treatment of ewing’s sarcoma
TRANSCRIPT

Treatment of Ewing’s Sarcoma
Dr. Rajib BhattacharjeeMD PGT, IPGMER
May 22nd 2015
Introduction ….. Identified in 1921 by
James Ewing 2nd most common
bone tumor in children Ewing’s Sarcoma
Family of tumors: Ewing’s sarcoma (Bone
–87%) Extraosseous Ewing’s
sarcoma (8%) Peripheral PNET(5%) Askin’s tumor
• 2% of all childhood malignancies
Occurs most commonly in 2nd decade◦ 80% occur between
ages 5 and 25 M:F 1.3:1 < 10 yrs
1.6:1 > 10 yrs
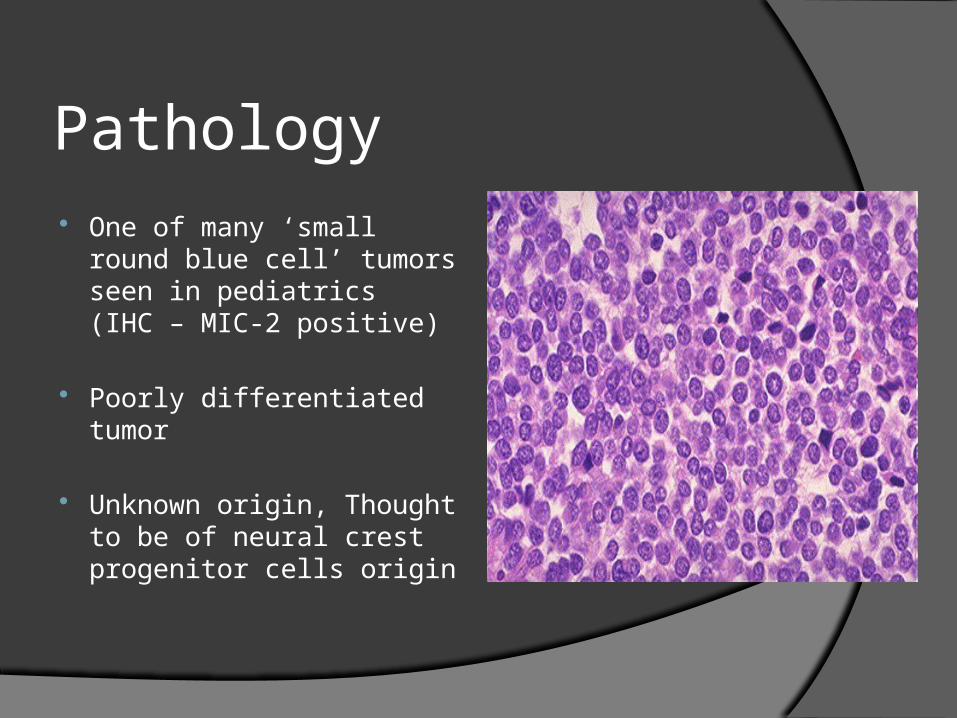
Pathology
One of many ‘small round blue cell’ tumors seen in pediatrics (IHC – MIC-2 positive)
Poorly differentiated tumor
Unknown origin, Thought to be of neural crest progenitor cells origin
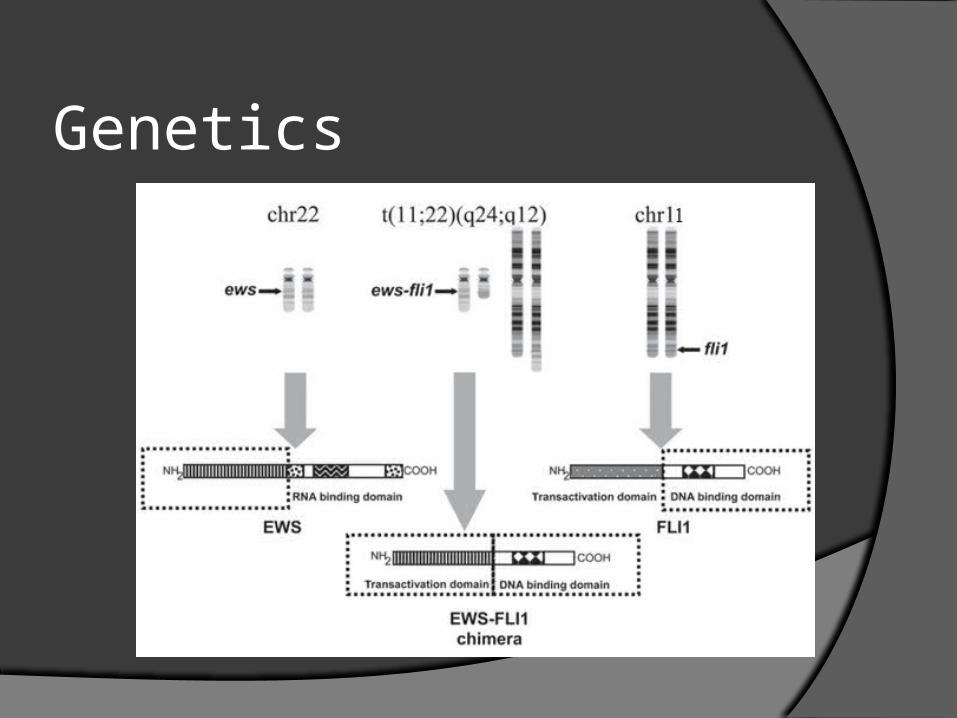
Genetics

