treatment with inhaled corticosteroids in asthma is too often discontinued
TRANSCRIPT

ORIGINAL REPORT
Treatment with inhaled corticosteroids in asthmais too often discontinuedy
Nancy S. Breekveldt-Postma PhD1, Jeroen Koerselman MD, PhD1, Joelle A. Erkens PhD1,Thys van der Molen MD, PhD2, Jan-Willem J. Lammers MD, PhD3
and Ron M. C. Herings PhD1,4* for the CAMERA Study Groupz
1PHARMO Institute, Utrecht, The Netherlands2Department of General Practice, University Medical Center Groningen, Groningen, The Netherlands3Department of Pulmonary Diseases, University Medical Center Utrecht, Utrecht, The Netherlands4Department of Health Policy & Management, Erasmus Medical Center, Rotterdam, The Netherlands
SUMMARY
Purpose To study persistence with inhaled corticosteroids (ICS) and its determinants in asthma-patients.Methods From the PHARMO database, asthma-patients (age< 35 years) with a first dispensing for ICS in 1999–2002and� 2 dispensings in the first year were included. Persistence during the first year was defined as the number of days fromstart to time of first failure to continue renewal of the initial ICS. Potential determinants of persistence were assessed atICS-start and 1 year before.Results The study-cohort included 5563 new users of single ICS and 297 of fixed-combined ICS. Less than 10% of patientsusing single ICS and 15% of patients using fixed-combined ICS were persistent at 1 year. Similar persistence-rates wereobservedwhen stratified for age (children/adolescents: 0–18 years and adults: 19–34 years). Increased persistencewith singleICS was observed with the type of ICS (budesonide), prescriber (specialist), prior use of long-acting beta-agonists, previoushospitalization for asthma, metered-dose inhaler, low starting-dose and once-daily dosing regimen at start. Persistence withfixed combined ICS-treatment increased with younger age and was decreased in patients having high starting-dose of ICSand prior use of antibiotics.Conclusion New users of both single and fixed combined ICS have alarming low persistence rates with ICS-treatment inthe first year of follow-up. Persistence was mainly related to patient factors, such as severity of disease, and totreatment-related factors, such as once-daily dosing frequency. Copyright # 2008 John Wiley & Sons, Ltd.
key words—adherence; asthma; inhaled corticosteroids; linkage; persistence; pharmacoepidemiology
Received 1 August 2007; Revised 10 December 2007; Accepted 11 December 2007
pharmacoepidemiology and drug safety 2008; 17: 411–422Published online 21 January 2008 in Wiley InterScience (www.interscience.wiley.com) DOI: 10.1002/pds.1552
*Correspondence to: Dr R. M. C. Herings, PHARMO Institute, P.O. Box 85.222, 3508 AE Utrecht, The Netherlands.E-mail: [email protected] of Interest: ALTANA Pharma bv. had no role in study design, in the collection, analysis and interpretation of data, in the writing ofthe report or in the decision to submit the report for publication. As a research organization, the PHARMO Institute has performedprotocolled studies for Pfizer, Altana, Boehringer Ingelheim and GSK. N. S. Breekveldt-Postma, J. Koerselman, J. A. Erkens and R. M. C.Herings have no other competing interests to declare. J-W. J. Lammers has received several non-restricted research grants from differentpharmaceutical companies. T. van der Molen has participated as a speaker in several conferences financed by ALTANA, GSK, AstraZenecaand participated in advisory boards ofMerck, AstraZeneca and ALTANA. He also received a research grant of EUR 84 000 fromALTANA in2005.zMembers listed in the Appendix.
Copyright # 2008 John Wiley & Sons, Ltd.

INTRODUCTION
Inhaled corticosteroids (ICS) are considered to be thecornerstone of asthma treatment. Treatment with ICShas been shown to be associated with a reduction in thefrequency and severity of exacerbations, to preventadmissions to hospitals and to decrease the risk of deathfrom asthma.1–7 Furthermore, improved adherencewith ICS has also been associated with decreasedasthma-associated morbidity and mortality.4,8–10 Inspite of this potential and the chronic state of thedisease, several studies have shown that adherencewithICS-treatment is low, ranging from 10% to 70%.1,11–13
A variety of different factors that relate directly topatients characteristics and treatment regimen influ-ence adherence with ICS. These factors are complexand involve psychosocial, social and medical issuesincluding fear of potential side effects (e.g. impairedgrowth in children, decreased bone mineral density),experience of side effects (like hoarseness, candidia-sis) and complexity of treatment regimens (e.g.multiple daily dosing).2,11–18
In addition to single ICS-treatments, fixedcombinations of ICS and long acting beta-agonists(LABA) have been developed for the treatment ofasthma, in order to provide convenience of therapy forpatients requiring treatment of both airway inflam-mation and smooth muscle dysfunction at the sametime.19–21 The use of a single device including bothtypes of drugs allows a greater concentration of bothmedications to reach the target cells in the airways,and may potentially offer an increased opportunity forsynergistic interaction.22,23 In addition, it is assumedthat the application of a single device may increaseadherence with the prescribed asthma medicationthrough more convenient treatment administration.However, at this point, only one study has beenperformed so far indicating that the combined deviceincreased ICS refill persistence compared withpatients using two separate inhalers.15
Several studies have been published on potentialdeterminants of adherence with inhaled corticosteroidtreatment in patients with asthma.11,12,15,24–29 However,the studied determinants were quite different among thestudies, and in some cases, the populations studied hadsome limitations, or the studies concerning dosefrequency issueswere performed a long time ago.26,28,29
Therefore, the aim of the present study was toinvestigate adherence in terms of persistent usewith inhaled corticosteroid treatment and its determi-nants in patients with asthma in current clinicalpractice, both for single ICS-treatment and fixedcombined ICS-treatment.
