treatment of advanced colorectal cancer · •review future directions in the treatment of advanced...
TRANSCRIPT

Treatment of Advanced Colorectal Cancer
Alexis D. Leal, M.D.Assistant Professor, GI Medical Oncology
University of Colorado Cancer Center
Disclosures
• None
Objectives
• Review the basics of advanced colorectal cancer
• Review treatment and management of resectable and unresectablecolorectal cancer
• Review future directions in the treatment of advanced colorectal cancer

Colorectal Cancer 101:
*Source: American Cancer Society
History and Physical Examination
• Hematochezia – 58%
• Abdominal Pain – 52%
• Unexplained Iron Deficiency Anemia – 57%
• Weight Loss – 39%
• Altered Stools – 25%
• Obstruction – 4%

Diagnosis/Staging
• Labs– CBC, CMP, CEA
• Procedures– Colonoscopy with biopsy– Flexible sigmoidoscopy with biopsy
• Radiology– CT scan– Chest/Abdomen/Pelvis (Chest is controversial)– PET/CT (?)– Liver MRI (?)
http://www.uptodate.com/contents/image?imageKey=GAST%2F83618&topicKey=ONC%2F2496&rank=1~150&source=see_link&search=colorectal+cancer&utdPopup=true
Prevalence & Survival by Stage
Tumor• Resectability• Biology• Symptoms
Treatment• Efficacy• Toxicity• Availability
Patient• Age• General Health• Other Diseases• Preference
Factors Influencing Treatment Selection

Colorectal Cancer:Management of early-stage disease
Limited Stage Colon Cancer
• Stage I through III Colon Cancer (no distant metastases)– Surgical resection first
• Adjuvant Chemotherapy – 3-6 months of chemotherapy– High-Risk stage II
• Poorly differentiated, T4 tumor, Obstruction/Perforation, Vascular invasion, < 12 Lymph Nodes removed
– Stage III (any lymph node involvement)• FOLFOX (5-fluorouracil and oxaliplatin)
Limited Stage Colon Cancer• IDEA Trials Summary
Presented at ASCO 2017 by Qian Shi, PhD on behalf of IDEA collaborators

IDEA Collaboration
Presented at ASCO 2017 by Qian Shi, PhD on behalf of IDEA collaborators
IDEA CollaborationDFS Comparison by Risk Group & Regimen
Presented at ASCO 2017 by Qian Shi, PhD on behalf of IDEA collaborators
IDEA Clinical Consensus: Risk based approach to adjuvant therapy for stage III Colon cancer
Presented at ASCO 2017 by Qian Shi, PhD on behalf of IDEA collaborators

Limited Stage Rectal Cancer
• Stage I – Surgical Resection First
• Stage II or higher– “Neoadjuvant” chemotherapy and radiation (chemoXRT)– 5-FU/leucovorin or capecitabine combined with radiation therapy (5
weeks)
ChemoXRT(5 weeks)
5-FU or CapeSurgery
Chemotherapy(4 months)FOLFOX
Colorectal Cancer:Management of advanced disease
Treatment of Advanced Colon Cancer
Resectable • Oligometastatic disease
– Resectable metastases in liver or lung– Potentially curable with multi-disciplinary
approach • Surgery adjuvant chemotherapy• Neoadjuvant chemotherapy surgery
adjuvant chemotherapy
Unresectable• Multi-agent chemotherapy +/- biologics• Clinical trials • Radiation therapy• Interventional radiology
– Radiofrequency ablation (RFA)– Embolization
• Chemoembolization • Y-90

Surgical Resection of Liver Tumors
Radiation Therapy
Used prior to surgery or
sometimes to treat metastases
High frequencyalternating current
Ionic vibration &heat generation
45°C: Proteindenaturation
70°C: Thermalcoagulation
100°C: Tissuedesiccation
Radiofrequency Ablation (RFA)
Adapted from Minami Y, Kudo M. Int J Hepatol. 2011;doi:10.4061/2011/104685
The radiofrequency probe is inserted into the liver tumor
The interventional radiologist deploys electrodes from the probe, which deliver radiofrequency energy. This high heat causes death of tumor cells
Following the procedure, the tumor cells are destroyed and will eventually be replaced by scar tissue.
Used either in conjunction with surgery or alone to
treat metastases

