treatment with ventricular assist devices
TRANSCRIPT
WHEN IT’S LATE
BUT NOT “TOO LATE” IN
HEART FAILURE:Ventricular Assist Devices
Mariell Jessup MD FESC, FAHA
Professor of Medicine
University of Pennsylvania
Philadelphia, Pennsylvania

Presenter Disclosure InformationWHEN IT’S LATE
BUT NOT “TOO LATE” IN HEART FAILURE:
Ventricular Assist Devices
I will discuss off label use or investigational use in my presentation.
I have financial relationships to disclose:
Employee of: University of Pennsylvania
Consultant for: none
Stockholder in: none
Research support to my program from:
Thoratec, HeartWare
Honoraria from: none
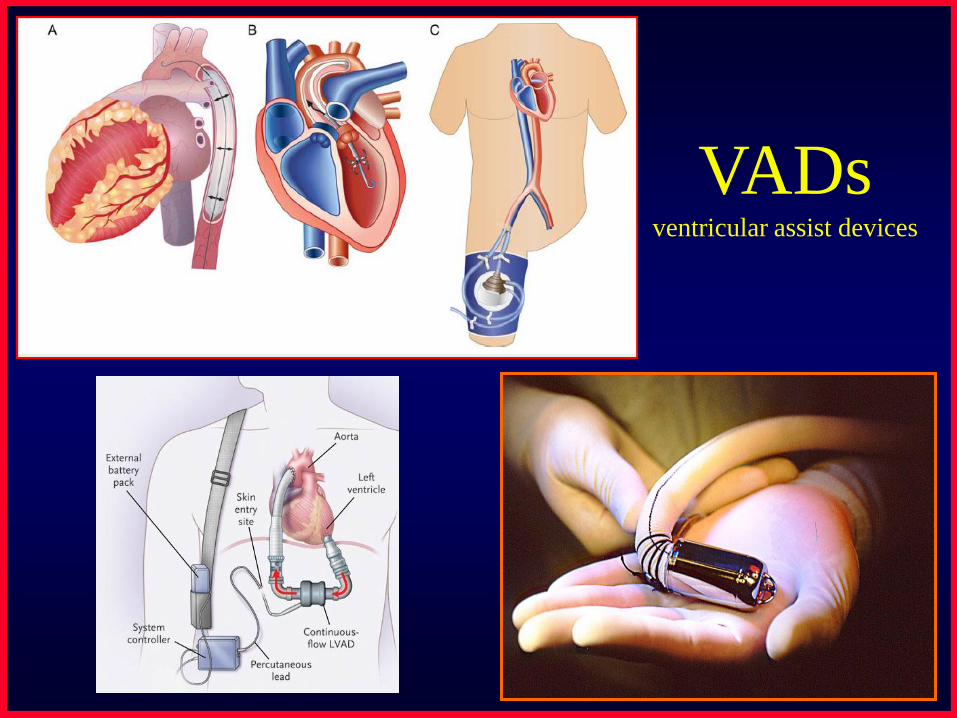
VADsventricular assist devices
Step #1:Evaluating the patient and
the full extent of the heart failure syndrome
Step # 2:The choice of VADsthe right pump for the right patient
• The good news
– Lots of pumps to choose from
• The bad news
– Limited availability at most hospitals
– Comparative trials infrequent
– Physician preference clouds a lot of the discussion
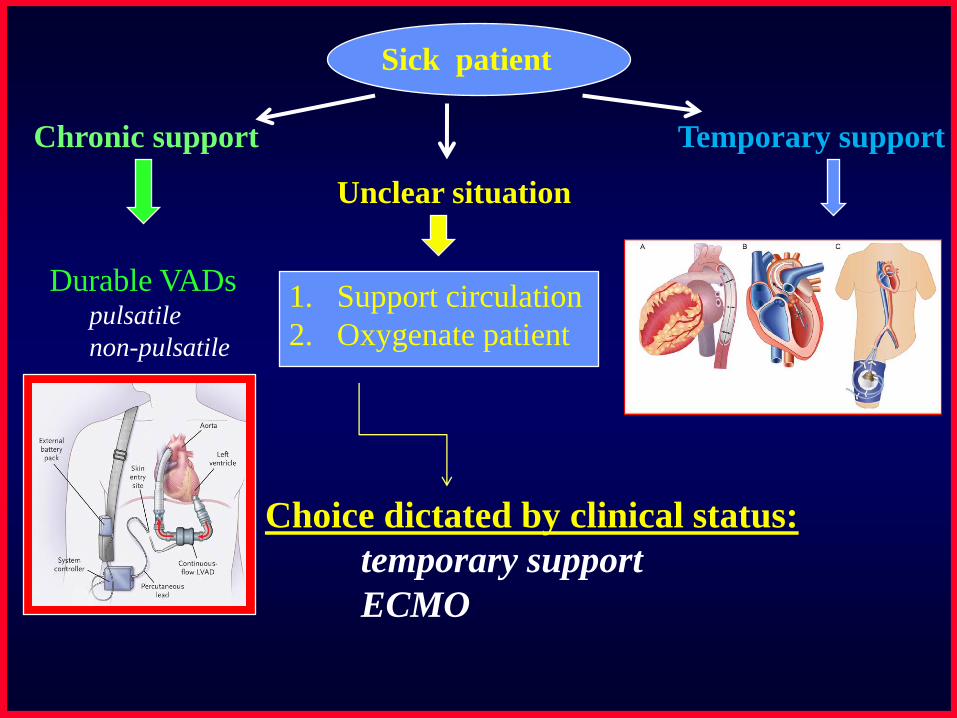
Sick patient
Temporary supportChronic support
Unclear situation
1. Support circulation
2. Oxygenate patient
Choice dictated by clinical status:
temporary support
ECMO
Durable VADspulsatile
non-pulsatile

