treating sinusitis? - mccombs school of business | the .../media/files/msb/centers/health... ·...
TRANSCRIPT

Treating sinusitis? Managing obesity? Preventing heart disease? Preventing lung cancer? Managing individuals with multiple chronic diseases?
Providing care for long-term cancer survivors?
Managing depression? Treating substance abuse?
A. The US doesn’t spend enough on health care.
B. Doctors don’t know these are problems that should be addressed.
C. Competing demands make it impossible to do everything.
D. Practices are designed for care of acute problems and single chronic diseases.
E. The United States doesn’t address the underlying determinants of health.

In late January 2015, Tom’s father was diagnosed with Acute Myelogenous Leukemia.
This was quite a shock as his father had been walking nearly eight miles a day through the end of 2014 and had otherwise been very healthy.
As a result of his diagnosis, Tom’s father was hospitalized for a couple of weeks and is now completing his second round of chemotherapy.

What struck Tom as he sat in his father’s hospital room the first week after he was diagnosed was how little choice his dad was given in his treatment.
He particularly noted the nurses and oncologists being clear that they would be meeting without his dad to determine the best course of treatment and they would let him know how they would proceed.
A couple of years previously, before his role as Executive Director of NAPCRG, it may have been reassuring or comforting that the doctors were “handling” things on behalf of his dad.
But now, he was actually quite shocked by their complete lack of consideration for what his dad might actually want in terms of his treatment.

“After spending the better part of the past two years working alongside Jack Westfall, MD to create and manage the Patient and Clinician Engagement initiative that PCORI has generously funded - it was like a light went off in my brain and now I can’t shut it off.”
“My observations of my dad’s care do not square with the values we are working to achieve in valuing and respecting the patient first and foremost. I suddenly had a very real and deep appreciation for our work and I’m grateful for it.”

Adapted from http://historical.hsl.virginia.edu/kerr/bio.cfm
Adult population at risk
Adults reporting one or more illnesses or injuries per month
Adults consulting a physician one or more times per month
Adult patients admitted per month
Adult patients referred to another physician per monthAdult patients referred to a university medical center per month
1000
750
250
9
5
1

Helen slumps in the corner of the exam room. Dr. Jones, a family doctor, enters for his 10 minute visit.
Dr. Jones looks at Helen and asks, “How many seizures are you having?”
This is the 12th visit in 2 years with multiple providers for this 46 year old woman with chronic problems of abdominal complaints, seizures, hypertension, type 2 diabetes, and depression.
How can Dr. Jones meet the patient-centered needs of Helen?
9

Barbara Starfield’s international comparisons of primary care and the lag by US
IOM Chasm Report of 2001 finds huge quality gaps
Future of Family Medicine Report of 2004 proposes major practice redesign
NCQA, ACA, Meaningful Use and a whole host of disruptions!

12
Informed, Activated
Patient
ProductiveInteractions
Prepared, ProactivePractice Team
DeliverySystemDesign
DecisionSupport
ClinicalInformation
Systems
Self-Management
Support
Health System
Resources and Policies
Community
Health Care Organization
Chronic Care Model
Improved Outcomes
Community and Practice Resources
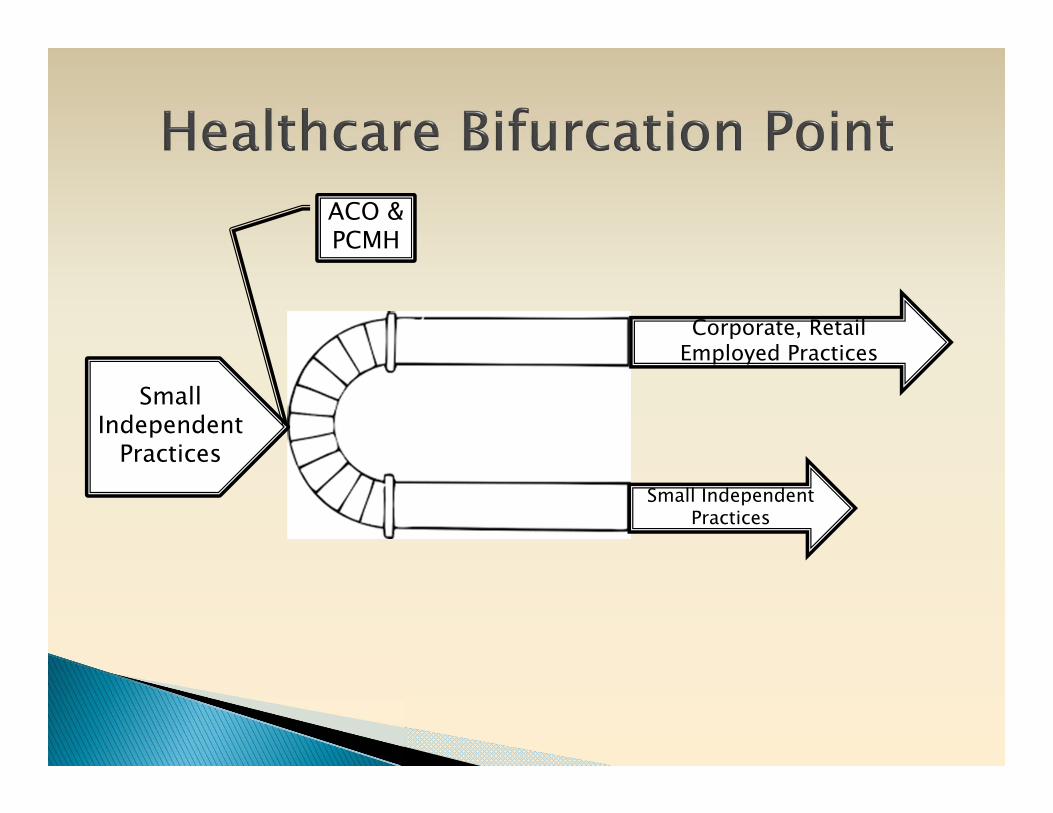
Small Independent Practices
Small Independent
Practices
Corporate, Retail Employed Practices
ACO & PCMH

