tructions & disclosure statement course 30: ot · and neck are the elimination of chronic...
TRANSCRIPT

INSCou
PurpThe sinus Targ
ObjeAfter
ReqUsin
12
34
5
6
SpoNeithcoma pu This provthat not ipres The
TRUCTIOurse 30: Ot
pose/goal purpose of tses, and wit
get Audien
ectives r reading this Identify k
quirementsng this self-d1. Review t2. Read and
http://ww3. Access t4. Provide y
have trou5. Complete
70% is re6. Receive
CNOR a
onsorship her the progmercial or inrpose other
activity wasvider of contiare approvemply that CCentation.
contact hou
ONS & DISCtorhinolary
Statementthis chapter hin the soft t
nce: Periop
s chapter, thkey nursing c
s for Succeirected learnhe above lead review the
ww.cc-instituthe online quyour purchasuble locatinge the evaluaequired to pacertificate ofnd or CRNF
ram plannern-kind suppothan for whi
s approved fonuing educa
ed by CCI arCI or the Ca
rs for this ac
CLOSUREyngological
t is to describtissues of th
erative RNs
he participanconsideratio
essful Comning modulearning objec
e course white.org/docs/puiz which is ase order numg this, pleaseation questioass, and youf completion
FA credential
rs, authors, oort has been ich it is appr
or 1.4 contaation by the Cre recognizelifornia State
ctivity will ex
E STATEM Surgery
be common he oropharyn
nt should be ns for patien
mpletion :
ctives. ch is availabphippenchapavailable at mber as foune contact CCns and succ
u have two an and 1.4 conl, the contac
or reviewersobtained fo
roved by the
ct hours by California Std as continue Board of N
xpire on June
ENT
procedures nx and head
able to: nts undergoi
ble at: pters/2012/0http://start.cnd on the CCCI at 888-257cessfully pasattempts. ntact hours i
ct hours will b
s have any cr this offerin FDA.
the Competetate Board o
uing educatioNursing appr
e 17, 2014.
in the ear, wand neck.
ing otorhinol
08/30/coursec-institute.orCI bookstore7-2667. ss the ten ite
in approximabe added to
conflict of intg. There is n
ency and Crof Nursing, Pon for registeroves or end
within the no
laryngologic
e-30.pdf rg/s3/Phippee order confi
em multiple-c
ately 2-3 weo your online
erest relatedno discussio
redentialing Provider numered nurses
dorses any p
ose and para
cal surgical p
en-Course-3irmation ema
choice quiz.
eeks. If you CCI accoun
d to this progon of a produ
Institute, anmber 15613.
. This recogproduct in the
anasal
procedures.
30 ail. If you
A score of
hold the nt.
gram. No uct used for
n approved Activities nition does e

CHAPTER 30
Chapter Contents1081 Introduction
1081 Anatomy
1086 Special Precautions During
Otolaryngeal Procedures
1086 Procedures of the Ear
1104 Procedures of the Nose and
Paranasal Sinuses
1114 Procedures of the Oropharynx and
Head and Neck
1135 Endnote
1135 References
Otorhinolaryn-gological SurgeryRose Moss
INTRODUCTIONTh e fi eld of otorhinolaryngological surgery (ie, ear, nose, throat, head, and neck surgery) has diversifi ed during the past 50 years. Th e numerous operative or invasive procedures involving this part of the anatomy have led to subspecialty training in certain fi elds. Th e goals of most procedures in the ear, nose, and throat and in the head and neck are the elimination of chronic infections, the extirpation of tumors, the preservation or improvement of hearing, and the manip-ulation of the food and air passages when obstructed or injured.
Th is chapter focuses on the common procedures in the ear, within the nose and paranasal sinuses, and within the soft tissues of the oropharynx and head and neck.
ANATOMYEars
Th e ears are special sense organs involved in enabling hearing as well as maintaining balance. Th ey are divided into external, middle, and inner regions. Th e external ear is made up of the visible auricle and the external auditory canal. Th e ear and canal act as a funnel for the transmission of air vibrations that are eventually transformed into understandable sound. Th e external auditory canal ends at the tym-panic membrane, or eardrum. Th e eardrum is the division between the external ear and the middle ear.
On the other side of the tympanic membrane is the middle ear cavity, or tympanic cavity. Within the middle ear cavity are the three bones that are involved in the transmission and modifi cation of

1082 Section 3: Operative and Invasive Procedures
sound energy. Th is energy is transported to the inner ear through the oval window. Th e fi rst bone is called the malleus (“hammer”), the second is the incus (“anvil”), and the third bone is the stapes (“stirrup”). Th e footplate of the stapes sits within the oval window.
Th e inner ear is located deep within the temporal bone. It is composed of a bony portion as well as a membranous portion. Th e membranous portion contains a special fl uid that is placed in motion when sound energy is transmitted from the tympanic membrane through the bones of hearing. Within the area called the bony labyrinth are the vestibule, the semicircular canals, and the cochlea. Th e vestibule and the semicircular canals are involved in balance mechanisms. Th e cochlea is the organ of hearing.
Nose and Paranasal SinusesTh e nose is made up of a combination of bone, cartilage, and mucous membrane
(Fig. 30.1). Th e upper third of the external nose is composed of the nasal frontal, ethmoid, and maxillary bones. Th e lower two thirds of the nose are made up of carti-lage. Th e internal nose contains openings on each side called the nares. Th e posterior openings into the nasopharynx are called choanae. Th e anterior skin-lined portion of the nasal cavity is called the vestibule.
Th e nasal septum divides the nose into two chambers lined by mucous mem-brane. Th e septum can become deviated and cause obstruction of the nasal airway. Th e nasal cavity communicates with the ear through the eustachian tube. Th e hard and soft palates divide the nasal cavity from the oral cavity. Th e lateral wall of the nasal cavity contains mucous membrane-lined bony projections called turbinates, or conchae (Fig. 30.2). Usually, there are bilateral inferior, middle, and superior turbinates. Rarely seen is a fourth turbinate called the supreme turbinate.
Figure 30.1
External portion of the nose.

Chapter 30: Otorhinolaryngological Surgery 1083
30
Th e grooves between the turbinates and the lateral nasal walls are called meati. Th e inferior meatus contains the nasolacrimal duct opening. Th e lacrimal glands produce tears, which eventually fl ow into the nasal cavity. Th e middle meatus is the most important to know about. Th is is the one into which the maxillary, frontal, and anterior ethmoidal sinuses drain. Th e sphenoidal sinuses drain posteriorly and superiorly within the nasal cavity (Fig. 30.3).
Th e sinuses are air-fi lled pockets lined with mucous membranes. Th e maxillary sinuses are the largest and most accessible. Th e paranasal sinuses drain into the nasal cavity through openings called ostia. When these ostia become blocked, infections usually follow.
Th e nasal cavity has a rich vascular supply from both the external and internal carotid arteries. Th e proximity to the brain and the orbit makes infections within the nasal cavity and sinuses potentially dangerous.
Figure 30.2
Anatomical structures of the
lateral nasal wall.
Figure 30.3
Lateral wall of the sinuses
shown without turbinates.

1084 Section 3: Operative and Invasive Procedures
Tonsils and AdenoidsTh e tonsils are found within the oropharynx, which is posterior to the oral cavity
(Fig. 30.4). Th e tonsils are part of the ring of Waldeyer lymphoid tissue present in the throat. Th ey are found between the folds of mucosa known as the anterior and posterior tonsillar pillars and are usually seen on either side of the throat when the mouth is opened and the tongue is depressed. Th e ease of visualization depends on the size of the tonsils.
In contrast, the adenoid tissue, which is oft en called a pharyngeal tonsil, is not easily visualized. Th e adenoid tissue is found in the nasopharynx, which is the most superior portion of the throat. Although visualization of the adenoid is occluded by the soft palate and the uvula, the adenoid pad and the nasopharynx can be seen by using a mirror. In this indirect fashion, cooperative patients can be examined.
Parotid GlandTh e parotid gland is the largest of the major salivary glands. Th e gland is found
on either side of the face in the area of the angle of the mandible (Fig. 30.5). Th e salivary glands deliver their secretory product, saliva, into the oral cavity and the oropharynx. Saliva functions as a lubricant and an acid buff er and contributes to the digestion of food. Diseases aff ecting the salivary glands are seen as either altera-tions in the production of saliva or abnormalities of the gland itself.
Th e parotid gland consists of two portions. Th ere is a superfi cial lobe, as well as a deep lobe that is in contact with the parapharyngeal space. Th e parotid gland emp-ties its contents through the parotid duct (also known as Stensen’s duct). It enters the oral cavity opposite the second upper molar tooth.
Th e facial nerve is the most important structure associated intimately with the parotid gland. Th e most superfi cial portion of the facial nerve passes through the main substance of the parotid gland. It divides into fi ve main branches: temporal, zygomatic, buccal, mandibular, and cervical. Th e mandibular branch is especially important because it lies deep under the platysma muscle in the neck.
Figure 30.4
Tonsils and oropharynx.

Chapter 30: Otorhinolaryngological Surgery 1085
30
TracheaExamination of the neck involves identifi cation of palpable structures (Fig. 30.6).
In infants, the most easily palpable structures are diff erent from those in the adult. In the adult, the most prominent structure in the neck is the thyroid cartilage, or the Adam’s apple. Th is is usually found along the midline of the neck. Immediately below this prominent cartilage is the cricoid cartilage. In adults, the cricothyroid membrane is easily palpable between the cricoid and the thyroid cartilage most of the time. Th e cricothyroid membrane can be entered in an emergency in most adults.
In infants up to 2 months of age, the most palpable structure is usually the hyoid bone. Th is horseshoe-shaped bone is found superior to the thyroid cartilage. Most infants and young children have short necks with a large amount of subcutaneous fat, which makes palpation diffi cult. In addition, the cartilages are much soft er. Th erefore, emergency access through the neck into a pediatric airway is much more diffi cult than in the adult.
Figure 30.5
The parotid gland.
Figure 30.6
Trachea and thyroid cartilage.
1086 Section 3: Operative and Invasive Procedures
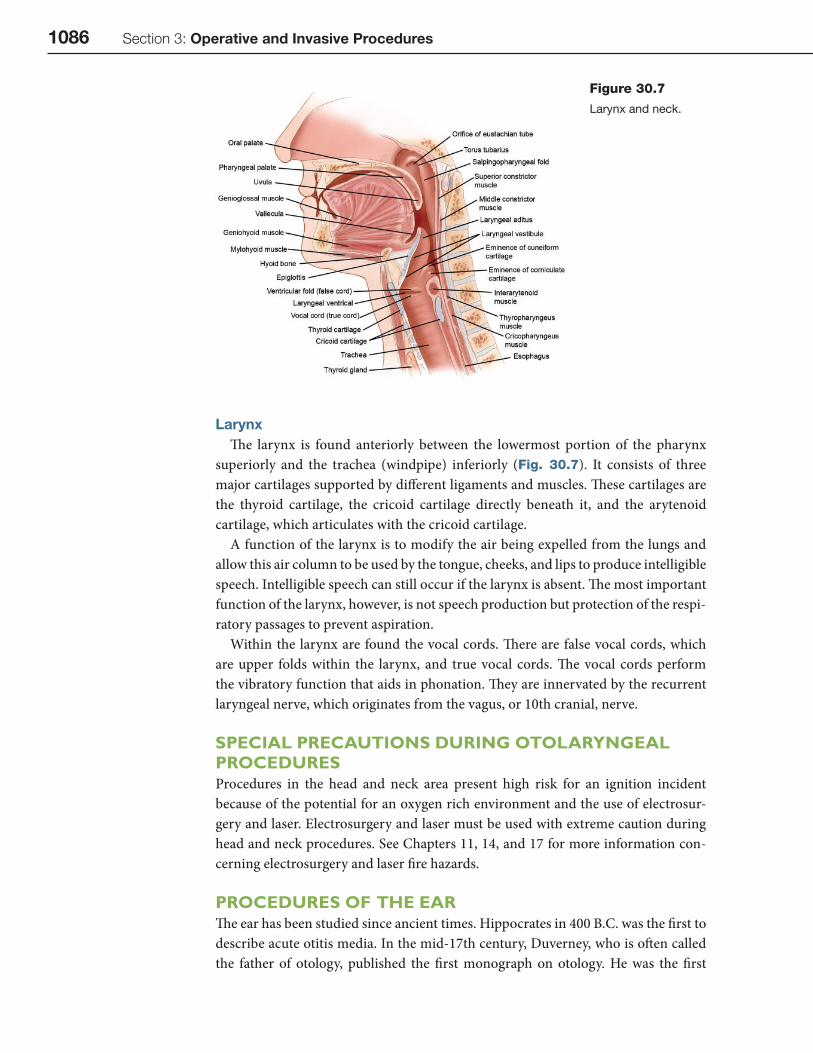
LarynxTh e larynx is found anteriorly between the lowermost portion of the pharynx
superiorly and the trachea (windpipe) inferiorly (Fig. 30.7). It consists of three major cartilages supported by diff erent ligaments and muscles. Th ese cartilages are the thyroid cartilage, the cricoid cartilage directly beneath it, and the arytenoid cartilage, which articulates with the cricoid cartilage.
A function of the larynx is to modify the air being expelled from the lungs and allow this air column to be used by the tongue, cheeks, and lips to produce intelligible speech. Intelligible speech can still occur if the larynx is absent. Th e most important function of the larynx, however, is not speech production but protection of the respi-ratory passages to prevent aspiration.
Within the larynx are found the vocal cords. Th ere are false vocal cords, which are upper folds within the larynx, and true vocal cords. Th e vocal cords perform the vibratory function that aids in phonation. Th ey are innervated by the recurrent laryngeal nerve, which originates from the vagus, or 10th cranial, nerve.
SPECIAL PRECAUTIONS DURING OTOLARYNGEAL PROCEDURESProcedures in the head and neck area present high risk for an ignition incident because of the potential for an oxygen rich environment and the use of electrosur-gery and laser. Electrosurgery and laser must be used with extreme caution during head and neck procedures. See Chapters 11, 14, and 17 for more information con-cerning electrosurgery and laser fi re hazards.
PROCEDURES OF THE EARTh e ear has been studied since ancient times. Hippocrates in 400 B.C. was the fi rst to describe acute otitis media. In the mid-17th century, Duverney, who is oft en called the father of otology, published the fi rst monograph on otology. He was the fi rst
Figure 30.7
Larynx and neck.

