trends in unexpected infant deaths in sheffield
TRANSCRIPT

1121
Child Health
TRENDS IN UNEXPECTED INFANT DEATHSIN SHEFFIELD
ELIZABETH M. TAYLOR JOHN L. EMERY
Wolfson Unit, Department of Paediatrics, University of Sheffield,The Children’s Hospital, Sheffield S10 2TH
Summary A study of 250 post-perinatal deaths inSheffield during the past 8 years has shown
an increased rate of unexpected infant death. This increaseappears to be mainly caused by deaths in children withminor disease in families where the father is either absent or
unemployed. The number of children who die during thecourse of more serious disease continues to fall. The numberof infant deaths from other causes is unchanged.
INTRODUCTION
SINCE 1973, confidential inquiries have been made intoall post-perinatal deaths in Sheffield. The prospective studywhich we report started in April, 1979. In 1973, thepost-perinatal mortality rate in Sheffield was above the UKnational average and equivalent to that of other majorindustrial cities. A programme of increased primary carewas started for selected children and a striking fall in thepost-perinatal mortality rate was seen over the following 5years.l Recently, however, an increase in the number ofunexpected infant deaths in Sheffield has occurred. Afterseveral years of a slow but steady fall, the UK post-perinataldeath rate increased in 1986 entirely because of an increasein the number of deaths registered as unexpected death ininfancy.3 3
It is now generally believed that unexpected death ininfancy (sudden infant death syndrome) is multifactorial. Aspart of our confidential inquiries all deaths are divided intosub-groups related to the possibility of prevention,4 and wereport the trends in incidence that have occurred in thedifferent groups over the past 8 years.
MATERIALS AND METHODS
Sheffield is the fifth largest industrial city in England, with apopulation of approximately 500 000 and over 6000 births eachyear. This study was done in the district health authority, which hasthe same boundaries. Sheffield is unusual, for its size, in thegeographical stability of the population.A confidential inquiry is held on the deaths of all children
between the ages of 1 week and 1 year, except those after which a
parent or guardian is charged with a criminal offence. Deaths arereported from paediatric wards, and by the mortuary technicians forchildren who die outside hospital, and are checked against theweekly returns of the Registrar for Births, Marriages, and Deaths. Aquestionnaire on each child is completed from obstetric andpaediatric records and by family doctors and health visitors; reportsare obtained from the domiciliary midwife and social workers if theyhad been recently involved with the family. The paediatric necropsyreport is obtained: full paediatric necropsies have been done in thesame pathology department throughout the study on all unexpectedinfant deaths. One of the doctors involved in the study visits thehome, usually for 2 hours, about 3 to 4 weeks after the child’s death.Home visits are usually made in the evenings to allow workingfathers to be present. When data collection is complete, a casediscussion is arranged in the family doctor’s surgery for childrenwho died at home, and in the research unit for other deaths. Case
TABLE 1—POST-PERINATAL* DEATHS IN SHEFFIELD 1980-1987 %
*1 week to 1 year of age. UID = unexpected infant death.
discussions are restricted to the professionals actively involved inthe case: observers are discouraged because they inhibit discussion,which is concentrated upon possible contributory factors that led tothe child’s death. This information is used to plan the futuresupport of the family, and to decide on health care when the nextchild is born. After each case discussion, the death is classifiedretrospectively into 6 categories according to necropsy findings andclinical history alone. Group A comprised infants who had acondition with a poor prognosis (eg, congenital abnormality, grossprematurity, or tumour); infants in group B died in the course of atreatable disease (eg, overt infection); group C infants died during amild illness (eg, upper respiratory tract infection); for infants ingroup D no disease was found; group E infants died in an accident;and infants in group F were thought to have died because of overt orconcealed non-accidental injury.
Relevant social factors are also assessed. Family and backgroundfactors are recorded under the following headings: mother’s
upbringing and home background; father’s upbringing and homebackground; domestic and financial problems; housing problems;parents’ health; mother’s intelligence; father’s intelligence; mother’scompetence; father’s competence; level of maternal/infant bonding;competence of other non-professional carers; family crisis; andfailure of communication (a possible 13 factors). Only gross socialfactors are scored (eg, the father being in prison during the child’slife, or family violence or breakdown; mother’s intelligence was onlyrecorded if she had needed special educational provision; in themother’s or father’s background an adverse factor was only scored ifthere was a clear history of violence, a broken family, or if the parenthad been in care as a child). Minor failures of parenting are notrecorded and unemployment is not considered to constitute anadverse factor unless aggravated by other financial problems.The authors have been involved in data collection and case
discussion throughout the study. All cases have been been recentlyreassessed to exclude any progressive bias.
ncan
Fig 1-Post-perinatal deaths in Sheffield, 1980-1987.