2000
• Keystone III Conference • Family Medicine recognition that the health care system is
in serious trouble, commissioned study in 2002.
2004
• Future of Family Medicine Report• New Model of practice and recommended “proof of concept”
demonstration project in typical family practices
2006
• AAFP creates TransforMED and begins NDP• 36 family medicine practices randomized to two arms to
implement NDP Model with independent evaluation

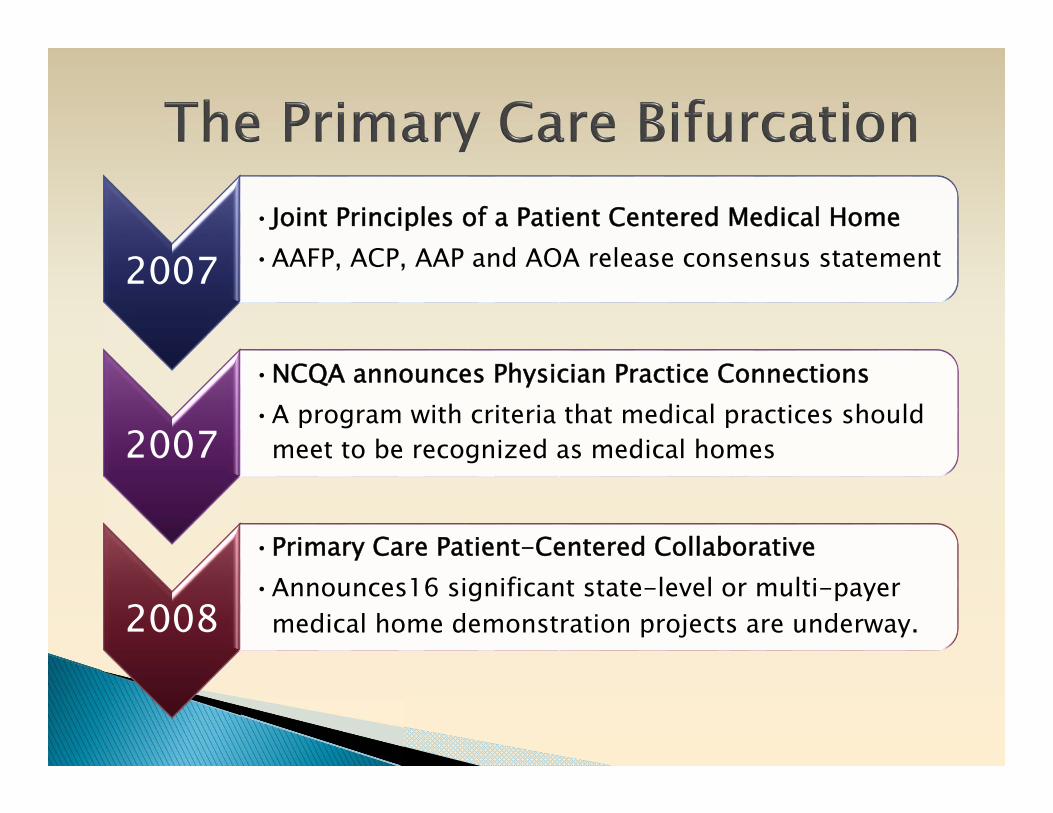
2007•Joint Principles of a Patient Centered Medical Home•AAFP, ACP, AAP and AOA release consensus statement
2007
•NCQA announces Physician Practice Connections•A program with criteria that medical practices should
meet to be recognized as medical homes
2008
