treatment regimens for the public health approach: do we...
TRANSCRIPT

Treatment regimens for the public health approach: do we need to change?
Nicholas Paton MD FRCP
Professor of Medicine
National University of Singapore

2
Disclosures (1)
Dr Paton has received research grants awarded
to his institution from Janssen, GSK, and Merck;
has received speakers fees from AbbVie, Janssen,
and Merck; and serves as a member of data-
monitoring committees for Roche-sponsored
clinical trials.

3
Estimated numbers on ART P
eo
ple
re
ceiv
ing
AR
T (m
illio
ns)
Global AIDS Response Progress Reporting (UNAIDS/UNICEF/WHO). Available at: http://www.who.int/hiv/data/art_2003_2015.png?ua=1
3Global AIDS Response Progress Reporting (UNAIDS/UNICEF/WHO). Available at: http://www.who.int/hiv/data/art_2003_2015.png?ua=1
0,0
2,0
4,0
6,0
8,0
10,0
12,0
14,0
16,0
18,0
20,0
非洲地区
美洲地区
地中海东部地区
欧洲地区
东南亚地区
西太平洋地区
>20m in 2017
2000 2010 2016 year
<1m
7.5m
Source: UNAIDS/WHO estimates.
African region
Region of the Americas
Eastern Mediterranean region
European region
South-East Asia region
Western Pacific region

4
Standardised ART sequence in WHO public health approach
Standardised first line Standardised second line~3% fail/year Standardised third line
ART, antiretroviral therapy; NRTI, nucleoside reverse-transcriptase inhibitors;NNRTI, non-NRTI; PI, protease inhibitor; RAL, raltegravir; WHO, World Health Organization.
PINRTIPINNRTI
NRTI
NRTI
NRTI
5
WHO ART Guidelines 2003
WHO ART guidelines 2003

6
First-line therapy (2016 guidelines)
WHO guidelines, 2016. Available at: http://apps.who.int/iris/bitstream/10665/208825/1/9789241549684_eng.pdf?ua=1. Accessed May 2017.
3TC, lamivudine; ABC, abacavir; AZT, zidovudine; DTG, dolutegravir; EFV, efavirenz; HIV, human immunodeficiency virus; FTC, emtricitabine;
LPV/r, lopinavir/ritonavir; TB, tuberculosis; TDF, tenofovir disoproxil fumarate; NVP; nevirapine.
First-line ART Preferred first-line regimens Alternative first-line regimens
Adults TDF + 3TC (or FTC) + EFV AZT + 3TC + EFV (or NVP) TDF + 3TC (or FTC) + DTG*
TDF + 3TC (or FTC) + EFV400*
TDF + 3TC (or FTC) + NVP
Pregnant or breastfeeding women
TDF + 3TC (or FTC) + EFV AZT + 3TC + EFV (or NVP) TDF + 3TC (or FTC) + NVP
Adolescents TDF + 3TC (or FTC) + EFV AZT + 3TC + EFV (or NVP) TDF (or ABC) + 3TC (or FTC) + DTG*
TDF (or ABC) + 3TC (or FTC) + EFV400*
TDF (or ABC) + 3TC (or FTC) + NVP
Children 3 years to less than10 years
ABC + 3TC + EFV ABC + 3TC + NVP AZT + 3TC + EFV (or NVP) TDF + 3TC (or FTC) + EFV (or NVP)
Children less then 3 years ABC (or AZT) + 3TC + LPV/r ABC (or AZT) + 3TC + NVP
*Safety and efficacy data on the use of DTG and EFV400 in pregnant women, people with HIV/TB coinfection and adolescents younger than 12 years of age are not yet available