Clinical presentation
Pain & swelling of affected area
May also have systemic symptoms: Fever Anemia Weight loss
Pathological fracture

Routes of spread Direct extension into
adjacent bone or soft tissue.
Metastases generally spread through bloodstream
25% present with metastatic diseaseLungsBoneBone Marrow
Nearly all pts. have micro-metastasis at diagnosis, so all need chemotherapy.

Diagnostic & staging work up
-LDH-LFT
-CBC, KFT, LFT,-LDH
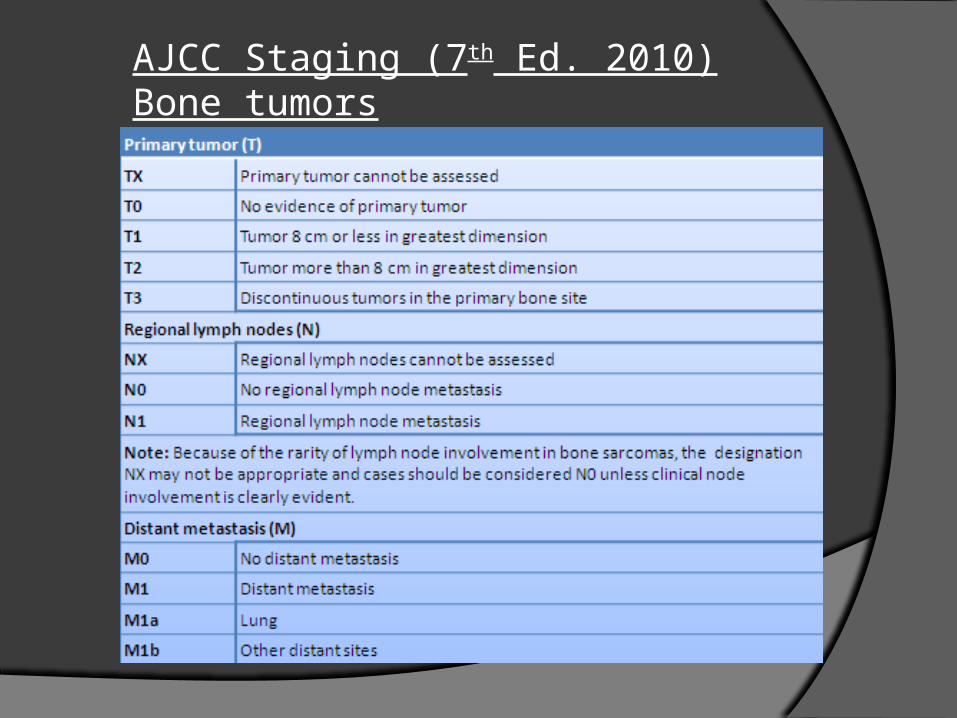
AJCC Staging (7th Ed. 2010) Bone tumors

Prognostic factors
Patient factors
•Age •sex
Tumor characteristics•Site •Size/volume•Pretreatment necrosis•Metastasis•Serum LDH•Cytogenetics •Molecular characteristics•2nd malignancy
Treatment related issues
•Response to induction•“surgery not a part of local treatment”