Chapter 30: Otorhinolaryngological Surgery 1087
30
anatomist to describe the mastoid air cells communicating with the middle ear cav-ity. He also established that pus coming from the ear did not originate in the brain.
Infections of the ear and mastoid were potentially deadly before the advent of antibiotics. Th e operations designed at the birth of otology revolved around the elimination of infection. It was not until the 19th century that operations to cure infec-tion were successfully performed on a regular basis. In the early 1900s, the operating microscope added a new dimension to ear operations designed to cure infection and deafness. With the advent of antimicrobial agents, the necessity for operative inter-vention within the ear decreased dramatically. Th e most common surgical procedure performed in the ear today is the insertion of ventilation tubes.
MyringotomyDefi nition and Indications
Myringotomy refers to a tiny incision of the tympanic membrane (eardrum) to remove thickened secretions; in most cases, a small tympanostomy tube is inserted into the tympanic membrane to aerate the middle ear for a prolonged time ( MedicineNet.com, 2008a). Myringotomy is either diagnostic or therapeutic. It is usually performed on a pediatric patient who has had chronic middle ear eff u-sions or recurrent acute otitis media. Other indications for this procedure include (MedicineNet.com, 2008a):
• Malformation of the tympanic membrane or Eustachian tube • Downs syndrome • Cleft palate • Barotrauma (injury to the middle ear due to a reduction of air pressure)
Nursing Implications
ANESTHESIA
Most myringotomies are performed with general inhalation anesthesia. Th e use of intravenous (IV) catheters is usually not necessary, but the decision is made by the anesthesia provider. Th e procedure can be performed using local anesthesia. Th is type of anesthesia, however, is typically reserved for older children and adults.
POSITION
Th e patient is placed in the supine position. Aft er general anesthesia is induced and appropriate monitoring devices are placed, the procedure is initiated by turning the patient’s head with the operative ear facing the surgeon.
ESTABLISHING AND MAINTAINING THE STERILE FIELD
Myringotomy is considered by some surgeons as a minor procedure. It does, how-ever, deserve the same preparation as for any procedure. Th e ear is usually draped with sterile towels only. Before any sterile towels are placed, the microscope should be in position to be easily swung into the operative fi eld. A sterile sheet may or may not be placed over the chest and body of the patient. Th e skin preparation is determined by the surgeon. Many surgeons use alcohol or another skin antiseptic agent. Some surgeons do not request skin preparation. If the ear is prepared, the circulating nurse
IVIntravenous

1088 Section 3: Operative and Invasive Procedures
should include the ear, the postauricular area, and the face. Th e scrub person may stand next to the surgeon or across from him or her and close to the Mayo stand.
EQUIPMENT AND SUPPLIES
A dedicated myringotomy tray should be available. Table 30.1 lists recommended instruments for a myringotomy set. Th e diff erent types of ventilation tubes available can be confusing. Th e ventilation tube is usually chosen by the surgeon before or at the time of the procedure. Th erefore, it is wise to have the ventilation tubes located where they are easily accessible to the nursing personnel. A microscope with either a 200- or a 250-mm focal length lens is most oft en used.
PHYSIOLOGICAL MONITORING
Myringotomies are normally quick procedures. Th e patient may or may not be intubated. Th e circulating nurse must be readily available to assist the anesthesia provider, especially during initial induction of and recovery from anesthesia.
SPECIMENS AND CULTURES
A culture may be taken to determine the type of microorganism present.
DRUGS AND SOLUTIONS1
Normal saline, skin antiseptic solution, and an otic antibiotic solution should be available.
PHYSICIAN ORDERS
Th e patient is given liquids when awake and is discharged when he or she is alert and stable, and meets all of the discharge criteria.
Procedure
EXPOSURE AND INCISION
An ear speculum is inserted in the external auditory canal while the ear is viewed under the microscope. Cerumen is usually removed with cerumen spoons. Aft er this is completed, the ear can be irrigated with alcohol or other skin antiseptic agent. Th e use of a skin antiseptic is usually followed by copious irrigation with normal
Table30.1
Myringotomy Instruments
Wire loop or cerumen remover
Alligator forceps
Beaver handle and myringotomy blade (No. 7100 or 7120)
45° pick
90° pick
Rosen pick
Nos. 3, 5, and 7 Baron suction tubes

Chapter 30: Otorhinolaryngological Surgery 1089
30
saline. Aft er the tympanic membrane has been identifi ed and described by the sur-geon, a myringotomy scalpel is used to incise the tympanic membrane (Fig. 30.8). Aft er the incision is made, it is imperative to have the appropriate Baron suction tips that are used to aspirate any middle ear eff usion. Because some of the eff usions may be tenacious, duplicate suction catheters should be available.
DETAILS
Th e various ventilation tubes are then inserted through the myringotomy incision using either alligator forceps or special introducers. Mounting of the ventilation tube is at the discretion of the surgeon. Th e scrub person should be aware of the surgeon’s preference. It is important at the time of mounting of the ventilation tube that a min-imal amount of contact exists between the gloves of the scrub person or the surgeon and the ventilation tube. Th e ventilation tube should be primarily handled with the tip of the alligator forceps or the introducer. Th e alligator forceps or the introducer should be handed to the surgeon so that the surgeon does not have to look away from the microscope. A 45-degree pick or a curved Rosen pick may also be used for proper positioning of the tube.
CLOSURE
Aft er the tube is placed, an antibiotic solution may or may not be used by the sur-geon. If it is used, it is introduced by placing the drops through the ear speculum or with a syringe. A cotton ball is usually placed in the ear canal aft er the instillation of antibiotic solutions. Occasionally, a small amount of bleeding occurs. Because blood
Figure 30.8
(A) Myringotomy incision,
(B) Aspiration of fl uid,
(C) Insertion of ventilation tube,
and (D) Ventilation tube in place.

1090 Section 3: Operative and Invasive Procedures
can occlude the lumen of the ventilation tube, vasoconstricting solutions should be available for instillation into the ear before transferring the patient to the postanes-thesia care unit (PACU).
Postprocedure Care
Aft er the procedure is completed, the patient is awakened and transported to the PACU. Because the procedure is short, the patient usually awakens quickly. If the patient is a child, the postanesthesia period can be traumatic. Th e child should be reunited with the parent as soon as it is feasible. Th ere is no dressing. However, cotton may be placed in the ears.
Potential Complications
Otorrhea and bleeding may occur.
TympanoplastyDefi nition and Indications
Tympanoplasty is a broad term that has been used to refer to any procedure per-formed to repair perforations within the eardrum or repair defects of middle ear structures for restoring sound conduction pathways. Simple tympanoplasty can be done to protect middle ear structures from direct exposure owing to loss of the membrane cover. Tympanoplasties are classifi ed as Types 1 through 5 (Encyclopedia of Surgery, 2008a):
• Type I tympanoplasty—also called myringoplasty, involves only the restoration of the perforated eardrum by graft ing the area of the perforation.
• Type II tympanoplasty—this procedure is used for tympanic membrane per-forations with erosion of the malleus; it involves graft ing onto the incus or the remains of the malleus.
• Type III tympanoplasty—this procedure is indicated for destruction of two ossicles, with the stapes still intact and mobile; it involves placing a graft onto the stapes, and providing protection for the assembly.
• Type IV tympanoplasty—this procedure is used for ossicular destruction, which includes all or part of the stapes arch; it involves placing a graft onto or around a mobile stapes footplate.
• Type V tympanoplasty—used when the footplate of the stapes is fi xed.
Nursing Implications
ANESTHESIA
Tympanoplasty can be performed with the use of local anesthesia, but general anesthesia is usually preferred by most surgeons. One of the techniques used is hypotensive anesthesia, which helps create a bloodless fi eld. If nitrous oxide is used, it is discontinued before the graft is placed. Nitrous oxide diff uses into the middle ear cavity and leads to disruption of the graft ing procedure.
POSITION
Most oft en, the surgeon performs this procedure while sitting. Before transferring the patient to the bed, the bed should be turned so that the patient’s head rests on the
PACUPostanesthesia Care
Unit

Chapter 30: Otorhinolaryngological Surgery 1091
30
foot of the bed and the feet are positioned at the head of the bed. Th is facilitates place-ment of the base of the microscope under the bed and enables the surgeon to position his or her feet under the bed. Th e patient is placed in the supine position, close to the edge of the bed, with the head turned and the operative ear up and stabilized. A doughnut-shaped stockinet or small headrest support device is used to stabilize the head and protect the nonoperative ear. Th e circulating nurse should ensure that the nonop-erative ear is within the hole of the doughnut or headrest to avoid pressure on the ear.
ESTABLISHING AND MAINTAINING THE STERILE FIELD
Th e ear and the hair immediately around the ear may or may not be shaved. Th e operating microscope is placed at the head of the bed. It is draped in a sterile fash-ion, because it will be manipulated by the surgeon. Th e surgeon may examine the ear before the circulating nurse scrubs and prepares the patient. Th erefore, a simple myringotomy set should be available for this purpose. Aft er the patient’s head has been positioned, the ear can be prepared with a variety of antibacterial solutions. Th e region to be prepared should include the ear, the postauricular area, and the face just past the midline.
Th e eye on the operative side is taped closed with an eye occluder. Aft er this is done, a plastic drape with a preformed hole can be pressed onto the skin with the ear protruding through the hole. Lint-free drapes are preferred. It is imperative that gloves used by the surgeon and the scrub person be free from powder and lint. For-mation of granulomas secondary to powder within the middle ear has been reported to cause irreversible hearing loss.
EQUIPMENT AND SUPPLIES
As for any otological procedure, a proper assortment of otological instruments is necessary. Most of these instruments are used in conjunction with the operating microscope. Because many of these instruments are unique for otological proce-dures, it is important for the scrub person to be fully familiar with the instruments. Diff erent sets are available commercially and include a variety of fi ne instruments for the mobilization of tissue within a small space. Varieties of fi ne ossicular instru-ments are also essential. Appropriate suction catheters are also found within these sets. In addition to the microinstruments, a basic surgical set should also be avail-able. Th is should include fi ne scissors, (eg, iris and Metzenbaum scissors) to harvest a graft . Bone instruments, including power drills, must be readily available if drilling becomes necessary during a simple tympanoplasty.
Table 30.2 lists a sample tympanoplasty set. Other supplies include bone wax, oxidized cellulose, absorbable hemostatic sponges, and a nerve stimulator (in rare cases the facial nerve may be encountered). Th e surgeon may use Silastic sheeting rather than the patient’s teraporalis fascia autograft .
PHYSIOLOGICAL MONITORING
A tympanoplasty can be a short procedure or it can take several hours, depending on the surgeon’s fi ndings. If the procedure is performed using local anesthesia, constant monitoring of the patient’s electrocardiogram (ECG), blood pressure, and oxygen saturation by pulse oximetry is essential. Th e patient is asked to lie supine with the head
ECGElectrocardiogram

1092 Section 3: Operative and Invasive Procedures
turned in one position for a period of time; therefore, the patient’s comfort level is mon-itored constantly. Comfort measures such as padding for elbows and heels are supplied aft er positioning the patient on the bed. A pillow under the knees is off ered to reduce pressure on the back. Th e patient may even be placed in a fl exed (lawn chair) position for comfort, with care not to compromise adequate operating position for the surgeon.
If the patient is placed under general anesthesia, the same comfort measures are applied. Th e circulating nurse must be readily available to assist the anesthesia provider during induction of and emergence from anesthesia. Th e suction must be in close reach of the anesthesia provider.
SPECIMENS AND CULTURES
Specimens may include excess tissue used for the graft and/or remnants of the tympanic membrane. Cultures are taken as indicated by clinical fi ndings.
DRUGS AND SOLUTIONS
Drugs and solutions that may be needed include the following:
• Lidocaine (Xylocaine) 1% with 1:100,000 epinephrine (Adrenalin) • 1:100,000 epinephrine • Neosporin ointment
Tympanoplasty Set
Sickle knife
Lancet knife
Round (weapon) knife
Flap knife
Rosen knife
Roller knife
Stapes knife
Tympanoplasty knife
Micro-cup forceps: right, left, and straight
Alligator forceps: fi ne, plain, or serrated
Bellucci scissors
45° pick
90° pick
Rosen pick
Drum elevator
Gimmick elevator
Duckbill elevator (three sizes)
Fisch excavators: left and right
Microcurettes
Iris and tenotomy scissors
Iris forceps with and without teeth
Tenon block
Table30.2

Chapter 30: Otorhinolaryngological Surgery 1093
30
• Colistin sulfate (Coly-Mycin) otic suspension • Absorbable hemostatic sponges or oxidized cellulose • Tis-U-Sol solution
PHYSICIAN ORDERS
Th e patient is given a regular diet. Th e IV catheter should be kept open until the patient is taking liquids successfully. Antiemetic and analgesic drugs are adminis-tered. Th e patient can ambulate depending on comfort level.
LABORATORY AND DIAGNOSTIC STUDIES
CBC, urinalysis, chest radiographs, and ECG are obtained as indicated. Th e sur-geon may also order an audiogram with pure-tone air and bone conduction curves with adequate narrow-band masking as well as speech discrimination scores; mas-toid radiographs; and computed tomography (CT) scans, which may help in deter-mining ossicular defects and cholesteatoma size and extension.
Procedure
INCISION AND EXPOSURE
Th e procedure usually begins with an injection of a local anesthetic mixed with epi-nephrine. Th e injections are performed in a four-quadrant fashion within the external auditory canal. Incisions are then made within the canal skin at 6 and 12 o’clock posi-tions. Th ese incisions are connected with diff erent canal microknives. Th is forms a fl ap. Th e fl ap is raised medially until the entire fi brous portion of the tympanic mem-brane is identifi ed. Before beginning the procedure or at the surgeon’s discretion, the graft can be taken from the temporalis muscle fascia. Th e incision is made within the hairline using standard surgical scalpels. Th e incision is carried down through the subcutaneous tissue until the fascia of the muscle can be identifi ed (Fig. 30.9). A portion of the fascial layer is removed that is slightly larger than the size of the perforation to be repaired. Aft er the graft has been harvested, it is usually given to the surgical assistant or the scrub person for preparation. Th e graft is prepared by compressing it between a fascia press forceps. Th en it is placed on a Tefl on block for drying. A dry graft allows the surgeon better pliability during the graft ing stage.
CTComputed
Tomography
Figure 30.9
Incision for tympanoplasty
and mastiodectomy.