DTG + 2NRTIs

8
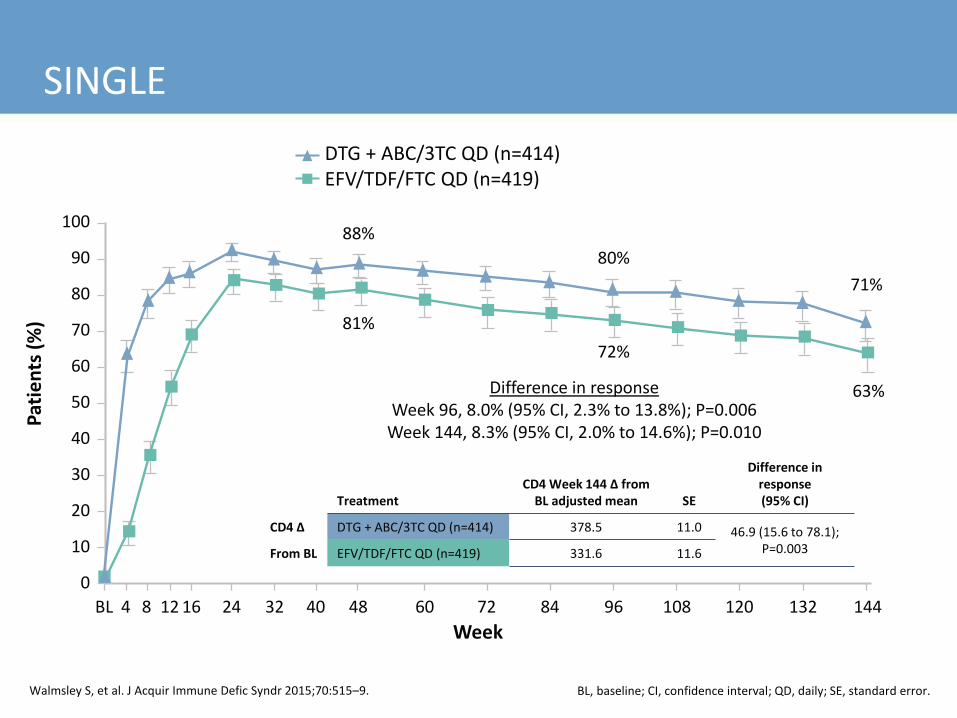
SINGLE
100
90
80
70
60
50
40
30
20
10
0
BL 4 8 12 16 24 32 40 48 60 72 84 96 108 120 132 144
Pat
ien
ts (
%)
Week
TreatmentCD4 Week 144 ∆ from
BL adjusted mean SE
Difference in response(95% CI)
CD4 ∆ DTG + ABC/3TC QD (n=414) 378.5 11.0 46.9 (15.6 to 78.1);P=0.003From BL EFV/TDF/FTC QD (n=419) 331.6 11.6
Difference in responseWeek 96, 8.0% (95% CI, 2.3% to 13.8%); P=0.006
Week 144, 8.3% (95% CI, 2.0% to 14.6%); P=0.010
88%
81%
80%
72%
71%
63%
BL, baseline; CI, confidence interval; QD, daily; SE, standard error.
DTG + ABC/3TC QD (n=414)EFV/TDF/FTC QD (n=419)
Walmsley S, et al. J Acquir Immune Defic Syndr 2015;70:515–9.

9
SINGLE (2)
c/mL=copies/mL; VL, viral load.
VL failure (2 VL > XX c/mL after Week 24):
DTG EFV
≥50 c/mL: 39/414 (9%) 33/419 (8%)
>200 c/mL: 29 (7%) 23 (5%)
>1000 c/mL: 5 (1%) 2 (<1%)

10
SINGLE (3): AEs leading to discontinuation
Walmsley S, et al. N Engl J Med 2013;369:1807–18. AE, adverse event.
AEsDTG + ABC/3TC
(n=414)
EFV/TDF/FTC
(n=419)
Number of participants (%)
AE leading to discontinuation ofstudy drug (by Week 48)
10 (2%) 42 (10%)
Psychiatric disorder 2 (<1%) 15 (4%)
Nervous system disorder 0 (0%) 13 (3%)
Skin and subcutaneous-tissue disorder 2 (<1%) 8 (2%)
Gastrointestinal disorder 0 (0%) 8 (2%)
General disorder or administration-site condition 0 (0%) 7 (2%)
11
SINGLE
100
90
80
70
60
50
40
30
20
10
0
BL 4 8 12 16 24 32 40 48 60 72 84 96 108 120 132 144
Pat
ien
ts (
%)
Week
TreatmentCD4 Week 144 ∆ from
BL adjusted mean SE
Difference in response(95% CI)
CD4 ∆ DTG + ABC/3TC QD (n=414) 378.5 11.0 46.9 (15.6 to 78.1);P=0.003From BL EFV/TDF/FTC QD (n=419) 331.6 11.6
Difference in responseWeek 96, 8.0% (95% CI, 2.3% to 13.8%); P=0.006
Week 144, 8.3% (95% CI, 2.0% to 14.6%); P=0.010
88%
81%
80%
72%
71%
63%
BL, baseline; CI, confidence interval; QD, daily; SE, standard error.
DTG + ABC/3TC QD (n=414)EFV/TDF/FTC QD (n=419)
Walmsley S, et al. J Acquir Immune Defic Syndr 2015;70:515–9.

12
Resistance in SINGLE
Tested for resistance in all with VL >50 copies/mL
At week 144:
• DTG: 0/414 (0%) EFV: 7/419 (1.7%; 6 NNRTI, 1 K65R)
• DTG has a high barrier to resistance
• Like PI, but also protects the NRTIs
Walmsley S, et al. JAIDS 2015;70:515–9.

13
Key populations: DTG
Patients with TB Pregnant women
PK and efficacy PK and efficacy (rifampicin, UGT1A1) Safety

14
Effect of RIF on DTG
7.00
6.00
5.00
4.00
1.00
0.000 4 8 12 16 20 24
DTG
co
nce
ntr
atio
n (
µg
/mL)
Time after dose (h)
3.00
2.00
DTG 50 mg QDDTG 50 mg BID
BID, twice daily; h, hour; RIF, rifampin.Dooley KE, et al. J Acquir Immune Defic Syndr 2013;62:21–7.

15
Effect of RIF on DTG
7.00
6.00
5.00
4.00
1.00
0.000 4 8 12 16 20 24
DTG
co
nce
ntr
atio
n (
µg
/mL)
Time after dose (h)
3.00
2.00
DTG 50 mg QDDTG 50 mg BIDDTG 50 mg BID + RIF 600 mg QD
BID, twice daily; h, hour; RIF, rifampin.Dooley KE, et al. J Acquir Immune Defic Syndr 2013;62:21–7.

