trigger point dry needling robert whittaker, spt
TRANSCRIPT

Trigger Point Dry NeedlingRobert Whittaker, SPT

History
Acupuncture has been practiced for more than 2000 years
1942 - Dr. Janet Travell published method of injections into trigger points & introduced the term myofascial trigger points (MTrP)
1979 - Dr. Karel Lewit concluded the effect of injections were caused by the mechanical stimulation from the needle alone.
1989 - Maryland became the first jurisdiction to allow intramuscular therapy

Trigger Point Dry Needling (TDN)
Trigger point – the presence of exquisite tenderness at a nodule in a palpable taut band of muscleAble to produce referred pain, either spontaneously or
on digital compressionActive – actively refers pain either locally or to another
location (refer along nerve pathways) Latent – one that exists but doesn’t yet refer pain
actively but may do so when pressure/strain is appliedKey – one that has pain referral pattern along a nerve
pathway that activates a latent MTrP Satellite – one which is activated by a key MTrP


What causes them?8
Chronic overload/repetition of muscles with poor mechanics
Acute overload (ie slipping/lifting/MVA)
In poorly conditioned muscles
Prolonged positions (posture)
Treatment Contract–relax–passive/contract-relax-active stretch done
repeatedly until the muscle lengthens Trigger point release – apply direct equal pressure over MTrP 8-20
sec until pain absent, repeat 3-4x if not resolved, gentle stretch/STM after
Spray & stretch Injection or Trigger Point Dry Needling (TDN)
Use of a fine filament needle to deactivate a MTrP within a taut muscle band

TDN6,7
Goal of TDN: desensitize supersensitive structures & restore motion & function Release shortened muscle, remove source of irritation, promotes healing
through local inflammation, decreases spontaneous electrical activity (SEA) at TP site
Mechanism of TDN Disrupts a dysfunctional motor endplate Needling results in a local twitch response (LTR) – alters muscle fiber
length as well as having an inhibitory effect on antagonistic muscle, may also utilize excessive Ach which previously was triggering increased firing of localized fibers
Chemical effects – Reduction immediately following an LTR of bradykinin, substance P, & CGRP which were present in trigger points, hypoxic MTrP causing an acidic environment which can lead to swelling, distorted nerve ending & muscle pain
Neurophysiological effects – stimulates afferent sensory A-delta nerve fibers for as long as 72 hours post TDN, may activate the inhibitory dorsal horn interneurons which may release opioid medicated pain suppression along with increasing overall BF

TDN
Treats Chronic pain, athletic population w/ specific reoccurring
injuries, elderly population, weekend warriors, anyone w/ pain & dysfunction
Contraindications masses/tumors, use of blood thinners, active infection,
hematomas
Complications allergic reactions, vasodepressive syncope, hematoma,
nerve/vascular injury, trauma to brainstem/spinal cord, increased spasm & pain of the muscle injected, penetration of visceral organ (lung 15%/bowel/kidney), infection, muscle edema

Performing TDN
Technique Position NOT SEATED, prepare skin with alcohol, apply
gloves, identify taut band first & palpate nodule Needle placed perpendicular to skin, needle angled
toward TP, can apply micro current/TENS, hemostasis is achieved by post-needling compression
May feel sore immediately after tx (lasts 24-48 hours feels like intense workout), common to have bruising (shoulder, base of neck, head/face, arms/legs)
Pt. may feel tired, sweaty, light headed, nauseous, emotional, or “out of it” (autonomic response) which can last for 1-2 hours

TDN
Failure Diagnostic error,
incomplete management of perpetuating factors, TP missed or inadequately treated, pain zone needled but not primary TP, irrelevant TP was needled, inadequate post needling care
Emergency Difficulty breathing, chest
pain, feeling light headed, having difficulty breathing, other concerning symptoms

After Needling
Stretch!
Increase water intake, hot bath/tub, work out/stretch, massage area, tylenol/ibuprofen/motrin
Reoccurrence?
Can be completed in same tissue once very 5-7 days

