treatment of complicated urinary tract infections with lomefloxacin
TRANSCRIPT

ANTIMICROBIAL AGENTS AND CHEMOTHERAPY, June 1994, p. 1368-13730066-4804/94/$04.00+0Copyright C) 1994, American Society for Microbiology
Treatment of Complicated Urinary Tract Infections withLomefloxacin Compared with That with
Trimethoprim-SulfamethoxazoleLINDSAY E. NICOLLE,l* TOM J. LOUIE,2 JACQUES DUBOIS,3 ALAIN MARTEL,4
GODFREY K. M. HARDING,' AND CHRISTIAN P. SINAVE5University of Manitoba, Winnipeg, Manitoba,1 University of Calgary, Calgary, Alberta,2 University of Sherbrooke,
Sherbrooke,3 and Laval University, Quebec City,4 Quebec, and Memorial University,St. John's, Newfoundland,5 Canada
Received 20 December 1993/Returned for modification 23 February 1994/Accepted 31 March 1994
The efficacy of lomefloxacin given at 400 mg once daily for 14 days compared with that of trimethoprim-sulfamethoxazole at 160 and 800 mg, respectively, given twice daily for 14 days in the treatment of symptomaticcomplicated urinary tract infections was studied in a prospective, randomized, single-blind multicenter study.A total of 133 subjects presenting with signs and symptoms of urinary tract infection and an underlyingabnormality consistent with complicated urinary tract infection were enrolled in the study. Bacteriologic curewas significantly better in 68 subjects randomized to lomefloxacin than in 65 subjects randomized totrimethoprim-sulfamethoxazole at short-term follow-up (88 versus 52%; 95% confidence intervals [CIs] 77 and94% and 39 and 65%, respectively) this difference was no longer significant at long-term follow-up (64 versus
47%; CIs, 52 and 75% and 32 and 57%, respectively). Clinical outcomes were similar for both therapeuticregimens at short- and long-term follow-ups. The organisms that infected the subjects pretherapy were more
frequently resistant to trimethoprim-sulfamethoxazole, and drug therapy was discontinued more frequently insubjects treated with trimethoprim-sulfamethoxazole because of adverse antimicrobial effects. In secondaryanalyses, outcomes did not differ with age or underlying genitourinary abnormality. Lomefloxacin was,however, superior to trimethoprim-sulfamethoxazole for the eradication of gram-negative organisms at bothshort- and long-term follow-ups (bacteriologic cure rates, 96% [CI, 91 and 100%/] versus 70% [CI, 56 and 84%]and 86% [CI, 81 and 91%] versus 59% [CI, 45 and 73%]) and for bacteriologic cure for the 41 men enrolledin the study (bacteriological cure rates, 95% [CI, 73 and 98%] versus 43% [CI, 23 and 66%] at short-termfollow-up and 80%o [CI, 56 and 93%] versus 25% [CI, 12 and 52%] at long-term follow-up). Lomefloxacin issuperior to trimethoprim-sulfamethoxazole for the treatment of symptomatic complicated urinary tractinfection and for bacteriologic eradication at short-term follow-up. At long-term follow-up, a bacteriologicbenefit remained for eradication of the initial infecting gram-negative organisms and for men.
Complicated urinary tract infection is defined as a urinarytract infection in the presence of structural or functionalabnormalities of the genitourinary tract (8). These usuallyinclude abnormalities associated with obstruction, includingstones, strictures, or tumors as well as indwelling catheters orurodynamic abnormalities leading to impaired voiding. Thetreatment of complicated urinary tract infection is generallyless successful than treatment of uncomplicated urinary tractinfection. The reasons for this include the underlying abnor-malities, particularly obstruction, which may prevent organismeradication; the tendency for recurrent infections if the under-lying abnormality is not corrected; and the presence of organ-isms with increasing levels of resistance to antimicrobial agentsafter repeated courses of antimicrobial therapy for previousinfections. The recommended duration of therapy of 10 to 14days for complicated urinary tract infection is longer than thatfor uncomplicated urinary infection, reflecting the difficulty oftherapy for complicated urinary tract infections. Even withappropriate antimicrobial therapy, recurrence rates of 50% at4 to 6 weeks posttherapy are the expected outcome (8).
Lomefloxacin is a fluoroquinolone antimicrobial agent witha wide spectrum of activity, including activity against most
* Corresponding author. Mailing address: Health Sciences Centre,MS673-820 Sherbrook Street, Winnipeg, Manitoba R3A 1R9, Canada.Phone: (204) 787-4655. Fax: (204) 787-4699.
gram-negative organisms which are important uropathogens(12). The antimicrobial agent has a prolonged half-life, per-mitting once-daily dosing (10). The study described here wasundertaken to compare the efficacy of orally administeredlomefloxacin in the treatment of symptomatic complicatedurinary tract infection in comparison with that of trimeth-oprim-sulfamethoxazole, a widely used standard oral antimi-crobial agent for the treatment of urinary tract infections.
(The study described here was presented in part at the 30thInterscience Conference on Antimicrobial Agents and Chemo-therapy, Atlanta, Ga., 21 to 24 October 1990, and the 4thInternational Symposium on New Quinolones, Munich, Au-gust 1992.)
MATERIALS AND METHODS
Study subjects. Study subjects were recruited from bothinpatients and outpatients at five Canadian medical centers.Subjects of either sex aged 18 to 65 years were eligible forenrollment in the study if they presented with at least twosymptoms or signs of symptomatic urinary tract infection,including dysuria, frequency, urgency, suprapubic pain, fever(>380C), hematuria, low back pain, or costovertebral angletenderness and if 2105 CFU of organisms was found per ml ofurine. To fulfill the criteria for a diagnosis of complicatedurinary tract infection, at least one the following had to be
1368
Vol. 38, No. 6
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/a
ac o
n 06
Jan
uary
202
2 by
179
.97.
