true bifurcation lm stenosis (medina with very extensive ... · true bifurcation lm stenosis...
TRANSCRIPT

True Bifurcation LM Stenosis (Medina 1,1,1) With Very Extensive Calcification:
CABG Or PCI ?
T. SantosoUniversity of Indonesia Medical School,
Medistra Hospital,
Jakarta, Indonesia
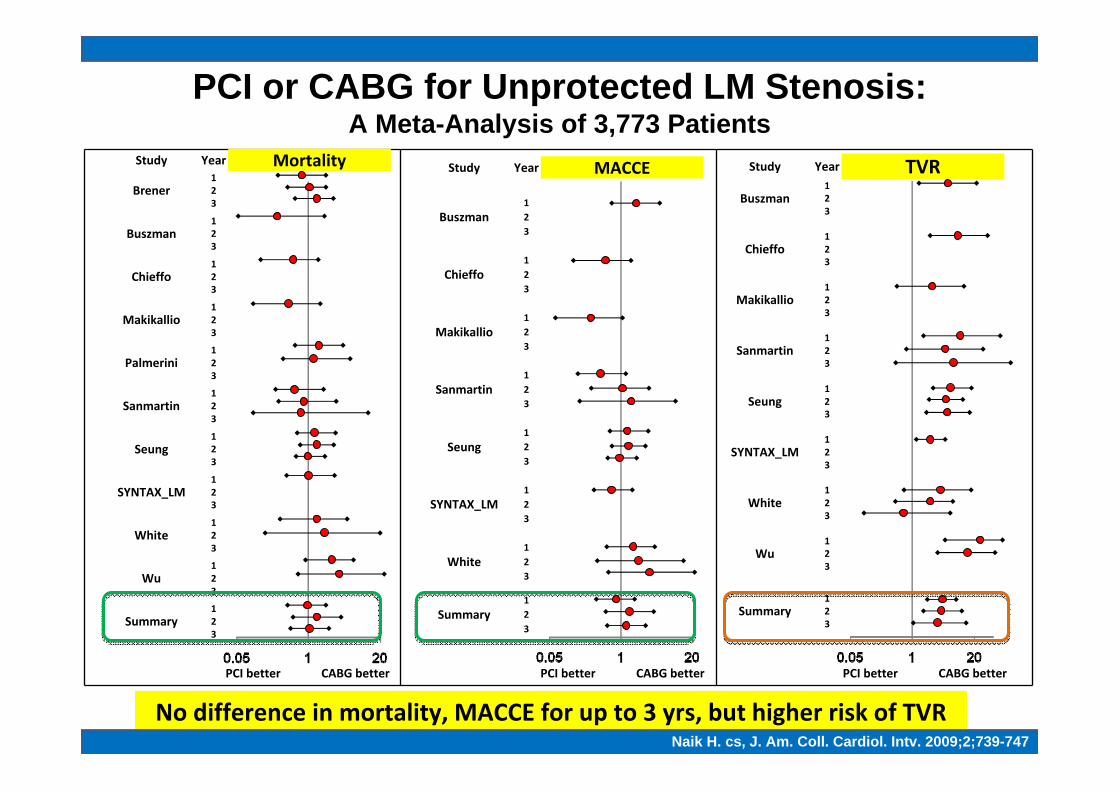
PCI or CABG for Unprotected LM Stenosis:A Meta-Analysis of 3,773 Patients
Study Year Mortality
Brener123
Buszman123
Chieffo123
Makikallio123
Palmerini123
Sanmartin123
Seung123
SYNTAX_LM123
White123
Wu123
Summary123
PCI better CABG better
Study Year MACCE
Buszman123
Chieffo123
Makikallio123
Sanmartin123
Seung123
SYNTAX_LM123
White123
Summary123
PCI better CABG better
Study Year TVRBuszman
123
Chieffo123
Makikallio123
Sanmartin123
Seung123
SYNTAX_LM123
White123
Wu123
Summary123
PCI better CABG better
Naik H. cs, J. Am. Coll. Cardiol. Intv. 2009;2;739‐747
No difference in mortality, MACCE for up to 3 yrs, but higher risk of TVRNaik H. cs, J. Am. Coll. Cardiol. Intv. 2009;2;739-747