Deaths aged 1 week to 1 year 1000 live births ’’3-year rolling means,’. UID =unexpected infant deaths.Broken line shows unemployment rate (%) ’.
1122
RESULTS
From 1979 to 1987,49128 births and 250 post-perinataldeaths were recorded in Sheffield (5-08/1000 births). 103deaths were registered as unexpected death in infancy(2.0/1000 births, see table I.)
6 unexpected post-perinatal deaths which were not
explained by severity of the illness, but were thoughtprobably to be unpreventable because of longstandingdisease, were included in group A; 3 of these children hadserious underlying defects, and 2 had a very low birthweight(< 1000 g) with persistent pulmonary and cerebral damage.Accidental suffocation was thought to be the main probablefactor for 3 deaths, which were included in group E. For 7deaths, active parental intervention was considered by allpresent at the case discussion to be overwhelmingly the mostlikely cause of death, although without appropriate evidencefor legal action, these were placed in group F.
Fig 1 shows post-perinatal death rates and registeredunexpected infant deaths per 1000 live births over the studyperiod: the total post-perinatal mortality rate has remainedsteady, but there has been a progressive increase in thenumber of children dying unexpectedly (designated as
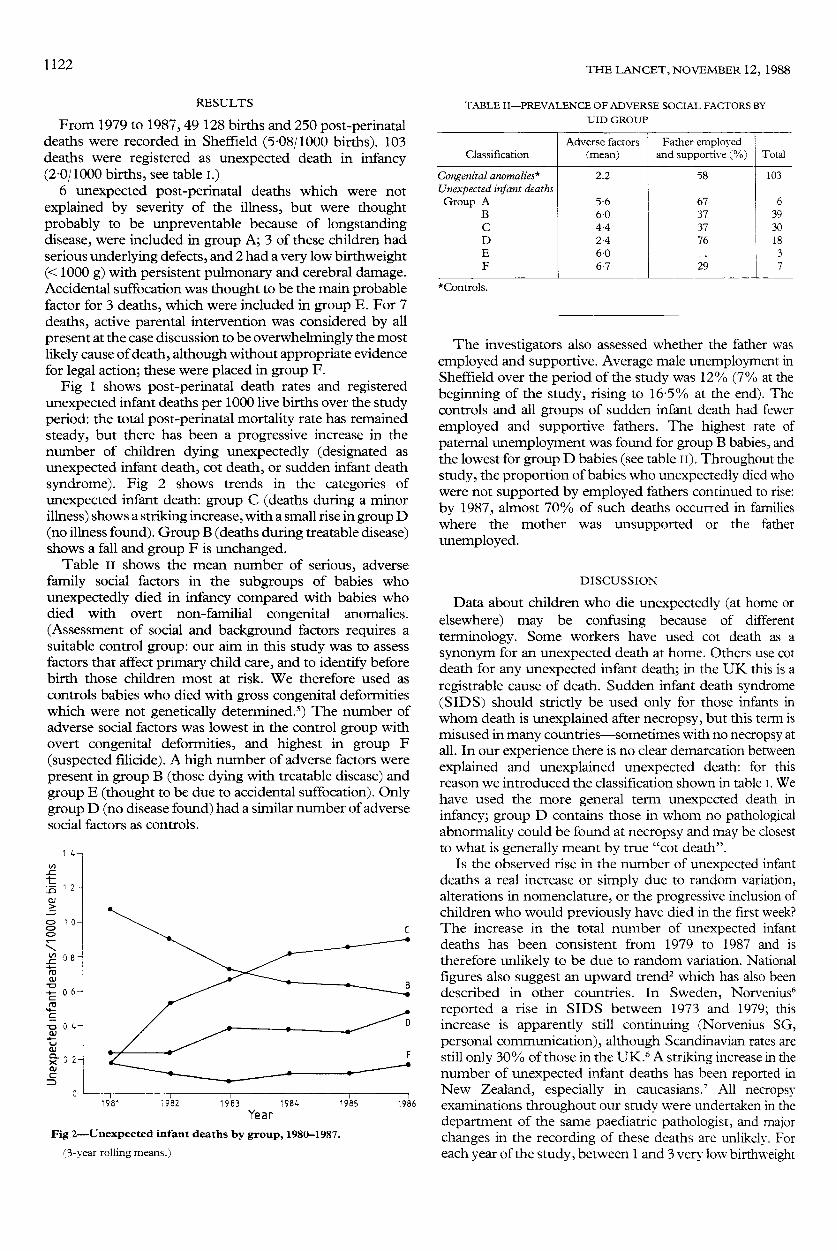
unexpected infant death, cot death, or sudden infant deathsyndrome). Fig 2 shows trends in the categories of
unexpected infant death: group C (deaths during a minorillness) shows a striking increase, with a small rise in group D(no illness found). Group B (deaths during treatable disease)shows a fall and group F is unchanged.