mCRC Outcomes Have Improved With the Evolution of Treatment Options
1. Cunningham D, et al. Lancet. 1998;352(9138):1413-1418. 2. Van Cutsem E, et al. Br J Cancer. 2004;90(6):1190-1197. 3. Rothenberg M, et al. J Clin Oncol. 2003;21(11):2059-2069. 4. Hurwitz H, et al. N Engl J Med. 2004;350(23):2335-2342. 5. Cunningham D, et al. N Engl J Med. 2004;351(4):337-345. 6. Van Cutsem E, et al. N Engl J Med. 2009;360(14):1408-1417. 7. Van Cutsem E, et al. J Clin Oncol. 2007;25(13):1658-6164. 8. Van Cutsem E et al. J Clin Oncol. 2012;30(28):3499-3506. 9. Grothey A, et al. Lancet. 2013;381(9863):303-312. 10. MayerRJ et al. N Engl J Med. 2015 May 14;372(20):1909-19.
Median OSMonths
1980s 1990s 2000s
Cetuximab5,6
BSC
Irinotecan1
Capecitabine2
Oxaliplatin3
Bevacizumab4
5-FU
Panitumumab7
15
10
5
0
20
25
30
Aflibercept8
Regorafenib9
TAS-10210
“Cytotoxics” Mechanism1. 5-Fluorouracil (5-FU) pyrimidine analog2. capecitabine oral 5-FU pro-drug3. TAS-102 5-FU drug with metabolism inhibitor4. irinotecan topoisomerase I inhibitor5. oxaliplatin 3rd generation platinum
“Biologics/Targeted” Mechanism1. cetuximab antibody against EGFR2. panitumumab antibody against EGFR 3. bevacizumab antibody against VEGF4. ziv-aflibercept VEGF trap5. ramucirumab antibody against VEGFR26. regorafenib tyrosine kinase inhibitor7. ramucirumab antibody against VEGFR28. pembrolizumab/nivolumab antibody against PD-1 (MSI-high only)
VEGF = Vascular Endothelial Growth FactorEGFR = Epidermal Growth Factor ReceptorPD-1 = Programmed death ligand-1MSI = microsatellite instability
14 FDA Approved Drugs for Colorectal Cancer
Colorectal Cancer is Expensive• 5-FU (500 mg/m2) $6• Leucovorin (500 mg/m2) $85• Capecitabine (2000 mg/m2/day) $3,250• Irinotecan (180 mg/m2) / generic $2,300 / $480• Oxaliplatin (85 mg/m2) / generic $4,190 / $590• Bevacizumab (5 mg/kg) $2,560• Cetuximab (250 mg/m2) $5,120• Panitumumab (6 mg/kg) $4,360• Aflibercept (4 mg/kg) $5,380• Regorafenib (160 mg, 3/1) $5,952• TAS-102 (15-6.14mg) $7,139
1997: 6 months of 5-FU/LV costs ~$5002017: 30 months of therapy with combinations costs >$400,000

Overview of EGFR and VEGFR Growth Signaling Pathways
TumorCell EndothelialCell
RAS
RAF BRAF
MEK
ERK
Pl3K
AKT
mTOR
ONCOGENESISANGIOGENESIS
TUMORMICROENVIRONMENT
VEGFREGFR PDGFR-βKIT
Targetedbycetuximabandpanitumumab
Targetedbybevacizumab
andaflibercept*
VEGF
Targetedbyramucirumab
Krasinskas et al, 2011; Sitohy et al, 2012; Bendardaf et al, 2008; Kitadai et al, 2006; Jayson et al, 2005; FDA News Release.
*aflibercept also targets PIGF
EGFR = epidermal growth factor receptorPDGFR = platelet-derived growth factor receptorVEGFR = vascular endothelial growth factor receptor
KRAS Mutations Predict (Lack of) Benefit to EGFR Therapy
Refractory CRC RCetuximab alone
Best supportive care
Karapetis et al. NEJM 2008, 359 (17): 1757
RAS wt~50%
KRAS mt~40%
New RAS mt~10%
Rare KRAS Mutations
NRAS Mutations
Distribution of Mutations in mCRC

“PRIME” Trial Schema
Douillard et al. J Clin Oncol 2010.
KRAS MT group
Douillard et al., NEJM 2013:369(11)
“PRIME” Trial: KRAS, Atypical KRAS, NRAS
BRAF• BRAFV600E present in ~ 7% of metastatic CRC
– Results in constitutive activation of MAPK signaling – Associated with aggressive biology, shorter OS, limited response
to chemotherapy
• Associated with:– Right-sided tumors– High grade– Older age– Female– MSI-high– Serrated (as opposed to tubular adenoma pathway)
• BRAF and KRAS mutations appear to be mutually exclusive