Profile Of Case: Calcified LM• Male, 75 yrs old with progressive angina at rest since one week• Other illnesses: hypertension, Type II DM, chronic renal failure (on dialysis), COPD, history of left lower pulmonary lobectomy
• Underwent coronary angiography 3 weeks ago, told to have high risk for PCI or surgery.
• PE: BP 180/91, otherwise unrevealing• Lab: Hb 10.6 g/dL, ureum 80 mg/dL, creatinine 2.35 mg/dL, blood sugar 135 / 243 mg/dL, enzymes slightly elevated
• ECG: normal• Chest film: mild cardiomegaly, no pulmonary congestion• Echo: LVH, EF 75%• Treatment on admittance: clopidogrel, aspirin, cilostazol, carvedilol, irbesartan, ISDN (IV drip), enoxaparin, short actinginsulin (actrapid)

• Very tight LM ostial stenosis
• GC: 7F EBU, difficult to engage
• Damping of pressure every time GC was engaged (required GW insertion to avoid this)
• Fluoroscopy: massive calcification noted in LM & proximal‐mid‐LAD
Coronary Angiogram

• LM: short, with tight ostial stenosis 90% until bifurcation (Medina 1,1,1)• LAD: diffuse 70‐90% stenosis in the prox‐mid‐segments• LCX: ostial 80% stenosis, then another 80% stenosis in the proximal segment• RCA: 80% stenosis distally (not shown)
SYNTAX SCORESYNTAX SCORE : 39 EuroSCORE : 8 : 39 EuroSCORE : 8 Parsonnet SCORE : 28Parsonnet SCORE : 28Clinical SYNTAX SCORE : 78Clinical SYNTAX SCORE : 78 Global Risk Class: HighGlobal Risk Class: High
Coronary Angiogram

How Should We Treat This Patient?
1. PCI
2. CABG

Risk Assessment In Pts Undergoing Revascularisation With LM Is Of Paramount Importance
Risk Assessment In Pts With LM Lesions1
Risk ModelRisk Model ClinicalClinical AngiographicAngiographic PCIPCI CABGCABG
EuroSCORE 17 0 + + +
Mayo Clinic Risk Score 17 0 + + ‐
ACEF 3 0 ‐ + ‐
AHA/ACC Classification 0 11 (per lesion) + ‐ +
SYNTAX 0 11 (per lesion) + + +
STS 40 2 ‐ + ‐
Clinical SYNTAX Score 3 11 (per lesion) + ‐ +
Global Risk Classification 17 11 (per lesion) + + +
NERS2 21 33 + ‐ +
Specific evaluation in LM pts
1. Modified after Garg S, cs. JACC Intv 2010;3:891‐901; 2. Chen SL, cs. JACC Intv 2010;3:632‐41; 3. Capodanno D., et al. JACC Intv. 2011;4;287‐297
No. variables used to calculate score
Validated in PCI/CABG

This patient has SYNTAX SCORE = 39→ higher risk for PCI
High score (>33) LM disease (& Registry pts) are best treated with CABG at least in the short term (3 years follow‐up)
This patient has Parsonnet Score = 28 & EuroSCORE = 8 → High risk for CABG
Clinical (Parsonnet & EuroSCORE) Scores
Nashef SAM, cs. Eur J Cardiothoracic Surg 1999;16:9-13; Parsonnet V, cs.Circulation 1989;79(suppl I):I-3-I-12; Kappetein P, TCT 2010
P=0.004 31.4%
17.9%
Months Since Allocation
Cum
ulat
ive
Even
t Rat
e (%
)
0 12 24
40
0
20
30
10
36
TAXUS™ (N=155)CABG (N=166)High SYNTAX Scores (33) LM Subset
Preoperative Risk Classification
30d Ope
rative M
ortality
Percen
tEuroSCORE Patients Died
0 ‐ 2 (low risk) 4529 36 (0.8%)
3 ‐ 5 (medium risk) 5977 182 (3.0%)
> 6 (high risk) 4293 480 (11.2%)
Total 14799 698 (4.7%)
Parsonnet Score EuroSCORE
Angiographic Score (SYNTAX)

0
Time (months)
Cardiac de
ath free
survival (%)
100
90
80
70
60
12 24
SYNTAX score
96.1%
94.6%
78.1%
LOWMIDDLEHIGH
P = 0.004*
0 Time (months)
Cardiac de
ath free
survival (%)
100
90
80
70
60
12 24
GRC
98.4%
84.0%
68.6%LOWMIDDLEHIGH
P < 0.001*
Capodanno et al, Am Heart J 2010:159:103-9
Combined Clinical (EuroSCORE) & Angiographic (SYNTAX) Scores:Global Risk Classification (GRC)
GRC has the better predictive ability for both safety & efficacy endpointsThis patient is in the high risk class both for PCI & CABG
Low Low Inter-mediate
Low Low Inter-mediate
Inter-mediate
Inter-mediate High
0-2
3-6
> 6
< 22 23-32 > 33
SYNTAX score
Euro
SCO
RE