1094 Section 3: Operative and Invasive Procedures
DETAILS
Aft er the perforation is identifi ed, diff erent micropicks are used to freshen the perforation margin. Th is can also be done with fi ne curettes or cup-biting forceps. Next, the previously created tympanomeatal fl ap is raised superiorly (Fig. 30.10). Absorbable gelatin sponge is then placed within the middle ear cavity to act as a support for the graft . Th e graft is then taken and placed in the medial surface of the tympanic membrane. Aft er the graft is placed in its proper position, the tympanomeatal fl ap is brought down to its normal position. Th e external auditory canal is then packed with absorbable gelatin. Antibiotic solution or ointment can also be used for this purpose.
CLOSURE
A wide variety of techniques exists for packing the external auditory canal. Th e scrub person should inquire as to the surgeon’s preference. If a simple tympanoplasty was performed without any external incisions, the ear can be dressed in a variety of ways. Dressings are not necessary, however, if the incisions were all within the external auditory canal. A mastoid dressing is described later. Th e area of graft ing is closed in a standard fashion using absorbable suture for the subcutaneous tissue and nonabsorbable suture for the skin.
Postprocedure Care
Th e patient is immediately transported to the PACU. Typical postprocedure orders include the administration of antiemetics as well as analgesics. Most tym-panoplasties of the simple type can be performed on an outpatient basis. Th e patient is instructed to keep water away from the operative ear until further advised. If the procedure was performed through the external canal only, the dressing may be an adhesive bandage (Band-Aid). If a postauricular incision was created, however, a pressure bandage of fl uff s (Kerlix) and Kling bandage is used to wrap around the head and over the operative ear.
Figure 30.10
Perforation and fl aps for
tympanoplasty.

Chapter 30: Otorhinolaryngological Surgery 1095
30
Potential Complications
As with any wound, there is always the potential for infection within the operated area. Th e graft site rarely becomes infected. However, hematomas forming in this area have been reported. Additional complications include the failure of the graft to take, with a persistence of the perforation.
MastoidectomyDefi nition and Indications
A mastoidectomy is performed for eradication of infected mastoid air cells result-ing from ear infections, (ie, mastoiditis or chronic otitis, or by infl ammatory disease of the middle ear [cholesteatoma]); the procedure involves removal of the infected portion of the mastoid bone when medical treatment is ineff ective (Encyclopedia of Surgery, 2008b). Mastoidectomy may or may not be done in conjunction with a tym-panoplasty. In addition, a mastoidectomy may be performed along with an ossicular reconstruction.
A simple mastoidectomy involves a postauricular incision through which the air cells of the mastoid process are eradicated by drilling through the bone with burrs. Th e external canal and the middle ear are at times not involved (Fig. 30.11). A modifi ed radical mastoidectomy involves removal of a portion of the ear canal, allowing drainage from the mastoid into the canal. Th e tympanic membrane and middle ear ossicles are preserved. A radical mastoidectomy is performed for severe chronic mastoiditis. In this procedure, the middle ear cavity and the mastoid antrum are combined into a large single cavity. Periodically, this cavity is inspected and cleaned on an outpatient basis. Usually, the ossicles and the tympanic membrane are entirely removed. Th roughout these procedures, an additional structure that becomes important to identify and protect is the facial nerve.
Nursing Implications
ANESTHESIA
As for other ear procedures, mastoidectomy is performed using general hypoten-sive anesthesia. Before the procedure is started, the surgeon oft en injects a combina-tion of local anesthetic with epinephrine.
POSITION
Th e patient’s head is turned with the operative side up and stabilized. As for tympanoplasty, the bed is reversed before positioning the patient. Th e basic prin-ciples described earlier are also used for mastoidectomy as well as other middle ear procedures.
ESTABLISHING AND MAINTAINING THE STERILE FIELD
Th e sterile fi eld is established by clipping hair behind the ear (if ordered by the surgeon) and preparing the ear and the surrounding areas with a skin antiseptic agent. Th e ear is covered with a plastic drape with a preformed hole. Th e operating microscope is also draped with a sterile plastic drape.

1096 Section 3: Operative and Invasive Procedures
EQUIPMENT AND SUPPLIES
In addition to a tympanoplasty set, additional instruments that should be included for a mastoidectomy are outlined in Table 30.3. Micro ear instruments and an air-powered drill with a variety of burrs must be available. Th e burrs are of two types. Th ese are designated as cutting burrs and diamond burrs. Cottonoids and cotton balls moistened with Tis-U-Sol are oft en used. Th ey must always be counted. At times, solutions of diluted epinephrine are used to assist in hemostasis. Prosthetic devices for reconstruction of the ossicular chain must be readily available in a wide variety of types and sizes. Because the facial nerve is at risk during a mastoidectomy, nerve stimulators may be used to identify the facial nerve. Evoked potential audiom-etry can also be used to monitor the facial nerve.
Figure 30.11
Simple mastoidectomy.

Chapter 30: Otorhinolaryngological Surgery 1097
30
PHYSIOLOGICAL MONITORING
During mastoidectomy, the patient is placed under general anesthesia (see the discussion of tympanoplasty).
SPECIMENS AND CULTURES
Mastoid bone fragments, granulation tissue, and/or cholesteatoma may be sent to the pathology department for study or microbiology for culture if indicated.
DRUGS AND SOLUTIONS
Drugs and solutions that should be available include the following:
• Lidocaine 1% with 1:100,000 epinephrine • Gelfoam 100 • 1:1000 epinephrine • Cortisporin ointment • Cortisporin Otic suspension • Tis-U-Sol Solution
PHYSICIAN ORDERS
Th e patient is given IV fl uids and antibiotics. A regular diet is ordered. Antiemetic and analgesic drugs are administered. Th e patient is advised not to use straws with liquids and to sneeze with the mouth open.
LABORATORY AND DIAGNOSTIC STUDIES
See the discussion of tympanoplasty.
Table30.3
Mastoidectomy Instruments
Elevators
Incudostapedial joint knife
Myringotomy knife
Picks: 90° and 40° (curved, straight, and right angle)
Knives: Guilford, tympanoplastic sickle-shaped
Knives: Rosen, House
Strut caliper
Tabb knives: 45° and 90°
Retractors: Weitlaner, Wullstein
Rongeurs
Suction irrigation system
Rosen suction tube, sizes 18 to 24
House adapter
Absorbable gelatin sponge (Gelfoam) press
Shea ear specula

1098 Section 3: Operative and Invasive Procedures
Procedure
INCISION AND EXPOSURE
Mastoidectomy can involve only a postauricular incision. Most oft en, however, the procedure is combined with a tympanoplasty. Th is is better known as a tym-panomastoidectomy. Th e procedure is started by palpating the tip of the mastoid process. Aft er external landmarks have been identifi ed, a postauricular incision is made close to the postauricular sulcus. Th is incision is made with a surgical blade or electrosurgery. Th e microscope is usually not used for this portion of the procedure.
A dissection is carried down to the temporalis fascia superiorly and down through the periosteum just below the temporalis muscle insertion. At this time, a portion of temporalis muscle fascia is obtained if a graft will be placed later during the proce-dure. If the procedure is going to be combined with a tympanoplasty, external audi-tory canal incisions are made as described earlier.
Aft er the tympanomeatal fl ap is elevated, the operation proceeds through the postauricular incision and, if necessary, through the ear canal. Th e postauricular incision, however, exposes the ear canal also. Aft er the periosteum is exposed, it is elevated anteriorly with an elevator, such as a 4-mm periosteal elevator. Aft er the external auditory canal incision is visualized through the postauricular incision, dif-ferent canal instruments can be used to expose the middle ear fully through the canal. A self-retaining retractor is placed and opened widely. At this point, the air-powered drill is used with the largest available cutting burr.
DETAILS
Aft er the dissection has proceeded beyond the superfi cial bony landmarks, a microscope is brought in for fi ner detail. Depending on the indications for the operation, the middle ear can be entered from the mastoid approach as well. It is important that the surgeon be as comfortably seated as possible. It is also important that the scrub person have a thorough knowledge of the anatomy and procedure to anticipate the use of the appropriate instruments. Ideally, the surgeon should never have to look away from the microscope for instruments. A surgeon should be able to request an instrument by name and have it handed to him or her by the scrub person.
If reconstructive procedures are indicated, the surgeon selects from a wide variety of prosthetic devices. If a tympanic membrane perforation is to be repaired, the pre-viously harvested graft is used in a manner similar to that described earlier.
CLOSURE
Th e postauricular wound is copiously irrigated, and the wound is closed by approximating the previously raised periosteum. Periosteum is usually closed with absorbable sutures of the surgeon’s choice. Th e subcutaneous tissues are then reapproximated in the postauricular area. A drain may be placed and brought out through the most inferior portion of the postauricular incision. Th e skin is usually closed with a nylon or polypropylene (Prolene) stitch. A subcuticular suture may be used to alleviate the necessity for suture removal later.

Chapter 30: Otorhinolaryngological Surgery 1099
30
Again, the preference of the surgeon should be determined before the procedure is started. Aft er the postauricular incision is closed, the ear canal is examined in the usual fashion. A variety of ear specula is used to visualize the canal. Th e tympanomeatal fl ap is replaced, and the external auditory canal is packed as previously described. Aft er the procedure, a mastoid dressing is used. A nonadhering bandage is placed behind the ear. Th e postauricular incision is then supported with gauze squares. Rolls of self-adhering gauze are used to surround the head from the occiput to the fore-head. Gauze may be used to place pressure on the wound to prevent a hematoma.
Postprocedure Care
Th e patient is transferred immediately to the PACU. Aft er operations of the mas-toid and the middle ear, it is important to assess the hearing capability of the patient as well as assess for vertigo. As soon as the patient is conscious, diff erent tuning fork tests may be used to assess hearing. Th e facial nerve function is also routinely evaluated (eg, smiling, wrinkling of the nose on the operative side, and closing of the eye).
Potential Complications
Complications that may occur include hearing loss, facial nerve injury, vertigo, taste changes, bleeding and hematoma formation, and infection.
StapedectomyDefi nition and Indications
Stapedectomy is a surgical procedure in which the stapes is removed and replaced with a prosthesis; it is performed to improve the movement of sound to the inner ear (Encyclopedia of Surgery, 2008c). In some patients, a conductive hearing loss is identifi ed. A common reason for this hearing loss is the formation of spongy bone within the capsule of the bony labyrinth of the inner ear. In such conditions, nor-mal bone is replaced by vascular otosclerotic bone, which eventually involves the footplate of the stapes. Th e stapes thus becomes locked and unable to vibrate. Th is condition, commonly known as otosclerosis, is a hereditary defect. Th e procedure of stapedectomy with the insertion of a prosthesis has been developed to restore hearing to the ear.
Th e indications for stapedectomy include treatment of progressive hearing loss caused by otosclerosis, a condition in which spongy bone hardens around the base of the stapes (Encyclopedia of Surgery, 2008c) and also the fi nding of a conductive hearing loss without any evidence of other middle ear disease.
Related Procedures
Stapedotomy is a related procedure.
Nursing Implications
ANESTHESIA
As for other ear procedures, stapedectomy is usually performed using general anesthesia. In cooperative adults, however, local anesthesia may be used so that the patient can assist the surgeon by informing him or her of an immediate improve-ment in hearing.

1100 Section 3: Operative and Invasive Procedures
POSITION
Th e patient is positioned as described for tympanoplasty.
ESTABLISHING AND MAINTAINING THE STERILE FIELD
Th e sterile fi eld is established and maintained as for other ear procedures. Th e position of the sterile fi eld is identical to that for other ear procedures.
EQUIPMENT AND SUPPLIES
All microinstruments for ear procedures should be available, to include fi ne stapes dissectors and manipulators. A variety of prosthetic devices has been described for use in this procedure. A tympanoplasty set is used with the additional instruments outlined in Table 30.4.
PHYSIOLOGICAL MONITORING
See the discussion of tympanoplasty.
SPECIMENS AND CULTURES
Th e stapes superstructure is sent for pathological study.
DRUGS AND SOLUTIONS
See the discussion of mastoidectomy.
PHYSICIAN ORDERS
See the discussion of tympanoplasty.
LABORATORY AND DIAGNOSTIC STUDIES
See the discussion of tympanoplasty.
Procedure
INCISION AND EXPOSURE
A tympanomeatal fl ap is raised as previously described for simple tympanoplasty. Th e fi brous annulus of the tympanic membrane is identifi ed and lift ed superiorly
Table30.4
Stapedectomy Instruments
Hough hoe excavators: 45° and 90°
Footplate picks: 1 mm and 2 mm
Straight pick or 30° obtuse pick
Perforator
Crimper: House and/or McGee
Strut caliper (measuring stick)
Prostheses of different sizes and shapes
House incudostapedial joint knife
Guilford-Wright joint knife

Chapter 30: Otorhinolaryngological Surgery 1101
30
with a tympanomeatal fl ap (Fig. 30.12). Oft en, a small portion of bone from the edge of the bony ear canal is removed for better visualization of the joint between the incus and the stapes. Th e chorda tympani nerve is located in this area. Care is taken not to injure this nerve, which supplies taste to the lateral portion of the tongue on that side. Microinstruments are used to sever the connection between the incus and the stapes. Th e stapes bone is fractured and removed along with the remnant foot-plate. Some surgeons use lasers as well.
A graft is also necessary during this procedure. Th is graft may be vein, perichon-drium, fascia, fat, or absorbable hemostatic sponges. Th e graft is placed over the oval window of the inner ear.
DETAILS
Aft er the prosthesis has been selected, the previously obtained graft is placed over the oval window where the stapes footplate previously existed. A prosthesis is then inserted and connected from the incus to the graft . Th is restores sound conduction. If the procedure is being performed under local anesthesia, the surgeon can reposition the tympanic membrane and talk to the patient while testing for a hearing improve-ment. As in other microsurgical procedures, the operating microscope must be used.
Figure 30.12
Stapedectomy procedure.

1102 Section 3: Operative and Invasive Procedures
CLOSURE
Th e tympanomeatal fl ap is replaced as previously described.
Postprocedure Care
Postprocedure care is the same as that for other ear procedures.
Potential Complications
Hearing loss, dizziness (vertigo), a change in taste, and injury to the facial nerve may occur.
Cochlear ImplantDefi nition and Indications
A cochlear implant is a small, intricate electronic device that can assist in provid-ing a sense of sound to a person who is profoundly deaf or severely hard-of-hearing; it does not restore normal hearing, rather it can give a deaf person a useful repre-sentation of sounds in the environment, which helps him/her to understand speech (NIDCD, 2007). It works by directly stimulating any functioning auditory nerves inside the cochlea with an electric fi eld stimulated through an electric impulse ( Wikipedia, 2008a). Th e implant consists of two portions: an external portion that sits behind the ear and a second portion that is surgically implanted under the skin as follows (NIDCD, 2007):
• A microphone, which picks up sound from the environment; • A speech processor, which selects and arranges sounds picked up by the
microphone; • A transmitter and receiver/stimulator, which receive signals from the speech
processor and convert them into electric impulses; and • An electrode array, which is a group of electrodes that collects the impulses
from the stimulator and sends them to diff erent regions of the auditory nerve.
Cochlear implants are indicated for children (most who receive them are between 2 and 6 years old) and adults who are deaf or severely hard-of-hearing, as well as adults who have lost all or most of their hearing later in life (NIDCD, 2007).
Nursing Implications
ANESTHESIA
Th e procedure is performed under general anesthesia.
POSITION
See the discussion under mastoidectomy.
ESTABLISHING AND MAINTAINING THE STERILE FIELD
See the discussion under mastoidectomy.
EQUIPMENT AND SUPPLIES
All instruments for ear procedures should be available, including a microscope and bone drill.