16
DTG and TB Treatment: INSPIRING Trial
PatientsHIV (ART naïve, starting ART) + DS-TB (on RIF-based TB Rx for ≤ 8 weeks)
Randomisation: 2NRTIs + DTG vs 2NRTIs + EFV NRTIs investigator-selected; DTG 50mg bd during TB Rx +2wks, then 50mg daily; EFV: 600mg once daily throughout
Primary outcome: HIV RNA < 50 copies/ml at week 48
Week 24 (interim) analysis: DTG: 56/69 (81%) (95% CI: 72%, 90%) EFV: 39/44 (89%) (95% CI: 79%, 98%) [Difference due to 7% discontinuations in DTG arm vs 0% in EFV arm]
Conclusions (to date):DTG effective in suppressing VL with RIF-containing TB Rx[NB: no information about TB outcomes]
Dooley et al, CROI 2018, Abstract O-03

17
DTG PK in pregnancy
DTG AUC and trough lower in pregnancy (compared with post-partum)
Levels similar to those in non-pregnant adults
Mulligan, CROI 2016
DTG efficacy in pregnancy: DOLPHIN and VESTED trials

18
DTG efficacy in pregnancy
Hill J Vir Erad 2018

19
DTG Safety in Pregnancy
18 May 2018, WHO statement:
Update from Botswana study
0.9% of babies (4 of 426) whose mothers became pregnant while taking DTG had a neural tube defect
0.1% of babies (14 of 11,173) whose mothers took other HIV meds had neural tube defect
EMA guidance:

20
Relevance of DTG + 2NRTI as first-line regimen (from perspective of public health approach)
• Advantages
– Reduced toxicity c/w EFV (but other strategies for that)
– Potential resistance prevention (impact on outcomes not known)
– Reduced cost (eventually)
• Neutral
– Not virologically superior to EFV
– Efficacy during TB treatment demonstrated (need complete data)
• Disadvantages
– Efficacy in pregnancy (not known)
– Safety in pregnancy (potential risk)
– Dose modification for TB (almost certainly needed)
– First-line DTG would mean retrench EFV from prescription armamentarium
– Logistics of change
– Generally limited comparative data in resource limited settings / strategic thinking
• Conclusion: Relevant, but considerations are complex

EFV (lower dose) + 2NRTIs

22
Lower-dose EFV (400 mg)Mean change in HIV RNA viral load from BL to Week 96 for the
modified ITT population
EFV 400 mgEFV 600 mg
0
–0.5
–1.0
–1.5
–3.5
–4.00 12 24 36 48 72 96
Ch
ange
fro
m B
L H
IV R
NA
Log 1
0 c
op
ies
pe
r m
L
Week
–2.0
–3.0
60 84
–2.5
Mean difference –0.02 Log30 copies/mL(95% CI, –0.14 to 0.10); P=0.74
321309
316302
312301
310299
312295
307291
304290
300289
299286
Number at riskEFV 400 mgEFV 600 mg
ITT, intention-to-treat.ENCORE 1 Study Group. Lancet Infect Dis 2015;15:793–802.

23
EFV 400-mggroup (n=321)
EFV 600-mg group (n=309)
Difference(95% CI)
Pvalue
AEs (total=3337)
Total number of AEs 1653 (49.5) 1684 (50.5) – 0.42
Grade 1 1202 (73) 1236 (73) – –
Grade 2 381 (23) 363 (22) – –
Grade 3 62 (4) 77 (5) – –
Grade 4 8 (1) 8 (1) – –
Patients reporting AEs 291 (91) 285 (92) –1.6 (–2.8 to 5.9) 0.48
Patients with AE related to EFV* 126 (39) 148 (48) –8.6 (–16.4 to –0.9) 0.03
Patients stopping EFV because of treatment-related AE*†
16 (13) 32 (23) –10.3 (–19.2 to –1.4) 0.03
Serious AEs
Total number of serious AEs 32 (40) 48 (60) - -
Patients reporting serious AEs 24 (8) 32 (10) –2.9 (–7.3 to 1.5) 0.20
Patients reporting serious AEs related to EFV*‡ 2 (1) 4 (1) –0.7 (–2.4 to 1.1) 0.44
Lower-dose EFV (400 mg)
AEs and serious AEs
Data are n (%) unless otherwise indicated.*Definitely or probably related to EFV.
†Relationship interaction P=0.046.‡Events included Grade 3 dizziness and possible Stevens-Johnson syndrome
with the 400-mg dose and rash with fever, septic shock possibly due to an adverse reaction, rash with labial oedema, suicide and attempted suicide
with the 600-mg dose (1 event each in 3 patients, except for rash with fever and septic shock, which occurred in the same patient).
ENCORE 1 Study Group. Lancet Infect Dis 2015;15:793–802.
24
Key populations: EFV400
Patients with TB Pregnant women
PK and efficacy PK and efficacy (rifampicin, CYP3A4) Safety

25
EFV400 with TB treatment
Cerrone et al, CROI 2018, Abstract 1824
Limited changes in EFV400 exposure (<25%)Plasma levels > 1000 ng/ml (MEC from ENCORE-1) irrespective of CYP2B6 genotype EFV400 maintained undetectable VL in allEFV400 can be administered with TB treatment
Open label PK study; HIV+ (not active TB) 26 enrolled, 22 completed PK2 (42d on RIF/INH), 18 completed PK3 (92d on RIF/INH) 4 withdrawals due to EFV levels < 800ng/ml