METHODS
Setting
Data were obtained from the PHARMO RecordLinkage System (PHARMO RLS), which includes,among other databases, the drug-dispensing recordsfrom community pharmacies and hospital dischargerecords of more than two million community-dwellinginhabitants of 40 demographically defined areas inThe Netherlands. For all residents, the computerizeddrug-dispensing histories contain data concerningthe dispensed drug, type of prescriber, dispensing date,dispensed amount, prescribed dose regimens and thelegend duration of use (dispensing length). All drugsare coded according to the Anatomical TherapeuticChemical (ATC) Classification. The hospital recordsinclude detailed information concerning the primaryand secondary diagnoses, procedures and dates ofhospital admission and discharge. All diagnoses arecoded according to the International Classification ofDiseases, Ninth Revision, Clinical Modification(ICD-9-CM). For a detailed description of thedatabase, we refer to the previous work.30
All data obtained from the PHARMO RLS werewithout identifying patient information. Therefore,and according to the national guidelines involved, forthis study, we were not obliged to obtain approval byan ethics committee or patient’s informed consent.
Cohort definition
The study population included all patients with atleast one dispensing for ICS between 1 January 1999and 31 December 2002. The types of single andfixed combined ICS included in the studycomprised beclomethasone (ATC-code: R03BA01),budesonide (ATC-code: R03BA02), fluticasone (ATC-code: R03BA05), salmeterol/fluticasone (ATC-code:R03AK06) and formoterol/budesonide (ATC-code:R03AK07). The date of the first ICS-dispensing wasconsidered as the cohort entry date and the type of ICSprescribed was defined as the index drug. Patients didnot use ICS for at least 1 year before the cohort entrydate. Further, patients had to be registered in thePHARMO database for at least 1 year before and1 year after the cohort entry date.
To increase the likelihood that patients receivedICS for the treatment of asthma, only patients below35 years of age at the cohort entry datewere included inthe study.12 In addition, patients had at least onedispensing for other drugs with a labelled indication ofasthma (ATC-code: R03) in the year before, or at the
Copyright # 2008 John Wiley & Sons, Ltd. Pharmacoepidemiology and Drug Safety, 2008; 17: 411–422DOI: 10.1002/pds
412 n. s. breekveldt-postma ET AL.

cohort entry date, and at least one refill for ICS in thefirst year of treatment to ensure that only patientstreated for chronic respiratory disease were includedin the study. Patients were excluded from the cohort ifthey used nebulizers as ICS-administration form asthese include a limited and selective group of patients.In addition, patients with a hospitalization foremphysema (ICD-9-CM: 492), chronic bronchitis(ICD-9-CM: 491) or chronic airway obstruction(ICD-9-CM: 496) were excluded from the study cohort.
Persistence with ICS
The dispensing patterns were ascertained for eachpatient in the first year after the index dispensing. For
each dispensing, the legend duration of use wascalculated by dividing the number of units dispensedby the number of units to be used per day as defined inthe pharmacies. All dispensings were subsequentlyconverted into treatment episodes of consecutive useof ICS based on the method of Catalan (seeFigure 1).31 Patients were considered persistent withtheir initial ICS-therapy until the time of first failure tocontinue renewal of ICS. The permissible gap betweentwo consecutive dispensings was set at half theduration of the former dispensing or 7 days, whicheverwas greater. In case the period between twodispensings exceeded the permissible gap, the patientwas considered to discontinue treatment. Persistencewas defined as the number of days from the first
Figure 1. The concept of episodes of drug use and persistence with treatment (from Catalan)31
Copyright # 2008 John Wiley & Sons, Ltd. Pharmacoepidemiology and Drug Safety, 2008; 17: 411–422DOI: 10.1002/pds
persistence with inhaled corticosteroids-treatment in asthma 413

dispensing date to the time of first failure to continuerenewal of the initial ICS.In all cases, the treatment episode ended when a
dispensing for an ICS other than the index drug wasfilled during the first episode. In addition, for patientscontinuously treated during the follow-up period, theduration of treatment was censored after 1 year.
Outcome definition
The persistence with ICS-treatment was defined as thenumber of days from the index date to the time of firstfailure to continue renewal of ICS (i.e. the duration ofthe first episode) in 1 year. One-year persistence ratesfor ICS were defined as the percentage of patients thatused ICS for at least 365 days.32
Determinants of persistence
Potential determinants of persistence with ICS-treatment were based on previous persistence studiesand included gender, age, year of start ICS, type ofprescriber, type of ICS, inhaler type, initial dose anddosing frequency at start ICS.12 All these potentialdeterminants were determined at the cohort entry date.In the year prior to the cohort entry date, proxies forseverity of asthma were assessed as possibledeterminants for persistence with ICS. These markersincluded previous hospitalizations for asthma andprior use of drugs with a labelled indication of asthma,as described by others.4,5
The dose of ICS was expressed as a fraction ofWHO’s defined daily dose (DDD equivalents orDDDeq). The defined daily doses for the different ICSwere 800mg for beclomethasone and budesonide. Thesame DDD was used for formoterol/budesonide. TheDDD according to the WHO for fluticason is 600mg,however, because of available formulations the DDDused in clinical practice is 500mg and this was used inthe present study. This dose was also applied for thefixed combination salmeterol/fluticasone. The dailydose for patients aged 12 years or younger wasdefined as two-third of the dose for adults.33 DDDeqswere estimated by dividing the prescribed anddefined daily dose. For example, the DDDeq of aprescribed daily dose of 1000mg beclomethasone witha defined daily dose of 800mg is 1000/800¼ 1.25DDDeq.The use of drugs with a labelled indication of
respiratory diseases (ATC-code: R03) included short-acting beta-agonists (ATC-code: R03AC minusR03AC12 and R03AC13), long-acting beta-agonists(ATC-code: R03AC12 and R03AC13), systemic
sympathicomimetics (ATC-code: R03C), cromogly-cates (ATC-code: R03BC), parasympathicolytics (ATC-code: R03BB), xanthine-derivatives (ATC-code:R03DA), leukotriene receptor antagonists (ATC-code:R03DC) and fixed combinations of beta-agonists andparasympathicolytics (ATC-codes: R03AK03 andR03AK04).