Table II shows the mean number of serious, adversefamily social factors in the subgroups of babies whounexpectedly died in infancy compared with babies whodied with overt non-familial congenital anomalies.
(Assessment of social and background factors requires asuitable control group: our aim in this study was to assessfactors that affect primary child care, and to identify beforebirth those children most at risk. We therefore used ascontrols babies who died with gross congenital deformitieswhich were not genetically determined.5) The number ofadverse social factors was lowest in the control group withovert congenital deformities, and highest in group F
(suspected filicide). A high number of adverse factors werepresent in group B (those dying with treatable disease) andgroup E (thought to be due to accidental suffocation). Onlygroup D (no disease found) had a similar number of adversesocial factors as controls.
-
Fig 2-Unexpected infant deaths by group, 1980-1987.
(3-year rolling means.)
TABLE II-PREVALENCE OF ADVERSE SOCIAL FACTORS BY
UID GROUP
*Controls.
The investigators also assessed whether the father wasemployed and supportive. Average male unemployment inSheffield over the period of the study was 12% (7% at thebeginning of the study, rising to 16-5% at the end). Thecontrols and all groups of sudden infant death had fewer
employed and supportive fathers. The highest rate of
paternal unemployment was found for group B babies, andthe lowest for group D babies (see table II). Throughout thestudy, the proportion of babies who unexpectedly died whowere not supported by employed fathers continued to rise:by 1987, almost 70% of such deaths occurred in familieswhere the mother was unsupported or the father
unemployed.
DISCUSSION
Data about children who die unexpectedly (at home orelsewhere) may be confusing because of different
terminology. Some workers have used cot death as a
synonym for an unexpected death at home. Others use cotdeath for any unexpected infant death; in the UK this is aregistrable cause of death. Sudden infant death syndrome(SIDS) should strictly be used only for those infants inwhom death is unexplained after necropsy, but this term ismisused in many countries-sometimes with no necropsy atall. In our experience there is no clear demarcation betweenexplained and unexplained unexpected death: for thisreason we introduced the classification shown in table I. Wehave used the more general term unexpected death ininfancy; group D contains those in whom no pathologicalabnormality could be found at necropsy and may be closestto what is generally meant by true "cot death".
Is the observed rise in the number of unexpected infantdeaths a real increase or simply due to random variation,alterations in nomenclature, or the progressive inclusion ofchildren who would previously have died in the first week?The increase in the total number of unexpected infantdeaths has been consistent from 1979 to 1987 and istherefore unlikely to be due to random variation. Nationalfigures also suggest an upward trend2 which has also beendescribed in other countries. In Sweden, Norveniusb
reported a rise in SIDS between 1973 and 1979; thisincrease is apparently still continuing (Norvenius SG,personal communication), although Scandinavian rates arestill only 30% of those in the UK.6 A striking increase in thenumber of unexpected infant deaths has been reported inNew Zealand, especially in caucasians.’ All necropsyexaminations throughout our study were undertaken in thedepartment of the same paediatric pathologist, and majorchanges in the recording of these deaths are unlikely. Foreach year of the study, between 1 and 3 very low birthweight

1123
babies have died unexpectedly in infancy, but no upwardtrend has occurred. Has there been a progressive bias ingrading? All data on each individual death has beenreviewed to exclude the possibility of a progressive change inthe criteria used in group classification. Only 3 cases wereconsidered to be wrongly allocated and re-graded; thesewere not all in the same direction. We therefore feel that thetrends are genuine.We found a progressive decline in the number of children
who die unexpectedly in whom treatable terminal diseasewas found at necropsy. This may merely reflect a downwardtrend in infectious disease and inflammatory changes foundat necropsy in childhood deaths (other than those due togross anomalies) during the last 40 to 50 years, or may be dueto the Sheffield scoring system and intervention
programme. (All babies born in Sheffield are scored for riskof unexpected death in infancy: this system predicts group Bdeaths far more effectively than deaths in other groups,8 andenables increased health visitor care. Family doctors are alsoinformed because these deaths are the most likely to bepreventable.)The epidemiological characteristics of the different
groups will be presented elsewhere. However, two aspectsstand out: adverse social factors in the family, and
unemployment.In the assessment of adverse social, family, and
background factors we recorded only those which wereconsidered at the case discussion to be clearly outsideaccepted normal limits: minor failures of parenting thatoccur in all families were not recorded. Nevertheless, out of apossible total of 13 adverse social factors, the families of 3groups (B, E, and F) had a mean score of 6 or more. Onlygroup D (classic "cot death") showed no difference from thecontrols. Families with a group C death (the group whichshowed the most striking rise between 1980 and 1987) hadtwice as many adverse social factors as controls. When wereviewed group C deaths we found that many of the familiesin this group seemed to belong to a small subculture withinwhich morbidity, poverty, excess smoking and alcoholconsumption, and a fatalistic outlook predominate. Thesebabies would also have been at greater risk because of anadverse intrauterine environment.The employment status of both the mother and her
partner have been found to be important in some scoringsystems for risk of cot death.9 In Sheffield, the increase in cotdeaths has paralleled an increase in the rate of
unemployment (fig 1). We cannot show a direct causalrelation: indeed, we have anecdotal evidence of individualfamilies where the presence of a father at home, after loss ofan often poorly paid job, has improved child care. However,the proportion of unexpected infant deaths in families wherethe father is either absent or unemployed has steadilyincreased.Many unexpected infant deaths are mutifactorial in
origin; possibilities for prevention have social, political, andeducational as well as medical implications.