26
EFV 400 in pregnancy
22 pregnant HIV+ women (African origin) on TDF/FTC/EFV600 with VL<50 copies/ml switched to TDF/FTC/EFV400
All women maintained VL< 50
Conclusion: EFV400 can be used in pregnancy
Lamorde et al., IAS 2017
In 3rd trimester, Cmax, AUC, and C24h were 14%, 26% and 38% lower compared to post-partum (both on EFV400)
Levels within ranges for EFV600 during 3rd trimester in previous studies (Schalkwijk et al. 2016)
and in ARV-naïve patients on EFV400 (Dickinson et al. 2015).

27
Relevance of EFV400 +2NRTI first-line regimen (for public health approach)
• Advantages – Reduced toxicity c/w standard EFV dose– Reduced cost
• Neutral– Equal VL efficacy c/w standard EFV dose – Equal efficacy in pregnancy (limited data) – Equal efficacy with TB treatment (limited data)
• Disadvantages -
• Conclusion: Highly relevant

28
DTG vs EFV400

29
NAMSAL trial
• Phase III, randomized, open-label trial
• N=606; Cameroon
• Randomised to
– DTG + TDF/XTC
– EFV 400 + TDF/XTC
•Primary outcome: VL < 50 c/ml at 48 weeks
• Estimated completion: September 2018

30
Impact of pre-treatment drug resistance on treatment outcomes
Philipps Lancet HIV 2017
OPTION 1: Start EFV in all (current policy, no change)
OPTION 2: Resistance tests for ART initiators with previous ART exposureStart DTG if NNRTI resistance
OPTION 3: Resistance tests for all ART initiators. Start DTG if NNRTI resistance
OPTION 4: Start DTG for ART initiators with previous ART exposure
OPTION 5: Start DTG in all

31
The Lancet HIV 2018 5, e146-e154DOI: (10.1016/S2352-3018(17)30190-X)
Mean annual cost (2018-38) according to policy option where > 10% initiators have NNRTI resistance
Impact of pre-treatment drug resistance on costs
Philipps Lancet HIV 2017

32
Impact of pre-treatment NNRTI resistance
Gupta et al, Lancet Infectious Diseases, 2017

33
Second-line ART: WHO 2016 guidelines

PI/r + INSTI in second-line therapy
35
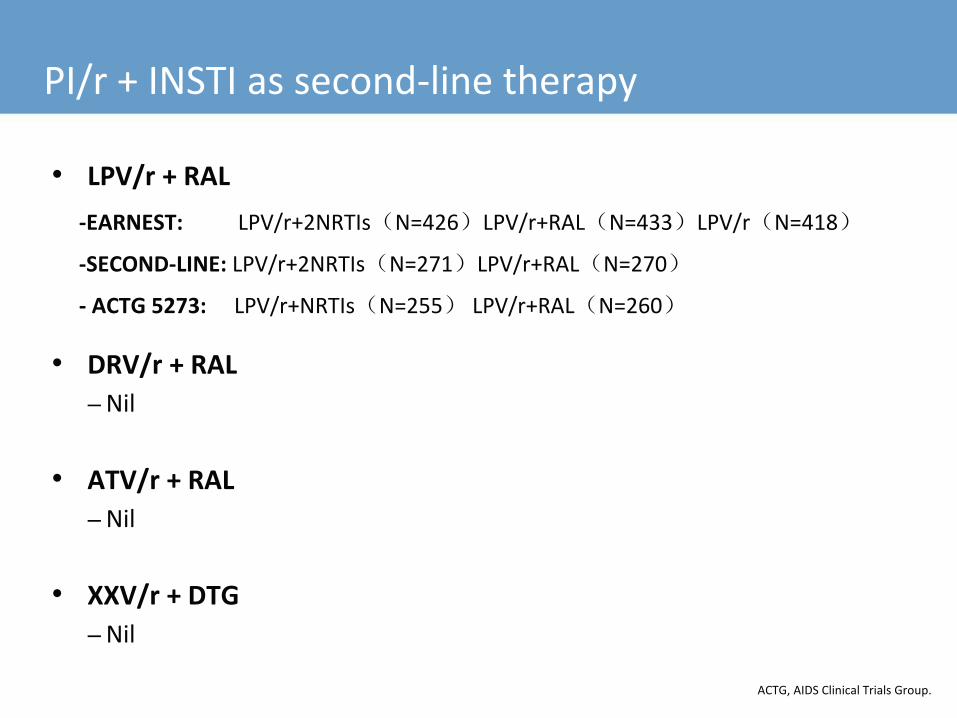
PI/r + INSTI as second-line therapy
• LPV/r + RAL
-EARNEST: LPV/r+2NRTIs(N=426)LPV/r+RAL(N=433)LPV/r(N=418)
-SECOND-LINE: LPV/r+2NRTIs(N=271)LPV/r+RAL(N=270)
- ACTG 5273: LPV/r+NRTIs(N=255) LPV/r+RAL(N=260)
• DRV/r + RAL
– Nil
• ATV/r + RAL
– Nil
• XXV/r + DTG
– Nil
ACTG, AIDS Clinical Trials Group.