Treatment of Ewing Sarcoma
Induction chemotherapy
Local therapySurgery
Radiation
Maintenancechemotherapy
Chemotherapy
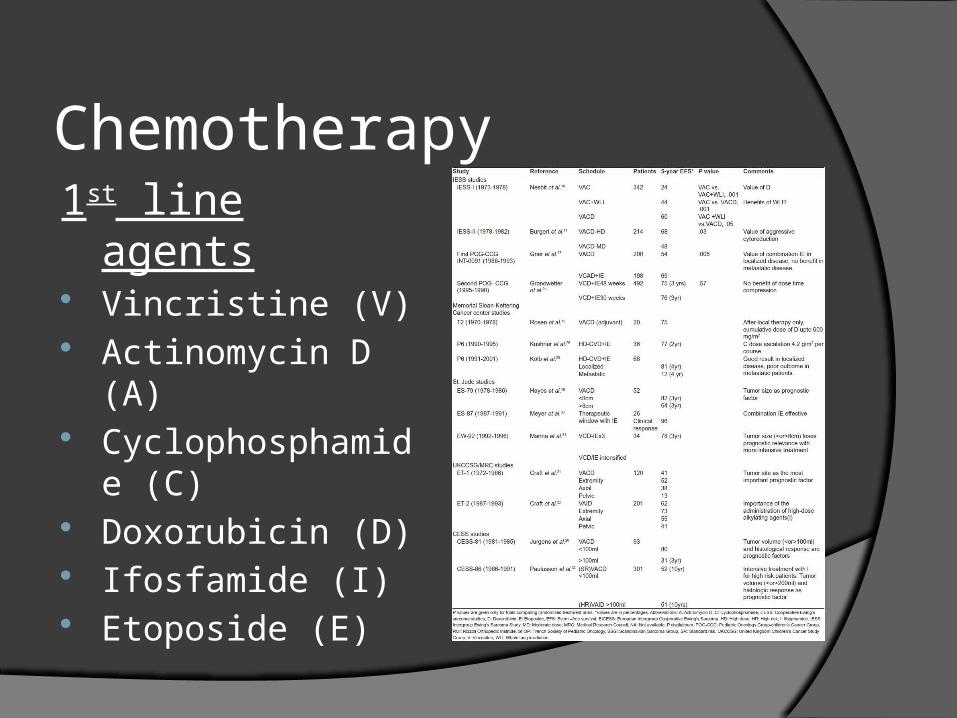
1st line agents Vincristine (V) Actinomycin D (A) Cyclophosphamide
(C) Doxorubicin (D) Ifosfamide (I) Etoposide (E)

Historical perspective
Pre-chemotherapy era – 5Y OS <10% Chemotherapy – 5 Y OS >40% 1962 - Sutow and Sullivan - use of
cyclophosphamide Hustu et al. - Vincristine and
Cyclophosphamide. 1974 - Rosen et al.(MSKCC) – VACD
Regimen
5 Y OS (‘73-’77) – 36%
5 Y OS (‘93-’97) – 59%

Multiagent chemotherapyIESS-I (Nesbit et al.)
1973-1978
Schedule 5Y EFS
VAC 24%
VAC+WLI 44%
VACD 60%
CONCLUSION - Addition of Doxorubicin provides clear survival advantage
IESS-II
1978-1982
schedule 5Y EFS
VACD-HD 68%
VACD-MD 48%
CONCLUSION – Intermittent high dose VACD is superior to continuous moderate dose therapy

American Intergroup Ewing’s trial (INT-0091 - POG-8850/CCG-7881)
localized Ewing’s Sarcoma
VD(A)C/IE VD(A)C
69% 5 Y EFS 54%
CONCLUSION – Addition of IE has advantage in:-
localized disease
large tumors
pelvic primary

Dose dense approach Children’s Oncology Group AEWS-0031 study
localized Ewing’s Sarcoma
dose dense therapy standard therapy
VD(A)C/IE VD(A)C/IE
q 14 days q 21 days
73% 5 Y EFS 65%
CONCLUSION – Dose dense VD(A)C/IE with G-CSF support is the standard of care in localized Ewing’s sarcoma

Standard Schedule
Vincristine 1.2mg/m2
• IV D1
Doxorubicin 75mg/m2
• IV D1
Cyclophosphamide 1200mg/m2
• IV D1
Ifosfamide 1800mg/m2
• IV D1-D5
Etoposide 100mg/m2
• IV D1-D5 • Alternate 2 week cycle • G-CSF support• Total duration of chemotherapy is 30 weeks• Local therapy after 12 weeks• Replace Doxorubicin by Actinomycin-D(1.2mg/m2) on 11th cycle