17.1
76.

TREATMENT OF COMPLICATED URINARY TRACT INFECTIONS 1369
TABLE 1. Demographic characteristics, infecting organisms, andunderlying urinary tract abnormalities of subjects enrolled in
the study
Characteristic
Median age ([range] yrs)
Caucasian (no.[%])
Female (no. [%])
Infecting organism
(no. [%] of organisms)Escherichia coliKlebsiella spp.
Citrobacter spp.
Enterobacter spp.
Proteus mirabilisPseudomonas aeruginosaOther gram-negative organismsStaphylococcus aureus
Coagulase-negativestaphylococciStreptococcus spp. or
Enterococcus spp.
Underlying abnormalities(no. [%] of subjects)aNeurogenic bladderUrologic instrumentationObstructionUrologic malignancyCalculusRelapsing pyelonephritisBenign prostatic hypertrophyPolycystic kidney disease
Therapeutic regimen
Lomefloxacin Trimethoprim-(n= 68) sulfamethoxazole
~(n 65)
71 (23-94) 70(24-100)
60 (88) 63 (97)
48(71) 44 (68)
46(61)8(11)4(5.3)4(5.3)4(5.3)1 (1.3)2 (2.6)2 (2.6)2 (2.6)
3 (3.9)
31 (45)31 (46)5 (7.4)4(5.9)3 (4.4)7(10)6 (8.8)1 (1.5)
34 (48)6(8.5)5 (7.0)4(5.6)6(8.5)2 (2.8)7 (9.9)1 (1.4)0
6 (8.5)
34 (52)28 (43)5 (4.6)2(3.1)4(6.1)5 (7.8)8(12)0
a Some subjects had more than one abnormality.
known to be present prior to enrollment in the study: obstruc-tion, neurogenic bladder, calculus, urologic malignancy, benignprostatic hypertrophy, relapsing pyelonephritis, urologic in-strumentation within the previous 4 weeks, or polycystic kidneydisease. Written informed consent was obtained from thesubjects prior to enrollment in the study.For female subjects, exclusion criteria included pregnancy,
breastfeeding, or the lack of use of a reliable means ofcontraception in premenopausal women. Subjects were alsoexcluded if they were terminally ill or had other conditionsprecluding evaluation of the response to therapy; had a
favorable response to prior antimicrobial therapy for thepresent episode or were currently receiving concomitant anti-microbial therapy; had a history of hypersensitivity to thefluoroquinolones, trimethoprim, or sulfonamides; had a serum
creatinine level of greater than 1.5 times the upper limit ofnormal or hepatic enzyme elevations more than twice theupper limit of normal; had concomitant infections which couldconfuse interpretation of the results; had a prior history ofconvulsive disorders; had received mineral antacid therapywithin 48 h of the initial dosing or required antacid therapyduring the study; required concomitant fenbufen; had a
chronic indwelling bladder catheter or an ileal loop conduit;had documented or suspected bacteremia; had received otherinvestigational drugs within 4 weeks; or had a known glucose6-phosphate dehydrogenase deficiency.
Study design and therapeutic regimens. The study was aprospective, randomized, single-blind comparative evaluationof 400 mg of lomefloxacin administered orally once daily and160 and 800 mg of trimethoprim-sulfamethoxazole, respec-tively, administered orally twice daily. Randomization wasperformed centrally for each site in a one-to-one ratio, withpatients enrolled sequentially at the different centers. Subjectsrandomized to lomefloxacin received one medication bottlecontaining 28 capsules of 200 mg each with instructions to takea single daily dose of two capsules in the morning. Subjectsrandomized to trimethoprim-sulfamethoxazole received a bot-tle of 28 tablets each containing 160 and 800 mg of trimeth-oprim-sulfamethoxazole, respectively, with instructions to takeone tablet every 12 h. The duration of therapy was 10 to 14days. The identity of the treatment to which the patient wasassigned was concealed from the study investigators, and thedrug was dispensed by a pharmacy or through a study nurse.Patients were instructed, should they have any questions withrespect to the medication, to discuss the medications with thepharmacist or study nurse and not to mention the dosage ordosing schedule to the investigator.
Microbiologic methods. Urine specimens were obtained by aclean-catch or catheter method. Quantitative urine culturewith organism identification was performed by standard meth-ods at the clinical microbiology laboratory at each study center.Susceptibility testing was done by the Kirby-Bauer disk diffu-sion method or microdilution (6, 7). Breakpoints for suscepti-bility were a zone size of l18 mm and an MIC of .8,ug/ml forlomefloxacin and a zone size of .16 mm or MICs of .4 and 76,ug/ml, respectively, for trimethoprim-sulfamethoxazole.
Monitoring. Baseline clinical and laboratory data wereobtained within 48 h prior to the initiation of antimicrobialtherapy and included a history, physical examination, testing ofa urine specimen by culture and susceptibility testing, andstandard biochemical and hematologic laboratory evaluations.Urine specimens were obtained for culture within 48 h prior tothe initiation of therapy, days 2 to 4 after administration of thefirst antimicrobial dose, and days 5 to 9 posttreatment andweeks 4 to 6 posttreatment. Study subjects were assessedclinically prior to therapy, at 2 to 4 days after the initiation oftherapy, and at both short-term and long-term follow-up visits.At these visits, subjects were examined for signs and werequestioned with respect to signs and symptoms of infection orpotential adverse events.