•Primary Care Patient-Centered Collaborative•Announces16 significant state-level or multi-payer
medical home demonstration projects are underway.
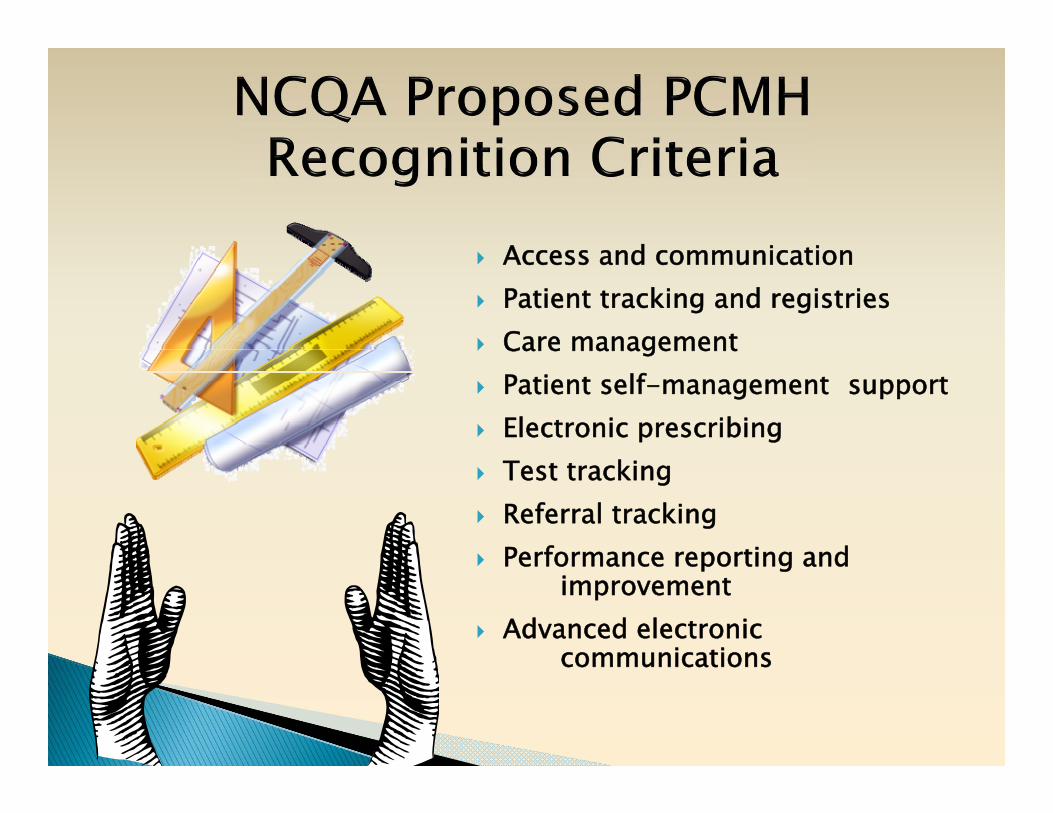
Access and communication Patient tracking and registries Care management Patient self-management support Electronic prescribing Test tracking Referral tracking Performance reporting and
improvement Advanced electronic
communications
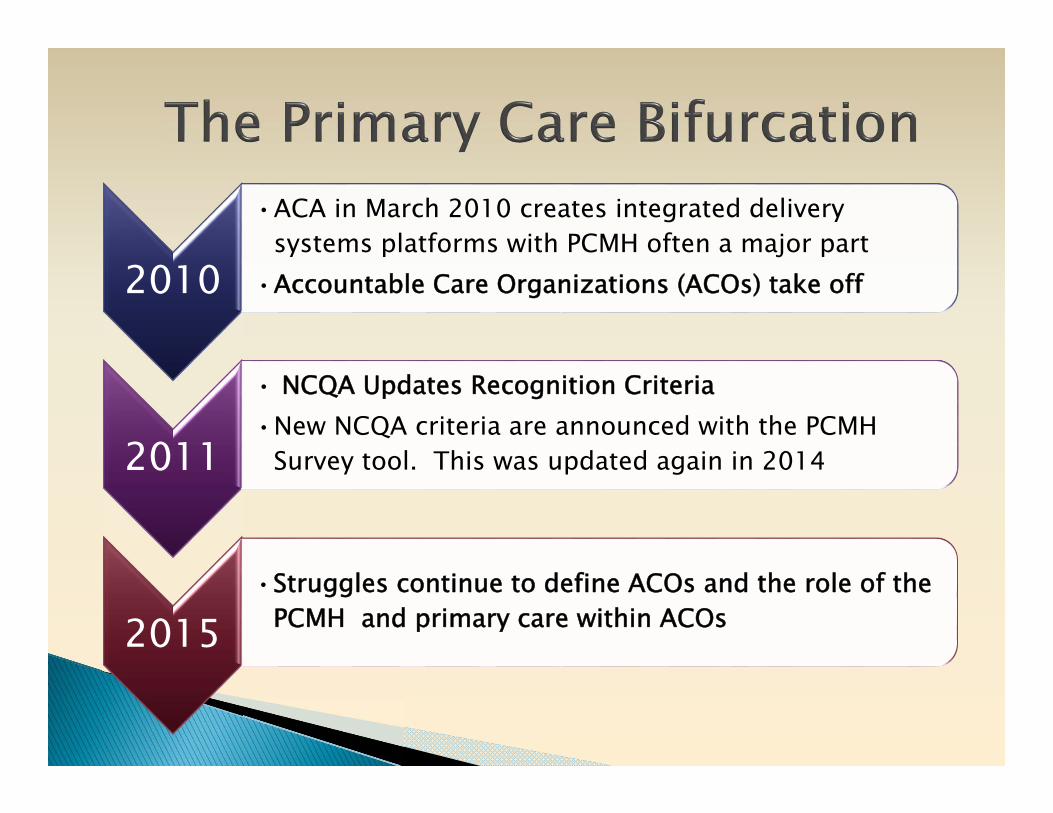
2010
•ACA in March 2010 creates integrated delivery systems platforms with PCMH often a major part
•Accountable Care Organizations (ACOs) take off
2011
• NCQA Updates Recognition Criteria•New NCQA criteria are announced with the PCMH
Survey tool. This was updated again in 2014
2015•Struggles continue to define ACOs and the role of the
PCMH and primary care within ACOs