Local control
“ the first indication is for treatment by radiation in full doses, and over considerable periods. This recommendation is based on the reported cure of certain cases….by radiation alone, and on the clinical disappearance of the disease by variable periods in many more cases. The response to radiation also confirms the diagnosis….”
James Ewing, 1940
“ Neoplastic Diseases”, 4th Edn

Surgery vs RT as local therapy
Disadvantages of RT Secondary
malignancies Effect on growth
plates
Advantages of surgery Limb salvage Structural bone
function preservation

Choice of local therapy : Surgery vs RT

Surgery or radiotherapy ???
Local recurrence rate – after surgery - 7.5%
after definitive RT - 26.3%

Unfair bias against RT Recurrence rate after RT is
strongly correlated with the primary site
Extremities – 5 to 10%
Pelvis – 15 to 70%
Tumor size is strongly related to Recurrence rates
< 8cms = ≤ 80%
> 8cms = 90 %
Combined modality trials are
designed to evaluate
[RT Vs Surgery + RT] not [Surgery Vs Surgery + RT]
Quality of the RT delivered in some negative trials is doubtful
Surgical series always select patients at low-risk (e.g. Extremity lesions with low volume disease)
Second malignancies are related not to RT alone but to chemotherapy as well (Anthracyclines & alkylating agents)
Conclusion Ewing’s sarcoma is a radiation responsive malignancy.
No randomized trials compared Radiotherapy to surgery for local control of Ewing’s sarcoma.
Radiotherapy can achieve local control, but complete surgery when feasible has to be regarded as the first choice of local therapy.**
**ESMO clinical practice Guidelines for diagnosis, treatment and follow-up for Bone sarcomas.
Ref. Annals of Oncology 21 (Supplement 5) 13,2010
Surgery as local therapy Surgical Indications
Expendable bone (fibula, rib, clavicle) Bone defect able to be reconstructed with modest loss of
function May consider amputation if considerable growth
remaining After pre-op RT
Limb-salvage surgery is preferred.
Curative surgery requires wide local excision and negative margin Bony margins of at least 1 cm. Soft tissue margin of at least 5mm.
Radiotherapy in Ewing’s Sarcoma

Indications of RTDefinitive Radiation therapy Unresectable tumor
Inaccessible site
Patient with poor surgical risk
Patient refusing surgery
Indications of RTPost-operative Radiation Therapy Intra-Lesional Resection
Marginal Resection
Wide-resection with Poor Histological response to Neo-adjuvant Chemotherapy (>10% viable tumor cells in the specimen)
Based on CESS-81, CESS-86, EICESS-92 Studies : Schuck et al,IJROBP-1998 & 2003

Indications of RT
Pre-operative Radiation Therapy
When Narrow resection margins are expected
Principle : To sterilize the tumor compartment before surgery & to potentially reduce the risk of dissemination during surgery
Local recurrence with pre-op RT : <5%
EI-CESS-92 : Schuck et al – IJROBP-1998 & 2003

Radiotherapy techniques Patient position - supine, prone or
lateral. Energy – Co-60, 6MV LINAC. Tailored portals for every patient. Field should not cross joints unless
essential. Strip(1-2cm) of normal tissue spared
for lymph drainage.

Schematic depiction of GTV1 (pre-induction bone and pre-induction soft tissue extent) and GTV2 (post-induction soft tissue extent)

Planning Definitive RT
◦ PHASE 1: Gross tumor in bone and soft tissue (pre chemo ) + 2-
4 cm longitudinal margins + 2 cm lateral margins.
Dose:45 Gy @1.8Gy/#.
◦ PHASE 2 :
Cone down to original bony extent + 2 cm margins
Complete response - 45 Gy (no boost)
Chemotherapy response > 50% - 55.8 Gy (10.8Gy/6#)
Chemotherapy response < 50% - 59.4 Gy (14.4Gy/8#)

Post operative RT planningPHASE 1
Pre chemo GTV + surgical scar + 2cm margin – 45 Gy
PHASE 2
resection histological response boost dose
R0 100% no Adj RT
< 100% no boost
R1 100% no boost
< 100% 5.4 Gy/3#
R2 100% 5.4 Gy/3#
< 100% 10.8 Gy/6#
---------------------------------------------------------------------------------------------
Pre operative RT planning Pre chemo GTV + 2 cm margin – 36-45 Gy