Subjects infected with pathogens at the initial baselineexamination that were subsequently found to be resistant toboth lomefloxacin and trimethoprim-sulfamethoxazole werewithdrawn from the study. For patients who were empiricallystarted on therapy and in whom the initial pathogen wassubsequently found to be resistant to one but not both studydrugs, the blind was broken. Patients receiving an antimicro-bial agent to which their organism was susceptible werecontinued on therapy, but therapy with the study medicationwas discontinued for those receiving an agent to which theinfecting organism was resistant and were considered treat-ment failures.
Definitions and data analysis. Assessment of efficacy wasperformed at the short-term (5- to 9-day) and long-term (4- to6-week) posttherapy visits. Definitions for bacteriologic effec-tiveness included cure if the initial pathogen was eradicatedwith therapy and was not subsequently isolated in any quanti-tative counts of >104 CFU/ml at either follow-up visit andreinfection if the initial pathogen was eradicated but a differentpathogen (2105 CFU/ml) was isolated posttherapy. The or-ganism was considered to be eradicated if the patient wascured or reinfected. Failure was the presence of the initial
VOL. 38, 1994
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/a
ac o
n 06
Jan
uary
202
2 by
179
.97.
17.1
76.
ANTIMICROB. AGENTS CHEMOTHER.
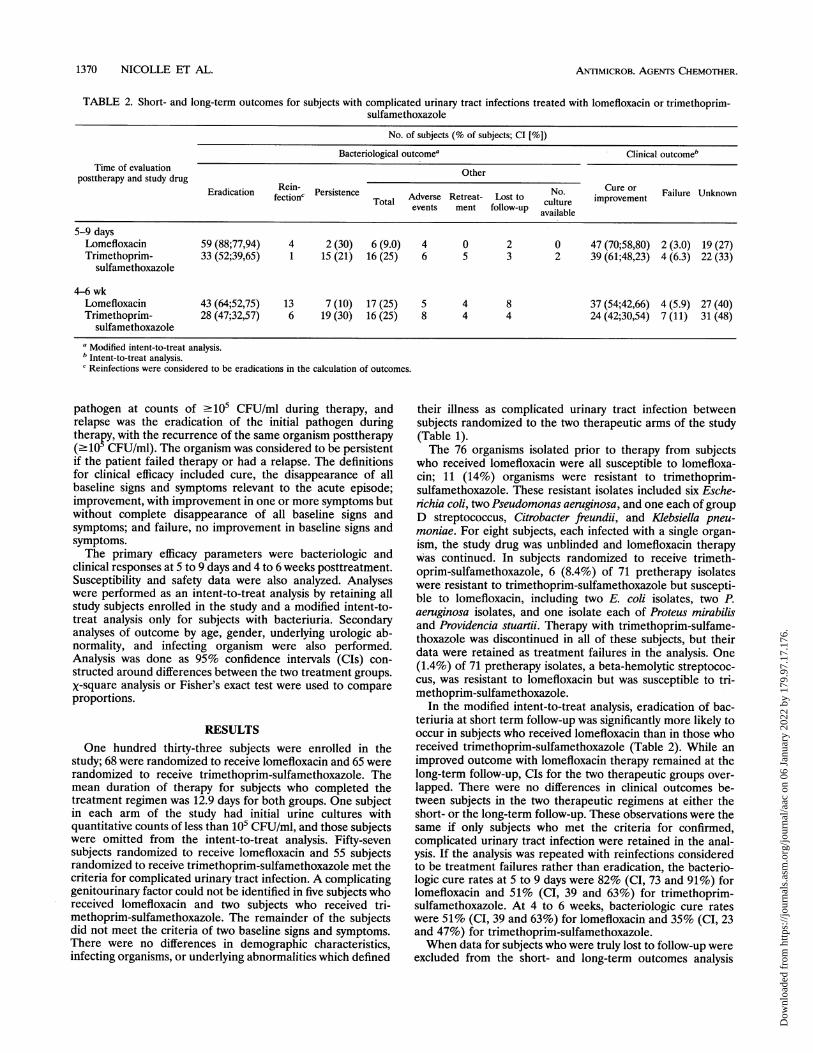
TABLE 2. Short- and long-term outcomes for subjects with complicated urinary tract infections treated with lomefloxacin or trimethoprim-sulfamethoxazole
No. of subjects (% of subjects; CI [%])
Bacteriological outcomea Clinical outcome'Time of evaluation Other
posttherapy and study drugEradication Ri-PersistenceNo Cuer FaleUnowfectionc Total Adverse Retreat- Lost to cuNtore improvement
eventsmet
follow-up available5-9 days
Lomefloxacin 59 (88;77,94) 4 2 (30) 6 (9.0) 4 0 2 0 47 (70;58,80) 2 (3.0) 19 (27)Trimethoprim- 33 (52;39,65) 1 15 (21) 16 (25) 6 5 3 2 39 (61;48,23) 4 (6.3) 22 (33)
sulfamethoxazole
4-6 wkLomefloxacin 43 (64;52,75) 13 7 (10) 17 (25) 5 4 8 37 (54;42,66) 4 (5.9) 27 (40)Trimethoprim- 28 (47;32,57) 6 19 (30) 16 (25) 8 4 4 24 (42;30,54) 7 (11) 31 (48)
sulfamethoxazolea Modified intent-to-treat analysis.b Intent-to-treat analysis.c Reinfections were considered to be eradications in the calculation of outcomes.
