trombosi venosa profonda post chirurgica · critical limb ischemia (cli) tasc 2007 chronic...
TRANSCRIPT


FINANCIAL DISCLOSURES
Employment No conflict of interest to disclose
Research support Bayer, Daiichi Sankyo, Pfizer
DSMB Pluristem
Consultancy No conflict of interest to disclose
Speakers bureau No conflict of interest to disclose
Major stockholder No conflict of interest to disclose
Patents No conflict of interest to disclose
Honoraria Bayer, Italfarmaco, Alfa
Wassermann, Aspen
Travel support No conflict of interest to disclose
Other No conflict of interest to
disclose

PAD (Tasc 2017, AHA 2016) / LEAD (ESC 2011, ESC ESVS 2017)
CLI - CTLI

Sopravvivenza a lungo termine in pazienti con
arteriopatia periferica
Criqui MH et al. N Engl J Med 1992;326:381-6
Normali
Arteriopatia asintomatica
Arteriopatia sintomatica
Arteriopatia sintomatica grave
100
75
50
25
0 2 4 6 8 10 12
So
pra
vv
iven
za (
%)
Anni
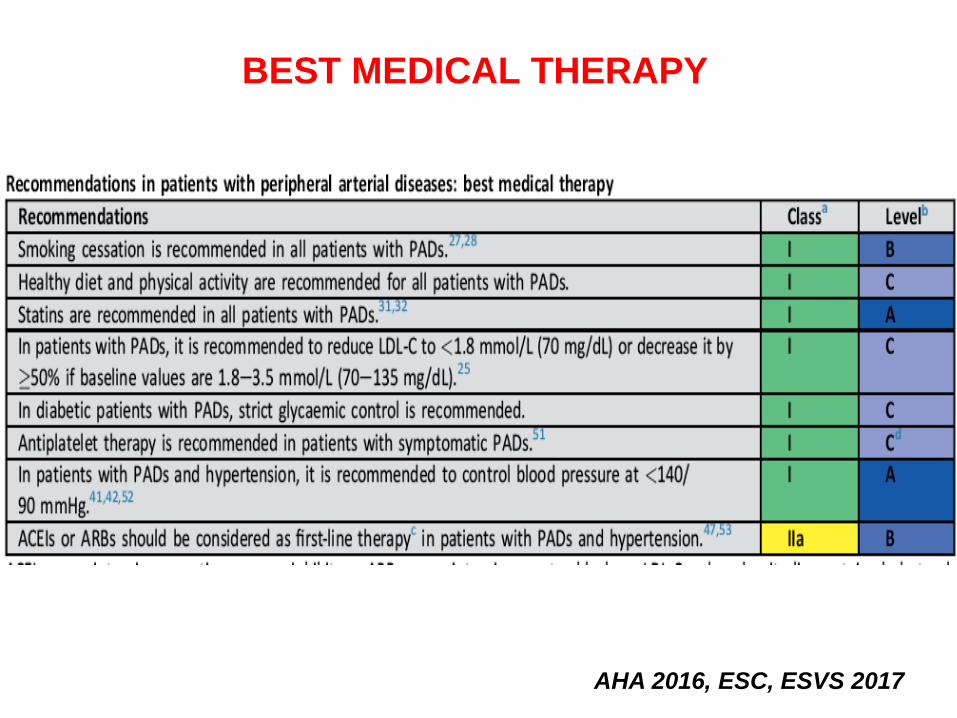
BEST MEDICAL THERAPY
AHA 2016, ESC, ESVS 2017

Critical Limb Ischemia (CLI) TASC 2007, AHA 2015
Chronic limb-threatening ischaemiaESC /ESVS 2017
• Clinical patterns with a threatened
limb viability related to several factors
• In contrast to the former term ‘critical
limb ischaemia’, severe ischaemia is
not the only underlying cause.