Van Cutsem et al, J Clin Oncol 2011
BRAF mutation is a negative prognostic factor
“CRYSTAL” Trial: 1st Line FOLFIRI/Cetuximab
Right vs. Left Colon Cancer (Sidedness)
LEFTN = 732
(68%)
RIGHTN = 293(27%)
Analysis of CALGB/SWOG 80405
• Patients with right-sided colon cancer did not benefit from treatment with EGFR inhibitor – even if RAS wild-
type
Presented at ASCO 2016 by Alan P. Venook, MD

Current Cancer Treatment Strategy: One-size-fits-all
Future Directions in Treatment of Colorectal Cancer
BRAF inhibition in Melanoma

BRAF Inhibition in Melanoma
Wagle et al. J Clin Oncol. 2011.
BRAF Inhibition in Melanoma
Wagle et al. J Clin Oncol. 2011.
Minimal Efficacy with BRAF or Dual BRAF + MEK Inhibition
Corcoran et al ASCO ‘12, Kopetz et al ASCO ‘10
-100
-75
-50
-25
0
25
50
75
100
%C
hang
e Fr
om B
asel
ine
(Sum
of L
esio
n Si
ze)
5% Response Rate
BRAF inhibition
Vemurafenib
12% Response Rate
BRAF + MEK inhibition
GSK212 + GSK436

A key finding: Feedback EGFR signaling after BRAF inhibition
BRAFmut
PI3K
AKT
RAS
ERK
EGFRand others
pERK1/2
Vinculin
HT29 Colo205
EGFR
Mao et al CCR ‘12, Prahallad et al Nature ‘12
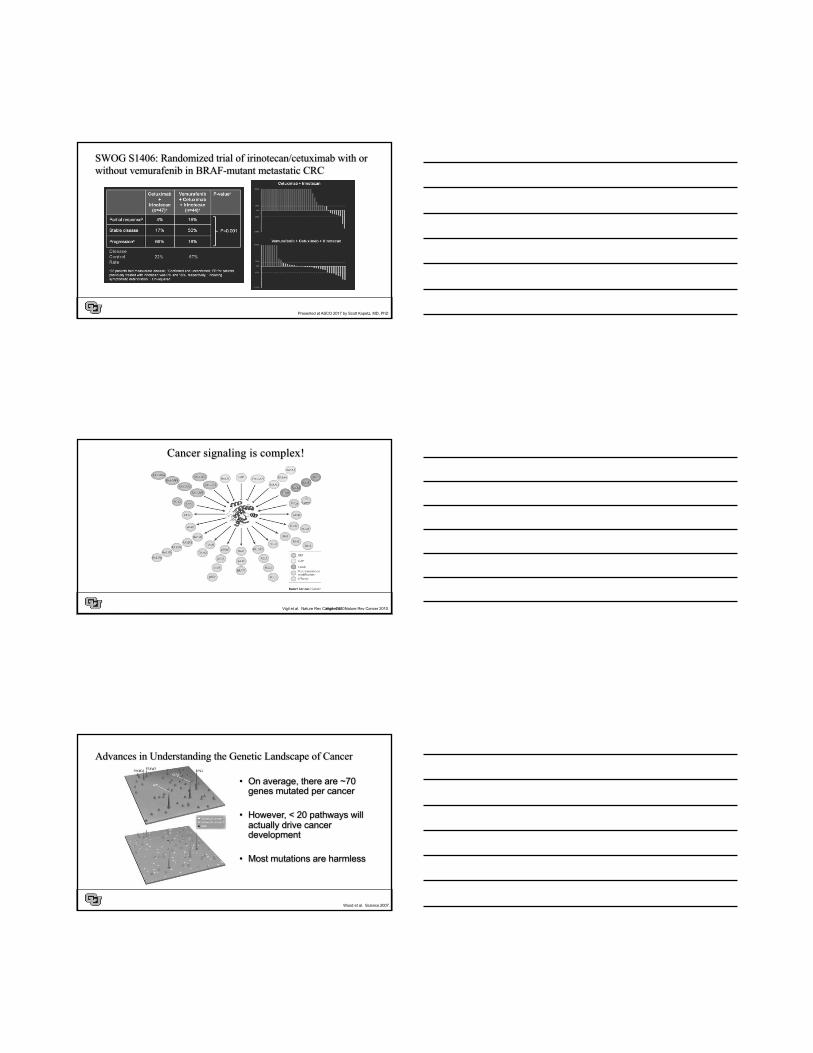
SWOG S1406: Randomized trial of irinotecan/cetuximab with or without vemurafenib in BRAF-mutant metastatic CRC
Presented at ASCO 2017 by Scott Kopetz, MD, PhD
SWOG S1406: Randomized trial of irinotecan/cetuximab with or without vemurafenib in BRAF-mutant metastatic CRC
Presented at ASCO 2017 by Scott Kopetz, MD, PhD
SWOG S1406: Randomized trial of irinotecan/cetuximab with or without vemurafenib in BRAF-mutant metastatic CRC
Presented at ASCO 2017 by Scott Kopetz, MD, PhD
Cancer signaling is complex!
Vigil et al. Nature Rev Cancer 2010.Vigil et al. Nature Rev Cancer 2010.
Advances in Understanding the Genetic Landscape of Cancer
• On average, there are ~70 genes mutated per cancer
• However, < 20 pathways will actually drive cancer development
• Most mutations are harmless
Wood et al. Science 2007.
Roadmap of Precision Oncology
Microsatellite Unstable CRCMSI-high
Hallmarks of Cancer
http://www.researchcancerimmunotherapy.com/images/overview/evading-immune-destruction/hallmark-cancer.png