pathogen at counts of 2105 CFU/ml during therapy, andrelapse was the eradication of the initial pathogen duringtherapy, with the recurrence of the same organism posttherapy(210 CFU/ml). The organism was considered to be persistentif the patient failed therapy or had a relapse. The definitionsfor clinical efficacy included cure, the disappearance of allbaseline signs and symptoms relevant to the acute episode;improvement, with improvement in one or more symptoms butwithout complete disappearance of all baseline signs andsymptoms; and failure, no improvement in baseline signs andsymptoms.The primary efficacy parameters were bacteriologic and
clinical responses at 5 to 9 days and 4 to 6 weeks posttreatment.Susceptibility and safety data were also analyzed. Analyseswere performed as an intent-to-treat analysis by retaining allstudy subjects enrolled in the study and a modified intent-to-treat analysis only for subjects with bacteriuria. Secondaryanalyses of outcome by age, gender, underlying urologic ab-normality, and infecting organism were also performed.Analysis was done as 95% confidence intervals (CIs) con-structed around differences between the two treatment groups.X-square analysis or Fisher's exact test were used to compareproportions.
RESULTSOne hundred thirty-three subjects were enrolled in the
study; 68 were randomized to receive lomefloxacin and 65 wererandomized to receive trimethoprim-sulfamethoxazole. Themean duration of therapy for subjects who completed thetreatment regimen was 12.9 days for both groups. One subjectin each arm of the study had initial urine cultures withquantitative counts of less than 105 CFU/ml, and those subjectswere omitted from the intent-to-treat analysis. Fifty-sevensubjects randomized to receive lomefloxacin and 55 subjectsrandomized to receive trimethoprim-sulfamethoxazole met thecriteria for complicated urinary tract infection. A complicatinggenitourinary factor could not be identified in five subjects whoreceived lomefloxacin and two subjects who received tri-methoprim-sulfamethoxazole. The remainder of the subjectsdid not meet the criteria of two baseline signs and symptoms.There were no differences in demographic characteristics,infecting organisms, or underlying abnormalities which defined
their illness as complicated urinary tract infection betweensubjects randomized to the two therapeutic arms of the study(Table 1).The 76 organisms isolated prior to therapy from subjects
who received lomefloxacin were all susceptible to lomefloxa-cin; 11 (14%) organisms were resistant to trimethoprim-sulfamethoxazole. These resistant isolates included six Esche-richia coli, two Pseudomonas aeruginosa, and one each of groupD streptococcus, Citrobacter freundii, and Klebsiella pneu-moniae. For eight subjects, each infected with a single organ-ism, the study drug was unblinded and lomefloxacin therapywas continued. In subjects randomized to receive trimeth-oprim-sulfamethoxazole, 6 (8.4%) of 71 pretherapy isolateswere resistant to trimethoprim-sulfamethoxazole but suscepti-ble to lomefloxacin, including two E. coli isolates, two P.aeruginosa isolates, and one isolate each of Proteus mirabilisand Providencia stuartii. Therapy with trimethoprim-sulfame-thoxazole was discontinued in all of these subjects, but theirdata were retained as treatment failures in the analysis. One(1.4%) of 71 pretherapy isolates, a beta-hemolytic streptococ-cus, was resistant to lomefloxacin but was susceptible to tri-methoprim-sulfamethoxazole.
In the modified intent-to-treat analysis, eradication of bac-teriuria at short term follow-up was significantly more likely tooccur in subjects who received lomefloxacin than in those whoreceived trimethoprim-sulfamethoxazole (Table 2). While animproved outcome with lomefloxacin therapy remained at thelong-term follow-up, CIs for the two therapeutic groups over-lapped. There were no differences in clinical outcomes be-tween subjects in the two therapeutic regimens at either theshort- or the long-term follow-up. These observations were thesame if only subjects who met the criteria for confirmed,complicated urinary tract infection were retained in the anal-ysis. If the analysis was repeated with reinfections consideredto be treatment failures rather than eradication, the bacterio-logic cure rates at 5 to 9 days were 82% (CI, 73 and 91%) forlomefloxacin and 51% (CI, 39 and 63%) for trimethoprim-sulfamethoxazole. At 4 to 6 weeks, bacteriologic cure rateswere 51% (CI, 39 and 63%) for lomefloxacin and 35% (CI, 23and 47%) for trimethoprim-sulfamethoxazole.When data for subjects who were truly lost to follow-up were
excluded from the short- and long-term outcomes analysis
1370 NICOLLE ET AL.
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/a
ac o
n 06
Jan
uary
202
2 by
179
.97.
17.1
76.
TREATMENT OF COMPLICATED URINARY TRACT INFECTIONS 1371
rather than retained as treatment failures, the bacteriologiccure rates at short-term follow-up were 91% (Cls, 84 and 98%)for lomefloxacin and 57% (CI, 44 and 70%) for trimethoprim-sulfamethoxazole (Table 2). At the long-term follow-up, thebacteriologic cure rates were 73% (CI, 62 and 84%) and 47%(CI, 34 and 60%) for lomefloxacin and trimethoprim-sulfame-thoxazole,' respectively. Two subjects who received trimeth-oprim-sulfamethoxazole and from whom no organism wasisolated in cultures at 5 to 9 days posttreatment were areinfection and a cure, respectively; at the long-term follow-up.The organisms isolated from subjects with reinfections at
short-term follow-up were one each of E. coli, P. aeruginosa, C.freundii, and Enterococcus sp. in subjects who received lome-floxacin and an E. coli isolate in a subject who receivedtrimethoprim-sulfamethoxazole. At long-term follow-up, theorganisms isolated from subjects who received lomefloxacinincluded six Enterococcus spp, two Citrobacter spp., and a
coagulase negative staphylococcus. From subjects who re-ceived trimethoprim-sulfamethoxazole, two isolates each ofEnterococcus spp. and K pneumoniae and one P. aeruginosaisolate were isolated. All of these isolates were susceptible tothe study drug received by the subject, with the exception ofthe E. coli organism isolated at the short-term follow-up in asubject who received trimethoprim-sulfamethoxazole and agroup D streptococcus isolated at the long-term follow-upfrom a subject who received lomefloxacin.