Chapter 30: Otorhinolaryngological Surgery 1103
30
PHYSIOLOGICAL MONITORING
See the discussion under tympanoplasty.
SPECIMENS AND CULTURES
Bone fragments and other tissue may be sent to the pathology department for study or microbiology for culture if indicated.
DRUGS AND SOLUTIONS
See the discussion under mastoidectomy.
PHYSICIAN ORDERS
See the discussion under mastoidectomy.
LABORATORY AND DIAGNOSTIC STUDIES
In addition to the routine preoperative testing protocols, other preoperative studies include (US FDA, 2004):
• examination of external, middle, and inner ear for signs of infection or abnormality;
• various tests of hearing, such as an audiogram; • a trial of hearing aid use to assess its potential benefi t; • exams to evaluate middle and inner ear structures, for example: • CT (computerized tomography) scan—to assess the shape of the cochlea. It
is particularly important if the patient has a history of meningitis because it helps to ascertain if there is new bone growth in the cochlea that could interfere with the insertion of the implant; it also may indicate which ear should be implanted;
• MRI (magnetic resonance imaging) scan; • psychological examination to see if the patient can cope with the implant; and • physical exam to prepare for general anesthesia.
A detailed evaluation by the cochlear implant team must also be conducted for those who are considered as candidates for the cochlear implant; in addition, both the preprocedure and postprocedure training are important to the overall success of the device (Levenson, 2008).
Procedure
A small incision is made in the skin just behind the ear; the surgeon drills into the mastoid bone to create a seat to hold and protect the receiver/stimulator. Th e sur-geon then drills through the mastoid bone to the inner ear where the electrode array is inserted into the cochlea. Th e receiver/stimulator is secured to the skull, the inci-sion is closed with absorbable sutures, and the head is bandaged (Wikipedia, 2008a; University of Miami School of Medicine, 2008).
Postprocedure Care
Th e patient may be discharged the day of surgery, or may be required to stay in the hospital for 1 to 2 days, depending on the length of the surgery. Th e patient may experience minimal side eff ects such as temporary swelling. Other side minor eff ects
MRIMagnetic Resonance
Imaging

1104 Section 3: Operative and Invasive Procedures
include pain, changes in taste, dizziness, infl ammation, and bleeding; if these do occur, they are generally temporary (Berke, 2007). Patients return to school or work within a week of surgery; activation of the implant occurs two to four weeks aft er implantation, allowing enough time for the incision to heal properly (University of Miami School of Medicine, 2008).
Potential Complications
Th e potential complications associated with this procedure include (Wikipedia, 2008a):
• skin infection; • onset of tinnitus; • damage to the vestibular system; • damage to facial nerves that can cause muscle weakness, or, in severe cases,
disfi guring paralysis; • device failure, usually in cases where the incision does not heal properly; and • destruction of any residual hearing the patient may have.
PROCEDURES OF THE NOSE AND PARANASAL SINUSESOperations inside the nose and sinuses are primarily performed to correct obstruction or alleviate infection. Other operations have been designed to control intractable nosebleeds. Tumors within the nasal cavity and sinuses are rare. When tumors are discovered, however, extensive resection of these structures is oft en necessary.
Special Instruments, Supplies, and EquipmentA dedicated nasal set should always be available for procedures within the nasal
cavity. Th is set usually includes a variety of elevators, dissectors, curved scissors, and curettes, plus nasal specula of diff erent lengths. Dedicated sinus endoscopy sets should be readily available in operative and invasive procedure suites that provide otolaryngological services. Th e scrub person should be thoroughly familiar with the names of the various forceps that are oft en used in endoscopic sinus surgery. Th e use of diff erent lasers within the nasal cavity has been undertaken.
Septoplasty (Septorhinoplasty)Defi nition and Indications
Septoplasty refers to the excision of the cartilaginous or bony portions of the nasal septum that lie between the fl aps of the mucous membrane and the perichondrium (Fig. 30.13). Th e goal of this procedure is to correct defects or deformities of the septum (Encyclopedia of Surgery, 2008d). Th e primary indications for septoplasty or septorhinoplasty are relief of obstruction resulting from nasal deformity. Th e deformity might be only within the internal nasal cavity, but it is frequently seen in conjunction with the deviation of the external nose as well. Deviation of the sep-tum oft en leads to other problems besides obstruction of the nasal airfl ow. Severe deviations are aggravating factors in recurrent sinusitis. When there are defects of the bony framework, the bones of the nose must be reshaped. Th erefore, the prepro-cedure evaluation of the entire external and internal nose is essential.

Chapter 30: Otorhinolaryngological Surgery 1105
30
Related Procedures
Submucous resection is a related procedure.
Nursing Implications
ANESTHESIA
Septoplasty and septorhinoplasty are oft en performed under local anesthesia with moderate sedation. When this is done, cocaine solutions can be applied intrana-sally on cottonoids to provide vasoconstriction and anesthesia. Other agents oft en used include lidocaine in addition to oxymetazoline (Afrin). Th ese drugs can cause adverse reactions in the patient. Th e initial symptoms consist of central nervous sys-tem stimulation, which is eventually followed by cardiovascular depression. Usually mild symptoms, such as mild excitation, can be seen if the patient is awake. If the patient is under general anesthesia, an increase in heart rate is frequently the only fi nding. If general anesthesia is going to be used for the procedure, oft en a throat pack is placed in the back of the throat aft er the patient is intubated to decrease the chance of aspiration of blood.
POSITION
Th e patient is placed in the supine position. A headrest should be available to sta-bilize the head. Th e same comfort measures are used as for tympanoplasty patients.
ESTABLISHING AND MAINTAINING THE STERILE FIELD
Even though the nasal membranes are contaminated, the mucus within the sinuses should be considered sterile; therefore, a sterile fi eld is created.
EQUIPMENT AND SUPPLIES
Because illumination is provided by the endoscope, or a headlight, it must be in working order. On rare occasions, a microscope may be used. If endoscopes are used, appropriate light connectors for each type of endoscope must be available. Th e entire lighting mechanism must be thoroughly checked before initiation of the procedure.
Figure 30.13
Anatomy of the nose.

1106 Section 3: Operative and Invasive Procedures
Th e nurse should verify with the surgeon his or her preference for nasal packing and/or splinting supplies and have these available for use at the end of the procedure.
PHYSIOLOGICAL MONITORING
Th e patient must be monitored at all times by vital signs measurement, ECG, and pulse oximeter. Th e circulating nurse must always record the amount of local anes-thesia that is administered. All sponges and cottonoids must be counted. Because the cottonoids that are commonly used are small, they can present a hazard if mis-counted, or not tagged. Th roughout the procedure, cottonoids soaked in a vasocon-stricting agent such as oxymetazoline are used. Suction must be available at all times, along with varying sizes of suction catheters.
SPECIMENS AND CULTURES
Nasal cartilage and bone and the turbinates are studied.
DRUGS AND SOLUTIONS
Drugs and solutions that should be available for this procedure include the following:
• Lidocaine 1% with 1:1000 epinephrine • Cocaine solution or crystals • Antibiotic ointment or cream • Gelfoam • Neosporin 1% • 1:1000 epinephrine
PHYSICIAN ORDERS
Th e IV catheter is kept open until the patient is tolerating liquids. Analgesics are administered for pain and antiemetics for nausea. Th e patient is advised not to drink with straws and to sneeze with the mouth open.
LABORATORY AND DIAGNOSTIC STUDIES
Routine CBC, urinalysis, prothrombin time (PT), and partial thromboplastin time (PTT) are ordered. Before procedures within the nose or the sinuses are started, radiographs or CT scans are oft en obtained to evaluate the problem fully. It is essen-tial that these radiographs or scans are present in the operative suite.
Procedure
INCISION AND EXPOSURE
Unless endoscopes are used along with a camera and monitor, procedures inside the nose can be diffi cult to follow by the scrub person. Th e initial portion of the pro-cedure involves the placement of local anesthetic-soaked sponges or cottonoids, as well as the injection of a local anesthetic and epinephrine solution. Aft er this is done, an appropriate time for vasoconstriction is allowed and the nose is examined with a nasal speculum. Th e initial incision is made inside the nose along the tip of the nasal septum. Th e initial steps involve the separation of the soft tissues, which include
PTProthrombin Time
PTTPartial Thromboplastin
Time

Chapter 30: Otorhinolaryngological Surgery 1107
30
the mucous membrane and underlying perichondrium, from the cartilaginous and bony septum. In a previously traumatized nose, this may be a diffi cult aspect of the operation. Diff erent elevators, such as the Cottle elevator, are used to lift the per-ichondrium off the septum.
DETAILS
Aft er the deformed portion of the septum is identifi ed, it may be removed, straight-ened, or misplaced. A variety of instruments oft en found in nasal sets is used for this purpose. If the external nasal framework is also to be reshaped (rhinoplasty), this is accomplished using a variety of osteotomes as well as mallets.
CLOSURE
Aft er the nose is shaped in the desired way, and the internal septal deviation is corrected, it is imperative that attempts be made to stabilize the internal and exter-nal nasal framework. Th is can be done in a variety of ways. Tight nasal packing has been used in the past. More commonly, however, internal nasal splints such as Doyle splints may be used to stabilize the septum. Tefl on sheeting has also been used for this purpose. Th e internal splints are stabilized with nonabsorbable sutures. Before placement of the splints, the previously made mucosal incisions are closed using small absorbable sutures. Diff erent ways of stabilizing the external nasal framework have been proposed. Plaster is still used and is eff ective. Commercially available rigid shields can protect the external nose also. At the completion of the procedure, the throat pack must be removed.
Postprocedure Care
Aft er the procedure, the patient is transferred to the PACU. Th e head of the bed should be elevated to lessen edema. Analgesics are oft en prescribed to reduce the discomfort. At times, sedation is necessary in the postprocedure period. A nasal drip pad is oft en in place under the nose. Because there might be packing inside the nose, the patient is breathing primarily through the mouth. Th is necessitates good oral care. If the nose is packed bilaterally, humidifi ed oxygen is oft en given by means of face mask. However, intake of oral fl uids must not be started until the eff ects of the local anesthetic are gone. If oral fl uids are started too early, aspiration could occur. Most septoplasties and septorhinoplasties are performed on an outpatient basis. Th erefore, discharge instructions should be discussed at length with the patient.
Potential Complications
Bleeding may occur. Toxic shock has also been reported.
Functional Endoscopic Sinus SurgeryDefi nition and Indications
Functional endoscopic sinus surgery (FESS) refers to procedures performed on the sinus cavities with endoscopic guided resection to open sinus air cells and sinus ostia in order to restore normal drainage of the sinuses (Encyclopedia of Surgery, 2008e). With the advent of sinus endoscopes, the extent of visualization inside the nose as well as knowledge of its anatomy and physiology has dramatically improved.
FESSFunctional Endoscopic
Sinus Surgery

1108 Section 3: Operative and Invasive Procedures
Endoscopes allow precise operations within the nasal cavity. Indications for endoscopic sinus procedures include the removal of diseased mucosa and resection of the necessary bony portions of the nasal cavity to establish natural drainage of the paranasal sinuses.
Patients have endoscopic sinus surgery only aft er an extensive medical and allergic evaluation. When medical treatment has failed and the patients persist with sinusitis, the surgeon oft en recommends operative intervention. A septoplasty may or may not be performed at the time of the endoscopic procedure. Occasionally, septoplasty becomes necessary to gain access to the nasal cavity with the endoscopes. Th e extent of the procedure depends on the location of the diseased mucosa and the extent of bony abnormalities within the nasal cavity and sinuses.
Related Procedures
Caldwell-Luc procedure and external ethmoidectomy are related procedures.
Nursing Implications
ANESTHESIA
Endoscopic sinus procedures can be performed using local anesthesia. However, general anesthesia is preferred because of the inability to anesthetize posterior por-tions of the nose. Th e principles previously discussed for septoplasty and septorhi-noplasty must be followed.
POSITION
See the discussion of septoplasty.
ESTABLISHING AND MAINTAINING THE STERILE FIELD
See the discussion of septoplasty.
EQUIPMENT AND SUPPLIES
Of greatest importance is the availability and thorough knowledge of the appropriate equipment. Complications of the operation have occurred in the past because of lack of appropriate instrumentation. Commercially available endoscopic sinus surgery sets contain a wide variety of telescopes. Th e endoscopes are usually either 2.7 or 4 mm. in diameter. Th ese have 0-, 25-, 30-, 70-, and 120-degree viewing angles (Fig. 30.14). Endoscopes require an external light source; therefore, precaution should be taken in case of burnout of the bulb. Also needed is a camera with a color monitor and a video recorder. A designated endoscopy cart housing all video equipment is essential.
Lasers have been advocated for use intranasally. Th is, however, is somewhat con-troversial. If the laser is used, all appropriate precautions as established by the laser safety standards of the facility must be followed.
PHYSIOLOGICAL MONITORING
See the discussion of septoplasty.
SPECIMENS AND CULTURES
Specimens of nasal cartilage and bone and of the contents of diff erent sinuses (eg, ethmoid and maxillary) may be sent for study.

Chapter 30: Otorhinolaryngological Surgery 1109
30
DRUGS AND SOLUTIONS
See the discussion of septoplasty.
PHYSICIAN ORDERS
See the discussion of septoplasty.
LABORATORY AND DIAGNOSTIC STUDIES
Routine laboratory studies as described for septoplasty are performed. Of utmost importance is the availability of previously obtained CT scans. Because the CT scan provides the “road map” for the surgeon, the patient should not come into the pro-cedure room unless the CT scan is readily available.
Procedure
INCISION AND EXPOSURE
Th e procedure is usually initiated as for a septoplasty. Local anesthetic or vasocon-stricting solutions are used. Th ese are placed intranasally on soaked cottonoids. Th ey are placed in the area of the operation (ie, the middle meatus) (Fig. 30.15). Th e area to be operated on is injected with local anesthetic and epinephrine solutions. If a septo-plasty is going to be combined with the operation, this is performed fi rst. Aft er the cot-tonoids have been left in place to allow for vasoconstriction, the operation is initiated.
Diff erent sharp instruments, such as sickle-shaped knives and scissors, are used for the initial incisions within the middle meatus. A wide variety of straight and angled-biting forceps (usually available in the endoscopic sinus surgery sets) is used for removal of the diseased bony abnormality as well as mucosa. A wide variety of curved suction catheters is also used. Th e telescope is inserted intranasally and advanced into the ethmoid sinus, and if necessary the sphenoid sinus. Th e sinus endoscopes are used to visualize anteriorly within the nasal cavity and also into the frontal sinus.
DETAILS
Because the operation proceeds in close proximity to the eye and the brain, care is taken to identify the walls of the orbit and the base of the skull. It is important not to
Figure 30.14
Endoscopic instruments.