Temporary support:Background
• Cardiogenic shock
– Compromise of cardiac output leading to end-
organ hypo-perfusion
– Complex cascade of end-organ dysfunction
combined with activation of inflammatory
pathways
– Complicates about 7% of ST segment elevation
MI1 and about 2.5% of non-ST segment
elevation MI2
1Holmes DR Jr, Berger PB, et. al. Circulation 1999; 100:2067–2073.2Hasdai D, Harrington RA, et. al JACC 2000;36:685–692.

Who would benefit from temporary support?
Acute cardiogenic shock
Acute myocardial infarction
Acute myocarditis
Complications post MI
Papillary muscle rupture
Ventricular septal defect
Post cardiotomy failure
Acute on chronic (end-stage) heart failure
Electrical “storm”, or post-VT ablation
Drug overdose with myocardial depression
HypothermiaWindecker S. Curr Opin Crit Care 13:521–527. 2007

The pump choices for
the acutely ill patient.
• Intra-aortic balloon pump
• Extracorporeal membrane oxygenation
(peripheral cardio-pulmonary bypass)
• Tandem Heart
• Impella
• Traditional ventricular assist devices
• Total Artificial Heart
Percutaneous
Surgical

Advantages of Percutaneous Device
• Placed quickly
• Avoid need for “open surgery”
• Placed at many centers even those without
VAD or transplant program
• More easily removed in setting of recovery
• Placed by interventional cardiologists and
surgeons
• Allow for recovery or transport to another
center

Disadvantages of Percutaneous Devices
Bleeding
Limited to left ventricular support (except
ECMO)
Not for biventricular support
Not for RV support (?yet)
Ventricular arrhythmias
Ischemic limb
Unable to mobilize or rehab
Sepsis

ECMO
http://www.emedicine. medscape.com/article/904996-overview

ECMO - Advantages
Cardio-pulmonary bypass
Can be placed peripherally (without
thoracotomy)
The only percutaneous option for biventricular
support
The only option in the setting of lung injury

ECMO - Disadvantages
• Requires trained team and equipment
availability on-site and early in resuscitation
• Higher risk of infection, bleeding and
vascular injury

The Data - ECMO
• Several centers have reported their
experience with ECMO in the setting of
CPR/Cardiogenic shock
– Survival rates of 31 to 63%
Hoefer D, Ruttmann E, et. al. Ann Thorac Surg 2006;82:28 –34
Chen Y, Chao A, et. al. JACC 41:2, 2003: 197-203
Linden H, Wiklund L. et.al. Scand Cardiovasc J.2009

Intra-aortic Balloon Pump
IABP - Advantages
• Easily placed in the catheterization
laboratory or operating room
• Improves coronary perfusion
• Decreases afterload
• Decreases myocardial oxygen demand
• Can transport patient to another center
• Established technology that is widely
available
IABP Disadvantages
• Does not directly support cardiac output
• Limited support in the setting of tachycardia
and arrhythmia
• May be less effective in older patients with
significant atherosclerosis in aorta

Impella

Impella Advantages
• Small rotary pump
• Can be placed percutaneously from femoral
artery across aortic valve without need of
trans-septal puncture or venous access
• Can be easily removed