36
VL suppression
86%
76%
90%
81% 80%
92%
0%
20%
40%
60%
80%
100%
EARNESTWeek 144<400 c/mL
SECOND-LINEWeek 96
<200 c/mL
ACTG 5273Week 48
<400 c/mL
Pe
rce
nta
ge s
up
pre
sse
d
PI/NRTI PI/RAL
~ ~
EARNEST: Hakim J, et al. CROI 2015. Seattle, WA. Poster 552; SECOND-LINE: Amin J, et al. PLoS ONE 10:e0118228;ACTG 5273: La Rosa AM, et al. CROI 2016. Boston, MA. Abstract 30.

37
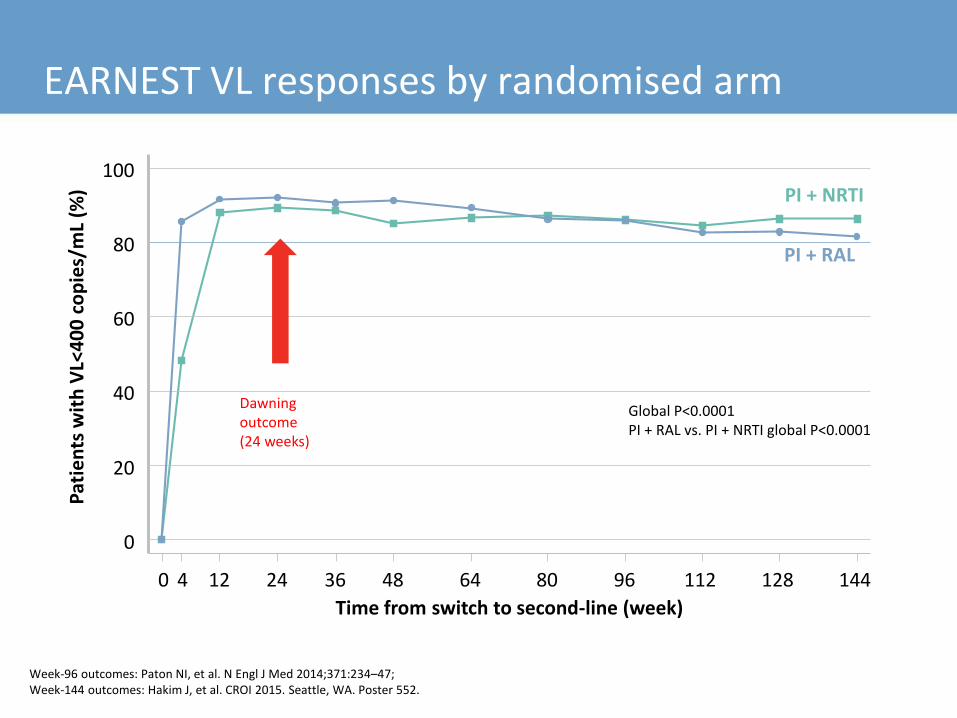
Week-96 outcomes: Paton NI, et al. N Engl J Med 2014;371:234–47;Week-144 outcomes: Hakim J, et al. CROI 2015. Seattle, WA. Poster 552.
VL responses by randomised arm
0
20
40
60
80
100
Pat
ien
ts w
ith
VL<
40
0 c
op
ies/
mL
(%)
0 4 12 24 36 48 64 80 96 112 128 144
Time from switch to second-line (week)
PI + NRTI
PI + RAL
Global P<0.0001 PI + RAL vs. PI + NRTI global P<0.0001

38
HR (PI + RAL : PI + NRTI) = 1.08 (0.81, 1.43)
Grade 3/4 AEsP
rob
abili
ty o
f re
mai
nin
gG
rad
e 3
/4 A
E-fr
ee
0.00
0.25
0.50
0.75
1.00
0 24 48 72 96Time from randomisation (week)
PI + RAL
PI + NRTI
PI + NRTI PI + RAL PI-mono
Total participants 426 433 418
Participants with Grade 3/4 AEs, n (%) 94 (22) 100 (23) 100 (24)
HR, hazard ratio.

39
Relevance of PI + INSTI as second-line regimen (for public health approach)
• Advantages
– Theoretical advantage of non-overlapping classes with first-line (but no benefit shown)
• Neutral
– Efficacy equivalent
• Good evidence for LPV/r + RAL (3RCTs)
• Don’t know about other PI + INSTI combinations
– Toxicity equivalent
• Advantage of PI/RAL may be enhanced if AZT increasingly used in second-line in PHA
• Disadvantages
– Higher cost of INSTI (RAL) vs 2NRTI
• Conclusions
– Possibly relevant for the future, but first need to show either:
• Clear virological superiority over PI/r + 2NRTI AND/OR
• Much reduced toxicity compared to PI/r + 2NRTI AND/OR
• Cost of INSTI below 2NRTI
– Clinical trial with DRV/r + DTG (vs DRV/r + 2NRTI) … may show 1 or more of these
PHA, people living with HIV/AIDS; RCT, randomised clinical trial.