Combined Clinical & Angiographic Risk Scores:Clinical SYNTAX Score (CSS)*
*CSS = SYNTAX Score x (age/EF + 1 for each 10 mL the CrCl < 60 mL/min per 1.73 m2)
0
10
20
30
40
0 180 360 540 720Time (days)
Cum
ulat
ive
card
iac
mor
talit
y ra
te
(%)
PCI
Log-Rank P<0.001
High CSS: 25.6%
Low CSS: 2.6%Mid CSS: 1.0%
0
10
20
30
40
0 180 360 540 720Time (days)
Cum
ulat
ive
card
iac
mor
talit
y ra
te
(%)
CABG
Log-Rank P=0.011
High CSS: 9.1%
Mid CSS: 2.7%Low CSS: 3.9%
1. Garg S, cs. Circ Cardiovasc Interv 2010;3:317-326; 2. Capodanno D, cs. JACC Intv. 2011;4;287-297
CSS < 15.6 : lowCSS 15.6-<27.5: mid
CSS > 27.5: high
CSS of patient: 78 CSS of patient: 78 →→ patient is in a high risk for PCI & CABGpatient is in a high risk for PCI & CABG
With a EuroSCORE of 8, SYNTAX Score of 39,Clinical SYNTAX Score of 78, High GRC
the patient is clearly in ahigh risk for either PCI or CABG
What would you do ?

Favoring CABG:• Very diffuse multi-vessel disease with SYNTAX scores>33 may increase
the likelihood of incomplete revascularization (which will lead to worse long term outcome)7
• Heavily calcified lesions are unsuitable for stenting8
• Left main plus tight RCA stenosis may increase the risk of PCI• ? Renal Dysfunction (HR=12 if Sr Cr>2 mg/dl)
Clinical & Angiographic Characteristics Influencing The Choice Of Treatment Strategy In This Patient
1.Lee MS, et al.JACC 2006;47:864‐70; 2.Rodes‐Cabau J, et al. Circulation 2008;118:2374‐81; 3. Tamburino C, et al. Am J Cardiol 2009;103:187‐93; 4. Kim YH, et al. Am J Cardiol 2009;98:1567‐70;
5.Tamburino C, et al. Cathet Cardiovasc Interv 2009;73:291‐8; 6. Kim WJ, et al. JACC Interv 2009;2:956‐63; 7. Capodano D. cs, JACC Intv. 2009;2;731‐738; 8. Park SJ, et al. Circ Cardiovasc Intervent 2009;2:59‐68
Favoring PCI:• LM stenosis with high EuroSCORE & presented with acute coronary
syndrome is associated with increased risk of death & MI1-5
• Elderly patient has lower risk of stroke with PCI compared to CABG2
• Patient is already fully anticoagulated• Even though the patient is a diabetic, in LM stenosis, aside of increased
TVR, PCI results in similar rates of death, MI, stroke compared to CABG6

If you want to do PCI, how ?
Guiding Catheter (GC) ?:1. 6F 2. 7 F3. 8F
GC: good back up, 7 or 8F. Be careful not to induce ostial LM spasm or dissection
If you want to do PCI, how ?
Guide Wire (GW) ?:1. Single 2. Double (LAD / LCX)

GC: good back up, 7 or 8F. Be careful not to induce ostial LM spasm or dissectionGW: double (LAD / LCX)
If you want to do PCI, how ?
Balloon ?:1. Semicompliant balloon2. High pressure balloon 3. Cutting balloon

GC: good back up, 7 or 8F. Be careful not to induce ostial LM spasm or dissectionGW: double (LAD / LCX)
Balloon: high pressure balloon (compliant/semicompliant balloon may increase the chance of edge dissection, balloon rupture, or even vessel rupture). Cutting balloon – difficult to introduce
If you want to do PCI, how ?
DES or BMS ?:1. DES 2. BMS
GC: good back up, 7 or 8F. Be careful not to induce ostial LM spasm or dissectionGW: double (LAD / LCX)
Balloon: high pressure balloon (compliant/semicompliant balloon may increase the chance of edge dissection, balloon rupture, or even vessel rupture). Cutting balloon – difficult to introduce DES: DES with minimal late loss, & bigger cell size if another
DES needs to be implanted in the SB
If you want to do PCI, how ?
Is lesion preparation important?:1. Yes2. No