Critical Limb Ischemia (CLI) TASC 2007
Chronic limb-threatening ischaemiaESC/ESVS 2017
1^ Critical’ implies that treatment is urgent to avoid
limb loss, while some patients can keep their legs for long
periods of time even in the absence of revascularization
2^ The increasing predominance of diabetes in these situations,
present in 50–70% of cases, presents mostly as neuro-ischaemic
diabetic foot ulcers
3^ The risk of amputation not only depends on the severity of
ischaemia, but also the presence of a wound and infection. This
explains why ankle or toe pressures, measured to address LEAD
severity, are not a definition component of CLTI.

CLTI: severity and risk stratification The Wound Ischemia Foot Infection classification: Target population
• Ischaemic rest pain, typically in the forefoot with objectively confirmed haemodynamic studies (ABI <0.40, ankle pressure <50mmHg, toe pressure <30 mmHg, TcPO2 <30mmHg)
• Diabetic foot ulcer
• Non-healing lower limb or foot ulceration > 2 weeks duration or
• Gangrene involving any portion of the foot or lower limb
ESC/ESVS 2017
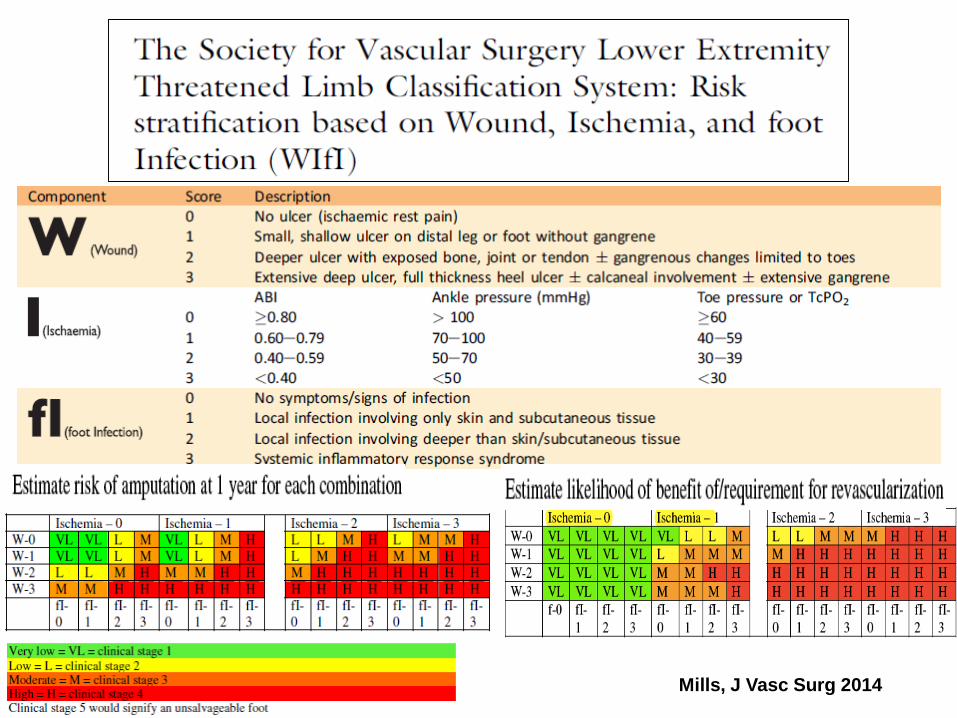
Mills, J Vasc Surg 2014

DECISION MAKING NEL
PAZIENTE CON CLI
PLAN
• Patient risk
• Limb threat severity (class. WIFI)
• ANatomic pattern (class. GLASS)

GLASS CLASSIFICATION
STADIO
GLASS
INSUCCESSO
TECNICO
PERVIETA’ AD
UN ANNO
I <10% >70%
II 10-20% 50-70%
III >20% >50%
Global Vascular Guidelines on CLTI, presented at the 2017 ESVS Annual Meeting

ESC/ ESVS 2017

EJVES 2017

Interdisciplinary care team for
PAD>CLI
AHA, 2016

Grazie per Attenzione!