Impella Disadvantages
• Hemolysis – although not felt to be
clinically relevant
• Provides partial cardiac output support – up
to 2.5 liters/minute in percutaneous model
• Difficult to place in setting of severe
peripheral vascular disease

Impella: Datathe ISAR-SHOCK trial
Seyfarth M, Sibbing D., et. al. JACC 2008;52:1584–8
Improved cardiac power index No difference in survival

Tandem Heart
Tandem Heart Advantages
• Can be placed easily in the catheterization
laboratory
• Can supply up to 5 l/min flow
• Can be easily removed

Tandem Heart Disadvantages
• Requires trans-septal placement
• Difficult to place in setting of severe
peripheral vascular disease
Tandem Heart Data
• Compared to IABP in acute MI with shock
(n=41) (Single Center)
– Improved cardiac power index, decreased
lactate, improved renal function as compared to
IABP
– No difference in 30 day survival and more
complications in Tandem Heart group
Thiele H, Sick P, et al. Eur Heart J 2005; 26:1276–1283.

Tandem Heart Data
• Multi-center trial comparing Tandem Heart
and IABP in acute MI with shock (N=42)
– Tandem Heart improved cardiac output,
decreased PCWP and increased mean arterial
pressure as compared to IABP
– No difference in 30 day survival
– Similar complication rates
Burkhoff D, Cohen H. Amer Heart J, 152:3, September 2006.
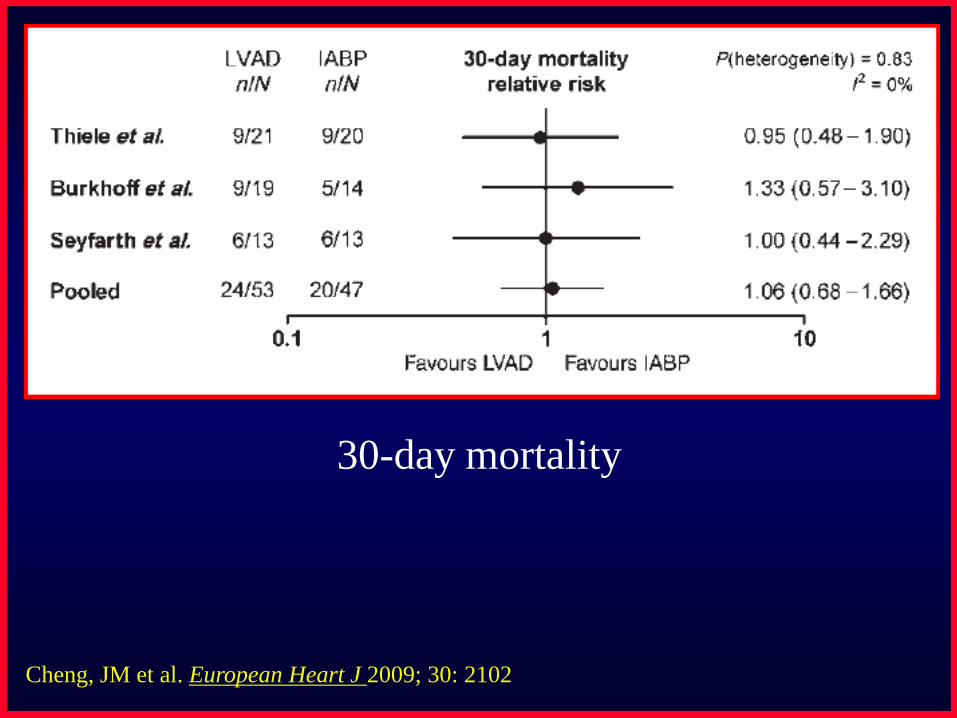
Cheng, JM et al. European Heart J 2009; 30: 2102
30-day mortality

Cheng, JM et al. European Heart J 2009; 30: 2102

Limitations
• Studies done to date have been small and at
a limited number of centers
• Inclusion and exclusion criteria are
challenging in the setting of sudden shock
• Populations studied have been somewhat
heterogeneous including acutely and
chronically ill patients
• The data for “prophylactic use” to support
procedures is very encouraging
Conclusions: Percutaneous devices
• Circulatory support in the setting of
cardiogenic shock improves outcomes
• Most centers do not have access to surgical
ventricular assist devices
• Percutaneous assist devices play an
important role in providing rapid support in
cardiogenic shock and support for high risk
procedures and can be used at many centers
• Additional studies are needed to define the
role of these important tools

Sick patient
Temporary supportChronic support
Unclear situation
1. Support circulation
2. Oxygenate patient
Choice dictated by clinical status:
temporary support
ECMO
Durable VADspulsatile
non-pulsatile