GC: good back up, 7 or 8F. Be careful not to induce ostial LM spasm or dissectionGW: double (LAD / LCX)Balloon: high pressure balloon (compliant/semicompliant balloon
may increase the chance of edge dissection, balloon rupture, or even vessel rupture). Cutting balloon – difficult to introduce DES: DES with minimal late loss, & bigger cell size if another DES
needs to be implanted in the SBLesion preparation important: rotablation
If you want to do PCI, how ?
Any adjunctive devices needed?1. IVUS, FFR 2. IABP3. All

GC: good back up, 7 or 8F. Be careful not to induce ostial LM spasm or dissectionGW: double (LAD / LCX)Balloon: high pressure balloon (compliant/semicompliant
balloon may increase the chance of edge dissection, balloon rupture, or even vessel rupture). Cutting balloon – difficult to introduce DES: DES with minimal late loss, & bigger cell size if another
DES needs to be implanted in the SBLesion preparation important: rotablation IVUS, FFR important: IVUS catheter may be difficult to introduce
in the presence of heavy calcificationNo IABP
If you want to do PCI, how ?

PCI
Massive calcification & long segmental, severe stenosis in the proximal & mid‐LAD precluded the use of IVUS.
After predilatation of the LM & LCX ostial lesions, proximal LCXstenosis was stented with good result

Note: the lines of calcifications along the LAD course.The long segmental LAD stenosis was very resistant to high pressure balloon dilatation (note: the dog boning effect)
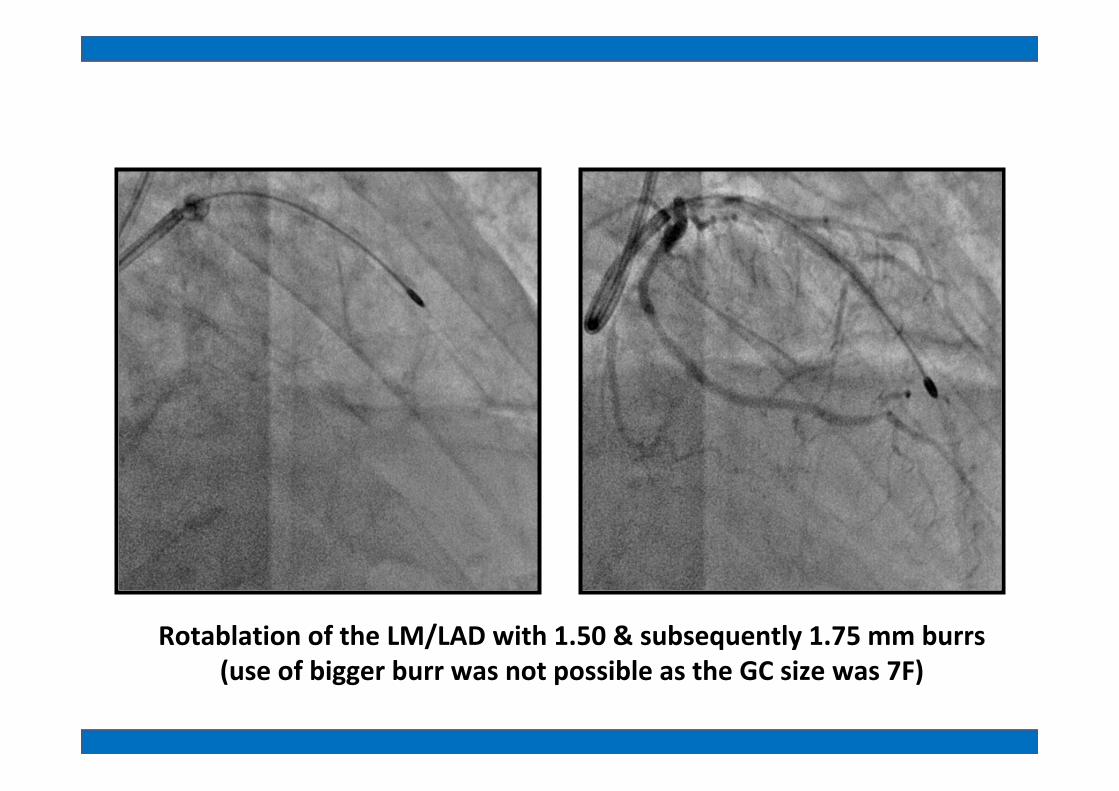
Rotablation of the LM/LAD with 1.50 & subsequently 1.75 mm burrs(use of bigger burr was not possible as the GC size was 7F)