Patient Centered Medical Home

Team of people embedded in a community seeking to improve health and healing in that community & consisting of:
Fundamental tenets of primary care◦ First contact access◦ Comprehensiveness◦ Integration / coordination◦ Relationships involving sustained partnership
New ways of organizing practice Development of practice internal capabilities Health care delivery system & payment changes



Vermont Blueprint for Health created Community Health Teams to work with primary care providers to assess patients’ needs, coordinate support services, and provide multidisciplinary care.
Web-based central health registry of patient data.
State support for practice facilitators to work with primary care practices to obtain NCQA PCMH Recognition.
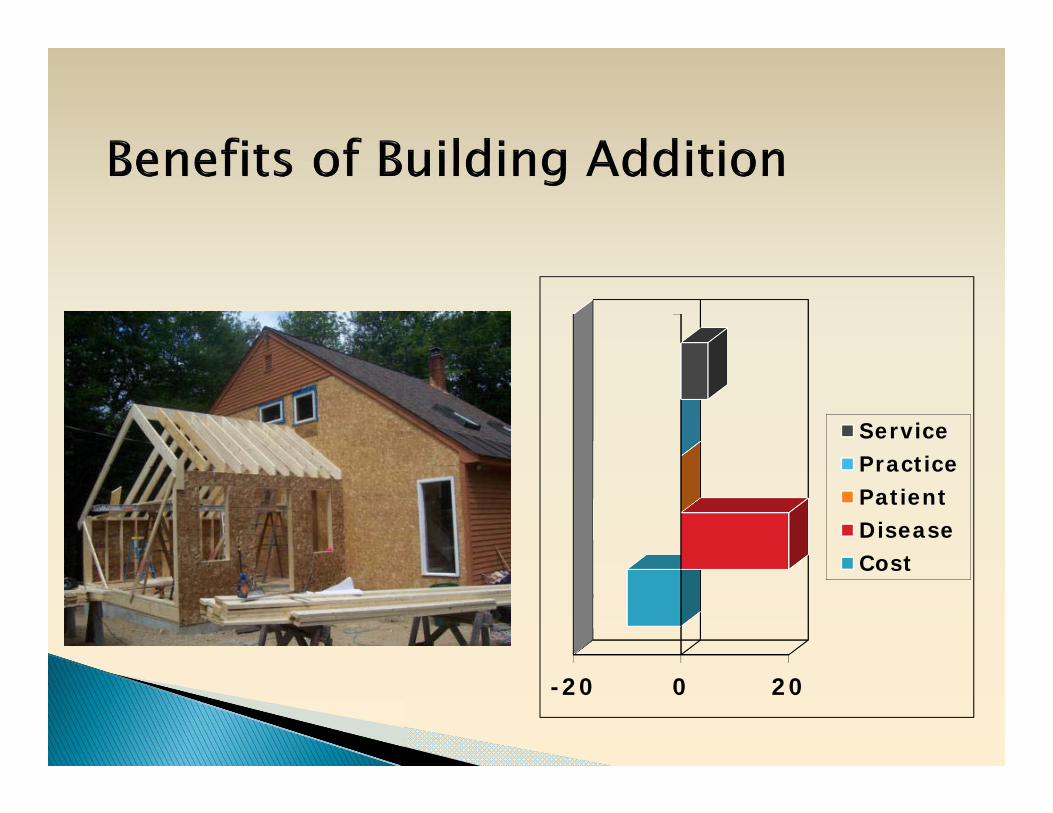
-20 0 20
ServicePracticePatientDiseaseCost


Virginia Mason Bainbridge Island adopted Toyota Lean and taught this to all leaders and many staff.
Using their existing personnel, they created teams of 2 physicians, one mid level, 1 RN, and 2 MA’s, with all teams sharing a clinical pharmacist. Joint workspaces created for MA’s/clinicians, with nurses located.
Created “Flow Stations” by up-skilling traditional MA roles and creating partnerships of a clinicians and MA’s who always worked together.
MA called flow manager and manages the flow of patients and all the paperwork.
Pharmacy and Care manager are available if needed to keep things flowing.
All work is finished by end of the day.