Other related co-medication commonly used duringtreatment of exacerbations included antihistamines(ATC-code: R06A), mucolytics (ATC-code: R05CB),coughing agents (ATC-code: R05D), nasal prep-arations (ATC-code: R01A), oral corticosteroids(ATC-code: H02AB) and antibiotics (ATC-code: J01).
Analyses
Baseline characteristics of new ICS users weredetermined and frequency distributions are presented.
Survival functions describing persistence withICS treatment over time were computed usingKaplan–Meier survival analyses, separately for singleand fixed combined ICS-treatment. Crude and multi-variate analyses to identify independent determinantsof 1-year persistence with ICS-treatment wereconducted using Cox’s proportional hazard analyses.Variables potentially associated with 1-year persist-ence in the crude analyses, and related to asthma, wereincluded in the multivariate analyses. Analyses wereperformed separately for single and fixed combinedICS-treatment. Statistical significance was defined atan alpha level of 0.05.
Stratified analyses were performed stratifiedfor children/adolescents (<19 years) and adults(19–34 years). Kaplan–Meier survival analyses andCox’s proportional hazard analyses were performedfor both age groups.
All data were analysed using SAS programmesorganized within SAS Enterprise Guide version 2.0(SAS Institute Inc., Cary, NC, USA) and conductedunder UNIX using SAS version 8.2.
RESULTS
A total of 5860 patients met the inclusion criteria ofour study. Of these patients, 5563 were new usersof single ICS-treatment (1507 beclomethasone, 903budesonide and 3153 fluticasone) and 297 were newusers of fixed combined ICS-treatment (228 ofsalmeterol/fluticasone and 69 of formoterol/budeso-nide). Patient characteristics are presented in Table 1.About one third of the patients receiving newtreatment with single ICS were 0–4 years old andanother 30% of the patients were 19–34 years of age.
Copyright # 2008 John Wiley & Sons, Ltd. Pharmacoepidemiology and Drug Safety, 2008; 17: 411–422DOI: 10.1002/pds
414 n. s. breekveldt-postma ET AL.

Table 1. Patient characteristics at baseline for new users of inhaled corticosteroids for asthma in the period 1999–2002
Characteristic Single ICS-treatmentN¼ 5563
Fixed combinationof ICS-treatment
N¼ 297
n % n %
GenderMale 2697 48.5 127 42.8Female 2866 51.5 170 57.2
Age group (in years)0–4 1684 30.3 10 3.45–8 860 15.5 20 6.79–14 839 15.1 44 14.815–18 420 7.5 39 13.119–34 1760 31.6 184 62.0
Year of start ICS1999 1512 27.2 10 3.42000 1430 25.7 31 10.42001 1399 25.1 119 40.12002 1222 22.0 137 46.1
Type of ICS at startBeclomethasone 1507 27.1 — —Budesonide 903 16.2 — —Fluticasone 3153 56.7 — —Salmeterol/fluticasone — — 228 76.8Formoterol/budesonide — — 69 23.2
Prescriber at startGeneral practitioner 4826 86.8 187 63.0Pulmonologist 89 1.6 44 14.8Pediatrician 343 6.2 18 6.1Specialist, other 305 5.5 48 16.2
Inhaler type at startMetered-dose 2863 51.5 — —Dry-powder 2700 48.5 297 100
Daily dose at start (DDDeq)0.01–0.74 2919 52.5 41 13.80.75–1.24 1777 31.9 190 64.0�1.25 867 15.6 66 22.2
Dosing frequency at startOnce daily 791 14.2 33 11.1Twice daily 4276 76.9 247 83.2>Twice daily 302 5.4 11 3.7Undefined 194 3.5 6 2.0
One year prior to start of ICSDrugs for asthmaShort-acting beta-agonists 5206 93.6 257 86.5Long-acting beta-agonists 331 6.0 33 11.1Systemic sympathicomimetics 164 2.9 1 0.3Cromoglycates/nedocromil 104 1.9 7 2.4Parasympathicolytics 238 4.3 11 3.7Xanthine-derivatives 3 0.1 — —Leukotriene receptor antagonists 5 0.1 11 3.7Fixed combinations of beta-agonists and para-sympathicolytics 82 1.5 6 2.0
