shows as solid areas of cells instead• Distant metastasis and perineural invasion, infra-orbital, maxillary,
greater palatine and olfactory nerves

Diagnostic TechniquesDiagnostic Techniques
• Tissue Biopsy:• This is the mainstay of tumor
diagnosis coupled with high degree of suspicion
• Fine needle aspiration:• A 22-gauge needle
attached to small volume syringe
• Smear is prepared and stained after fixation with alcohol
• Minimize tumor spillage and sample error in small lesion

Diagnostic TechniquesDiagnostic Techniques
• Toluidine blue vital staining:
• Acidophilic metachromatic nuclear stain that colors sites of squamous cell carcinoma but not adjacent normal mucosa surfaces
• 1 – 2% applied to dry surfaces and the dye diffuse into tissue through the large intercellular canaliculi

Diagnostic TechniquesDiagnostic Techniques
• Incisional:• Small portion of the lesion
with the adjacent normal tissues to facilitate correct diagnosis
• To visualize the transitional zone between tumor and normal tissue
• Performed at the periphery to avoid the necrotic central area
• Excisional:• Removal of the entire lesion• Done as a primary
treatment

Surgical anatomySurgical anatomy
• Radiography:• Routine X-Ray studies:
• Useful in cases of bony involvement • Panoramic views shows lytic lesions• Lateral soft-tissue films shows the extend into the nasopharynx
or hypopharynx
• Angiography:• Define oral malignancy – mainly avascular• Shows the relation to major vessels prior to surgery• Selective transcatheter embolization for bleeding control or
decreasing tumor vascularity preoperatively

Diagnostic TechniquesDiagnostic Techniques
• Sialography:• Cannulation of parotid and submandibular ducts and the
infusiopn of contrast material
• CT-Scan:• Define the gross limits and determine the actual depth of
tumor• Evaluate adjacent bony structures and erosions involving the
paranasal sinuses, base of skull and the cervical spine
• Magnetic Resonance Imaging:• Gives a better resolution for soft tissue tumors

Diagnostic TechniquesDiagnostic Techniques
• Nuclear Scanning:• The use of tumor-seeking radiopharmaceutical
material• Bone scanning:
• Uses Technetium 99-labeled phosphate complexes• Very sensitive and positive in the presence of bony lesions
before their detection by conventional radiographs• Lacks specificity, infection, inflammation and even
trauma result in positive scan

Diagnostic TechniquesDiagnostic Techniques
• Salivary gland scanning:• I.V. Technetium shows an increased uptake in papillary
cystadenoma.• Might occur with other benign or malignant tumors as a
focal areas
• Gallium-67 scanning:• Gallium isotopes concentrate in a rapidly growing tumors• Best in epidermoid carcinomas and lymphomas • Used in lymphoma staging

Diagnostic TechniquesDiagnostic Techniques
• Tumor markers:• Tumor markers are molecules occurring in blood or
tissue that are associated with cancer and whose measurement or identification is useful in patient diagnosis or clinical management.
• Tumor markers are most useful for monitoring response to therapy and detecting early relapse
• They are generally products of the cancer cell, although none is unique to cancer cells; they represent aberrant tumor production of a normal element

Diagnostic TechniquesDiagnostic Techniques
• Tumor markers can be used for one of four purposes:
• 1- screening a healthy population or a high risk population for the presence of cancer
• 2- making a diagnosis of cancer or of a specific type of cancer
• 3- determining the prognosis in a patient• 4- monitoring the course in a patient in remission or
while receiving surgery, radiation, or chemotherapy.

Diagnostic TechniquesDiagnostic Techniques
• Carcinoembryonic Antigen “CEA”• The CEA was one of the first oncofetal antigens to be
described and exploited clinically. • It is a complex glycoprotein and is associated with the
plasma membrane of tumor cells, from which it may be released into the blood.
• The primary use of CEA is in monitoring colorectal cancer, especially when the disease has spread and to check recurrence
• Other cancers produce elevated levels of this tumor marker, including lymphoma, head and neck cancer and cancers of the breast, lung, pancreas