PI + NRTIs in second line therapy –contribution of NRTIs

41
PI/NRTI(0) (N>149)PI/NRTI(1) (N>86)PI/NRTI(2-3) (N>17)PI + RAL (N>280)PI Monotherapy (N>374)
Within PI+NRTIs global p=0.02
88%
77%
85%81%
61%
Perc
ent
wit
h V
L<4
00
co
pie
s/m
l
Weeks from switch to second-line
0
20
40
60
80
100
0 4 12 24 36 48 64 80 96 144128112
Global p<0.0001
NRTI() = number or active(susceptible-low resistance) NRTIs
VL response by number of active NRTIs in the regimen

42
MOBIDIP trial
ELIGIBILITY Stable PI/NRTI second-line VL ≤200 copies/mLCD4 >100Adherence >90%
OUTCOME Failure:Confirmed VL ≥500 c/mLReintroduction of NRTIsPI interruption
LPV/r +3TC
LPV/r
LPV/r +3TC
DRV/r + 3TC
DRV/r
Randomisation
96-weekfollow up
Reintroduce NRTIs (2Lady) if HIV plasma RNA >500 copies/mL
after 1 month
Arm A:FTC/TDF/LPV/r
Arm B:ABC/DDI/LPV/r
Arm C:FTC/TDF/DRV/r
48-week2Lady
Ciaffi L et al. HIV Glasgow 2016. Abstract O122; https://clinicaltrials.gov/ct2/show/NCT01905059. Accessed May 2017.

43
MOBIDIP trialResults
• 265 patients randomised (133 mono, 132 dual)
• 96% M184V mutation at first-line failure
• Week 48 VL failure:
‒ Mono 22.6% (95% CI: 15.8–30.6)
‒ Dual 3.0% (95% CI: 0.8–7.6; P<0.001)
‒ Mono discontinued by DSMB
• Week 96
Ciaffi L et al. HIV Glasgow 2016. Abstract O122.
AtWeek96PI/r+3TCn=129
VL<50copies/ml,n(%) 102(79%)
VL<200copies/ml,n(%) 118(91%)
VL<500copies/ml,n(%) 123(95%)
VL<1000copies/ml,n(%) 125(97%)
http://programme.ias2017.org/Abstract/Abstract/915

INSTI + NRTIs in second-line therapy

9th IAS Conference on HIV Science; July 23-26 2017; Paris, France
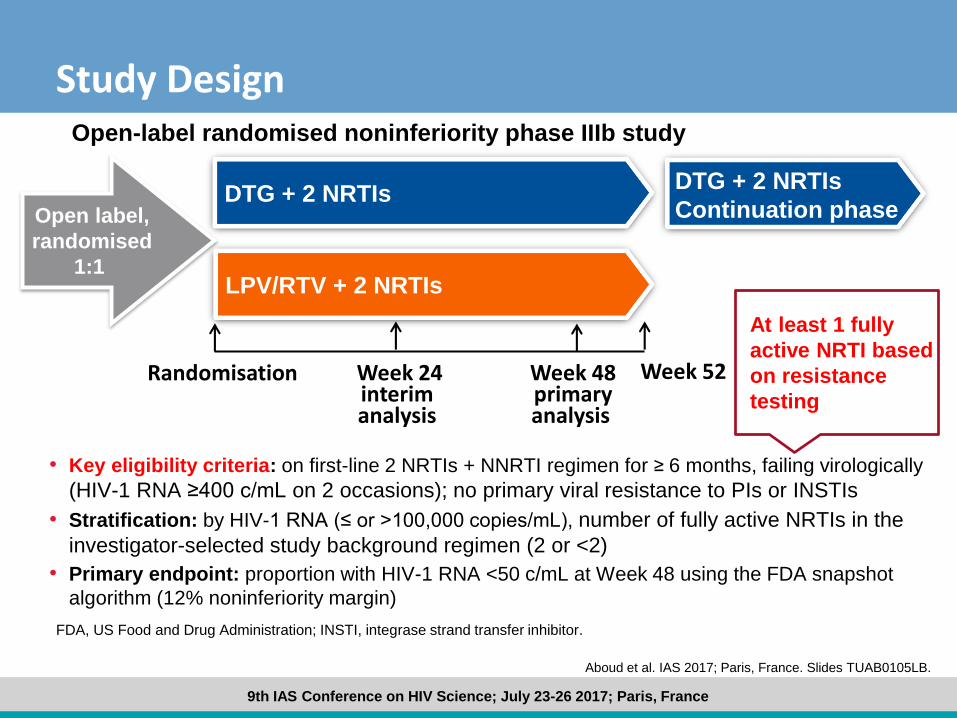
• Key eligibility criteria: on first-line 2 NRTIs + NNRTI regimen for ≥ 6 months, failing virologically
(HIV-1 RNA ≥400 c/mL on 2 occasions); no primary viral resistance to PIs or INSTIs
• Stratification: by HIV-1 RNA (≤ or >100,000 copies/mL), number of fully active NRTIs in the
investigator-selected study background regimen (2 or <2)
• Primary endpoint: proportion with HIV-1 RNA <50 c/mL at Week 48 using the FDA snapshot
algorithm (12% noninferiority margin)
Study Design
Week 48primaryanalysis
Randomisation
FDA, US Food and Drug Administration; INSTI, integrase strand transfer inhibitor.
Open-label randomised noninferiority phase IIIb study
DTG + 2 NRTIsOpen label,
randomised
1:1LPV/RTV + 2 NRTIs
DTG + 2 NRTIs
Continuation phase
Week 24interim analysis
Week 52
Aboud et al. IAS 2017; Paris, France. Slides TUAB0105LB.