-10 0 10
ServicePracticePatientDiseaseCost

Lehigh Family Medical Associates combined elements of Virginia Mason and the Vermont Blueprint.
Created Community Health Teams to work with primary care providers to assess patients’ needs, coordinate support services, and provide multidisciplinary care.
Using their existing personnel, they created teams of physicians, mid-levels, RN’s, and MA’s who also work together.
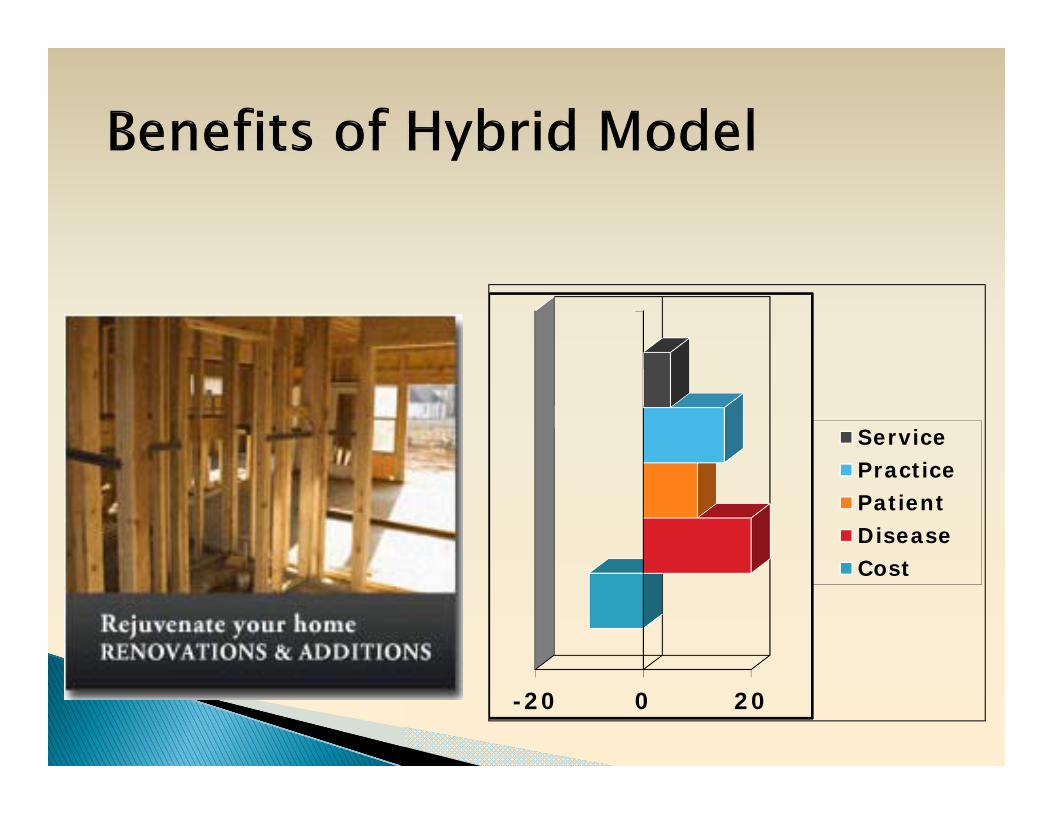
-20 0 20
ServicePracticePatientDiseaseCost


Southcentral Foundation is an Alaska Native-owned, nonprofit health care organization run by a community board
Primary care provider and teams include:◦ One or two medical assistants◦ Full-time nurse care coordinator◦ Administrative assistant for case management support
Members added or subtracted needs change:◦ Pharmacists◦ Nurse midwives◦ Chiropractors◦ Other specialists
Reduced urgent care and ER utilization by 50%, hospital admissions by 53%, and specialist use by 65% while rising to the 75-90th percentile on most HEDIS outcome and quality measures.
-20 0 20
Service
Practice
Patient
Disease
Cost