Blood Pump TechnologyBlood Pumps
Pulsatile TAHRotary
• Thoratec PVAD
• HeartMate XVE
• WorldHeart, Novacor
•Arrow LionHeart
• Thoratec IVAD
•AbioMed, AB5000
• Berlin Heart EXCOR
• Medos HIA
• WorldHeart, HeartSaver
White font = FDA/CE Orange font = CE Mark(* US clinical trial)
Yellow font = R or D phase
Axial
• MicroMed DeBakey*
• Berlin Heart INCOR
• Jarvik 2000
• HeartMate II
•Circulite
•Impella
Centrifugal
• VentraCor, VentrAssist
• HeartMate III
. Terumo, DuraHeart
• HeartWare
• WorldHeart/Levacor
• Arrow, CorAide
•Levotronics
•Tandem Heart
• Abiomed, AbioCor
• CardioWest
Red font -No longer available
Issues in the implantation of
durable VADs
• Proper selection of patients
– Recognizing the patient who is “too sick”, with end-
organ damage
– Recognizing the patient who is too debilitated or
malnourished
– Recognizing the patient who needs bi-ventricular
support
• Timing of surgery
– Especially important in the elderly “destination”
patient

HFA/ESC: Advanced heart failure

HFA/ESC: Advanced heart failure

1. Critical Cardiogenic Shock: low BP unresponsive to support, compromised
organ perfusion.
2. Progressive Decline: not in imminent danger but worsening despite inotropic
support, with declining renal function, nutrition, ambulation, other.
3. Stable but Inotrope dependent: unable to be weaned from inotropic support.
4. Recurrent advanced heart failure: recurrent congestion despite good
maintenance, needing repeated interventions beyond escalation of oral
diuretics.
5. Exertion intolerant: comfortable at rest without obvious fluid overload but
limited activities of daily living (ADL).
6. Exertion limited: comfortable at rest and with ADL but meaningful activity
limited.
7. Advanced NYHA Class 3.
Clinical Patient Profiles
Stevenson et. al. JHLT 2009;28: 535
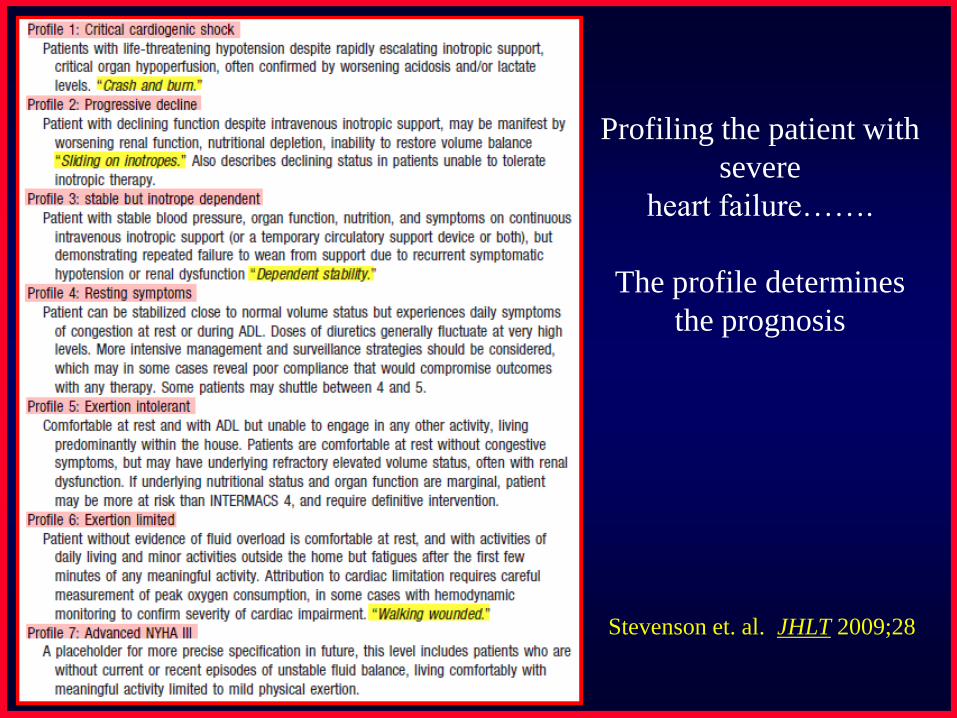
Profiling the patient with
severe
heart failure…….
The profile determines
the prognosis
Stevenson et. al. JHLT 2009;28
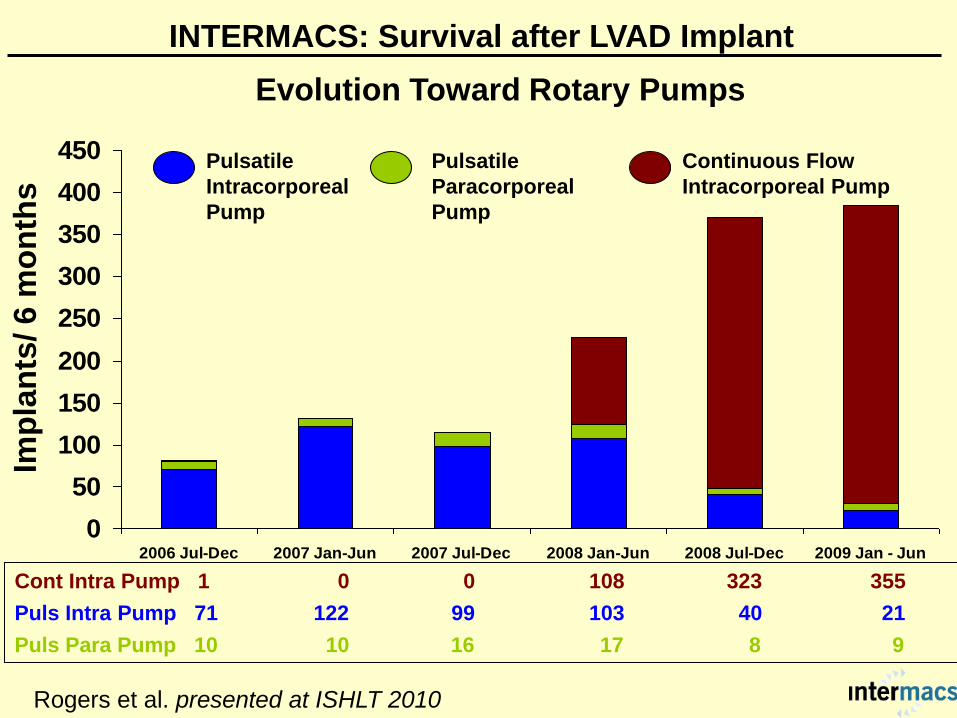
Evolution Toward Rotary Pumps
INTERMACS: Survival after LVAD Implant
0
50
100
150
200
250
300
350
400
450
2006 Jul-Dec 2007 Jan-Jun 2007 Jul-Dec 2008 Jan-Jun 2008 Jul-Dec 2009 Jan - Jun
Pulsatile
Intracorporeal
Pump
Continuous Flow
Intracorporeal Pump
Imp
lan
ts/ 6 m
on
ths
Cont Intra Pump 1 0 0 108 323 355
Puls Intra Pump 71 122 99 103 40 21
Puls Para Pump 10 10 16 17 8 9
Pulsatile
Paracorporeal
Pump
Rogers et al. presented at ISHLT 2010