Meta-analysis of TDN on UQ3
12 RCTs selected Sham/placebo & use of other pain reducing injections (ie
lidocaine) compared to TDN
Conclusion Dry needling recommended compared to sham/placebo for
decreasing pain immediately after treatment & at 4 weeks for UQ myofascial pain syndrome (MPS)
When LTR elicited in studies comparing other tx, no significant differences
Total Effect Size (CI)
Immediate 4 weeks
TDN v Sham
1.06 (0.05, 2.06) 1.07 (-0.21, 2.35)
TDN v Other
-0.64 (-1.21, -0.06)
-0.07 (-1.39, 1.26)

TDN on TKA RCT5
40 subjects assigned to TND & sham group PT applied TDN to identified MTrP
while pt. anesthetized before start of surgery
Measured VAS, prevalence of MPS, & WOMAC at 1, 3, & 6 month follow up
Results Variation rate of pain higher in T
group, -54.5 (56.6) vs -30.5 (63.2) (p=0.048) at 1 month
MPS 30% difference in T compared to 11% S, but not statistically different (p=0.06)
WOMAC worse in T group through whole study*
TDN better than placebo, results different at 1 month
ResultsBaseline
1 mo 3 mo 6 mo
T VAS
56.8 (22.3)
23.8 (24.9)
20.6 (21.5)
23.5 (22.5)
S VAS
50.4 (16.8)
32.3 (25.7)
25.3 (20)
20.9 (18.6)
T MPS
80% 50% 50% 59%
S MPS
70% 59% 53% 64%

Rabbits & Pain/Inflammation/Hypoxia2
80 rabbits in 1D/1Dsham and 5D/5Dsham group TNF-α, substance P, COX-2 pain
from periphery to CNS β-endorphin can suppress
neurons from releasing substance P
Hypoxia responsive proteins – VEGF, iNOS, HIF-1α
Results Short term – 1D produces short
term analgesic effect, no lasting effect,
Long term – 5D increased proteins for capillary formation, excessive muscle damage from overload (muscle fibrosis?) β-endorphin predominate in later
phases of inflammation

Posture Effects on TDN using Shear-Wave Elastography4
7 female subjects w/ palpable MTrPs TDN to upper trapezius
muscle Ultrasound SWE allows for
quantification of soft tissue stiffness
Results Pre/post 29.5% reduction
(p<.01) Posture 21% reduction
(p<.05) Shear Modulus significantly
reduced in prone vs. sitting
Shear Modulus (kPA)
Sitting Prone
Before
After Before
After
Mean
13.56 9.11 10.23 7.67
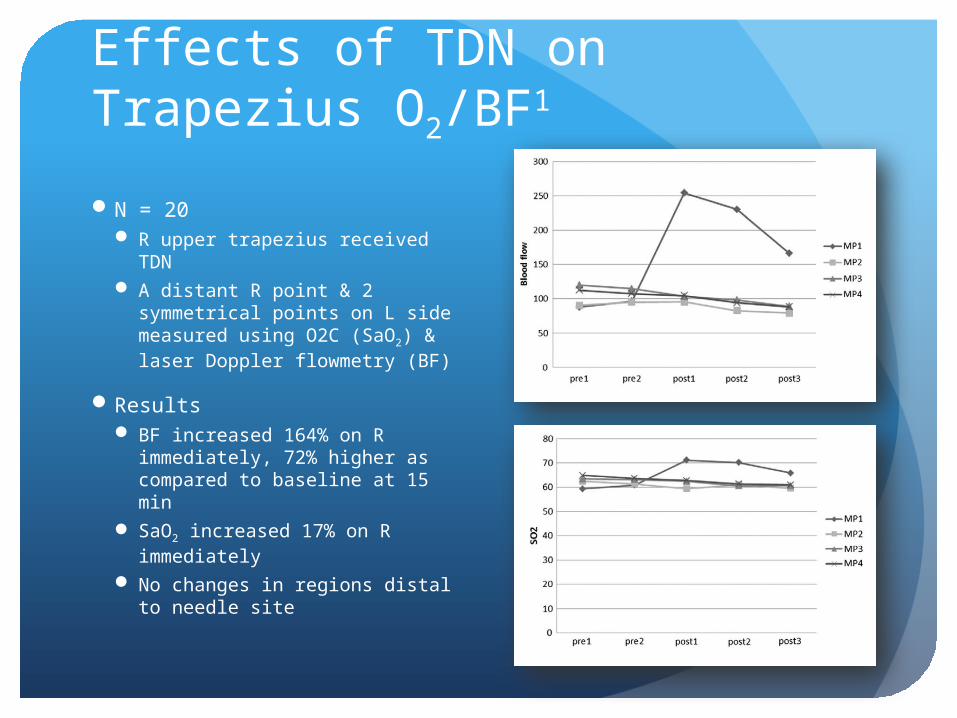
Effects of TDN on Trapezius O2/BF1
N = 20 R upper trapezius received
TDN A distant R point & 2
symmetrical points on L side measured using O2C (SaO2) & laser Doppler flowmetry (BF)
Results BF increased 164% on R
immediately, 72% higher as compared to baseline at 15 min
SaO2 increased 17% on R immediately
No changes in regions distal to needle site