Sixteen (24% of the total) of 68 subjects who receivedlomefloxacin and 25 (38%) of 65 subjects who received tri-methoprim-sulfamethoxazole had any adverse event (X2 =
3.47; P = 0.06); the adverse events in 10 (15% of subjects) and18 (28%) of these subjects, respectively, were moderate orsevere in intensity. Nine subjects (13%) in the lomefloxacingroup and 13 subjects (20%) who received trimethoprim-sulfamethoxazole were considered to have study drug-relatedadverse events. Therapy was withdrawn from five (7.7%)subjects in the lomefloxacin group because of adverse events ata mean of 6.2 days of therapy (range, 3 to 12 days); the adverseevents in only 3 (4.4%) subjects were felt to be drug related.Therapy was withdrawn from 10 (15%) subjects who receivedtrimethoprim-sulfamethoxazole because of drug-related ad-verse events at a mean of 5 days (range, 2 to 8 days) (byFisher's exact test, P = 0.04 for medication withdrawal fordrug-related adverse events). The primary adverse eventsleading to drug withdrawal in subjects who received lomefloxa-cin were gastrointestinal. Drug therapy was discontinued forfive subjects in the trimethoprim-sulfamethoxazole group be-cause of a rash and for 5 subjects because of gastrointestinalcomplaints (the latter group included one subject with hepati-tis).When the bacteriological outcome analysis was repeated by
excluding subjects whose therapy was discontinued because ofadverse events or infection with resistant organisms, the bac-teriological cure rates were 91% (CI, 84 and 98%) for thelomefloxacin group and 60% (CI, 46 and 74%) for the tri-methoprim-sulfamethoxazole group at the short-term fol-low-up and 69% (CI, 57 and 81%) for the lomefloxacin groupand 55% (CI, 41 and 69%) for the trimethoprim-sulfamethox-azole group at the long-term follow-up. Thus, the superiority oflomefloxacin for bacteriological eradication at the short-termfollow-up was not explained solely by differences in adverseevents between the two regimens or greater initial bacterialresistance to trimethoprim-sulfamethoxazole.
Additional analyses were performed with subjects stratifiedby age, gender, and underlying abnormality (Table 3). Therewere no apparent age-associated differences in efficacy foreither antimicrobial regimen, and the observation of the
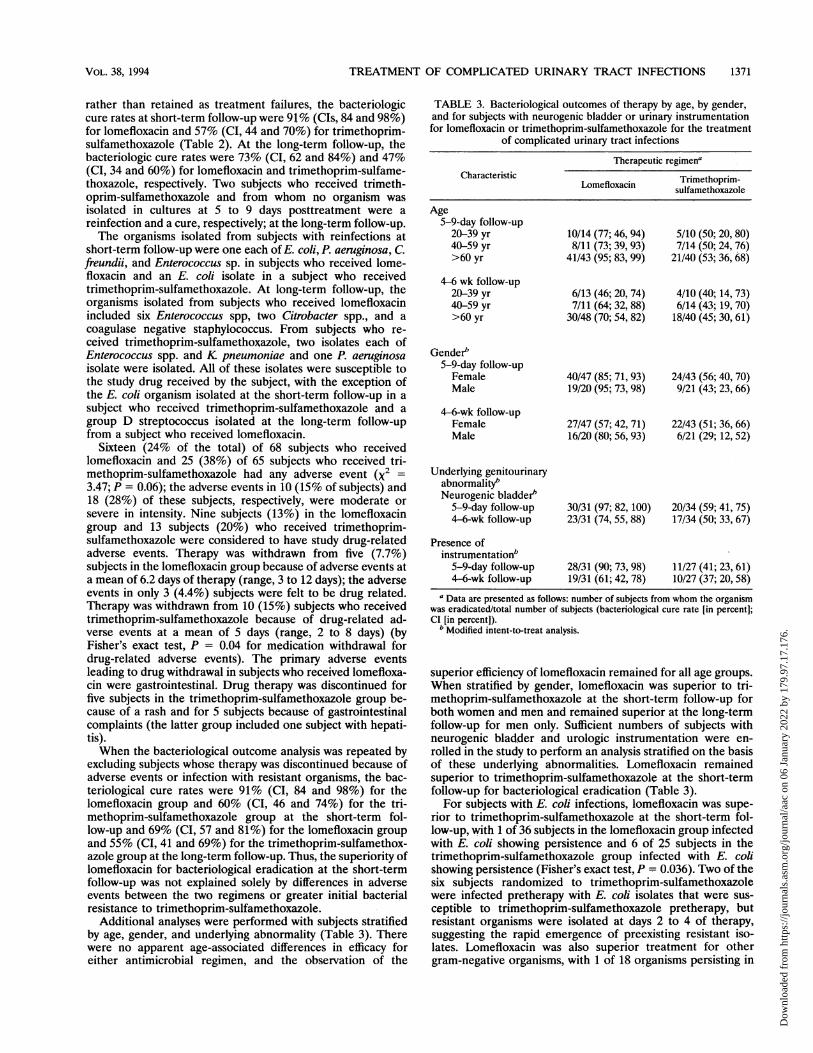
TABLE 3. Bacteriological outcomes of therapy by age, by gender,and for subjects with neurogenic bladder or urinary instrumentationfor lomefloxacin or trimethoprim-sulfamethoxazole for the treatment
of complicated urinary tract infections
Therapeutic regimenaCharacteristic Trimethoprim-
Lomefloxacin sulfamethoxazole
Age5-9-day follow-up
20-39 yr 10/14 (77; 46, 94) 5/10 (50; 20, 80)40-59 yr 8/11 (73; 39, 93) 7/14 (50; 24, 76)>60 yr 41/43 (95; 83, 99) 21/40 (53; 36, 68)
4-6 wk follow-up20-39 yr 6/13 (46; 20, 74) 4/10 (40; 14, 73)40-59 yr 7/11 (64; 32, 88) 6/14 (43; 19, 70)>60 yr 30/48 (70; 54, 82) 18/40 (45; 30, 61)
Gender"5-9-day follow-upFemale 40/47 (85; 71, 93) 24/43 (56; 40, 70)Male 19/20 (95; 73, 98) 9/21 (43; 23, 66)