• DTG + 2 NRTIs is superior to LPV/RTV + 2 NRTIs with respect to snapshot in the ITT-E (<50 c/mL) at Week 24, P<0.001
Snapshot Outcomes at Week 24: ITT-E and PP Populations
CI, confidence interval; ITT-E, intent-to-treat exposed; PP, per protocol.Aboud et al. IAS 2017; Paris, France. Slides TUAB0105LB.
82
69
86
72
0
20
40
60
80
100
Virologicsuccess
HIV
-1 R
NA
<50
c/m
L, %
DTG + 2 NRTIs (ITT-E,n=312)
LPV/RTV + 2 NRTIs(ITT-E, n=312)
DTG + 2 NRTIs (PP,n=282)
LPV/RTV + 2 NRTIs(PP, n=275)
Virologic outcomes Treatment differences (95% CI)
LPV/RTV DTG
13,8
14,5
-12-10 -8 -6 -4 -2 0 2 4 6 8 10 12 14 16 18 20 22 24
ITT-E
PP
7.3 20.3
21.08.1

Summary of Adverse Events (Randomised Phase)
Aboud et al. IAS 2017; Paris, France. Slides TUAB0105LB.
DTG + 2 NRTIs(n=314)a
LPV/RTV + 2 NRTIs(n=310)
Any adverse event, n (%) 204 (65) 231 (75)
Most common AEs (≥5% in either arm)
Diarrhoea 28 (9) 98 (32)
Upper respiratory tract infection 37 (12) 34 (11)
Nausea 11 (4) 28 (9)
Headache 22 (7) 16 (5)
Lower respiratory tract infection 11 (4) 14 (5)
Vomiting 5 (2) 17 (5)
Any neuropsych AE
Drug-related AE
19 (6)
47 (15)
15 (5)
113 (36)
All drug-related grade 2-4 AEs 9 (3) 40 (13)
Diarrhoea 1 (<1) 22 (7)
Serious AEs or deathb 17 (5) 18 (6)
Drug-related serious AEs 2 (<1) 2 (<1)
AEs leading to withdrawal 7 (2) 17 (5)aTwo patients received LPV/RTV instead of DTG + 2 NRTIs. bFour fatal SAEs: DTG + 2 NRTIs, n=1 (pneumonia); LPV/RTV, n=3 (pneumonia, encephalitis/IRIS, encephalitis).

RELEVANCE OF DAWNING TRIAL FOR THE PUBLIC HEALTH APPROACH?
9th IAS Conference on HIV Science; July 23-26 2017; Paris, France
• Key eligibility criteria: on first-line 2 NRTIs + NNRTI regimen for ≥ 6 months, failing virologically
(HIV-1 RNA ≥400 c/mL on 2 occasions); no primary viral resistance to PIs or INSTIs
• Stratification: by HIV-1 RNA (≤ or >100,000 copies/mL), number of fully active NRTIs in the
investigator-selected study background regimen (2 or <2)
• Primary endpoint: proportion with HIV-1 RNA <50 c/mL at Week 48 using the FDA snapshot
algorithm (12% noninferiority margin)
Study Design
Week 48primaryanalysis
Randomisation
FDA, US Food and Drug Administration; INSTI, integrase strand transfer inhibitor.
Open-label randomised noninferiority phase IIIb study
DTG + 2 NRTIsOpen label,
randomised
1:1LPV/RTV + 2 NRTIs
DTG + 2 NRTIs
Continuation phase
Week 24interim analysis
Week 52
Aboud et al. IAS 2017; Paris, France. Slides TUAB0105LB.
At least 1 fully
active NRTI based
on resistance
testing
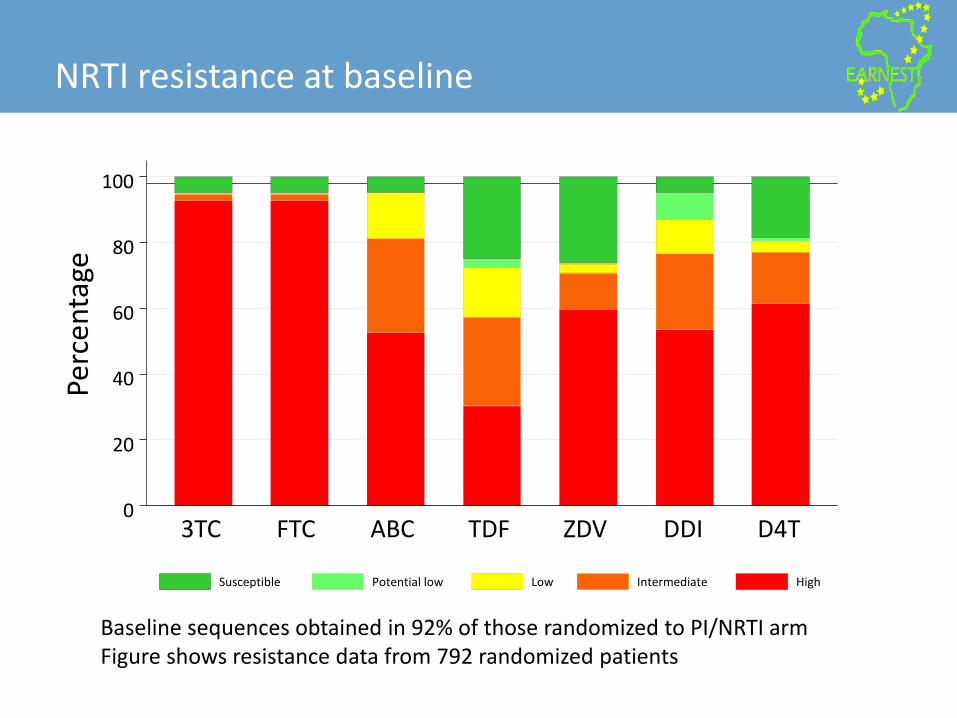
NRTI resistance at baseline
0
20
40
60
80
100
Perc
en
tage
3TC FTC ABC TDF ZDV DDI D4T
Susceptible Potential low Low Intermediate High
Baseline sequences obtained in 92% of those randomized to PI/NRTI armFigure shows resistance data from 792 randomized patients