Co-medication related to respiratory diseaseAntihistamines 1481 26.6 91 30.6Mucolytics 156 2.8 10 3.4Coughing agents 467 8.4 32 10.8Nasal preparations 1216 21.9 87 29.3Oral corticosteroids 464 8.3 43 14.5Antibiotics 2959 53.2 133 44.8
(Continues)
Copyright # 2008 John Wiley & Sons, Ltd. Pharmacoepidemiology and Drug Safety, 2008; 17: 411–422DOI: 10.1002/pds
persistence with inhaled corticosteroids-treatment in asthma 415
The majority of the patients received their firstdispensing from the general practitioner (86.8%),received a low starting dose (52.2%) and wereprescribed a twice-daily regimen (76.9%). More than60% (62%) of the patients starting treatment withfixed combined ICS was 19–34 years of age, and 37%of all patients received their initial dispensing from aspecialist. Most patients received the standard dailydose (64.0%) and were also dosed twice daily(83.2%).For both types of treatment, almost all patients had
used short-acting beta-agonists prior to start ICS-treatment (around 87–94%). The most commonlyused other respiratory drugs were long-actingbeta-agonists (6.0% for single ICS and 11.1% forfixed combined ICS). Other medications frequentlyused in patients using single or fixed combined ICSwere antibiotics (around 45–53%), antihistamines(around 27–31%) and nasal preparations (around22–29%). About 14.5% of patients treated with fixedcombined ICS had used oral corticosteroids comparedwith 8.3% of patients treated with single ICS. For bothtypes of treatment, a similar percentage (1.7%) of thepatients had a hospitalization for asthma in the yearprior to the start of the ICS-treatment.Of all patients, 42.8% of patients with fixed
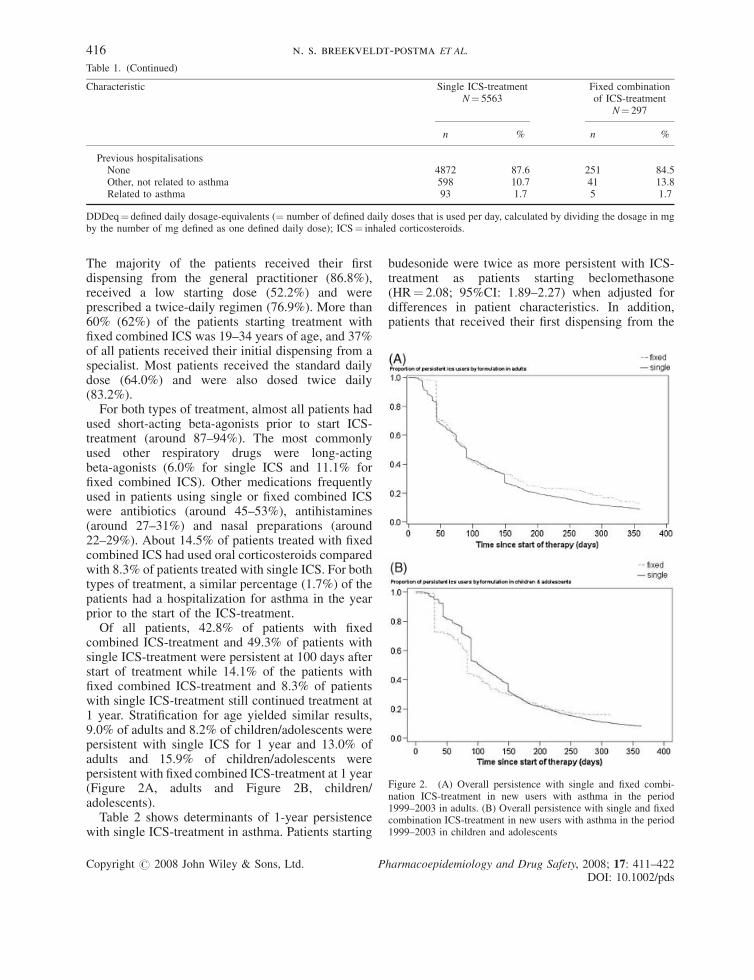
combined ICS-treatment and 49.3% of patients withsingle ICS-treatment were persistent at 100 days afterstart of treatment while 14.1% of the patients withfixed combined ICS-treatment and 8.3% of patientswith single ICS-treatment still continued treatment at1 year. Stratification for age yielded similar results,9.0% of adults and 8.2% of children/adolescents werepersistent with single ICS for 1 year and 13.0% ofadults and 15.9% of children/adolescents werepersistent with fixed combined ICS-treatment at 1 year(Figure 2A, adults and Figure 2B, children/adolescents).Table 2 shows determinants of 1-year persistence
with single ICS-treatment in asthma. Patients starting
budesonide were twice as more persistent with ICS-treatment as patients starting beclomethasone(HR¼ 2.08; 95%CI: 1.89–2.27) when adjusted fordifferences in patient characteristics. In addition,patients that received their first dispensing from the
Table 1. (Continued)
Characteristic Single ICS-treatmentN¼ 5563
Fixed combinationof ICS-treatment
N¼ 297
n % n %
Previous hospitalisationsNone 4872 87.6 251 84.5Other, not related to asthma 598 10.7 41 13.8Related to asthma 93 1.7 5 1.7
DDDeq¼ defined daily dosage-equivalents (¼ number of defined daily doses that is used per day, calculated by dividing the dosage in mgby the number of mg defined as one defined daily dose); ICS¼ inhaled corticosteroids.
Figure 2. (A) Overall persistence with single and fixed combi-nation ICS-treatment in new users with asthma in the period1999–2003 in adults. (B) Overall persistence with single and fixedcombination ICS-treatment in new users with asthma in the period1999–2003 in children and adolescents
Copyright # 2008 John Wiley & Sons, Ltd. Pharmacoepidemiology and Drug Safety, 2008; 17: 411–422DOI: 10.1002/pds
416 n. s. breekveldt-postma ET AL.