Successful placement of overlapping drug‐eluting stents BioMatrixTM in the proximal‐mid‐LAD

A. LM‐LCX stenting (BioMatrixTM)
B. Balloon crushing of LM‐LCX stent
C. After GW exchange, further dilatation of LM‐LCX stent
D. Kissing balloon dilatation
A
B
C
D
DK Crush Technique (1)

DK Crush Technique (2)
E. DES stent (NOBORI 3.5x24 mm) placement from LM ostium to proximal LAD (overlapping with previously implanted stent)
F. Balloon was slightly withdrawn & inflated again with a higher pressure & to create the flaring effect in the LM ostium (to be followed by final kissing balloon dilatation)
E F

Suddenly blood pressure dropped to below 23/9 mmHg & HR to 28 bpm. Patient became apneic. Patient was intubated & CPR was rapidly
instituted. Adrenaline, dopamine & dobutamine were administered.Contrast injection demonstrated big perforation in the proximal LAD &
cardiac tamponade.
1. Call a surgeon2. Ask for an echo‐machine3. Immediate fluoroscopy
guided‐pericardiocentesis4. Others
What would you do ?

Suddenly blood pressure dropped to below 23/9 mmHg & HR to 28 bpm. Patient became apneic. Patient was intubated & CPR was rapidly
instituted. Adrenaline, dopamine & dobutamine were administered.Contrast injection demonstrated big perforation in the proximal LAD &
cardiac tamponade. A balloon was introduced & inflated to temporarily seal the leakage..

While doing cardiac massage, fluoroscopy guided pericardial paracenthesis was rapidly performed. Subsequently covered stent (3x16 mm) was implanted to seal the perforation.
After 500 cc of pericardiocenthesis, blood pressure increased to 218/96 mmHg. IABP was not inserted.Repeat contrast injection confirmed complete sealing of perforation.

Gradually patient’s condition improved. No protamine injection was given.
Fluoroscopy showed no more contrast accumulation in the pericardial cavity.Blood pressure was stabile at 161/63 mmHg & spontaneous breathing was noted.

On the third day, before pulling out of the drainage catheter, angiogram was repeated. This showed beautiful result with no residual stenosis, TIMI III
flow, Gr 3 myocardial blushing, & absence of perforation.
Patient survived !!

1. CABG (as soon as possible)2. CABG (elective)3. Medical treatment
What would you do further?

• Patient was put on triple antiplatelet therapy:–Aspirin, clopidogrel and cilostazol–At least for one year
•Other medications: carvedilol, irbesartan, oral nitrates, rosuvastatin, short acting insulin (actrapid)
•Chronic dialysis continued
• Patient died 2 months later because of hemorrhagic stroke
Medications

• Risk stratification is necessary to determine treatment strategy
• This elderly patient is at high surgical risk (high EuroSCORE & Parsonnet SCORE, high GRC), but also at high risk for PCI (high SYNTAX SCORE, high CSS, high GRC)
• As the patient presented with acute coronary syndrome, & was already anticoagulated, PCI was still considered a reasonable option
• However, the severe, extensive calcification and multiple & diffuse long lesion made it not very suitable for stenting .
• Patient has perforation during postdilatation (before final kissing balloon dilatation) which was successfully managed by fluoroscopy guided pericardiocentesis.
Summary (1)

Lessons learned regarding the technique:• Do not panic or give up• Lesion preparation, especially in complex anatomy, is important.• Calcification is a big enemy of interventionist. In case of extensive,
severe calcification:– For predilatation never use compliant balloon (1. balloon may rupture,
2.”dog‐boning effect” at the proximal/distal end of balloon or balloon oversizing at full inflation may lead to dissection/perforation)
– Rotablation is helpful. Be reminded that LM & proximal LAD are big vessels. Use of burr > 2.00 mm may be necessary to achieve better debulking.
– For postdilatation also use appropriately sized high pressure (non‐compliant) balloon
• If possible, use of IVUS is important• Fluoroscopy guided pericardiocentesis is always faster than echo‐
guided pericardiocentesis
Summary (2)