Early Constant
Risk Factor Hazard ratio p-value Hazard ratio p-value
Female 1.71 0.04 --- ---
Age (older) 1.141 0.006 1.131 0.008
Previous CABG 2.71 <0.0001 --- ---
Previous Valve Surgery 1.99 0.01 --- ---
Dialysis (current) 2.45 0.01 --- ---
INR (higher) 1.492 0.003 --- ---
Ascites 2.32 0.002 --- ---
RVEF: Severe --- --- 2.33 0.04
RA Pressure (higher) 1.523 0.02 --- ---
Cardiogenic Shock 1.98 0.003 --- ---
BTC or DT --- --- 3.00 0.01
Pulsatile pump --- --- 3.02 0.001
1 Hazard ratio denotes the increased risk with a 20 year increase in age
2 Hazard ratio denotes the increased risk with a 1.0 increase in INR
3 Hazard ratio denotes the increased risk of a 10-unit increase in RA pressure
INTERMACS: Survival After LVAD Implant
Adult Primary Intracorporeal LVADs (n=1366)
Rogers et al. presented at ISHLT 2010


Patient thresholds for LVAD insertion parallel
objective survival and functional data. HF patients
would be receptive to referral for discussion of
LVAD by the time expected mortality is
12 months and activity remains limited to 1 block.
“one year or 1 block”

Sick patient
Temporary supportChronic support
Unclear situation
1. Support circulation
2. Oxygenate patient
Choice dictated by clinical status:
temporary support
ECMO
Durable VADspulsatile
non-pulsatile