The Importance of Mismatch Repair
Wakamatsu et al. J Bio Chem 2010;285: 9762-9769
Microsatellite High Colorectal Cancer
• Germline (Hereditary): “HNPCC” or Lynch Syndrome– Due to mutations in one of the mismatch repair (MMR) genes
• MLH1, MSH2, MSH6, PMS2, and/or EPCAM– Increased lifetime risk of colorectal, endometrial, stomach, ovarian, urothelial, and other cancers
• Acquired MSI– Most due to hypermethylation of the MLH1 promoter and epigenetic silencing of MLH1– Can also have “double somatic” MSI caused by mutations in MMR genes
• Two methods for testing– PCR – identify variation in genomic repeats– IHC – loss of expression of one or more MMR proteins
MSI-high tumors have more mutations

MSI-high Cancers Have Tumor Infiltrating T-cells (which can help kill cancer)
Redston M. Mod Pathol 2001;14(3).
MSI-H in Colon Cancer:Prevalence and Prognosis
Stage Prevalence Prognosis Compared to MSS
II 15%-20% excellentIII 8%-10% sameIV 4%-5% same or worse
• Hypermutated cancers too “deranged” to metastasize• Immune system can prevent spread• But once a metastatic clone has been selected, same or worse
prognosis than microsatellite stable CRC
MSI-H, high levels of microsatellite instability; MSS, microsatellite stability.
The Cancer Genome Atlas, 2012.
Presented By Dung Le at 2015 ASCO Annual Meeting

PD-1 and PD-L1 Function as Immune Checkpoints: Prevents Activation
http://directorsblog.nih.gov/2015/06/09/a-surprising-match-cancer-immunotherapy-and-mismatch-repair/
Slide 8
Presented By Dung Le at 2015 ASCO Annual Meeting
Slide 11
Le et al. NEJM 2015; 372:2509-20.

Le, NEJM 2015
Responses in MSI-high CRC
Le et al. NEJM 2015; 372:2509-20.
Responses in MSI-high CRC
Le et al. NEJM 2015; 372:2509-20.

Treatment of Colorectal Cancer • The revolution of genetic information on tumors over the last 5 years has greatly increased
understanding of tumor biology
• But… this has not yet translated into the clinic, since surgery is still the mainstay of curing solid tumors like colorectal cancer
• Ignorance (lack of research) is costly and deadly; without knowledge of KRAS/NRAS, for instance, we would be spending >$800,000,000 per year harming patients
• Knowledge of relevant biomarkers is critical in caring for colorectal cancer patients; however, important to use markers that have been validated/qualified across multiple studies
Take Home Points
• Some patients with metastatic CRC can be cured with multidisciplinary approach
• RAS mutations predict lack of benefit to EGFR inhibitors
• BRAF
• Metastatic/unresectable MSI-H CRC may benefit from immunotherapy– Clinical trial open at UCD – 1st line chemo vs. pembrolizumab
• Consider clinical trial options for patients with metastatic disease and good PS
Thank you!!