Chest wall primaries with pleural involvement
Phase 1HEMITHORAX IRRADIATION15-20 Gy(1.5-1.8Gy/#)
Phase 2Cone down primary siteDose based on resection margins

Proton beam therapy
Spares normal tissues
No evidence of enhanced functional outcome or reduced risk of secondary malignancy
Effect on local recurrence uncertain
Rombi, Barbara, et al. "Proton radiotherapy for pediatric Ewing’s sarcoma: initial clinical outcomes." International Journal of Radiation Oncology* Biology* Physics 82.3 (2012): 1142-1148.

Surveillance
Physical examination, CXR
• Every 2- 3 months• Increase interval after 24 months• Annually after 5 years indefinitely
CBC & other lab works as indicated
Bone scan & FDG-PET
# NCCN

Relapse
30% of patients develop relapse with survival < 20%
• Median time to relapse – 16-21 months
Late relapse ( >2 years)
• Repeat the same regimen
Early relapse ( <2years)• Survival <10%• No established salvage regimen• Cyclophosphamide & Topotecan; Irinotecan &
Temozolomide; Ifosfamide, Carboplatin & Etoposide; Gemcitabine & Docetaxel
• Myeloablative chemotherapy

Metastasis
Metastasis 5 Y RFS
Lung 29%
Bone & bone marrow 19%
Both 8%

Metastatic disease
The addition of Ifosfamide & Etoposide in the metastatic group provided no survival advantage
# NEJM 2003

Lung bath
Whole lung irradiation
After completion of chemotherapy/ metastasectomy
>14 years - 18Gy @ 1.5Gy/#
<14 years - 15Gy @ 1.5Gy/#
< 6 years – 12 Gy@ 1.5Gy/#
Paulussen, M., et al. "Primary metastatic (stage IV) Ewing tumor: survival analysis of 171 patients from the EICESS studies." Annals of oncology 9.3 (1998): 275-281.

Disseminated metastasesDisseminated disease
Approach 3 Y EFS
Both 47%
Surgery 25%
RT 23%
No local T/t 13%
Conclusion – adequately treat primary and all the metastasis.
Disseminated bone mets
Approach 3Y EFS
RT to mets site 35%
No local therapy 16%
Conclusion – treat all lesions in disseminated bone metastases. (whole body MRI f/b compartmental irradiation upto 54 Gy)
# Haeusler, Julia, et al. "The value of local treatment in patients with primary, disseminated, multifocal Ewing sarcoma (PDMES)." Cancer 116.2 (2010): 443-450.

Treatment in a nutshell
Localized disease
Induction chemo (DDVAC/IE)
12 weeks
Surgery or Radiotherapy
Adj RT
Maintenance chemo
(DDVAC/IE)
18 weeks
Metastatic disease
Treatment of primary (Local T/t)
local T/t of the metastatic site
(bone irradiation, WLI)
___________________________
Follow up Relapse
2nd line chemo Myeloablative therapy

Extra-osseous Ewing’s Sarcoma
Traditional approach
• Treat EOES as Rhabdomyosarcoma
• Regimen:- I - Ifosfamide V - Vincristine A - Actinomycin-D

To Dox or not to Dox; that is the question !!!
Extraosseous Ewing’s Sarcoma
MMT strategy OET strategy No Anthracyclin Anthracyclin
59% OS 83%
44% EFS 75%
CONCLUSION – The regimen of osseous Ewing’s sarcoma may be used in extraosseous Ewing’s sarcoma
Sequelae of treatment
Radiation Premature closure of
epiphysis Pathologic fractures Decrease range of
motion due to fibrosis Skin changes Lymphoedema Infertility Second malignancies
Chemotherapy Secondary leukemia Bladder toxicity Cardiotoxicity SIADH

Future directions Use of 3D-CRT / IMRT as a standard protocol
PET scan shows potential in both diagnosis and treatment
Proton therapy needs further evaluation
TARGETED therapy : against IGF1 or IGF1R Small molecule therapy – Mithramycin inhibits EWS-
FLI1 downstream targets (including c-myc)
YK-4-279 stops EWS-FLI fusion protein from sticking to RNA Helicase A
Thank you