NCQA Recognition Accountable Care Organizations Meaningful Use Pay for performance on disease outcomes Employer mandates
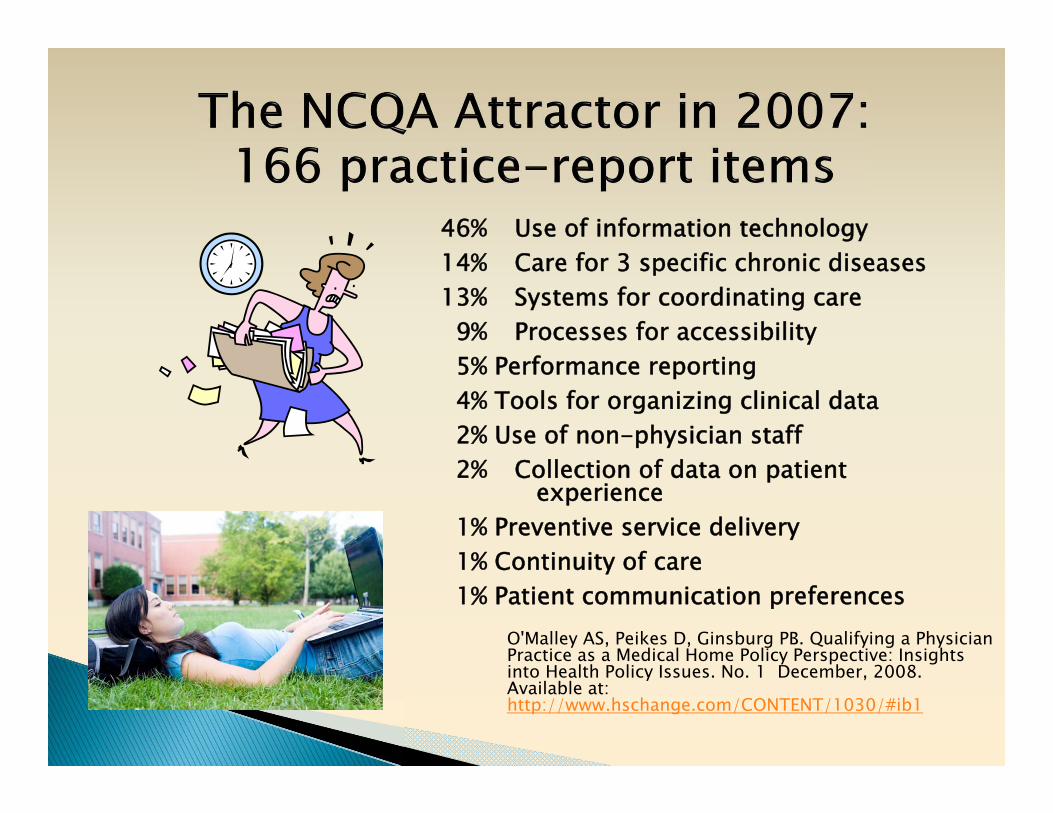
46% Use of information technology14% Care for 3 specific chronic diseases 13% Systems for coordinating care
9% Processes for accessibility5% Performance reporting4% Tools for organizing clinical data2% Use of non-physician staff 2% Collection of data on patient
experience1% Preventive service delivery1% Continuity of care 1% Patient communication preferences
O'Malley AS, Peikes D, Ginsburg PB. Qualifying a Physician Practice as a Medical Home Policy Perspective: Insights into Health Policy Issues. No. 1 December, 2008. Available at: http://www.hschange.com/CONTENT/1030/#ib1

Network of doctors and hospitals that share financial and medical responsibility for providing coordinated care.
Since January 2013, nearly 200 new public and private ACOs have been formed:◦ Medicare Shared Savings Program (MSSP) Accountable
Care Organizations◦ Medicaid Accountable Care Organizations◦ Integrated Delivery Systems◦ Multispecialty Group Practice (usually don’t own the
health plan, but contract with multiple plans)◦ Independent Practice Associations
Drastic shift away from private independent practices to affiliated and owned practices

Implement drug-drug and drug-allergy interaction checks
Maintain up-to-date problem list of current and active diagnoses
Generate and transmit permissible prescriptions electronically
Maintain active medication list Record demographics and vital signs Implement clinical decision support rule for high
clinical priority and track compliance Patients can view online, download, and transmit
information Provide clinical summaries for patients for each
office visit

Focus on technology for information management and control
Diseases controlled care and not necessarily patient-centered care
Focus on corporate mandates



Crabtree BF, Nutting PA, Miller WL, McDaniel RR, Stange KC, Jaen CR, Stewart EE. Primary care practice transformation is hard work: Insights from a 15 year developmental program of research. Medical Care, 49(Dec Suppl): S28-35, 2011.