Table 2. Determinants of 1-year persistence with single ICS-treatment in asthma
Determinant Crude Adjusted�
HR 95%CI HR 95%CI
Type of ICS at startBeclomethasone 1.0 (ref.) — 1.0 (ref.)Budesonide 1.89y 1.75–2.08 2.08y 1.89–2.27Fluticasone 1.04 0.97–1.11 0.97 0.90–1.04
GenderMale 1.09y 1.02–1.14 1.02 0.96–1.08Female 1.0 (ref.) — 1.0 (ref.) —
Age group (in years)0–4 1.23y 1.15–1.33 1.03 0.93–1.155–8 1.22y 1.12–1.33 1.10 0.99–1.229–14 0.99 0.91–1.09 1.02 0.93–1.1215–18 0.87y 0.78–0.97 0.83y 0.74–0.9319–34 1.0 (ref.) — 1.0 (ref.) —
Year of start ICS1999 1.11y 1.03–1.20 1.02 0.94–1.112000 1.06 0.98–1.15 0.98 0.91–1.062001 1.01 0.93–1.09 0.96 0.89–1.042002 1.0 (ref.) — 1.0 (ref.) —
Prescriber at startGeneral practitioner 1.0 (ref.) — 1.0 (ref.) —Pulmonologist 1.85y 1.47–2.33 1.69y 1.33–2.17Pediatrician 1.52y 1.35–1.72 1.47y 1.30–1.67Specialist, other 1.43y 1.27–1.61 1.37y 1.19–1.54
Inhaler type at startMetered-dose 1.28y 1.22–1.35 1.28y 1.18–1.41Dry-powder 1.0 (ref.) — 1.0 (ref.) —
Daily dose at start (DDDeq)0.01–0.74 1.34y 1.26–1.43 1.35y 1.25–1.450.75–1.24 1.0 (ref.) — 1.0 (ref.) —�1.25 0.90y 0.83–0.98 0.92 0.84–1.01
Dosing frequency at startOnce daily 1.39y 1.28–1.52 1.20y 1.11–1.30Twice daily 1.0 (ref.) — 1.0 (ref.) —>Twice daily 0.65y 0.57–0.73 0.641y 0.56–0.72Undefined 1.06 0.92–1.23 1.00 0.86–1.16
One year prior to start of ICSDrugs for asthmaShort-acting beta-agonists 0.76y 0.67–0.85 0.96 0.84–1.10Long-acting beta-agonists 1.49y 1.33–1.69 1.41y 1.22–1.61Parasympathicolytics 1.16y 1.01–1.33 1.00 0.86–1.15
Co-medication related to respiratory diseaseAntihistamines 1.08y 1.01–1.14 1.04 0.98–1.11Mucolytics 1.05 0.89–1.25 — —Coughing agents 0.88y 0.81–0.98 0.96 0.87–1.06Nasal preparations 1.01 0.94–1.09 — —Oral corticosteroids 1.02 0.93–1.14 — —Antibiotics 0.99 0.93–1.04 — —
Previous hospitalizationsNone 1.0 (ref.) — 1.0 (ref.) —Other, not related to asthma 1.12y 1.03–1.23 1.02 0.93–1.11Related to asthma 1.61y 1.28–2.00 1.35y 1.06–1.72
�Adjusted analyses included all determinants that were associated with persistence in the crude analyses.ySignificantly different (p< 0.05).CI¼ (95%) confidence interval; DDDeq¼ defined daily dosage-equivalents (¼ number of defined daily doses that is used per day, calculatedby dividing the dosage in mg by the number of mg defined as one defined daily dose); HR¼ hazard ratio; ICS¼ inhaled corticosteroids;ref.¼ reference category.
Copyright # 2008 John Wiley & Sons, Ltd. Pharmacoepidemiology and Drug Safety, 2008; 17: 411–422DOI: 10.1002/pds
persistence with inhaled corticosteroids-treatment in asthma 417

specialist were 1.7 times more likely to stay on ICStherapy than patients receiving their first dispensingfrom the general practitioner (HR¼ 1.69; 95%CI:1.33–2.17). Other determinants of statistically higherpersistence rates with single ICS-treatment were prioruse of long-acting beta-agonists, previous hospitaliz-ation for asthma, use of a metered-dose inhaler at start,a low starting dose (0.01–0.74 DDDeq) and aonce-daily regimen at the start of ICS. Persistencerates were decreased for patients with a more thantwice-daily regimen and who were aged between15 and 18 years at the start of ICS therapy.Stratified analyses for age yielded similar results for
most determinants, except for age, dose and hospi-talization. With regard to age, children were morepersistent with ICS-treatment than adolescents(15–18 years) (HR of about 1.2 for all younger agegroups), whereas in adults persistence slightlyincreased with increasing age (HR¼ 1.02; 95%CI:1.01–1.03). With regard to dose, children/adolescentswith a high starting dose were more persistent withICS-treatment compared to the normal dose(HR¼ 1.15; 95%CI: 1.02–1.30), while in adultspatients with a high starting dose were less persistentwith ICS-treatment (HR¼ 0.71; 95%CI: 0.61–0.83).Prior hospitalization for asthma was not related topersistence with ICS-treatment in adults.Adjusted analyses of determinants of persistence
with fixed combined ICS-treatment showed thatpersistence rates were increased in younger patients(0–4 and 5–8 years) compared to adults (Table 3).Persistence rates significantly decreased for patientson fixed combined ICS-treatment starting treatment in1999 compared with 2002, starting at high dose(�1.25 DDDeq) and who had used antibiotics inthe 1-year period prior to the start of ICS. Analyseswere not stratified for age groups because of smallnumbers.
DISCUSSION
The results of the present population-based cohortstudy among new users of single or fixed combinedICS-treatment for asthma indicate that 1-year persist-ence rates with ICS are alarmingly low. Less than 10%of patients starting single ICS-treatment and about15% of patients starting fixed combined ICS-treatmentused ICS continuously during the first year oftreatment.In the present study, patterns of persistence were
similar for single and fixed combined ICS-treatment,despite limited numbers in the latter group. The
observed low persistence rates in our study are in linewith previously published studies for single ICSand inhaled respiratory drugs in general that reportedadherence ranges from 10% to 70%.1,11–13,17 Infor-mation on adherence with fixed combined ICS is,however, limited. One other observational study byStoloff et al. showed that refill persistence (measuredas the medication possession ratio) with the fixed com-bined salmeterol/fluticasone was about 70% andincreased compared with the two single compounds.15
Their study was limited to patients with a hospital-ization for asthma only which may explain the higherpersistence rates. These patients may be more severeand may be more aware of their need to take theirmedication as directed, resulting in higher adherencerates.12,17,34
Persistence with budesonide was increased com-pared with beclomethasone, the exact reason for this isunknown. Differences between budesonide andbeclomethasone seemed to be independent of thetype of inhaler (metered dose or dry powder).However, as different formulations and doses areavailable for the various ICS we may not be able tofully adjust for this. For instance, the results may be(partly) biased by the difference in duration ofdispensing, with a median duration of 100 days forbudesonide and a median duration of 60 days forbeclomethasone. Persistence rates were increasedwith metered-dose inhalers compared with dry-powder inhalers and persistence rates were especiallylow with inhalers using capsules, which is most likelyexplained by the patient’s preference for certaininhalers.35 Choice of delivery device depends amongstothers on the device/drug availability, the patient ageand the ability to use the selected device correctly.36 Apositive patient-attitude towards the treatment, appro-priate patient training and device education and theright inhalation technique have been shown to becrucial to improved patient adherence with inhaleddrug therapy.37
Once-daily dosing also increased persistence com-pared with the multiple dosing. Reduction of dosingfrequencies has been shown to increase medicationadherence in asthma and several other chronicdiseases, probably because of the enhanced conven-ience for the patient.38,39
Persistence rates with single ICS-treatment werealso increased for patients who received their initialdispensing from a specialist, who had used long-actingbeta-agonists or had a previous hospitalization forasthma. These determinants may all reflect a higherdisease severity, and as patients and physicians aremore aware of the underlying severity of the disease,
Copyright # 2008 John Wiley & Sons, Ltd. Pharmacoepidemiology and Drug Safety, 2008; 17: 411–422DOI: 10.1002/pds
418 n. s. breekveldt-postma ET AL.