1110 Section 3: Operative and Invasive Procedures
have the eyes taped shut. If the orbit is accidentally entered, what might be perceived as nasal mucosa could be orbital contents. When pulling on these contents, move-ment of the eyeball is seen. Th is can be occluded if the eyes are taped shut.
Aft er the diseased mucosa and bony abnormalities have been removed from within the nasal cavity, evaluation of the operative fi eld reveals a common cavity between the anterior and posterior ethmoidal cells. However, if diseased mucosa is not encountered in the posterior portion of the ethmoidal cavity, it is not disturbed. Backward cutting antral punches are used to widen the maxillary sinus ostia.
CLOSURE
As the procedure is concluded, hemostasis is obtained with either bipolar electro-surgery or monopolar suction electrosurgery. Because the operation is performed between the lateral nasal wall and the middle turbinate, stents are used that are later removed, to prevent the formation of scarring. Diff erent materials have been used; commercially available Merocel sponges have been designed for this purpose. Most commonly, however, rolled absorbable gelatin fi lm (Gelfi lm) dressing is used as a stent within the operated cavity. Th is is removed at a later date. Usually, no drains or packing is necessary. If extensive bleeding is encountered, however, an anterior nasal pack might be left in place temporarily.
Postprocedure Care
Th e same nasal dressing as described for septoplasty is applied. Principles previ-ously described are applicable in this situation as well. Of utmost importance, how-ever, is the assessment of vision. Reports of complications stemming from swelling around the eye to blindness have been reported. It is critical that this be evaluated as early as possible. If diffi culty with vision is encountered, the surgeon must be noti-fi ed immediately. Further procedures might become necessary to prevent blindness. If the base of the skull has accidentally been entered, this might not be immediately known. However, profuse clear drainage from the nose may indicate cerebrospinal fl uid leak. Again, the surgeon must be notifi ed immediately.
Figure 30.15
Location of turbinates
and meati for
endoscopic sinus
surgery.

Chapter 30: Otorhinolaryngological Surgery 1111
30
Potential Complications
Complications may include blindness, perforation of the base of skull with subsequent central nervous system infection, injury to the lacrimal duct, and bleeding.
Caldwell-Luc ProcedureDefi nition and Indications
Th e Caldwell-Luc procedure is an intraoral procedure for entering the maxillary antrum through the canine fossa above the maxillary premolar teeth. Aft er the max-illary antrum is opened, the sinus mucosa is stripped from the sinus wall; in addi-tion, an intranasal antrostomy is made (Medcyclopaedia, 2008).
Th e Caldwell-Luc operation has been a standard procedure for the sinus surgeon. Additional thought and improved knowledge of the physiology of the sinuses have decreased the use of this operation. However, there are still times when tremendous amount of diseased mucosa and polyps exist within the maxillary sinus. Th is opera-tion is designed to gain access to the maxillary sinus through an incision underneath the upper lip in the area of the anterior wall of the maxillary sinus. Sinus endoscopes have oft en been used to visualize maxillary sinus contents also. A trocar can be used to penetrate the anterior wall of the maxillary sinus. Aft er the trocar has entered the sinus, the scope can be placed through a sheath into the sinus. Th is helps in assessing the extent of the maxillary sinus operation.
Related Procedures
Creation of nasal antral windows (antrostomy) is a related procedure.
Nursing Implications
ANESTHESIA
Th e Caldwell-Luc operation is oft en performed in conjunction with other intra-nasal procedures. Th erefore, previously discussed anesthesia regimens should be followed.
POSITION
See the discussion of septoplasty.
ESTABLISHING AND MAINTAINING THE STERILE FIELD
Th e patient is prepared and draped as previously described for nasal procedures.
EQUIPMENT AND SUPPLIES
A general nose set is used. Also used is a Caldwell-Luc set, which includes an antral punch and Coakley antrum curettes.
PHYSIOLOGICAL MONITORING
See the discussion of septoplasty.
SPECIMENS AND CULTURES
Polyps and diseased nasal mucosa may be sent to the pathology department.

1112 Section 3: Operative and Invasive Procedures
DRUGS AND SOLUTIONS
See the discussion of septoplasty.
PHYSICIAN ORDERS
See the discussion of septoplasty.
LABORATORY AND DIAGNOSTIC STUDIES
Routine CBC, urinalysis, PT, PTT, CT scan, and/or sinus radiographs are obtained.
Procedure
INCISION AND EXPOSURE
Th e maxillary sinus to be operated on is approached through an incision in the oral mucous membrane above the canine teeth. Th is mucosal fl ap is retracted until periosteum is incised (Fig. 30.16). A section of maxillary bone is cut out to gain access into the maxillary sinus.
DETAILS
Th rough this opening, polyps or diseased mucosa are removed. Th rough the nasal cavity, a fl ap and opening is created into the maxillary sinus through the infe-rior meatus. Aft er this connection has been created, the sinus is packed with gauze impregnated with antibiotic ointment. One end of the gauze is brought out through the opening made in the nasal cavity. Th is packing is eventually removed through
Figure 30.16
Caldwell-Luc procedure.

Chapter 30: Otorhinolaryngological Surgery 1113
30
the nose. Aft er the gauze is in place, care must be taken not to lose the end of the gauze that is brought out through the nasal cavity.
CLOSURE
Th e periosteum is reapproximated, and the mucosal incision is closed with absorbable suture.
Postprocedure Care
Postprocedure care is similar to that for other intranasal procedures previously described.
Potential Complications
Complications may include injury to the roots of the teeth in children, injury to the infraorbital nerve leading to anesthesia of the cheek, injury to the orbital con-tents, injury to the tooth sockets, and edema.
Closed Repair of Nasal FractureDefi nition
Closed repair of nasal fracture refers to the manipulation of a nasal fracture without incision. Th is procedure is oft en performed aft er trauma to the face. Intranasal manip-ulation can be used immediately aft er the injury. Occasionally, elevation of depressed bone or cartilage can be performed and the nose reshaped to its normal position.
Indications
Th e indications for closed reduction include unilateral or bilateral fracture of the nasal bones and fracture of the nasal septal complex that is deviated less than one half of the width of the nasal bridge; however, reduction of a nasal fracture is indi-cated in any patient with a signifi cant cosmetic deformity or functional compromise (Dev, 2006). Th e best time for reduction may be within the fi rst 3 hours aft er injury, otherwise, most believe that waiting 3–7 days is preferable in order to allow edema to resolve, and also facilitate positioning the bones correctly with more stability because infl ammation and fi brosis may make the fragments less mobile. If reduction is not possible within the fi rst 7–10 days, then the fractured segments begin forming a fi brous union (Dev, 2006).
Nursing Implications
ANESTHESIA
Most procedures to reduce the nasal cavity are most comfortably performed with the use of general anesthesia. Th is is especially true in children. However, local anes-thesia can be used and previously described principles followed.
ESTABLISHING AND MAINTAINING THE STERILE FIELD
See the discussion of septoplasty.
EQUIPMENT AND SUPPLIES
A general nose set or designated closed nasal fracture set and a headlight are needed.

1114 Section 3: Operative and Invasive Procedures
PHYSIOLOGICAL MONITORING
See the discussion of septoplasty.
SPECIMENS AND CULTURES
Typically there is no specimen.
DRUGS AND SOLUTIONS
See the discussion of septoplasty.
PHYSICIAN ORDERS
See the discussion of septoplasty.
LABORATORY AND DIAGNOSTIC STUDIES
CBC and urinalysis are performed.
Procedure
Intranasal manipulation is performed with a variety of blunt instruments. A Boies elevator is oft en used intranasally to elevate nasal bony depression. Diff erent types of forceps are also available for this purpose. It is important to know that clinical eval-uation of the nose is far more important than radiographic evaluation. Th erefore, radiographs are not necessarily obtained. Even if the operation is performed under general anesthesia, topical anesthesia and vasoconstrictors are placed on soaked cot-tonoids intranasally. Previously described substances such as cocaine or oxymetazo-line can be used.
Aft er the desired reduction is obtained, it is important to stabilize the nose exter-nally. Th e same principles should be used as for stabilization of the patient who has had a rhinoplasty.
Postprocedure Care
See the discussion of septoplasty.
Potential Complications
Th e complications of closed reduction are few. Some fractures cannot be satis-factorily reduced and that would necessitate a formal rhinoplasty at a later date. Unmanageable bleeding is rarely encountered. Nasal packing might be used tempo-rarily to control a nosebleed aft er the manipulation. Additional complications have been reported if nasal packing is used, some of which are infectious, such as toxic shock syndrome.
PROCEDURES OF THE OROPHARYNX AND HEADAND NECKTonsillectomy and AdenoidectomyDefi nition
Tonsillectomy and adenoidectomy refer to the excision of the pharyngeal tonsils and adenoids. No operation has attracted as much attention and heated controversy.

Chapter 30: Otorhinolaryngological Surgery 1115
30
Th e tonsillectomy and adenoidectomy procedure is the most common major surgery performed in children (Kavanaugh, 2008).
Indications
Th e indications for tonsillectomy and adenoidectomy have varied through the years. Th e three most common indications, however, are chronic infections, obstruction of breathing (Fig. 30.17), and excisional biopsy in the evaluation of tonsillar tumors. Tonsillectomy and adenoidectomy are not always performed at the same time. Diff erent indications exist for removal of the adenoid pad only. For example, the adenoid tissue aff ects the middle ear. Studies revealing the eff ects of adenoidectomy on chronic otitis media are well known. Th erefore, the decision to perform an adenoidectomy does not always include a tonsillectomy. Sometimes, a tonsillectomy alone is performed. Most adenoidal tissue involutes with age. Th e decision to remove it depends on the symptoms associated with an enlarged adenoid pad.
Nursing Implications
ANESTHESIA
Most tonsillectomies and adenoidectomies are performed using general anesthe-sia. Local anesthesia has been used successfully in adults. Th e discussion presented here, however, primarily refers to the patient under general anesthesia.
POSITION
Th e patient is usually in a supine position and is placed on the bed with his or her head at the foot. Th is facilitates the surgeon’s comfortable access to the patient. If the patient has the procedure under local anesthesia, the semi-Fowler position may be preferable.
ESTABLISHING AND MAINTAINING THE STERILE FIELD
Tonsillectomy and adenoidectomy is not considered a sterile procedure. Hospital policy specifi es whether the patient is or is not draped. Th e surgeon and scrub per-son, however, should don sterile gowns and gloves and wear appropriate head cover-ing, eye protection, and a mask according to standard precautions guidelines. Th e surgeon may sit at the patient's head or stand at the side of the bed.
Figure 30.17
Tonsils obstructing the
oropharynx.

1116 Section 3: Operative and Invasive Procedures
Lighting into the oral cavity is usually obtained with a headlight. Overhead lights, however, have been used. Lighting is superior, nevertheless, with a headlight. Aft er the patient has been intubated, the table may be turned to suit the surgeon, Th e patient’s head is draped to cover the eyes, which have been taped by the anesthesia provider.
If the surgeon sits at the head of the bed, a mouth gag is inserted to depress the tongue and expose the oropharynx. Most oft en, a Davis-Crowe or palate-type mouth gag is used for this purpose. Th ese gags are designed to open the oral cavity while simul-taneously depressing the tongue. Aft er this is obtained, the gag is secured to a suspen-sion apparatus. Diff erent suspension apparatus designs are available. Most commonly, however, suspension is obtained by placing the tongue blade on a Mayo stand. Th is is probably the most common way of suspending the mouth gag; however, independent suspension apparatuses are superior. Independent suspension apparatuses provide free movement of the table without having the worry of the Mayo stand height or location.
Because a tonsillectomy and adenoidectomy can be a bloody procedure, appro-priate suctioning with Yankauer tips is required. Th e incision and dissection have been described in a number of ways. A cold knife, electrosurgery, and laser have been used to perform the operation. Th ere have been diff erent advocates for the various techniques. No single technique is considered superior. Th ere should be an eff ort, however, to decrease bleeding during the procedure. Aft er the oropharynx is exposed, the decision is made to begin either the adenoidectomy fi rst or the tonsil-lectomy. Sometimes removal of the adenoid tissue fi rst allows more time for packing of the nasopharynx and easier hemostasis.
EQUIPMENT AND SUPPLIES
A tonsil and adenoid set is needed, as well as the surgeon-preferred mouth gag. Th ese may range from the Jennings, to Davis-Crowe, to a palate-type mouth gag. Th e nurse may anticipate the use of a Davis-Crowe or McGivor mouth gag if the surgeon sits or stands at the patient’s head during the procedure. Th e Jennings mouth gag, however, is more routinely used if the surgeon stands at the patient’s side during the procedure.
Th e suction coagulator is necessary, and the possible use of a handswitch electro-surgery pencil should be anticipated. Th e foot pedal of the electrosurgery genera-tor is necessary for the use of the suction coagulator. As for the use of all electrical equipment, the nurse should ensure that these pieces of equipment are operating correctly before the beginning of the procedure. If the laser is used, all laser precau-tions should be in place before the procedure.
PHYSIOLOGICAL MONITORING
Th e patient is monitored at all times as for previously described procedures.
SPECIMENS AND CULTURES
Th e right and left tonsils and adenoid tissue are sent for study.
DRUGS AND SOLUTIONS
Drugs and solutions needed for this procedure include the following:
• Normal saline • Lidocaine 1% with 1:100,000 epinephrine

Chapter 30: Otorhinolaryngological Surgery 1117
30
• Phenylephrine (Neo-Synephrine) • Tannic acid • Bismuth subgallate • 1:1000 epinephrine • Defogging solution (Antifog, pHisoHex)
PHYSICIAN ORDERS
Th e IV catheter is maintained at a keep-open rate until the patient is taking fl u-ids without nausea and vomiting. Th e patient is given a soft diet. Th e following are administered: an analgesic of the surgeon’s preference for pain (most common is acetaminophen with codeine), promethazine suppository for nausea, and dexam-ethasone (optional) for swelling.
LABORATORY AND DIAGNOSTIC STUDIES
Results of a CBC, urinalysis, PT, and PTT are obtained.
Procedure
INCISION AND EXPOSURE
Th e procedure is initiated by making a decision whether the tonsillectomy or the adenoidectomy will be performed fi rst. Th e tonsillectomy is performed as follows: Th e tonsil is retracted with an Allis or similar tonsil clamp. Other material can be used to retract the tonsil as well. Sometimes, a 0-plain catgut suture is used on a curved urological needle. Th is is placed through the tonsillar tissue itself in a fi gure-of-eight knot. Th is provides good retraction without fragmenting the tonsillar tissue, which can happen with clamps. By retracting the tonsil medially, the anterior pillar is incised by whatever means the surgeon decides.
DETAILS
Th e incision is carried down until the capsule of the tonsil becomes visible. As previously mentioned, a knife, electrosurgery, or lasers can be used for this purpose. Using blunt and sharp dissection, the capsule of the tonsil is exposed from the ton-sillar fossa. Th e availability of a suction coagulator helps in the hemostasis. As the dissection continues, the superior pole of the tonsil is exposed and retracted from the tonsillar fossa. As blood vessels are encountered, they may be either cauterized or tied with suture. Slipknots of 2-0 or 3-0 catgut are placed around these vessels. Th e tonsil dissection then continues until the most inferior portion of the tonsil is exposed. At this time, the tonsil is removed from the tonsillar fossa with a snare, or with sharp dissection using electrosurgery, laser, or scissors. Aft er this is performed, the fossa of the tonsil is carefully inspected and any bleeding vessel is either cauter-ized or clamped and tied. Th e opposite tonsil is then removed in a similar fashion. An adenoidectomy should be performed with indirect vision using a mirror. A “blind” adenoidectomy is discouraged because the eustachian orifi ce can be injured.
Th e easiest way to expose the nasopharynx is by placing soft rubber catheters through the nasal cavity and bringing them out through the oral cavity. Before the catheters are placed through the nose, the surgeon oft en inspects the soft palate.