Observation InterventionDOPC STEP-UP
IMPACT
Direct Observation of Primary Care (1994-1997)
NCI R01
Study To Enhance Prevention by Understanding
Practice (1996-2000)NCI R01
Insights from MultimethodPractice Assessment of Change
over Time (2001-2004)NCI R01
P&CDPrevention & Competing
Demands in Primary Care (1996-1999)
AHRQ R01ULTRA
Using Learning Teams for Reflective
Adaptation (2002-2007)NHLBI R01
SCOPESupporting Colorectal
Outcomes through Participatory Enhancements
(2005-2010)NCI R01
46
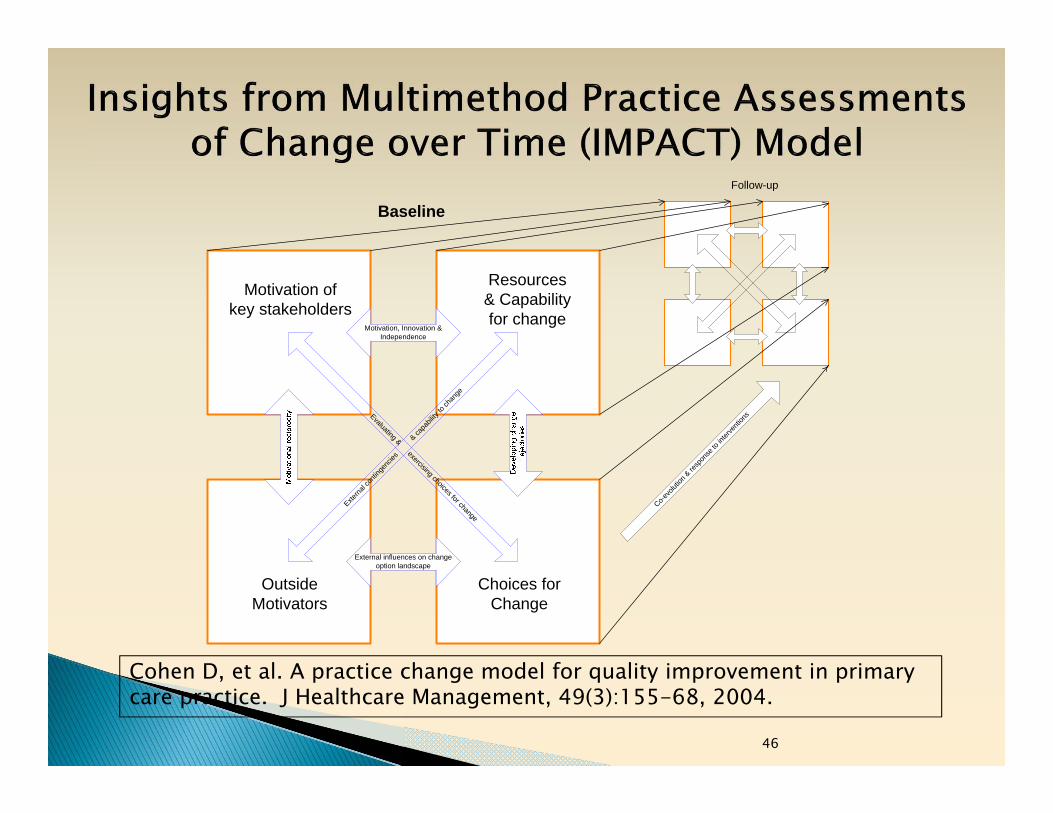
External influences on change option landscape
Motivation, Innovation & Independence Evaluating & exercising choices for change
Externa
l con
tinge
ncies
& ca
pabil
ity to
chan
ge
Motivation of key stakeholders
Resources & Capability for change
OutsideMotivators
Choices for Change
Baseline Follow-up
Co-evo
lution
& re
spon
se to
inter
venti
ons
Cohen D, et al. A practice change model for quality improvement in primary care practice. J Healthcare Management, 49(3):155-68, 2004.
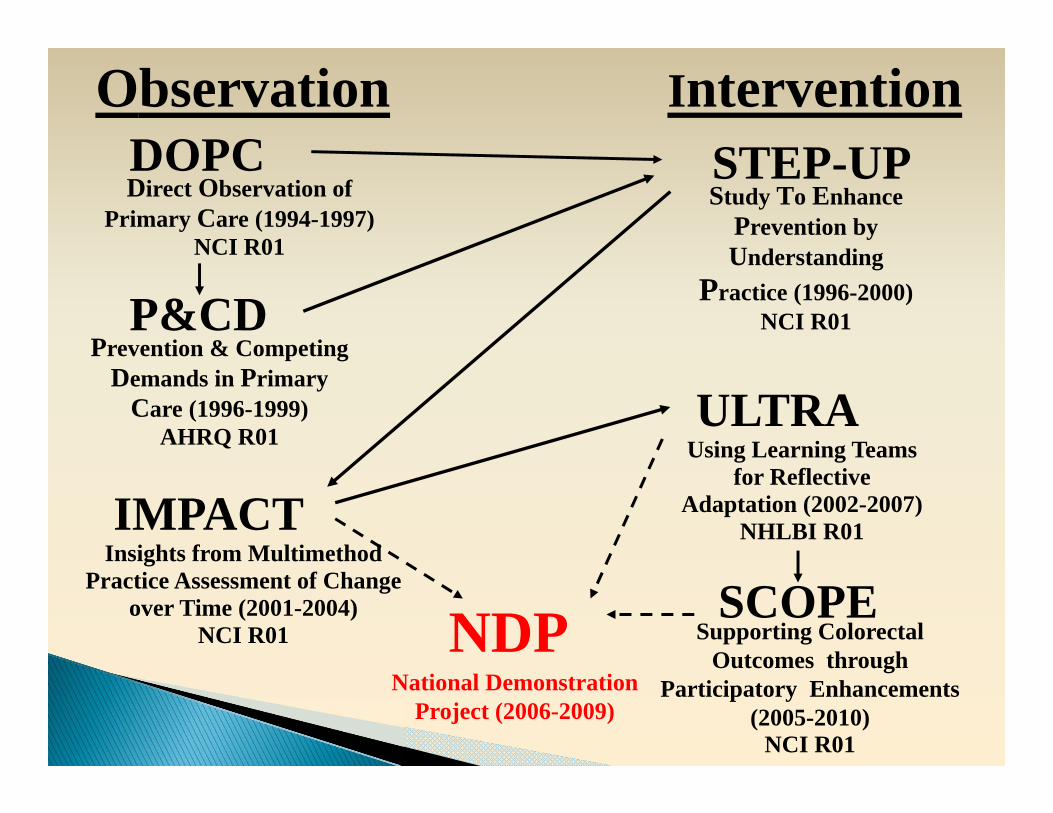
Observation InterventionDOPC STEP-UP
IMPACT
Direct Observation of Primary Care (1994-1997)
NCI R01
Study To Enhance Prevention by Understanding
Practice (1996-2000)NCI R01
Insights from MultimethodPractice Assessment of Change
over Time (2001-2004)NCI R01
P&CDPrevention & Competing
Demands in Primary Care (1996-1999)
AHRQ R01ULTRA
Using Learning Teams for Reflective
Adaptation (2002-2007)NHLBI R01
NDPNational Demonstration
Project (2006-2009)
SCOPESupporting Colorectal
Outcomes through Participatory Enhancements
(2005-2010)NCI R01