Training
www.kinetacore.com & www.myopainseminars.com Level 1 - 3 day course of lecture, demonstration &
large amount of hands on laboratory work Must be licensed as PT, DC, DO, MD, PA, or nurse
practitioner with a minimum of 1 year practicing Hip, lumbar spine, thigh, c-spine, shoulder, UE/LE
Level 2 – advanced hip/lumbar/UE/LE/c-spine, TMJ/face, t-spine, Completion of L1 & 200 logged TDN tx sessions or
complete of Functional Therapeutics: Application for Dry Needling & 100 logged sessions
Pelvic floor

Montana Practice Act
The Montana Board of Physical Therapy has determined that trigger point dry needling is within the scope of practice for physical therapists. The board has formed a committee to begin the process of setting rules for trigger point dry needling which met for the first time June 30, 2011 & their work continues presently.
Training guidelines – currently drafting (July 2013)
Mountain View PT, Great Northern PT, Professional Therapy Associates
Not within practice act: Idaho, New York, Hawaii, Florida, California, & Pennsylvania. KS/SD?

Billing
Check the payer’s coverage policy
Absent of specific payer policy, the use of CPT code 97140 for the performance of TND should not be utilized97140 – STM, joint mobilization, manipulation,
manual tractionNo code specifically for dry needling If no code exists, report the service using the
appropriate unlisted physical medicine/rehabilitation service or procedure code 97799
ABN for Medicare patients

http://www.apta.org/StateIssues/DryNeedling/

References
1. Cagnie B, Barbe T, De Ridder E, Van Oosterwijck J, Cools A, Danneels L. The influence of dry needling of the trapezius muscle on muscle blood flow and oxygenation. J Manipulative Physiol Ther. 2012;35(9):685-691. doi: 10.1016/j.jmpt.2012.10.005 [doi].
2. Hsieh YL, Yang SA, Yang CC, Chou LW. Dry needling at myofascial trigger spots of rabbit skeletal muscles modulates the biochemicals associated with pain, inflammation, and hypoxia. Evid Based Complement Alternat Med. 2012;2012:342165. doi: 10.1155/2012/342165 [doi].
3. Kietrys DM, Palombaro KM, Azzaretto E, et al. Effectiveness of dry needling for upper-quarter myofascial pain: A systematic review and meta-analysis. J Orthop Sports Phys Ther. 2013;43(9):620-634. doi: 10.2519/jospt.2013.4668 [doi].
4. Maher RM, Hayes DM, Shinohara M. Quantification of dry needling and posture effects on myofascial trigger points using ultrasound shear-wave elastography. Arch Phys Med Rehabil. 2013;94(11):2146-2150. doi: 10.1016/j.apmr.2013.04.021 [doi].
5. Mayoral O, Salvat I, Martin MT, et al. Efficacy of myofascial trigger point dry needling in the prevention of pain after total knee arthroplasty: A randomized, double-blinded, placebo-controlled trial. Evid Based Complement Alternat Med. 2013;2013:694941. doi: 10.1155/2013/694941 [doi].
6. Baldry P. Management of myofascial trigger point pain. Acupunct Med. 2002;20(1):2-10.
7. Shah JP, Danoff JV, Desai MJ, et al. Biochemicals associated with pain and inflammation are elevated in sites near to and remote from active myofascial trigger points. Arch Phys Med Rehabil. 2008;89(1):16-23. doi: 10.1016/j.apmr.2007.10.018 [doi].
8. Kisner C, Colby LA. Therapeutic exercise: Foundations and techniques. F a Davis Company; 2007.