1118 Section 3: Operative and Invasive Procedures
Th is is important to identify congenital defects of the palate that might be a con-traindication to an adenoidectomy. Th ese catheters can then be used to retract the soft palate. Using a dental mirror that has been defogged with defogging solution, the surgeon can visualize the nasopharynx. Only in this way can the eustachian tube orifi ces be identifi ed and protected.
Diff erent devices have been designed to remove the adenoid tissue. A variety of adenoid curettes are available, which are most commonly used to scrape the lym-phoid tissue from the nasopharynx. Diff erent basket punches also exist to remove any loose fragments of lymphoid tissue. Th e adenoidectomy is a somewhat more diffi cult procedure, because of the possibility of leaving fragments of lymphoid tissue in the nasopharynx. Hemostasis is usually obtained with packing as well as the suction coag-ulator. It must be emphasized that, when suction coagulation is used, the eustachian tube orifi ce must always be in full view to prevent debilitating scarring and intractable middle ear problems.
CLOSURE
Before the procedure is terminated, a fi nal inspection is performed to evaluate for any bleeding sites. Th e nasopharynx can be irrigated with ice or room temperature normal saline. Th e stomach contents should be suctioned out before the procedure is terminated to decrease the chance of nausea and vomiting aft er the procedure.
Postprocedure Care
Because bleeding from the operative site is the most serious complication, this must be watched for at all times in the immediate postoperative period. Any bleed-ing must be reported to the surgeon immediately. When the patient is transferred to the PACU, he or she is oft en lying on the side. Th is decreases the chance of aspi-ration of blood or secretions. Analgesia is almost always required for the patients. Th e discomfort aft er a tonsillectomy and adenoidectomy is oft en underemphasized. A balance must be made between narcotic administration and depression of the central nervous system. Analgesia is attempted; however, too much sedation should he avoided to prevent aspiration.
A liquid diet is initiated only if the patient is awake enough to ask. Antiemetic medication is also oft en prescribed.
Potential Complications
Complications may include bleeding that can be life threatening; pain and inabil-ity to swallow, which can cause dehydration in young children; injury to the eusta-chian tube orifi ces; aspiration of blood, leading to pulmonary complications; and aspiration, leading to airway obstruction and respiratory arrest.
ParotidectomyDefi nition and Indications
Parotidectomy refers to the partial or complete excision of the parotid gland. Th e primary purpose of parotidectomy is to remove neoplasms that occur in the parotid gland. Parotid gland neoplasms are usually benign (approximately 80%); tumors may

Chapter 30: Otorhinolaryngological Surgery 1119
30
spread from other areas of the body, entering the parotid gland via the lymphatic system (Encyclopedia of Surgery, 2008f). Th e minimal operation performed for these tumors is a superfi cial or lateral parotidectomy. Malignant lesions oft en necessitate the removal of the entire parotid gland, including the deep lobe. At times, a radical neck dissection or other more radical procedures are combined with a parotidec-tomy. However, for most parotid tumors, a lateral parotidectomy with preservation of the deep lobe and the facial nerve is all that is necessary.
Nursing Implications
ANESTHESIA
Operations performed on the parotid gland are always done using general anes-thesia. It is critical that no neuromuscular blockade be used during the procedure. Th is is because identifi cation of the facial nerve is oft en made not only with visual-ization but also by stimulation using a nerve stimulator. If blockade has been given, the nerve is not stimulated. Th is might lead to inadvertent severing of facial nerve branches.
POSITION
Th e position of the patient is supine with the aff ected side of the face up. A small roll underneath the shoulders, as well as a headrest, provides stabilization of the area.
ESTABLISHING AND MAINTAINING THE STERILE FIELD
Th is is a sterile procedure and therefore diff erent from the previously described techniques within the oral or nasal cavities. Th e establishment and maintenance of the sterile fi eld are critical and must adhere to the principles of aseptic technique. Because parotidectomy can be a lengthy procedure, padding must be provided for pressure points. Aft er the patient is asleep and intubated and appropriate positioning has been obtained, the patient’s face is prepared with antimicrobial solutions. Th e face is draped from the level of the forehead down to the level of the clavicle on the operative side. It is oft en a good practice to place a cotton ball or other type of wick into the ear canal to prevent preparation solutions from entering the ear canal.
It is important that the face be visible at all times. Stimulation of the facial nerve leads to movement of the muscles of facial expression. Th erefore, the ability to see movement in the face is of utmost importance. A self-adhering plastic drape can be used to cover the entire face and neck. Some surgeons prefer not to do this and just keep the face exposed. Towels are used to create a sterile fi eld. Lint-free sterile drapes are then used to cover the patient inferiorly and superiorily.
EQUIPMENT AND SUPPLIES
A general plastic set, a nerve stimulator, special parotid retractors, and bipolar electrosurgery unit should be available.
PHYSIOLOGICAL MONITORING
Because a parotidectomy can be a lengthy procedure, the patient’s comfort and safety are important. All bony prominences are padded to decrease the risk of nerve

1120 Section 3: Operative and Invasive Procedures
damage and a pillow is off ered for under the knees to decrease back strain. Th e ECG, blood pressure, and oxygen saturation are monitored by the anesthesia provider. Th e circulating nurse should be aware of monitoring and assist the anesthesia provider as necessary.
SPECIMENS AND CULTURES
Parotid tissue is sent to the pathology department.
DRUGS AND SOLUTIONS
No drugs or solutions are needed.
PHYSICIAN ORDERS
A regular diet is given. Th e IV catheter is kept open until the patient is tolerating fl uids. Antiemetic and analgesic of physician’s choice are administered. Facial func-tion should be checked. Th e patient may be up ad lib.
LABORATORY AND DIAGNOSTIC STUDIES
CBC, urinalysis, and CT scan are obtained.
Procedure
INCISION AND EXPOSURE
Th e incision is made immediately in front of the ear following natural skin creases. Th e incision extends below the earlobe and into the neck below the angle of the jaw. Th e incision is carried down into the neck to provide full visualization of the facial nerve. Anterior and posterior skin fl aps are developed. Th is incision is carried down sharply using a blade until the fascia overlying the parotid gland is seen. Monopolar electrosurgery should be used carefully because transmission of electrosurgical cur-rent to and subsequent injury of the facial nerve may occur. It is better to provide electrosurgery using a bipolar mode.
DETAILS
Aft er the parotid fascia is identifi ed, the next portion of the procedure involves careful dissection using curved clamps to separate the gland from the mastoid pro-cess and the cartilage of the external auditory canal. At times, there is troublesome bleeding, which can usually be controlled with bipolar electrosurgery. Th e tail of the parotid gland is then separated from the anterior and superior portions of the ster-nocleidomastoid muscle.
Th e most important portion of the operation is the identifi cation of the main trunk of the facial nerve. Using a small curved or delicate Crile clamp, the parotid fascia is carefully elevated. Th e fascia is then transected carefully and the main trunk is identi-fi ed. At times, identifi cation is diffi cult. Th e cartilage of the external auditory canal can be used as a guide to fi nding the main trunk. Aft er the main trunk is identifi ed, the dissection proceeds anteriorly and laterally. It is critical that the dissection fol-low the trunk of the facial nerve. Th e branches of the facial nerve are identifi ed most easily in this fashion. At times, the main trunk is not found readily. Identifi cation of

Chapter 30: Otorhinolaryngological Surgery 1121
30
a superfi cial branch can be made and followed posteriorly and deeply to the main trunk. However, the safest technique is to identify the main trunk and pursue the course of the branches in a posterior-to-anterior fashion. Th e nerve stimulator here becomes important to trace small branches of the facial nerve. As the branches of the facial nerve become visible, the substance of the parotid gland and the lesion within it can be dissected away safely. Aft er the freed portion of the superfi cial lobe is dissected from the facial nerve branches, the parotid duct is transected and ligated at the anterior wound margin.
CLOSURE
Aft er the parotid gland and the lesion are removed from the operative fi eld, the nerve fi bers are again identifi ed. Any areas of bleeding are either ligated with small silk ties or cauterized using bipolar cautery. Th e previously raised fl aps are then reap-proximated using 4-0 or 5-0 absorbable suture and the skin is closed using 5-0 or 6-0 nonabsorbable suture material. A small tissue drain, preferably a suction drain, may be placed in the most dependent portion of the wound.
Postprocedure Care
A fi rm pressure dressing (similar to the previously described mastoid dressing) is used. However, the self-adherent gauze is used in a similar fashion to a modifi ed Barton dressing. Care must be taken to support the external ear. Aft er the wound is dressed, the patient is transferred to the PACU. One of the most important aspects of transfer, especially if a suction drain is placed, is to prevent accidental dislodging of the suction drain.
Aft er the patient is awake, the facial nerve can be examined by asking the patient to follow commands regarding facial expressions. Analgesics are usually ordered. Th e amount of discomfort is usually that of a pressure sensation from the pressure dressing. Th e dressing is left in place for at least 24–48 hours. Aft er this, the dressing is changed and the wound evaluated. Th e suction drain is removed at the surgeon’s discretion.
Potential Complications
Complications may include facial nerve injury, temporary or permanent (if a branch or main trunk is sectioned, immediate repair is indicated); bleeding with subsequent hematoma formation; recurrence of the lesion; and abnormal sweating on the side of the face.
UvulopalatopharyngoplastyDefi nition and Indications
Uvulopalatopharyngoplasty (UPPP) is a procedure used to remove excess tissue in the throat to widen the airway, in order to allow air to move through the throat more easily during breathing, thereby reducing snoring (Essig, 2008). Th e tissue that may be removed includes the uvula; a portion of the soft palate; excess throat tissue; tonsils and adenoids; and the pharynx. Th e procedure is indicated as a remedy for severe obstructive sleep apnea (OSA) believed to be caused by obstructions in the nose or pharynx.
UPPPUvulopalatopharyngoplasty
1122 Section 3: Operative and Invasive Procedures
Related Procedures
Laser-assisted uvulopalatopharyngoplasty (LA-UPPP) and tracheotomy are related procedures.
Nursing Implications
ANESTHESIA
UPPP is performed under general anesthesia.
POSITION
Th e patient is placed in the supine position with a small roll underneath the shoulders; a headrest is also used to provide stabilization.
ESTABLISHING AND MAINTAINING THE STERILE FIELD
Sterile drapes are placed on the patient’s chest and torso to prevent soiling the clothing with secretions or blood. Eye coverage/protection/head drapes are used based on the surgeon’s preference.
EQUIPMENT AND SUPPLIES
A general plastic set and bipolar cautery should be available.
PHYSIOLOGICAL MONITORING
Th e patient is monitored at all times as for previously described procedures.
SPECIMENS AND CULTURES
Th e tissues removed are sent for pathological study.
DRUGS AND SOLUTIONS
No drugs or solutions are needed.
PHYSICIAN ORDERS/LABORATORY AND DIAGNOSTIC STUDIES
Th e routine presurgical physical evaluation is performed. Additional preopera-tive diagnostic studies may include a complete polysomnogram to rule out nonob-structive causes of sleep apnea and confi rmation of the site of obstruction through fi beroptic pharyngoscopy or cephalometric radiographs with tracing.
Procedure
Aft er orotracheal intubation, a self-retaining mouth gag is placed to maintain adequate exposure. Th e oropharyngeal structures are carefully outlined. Th e lower portion of the soft palate, including the uvula, is excised. Th e tonsils and adenoids, if present, will also be removed at this time (see Fig. 30.18). Absorbable sutures are used to approximate the tissue edges.
Postprocedure Care
Th e patient remains in the hospital one to two nights, followed by a minimum two-week recovery period (Encyclopedia of Surgery, 2008g). Postoperatively, the patient may require continuous positive airway pressure (CPAP) therapy; certain analgesics
LA-UPPPLaser-assisted
uvulopalatopharyngo-
plasty
CPAPContinuous Positive
Airway Pressure

Chapter 30: Otorhinolaryngological Surgery 1123
30
are avoided since they relax the throat muscles, which can cause the throat to narrow and cause apnea episodes (Essig, 2007). Th e IV catheter is maintained at a keep-open rate until the patient is taking fl uids without nausea and vomiting.
Potential Complications
Complications aft er UPPP may include (Wikipedia, 2008b):
• Sleepiness and sleep apnea related to postoperative medication; • Swelling; • Infection; • Bleeding; • A sore throat and/or diffi culty swallowing; • Drainage of secretions into the nose and a nasal quality to the voice; • Narrowing of the airway in the nose and throat, thereby constricting
breathing; • Snoring; and • Iatrogenically caused sleep apnea.
TracheotomyDefi nition and Indications
A tracheotomy is performed to open a direct airway through an incision in the trachea (Wikipedia, 2008c). Adult and pediatric tracheotomy procedures are diff erent.
Th e indications for tracheotomy vary, but they are all for a maintenance of an artifi cial airway:
• Prolonged intubation or need to undergo ventilation • Upper airway obstruction in which orotracheal intubation is diffi cult or not
possible • Pulmonary toilet and cleaning of secretions
A permanent tracheotomy is always performed when there is a laryngectomy, or removal of the voice box.
Figure 30.18
UPPP.