4-6-wk follow-upFemale 27/47 (57; 42, 71) 22/43 (51; 36, 66)Male 16/20 (80; 56, 93) 6/21 (29; 12, 52)
Underlying genitourinaryabnormality'Neurogenic bladder"
5-9-day follow-up 30/31 (97; 82, 100) 20/34 (59; 41, 75)4-6-wk follow-up 23/31 (74, 55, 88) 17/34 (50; 33, 67)
Presence ofinstrumentation"
5-9-day follow-up 28/31 (90; 73, 98) 11/27 (41; 23, 61)4-6-wk follow-up 19/31 (61; 42, 78) 10/27 (37; 20, 58)
a Data are presented as follows: number of subjects from whom the organismwas eradicated/total number of subjects (bacteriological cure rate [in percent];CI [in percent]).bModified intent-to-treat analysis.
superior efficiency of lomefloxacin remained for all age groups.When stratified by gender, lomefloxacin was superior to tri-methoprim-sulfamethoxazole at the short-term follow-up forboth women and men and remained superior at the long-termfollow-up for men only. Sufficient numbers of subjects withneurogenic bladder and urologic instrumentation were en-rolled in the study to perform an analysis stratified on the basisof these underlying abnormalities. Lomefloxacin remainedsuperior to trimethoprim-sulfamethoxazole at the short-termfollow-up for bacteriological eradication (Table 3).
For subjects with E. coli infections, lomefloxacin was supe-rior to trimethoprim-sulfamethoxazole at the short-term fol-low-up, with 1 of 36 subjects in the lomefloxacin group infectedwith E. coli showing persistence and 6 of 25 subjects in thetrimethoprim-sulfamethoxazole group infected with E. colishowing persistence (Fisher's exact test, P = 0.036). Two of thesix subjects randomized to trimethoprim-sulfamethoxazolewere infected pretherapy with E. coli isolates that were sus-ceptible to trimethoprim-sulfamethoxazole pretherapy, butresistant organisms were isolated at days 2 to 4 of therapy,suggesting the rapid emergence of preexisting resistant iso-lates. Lomefloxacin was also superior treatment for othergram-negative organisms, with 1 of 18 organisms persisting in
VOL. 38, 1994
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/a
ac o
n 06
Jan
uary
202
2 by
179
.97.
17.1
76.
ANTIMICROB. AGENTS CHEMOTHER.
comparison with 7 of 18 organisms persisting in subjects (P =0.022) who received trimethoprim-sulfamethoxazole. Bothagents were uniformly successful in treating gram-positiveinfections, with organisms from all six subjects treated withlomefloxacin and five subjects treated with trimethoprim-sulfamethoxazole being eradicated. At the long-term follow-up, the outcome with lomefloxacin remained superior to thatwith trimethoprim-sulfamethoxazole for treating E. coli, withorganisms from only 5 of 33 subjects treated with lomefloxacinpersisting and organisms from 11 of 29 subjects treated withtrimethoprim-sulfamethoxazole persisting (P = 0.041). Thiswas also the case for other gram-negative bacilli, with organ-isms from 2 of 16 subjects treated with lomefloxacin persistingor relapsing and organisms from 8 of 17 subjects treated withtrimethoprim-sulfamethoxazole persisting or relapsing (P =0.039). Again, gram-positive organisms were uniformly eradi-cated.