Table 3. Determinants of 1-year persistence with fixed combined ICS-treatment in asthma
Determinant Crude Adjusted�
HR 95%CI HR 95%CI
Type of ICS at startSalmeterol/fluticasone 1.0 (ref.) — 1.0 (ref.)Formoterol/budesonide 1.56y 1.15–2.13 1.23 0.83–1.85
GenderMale 1.00 0.78–1.28 1.02 0.79–1.32Female 1.0 (ref.) — 1.0 (ref.) —
Age group (in years)0–4 1.52 0.70–3.23 2.94y 1.23–7.145–8 1.20 0.72–2.00 2.50y 1.27–5.009–14 0.95 0.67–1.35 1.33 0.87–2.0415–18 1.00 0.69–1.45 0.99 0.68–1.4519–34 1.0 (ref.) — 1.0 (ref.) —
Year of start ICS1999 0.41y 0.21–0.79 0.40y 0.20–0.782000 0.88 0.57–1.33 1.08 0.69–1.672001 0.74y 0.56–0.96 0.78 0.59–1.022002 1.0 (ref.) — 1.0 (ref.) —
Prescriber at startGeneral practitioner 1.0 (ref.) —Pulmonologist 1.35 0.94–1.92Pediatrician 1.30 0.76–2.27Specialist, other 1.00 0.71–1.41
Daily dose at start (DDDeq)0.01–0.74 1.89y 1.28–2.78 1.49 0.91–2.440.75–1.24 1.0 (ref.) — 1.0 (ref.) —�1.25 1.04 0.77–1.41 0.61y 0.38–0.97
Dosing frequency at startOnce daily 0.94 0.65–1.39Twice daily 1.0 (ref.) —>Twice daily 0.65 0.35–1.23Undefined 1.59 0.59–4.35
One year prior to start of ICSDrugs for asthmaShort-acting beta-agonists 0.85 0.58–1.22Long-acting beta-agonists 1.47 0.98–2.22Parasympathicolytics 0.78 0.41–1.47
Co-medication related to respiratory diseaseAntihistamines 1.06 0.82–1.39Mucolytics 1.15 0.57–2.33Coughing agents 1.10 0.74–1.64Nasal preparations 0.82 0.63–1.08Oral corticosteroids 0.81 0.58–1.15Antibiotics 0.77y 0.60–0.99 0.76y 0.59–0.98
Previous hospitalizationsNone 1.0 (ref.) —Other, not related to asthma 0.99 0.70–1.41Related to asthma 0.59 0.24–1.45
�Adjusted analyses included all determinants that were associated with persistence in the crude analyses.ySignificantly different (p< 0.05).CI¼ (95%) confidence interval; DDDeq¼ defined daily dosage-equivalents (¼ number of defined daily doses that is used per day, calculatedby dividing the dosage in mg by the number of mg defined as one defined daily dose); HR¼ hazard ratio; ICS¼ inhaled corticosteroids;ref.¼ reference category.
Copyright # 2008 John Wiley & Sons, Ltd. Pharmacoepidemiology and Drug Safety, 2008; 17: 411–422DOI: 10.1002/pds
persistence with inhaled corticosteroids-treatment in asthma 419

patients may be more likely to take their medication asdirected.12,13,40
Persistence with single ICS-treatment wasdecreased with a high starting dose of ICS whichmay relate to the fact that patients experienced adverseevents.41 In addition, persistence rates were lower inpatients aged 15–18 years, which has been shownbefore.42
Although it may be anticipated that persistence withICS-treatment is different for children/adolescents andadults, as the diagnosis of asthma may be less clear inchildren and persistent ICS-treatment may be lessfavourable, the present study showed similar persist-ence rates and determinants of persistence for bothgroups of patients in case of single ICS-treatment. It isnot known whether the persistence rates remainsimilar after the first year of treatment.In case of fixed combined ICS-treatment, persist-
ence was increased in very young children comparedto adults but numbers were too low to allow stratifiedanalyses. Determinants of decreased persistence withfixed combined ICS-treatment were a high startingdose of ICS as was observed with single ICS and prioruse of antibiotics. The reason for the latter remains yetto be investigated. Persistence was somewhat lowershortly after introduction compared to more recentyears, which may relate to differences in patientcharacteristics or treatment strategies early afterintroduction. Although this study was not designedto compare fixed combined ICS-treatment with the useof both single compounds and the number of patientsusing fixed combined ICS preparations was limited,frequency distributions of first prescriber, prior use oflong-acting beta-agonists and oral corticosteroidsindicate that patients starting treatment with fixed com-bined ICS-treatment may have a higher disease seve-rity or less controlled disease than patients startingnew treatment with single ICS. The present study alsoindicates that overall persistence rates with fixedcombined ICS-treatment are still low, however, thenumber of patients was limited. Other studies showedincreased adherence rates with fixed combined ICS-treatment compared to single ICS-treatment. Thesestudies were restricted to certain patient groups andused refill rates to measure adherence.15,43 Moreresearch is required to study persistence with fixedcombined ICS in daily practice including sufficientnumbers of patients who are representative of thepopulation that is treated.Several limitations of this study may be addressed.