1124 Section 3: Operative and Invasive Procedures
Nursing Implications
ANESTHESIA
Tracheotomies are oft en performed using local anesthesia in adults. General anesthesia, however, is preferred in the pediatric patient. A small amount of local anesthetic with vasoconstricting agents may be used to infi ltrate the skin in the area of the incision.
POSITION
Several important aspects of positioning exist when performing a tracheotomy. Unless it is contraindicated, the neck is hyperextended. A roll is placed under the shoulders. In young children, the chin is pulled superiorly as much as possible. Tape may be used to help further in hyperextending a child’s neck. Th e tape can be secured from the chin to the head of the bed. Th e surface landmarks of the neck are identifi ed.
ESTABLISHING AND MAINTAINING THE STERILE FIELD
Even though the respiratory system is entered, the procedure should be considered sterile. A marking pen can be used to mark the structures that have been palpated. Th e skin incision can be either horizontal or vertical. Th e neck is prepared with a skin antiseptic agent, and sterile drapes are applied in standard fashion.
EQUIPMENT AND SUPPLIES
In a young child, appropriate pediatric instruments are required. Th is may include smaller curved hemostats than in an adult tracheotomy set, as well as fi ne tissue for-ceps. In addition, a wide variety of sizes and types of tracheotomy tubes are essential. A discussion of the diff erent types of tracheotomy tubes is beyond the scope of this chapter, but sizes ranging from those small enough to fi t premature infants to those suitable for the largest adult must be readily available.
PHYSIOLOGICAL MONITORING
If the procedure is performed with general anesthesia, routine care as discussed for previous procedures should be maintained. However, if the procedure is done using local anesthesia, it is vital that the circulating nurse explain the procedure and the sensations that the patient will experience before the procedure. Th e placement of a shoulder roll, the application of the electrosurgery patient return electrode and possible wrist restraints, and the feeling of “loss of breath” are all critical to explain to the patient. During this procedure, the nurse plays a vital role in decreasing the patient’s anxiety level by being close at hand. ECG, respirations, blood pressure, and pulse oximetry are monitored throughout the procedure.
SPECIMENS AND CULTURES
No specimens are obtained.
DRUGS AND SOLUTIONS
Drugs and solutions needed for this procedure include the following:

Chapter 30: Otorhinolaryngological Surgery 1125
30
• Lidocaine 1% with 1:100,000 epinephrine • Lubricant jelly • Lidocaine 4% transtracheal injection
PHYSICIAN ORDERS
Th e physician orders a chest radiograph, tracheostomy care as necessary, continu-ation of IV fl uid administration, pulmonary function studies if indicated, and respi-ratory therapy if necessary.
LABORATORY AND DIAGNOSTIC STUDIES
CBC, urinalysis, and a chest radiograph are obtained.
Procedure
INCISION AND EXPOSURE
A vertical incision technique is described. Aft er the skin incision has been made, it is carried deep through the platysma muscle (Fig. 30.19A). It is carried down until the fascia in the midline between the small strap muscles of the neck is identifi ed. Th e fas-cia is then incised in a sharp fashion using a blade. Th e strap muscles are then retracted laterally. Th is usually exposes the thyroid gland isthmus (ie, the connection between both sides of the thyroid gland). A decision must be made at this time whether the isthmus of the thyroid gland will be transected or merely retracted (see Fig. 30.19B). If a decision is made to transect the thyroid gland, curved hemostats are used to dissect the gland gently from the trachea below. Th e gland is transected between two curved hemostats and ligated using absorbable 3-0 suture material. Th is facilitates visualiza-tion of the structures below.
DETAILS
Th e cricoid cartilage should be fully visible. As the surgeon prepares to enter the windpipe, the scrub person must have the tracheotomy tube prepared and available to be inserted. Th e anesthesia provider is notifi ed that the airway will be entered. Th e technique of entering the airway varies in children and adults. In adults, a No. 11 blade knife can be used to cut a window of cartilage in the area of the second, third, or fourth tracheal arch (sec Fig. 30.19C). A fl ap of tracheal cartilage has also been advocated.
In young infants, however, before the airway is entered, it is important to place silk stay ties on the lateral portion of the trachea. Th ese can be used to help bring the trachea out into the neck incision in case of accidental decannulation. Also in the pediatric population, a sharp blade that is short (a Beaver 6900 blade is ideal) can be used to incise the tracheal arches. In the pediatric population, a portion of the tracheal arch is not removed. Instead an incision is made along the third, fourth, and, at times, fi ft h tracheal arch.
Aft er elevating the tracheal ring (see Fig. 30.19D), the surgeon places the trache-otomy tube, complete with the obturator, through the opening. Th e tracheotomyties

1126 Section 3: Operative and Invasive Procedures
and a syringe to infl ate the cuff are attached to the tube. Th e obturator is removed and an inner cannula is inserted. Sterile anesthesia connectors are then used to connect a tracheotomy tube to the anesthesia machine if the tube selected is not designed with the appropriate connector.
CLOSURE
Aft er the airway has been established, the tracheotomy tube can be secured using the tracheotomy ties usually included in tracheotomy tube sets. In addition, for extra pro-tection, the fl anges of the tracheotomy tube may be sutured to the skin of the neck.
Postprocedure Care
In the immediate postprocedure period, a chest radiograph should be obtained, especially for young infants. Th e possibility of pneumothorax exists in the younger patient. In addition, even small tracheotomy tubes are at times too long in the very young patient. Th is can cause the tracheotomy tube tip to ventilate only one side of the chest. Visualization of the tube tip on a chest radiograph helps prevent this complication. Th e excessive incision can be approximated using a single skin non-absorbable suture in the young patient. However, care must be taken not to create an airtight wound. Th is is because air escape from a tracheotomy tube almost always occurs. If the wound is closed tightly, there can be air dissection into the subcutane-ous tissues.
As the patient is transported to either the PACU or the intensive care unit, the most important portion of the transport is prevention of accidental dislodging of the tracheotomy tube. Elbow restraints should be used to prevent young children from pulling at the tracheotomy tube. If necessary, sedation is ordered by the surgeon.
Figure 30.19
Tracheotomy procedure.

Chapter 30: Otorhinolaryngological Surgery 1127
30
Performing pediatric tracheotomies should be discouraged in settings in which pedi-atric intensive care units are not readily available. Th e nursing staff is critical in pre-venting accidental decannulation and subsequent tragedies. Most patients require frequent suctioning of secretions in the fi rst 24 hours. Additional tracheotomy tubes of the size used must always accompany the patient. Th e previously placed tracheal stay sutures should be marked right and left . In case of accidental decannulation, these sutures may be used to elevate the trachea and aid in replacement of the tra-cheotomy tube. Th e obturator is secured to the head of the patient’s bed at all times to aid in replacement of the tube.
Potential Complications
Complications may include injury to the nerves of the vocal cords; injury to large blood vessels abnormally located in the area of the incision; pneumothorax; accidental decannulation during the postoperative period, especially in children; pneumonia; infections in the area of the skin or within the trachea; formation of a tracheoesophageal fi stula; tracheal stenosis; and erosion of blood vessels, leading to fatal hemorrhage.
Total Laryngectomy and Radical Neck DissectionDefi nition and Indications
Total laryngectomy refers to the excision of the entire larynx with the stoma open-ing into the larynx being permanent; the patient breathes through the stoma and must learn to talk in a new way (MedicineNet.com, 2008b). Radical neck dissec-tion refers to excision of a tumor, the surrounding anatomical structures, and lymph nodes on the aff ected side of the neck.
Th e primary indication for partial or total removal of the larynx and radical neck dissection is to treat cancer. Because patients undergoing laryngectomy or neck dis-section are usually heavy alcohol and tobacco users, their overall medical condition must be fully evaluated. At times, preoperative or adjuvant chemotherapy is also advocated.
Related Procedures
Hemilaryngectomy or partial laryngectomy and supraglottic laryngectomy are related procedures.
Nursing Implications
ANESTHESIA
Th e anesthesia implications are usually identical to those described for a trache-otomy using general anesthesia. Th e anesthesia provider should be positioned to the side of the patient on the unaff ected side of the neck. Usually, an arterial line is placed. Blood gas levels are oft en monitored.
POSITION
Th e positioning implications are usually identical to those described previously for a tracheotomy. If an accompanying neck dissection is to be performed, the head may

1128 Section 3: Operative and Invasive Procedures
need to be turned to the appropriate side. Th e comfort and safety devices described earlier for ear procedures are used.
ESTABLISHING AND MAINTAINING THE STERILE FIELD
Th e entire face, including the ears, the neck, and the chest to the nipple line should be prepared with a skin antiseptic agent. If necessary, the chest hair should be removed using clippers or depilatory. If a tracheostomy stoma is present, the stoma is included in the area to be prepped. Th e nurse must avoid getting solutions in the stoma. If the surgeon intends to obtain a graft , the thigh is prepared as well. Th e sterile fi eld is cre-ated using a head and neck drape pack. Care is taken in lift ing the patient’s head for application of the head drape, and the anesthesia provider is informed before this is done. Th e patient is then draped with appropriate sterile sheets.
EQUIPMENT AND SUPPLIES
A general plastic set, a tracheostomy set, a vascular set, bipolar cautery, a head-light, a nerve stimulator, an eggcrate or gel pad for the bed, a convective warming device, a scale for weighing sponges, antiembolism stockings (these may be applied preoperatively before transfer to the operative and invasive procedure suite), a naso-gastric feeding tube, a closed suction drain, bone cutters and an oscillating saw (for partial laryngectomy), a Foley catheter, and tracheostomy and/or laryngectomy tubes are assembled.
PHYSIOLOGICAL MONITORING
Most head and neck cancer cases are lengthy; therefore, a Foley catheter is usually inserted. In addition, a nasal feeding tube is usually passed through one naris down to the level of the throat. At the end of the procedure, this feeding tube is advanced into the esophagus and into the stomach. Th is tube is used to feed the patient in the postprocedure period.
Th e sponges are weighed throughout the procedure to obtain an estimate of blood loss during the procedure. Th e patient’s temperature is also monitored with a rectal probe. An oral temperature probe is contraindicated to decrease the number of tubes in the surgical fi eld. Blood gas and electrolyte values are monitored throughout the procedure.
SPECIMENS AND CULTURES
Contents of the radical neck dissection to include the lymphatics, the jugular vein, the 11th cranial nerve, the sternocleidomastoid muscle and the submandibular salivary gland, the ipsilateral portion of the thyroid gland, and the larynx are the surgical specimens.
DRUGS AND SOLUTIONS
Drugs and solutions required for this procedure may include those listed below:
• Lidocaine 1% with 1:100,000 epinephrine • Oxidized regenerated cellulose (Surgicel) • Lidocaine 4%

Chapter 30: Otorhinolaryngological Surgery 1129
30
• Hetastarch (Hespan) for anesthesia • Antibiotic of surgeon’s preference
PHYSICIAN ORDERS
Th e physician orders an IV, antibiotics of choice, the use of drains to suction, noth-ing by mouth for 48 hours, admittance to the intensive care unit, and a chest radio-graph. Vital signs are obtained every hour for 4 hours and then every 4 hours. Mouth care and tracheotomy care are given as necessary. Humidifi ed oxygen is given per tracheotomy collar at 5 L/minute. Analgesics and antiemetics of choice are ordered. Th e patient is advanced to tube feeding every 4 hours and is up to a chair on the fi rst postoperative day.
LABORATORY AND DIAGNOSTIC STUDIES
CBC, urinalysis, PT, PTT, SMA-15, electrolyte values, a chest radiograph, and CT scan are obtained.
Procedure
INCISION AND EXPOSURE
Aft er the neck has been prepared and draped as described previously, a decision is made about the skin incision. If a laryngectomy is going to be performed without a neck dissection, the head should stay in the midline and be hyperextended. If a partial laryngectomy (ie, a vertical or supraglottic laryngectomy) is the operative procedure, appropriate horizontal incisions are planned. If the procedure is to be a total laryngectomy without neck dissection, the incision is usually a midline vertical incision or midline transverse incision.
Because the operation is most commonly performed in conjunction with a neck dissection, the incisions planned can vary at the discretion of the surgeon. Th e description below is for the most comprehensive of laryngectomy procedures (a total laryngectomy and radical neck dissection).
Th e goal of the neck dissection is to remove all lymph node-bearing tissue from the midline anteriorly to the trapezius muscle posteriorly and also from the mandible superiorly to the clavicle inferiorly. All of this tissue between the deep cervical fascia and the platysma muscle externally is removed, except for the carotid artery system and the vagus, phrenic, and hypoglossal nerves. Th e brachial plexus is also preserved.
Th e contents of the neck that are removed include the jugular vein, the spinal accessory (11th cranial) nerve, the sternocleidomastoid muscle, and the subman-dibular salivary gland. Sometimes, the spinal accessory nerve can be preserved.
When the operation is combined with a total laryngectomy, the larynx, the mid-portion of the hyoid bone, and the epiglottis are also removed. Inferiorly, the laryn-gectomy also includes at least one or two tracheal arches. Th e patient requires a permanent tracheotomy.
Various skin incisions have been described. Th e most common incision is an apron incision extending from the mastoid tip inferiorly to approximately two fi nger breadths above the clavicle across the midline and frequently to the contralateral mastoid tip. Th e skin fl aps are then elevated, including the platysma muscle.