DISCUSSION
In the multicenter Canadian study described here, a fluoro-quinolone antimicrobial agent, lomefloxacin, was comparedwith trimethoprim-sulfamethoxazole for the treatment of com-plicated urinary tract infections. Trimethoprim-sulfamethox-azole has been a standard of antimicrobial therapy for com-plicated urinary tract infections for more than 10 years. Thequinolone antimicrobial agents have been introduced morerecently and have been used extensively for the treatment ofurinary tract infections. In the present study, lomefloxacin wassuperior to trimethoprim-sulfamethoxazole with regard tobacteriological outcome, with there being an approximately30% difference in the efficiency of the two regimens at theshort-term follow-up. The difference was no longer significantfor the bacteriological outcomes at the long-term follow-up,however, and there were no differences in clinical outcomes.While the bacteriological differences at long-term follow-up
were no longer significant in the primary analysis, somesecondary analyses suggested a continued benefit with lome-floxacin at the long-term follow-up. When data for subjectswho were lost to follow-up were excluded from the analysis,lomefloxacin remained superior to trimethoprim-sulfamethox-azole at the long-term follow-up. In addition, when eradicationof individual organisms was analyzed, lomefloxacin was supe-rior to trimethoprim-sulfamethoxazole for eradicating allgram-negative organisms at both the short- and the long-termfollow-ups. Finally, when outcome was stratified by gender,lomefloxacin remained superior to trimethoprim-sulfamethox-azole for men at the long-term follow-up. Current guidelinessuggest that at 4 to 6 weeks after therapy, follow-up informa-tion should be available for more than 50% of subjectsevaluated 5 to 9 days after the completion of therapy, andmicrobiological eradication should be documented in morethan 40% of patients (8). Both antimicrobial agents met thesecriteria in the present study, but lomefloxacin was significantlybetter than trimethoprim-sulfamethoxazole for bacteriologicaleradication at the long-term follow-up in the present analyses.There may be several possible reasons for the dichotomy in
the responses between the objective standard of bacteriuriaand the subjective standard of clinical signs and symptoms.First, symptoms in subjects with underlying urinary tractpathologies may be due not to bacteriuria but to othercomplicating factors. Thus, antimicrobial therapy may eradi-cate bacteriuria but not symptoms. Second, even if antimicro-bial therapy is not effective in eradicating bacteriuria, subin-hibitory levels of the antimicrobial agent in the urine mayinhibit multiplication of the organism or suppress the expres-
sion of organism virulence characteristics, ameliorating theinflammatory response (3). This could modify clinical manifes-tations without eradicating bacteriuria.The present study was a single-blind one. One concern with
the observation of the superior efficacy of one of the therapeu-tic regimens is bias favoring lomefloxacin because of inade-quate blinding. The differences observed between the twotherapeutic regimens, however, were in the objective outcomesof bacteriological results and, with adverse events, the devel-opment of a rash. Outcomes whose assessments would be moresubjective and that would more likely be subject to bias,including urinary tract symptoms and adverse events such asgastrointestinal intolerance, did not differ between the tworegimens. Thus, these observations do not suggest that thestudy results were compromised by the lack of a double-blinddesign.Both lomefloxacin and trimethoprim-sulfamethoxazole are
excreted in high concentrations in the urine (1, 11). In addi-tion, the spectra of activity of both antimicrobial agents includegram-negative organisms frequently isolated from patientswith complicated urinary tract infections. The most importantexception would be P. aeruginosa, which is generally suscepti-ble to lomefloxacin and other newer quinolones but which isresistant to trimethoprim-sulfamethoxazole. Why, then, waslomefloxacin superior for bacterial eradication? The higherproportion of initial infecting organisms resistant to tri-methoprim-sulfamethoxazole than to lomefloxacin explainssome of the difference. In addition, increased numbers ofadverse events requiring the termination of therapy wereobserved in subjects who received trimethoprim-sulfamethox-azole. Both of these outcomes were considered therapeuticfailures in the principal analysis. When the subjects with theseoutcomes were removed from the analysis, however, a benefitof lomefloxacin in bacteriological cure at the short-term fol-low-up remained. Thus, the characteristics of the antimicrobialagents must explain some of the observed difference. At theshort-term follow-up, this could be the persistence of low levelsof lomefloxacin in the urine because of the prolonged excretionof this antibiotic. This should not, however, be the case for thelong-term follow-up. For the male subset of study subjects,superior bacteriological efficacy was documented for bothshort- and long-term outcomes. The prostate is an importantsource of relapsing urinary tract infections in men, and iflomefloxacin were superior in eradicating infection or prolong-ing the time to relapse at this site, it could explain some of theobserved superior efficacy. The quinolones are effective for thetreatment of bacterial prostatitis (5), but limited comparativestudies are available. It would seem, however, that moreeffective antimicrobial killing of the organism or more effectivepenetration to the site of infection must explain some of theobserved differences in outcomes between the groups treatedwith the different antimicrobial agents.
Several studies have reported the relative efficacies of quin-olone antimicrobial agents in comparison with that of tri-methoprim-sulfamethoxazole for the treatment of complicatedurinary tract infections (5). Interpretation of the results ofmany of those studies is compromised by the inclusion ofsubjects with both uncomplicated as well as complicatedurinary tract infections or by small numbers of study subjects.Most studies also excluded patients infected with resistantorganisms from initially being enrolled in the study or fromanalysis of the outcome. Thus, it is difficult to make directcomparisons between the outcomes reported by other studiesand those reported here. As a general rule, however, previousstudies did not report differences in outcomes between subjectswho received a quinolone or trimethoprim-sulfamethoxazole.
1372 NICOLLE ET AL.
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/a
ac o
n 06
Jan
uary
202
2 by
179
.97.
17.1
76.

TREATMENT OF COMPLICATED URINARY TRACI INFECTIONS 1373
Several studies have compared two different quinoloneantimicrobial agents for the treatment of complicated urinarytract infections (2, 5, 9). In two recent studies with relativelylarge sample sizes, treatment with lomefloxacin and ciprofloxa-cin resulted in reported cure rates of 97 and 96%, respectively,at short-term follow-up (2), whereas the cure rate was 88% forlomefloxacin in the present study, and treatment with norfloxa-cin and ciprofloxacin resulted in cure rates of 72 and 79%,respectively, at long-term follow-up (9), whereas the cure ratewas 64% for lomefloxacin in the present study. Thus, ourobserved outcome for the quinolone therapeutic arm of thestudy appears to be consistent with those presented in otherreports.