51
Treatment simplification in second-line: How many NRTIs needed?
Paton N, et al. Lancet HIV, May 8, 2017, http://dx.doi.org/10.1016/S2352-3018(17)30065-6.
0 4 12 24 36 48 64 80 96 112 128 1440
20
40
60
80
100
VL
<40
0 c
op
ies/
mL
(%)
PI plus 0 active NRTIs (n>188)PI plus 2–3 active NRTIs (n>23)PI monotherapy (n>374)
PI plus 1 active NRTI (n>104)PI plus RAL (n>351)

9th IAS Conference on HIV Science; July 23-26 2017; Paris, France
Snapshot Outcomes by Key Baseline Subgroups at Week 24: ITT-E
8286
7074
84 83 82
6973
54 55
73
66
72
0
20
40
60
80
100
Overall ≤100,000 >100,000 2 <2 <200 ≥200
HIV
-1 R
NA
<50
c/m
L, %
DTG + 2 NRTIs
LPV/RTV + 2 NRTIs
HIV-1 RNA c/mL Fully active NRTIs
ITT-E, intent-to-treat exposed.
257/
312
215/
312
208/
242
181/
249
49/
70
34/
63
138/
166
100/
151
119/
146
Aboud et al. IAS 2017; Paris, France. Slides TUAB0105LB.
CD4+ count cells/mm3
45/
61
35/
64
212/
251
180/
248
115/
160
53
Week-96 outcomes: Paton NI, et al. N Engl J Med 2014;371:234–47;Week-144 outcomes: Hakim J, et al. CROI 2015. Seattle, WA. Poster 552.
EARNEST VL responses by randomised arm
0
20
40
60
80
100
Pat
ien
ts w
ith
VL<
40
0 c
op
ies/
mL
(%)
0 4 12 24 36 48 64 80 96 112 128 144
Time from switch to second-line (week)
PI + NRTI
PI + RAL
Global P<0.0001 PI + RAL vs. PI + NRTI global P<0.0001
Dawning outcome (24 weeks)

Compared with treatment for a lifetime…..

55
LIMITATIONS OF DAWNING TRIAL (for the public health approach)
1. Excluded people with no “fully active” NRTIs – trial population not generalizable to the public health approach
2. Excluded people with active CDC stage C conditions – trial population not generalizable to the public health approach
3. Strategy of resistance testing, regular VL monitoring (3 monthly?) not testing effects of prolonged failure –laboratory monitoring strategy of limited relevance to the public health approach
4. Duration of randomized follow-up 24 weeks (overall ≈ 36 weeks) – questionable relevance to the public health approach (or any approach to lifelong therapy)

56
Relevance of INSTI + 2NRTI as second-line regimen (for public health approach)
• Advantages
– Apparent virological advantage in short-term follow-up with DTG (vs PI + 2NRTIs)
– Apparent toxicity advantage with DTG (vs PI + 2NRTIs)
• Disadvantages
– Data are inadequate for typical populations in public health approach
– If DTG becomes first line, have no data on second line after DTG failure
– (Would not dare do this with RAL or other INSTIs)
– Have woefully inadequate long term data
• Conclusions
– Possibly relevant for the future, but need a trial relevant to the public health approach!
.

57
Potential revised ART sequence in WHO public health approach
PINRTI
PI
Standardised 1st line Standardised 2nd line≈ 3% fail/y Standardised 3rd line
NNRTI
NNRTI
DTG
58
Overall conclusions
• First-line– Lower dose EFV may become preferred regimen – DTG may be suitable for large-scale programme use (but concerns about
safety data in pregnancy)
• Second-line – PI + 2NRTI still preferred – May not need much NRTI activity: PI + 3TC may be OK (at least as switch) – PI + INSTI: no compelling case currently – INSTI + 2NRTI: early data with DTG look appealing (but study deceptive)
• Should be a high barrier for change in public health approach for RLS• Should require compelling RCT data to support change• Need to consider pragmatic issues, including monitoring support
RLS, resource-limited setting.