1130 Section 3: Operative and Invasive Procedures
Aft er the fl aps have been raised, care must be exercised that the external jugular vein is not accidentally cut. Th e vein should instead be doubly ligated with tie and suture ligature and then transected. Th e inferior border of the sternocleidomastoid muscle is identifi ed and a clamp is placed under the muscle. Th e muscle is then sec-tioned and retracted superiorly. Th e carotid sheath is then identifi ed, and the inter-nal jugular vein is isolated. Care is taken to preserve the vagus nerve also present within the carotid sheath.
DETAILS
A proximal suture ligature and a distal silk tie are placed above and below, respec-tively, the line of transection of the internal jugular vein. Th e vein is then sectioned. Th e muscle with internal jugular vein and associated lymph nodes and fat is raised superiorly. Th e radical neck dissection specimen also includes transection of the strap muscles immediately superfi cial to the larynx and trachea. At this time, the ipsilateral portion of the thyroid gland is transected and also taken with the speci-men. Th e trachea is now entered, and endotracheal anesthesia is directed into the distal portion of the trachea. Th e upper portion of the specimen includes the tra-cheal arches and the entire larynx. Th e uppermost portion of the laryngeal complex includes the hyoid bone. Th e hyoid bone is transected from all the attachments to the muscles of the throat and tongue. As the dissection continues, the junction of the upper end of the esophagus with the lower end of the hypopharynx becomes visible. Aft er this is done, the specimen, including the larynx and the upper portion of the trachea, is in connection with the radical neck specimen.
Th e pharyngeal defect is in the shape of a T. Th e remainder of the neck contents including the contents of the submandibular space, just described, is lift ed superiorly. Th roughout this submandibular space are large arteries and veins that necessitate suture ligatures. In addition, the duct of the submandibular gland must be ligated. Aft er this is done, the entire specimen is attached in the posterior and superior por-tion. Th e dissection is now carried from the anterior to the posterior direction until the internal jugular vein limits the dissection. At this time, a double ligation of the internal jugular vein is performed. A suture ligature is placed as well. Th e vein is then transected. Th e remaining portion includes the tail of the parotid, which is transected along with the attachment of the sternocleidomastoid muscle. Many ves-sels are encountered in this area and need ligation.
CLOSURE
Th e entire specimen, including the larynx, is now removed from the operative fi eld. Th e nasal feeding tube that was placed at the beginning of the procedure is advanced through the T-shaped pharyngeal defect until it is visible within the opera-tive fi eld. It is then directed into the distal esophagus and the defect is closed over it. Th e defect is closed in a continuous inverting fashion using an absorbable suture of the surgeon’s preference. Th e entire neck wound is then ready for closure.
Th e wound is copiously irrigated with either normal saline or an antibiotic solu-tion. A two-layer closure using absorbable suture is employed for the approximation of the platysma muscle and subcutaneous tissue. To close the skin, nonabsorbable

Chapter 30: Otorhinolaryngological Surgery 1131
30
suture or skin staples are used. Th e distal trachea is sutured to the skin using inter-rupted, nonabsorbable sutures. Two suction drains are used, taking care not to place them directly over the carotid artery (Fig. 30.20).
Appropriately sized laryngectomy tubes should be available. Laryngectomy tubes are similar to tracheotomy tubes, except that they are usually shorter and of wider inner diameters. Th e preparation of the tubes before insertion is identical to that for tracheotomy tubes.
Partial LaryngectomyTh ere are clinical situations when a total laryngectomy is not necessary (Fig. 30.21).
In malignancies of the larynx for which adequate margins can be obtained, preser-vation of a portion of larynx is preferred. In this way, a more functional voice can
Figure 30.20
Total laryngectomy.
Figure 30.21
Partial laryngectomy.
1132 Section 3: Operative and Invasive Procedures
be obtained. Diff erent procedures have been described. Th ese include a supraglottic laryngectomy in which the epiglottis, false vocal cords, and hyoid bone are removed but the rest of the larynx is preserved. Also possible is a vertical or frontolateral hemi-laryngectomy. With any conservation laryngectomies, a prophylactic tracheotomy is always performed.
Voice rehabilitation is a critical part of the short- and long-term followup of patients who have had any type of laryngectomy. Many surgeons advocate immediate insertion of a voice prosthesis aft er a total laryngectomy. Diff erent types of prostheses exist. Other ways of communicating include esophageal speech, an electrolarynx, or simply a writing tablet and pencil. Before a patient undergoes a laryngectomy, exten-sive counseling should be given on voice rehabilitation. Th e nurse can make the tran-sition to loss of the voice easier by being sensitive to the needs of this type of patient.
Postprocedure Care
Aft er the procedure is completed, a pressure dressing is applied by some surgeons, taking care not to occlude the laryngectomy opening. Many patients undergoing a lengthy oncological procedure stay in an intensive care unit setting overnight, or longer. Analgesics and antiemetics are given. Intense humidifi cation to the airway is given as well. Care must be taken not to dislodge the suction drains.
Potential Complications
Complications may include injury to uninvolved nerves as well as laceration of large blood vessels of the neck; injury to the lung pleura leading to a pneumotho-rax; necrosis of the skin and exposure of the carotid artery, leading to exsanguinat-ing hemorrhage; fi stula formation between the pharynx or esophagus and the skin aft er laryngectomy; recurrence of tumor; and stenosis of the remaining pharynx and esophagus.
PanendoscopyDefi nition and Indications
Panendoscopy is an integral part of the care of the patients with head and neck can-cers, hoarseness, dysphagia (diffi culty with swallowing) and/or dyspnea (shortness of breath), and evaluation and treatment of foreign bodies or trauma. Panendoscopy is a term that refers to the endoscopic evaluation of the pharynx, larynx, upper trachea, and esophagus (Medilexicon, 2008). Th e endoscopic evaluations are indicated to evaluate the extent and involved anatomical structures of the primary pathology and to rule out the possibility of secondary pathological processes. Panendoscopy has most clini-cal application in the diagnosis and workup of head and neck cancer patients. Th ese patients most commonly have squamous cell cancer. Th ey classically use tobacco and alcohol, which are known co-carcinogens of the upper aerodigestive tract mucosa. Th erefore, direct laryngoscopy, fl exible or rigid bronchoscopy, and esophagoscopy can be performed in conjunction with biopsies of suspicious areas to rule out synchronous primary lesions, which are found in up to 5% of patients. Frequently, lesions of the larynx, base of tongue, and hypopharynx require endoscopic visualization or palpa-tion to defi ne the optimal treatment. In today’s era of cost effi ciency these procedures

Chapter 30: Otorhinolaryngological Surgery 1133
30
may be combined with the anesthetic for defi nitive treatment or deleted if the chest radiograph and barium swallow/esophagogram arc normal.
Related Procedures
Microdirect laryngoscopy with biopsy and bronchoscopy/esophagoscopy and foreign body retrieval are related procedures (see brief description of each procedure below).
Nursing Implications
ANESTHESIA
Th ese endoscopic procedures are performed using general anesthesia. Previously, they were performed using topical anesthesia with or without sedation, but this is rarely done today.
POSITION
Th e patient is positioned supine on the table with the head at the end of the bed. Th e use of donut roll head supports and/or shoulder rolls varies from surgeon to surgeon but they are worth having available.
ESTABLISHING AND MAINTAINING THE STERILE FIELD
Th ese are not sterile procedures, but sterile drapes are placed on the patient’s chest/torso to prevent soiling the clothing with secretions or blood. Eye coverage/protection/head drapes are used based on the surgeon’s preference.
EQUIPMENT AND SUPPLIES
Th e number and type of scopes should be reviewed with the surgeon before induc-tion to ensure immediate access to the appropriate scope once the patient is asleep. Th e equipment and supplies for panendoscopy are outlined in Table 30.5.
Table30.5
Panendoscopy Instruments
Laryngoscopes (anterior commissure, Jackson, “wide mouth”)
Video tower
Suspension arm for laryngoscope
Rigid or fl exible esophagoscopes
Rigid or fl exible bronchoscopes
Light source for the above
Neurosurgical 1 × 3-cm cottonoids
Laryngoscopy suction—velvet eye
Bronchoscope suction—velvet eye
Tooth guard
Moist Telfa pads
Optional items include
Operating microscope with 350- or 400-mm lens
CO2 laser
Biopsy forceps

1134 Section 3: Operative and Invasive Procedures
PHYSIOLOGICAL MONITORING
Monitoring appropriate for general anesthesia should be done.
SPECIMENS AND CULTURES
Tissue samples should be meticulously labeled.
DRUGS AND SOLUTIONS
Saline, mineral oil, and oxymetazoline (Afrin) or another vasoconstrictor should be available.
PHYSICIAN ORDERS AND LABORATORY AND DIAGNOSTIC STUDIES
Routine preprocedure testing and evaluation by a medical doctor.
Procedure
Direct laryngoscopy is performed to evaluate the larynx, including vocal cords, epi-glottis, and adjacent areas such as the base of the tongue, pyriform sinuses, lateral/posterior pharynx, and the postcricoid region. Before commencing the visualization, the teeth are evaluated for previous injury, loose/injured teeth are noted, and mucosal or mass lesions in the oral cavity are examined. Th e base of the tongue and pharynx are palpated for any signs of pathology. Most patients benefi t from a drying agent such as glycopyrrolate. Patients who require subacute bacterial endocarditis prophylaxis should receive antibiotics; otherwise, most surgeons do not give prophylactic antibiotic coverage (so as not to mask signs of aerodigestive tract injury or perforation). A tooth guard is utilized for the dentate patient. Th e surgeon introduces and drives the various scopes to evaluate the larynx, pharynx, esophagus, and tracheobronchial tree. Moist-ening the scopes or the patient’s lips with saline or mineral oil can help minimize trauma. If suction is required, the assisting nurse usually hands the device to the sur-geon aft er the tip has been placed in the lumen of the scope. If fl exible esophagoscopy is performed, many surgeons introduce the scope in the postcricoid region with direct visualization using the Jackson laryngoscope with the sleeve removed.
Flexible bronchoscopy is performed either through the endotracheal tube or by “driving” the scope beyond the cuff of the typically smaller endotracheal tube. Some surgeons extubate the patient and perform rigid bronchoscopy with or without ven-tilation. Th is is mandatory to visualize the subglottic area and proximal trachea.
Th e removal of the scope is the endpoint of the procedure. Th e laryngoscopes or bronchoscopes should not be removed from the surgical suite until the patient is awake and the airway is stable in case emergency access is needed.
Postprocedure Care
In the PACU and ensuing 24 hours, the patient is monitored for fevers, chest pain, and dysphagia, which can be associated with pneumothorax or esophageal perfora-tion. Many surgeons obtain postprocedure chest radiographs in the PACU to evalu-ate for pneumothorax/pneumomediastinum and widened mediastinum.
Potential Complications
Complications may include sore throat, dental trauma, lip contusion/laceration, laryngospasm, pneumothorax, and esophageal perforation.

Chapter 30: Otorhinolaryngological Surgery 1135
30
REFERENCES
ENDNOTE
1. Berke, J. (2007). Cochlear implant surgery. Retrieved August 28, 2008 from http://deafness.about.com/od/basicsofcochlearimplants/a/cisurgery.htm.
2. Dev, V.R. (2006). Facial trauma, nasal fractures. Retrieved August 29, 2008 from http://www. emedicine.com/plastic/topic482.htm.
3. Encyclopedia of Surgery. (2008a). Tympanoplasty. Retrieved August 29, 2008 from http://www. surgeryencyclopedia.com/St-Wr/Tympanoplasty.html.
4. Encyclopedia of Surgery. (2008b). Mastoidectomy. Retrieved August 29, 2008 from http://www. surgeryencyclopedia.com/La-Pa/Mastoidectomy.html.
5. Encyclopedia of Surgery. (2008c). Stapedectomy. Retrieved August 29, 2008 from http://www. surgeryencyclopedia.com/Pa-St/Stapedectomy.html.
6. Encyclopedia of Surgery. (2008d). Septoplasty. Retrieved August 29, 2008 from http://www. surgeryencyclopedia.com/Pa-St/Septoplasty.html.
7. Encyclopedia of Surgery. (2008e). Endoscopic sinus surgery. Retrieved August 29, 2008 from http://www. surgeryencyclopedia.com/Ce-Fi/Endoscopic-Sinus-Surgery.html.
8. Encyclopedia of Surgery. (2008f). Parotidectomy. Retrieved August 29, 2008 from http://www. surgeryencyclopedia.com/La-Pa/Parotidectomy.html.
9. Encyclopedia of Surgery. (2008g). Snoring surgery.Retrieved August 30, 2008 from http://www. surgeryencyclopedia.com/Pa-St/Snoring-Surgery.html.
10. Essig, M.G. (2007). Uvulopalatopharyngoplasty for obstructive sleep apnea. Retrieved August 30, 2008 from http://www.aolhealth.com/procedures/uvulopalatopharyngoplasty-for-obstructive-sleep-apnea.
11. Essig, M.G. (2008). Uvulopalatopharyngoplasty for snoring. Retrieved August 28, 2008 from http://www.webmd.com/sleep-disorders/uvulopalatopharyngoplasty-for-snoring.
12. Kavanaugh, K.T. (2008). Adenotonsillectomy. Retrieved August 29, 2008 from http://www.entusa.com/tonsils_adenoid_surgery.htm.
13. Levenson, M.J. (2008). Cochlear implants. Retrieved August 28, 2008 from http://www.earsurgery.org/cochlear.html.
14. Medcyclopaedia. (2008). Caldwell-luc procedure. Retrieved August 28, 2008 from http://www. medcyclopaedia.com/library/topics/volume_vi_2/c/caldwell_luc_procedure.aspx.
15. MedicineNet.com. (2008a). Ear tubes (myringotomy & tympanostomy tubes). Retrieved August 28, 2008 from http://www.medicinenet.com/ear_tubes/article.htm.
16. MedicineNet.com. (2008b). Defi nition of total laryngectomy. Retrieved August 28, 2008 from http://www.medterms.com/script/main/art.asp?articlekey=25443.
17. MediLexicon. (2008). Panendoscopy. Retrieved August 28, 2008 from http://www.medilexicon.com/medicaldictionary.php?t=64705.
18. National Institute on Deafness and Other Communication Diseases. (NIDCD). (2007). Cochlear implants. Retrieved August 28, 2008 from http://www.nidcd.nih.gov/health/hearing/coch.asp.
19. US Food and Drug Administration (US FDA). (2004). Before, during, and aft er implant surgery. Retrieved August 28, 2008 from http://www.fda.gov/cdrh/cochlear/beforeduringaft ersurgery.html.
20. University of Miami School of Medicine. (2008). Cochlear implant surgery. Retrieved August 28, 2008 from http://cochlearimplants.med.miami.edu/medical/01_Cochlear%20Implant%20Surgery.asp.
21. Wikipedia. (2008a). Cochlear implant. Retrieved August 28, 2008 from http://en.wikipedia.org/wiki/Cochlear_implants.
22. Wikipedia. (2008b). Uvulopalatopharyngoplasty. Retrieved August 28, 2008 from http://en.wikipedia.org/wiki/UPPP.
23. Wikipedia. (2008c). Tracheotomy. Retrieved August 30, 2008 from http://en.wikipedia.org/wiki/Tracheotomy.
1. Th e drugs and solutions listed in this chapter are examples of the agents that the surgeon may choose to use during a procedure. Th e types of agents employed vary with surgeon preference.