Complicated urinary tract infection is an umbrella designa-tion used to describe infections in a heterogeneous group ofsubjects with multiple distinct underlying abnormalities whichcould have different impacts on outcome following treatmentfor urinary tract infections. For instance, for patients withstruvite urolithiasis, no amount of antimicrobial therapy wouldbe expected to cure the infection. On the other hand, somepatients with neurogenic bladder, such as those with spinalcord injuries, may be cured with courses of therapy of as shortas 3 days (4). Thus, it may be important to stratify patients withcomplicated urinary tract infections into subgroups on thebasis of their underlying abnormalities to determine the opti-mal approach to therapy. When such stratification was per-formed for the present study, with sufficient numbers of studysubjects enrolled to perform an analysis by gender, age, andthe limited number of genitourinary complicating factors,outcomes were consistent with those obtained in the primaryanalysis.The fluoroquinolone antimicrobial agents have been widely
used following their introduction. Associated with this wide-spread use has been a fairly rapid emergence of resistanceamong gram-negative organisms classically considered to bedifficult to treat (13). These include P. aenrginosa, Serratiamarcescens, and some strains ofK pneumoniae and Citrobacterspp. All of these are important infecting organisms in patientswith complicated urinary tract infections. Subjects with com-plicated urinary tract infections, particularly those with under-lying abnormalities which cannot be corrected, are likely tobecome reinfected with resistant organisms following repeatedcourses of treatment with antimicrobial agents. Thus, whilelomefloxacin was about 30% superior to trimethoprim-sulfa-methoxazole for the treatment of complicated urinary infec-tions at the short-term follow-up in the present study, wide-spread empiric use of quinolones in such patients with anexpected high recurrence rate will ultimately impair the effec-tiveness of these antimicrobial agents because of the emer-gence of antimicrobial resistance. Characterization of theoptimal use of quinolones in these patients to balance thera-
peutic efficacy with potential problems of the emergence ofresistance requires further long-term assessment.
ACKNOWLEDGMENT
This study was supported by a grant from Searle Canada Inc.
REFERENCES1. Bach, M. D., 0. Gold, and M. Finland. 1973. Absorption and
urinary excretion of trimethoprim, sulfamethoxazole, and tri-methoprim-sulfamethoxazole: results with single doses in normalyoung adults and preliminary observations during therapy withtrimethoprim-sulfamethoxazole. J. Infect. Dis. 128(Suppl.):S584-S598.
2. Cox, C. E. 1992. A comparison of the safety and efficacy oflomefloxacin and ciprofloxacin in the treatment of complicated orrecurrent urinary tract infections. Am. J. Med. 92(Suppl. 4A):82S-86S.
3. Lorian, V., and C. G. Gemmell. 1991. Effect of low antibioticconcentrations on bacteria: effects on ultrastructure, virulence,and susceptibility to immunodefenses, p. 493-555. In V. Lorian(ed.), Antibiotics in laboratory medicine, 3rd ed. The Williams &Wilkins Co., Baltimore.
4. Mohler, J. L., D. L. Cowen, and R. C. Flanigan. 1987. Suppressionand treatment of urinary tract infection in patients with intermit-tently catheterized neurogenic bladder. J. Urol. 138:336-340.
5. Naber, K. G. 1989. Use of quinolones in urinary tract infectionsand prostatitis. Rev. Infect. Dis. 11(Suppl. 5):S1321-S1337.
6. National Committee for Clinical Laboratory Standards. 1990.Methods for dilution antimicrobial susceptibility tests for bacteriathat grow aerobically. Approved standard M7-A2. National Com-mittee for Clinical Laboratory Standards, Villanova, Pa.
7. National Committee for Clinical Laboratory Standards. 1990.Performance standards for antimicrobial disk susceptibility tests.Approved standard M2-A4. National Committee for ClinicalLaboratory Standards, Villanova, Pa.
8. Rubin, R. H., E. D. Shapiro, V. T. Andriole, R. J. Davis, and W. E.Stamm. 1992. Evaluation of new anti-infective drugs for thetreatment of urinary tract infection. Clin. Infect. Dis. 15:S216-S227.
9. Schaeffer, A. J., and R. U. Anderson. 1992. Efficacy and tolerabilityof norfloxacin vs ciprofloxacin in complicated urinary tract infec-tion. Urology 40:446-449.
10. Schentag, J. J., and T. F. Goss. 1992. Quinolone pharmacokineticsin the elderly. Am. J. Med. 92(Suppl. 4A):33S-37S.
11. Stone, J. W., J. M. Andrews, J. P. Ashby, D. Griggs, and R. Wise.1988. Pharmacokinetics and tissue penetration of orally adminis-tered lomefloxacin. Antimicrob. Agents Chemother. 32:1508-1510.
12. Wise, R., J. M. Andrews, J. P. Ashby, and R. S. Matthews. 1988. Invitro activity of lomefloxacin, a new quinolone antimicrobial agent,in comparison with those of other agents. Antimicrob. AgentsChemother. 32:617-622.
13. Wolfson, J. S., and D. C. Hooper. 1989. Bacterial resistance toquinolones: mechanisms and clinical importance. Rev. Infect. Dis.11(Suppl. 5):S960-S968.
VOL. 38, 1994
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/a
ac o
n 06
Jan
uary
202
2 by
179
.97.
17.1
76.