Correspondence should be addressed to E. M. T.
REFERENCES
1. Carpenter RG, Gardner A, Jepson M, et al Prevention of unexpected infant death.evaluation of the first seven years of the Sheffield intervention programme Lancet1983; i: 723-27.
2. Office of Population Censuses and Surveys. OPCS Monitor- DH3 88 1 London HM
Stationery Office, 1988.
3. Limerick S Sudden infant death cause for concern Health Visitor 1988, 61: 233-34.4 Tay lor EM, Emery JL, Two year study of the causes of post perinatal deaths classified
in terms of preventability Arch Dis Child 1982, 57: 668-735. Taylor EM, Emery JL Family and community facrors associated with infant deaths
that might be preventable Br Med J 1983, 287: 871-746 Norvenius SG, Sudden infant death syndrome in Sweden 1973-1977 and 1979, Acta
Paediatr Scand 1987, 333 suppl 123.
7 Hassall IB Sudden infant death syndrome a serious New Zealand health problemNZ Med J 1986, 99: 233-34
8 Tay lor E.M. Emery JL. Carpenter RG. Identification of children at risk of unexpecteddeath Lancet 1983, ii 1033-34
9 Peters TJ, Golding J Prediction of sudden intant death syndrome an independentevaluation of form scoring methods Stat Med 1986, 5: 113-26
Hospital Practice
MICROBIOLOGICAL LOOK AT URODYNAMICSTUDIES
S. R. PAYNE1S. T. MCKENNING2
L. J. PEAD3
A. G. TIMONEY1D. DEN HOLLANDER1
R. M. MASKELL3
Departments of Urology1 and Gynaecology,2 and Public HealthLaboratory,3 St Mary’s Hospital, Portsmouth
Summary Urine samples were cultured for aerobic,fastidious, and anaerobic bacteria in 88
patients (66 F, 22 M) before and after standard urodynamicinvestigations. 37 of 42 women with detrusor instability, and14 of 17 women with stress incontinence, had evidence ofbacteriuria with aerobic or fastidious bacteria before
investigation, as did 6 of 13 men with bladder outflowobstruction. 8 men (36%) acquired bacteriuria with aerobicbacteria after investigation, compared with 10 women
(15%). Recalcitrant, irritative urinary symptoms in womenmay be caused by an underlying infection, the urodynamicchanges being secondary. In men who have urodynamicstudies, antibiotic prophylaxis should be considered.
INTRODUCTION
URODYNAMIC studies are widely used in the
management of male and female patients with urinarysymptoms. Indications for such tests, their interpretation,and their implications for treatment have been widelydiscussed, but little attention has been paid to the
microbiological aspects. Any procedure that involvesinstrumentation of the urinary tract is liable to introduceorganisms into the bladder; how often does bacteriuriafollow urodynamic studies? Furthermore, infection-whether of the bladder or of the urethra and adjacentstructures-could be a cause of the symptoms that
prompted such studies, and may also be responsible forurodynamic findings of detrusor instability, sensory
frequency, and even bladder neck obstruction, should theinfection around the urethra be sufficiently severe andlongstanding as to cause fibrosis and constriction. The aimof this study was to determine the prevalence of bacteriuria(whether with aerobic or fastidious2 bacteria) before, and theincidence of bacteriuria after, standard urodynamicinvestigation.
MATERIALS AND METHODS
88 patients who had been referred for outpatient urodynamicinvestigations were studied. Patients who had had urethral