Practices are complex systems Change is HARD RELATIONSHIPS matter LEADERSHIP is key PERSONAL transformation is needed There is no such thing as “Plug ‘n Play” The promise of the patient-centered
medical home remains elusive AND, the healthcare world is rapidly
changing and our thinking needs to extend beyond the individual practice.


Does community ownership change the model? What is the impact of hierarchical corporate
governance? What is the appropriate corporate scale? (local,
regional, national) What kind of ACO can be family and patient-
centered? (physician led, hospital led, community led)
What is a Patient-Centered Health Care Neighborhood?
Current physicians (and others) must transform themselves.
Future professionals need to learn the basics of leadership, teamwork, and organizational behavior.
New professional roles need to be conceptualized and programs created to train for the future.
Cultures of teamwork and collaboration need to be established within and across primary care and specialty practices, as well as throughout the neighborhood.
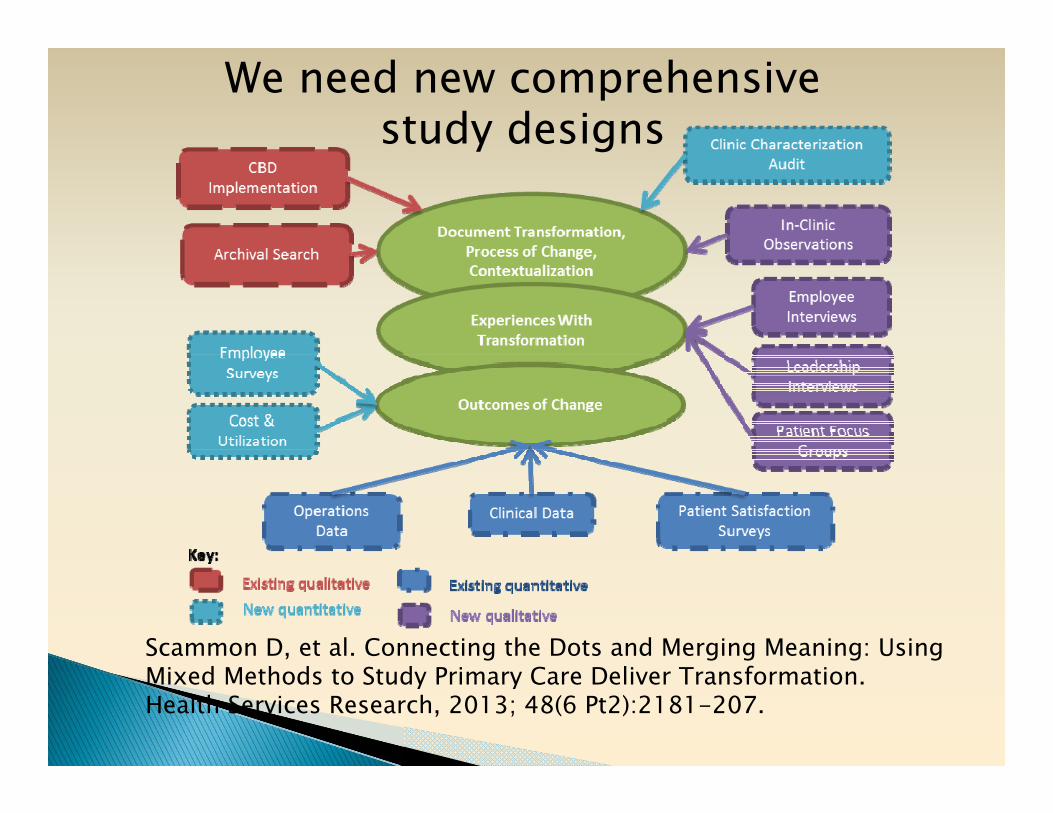
Scammon D, et al. Connecting the Dots and Merging Meaning: Using Mixed Methods to Study Primary Care Deliver Transformation. Health Services Research, 2013; 48(6 Pt2):2181-207.
We need new comprehensive study designs