First, no information on a definite diagnosis of asthmawas available in this study, but asthma patients weredefined on the basis of drug use and age. In order to
include patients that used ICS for chronic diseasesonly, we excluded patients that did not refill their ICSdispensing within 1 year. Still, patients with anotherdiagnosis may have been included in the study whichmay have resulted in an underestimation of persist-ence. Second, persistence with ICS in the same group(single or combined) was discontinued when patientsswitched from one type to another type of ICS. We didnot study the extent of switching between types ofICS, but a former study in a similar population wherepersistence was determined regardless of type of ICSshowed overall 1-year persistence rates of about 18%which is still very low.12 In addition, patients whoswitched from use of single ICS-treatment to fixedcombined ICS-treatment were excluded from thestudy, which may have underestimated the persistencewith fixed combined ICS-treatment. Third, the reasonsfor discontinuation of ICS are not known. There maybe good reasons to discontinue treatment andintermittent therapy may be appropriate for some ofthe patients. However, it is not likely that the beforementioned limitations entirely explain the lowpersistence rates observed in our study.
Poor adherence with ICS is recognized as acontributor to treatment failure resulting in theincreased morbidity and mortality, and increasedhealth care expenditures.44 An increased persistencewith ICS in daily clinical practice may result inreduced morbidity, increased quality of life and lead toreduced healthcare costs.38
CONCLUSION
In conclusion, the current study showed that new usersof both single and fixed combined ICS have alarminglow persistence rates with ICS-treatment in the firstyear of follow-up. Persistence was mainly related topatient factors, such as severity of disease, and to
KEY POINTS
� New users of both single and fixed combinedICS have alarming low persistence rates withICS-treatment in the first year of follow-up.
� Persistence with ICS-treatment was mainlyrelated to patient factors, such as severity ofdisease, and to treatment-related factors, suchas once-daily dosing frequency.
Copyright # 2008 John Wiley & Sons, Ltd. Pharmacoepidemiology and Drug Safety, 2008; 17: 411–422DOI: 10.1002/pds
420 n. s. breekveldt-postma ET AL.

treatment-related factors, such as once-daily dosingfrequency.
ACKNOWLEDGEMENTS
The authors acknowledge the critical review of thestudy proposal and manuscript by the other membersof the CAMERA Study Group. This study was finan-cially supported by an unconditional grant fromALTANA Pharma bv.
REFERENCES
1. Williams LK, Pladevall M, Xi H, et al. Relationship betweenadherence to inhaled corticosteroids and poor outcomes amongadults with asthma. J Allergy Clin Immunol 2004; 114:1288–1293.
2. Allen DB, Bielory L, Derendorf H, et al. Inhaled corticoster-oids: past lessons and future issues. J Allergy Clin Immunol2003; 112: S1–S40.
3. Suissa S, Ernst P. Inhaled corticosteroids: impact on asthmamorbidity and mortality. J Allergy Clin Immunol 2001; 107:937–944.
4. Suissa S, Ernst P, Benayoun S, et al. Low-dose inhaled corti-costeroids and the prevention of death from asthma. N Engl JMed 2000; 343: 332–336.
5. Blais L, Ernst P, Boivin JF, et al. Inhaled corticosteroids and theprevention of readmission to hospital for asthma. Am J RespirCrit Care Med 1998; 158: 126–132.
6. Blais L, Suissa S, Boivin JF, et al. First treatment with inhaledcorticosteroids and the prevention of admissions to hospital forasthma. Thorax 1998; 53: 1025–1029.
7. Busse WW. Inflammation in asthma: the cornerstone of thedisease and target of therapy. J Allergy Clin Immunol 1998; 102:S17–22.
8. Schatz M, Cook EF, Nakahiro R, et al. Inhaled corticosteroidsand allergy specialty care reduce emergency hospital use forasthma. J Allergy Clin Immunol 2003; 111: 503–508.
9. Suissa S, Ernst P, Kezouh A. Regular use of inhaled corticos-teroids and the long term prevention of hospitalisation forasthma. Thorax 2002; 57: 880–884.
10. Goldman M, Rachmiel M, Gendler L, et al. Decrease in asthmamortality rate in Israel from 1991-1995: is it related to increaseduse of inhaled corticosteroids? J Allergy Clin Immunol 2000;105: 71–74.
11. Lacasse Y, Archibald H, Ernst P, et al. Patterns and determinantsof compliance with inhaled steroids in adults with asthma. CanRespir J 2005; 12: 211–217.
12. Breekveldt-Postma NS, Gerrits CM, Lammers JW, et al. Per-sistence with inhaled corticosteroid therapy in daily practice.Respir Med 2004; 98: 752–759.
13. Cochrane MG, Bala MV, Downs KE, et al. Inhaled corticoster-oids for asthma therapy: patient compliance, devices, andinhalation technique. Chest 2000; 117: 542–550.
14. Rau JL. Determinants of patient adherence to an aerosol regi-men. Respir Care 2005; 50: 1346–1356; discussion 1349–1357.
15. Stoloff SW, Stempel DA, Meyer J, et al. Improved refillpersistence with fluticasone propionate and salmeterol in asingle inhaler compared with other controller therapies.J Allergy Clin Immunol 2004; 113: 245–251.
16. Chapman KR, Walker L, Cluley S, et al. Improvingpatient compliance with asthma therapy. Respir Med 2000;94: 2–9.
17. Clark N, Jones P, Keller S, et al. Patient factors and compliancewith asthma therapy. Respir Med 1999; 93: 856–862.
18. Boulet LP. Perception of the role and potential side effects ofinhaled corticosteroids among asthmatic patients. Chest 1998;113: 587–592.
19. Buhl R. Budesonide/formoterol for the treatment of asthma.Expert Opin Pharmacother 2003; 4: 1393–1406.
20. Barnes PJ. Scientific rationale for inhaled combination therapywith long-acting beta2-agonists and corticosteroids. EurRespir J 2002; 19: 182–191.
21. Chapman KR, Ringdal N, Backer V, et al. Salmeterol andfluticasone propionate (50/250 microg) administered via com-bination Diskus inhaler: as effective as when given via separateDiskus inhalers. Can Respir J 1999; 6: 45–51.
22. Nelson HS, Chapman KR, Pyke SD, et al. Enhanced synergybetween fluticasone propionate and salmeterol inhaled from asingle inhaler versus separate inhalers. J Allergy Clin Immunol2003; 112: 29–36.
23. Buhl R, Creemers JP, Vondra V, et al. Once-daily budesonide/formoterol in a single inhaler in adults with moderate persistentasthma. Respir Med 2003; 97: 323–330.
24. Dorais M, Blais L, Chabot I, et al. Treatment persistence withleukotriene receptor antagonists and inhaled corticosteroids.J Asthma 2005; 42: 385–393.
25. Jonasson G, Carlsen KH, Mowinckel P. Asthma drug adherencein a long term clinical trial. Arch Dis Child 2000; 83: 330–333.
26. Diette GB, Wu AW, Skinner EA, et al. Treatment patternsamong adult patients with asthma: factors associated withoveruse of inhaled beta-agonists and underuse of inhaled corti-costeroids. Arch Intern Med 1999; 159: 2697–2704.
27. Milgrom H, Bender B, Ackerson L, et al. Noncompliance andtreatment failure in children with asthma. J Allergy Clin Immu-nol 1996; 98: 1051–1057.
28. Coutts JA, Gibson NA, Paton JY. Measuring compliance withinhaled medication in asthma. Arch Dis Child 1992; 67:332–333.
29. Mann M, Eliasson O, Patel K, et al. A comparison of the effectsof bid and qid dosing on compliance with inhaled flunisolide.Chest 1992; 101: 496–499.
30. Herings RMC. PHARMO: a record linkage system for post-marketing surveillance of prescription drugs in The Nether-lands. Thesis. Utrecht: Utrecht University; 1993.
31. Catalan VS, Lelorier J. Predictors of long-term persistence onstatins in a subsidized clinical population. Value Health 2000; 3:417–426.
32. Monane M, Bohn RL, Gurwitz JH, et al. The effects of initialdrug choice and comorbidity on antihypertensive therapy com-pliance: results from a population-based study in the elderly.Am J Hypertens 1997; 10: 697–704.
33. National Heart, Lung, and Blood Institute. NAEPP: guidelinesfor the diagnosis and management of asthma - update onselected topics 2002. Expert Panel Report 2002; NIH Publi-cation No. 02-5075. Available from: http://www.nhlbi.nih.gov/guidelines/asthma/asthmafullrpt.pdf [cited 26 April 2006].
34. Cochrane GM, Horne R, Chanez P. Compliance in asthma.Respir Med 1999; 93: 763–769.
35. Crompton GK. Dry powder inhalers: advantages and limita-tions. J Aerosol Med 1991; 4: 151–156.
36. Dolovich MB, Ahrens RC, Hess DR, et al. Device selection andoutcomes of aerosol therapy: evidence-based guidelines: Amer-
Copyright # 2008 John Wiley & Sons, Ltd. Pharmacoepidemiology and Drug Safety, 2008; 17: 411–422DOI: 10.1002/pds
persistence with inhaled corticosteroids-treatment in asthma 421

ican College of Chest Physicians/American College of Asthma,Allergy, and Immunology. Chest 2005; 127: 335–371.
37. Crompton GK, Barnes PJ, Broeders M, et al. The need toimprove inhalation technique in Europe: a report from theAerosol Drug Management Improvement Team. Respir Med2006.
38. Guest JF, Davie AM, Ruiz FJ, et al. Switching asthma patientsto a once-daily inhaled steroid improves compliance andreduces healthcare costs. Prim Care Respir J 2005; 14: 88–98.
39. Claxton AJ, Cramer J, Pierce C. A systematic review of theassociations between dose regimens and medication compli-ance. Clin Ther 2001; 23: 1296–1310.
40. Wolfenden LL, Diette GB, Krishnan JA, et al. Lower physicianestimate of underlying asthma severity leads to undertreatment.Arch Intern Med 2003; 163: 231–236.
41. Hanania NA, Chapman KR, Kesten S. Adverse effects ofinhaled corticosteroids. Am J Med 1995; 98: 196–208.
42. Pohunek P, Tal A. Budesonide and formoterol in a single inhalercontrols asthma in adolescents. Int J Adolesc Med Health 2004;16: 91–105.
43. Stempel DA, Stoloff SW, Carranza Rosenzweig JR, et al.Adherence to asthma controller medication regimens. RespirMed 2005; 99: 1263–1267.
44. Barnes PJ, Jonsson B, Klim JB. The costs of asthma. EurRespir J 1996; 9: 636–642.
APPENDIX
The CAMERA Study Group consists of J-W. J. Lammers,MD, PhD, Department of Pulmonary Diseases,University Medical Center Utrecht, Utrecht; A. J.M. Schreurs, MD, PhD, Department of PulmonaryDiseases, Jeroen Bosch Hospital’s, Hertogenbosch; T.van der Molen, MD, PhD, Department of GeneralPractice, University Medical Center Groningen,Groningen; M. P. M. H. Rutten-van Molken, PhD,Institute for Medical Technology Assessment, Eras-mus Medical Center, Rotterdam; J. A. Erkens, PhDand R. M. C. Herings, PhD, PHARMO Institute,Utrecht; The Netherlands.
Copyright # 2008 John Wiley & Sons, Ltd. Pharmacoepidemiology and Drug Safety, 2008; 17: 411–422DOI: 10.1002/pds
422 n. s. breekveldt-postma ET AL.